Download - TRAUMATIC BRAIN INJURY (TBI)
TRAUMATIC BRAIN INJURY (TBI)
Written by: Beth Frisby, RN, BSN, CEN, CCRN, CFRN, RNC-OB
Julia Sandoval RN, BSN, CFRN, CCRN
06/20/2019

Objectives
1. Discuss common mechanism of TBI.
2. Identify common TBI.
3. Identify clinical presentation of the patient
with a TBI.
4. Discuss medical management of patient
diagnosed with TBI.
5. Scenario training.
Disclaimer
• No financial disclosures

Common mechanisms in TBI
• MVC
• Falls
• Occupational
• Recreational
• Assaults
• Risk factor: Being male

Acceleration/Deceleration
• Video

COUP - CONTRECOUP INJURY

• Primary injury
• Secondary injury
Primary vs. Secondary Brain Injury
Secondary Brain Injury
• Occurs in the minutes, hours, and days
following impact.

ABRUPT SYMPTOMS and RISK FACTORS. • Unwitnessed or unrecognized Seizure with post-ictal deficits
• Migraines
• Systemic Infections
• Tumors (more often a slower presentation)
• Psychogenic Paralysis (Diagnosis of exclusion) (Conversion disorder)
• Chronic SDH
• Cardiac Failure
• Toxic-metabolic disturbances (Hyperglycemia; Hypoglycemia< 45mg/dl,often improves with glucose; Hyponatremia, Hepatic Encephalopathy)
• Syncope
• Vertigo
Differential Diagnosis
Concussion
No identifiable lesion;
N/V, confusion,
disorientation, memory
loss, seizure
• Post-concussion
syndrome: symptoms
remain for an
extended time;
• Head CT: Negative
Post Concussion Symptoms
• Neuropsychiatric Impairments– Headaches
– Slow/difficulty responding to questions
– Inability to focus attention
– Emotionally labile
– Memory deficits
– Disruption in speech
– Must have resolution of all impairments before returning to sport• Second impact syndrome

Assessment for CT scan
• Canadian CT head Rule (CCHR)
• New Orleans/Charity Head Trauma/Injury
Rule (NOC)
• National Emergency X-Radiography
Utilization Study II (NEXUS II)
• Pediatric Emergency Care Applied
Research Network (PECARN)
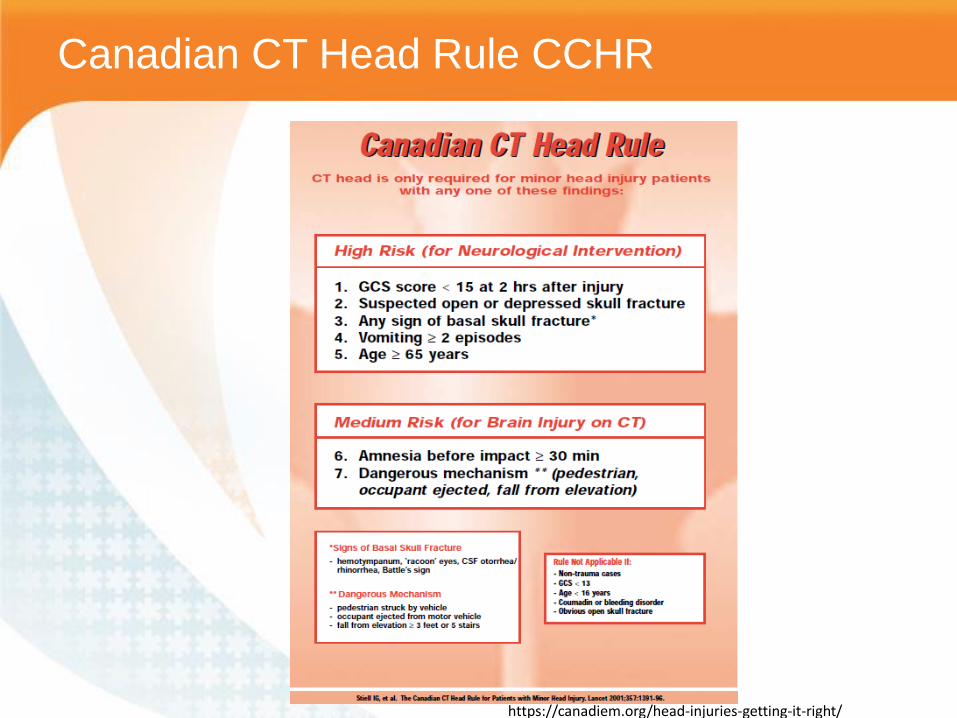
Canadian CT Head Rule CCHR
https://canadiem.org/head-injuries-getting-it-right/

