
Health: KwaZulu-Natal Form Reference Number: Paed/D Clinical Records: Paediatrics
Catalogue for Paediatric Forms Use this Catalogue and Original Forms when Photocopying or Ordering Forms for Paediatric Wards and the Nursery
Form Description Use Catalogue Number Record Keeping Instructions: Children’s Ward Paediatrics Paed/C Cover Page: Paediatric Patient Record (boys and girls) Paediatrics Paed/07 Admission Sheet Paediatrics Paed/08 Growth Chart: 0-36 months weight and length Paediatrics Paed/09 Growth Chart: 2-20 years weight and length Paediatrics Paed/10 Growth Chart: 0-36 months coh Paediatrics Paed/11 Gastro Continuation Sheet Paediatrics Paed/14 Paediatric Discharge/Referral Letter Paediatrics Paed/23 HIV Testing, Clinical Staging & Care Plan Paediatrics Paed/24 Rheumatic Heart Disease Prophylaxis Letter Paediatrics Paed/25 Brain Death Checklist Paediatrics Paed/27 Rheumatic Heart Disease Follow Up Record Paediatrics Paed/28 Monitoring Sheet for Paediatric Transfers Paediatrics Paed/29 Monitoring Sheet In-transit Paediatrics Paed/30 Burns Chart for Body Surface Area Paediatrics Paed/32 Children’s Coma Score Paediatrics Paed/36 Paediatric Record Audit Paediatrics Paed/38 ARV Appointment and Prescription Record Paediatrics Paed/HIV1 Admission/Discharge Slip Paediatrics Paed/A&D Slip Record Keeping Instructions: Nursery Nursery Paed/A Use of Infant Care Record Nursery Paed/B Newborn Care Record (complete foldout) Nursery Paed/01 Weight and Intake Continuation Sheet: Neonate Nursery Paed/02 Clinical Notes Continuation Sheet: Neonate Nursery Paed/03 Growth Chart and Ballard Score: Neonate Nursery Paed/04 HIE Score: Neonate Nursery Paed/05 Basic Nursing Care: Neonate Nursery Paed/06 KMC Score Sheet Nursery Paed/26 Monitoring Sheet for Neonatal Transfers Nursery Paed/31 Jaundice Chart Nursery Paed/34 Neonatal Record Audit Nursery Paed/37 Neonatal Discharge/Referral Letter Nursery Paed/39 Results Both Paed/16 Acid Base, Blood Gasses and Ventilator Settings Both Paed/17 Oxygen Delivery, Saturation and Nebs Monitoring Sheet Both Paed/18 Glucose Monitoring Sheet Both Paed/19 Ventilator & CPAP Observations Both Paed/20 Intake-Output: IV and Orals Both Paed/21 Intake-Output: Orals Only Both Paed/22 Letter in Support of Grant Application Both Paed/33 Catalogue Both Paed/D Ordering Form Both Paed/E
Keep a Master Copy File in your ward, both as a quality control tool and to use for photocopying Do not photocopy copies Always ensure that the forms you use match the originals EXACTLY, front and back Incorrectly copied forms MUST be sent back to stationery stores Do not use forms other than these for the designated purpose
B y u s i n g t h e s e f o r m s c o r r e c t l y , w e w i l l i m p r o v e t h e q u a l i t y o f c a r e o u r p a t i e n t s r e c e i v e a n d w e w i l l s a v e t h e h o s p i t a l m o n e y , a n d w e w i l l s a v e o u r s e l v e s t i m e a n d f r u s t r a t i o n


