
TKCC/Garvan Cancer Biology Seminars
Principles of multidisciplinary musculoskeletal tumour management
Prof David Thomas
4th March 2016

An state-of-the-art overview of: • Australian epidemiology • Etiology • Risk factors • Pathology • Staging • Treatment
Aims of presentation
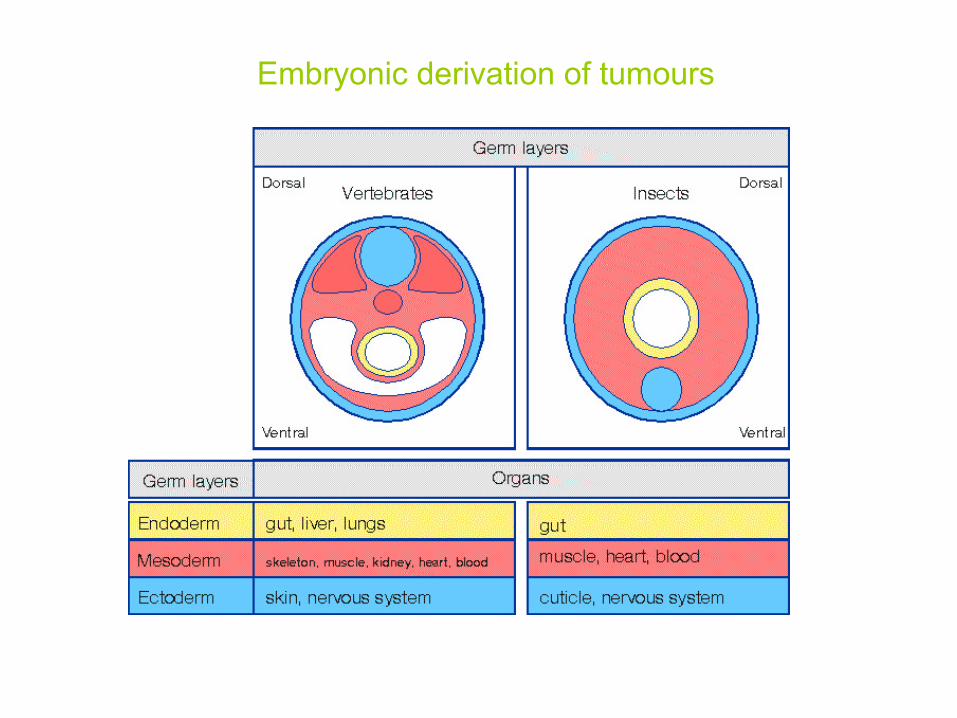
Embryonic derivation of tumours
Unique features of sarcomas
1. Rare and diverse 2. Younger patients 3. Patterns of spread typically non-lymphatic,
frequently metastasise to lungs (>80%) 4. Two genetic patterns
• Chromosomal instability/aneuploidy • Signature lesions with relative diploidy
5. Two (at least) pathologic groups • Neuroectodermal origin (SRBCT) • Mesodermal origins (spindle cell tumours)
6. Chemo- and radio-resistance (allegedly) 7. Scarcity of clinical trials

Sarcomas: malignant tumours of soft tissues and bone
Uncommon: 15% of childhood cancers
1% of adult cancers
853 sarcomas in Australia in 1988
Benign STS 100 times more common than malignant tumours Benign:
99% superficial to deep fascia, 95%< 5cm diamter
30% lipomas
30% fibrohistiocytic and fibrous tumours
10% vascular tumours
5% PNST