Pediatric Emergency Care Applied Research
Network PECARNS
https://www.aliem.com/2017/06/pecarn-pediatric-head-trauma-official-visual-decision-aid/

PECARNS over 2 years
https://canadiem.org/the-pecarn-pediatric-head-ct-rule-project/
• Etiology: acceleration-
deceleration thus the
shearing of axons
• A widespread disruption
of neurologic function
without focal lesions
• 12-24hrs later tiny
punctate lesions are seen
on CT
• Diffuse swelling, white
matter degeneration,
axon damage
• Immediate LOC, last days
to months with normal
ICP
• Posturing
• Loss of brainstem
reflexes
Diffuse Axonal Injury
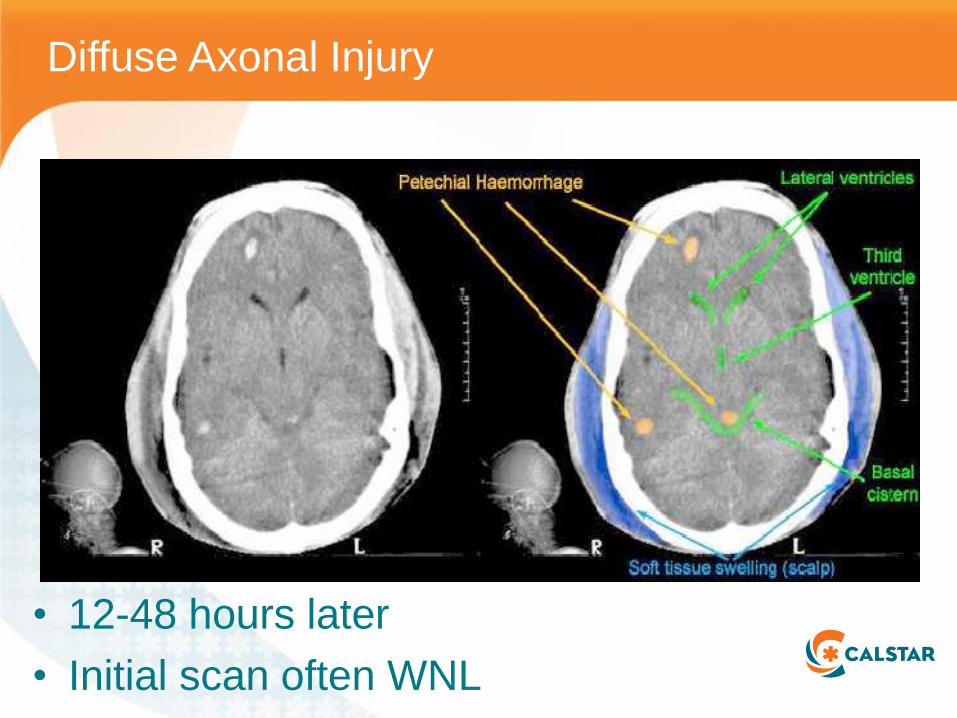
Diffuse Axonal Injury
• 12-48 hours later
• Initial scan often WNL