Health: KwaZulu-Natal Form Reference Number: Paed/E Clinical Records: Paediatrics
Order Sheet for Paediatric Forms Use this Ordering Sheet and Original Forms when Photocopying or Ordering Forms for Paediatric Wards and the Nursery
Ward: Ordered By:
Date:
Form Description Quantity Catalogue Number Record Keeping Instructions: Children’s Ward Paed/C Cover Page: Paediatric Patient Record (boys and girls) Paed/07 Admission Sheet Paed/08 Growth Chart: 0-36 months weight and length Paed/09 Growth Chart: 2-20 years weight and length Paed/10 Growth Chart: 0-36 months coh Paed/11 Gastro Continuation Sheet Paed/14 Paediatric Discharge/Referral Letter Paed/23 HIV Testing, Clinical Staging & Care Plan Paed/24 Rheumatic Heart Disease Prophylaxis Letter Paed/25 Brain Death Checklist Paed/27 Rheumatic Heart Disease Follow Up Record Paed/28 Monitoring Sheet for Paediatric Transfers Paed/29 Monitoring Sheet In-transit Paed/30 Burns Chart for Body Surface Area Paed/32 Children’s Coma Score Paed/36 Paediatric Record Audit Paed/38 ARV Appointment and Prescription Record Paed/HIV1 Admission/Discharge Slip Paed/A&D Slip Record Keeping Instructions: Nursery Paed/A Use of Infant Care Record Paed/B Newborn Care Record (complete foldout) Paed/01 Weight and Intake Continuation Sheet: Neonate Paed/02 Clinical Notes Continuation Sheet: Neonate Paed/03 Growth Chart and Ballard Score: Neonate Paed/04 HIE Score: Neonate Paed/05 Basic Nursing Care: Neonate Paed/06 KMC Score Sheet Paed/26 Monitoring Sheet for Neonatal Transfers Paed/31 Jaundice Chart Paed/34 Neonatal Record Audit Paed/37 Neonatal Discharge/Referral Letter Paed/39 Results Paed/16 Acid Base, Blood Gasses and Ventilator Settings Paed/17 Oxygen Delivery, Saturation and Nebs Monitoring Sheet Paed/18 Glucose Monitoring Sheet Paed/19 Ventilator & CPAP Observations Paed/20 Intake-Output: IV and Orals Paed/21 Intake-Output: Orals Only Paed/22 Letter in Support of Grant Application Paed/33 Catalogue Paed/D Ordering Form Paed/E
Copied by: Date:
Issued by: Do not photocopy copies Always ensure that the forms you use match the originals EXACTLY, front and back Incorrectly copied forms MUST be sent back to stationery stores
B y u s i n g t h e s e f o r m s c o r r e c t l y , w e w i l l i m p r o v e t h e q u a l i t y o f c a r e o u r p a t i e n t s r e c e i v e a n d w e w i l l s a v e t h e h o s p i t a l m o n e y , a n d w e w i l l s a v e o u r s e l v e s t i m e a n d f r u s t r a t i o n


Health: KwaZulu-Natal Form Reference number: Paed/C Clinical Records: Paediatrics
Clinical Record Keeping: Paediatrics
T h e r e i s a s t a n d a r d s t r u c t u r e f o r P a e d i a t r i c R e c o r d s , a n d f o r f i l i n g o f n o n - c u r r e n t r e c o r d s .
T h e P a e d i a t r i c P a t i e n t R e c o r d i s k e p t i n t h e y e l l o w “ O u t p a t i e n t F o l d e r ” . H o w e v e r , t h i s i s N O T a n o u t p a t i e n t r e c o r d . T h i s i s t h e p a t i e n t c l i n i c a l r e c o r d t h a t f o l l o w s t h e p a t i e n t t h r o u g h o u t t h e
i n s t i t u t i o n , w h e n e v e r a n d w h e r e e v e r t h e p a t i e n t i s s e e n .
All Paediatric Patient Records are exactly the same (inside the yellow “outpatient” folder)
Section Healthworker responsible 1) Cover page Doctor 2) Growth chart: Birth to 36 months weight and height (boy chart facing) Doctor 3) Growth chart: Birth to 36 months head circumference (boy chart facing) Doctor 4) Growth chart: 2 to 18 years (boy chart facing) Doctor 5) Results sheet Doctor 6) HIV testing and staging sheet Doctor 7) Continuation pages/History and Progress/Referral Letters Doctor
T h e O P D c l e r k s o r n u r s i n g s t a f f s h o u l d a s s e m b l e t h e “ p a c k a g e ” a n d b i n d t h e m i n t h e y e l l o w f o l d e r s . C o n t i n u a t i o n p a g e s a n d r e f e r r a l l e t t e r s m u s t b e b o u n d c h r o n o l o g i c a l l y . S p e c i a l i n v e s t i g a t i o n r e p o r t s
( C T S c a n , e c h o e t c . ) c a n b e b o u n d a f t e r t h e H I V s h e e t , o r c h r o n o l o g i c a l l y . T h e o r d e r l i n e s s o f t h e P a e d i a t r i c P a t i e n t R e c o r d i s t h e r e s p o n s i b i l i t y o f t h e l a s t d o c t o r t o m a k e a n e n t r y .
All Paediatric Inpatient Records are exactly the same (inside ward-based “Ring Binders”)
All charts are in chronological order
Section Order Temperature charts Front to Back Doctor’s obs (results page, scoring sheets etc) Front to Back Nursing obs (“routine”, ventilator, phototherapy, etc) Front to Back Nursing Process Back to Front Intake/Output/Feeds Back to Front Prescription Back to Front Road to health chart Keep in a safe place and update when appropriate
1) Non-current pages are removed after one-two days 2) Results must be entered on results page, signed by attending doctor and filed away from the active record 3) Each page should have patient’s name and inpatient number 4) Notes should be problem orientated and focussed 5) If any change is made to the management of the patient, this change and the reason for the change must
be documented 6) When “filing” non-current pages, use a paper binder and keep pages in chronological order 7) When “filing” non-current pages, bind like with like 8) All the different kinds of pages (progress, prescription, intake/output, special observations etc.) used in the
department are standardised 9) ALWAYS RECORD THE CHILD’S DATE OF BIRTH, IN ALL DESIGNATED PLACES
“ G o l d S t a n d a r d ” f o l d e r s s h o u l d b e d e v e l o p e d f o r e a c h u n i t , a n d u s e d t o r e f e r t o f o r s t r u c t u r i n g f o l d e r s a n d t o c o m p a r e w i t h d u r i n g c h a r t r e v i e w m e e t i n g s .