Clinical presentation Often painless Sometimes long-standing Deep to deep fascia >5cm
Courtesy of Peter Choong
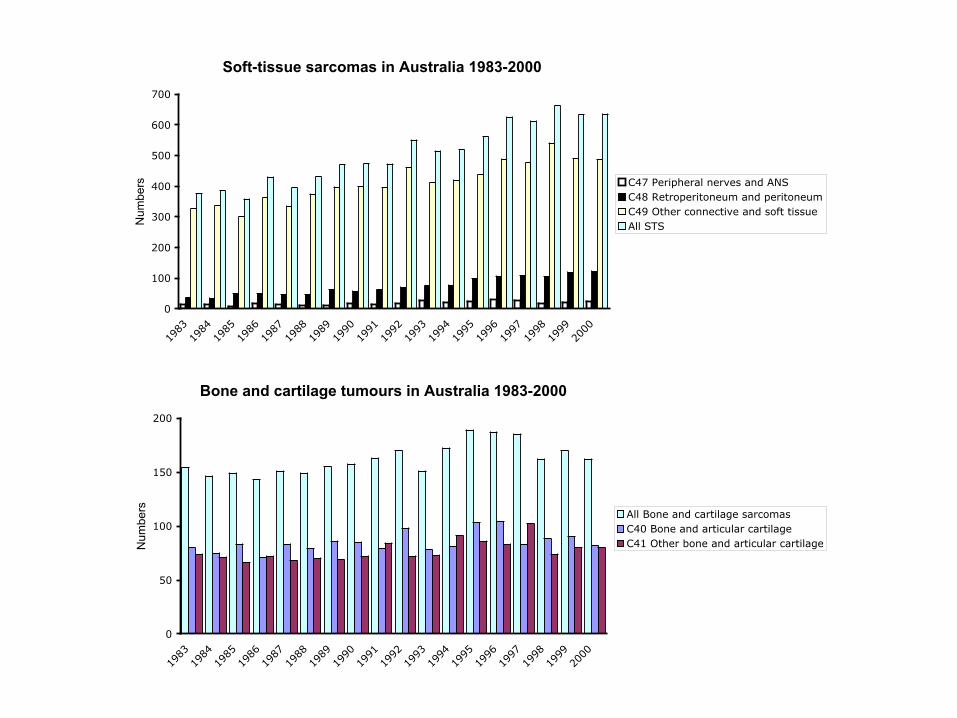
Soft-tissue sarcomas in Australia 1983-2000
0
100
200
300
400
500
600
700
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
Numbers C47 Peripheral nerves and ANS
C48 Retroperitoneum and peritoneumC49 Other connective and soft tissueAll STS
Bone and cartilage tumours in Australia 1983-2000
0
50
100
150
200
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
Numbers All Bone and cartilage sarcomas
C40 Bone and articular cartilageC41 Other bone and articular cartilage

Overview
Diagnosis and staging Imaging key biopsy critical
Multidisciplinary management
Surgery is critical Adequate margins Limb-preservation Reconstruction
Adjuvant treatment
Radiotherapy for STS Chemotherapy
PNET/Ewings sarcoma/SRBCT Osteosarcoma Relatively controversial:
high-risk STS where RT impractical evidence of chemosensitivity (eg Synovial cell sarcoma)
Supportive care AYA Rehabilitation and survivorship


Difficult and uncertain Pathologic review
ECOG sarcoma trials (424 patients): 10% not sarcoma 14% disagreement regarding subtype
SWCG trials (216 patients): 6% not sarcoma 27% subtype incorrect
Scandinavian Sarcoma Group 20% of diagnoses disputed
Sarcoma NOS or Malignant fibrous histiocytoma
Disputed entity MFH represents de-differentiated forms of other defined entities (Fletcher, 2001) OR MFH is a discrete category in its own right
Histopathology and sarcomas

(Fletcher et al., 2001, JCO)

Genetics of sarcomas

Importance of molecular subtype
The advent of targeted therapies makes accurate classification essential (Baselga and Arteaga, 2004)
GIST KIT Imatinib Dermatofibroma protruberans PDGFR Imatinib NSCLC EGFR Gefitinib PEComa mTOR Everolimus ASPS angiogenesis Cediranib Giant cell tumor of bone RANKL Denosumab PVNS/dTGCT CSF1 PLX3397/RG7155
Clear impact on efficacy and tolerability Implications for rational clinical trial design?

