
The Stomach…IT ’ S A G UT FE E L ING
MA UR E EN ST R E SINSHE, B SN, R N

SAY WHAT?
paunchgizzard

OBJECTIVES1. Describe the anatomy and physiology of the stomach
Structure of the stomach Function of the stomach Substances secreted by the by the stomach
2. Identifies disease of the stomach Contributing factors Symptoms Diagnosis and treatment
3. Identifies pharmacological agents used to treat diseases of the stomach Drug classifications Mechanism of action Therapeutic use

What is it?
J
Know Your Anatomy
Red face when blushing?
Your stomach lining turns red too!

Cardia
Upper opening of the stomach, where the esophagus enters
Cardiac mucosa primarily contains mucus-secreting cells that form a columnar epithelium
Just below the gastroesophageal junction
Transition point where the stratified squamous epithelium assumes the columnar structure

Fundus
The word “fundus” literally means “bottom”
Bulging part of the stomach above the level of the esophagus opening
Stores undigested food and gases released from chemical digestion

Body
Largest portion of the stomach Mucosa of the body of the
stomach has much deeper and less coiled gastric glands than that of the cardia.
Where mechanical and chemical digestive processes occur

Antrum
Lowermost part of the stomach which looks like a funnel.
Its wide end joins the lower part of the stomach body while the narrow part makes a connection with the pyloric canal.

Pylorus
Narrowest portion of the stomach Measures roughly an inch in
diameter with thick loops of smooth muscles surrounding it
Pyloric canal makes a connection of the stomach with the duodenum, measuring about 2 to 3 cm in length
Pyloric orifice is the opening or passage between the stomach and duodenum.

LayersSerosa >Covers exterior of the stomach
Muscle layers >• Comprised of 3 different
types of muscle fibers• Contraction of these fibers
responsible PERISTALSIS
Submucosa >• Connective tissue, blood
vessels, lymphatics & nerves
Mucosa >• Secretes mucus https://upload.wikimedia.org/wikipedia/commons/6/64/Illu_stomach2.jpg

Physiology
• Food enters into stomach through the esophagus & lower esophageal sphincter
Storage
• Endocrine and exocrine functions
• Secretes acids, mucous & digestive enzymes
Secretion• Mechanical Digestion
• Chemical Digestion
Digestion
• Regulate production stomach acid
• Gradual release of food into the small intestine
Hormonal Control

STORAGE
• Hold an average of 1- 2 L of food & drink during the average meal
• Can expand to hold 3 -4 L of food & drink when we overdo it
• Stomach distention to its maximum size can make digestion difficult, not allowing for proper contractions
• Stores food as digestion begins • Pyloric sphincter control gastric emptying and the
release of chyme into duodenum, maximizing the digestion and absorption of nutrients in the intestines

EXOCRINE SECRETION
Gastric Juice • a mixture of mucus, hydrochloric acid, and digestive
enzymes that promotes digestion.
Mucus • Spreads across the surface of the mucosa to coat the
lining of the stomach with a thick, acid- and enzyme-resistant barrier.
• Stomach mucus is also rich in bicarbonate ions, which neutralize the pH of stomach acid.
Inner stomach lining is covered with layers of fresh mucus
every 2 weeks

EXOCRINE SECRETION
Gastric PitProduces Parietal Cells & Chief Cells

EXOCRINE SECRETION
Parietal Cells (“fried egg”)• Intrinsic factor and Hydrochloric Acid• Intrinsic factor is a glycoprotein that binds to the
vitamin B12 in the stomach and allows the vitamin to be absorbed in the small intestine. Vitamin B12 is an essential nutrient for the formation of red blood cells.
• Hydrochloric acid protects the body by killing pathogenic bacteria naturally found in food. Helps to digest proteins by denaturing them into an unfolded shape that is easier for enzymes to digest. The protein digesting enzyme pepsin is activated by exposure to hydrochloric acid inside the stomach.
www.dreamstime.com