Health: KwaZulu-Natal Form Reference number: Paed/07 Clinical Records: Paediatrics
Paediatric Patient Record Cover Page
Birth Registration/ID Number:
Name: OP Number:
Address: IP Number:
Date of Birth:
Phone Number: Gender: Male / Female (use sticker if available)
Date Problem (enter significant problems only) ICD Code Management
Admissions Register
DoA DoD Reason for Admission ICD Code Follow Up Place and Date

Name:________________________ Folder No:___________________
2
Background Information
Perinatal History
Antenatal Care: Site: Mother WR: + / - / ? Mother HIV: + / - / ?
Delivery: Mode: Place: Apgars:
Gestation: Birthweight: Length: COH:
Problems:
PMTCT: Not tested Mother Nevirapine: Y / N / ? Baby Nevirapine: Y / N / ?
Follow up site for PCR/Cotrimoxazole/CD4:
Vaccinations (insert date given, don’t tick) At birth: BCG: Y / N Polio: Y / N
Vaccine 6 weeks 10 weeks 14 weeks 9 months 18 months Preschool
Polio
DTP Td
HiB
Hep B
Measles
Vitamin A
Social History
Primary caregiver: Name: Relationship:
Household Income: Number of Dependents:
Qualifies for Grant: CSG / CDG / FCG Caregiver advised: Y / N Referral letter given: Y / N
Nutrition: Referred to Integrated Nutrition Programme: Y / N
Family History
Development (insert age achieved)
Smiled: _____ months Sat: _____ months Crawled: _____ months
Walked: _____ months Talked: _____ months School: Year _____ Grade: _____
Past Medical History (list admissions on first page)

Health: KwaZulu-Natal Form Reference Number: Paed/08 Clinical Records: Paediatrics
Paediatric patient admission sheet (to be completed by admitting doctor after usual clerking notes) Name: Date of Birth: DoA: ToA:
Admitted from Gender: m / f Admitting Doctor (print)
Admitting to ICU High
care Medical Surgical Mixed Receiving Doctor (print)
Outcome Discharged Transferred Absconded Died DoD: ToD:
Referred Name of hospital/clinic:
Ⓨ / Ⓝ / Ⓤ If yes, from: Another hospital A clinic Private sector Unknown
If yes, from: Inside drainage area Outside drainage area Unknown
Social Caregiver Name: Telephone:
Mother Alive and well Dead Sick Unknown Mother Grandmother
Father Alive and well Dead Sick Unknown
Primary caregiver
Father Other: _____
Nutrition OWFA Normal UWFA Marasmus Kwashiorkor M-K Unknown Weight: _____kg
HIV / AIDS Laboratory test Negative Exposed Infected No result Not tested
(but indicated) Not tested
(not indicated) Unknown
Clinical Stage I Stage II Stage III Stage IV Not staged (but indicated)
Not staged (not indicated) Unknown
PMTCT Prophylaxis given Prophylaxis not given Mother negative at delivery Unknown
Feeding in 1st 6 months
Exclusive breast for 6/12 No breast, ever Mixed, from birth Unknown
Cotrimoxazole Current Ever Never (but indicated) Never (not indicated) Unknown
ARV (child) Current Ever Never (but indicated) Never (not indicated) Unknown
ARV (mother) Current Ever Never (but indicated) Never (not indicated) Unknown
Main diagnosis/reason for admission Illness/Condition ICD 10
Basis for diagnosis (tick relevant)
Previous diagnosis Symptoms Signs
Current Rx:
Reasons for admission 1. Life-threatening problems (tick applicable)
Airway Critical Narrow Normal
Breathing Needs IPPV Needs oxygen Hyperventilation Normal
Circulation Shock (cap refill>3s) Hypovolaemia Hypervolaemia Normal
Consciousness (AVPU) Unconscious Response to Pain Response to Voice Alert
Convulsions In hospital Before arrival Past Never
Dehydration 10% 5% Oedema Normal
IMCI classification “Red” “Yellow” “Green”
Infection SIRS (“toxic shock”) Needs IV agent Needs oral agent No
2. Diagnostic workup (e.g. tuberculosis): 3. Social (e.g. poverty, distance, caregiver): 4. Specialist review/opinion:
5. Other:

Health: KwaZulu-Natal Form Reference Number: Paed/08 Clinical Records: Paediatrics
2007/06/21 2
Priority problems / Red flags (circle applicable) 3 ‘T’s Tiny (< 2 months); Temperature (> 38°C or < 36°C); Trauma
3 ‘P’s Severe Pain; severe Pallor; Poisoning 3 ‘R’s Restlessness (or irritability or lethargy), Respiratory distress; urgent Referral
‘M’, ‘O’, ‘B’ Malnutrition; Oedema; Burns
readmission admitted within past 28 days for the same condition
last vaccine BCG / polio / diphtheria / pertussis / HiB / HepB / measles was / were given on: _______________
hypoglycaemia blood glucose < 2.6 mmol/ l Record actual blood sugar level:__________
Significant biochemical problems (record sats in room air FOR ALL ADMISSIONS & circle others applicable)
SpO2 in RA: pH < 7.2 K+ < 2.0 / K+> 6 Na+<120 Na+> 150 Albumin < 20
Urgent management Specific Rx Other Rx
Airway ETT: Bag/Mechanical IPPV:
Breathing Oxygen: Continue on way to ward:
Circulation/Shock Volume expand: Continue on way to ward:
Dehydration Rehydrate: Check Na:
Consciousness Protect airway: Coma position:
Infection IV antibiotic stat: Steroid/antipyretic:
Initial investigations (tick for “done”, circle for “to do”)
Chemistry acid-base renal FT’s liver FT’s blood glucose urine Na+ , K+ Urine protein:creatinine
Haematology FBC diff INR/PTT retics smear factorVIII/IX
Microbiology blood culture CSF urine dipstix urine MC&S stool MC&S Syphilis
Radiology chest X-ray abdo X-ray CT Brain MRI U/S Echo
TB skin test CSF Sputum AFB’s GW AFB’s Started TB Rx: yyyy/mm/dd
HIV rapid ELISA PCR CD4 Started ART: yyyy/mm/dd
Other Virus: Toxins/Drugs
Parameters for monitoring on arrival in ward (circle “to do”)
Temperature Respiratory rate
Sats/O2 requirement
Respiratory pattern Heart rate Blood
pressure Glucose Nurse
Weight Urine volume Stools Other:
Doctor Perfusion Acid-base Urea, creatinine
Serum Na+, K+ Hydration
Problem list and plans #1: #4:
Plan: Plan:
#2: #5:
Plan: Plan:
#3: #6:
Plan: Plan:
Pain Assessment No pain Mild pain Moderate pain Severe pain
Analgesia plan:
Sign: ________________________________ Date: ___________ Time: ___________

Health: KwaZulu-Natal Form Reference Number: Paed/A&D Slip Clinical Records: Paediatrics
*Admission / Discharge Slip (* delete whichever not applicable)
Attach this slip to Yellow File at admission, and to the Inpatient Records at discharge
Patient Name OP Number IP Number
Date Time Ward
Sign Contact Number MP Number
*Main reason for admission: *Discharge Diagnosis:
Health: KwaZulu-Natal Form Reference Number: Paed/A&D Slip Clinical Records: Paediatrics
*Admission / Discharge Slip (* delete whichever not applicable)
Attach this slip to Yellow File at admission, and to the Inpatient Records at discharge
Patient Name OP Number IP Number
Date Time Ward
Sign Contact Number MP Number
*Main reason for admission: *Discharge Diagnosis:
Health: KwaZulu-Natal Form Reference Number: Paed/A&D Slip Clinical Records: Paediatrics
*Admission / Discharge Slip (* delete whichever not applicable)
Attach this slip to Yellow File at admission, and to the Inpatient Records at discharge
Patient Name OP Number IP Number
Date Time Ward
Sign Contact Number MP Number
*Main reason for admission: *Discharge Diagnosis:


Paediatric Ward Admissions and Discharge Register Year:______________ Month:______________ Ward:__________________ Hospital:_________
No. Surname
Name Folder Number
Caregiver Name Telephone
Street, Town DoB Age DoA
ToA From? Weight
& Gender
Nutritionstatus: o/n/u/k/m/m-k
Diagnosis DoD ToD To?
ChIP reg y/n
Totals
DoB = date of birth; DoA = date of admission; ToA = time of admission; From? = enter where patient came from (e.g. another ward, home, clinic, another hospital); Nutrition status:o//n/u/k/m/m-k = overweight/normal/underweight for age/kwashiorkor/marasmus/marasmic-kwashiorkor; Dx = admission diagnosis (enter main reason for admission but update if diagnosis changes or child dies); DoD = date of discharge OR death; ToD = time of discharge OR death; To? = enter where patient was discharged to (e.g. another ward, home, clinic, POPD, another hospital, died); ChIP reg y/n = yes/no for entry on the Child PIP death register


L
E
N
G
T
H
L
E
N
G
T
H
W
E
I
G
H
T
W
E
I
G
H
T
Birth 3 96
Birth 3 1296 18 21 24 27 30 33 3615
2
3
4
5
6
7
10
12
14
16
8
6
kglb
AGE (MONTHS)
12 15 18 21 24 27 30 33 36kg
Mother’s Stature
Father’s Stature
Gestational
Date Age Weight Length Head Circ.
Age: Weeks
Birth
Comment
AGE (MONTHS)
8
9
10
11
12
13
14
15
16
17
90
95
100
cmcm
100
lb
16
18
20
22
24
26
28
30
32
34
36
38
40
45
50
55
60
65
70
75
80
90
95
85
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41in in
41
40
39
38
37
36
35
Birth to 36 months: Boys
L Weight-for-age percentilesength-for-age and
NAME
RECORD #
90
75
50
25
10
3
97
90
75
50
25
10
97
3
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Published May 30, 2000 (modified 4/20/01).

