Download - Update on Targeted Temperature Management

Targeted Temperature Management
Kristopher R. Maday, MS, PA-C, CNSCUniversity of Alabama at Birmingham
Pegasus Emergency Group
Is It Still “Cool” to Cool or Is It “Hot” to Not
OR

@PA_Maday #AAPA15
Follow Along at……
No Financial Disclosures

Objectives• Discuss history of hypothermia in
acute cardiac events• Evaluate the
advantages/disadvantages of hypothermia in post-arrest management
• Critically evaluate current literature regarding temperature end-points
• Discuss future trends of TTM

History of Hypothermia in Medicine

Hippocratescirca 400 B.C.
Guly H. Resuscitation. 2011;82(1):122-125.

William Osler1890s
The John Hopkins Hospital Reports. Volume V. 1895

Harvey Cushing1920s

1960s - Dr. Peter Safar
Acierno LJ. Clin. Cardiol. 2007;30:52-54.

1971 - Dr. Brian Barrat-Boyes of New Zealand
Barratt-Boyes BG. Circulation. 1971;43(Suppl 5):25-30.

Late 1970s
1980s
85o F (29oC) for days
Mild hypothermia
Numerous complications
Less complications
Case Reports• 1980 - Annals of Internal Medicine– 2 case reports of hypothermic
immersions
Sekar TS. Arch Intern Med. 1980;140(6):775-779.

Severity of Hypothermia

Benefits of Therapeutic Hypothermia
• Lowers tissue oxygen requirements
• Decreases cerebral metabolism and edema
• Improved tolerance to ischemia
• Decreases reperfusion inflammatory cascade Young RSK. JAMA. 1980;244:1233-1235 Globus MY. J Neurochem. 1995;65(4):1704-1711Busto R. Stroke. 1989;28(8):1113-1114

Breakthrough came in 2002
HACA Trial• 275 patients• 32-34o C vs
normothermia for 24 hr
• Primary Outcome– Neurologic function at
6 months
Bernard Trial• 77 patients• 33o vs 37o for 12
hr• Primary Outcome– Favorable
discharge location
HACA Investigators. NEJM. 2002;346(8):549-556. Bernard SA. NEJM. 2002;346(8):557-563.

Results of Initial Hypothermia Trials
HACA Investigators. NEJM. 2002;346(8):549-556. Bernard SA. NEJM. 2002;346(8):557-563.
Trials Criteria MortalityGood
Neurologic Outcomes
HACA
VT/VF rhythmResuscitation within 15minROSC within 60min32-34o for 24hr
Control – 55%Hypothermia – 41%
Control – 39%Hypothermia – 55%
Bernard
VF with persistent coma33o within 2hr for 12hr
Control – 68%Hypothermia – 51%
Control – 26%Hypothermia – 49%
Logistics of Therapeutic Hypothermia
Cooling ApparatiTiming
MedicationsMonitoring

4o C

Artic Sun Cooling System

VELOCITY Trial



Logistics of Therapeutic Hypothermia
Nolan JP. Circulation. 2003;108:118-121
When do you start cooling?
ASAP p ROSCSchwartz BG. Am J Cardio. 2012;110:461-466

Logistics of Therapeutic Hypothermia
Nolan JP. CIrculation. 2003;108:118-121
How long should patients be cooled?

Logistics of Therapeutic Hypothermia
Nolan JP. CIrculation. 2003;108:118-121
How fast do you re-warm?
0.5o/hr to 37o C

Logistics of Therapeutic Hypothermia
Nolan JP. CIrculation. 2003;108:118-121
Medications Monitoring
Hye JK. K J Anes. 2008;54(6):623-628