EXOCRINE SECRETION
Chief Cells• Pepsinogen and Gastric Lipase• Pepsinogen is precursor molecule of the very potent
protein-digesting enzyme pepsin. • Because pepsin would destroy the chief cells that produce it, it is secreted in its
inactive pepsinogen form. When pepsinogen reaches the acidic pH found in the stomach thanks to hydrochloric acid, it changes shape and becomes the active enzyme pepsin. Pepsin then breaks dietary proteins into their amino acid building blocks. Hydrochloric acid protects the body by killing pathogenic bacteria naturally found in food. Helps to digest proteins by denaturing them into an unfolded shape that is easier for enzymes to digest. The protein digesting enzyme pepsin is activated by exposure to hydrochloric acid inside the stomach.
• Gastric lipase is an enzyme that digests fats by removing a fatty acid from a triglyceride molecule.

ENDOCRINE SECRETION
G Cells• Found at the bottom of the gastric pits. • Release the hormone gastrin into the
bloodstream in response to many stimuli• signals from the vagus nerve; • presence of amino acids in the
stomach from digested proteins• stretching of the stomach wall
during a meal.

These cells work together
Junqueira’s Basic Histology, Chapter 15

MECHANICAL & CHEMICAL DIGESTION
Mechanical digestion physically divides a mass of food into smaller masses
• Mixing action of smooth muscles of stomach wall
• Mix food bolus with gastric juice > production of CHYME
Chemical digestion of large molecules into small subunits
• Gastric lipase splits triglyceride fats
• Pepsin breaks down proteins
• Completed when chyme reaches intestines

HORMONAL CONTROLRegulates the production of stomach acid and the release of food into the duodenum.
HORMONE ACTION
Gastrin
Produced by the G cells of the stomach. Increases activity of the stomach by stimulating increased gastric juice production, muscle contraction, and gastric emptying through the pyloric sphincter.
Cholecystokinin (CCK)
Produced by the mucosa of the duodenum. A hormone that acts to slow gastric emptying by contracting the pyloric sphincter. CCK is released in response to food rich in proteins and fats, which are difficult for the body to digest.
Secretin
Produced by the duodenum's mucosa. Responds to the acidity of chyme entering the duodenum from the stomach. Travels through the bloodstream to the stomach where it slows the production of gastric juice by the exocrine glands of the mucosa. Promotes the production of pancreatic juice and bile. Protects the intestines from the damaging effects of acidic chyme.

MYTH OR FACT?
Most elders tell you not to swallow chewing gum because it stays in the stomach for 7 years
Our digestive tract cannot break down the chewing gum’s synthetic resin but it is highly efficient enough to it pass all the way through to the end