L
E
N
G
T
H
L
E
N
G
T
H
W
E
I
G
H
T
W
E
I
G
H
T
Birth 3 96
Birth 3 1296 18 21 24 27 30 33 3615
2
3
4
5
6
7
10
12
14
16
8
6
kglb
AGE (MONTHS)
12 15 18 21 24 27 30 33 36kg
Mother’s Stature
Father’s Stature
Gestational
Date Age Weight Length Head Circ.
Age: Weeks
Birth
Comment
AGE (MONTHS)
8
9
10
11
12
13
14
15
16
17
90
95
100
cmcm
100
lb
16
18
20
22
24
26
28
30
32
34
36
38
40
45
50
55
60
65
70
75
80
90
95
85
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41in in
41
40
39
38
37
36
35
Birth to 36 months: Girls
L Weight-for-age percentilesength-for-age and
NAME
RECORD #
90
75
50
25
10
97
3
90
75
50
25
10
97
3
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Published May 30, 2000 (modified 4/20/01).

2 to 20 years: Boys
Stature Weight-for-age percentiles-for-age and
NAME
RECORD #
W
E
I
G
H
T
W
E
I
G
H
T
S
T
A
T
U
R
E
S
T
A
T
U
R
E
lb
30
40
50
60
70
80
lb
30
40
50
60
70
80
90
100
110
120
130
140
150
160
170
180
190
200
210
220
230
kg10
15
20
25
30
35
80
85
90
95
100
105
110
115
120
125
130
135
140
145
150
155
160
cm
cm
150
155
160
165
170
175
180
185
190
kg10
15
20
25
30
35
105
45
50
55
60
65
70
75
80
85
90
95
100
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
12 13 14 15 16 17 18 19 20
AGE (YEARS)
AGE (YEARS)
40
90
75
50
25
10
90
75
50
25
10
113 4 5 6 7 8 9 10
97
3
97
3
62
42
44
46
48
60
58
52
54
56
in
30
32
34
36
38
40
50
74
76
72
70
68
66
64
62
60
inDate
Mother’s Stature Father’s Stature
Age Weight Stature BMI*
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Published May 30, 2000 (modified 11/21/00).

2 to 20 years: Girls
Stature Weight-for-age percentiles-for-age and
NAME
RECORD #
W
E
I
G
H
T
W
E
I
G
H
T
S
T
A
T
U
R
E
S
T
A
T
U
R
E
kg10
15
20
25
30
35
80
85
90
95
100
105
110
115
120
125
130
135
140
145
150
155
cm
150
155
160
165
170
175
180
185
190
kg10
15
20
25
30
35
105
45
50
55
60
65
70
75
80
85
90
95
100
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
12 13 14 15 16 17 18 19 20
AGE (YEARS)
AGE (YEARS)
40
160
cm 113 4 5 6 7 8 9 10
90
75
50
25
10
90
75
50
25
10
97
3
97
3
lb
30
40
50
60
70
80
lb
30
40
50
60
70
80
90
100
110
120
130
140
150
160
170
180
190
200
210
220
230
Date
Mother’s Stature Father’s Stature
Age Weight Stature BMI*
62
42
44
46
48
60
58
52
54
56
in
30
32
34
36
38
40
50
74
76
72
70
68
66
64
62
60
in
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Published May 30, 2000 (modified 11/21/00).

W
E
I
G
H
T
W
E
I
G
H
T
14
20
18
14
16
12
10
8
6
4
2
9
8
7
2
9
8
7
22
20
18
14
16
24
26
28
30
32
34
36
38
40
42
44
in
cm
kglb1
3
12
13
14
15
16
17
W
E
I
G
H
T
12
10
11
46
48
50
22
24
18
19
20
21
22
10
11
6
5
4
90
50
25
10
75
kg
in
cmLENGTH lb
6
5
Date Age Weight Length Head Circ. Comment
46 48 50 52 54 56 58 60 62
64 66 68 70 72 74 76 78 80 82 84 86 88 90 9290 94 96 98100
414039383735 36343332313029282726
24232221201918
97
3
Birth to 36 months: Boys
Head circumference-for-age and
Weight-for-length percentiles
NAME
RECORD #
12
Birth 3 1296 18 21 24 27 30 33 3615
52
50
48
46
44
42
40
38
36
32
cm
52
50
48
46
44
cm
20
19
18
17
16
15
14
13
in
20
19
18
in H
E
A
D
C
I
R
C
U
M
F
E
R
E
N
C
E
34
17
H
E
A
D
C
I
R
C
U
M
F
E
R
E
N
C
E
AGE (MONTHS)97
90
50
25
10
3
75
30
42
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Published May 30, 2000 (modified 10/16/00).