Epidural
• Hemorrhage between skull and dura mater
• Most common is temporal impact, middle meningeal artery
• (+) LOC, can have brief lucid period then rapid decline
• Need evacuation emergent
• Prognosis if bleed
evac’d early can be
good! Delays bring
mortality rate to 50%.
• Often Lens shaped in
appearance on CT
scan
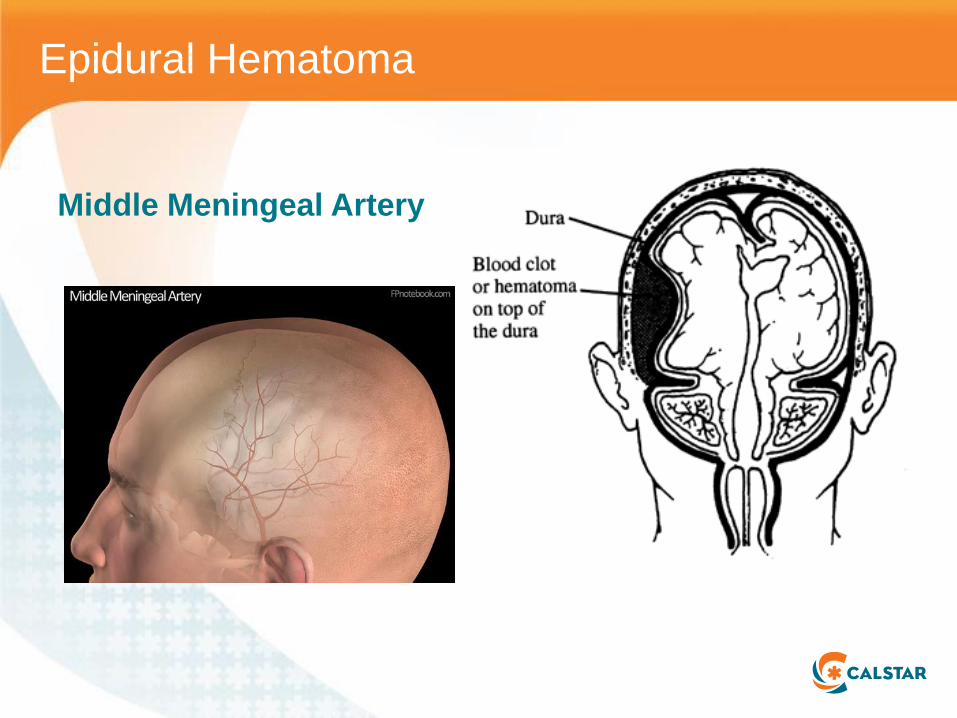
Epidural Hematoma
Middle Meningeal ArteryTemporal blow, middle meningeal artery
Epidural Hematoma

Protectors of the brain…
THE “B” TEAM: THE SKULL
Thinnest
portions

Epidural Hematoma

Epidural Hematoma with shift

Epidural Hemorrhage
• Cranial fractures are present in 70% to
90% of cases.
• 90% of epidural hematomas are caused
by head trauma with a skull fracture that
crosses a portion of the middle meningeal
artery or vein.
• The middle meningeal artery is torn in
60% of cases.