Deranged function in an organ due to a
disease.
Pathophysiology

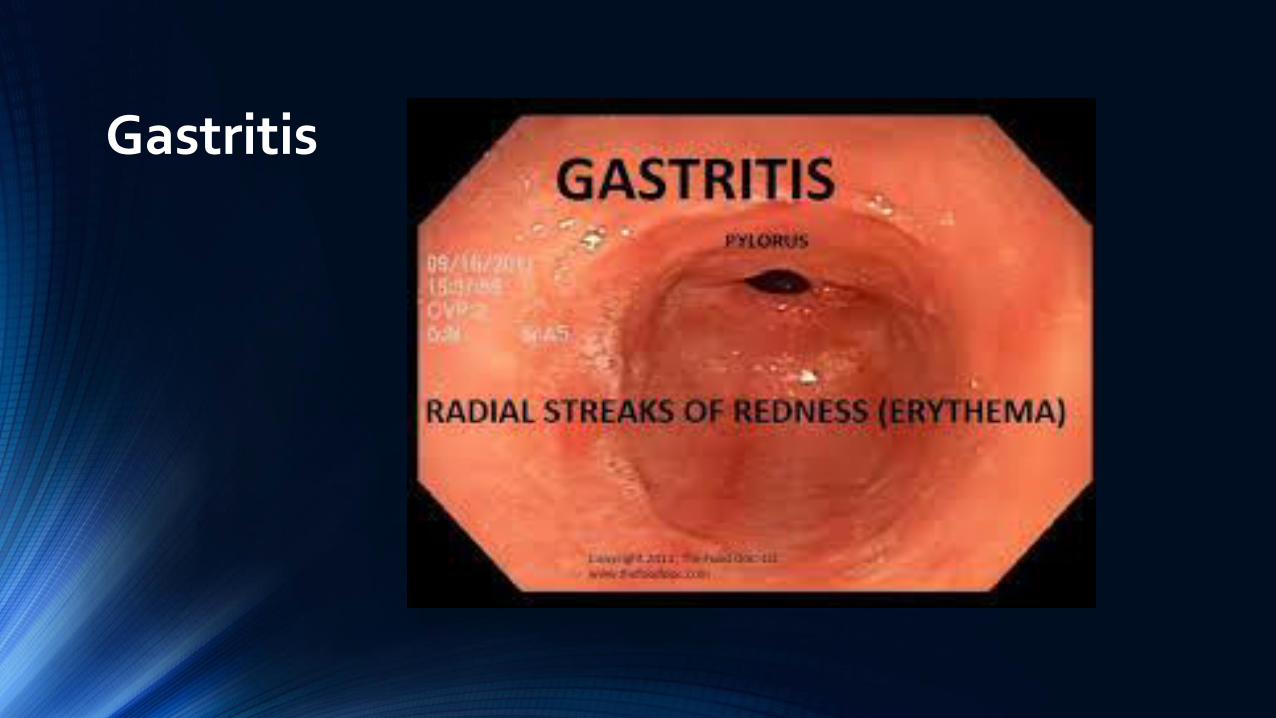
Gastritis
Inflammation/Irritation/Erosion of the gastric mucosa
Excessive alcohol useHeavy use of NSAIDsSmokingChemotherapeutic drugsSystemic Infection (Salmonella, CMV)Severe stress – trauma, surgery\Ingestion of corrosives (acid/lye)Radiation
Classified according to inflammatory pattern: Acute, Chronic or part specialized condition

Chronic Gastritis >Non-erosive, non-specific gastritis (NNG)Normal agingGastric UlcersPernicious anemiaGastric cancerH. pylori
Acute Gastritis > Erosive, hemorrhagicSerious illnessAlcoholismTobacco Use
Gastritis

Disease associated gastritis
Ménétrier’s disease
Eosinophilic gastritis
Sarcoidosis
Infections
http://www.journalnma.org/article/S0027-9684(15)30608-8/pdf

Nausea or recurring upset stomach
Abdominal Bloating and/or Pain
Vomiting
Indigestion
Burning or gnawing feeling in the stomach between meals or at night
Hiccups
Loss of appetite
Vomiting blood or coffee ground-like material
Black, tarry stools
Many patients may have no symptoms
Gastritis