Genetics of sarcomas

Congenital syndromes in sarcomas Disorder Inheritance Locus Gene Tumours
Albright osteodystrophy AD 20q13 GNAS1 Ectopic calcification and osteomasCarney complex AD 17q23-24, 2p16 PRKAR1AK Myxomas, schwannomasMazabrayd syndrome Sporadic 20q13 GNAS1 Polyostotic fibrous dysplasia, osteosarcoma, myxomasMcCune Albright syndrome Sporadic 20q13 GNAS1 Polyostotic fibrous dysplasia, osteosarcoma, myxomasOllier's disease Sporadic 3p21-22 PTHR1 Enchondromas, chondrosarcomasRubinstein-Taybi syndrome AD 16p13 CREBBP Myogenic sarcomasBannayan-Riley-Ruvucalba syndrome AD 10q23 PTEN Lipomas, haemangiomasCowden disease AD 10q23 PTEN Lipomas, haemangiomasRothmund-Thomson syndrome AR 8q24 RECQL4 OsteosarcomasBloom syndrome AR 15q26 BLM OsteosarcomasWerner syndrome AR 8p11-12 WRN Various bone and STSBeckwith-Wiedemann syndrome sporadic/AD 11p15 Complex (IGF2,
p57KIP2)Emb. Rhabdomyosarcomas, myxomas, fibromas
Familial Paget's disease of bone AD 18q21, 5q31, 5q35 TNFRSF11A OsteosarcomasFamilial expansile osteolysis AD 18q21 TNFRSF11A OsteosarcomasLi-Fraumeni syndrome AD 17p13, 22q11 TP53, CHEK2 Osteosarcomas, rhabdomyosarcomas, other STSLanger-Giedion syndrome Sporadic 8q24 EXT1 Osteochondromas, chondrosarcomasMultiple osteochondromas AD 8q24, 11p11-12 EXT1, EXT2 Osteochondromas, chondrosarcomasNeurofibromatosis I AD 17q11 NF1 Neurofibromas, MPNSTNeurofibromatosis II AD 22q12 NF2 SchwannomasFamilial adenomatous polyposis AD 5q21 APC Craniofacial osteomas, desmoid tumourFamilial infiltrative fibromatosis AD 5q21 APC Desmoid tumoursRetinoblastoma AD 13q14 RB1 Osteosarcomas, STSRhabdoid predisposition syndrome AD 22q11 SMARCB1 Malignant rhabdoid tumoursFamilial chordoma AD 7q33 ChordomasCostello syndrome sporadic RhabdomyosarcomasDiaphyseal meduallry stenosis with MFH AD 9p21-22 MFH of boneFamilial multiple lipomas AD LipomasSymmetrical lipomatosis Sporadic LipomasMaffucci syndrome Sporadic Enchondromas, chondrosarcomas, haemangiomas,
angiosarcomasMyofibromatosis AR MyofibromasProteus syndrome Sporadic LipomasVenous malformations with glomus cells AD 1p21-22 Glomus tumours
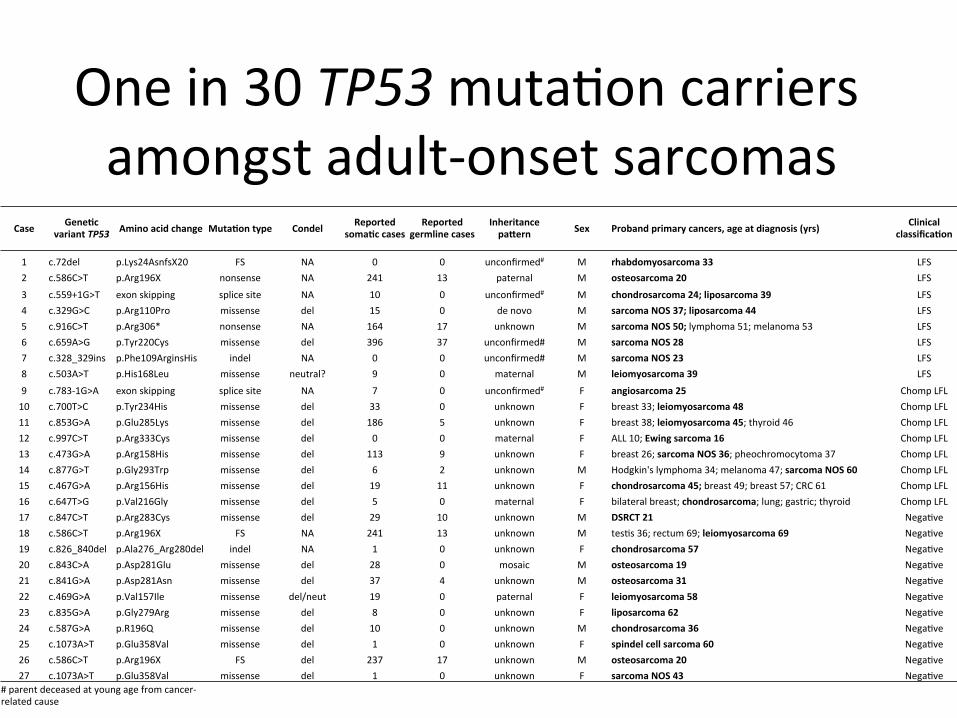
Onein30TP53muta,oncarriersamongstadult-onsetsarcomas
Case Gene(cvariantTP53 Aminoacidchange Muta(ontype Condel Reported
soma(ccasesReported
germlinecasesInheritancepa;ern Sex Probandprimarycancers,ageatdiagnosis(yrs) Clinical