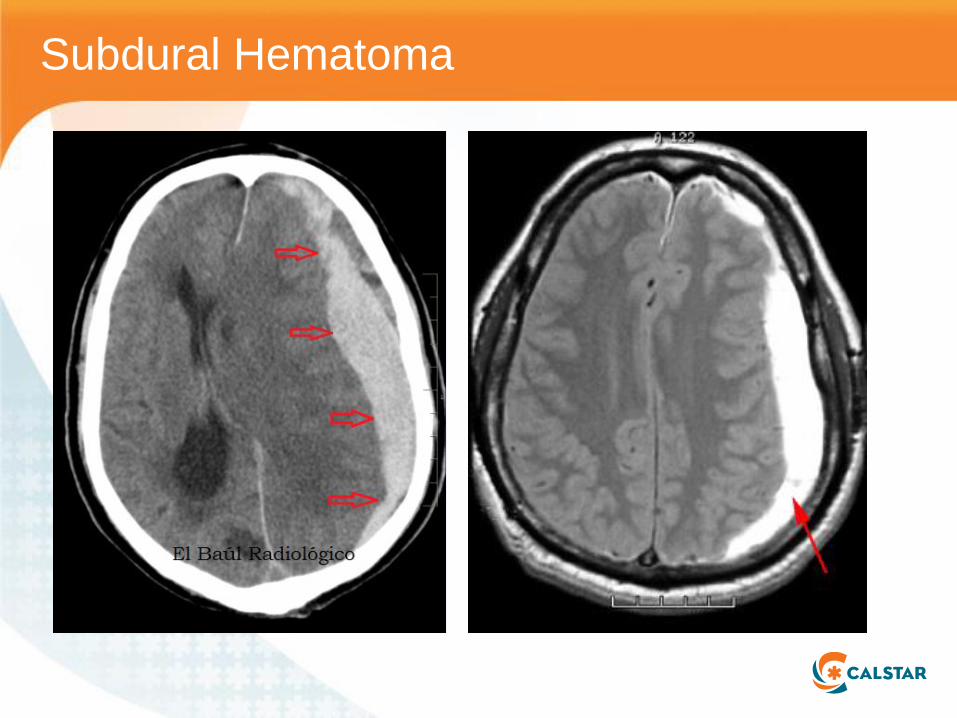
• Collection of blood between the dura mater and the arachnoid layer of the meninges
• Bridging veins torn
1. Acute (48hrs)
2. Subacute (2-14days)
3. Chronic (>14days)
Generally needs emergent evacuation
Subdural Hemorrhage
Subdural Hematoma

Subdural Hematoma

Subarachnoid Hemorrhage
• A diffuse collection of
blood between the
arachnoid mater and
the pia mater, from
SA vessels
• Seizure, vomiting,
LOC?
• 50% of traumatic
bleeds have SAH

Subarachnoid Hemorrhage

Brain Stem Hemorrhage
• Primary: direct blow or torsion
• Secondary: Compression from elevated
ICP’s, edema
– Midbrain: deep coma, fixed pupils at midpoint,
posturing (decerebration)
– Pons: Coma, small (pinpoint) nonreactive
pupils, opthalmophlegia, decerebration.

Skull Fractures
• Depressed
– Pushes the skull into the brain
• Basilar
– Occurs most commonly in temporal bone
• Middle meningial artery and vein
– Raccoon eyes
– Rhinorrhea or Otorrhea
– Hemotympanum
– Facial nerve palsies
• Linear

Pneumocephalus and CSF leak
• Most often seen with Basilar skull fracture
– CSF leak is slightly increased risk of
meningitis
• Not usually given antibiotic prophylaxis
• Usually resolve in 7 days

• Prompt recognition and treatment can improve
outcome
• Minimize secondary injury….
TBI: Goals

• Elevated ICP
• Low CPP
• Systemic hypotension/shock
• Hypoventilation/hypoxemia
• Hyperventilation
• Brain edema
• Brain herniation
• Brain hemorrhage
• Cerebral arterial vasospasm
• Inflammation
• Hyperthemia
• Chronic systemic illness
Secondary Brain Injury
• Inadequate fluid or blood
resuscitation
• Inadequate oxygen
delivery
• Hyperventilation
• Nosocomial infections
• Alcohol and other drug
intoxication
• Anticoagulants
Intrinsic Extrinsic or Iatrogenic

• Remember neuro exams can change fast
so use for first exam as a base to follow!

Glasgow Coma Scale

Primary Survey
• A irway: Patent?
• B reathing: tachypnea common, SpO2>94%
• C irculation: normotensive
• D isability: (before medication/RSI)
Directed Neuro: GCS, Pupils, motor Strength, gross sensory
• E xposure: Trauma?