Diagnosis
Upper Endoscopy
Blood Tests – serum gastrin, gastric analysis
TreatmentReview contributing factors patient medications, sepsis, H. pyloriStop smoking/alcohol intakeEliminate food triggersAntacids, Sucralfate, H2 Blockers, PPI, AntibioticsAntiemetics
Gastritis
Gastritis
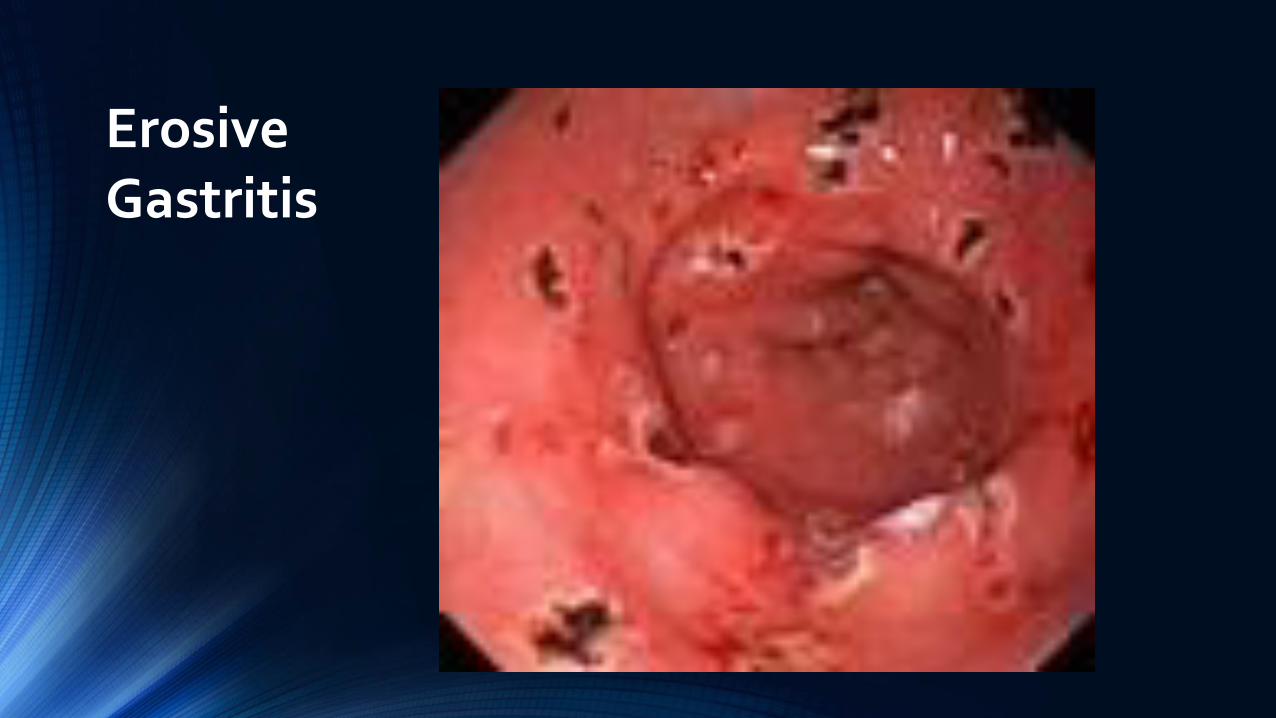
Erosive Gastritis

Stress Ulcers
Gastric mucosal stress erosions associated with serious illness
Severe traumaSepsisUndergoing treatment for serious illnessHave significant burn injurySustained intracranial trauma – craniotomy/TBI (Cushing’s Ulcer)Chronic NSAID or alcohol use

Stress Ulcer Cushing’s Ulcer
• Deep and of full-thickness• Prone to perforation• Ulcers are located in stomach lining• Due to elevated intracranial pressure, results in
vagal nuclei stimulation causing elevated gastric acid secretion

Stress Ulcer Curling’s Ulcer
• Acute gastric erosions• Complication of sever burns
• Reduced plasma volume → ischemia and cell
necrosis of gastric mucosa

Stress UlcersSymptoms
Massive upper GI Bleeding Can occur within hours of initial injuryRarely cause ulcer S &S prior to start of bleeding

Stress Ulcer Treatment
Control of Bleeding
Correcting Shock
Treatment of underlying disorder
Endoscopy
Angiographic embolization

Gastric Varices (GV)
Large gastric varices located at the fundus
Portal Hypertension may lead to development of collateral circulation
Commonly a result of alcoholic cirrhosis Compared with esophageal varices,
gastric varices are larger, more extensive, and lie deeper in the submucosa.
2/3 of patients with esophageal varices also have gastric varices
Accounts for 10-30% of all variceal hemorrhage
High mortality rate 35-90% will experience recurrent bleeding