classifica(on
1 c.72del p.Lys24AsnfsX20 FS NA 0 0 unconfirmed# M rhabdomyosarcoma33 LFS2 c.586C>T p.Arg196X nonsense NA 241 13 paternal M osteosarcoma20 LFS
3 c.559+1G>T exonskipping splicesite NA 10 0 unconfirmed# M chondrosarcoma24;liposarcoma39 LFS4 c.329G>C p.Arg110Pro missense del 15 0 denovo M sarcomaNOS37;liposarcoma44 LFS5 c.916C>T p.Arg306* nonsense NA 164 17 unknown M sarcomaNOS50;lymphoma51;melanoma53 LFS6 c.659A>G p.Tyr220Cys missense del 396 37 unconfirmed# M sarcomaNOS28 LFS7 c.328_329ins p.Phe109ArginsHis indel NA 0 0 unconfirmed# M sarcomaNOS23 LFS8 c.503A>T p.His168Leu missense neutral? 9 0 maternal M leiomyosarcoma39 LFS
9 c.783-1G>A exonskipping splicesite NA 7 0 unconfirmed# F angiosarcoma25 ChompLFL10 c.700T>C p.Tyr234His missense del 33 0 unknown F breast33;leiomyosarcoma48 ChompLFL11 c.853G>A p.Glu285Lys missense del 186 5 unknown F breast38;leiomyosarcoma45;thyroid46 ChompLFL12 c.997C>T p.Arg333Cys missense del 0 0 maternal F ALL10;Ewingsarcoma16 ChompLFL13 c.473G>A p.Arg158His missense del 113 9 unknown F breast26;sarcomaNOS36;pheochromocytoma37 ChompLFL14 c.877G>T p.Gly293Trp missense del 6 2 unknown M Hodgkin'slymphoma34;melanoma47;sarcomaNOS60 ChompLFL15 c.467G>A p.Arg156His missense del 19 11 unknown F chondrosarcoma45;breast49;breast57;CRC61 ChompLFL16 c.647T>G p.Val216Gly missense del 5 0 maternal F bilateralbreast;chondrosarcoma;lung;gastric;thyroid ChompLFL17 c.847C>T p.Arg283Cys missense del 29 10 unknown M DSRCT21 Nega,ve18 c.586C>T p.Arg196X FS NA 241 13 unknown M tes,s36;rectum69;leiomyosarcoma69 Nega,ve19 c.826_840del p.Ala276_Arg280del indel NA 1 0 unknown F chondrosarcoma57 Nega,ve20 c.843C>A p.Asp281Glu missense del 28 0 mosaic M osteosarcoma19 Nega,ve21 c.841G>A p.Asp281Asn missense del 37 4 unknown M osteosarcoma31 Nega,ve22 c.469G>A p.Val157Ile missense del/neut 19 0 paternal F leiomyosarcoma58 Nega,ve23 c.835G>A p.Gly279Arg missense del 8 0 unknown F liposarcoma62 Nega,ve24 c.587G>A p.R196Q missense del 10 0 unknown M chondrosarcoma36 Nega,ve25 c.1073A>T p.Glu358Val missense del 1 0 unknown F spindelcellsarcoma60 Nega,ve26 c.586C>T p.Arg196X FS del 237 17 unknown M osteosarcoma20 Nega,ve27 c.1073A>T p.Glu358Val missense del 1 0 unknown F sarcomaNOS43 Nega,ve
#parentdeceasedatyoungagefromcancer-relatedcause