• Comatose?
• Posturing: abnormal flexion or extension of extremities in response to pain (Brainstem)
• Preferential gaze?
• Abnormal changes in breathing
• VS changes: CUSHINGS TRIAD:
– HTN with widened pulse pressure, BRADY-CARDIA, RESPIRATORY CHANGES (decreased) (Brainstem). (THIS IS A SIGN OF IMPENDING HERNIATION!!!! )

RSI
• Place pt on high flow
N/C for intubation can
increase reservoir
and buy you extra
time during intubation.
• Lidocaine
– May decrease ICP
– May do nothing
• Ketamine/Etomidate
• Succinylcholine/
• Rocuronium
Management of TBI
• HOB elevated
• Neck aligned, no knee / hip flexion
• C-collar (too tight??)
• Keep ETCO2 35
• PaCO2 35-38
• Normothermic
• Sat’s >94% (avoid hypoxia / hyperventilation)
• Control Pain / Keep sedated
• Mannitol if needed
• Euvolemic– Foley
• Normotensive

• Benzodiazepines – Levetiracetam (Keppra)
– 1000mg IVPB over 15min
then Q12hr.
– Fosphenytoin (Cerebryx)
load (15mg/kg, max
150mg) then Q 8hr. OR
Seizure
Prevention
Coagulopathies
• Release of
thromblplastin and
tissue-activating
proteins from TBI.
• PT, PTT
• treat with FFP
• S/S of elevated ICP? Intubate and control ETCO2
• Maintain neck alignment
• HOB 30
• Analgesics IVP or gtts
• Midazolam IVP or gtt
• Proprofol gtt
• Paralyze (Nimbex, rocuronium)
• Mannitol if showing S/S of potential herniation. – 1mg/kg
Manage Increase Cerebral Pressure (ICP)
https://www.iemoji.com/view/emoji/2493/smileys-people/exploding-head

Hyperventilation and TBI
• Decrease in PaCO2 leads to decrease in
cerebral blood flow
• Linked to worse outcomes
• Goal is to have PaCO2 at 35

Hypotension and TBI
• Spaite et al
– Increased mortality with decreased blood
pressure
– Threshold of 90mmHg may be too low
– Increased mortality with every 10 point
grouping decrease in blood pressure
– Prevent secondary injury
• Even one low blood pressure can increase
mortality as blood flow to brain decreases.
Hypoxia
• Brain doesn't get enough oxygen and cells
will start to die
In Summary
• Treat primary injury and prevent
secondary injury
• Rememer the "H" Bombs
– Hypotension
– Hyperventilation
– Hypoxia