Gastric Varices Management
Hemodynamically stabilize the patient Stop acute bleeding Reduce portal pressure

Gastric Varices Sarin Classification

Gastric Varices Treatment
Gastric Variceal Band Ligation
Second alternative therapy to obturation High rate of re-bleeding from feeding vessels Repeat therapy at 1-2 week intervals until eradication

Gastric Varices Treatment
Gastric Variceal Sclerotherapy
Due to high volume of blood flow less successful treatment than in esophageal varices (EV)
Typically requires larger volume of sclerosant than for EV leads to more side effects Retrosternal/Abominal pain Ulcerations (causes ~50% of re-bleeding) Perforations
Control bleeding in 60-100% cases with re-bleeding rates up to 90% Not appropriate for fundal varices d/t ↓ rate hemostasis

Gastric Varices Treatment
Gastric Variceal Obturation
Essentially “flushing glue” into the varix until it is hard to palpation 2-octyl cyanoacrylate has been approved by the FDA for skin closure and
has also been used for the management of gastric varices → rapid polymerization on contact with living tissues
May be performed with endoscopic ultrasound guidance (↓complications)
Weeks to months after the injection, the mucosa overlying the glue cast sloughs off and the plug is extruded into the stomach.
Initial hemostasis rates of over 90% can be achieved. Thrombotic complications: cerebral embolization & stroke, portal vein
embolization, coronary & pulmonary emboli

Gastric Varices Treatment Transjugular Intrahepatic
Portosystemic Shunt (TIPS) Considered for refractory GV bleeding Primary hemostasis rate of TIPS for acute
GV bleeding is 92.3%. Other studies showed initial hemostasis of TIPS for acute refractory GV bleeding is between 87% and 100%
Complications of TIPS are encephalopathy and shunt stenosis/occlusion, with post-TIPS encephalopathy occurring in 4-16% of patients

Hiatal Hernia
Weakening of the muscles of the diaphragm around the esophagus
Incidence increases with age
Approximately 60% of individuals
aged 50 or older have a hiatal hernia
More common in women vs. men
Pregnancy, obesity, abdominal ascites can be contributing factors

Hiatal HerniaClassifications
“Sliding”Most commonWidening of the muscular hiatal
tunnel and circumferential laxity of the phrenoesophagealligament
Migration of GE junction into thoracic cavity
Associated with reflux disease
https://clinanat.com/100-mtd/428-phrenoesophageal-ligament

Hiatal HerniaClassifications
Paraesophageal hiatal hernia Herniation of gastric fundus
into the thoracic cavityalongside the esophagus
Defect in the phrenoesophageal ligament & GE Junction remains fixed
Progressive enlargement

Hiatal HerniaClassifications
Mix of Types I & IIPhrenoesophageal ligament
stretchesHerniation of both GE
Junctions and stomach“Sliding” element to Type II
hernia

Hiatal HerniaClassifications
Upside down stomachLarge defect in the
phrenoesophageal ligamenetColon, spleen, pancreas and
small intestine may enter the hernia sac.

Hiatal HerniaSymptoms
AsymptomaticOR
GERDDysphagiaChronic coughRegurgitation
AsymptomaticOR
Vague/intermittentr/t ischemia or obstructionEpigastric/substernal painPostprandial fullnessSubsternal fullnessNauseaRetchingAnemia
Mechanical ObstructionDyspnea
GERD Dyspepsia
Substernal Pain

Hiatal HerniaDiagnosis
EndoscopyCXREsophagram/Barium SwallowEsophageal ManometrypH Capsule > Hiatal Hernia Type ICBC → anemiaCourtesy of David Y. Graham, MD

Hiatal HerniaComplications
Iron deficiency anemia r/t intermittent
bleeding from associated
esophagitis
erosions (Cameron ulcers)
discrete esophageal ulcer
Incarcerated hiatal hernia