W
E
I
G
H
T
W
E
I
G
H
T
14
20
18
14
16
12
10
8
6
4
2
9
8
7
2
9
8
7
22
20
18
14
16
24
26
28
30
32
34
36
38
40
42
44
in
cm
kglb1
3
12
13
14
15
16
17
W
E
I
G
H
T
12
10
11
46
48
50
22
24
18
19
20
21
22
10
11
6
5
4kg
in
cmLENGTH lb
6
5
Date Age Weight Length Head Circ. Comment
46 48 50 52 54 56 58 60 62
64 66 68 70 72 74 76 78 80 82 84 86 88 90 9290 94 96 98100
414039383735 36343332313029282726
24232221201918
Birth to 36 months: Girls
Head circumference-for-age and
Weight-for-length percentiles
NAME
RECORD #
12
Birth 3 1296 18 21 24 27 30 33 3615
52
50
48
46
44
42
40
38
36
32
cm
52
50
48
46
44
cm
20
19
18
17
16
15
14
13
in
20
19
18
in H
E
A
D
C
I
R
C
U
M
F
E
R
E
N
C
E
34
17
H
E
A
D
C
I
R
C
U
M
F
E
R
E
N
C
E
90
50
25
10
75
30
AGE (MONTHS)
42
97
3
97
90
50
25
10
75
3
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Published May 30, 2000 (modified 10/16/00).

Health: KwaZulu-Natal Form Reference Number: Paed/14 Clinical Records: Paediatrics
Name: ____________________________ Folder no:_____________________
Progress notes for diarrhoeal disease Date: ___________________________ Note: If ½DD, Ringer’s or formula is not appropriate, then delete and write in the alternative
Time/Weight Time: Weight: Time: Weight: Time: Weight:
Intravascular vol ↑vol Ⓝvol ↓vol imminent arrest ↑ ↔ ↓ ↑ ↔ ↓ O2 + fluid Rx Bolus _____ml Ringer’s Bolus _____ml Ringer’s Bolus _____ml Ringer’s
Hydration Over normal 5% 10% Over normal 5% 10% Over normal 5% 10%
Stools: no., type ___ normal / ___ forming / ___ watery ___ normal / ___ forming / ___ watery ___ normal / ___ forming / ___ watery
Vomiting Nil + ++ Nil + ++ Nil + ++
Drinking Eagerly poorly nil Eagerly poorly nil Eagerly poorly nil
Urine output ____ ml = ____ ml/kg/hour not monitored ____ ml = ____ ml/kg/hour not monitored ____ ml = ____ ml/kg/hour not monitored
Assessment Well improving ISQ worse Well ☺ Well ☺
Calculation of fluid volumes
and types needed
Ⓜ ____ ml/kg/24 X wt hrs = ____ ml
Ⓡ ____ ml/kg/24 hrs X wt = ____ ml
Ⓛ ____ ml/kg/24 hrs X wt = ____ ml
As before
Ⓜ ____ ml/kg/24 X wt hrs = ____ ml
Ⓡ ____ ml/kg/24 hrs X wt = ____ ml
Ⓛ ____ ml/kg/24 hrs X wt = ____ ml
As before
Ⓜ ____ ml/kg/24 X wt hrs = ____ ml
Ⓡ ____ ml/kg/24 hrs X wt = ____ ml
Ⓛ ____ ml/kg/24 hrs X wt = ____ ml
As before
(ml/24hrs) Total ____ ml/kg/24 hrs X wt = ____ ml/24 hrs Total ____ ml/kg/24 hrs X wt = ____ ml/24 hrs Total ____ ml/kg/24 hrs X wt = ____ ml/24 hrs
If NPO, give as: ½ DD: ____ ml/hr ½ DD: ____ ml/hr ½ DD: ____ ml/hr
If taking orally, give as:
breast on demand or EBM/formula ___ ml X 8 / 6
PLUS IV½ DD ____ ml/hr or ORS ____ ml/hr via
NGT OR
ORS: ____ ml per stool or ORS: ad lib
breast on demand or EBM/formula ___ ml X 8 / 6
PLUS IV½ DD ____ ml/hr or ORS ____ ml/hr via
NGT OR
ORS: ____ ml per stool or ORS: ad lib
breast on demand or EBM/formula ___ ml X 8 / 6
PLUS IV½ DD ____ ml/hr or ORS ____ ml/hr via
NGT OR
ORS: ____ ml per stool or ORS: ad lib
Other Problems
and plans