Bibliography
• https://www.uptodate.com/contents/emergency-airway-management-in-the-patient-with-elevated-
icp?source=history_widget
• https://www.uptodate.com/contents/management-of-acute-severe-traumatic-brain-
injury?source=history_widget
• https://www.uptodate.com/contents/pretreatment-medications-for-rapid-sequence-intubation-in-
adults-outside-the-operating-room?source=history_widget
• https://www.uptodate.com/contents/cerebrospinal-fluid-physiology-and-utility-of-an-examination-in-
disease-states?source=history_widget
• https://www.uptodate.com/contents/skull-fractures-in-children-clinical-manifestations-diagnosis-
and-management?source=history_widget
• https://www.uptodate.com/contents/acute-mild-traumatic-brain-injury-concussion-in-
adults?source=history_widget
• https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5637731/
• https://www.uptodate.com/contents/severe-traumatic-brain-injury-in-children-initial-evaluation-and-
management?search=blood%20pressure%20traumatic%20brain%20injury&source=search_result
&selectedTitle=1~150&usage_type=default&display_rank=1
• https://www.uptodate.com/contents/management-of-acute-severe-traumatic-brain-
injury?search=blood%20pressure%20traumatic%20brain%20injury&source=search_result&select
edTitle=2~150&usage_type=default&display_rank=2
• https://www.uptodate.com/contents/sequelae-of-mild-traumatic-brain-
injury?sectionName=Second%20impact%20syndrome&search=second%20impact%20syndrome
&topicRef=91282&anchor=H4093484671&source=see_link#H4093484671
Bibliography
• https://canadiem.org/head-injuries-getting-it-right/
• https://www.aliem.com/2017/06/pecarn-pediatric-head-trauma-official-visual-decision-aid/
• https://www.uptodate.com/contents/evaluation-of-stupor-and-coma-in-
children?search=uncal%20herniation%20and%20pupils&source=search_result&selectedTitle=1~150&usage_type
=default&display_rank=1
• https://www.uptodate.com/contents/minor-head-trauma-in-infants-and-children-
evaluation?search=pecarn%20rules&source=search_result&selectedTitle=1~150&usage_type=default&display_ra
nk=1
• https://www.uptodate.com/contents/internuclear-
ophthalmoparesis?search=external%20ophthalmoplegia%20and%20trauma&source=search_result&selectedTitle
=1~150&usage_type=default&display_rank=1#H15
• https://www.uptodate.com/contents/intracranial-subdural-hematoma-in-children-epidemiology-anatomy-and-
pathophysiology?search=traumatic%20subdural%20hematoma%20injuries&source=search_result&selectedTitle=
1~150&usage_type=default&display_rank=1
• https://www.uptodate.com/contents/intracranial-epidural-hematoma-in-children-clinical-features-diagnosis-and-
management?search=traumatic%20epidural%20hematoma%20injuries&source=search_result&selectedTitle=1~1
50&usage_type=default&display_rank=1
TRANSEXAMIC ACID (TXA)
Written by: Beth Frisby, RN,BSN, CEN, CCRN, CFRN, RNC-OB
Julia Sandoval RN, BSN, CFRN, CCRN
06/20/2019

Objectives
1. Discuss the history of TXA.
2. How does TXA work?
3. Identify clinical applications of TXA.
4. Overview of dosing of TXA.
5. Take home points.
Disclaimer
• No financial disclosures

History of TXA administration in Trauma
• 1962- A Japanese husband
and wife team publish in
Keio Journal of Medicine
• 2010- CRASH-2 in Lancet
• 2012- MATTERs
• 2017- WHO updates
recommendations based
on WOMAN trial

How does TXA work?
• TXA binds to
plasminogen’s lysine
receptor site
• Blocks the conversion
of plasminogen to
plasmin
• Less plasmin, thus
less fibrin (clot) break
down occurs https://hipandkneebook.com/hemostasis

Applications
Approved use in US
• Tooth extraction in
patients with
hemophilias
• menorrhagia
“Off-label” use in the US
• Traumatic
hemorrhage
• Total joint arthroplasty
• Cardiac surgery
• Post partum
hemorrhage
http://s.hswstatic.com/gif/tooth-extraction-1.jpg
https://www.springermedizin.de/polytrauma/755660-themenseite/11070372
Administration
Adult:
• 1gram in 100mL of NS/LR over 10 min WITHIN 3 HOURS of INJURY
• Followed by…
• 1gram in 1000mL NS over 8 hours within 6 hours of first dose
Pediatric:
• 15 mg/kg to a max of 1 gram over 10 min WITHIN 3 HOURS of INJURY
• Followed by…
• 2mg/kg/hour – within 6 hours of first
dose
– For at least 8 hours or until bleeding subsides
Traumatic hemorrhage with SBP<90

Contraindications/precautions
• Greater than 3 hours
since injury
• Hypersensitivity to
TXA
http://clipart-library.com/images/6ir5b8MBT.jpg

Take home points
• Traumatic hemorrhage
• SBP<90
• 1st dose MUST be given WITHIN 3 hours
• Don’t forget the 2nd dose within 6 hours

Bibliography
• https://www.ncbi.nlm.nih.gov/books/NBK532909/
• http://www.txacentral.org/history
• https://maternova.net/blogs/news/txa-recommended-by-who-for-pph-treatment
• https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3086904/
• https://www.ncbi.nlm.nih.gov/pubmed/23477634
Scenarios