Prognostication After Therapeutic Hypothermia
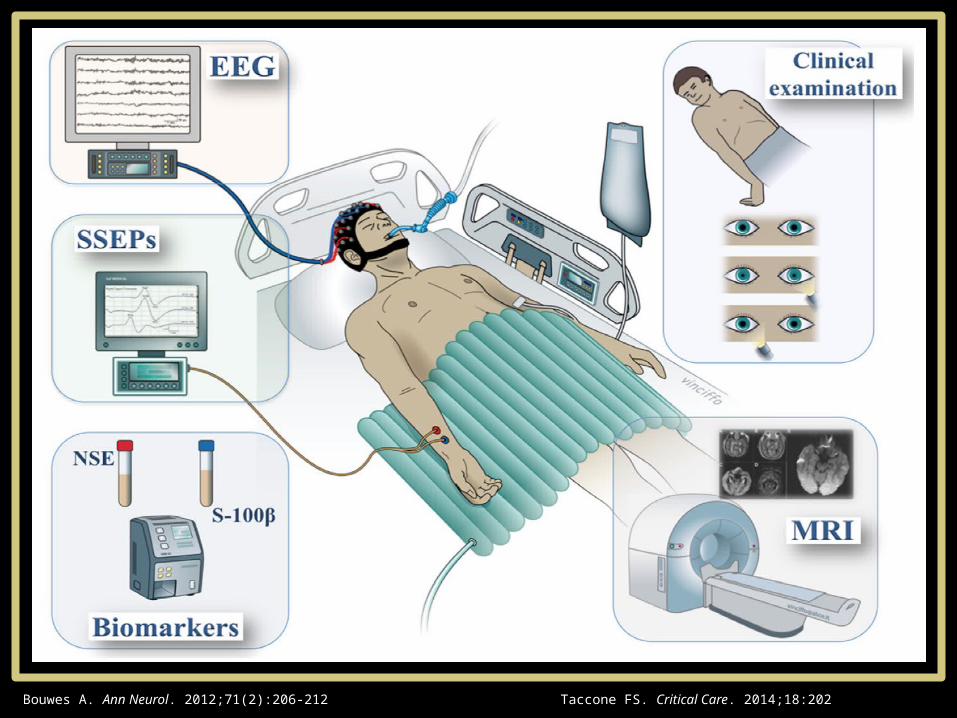
Prognosis Following Therapeutic Hypothermia
Taccone FS. Critical Care. 2014;18:202Bouwes A. Ann Neurol. 2012;71(2):206-212

Prognosis Following Therapeutic Hypothermia
Taccone FS. Critical Care. 2014;18:202Bouwes A. Ann Neurol. 2012;71(2):206-212

Complications of Therapeutic Hypothermia
Nolan JP. CIrculation. 2003;108:118-121 Schwartz BG. Am J Cardio. 2012;110:461-466


Targeted Temperature Management
Nielson N. NEJM. 2013;369:2197-2206

Targeted Temperature Management
• 939 patients in 36 ICU across Europe and Australia
• ***ALL RHYTHMS***• 2 study groups• Protocol• Outcomes– Primary – All cause mortality– Secondary – Neurologic status
Nielson N. NEJM. 2013;369:2197-2206

Targeted Temperature Management
Nielson N. NEJM. 2013;369:2197-2206
Outcome 33o Group
36o Group
HR/RR (95% CI)
P-value
Primary OutcomeDeath at end of trial 235/473
(50%)225/466 (48%)
1.06 (0.89-1.28) 0.51
Secondary outcomeNeurologic function at 180d CPC of 3-5 251/469
(54%)242/464 (52%)
1.02 (0.88-1.16) 0.78
MRS of 4-6 245/469 (52%)
239/464 (52%)
1.01 (0.89-1.14) 0.87
Death at 180d 226/473 (48%)
220/466 (47%)
1.01 (0.87-1.15) 0.92
Primary OutcomeNo difference in all-cause mortality
Secondary OutcomeNo difference in neurologic status
Shorter ICU and hospital stays in 36o group

TTM Protocol
1. 24 hours at 36o C2. 12 hours at 37o C3. 36 hours at 37.5o C (de-sedate)4. 36 hours at whatever (no sedation)
Prognosticate after 108 hours following ROSC

What Does This Mean Now?• 33o is not better than 36o
• Not just for VT/VF
• Easier on smaller hospitals
• Decreased hospital LOS

Future Considerations• What temperature is best?
• When to start cooling?
• Duration of cooling?
• Any complications with 36o?