Hiatal HerniaTreatment
No treatmentElevate head of bed 6 inchesAvoid lying down after mealsAvoid foods that trigger heartburn (chocolate,
onions, spicy foods, citrus fruits and tomato-based foods.
Avoid alcoholStop smokingWeight loss Stress reductionsProton Pump Inhibitors & H2 receptor blockersSurgical Intervention
Nissen Fundoplicaiton

Gastric Antral Vascular Ectasia (GAVE)

Gastric Antral Vascular EctasiaSymptoms
Gastrointestional Bleeding
Anemia
Hematemesis
Melena

Gastric Antral Vascular Ectasia
Exact cause unknown
Often associated with other chronic conditions(autoimmune diseases, atrophic gastritis, cirrhosis, scleroderma, pernicious anemia, portal hypertension, vascular disease, diabetes mellitus, chronic renal failure)
Absence of cirrhosis: 71% female, average age 73, presenting with occult blood loss leading to transfusion-dependent chronic iron-deficiency anemia, severe acute upper gastrointestinal bleeding, and nondescript abdominal pain.

Gastric Antral Vascular EctasiaDiagnosis
Visualized through endoscopy
Other tests may be used to help confirm diagnosis CT Scan and/or tagged red blood cell scan Endoscopic Ultrasound

Gastric Antral Vascular EctasiaTreatment
Argon plasma coagulation at site of bleeding
Treat underlying cause
Treat resulting anemia – possible blood transfusionshttp://www.gastrointestinalatlas.com/english/Watermelon_Stomach.html

Motor Dysfunctions:Dumping Syndrome
Rapid gastric emptying that may start 15-30 minutes post meal
Causes: Can result from gastric surgeries that include vagotomy
Symptoms: anxiety, weakness, dizziness, tachycardia, diaphoresis, flushing, abdominal cramping, diarrhea. Reactive hypoglycemia approximately 90- 120 minutes post meal lead to decreased level of consciousness.
Treatment: focuses on slowing intestinal delivery of nutrients/minimizing release of endogenous vasoactive peptides
Recommendations: High fat/high protein/low carbohydrate meals, minimal fluids while eating

Motor Dysfunctions:Gastroparesis
Delayed gastric emptying Idiopathic or commonly associated with diabetesCauses: Outlet obstruction of stomach (tumor/ulcer)
Neurological defect to pyloric sphincterDysrhythmic contractions of stomach
Symptoms: nausea and vomiting, vague stomach pain, early satiety, weight loss, fluctuating blood sugar
Diagnosis: endoscopy, barium swallow, radioisotope gastric emptying scan
Treatment: eat several small meals low in fat/fiber/roughage, pro-motility agent (Reglan), jejunal feeding tube, gastric pacemaker
Pacemaker Region

Bezoars:Phytobezoar
Continuous and prolonged ingestion of indigestible materials
Composed of indigestible fruit and vegetable fibers
Occur in patients with impaired gastric motility or digestion, following gastric surgery, low gastric acidity, and loss of normal pyloric function can all contribute to phytobezoar formation.
Symptoms: epigastric pain or discomfort, N&V, early satiety, weight loss, diarrhea, dysphagia, or upper gastrointestinal ulcerations and hemorrhage.Treatment: Cellulase/Papain, Reglan, surgical removal, endoscopic mechanical fragmentation

Bezoars:Trichobezoar
Einstein (São Paulo) vol.13 no.4 São Paulo Oct./Dec. 2015 Epub Sep 18, 2015
Composed of hair 90% occur in women
under age 20 Referral for a psychiatric
consultation
Continuous and prolonged ingestion of indigestible materials

Copyright © 2008 Hayashi et al; licensee BioMed Central Ltd.