Health: KwaZulu-Natal Form Reference Number: Paed/14 Clinical Records: Paediatrics
Name: ____________________________ Folder no:_____________________
Progress notes for diarrhoeal disease
Date: ___________________________ Note: If ½DD, Ringer’s or formula is not appropriate, then delete and write in the alternative
Time/Weight Time: Weight: Time: Weight: Time: Weight:
Intravascular vol ↑vol Ⓝvol ↓vol imminent arrest ↑ ↔ ↓ ↑ ↔ ↓ O2 + fluid Rx Bolus _____ml Ringer’s Bolus _____ml Ringer’s Bolus _____ml Ringer’s
Hydration Over normal 5% 10% Over normal 5% 10% Over normal 5% 10%
Stools: no., type ___ normal / ___ forming / ___ watery ___ normal / ___ forming / ___ watery ___ normal / ___ forming / ___ watery
Vomiting Nil + ++ Nil + ++ Nil + ++
Drinking Eagerly poorly nil Eagerly poorly nil Eagerly poorly nil
Urine output ____ ml = ____ ml/kg/hour not monitored ____ ml = ____ ml/kg/hour not monitored ____ ml = ____ ml/kg/hour not monitored
Assessment Well improving ISQ worse Well ☺ Well ☺
Calculation of fluid volumes
and types needed
Ⓜ ____ ml/kg/24 X wt hrs = ____ ml
Ⓡ ____ ml/kg/24 hrs X wt = ____ ml
Ⓛ ____ ml/kg/24 hrs X wt = ____ ml
As before
Ⓜ ____ ml/kg/24 X wt hrs = ____ ml
Ⓡ ____ ml/kg/24 hrs X wt = ____ ml
Ⓛ ____ ml/kg/24 hrs X wt = ____ ml
As before
Ⓜ ____ ml/kg/24 X wt hrs = ____ ml
Ⓡ ____ ml/kg/24 hrs X wt = ____ ml
Ⓛ ____ ml/kg/24 hrs X wt = ____ ml
As before
(ml/24hrs) Total ____ ml/kg/24 hrs X wt = ____ ml/24 hrs Total ____ ml/kg/24 hrs X wt = ____ ml/24 hrs Total ____ ml/kg/24 hrs X wt = ____ ml/24 hrs
If NPO, give as: ½ DD: ____ ml/hr ½ DD: ____ ml/hr ½ DD: ____ ml/hr
If taking orally, give as:
breast on demand or EBM/formula ___ ml X 8 / 6
PLUS IV½ DD ____ ml/hr or ORS ____ ml/hr via
NGT OR
ORS: ____ ml per stool or ORS: ad lib
breast on demand or EBM/formula ___ ml X 8 / 6
PLUS IV½ DD ____ ml/hr or ORS ____ ml/hr via
NGT OR
ORS: ____ ml per stool or ORS: ad lib
breast on demand or EBM/formula ___ ml X 8 / 6
PLUS IV½ DD ____ ml/hr or ORS ____ ml/hr via
NGT OR
ORS: ____ ml per stool or ORS: ad lib
Other Problems and plans