Anatomic imaging CT scan MRI scan Plain Xray
Functional imaging
Thallium scan Bone scan FDG PET
Biopsy
Critical Open vs core vs needle


Key surgical principles Adequate resection margins are critical Reconstruction essential, and often astonishingly successful Neo-adjuvant treatment can
Limit size of resection Be more effective than post-operative treatment, where tissue oxygenation is key Have prognostic value But also complicate wound healing
Radiotherapy principles
For curable STS, standard of care is pre-operative RT Usually 50-60Gy (radioresistant)
Note that PNET radiosensitive (usually 30-40Gy) Decreases local relapse rates to ~10% (cf 50%) Wound complications
Short-term Long-term
For palliation, shorter course RT


Pervaiz et al Cancer, 2008
18 trials, 1953 participants …but omitted results of EORTC 62931, a large randomised and negative study Conclusion—cannot be regarded as standard of care

Palliation of STS
Single agent efficacy Doxorubicin Ifosfamide DTIC
Newer regimens
Docetaxel/gemcitabine ET-743 Gemcitabine alone
Trials

Palliation of STS: Long-term benefit for a subset of patients
Van Glabbeke et al., JCO, 1999


Palliation of STS
Lancet, 2012

PNET/Ewings family tumors: prognostic factors

Primitive neuroectodermal tumors/Ewings family tumors
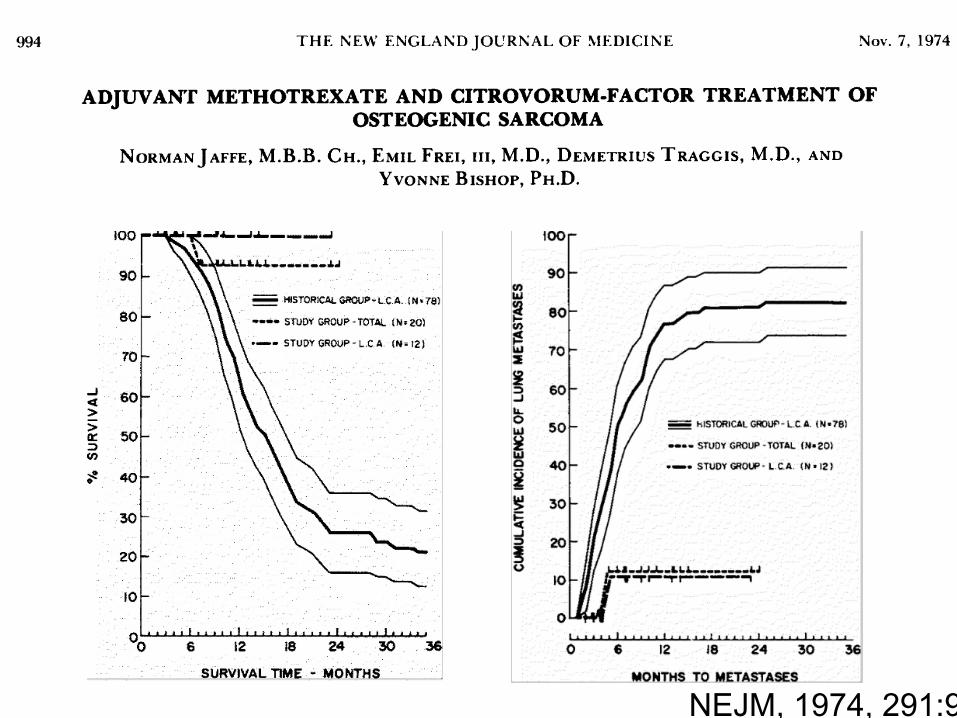
NEJM, 1974, 291:994

Osteosarcoma

Osteosarcoma

AOST0331
Current trials for resectable osteosarcoma

Giant cell tumor of bone
Lancet Oncology, 2009; 11:275

Tenosynovial Giant Cell Tumor
PNAS, 2006; Cancer, 2012

Diffuse-type Tenosynovial Giant Cell Tumor
Cancer Cell, in press

Sarcoma in summary How are we doing?


References
WHO Classification of tumours: Pathology and Genetics Tumours of soft-tissue and bone 2002 2nd Edition Eds Fletcher, Unni and Mertens Cancer: Principles & Practice of Oncology by Vincent T. Devita, Samuel Hellman, Steven A. Rosenberg 7th edition 2005