PHARMACOLOGY

Proton Pump Inhibitors (PPI’s)
Pantoprazol (Protonix)
Esomeprazole (Nexium)
Lansoprazole (Prevacid)
Dexlonsprazole (Dexilant)
Omeprazol (Prilosec)

Proton Pump Inhibitors (PPI’s)
Work by reducing the production of acid by blocking the enzyme in the wall of the stomach that produces acid.
Different PPI’s are similar in action but may differ in how they are metabolized by the liver. Generally well tolerated.
Most common side effects include: Headache, diarrhea, constipation, abdominal pain, fever, nausea, rash
Complications: C. difficile, osteoporosis related hip/wrist/spine fractures, ↓ Vit. B12
absorption, hypomagnesemia

Proton Pump Inhibitors (PPI’s)
Drug Interactions: Ketoconazole and Digoxin need stomach acid to be present. PPI’s reduce
absorption & blood concentration of Ketonconazole and increase concentration of digoxin (toxicity)
May reduce liver metabolization of some drugs leading to an increased blood concentration. Omeprazole most likely to interfere with Diazepam, Warfarin and Phenytoin. Also blocks the conversion of Clopidogrel(Plavix) to its active form.

Pantaprazole Lansoprazole Esomeprazole Dexlonsprazole Omeprazole
GERDErosive EsophagitisZollinger-Ellison
GERDErosive EsophagitisDuodenal Ulcer Gastric UlcerNSAID gastric ulcerPeptic ulcer - H.Pylorieradication
GERDErosive EsophagitisNSAID ulcer risk reductionPeptic ulcer - H.Pylorieradication
GERDErosive EsophagitisHeartburn
Errosive EsophagitisGERDHeartburnBengin Gastric UlcerDuodenal UlcerZollinger-Ellison
Proton Pump Inhibitors (PPI’s) -Indications

H-2 Receptor Antagonists
Ranitidine (Zantac)
Cimetidine (Tagamet)
Famotidine (Pepcid)
Nizatidine (Axid)

H-2 Receptor Antagonists
Works by blocking the action of histamine on the parietal cells, reducing the production of acid.
Most common side effects include: Diarrhea, headache, dizziness, fatigue, muscle pain, rash, impotence,
mild gynecomastia, leukopenia, thrymbocytopenia Complications:
Drinking alcoholic beverages while taking an H2-receptor antagonist has been reported to increase the blood levels of alcohol
Cigarette smoking tends to decrease the effect of H2-blockers by increasing the amount of acid produced by the stomach

H-2 Receptor Antagonists - IndicationsFamotidine Cimetidine Ranitidine Nizatidine
GERDEsophagitisDuodenal UlcerZollinger-Ellison(pathological hypersecretoryconditions)
GERDHeartburnDuodenal UlcerGastric Ulcer
Esophageal RefluxEsophagitisPeptic Ulcer DiseaseDuodenal UlcerZollinger-Ellison
GERDHeartburnAcid IndigestionPeptic Ulcer DiseaseDuodenal Ulcer

Antacids
Neutralize stomach acidContain ingredients such as aluminum, calcium, or magnesium
which act as bases (alkalis) to counteract the stomach acid and lower pH.
Mylanta, Milk of Magnesia, TUMS, Caltrate, Gavison, MaaloxWork to reduce acid reflux, heartburn or dyspepsiaMay not be suitable for sodium restricted dietsShort term use

Carafate (Sulcarafate) – Anti-ulcer
Works mainly in the lining of the stomach by adhering to ulcer sites and protecting them from acids, enzymes, and bile salts.
Sucralfate can heal an active ulcer, but it will not prevent future ulcers from occurring.
Take Carafate on an empty stomach, at least 1 hour before or 2 hours after a meal
Avoid taking any other medications within 2 hours before or after taking Carafate
Common Carafate side effects may include:nausea, vomiting, upset stomach; stomach pain; constipation, diarrhea; mild itching or skin rash; sleep problems (insomnia);dizziness, drowsiness, spinning sensation; headache; or back pain.