Health: KwaZulu-Natal Form Reference Number: Paed/24 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________ HIV Testing and Clinical Staging Record, and Comprehensive Care Plan
Test Date Age (Child) Result Child: exposed / infected
/ not infected Caregiver informed/post
test counselled (date)
Mother’s serology
Child’s serology
Initial PCR
Initial CD4
ART Started
CD4 % at time of staging (enter the most recent result)
Staging (at every HIV check-up, sign each parameter present; if uncertain, insert “?”) Date
Stage I Asymptomatic Persistent generalized lymphadenopathy Stage II Hepatosplenomegaly Papular pruritic eruptions Seborrhoeic dermatitis Extensive human papilloma virus infection Extensive molluscum contagiosum Fungal nail infections Recurrent oral ulcerations Lineal gingival erythema (LGE) Angular chelitis Parotid enlargement Herpes zoster Recurrent or chronic RTIs (otitis media, otorrhoea, sinusitis) Stage III Moderate unexplained malnutrition not adequately responding to standard therapy Unexplained persistent diarrhoea (14 days or more) Unexplained persistent fever (intermittent or constant, for longer than 1 month) Oral candidiasis (outside neonatal period) Oral hairy leukoplakia Acute necrotizing ulcerative gingivitis / periodontitis Pulmonary TB Tuberculous lymphadenopathy (axillary, cervical or inguinal) Severe recurrent presumed bacterial pneumonia Unexplained anaemia (<8gm/dl), &/or neutropenia (<500/mm3) &/or thrombocytopenia (<50 000/mm3) for > 1/12 Chronic HIV-associated lung disease including bronchiectasis Symptomatic lymphoid interstitial pneumonitis (LIP) Stage IV Unexplained severe wasting or severe malnutrition not adequately responding to standard therapy Pneumocystis pneumonia Recurrent severe presumed bacterial infection (eg empyema, pyomyositis, bone/joint inf, meningitis, but excl pneumonia) Chronic herpes simplex infection (orolabial or cutaneous of more than 1 month’s duration) Extrapulmonary TB Kaposi’s sarcoma Oesophageal candidiasis CNS toxoplasmosis (outside the neonatal period) HIV encephalopathy CMV infection (retinitis or infection of organs other than liver, spleen or lymph nodes; onset at age of ≥ 1 month) Extrapulmonary cryptococcosis including meningitis Any disseminated endemic mycosis (e.g. extrapulmonary histoplasmosis, coccidiomycosis, penicilliosis) Cryptosporidiosis Isosporiasis Disseminated non-tuberculous mycobacterial infection Candida of trachea, bronchi or lungs Visceral herpes simplex infection Acquired HIV-associated rectal fistula Cerebral or B cell non-Hodgkin’s lymphoma Progressive multifocal leukoencephalopathy (PML) HIV-associated cardiomyopathy or HIV-associated nephropathy
If HIV infected or exposed, turn over for comprehensive HIV care plan/schedule
Health: KwaZulu-Natal Form Reference Number: Paed/24 Clinical Records: Paediatrics
2007/06/08 2
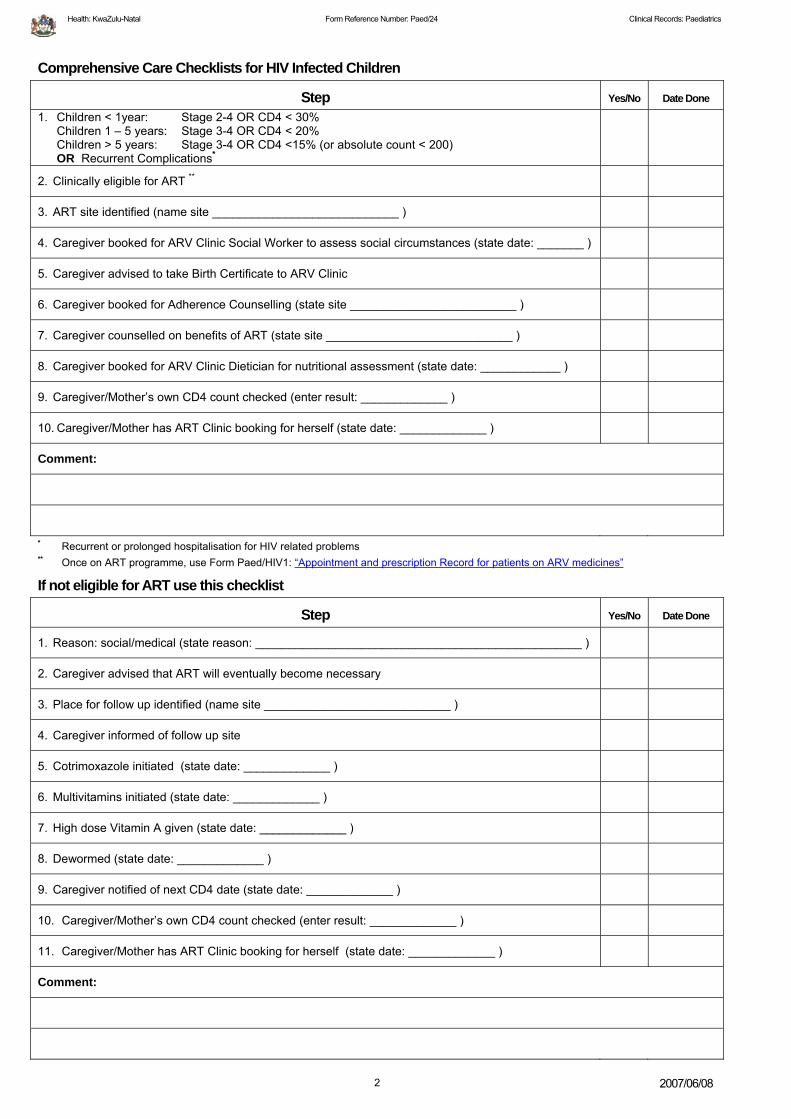
Comprehensive Care Checklists for HIV Infected Children
Step Yes/No Date Done 1. Children < 1year: Stage 2-4 OR CD4 < 30%
Children 1 – 5 years: Stage 3-4 OR CD4 < 20% Children > 5 years: Stage 3-4 OR CD4 <15% (or absolute count < 200) OR Recurrent Complications*
2. Clinically eligible for ART **
3. ART site identified (name site ____________________________ )
4. Caregiver booked for ARV Clinic Social Worker to assess social circumstances (state date: _______ )
5. Caregiver advised to take Birth Certificate to ARV Clinic
6. Caregiver booked for Adherence Counselling (state site _________________________ )
7. Caregiver counselled on benefits of ART (state site ____________________________ )
8. Caregiver booked for ARV Clinic Dietician for nutritional assessment (state date: ____________ )
9. Caregiver/Mother’s own CD4 count checked (enter result: _____________ )
10. Caregiver/Mother has ART Clinic booking for herself (state date: _____________ )
Comment:
* Recurrent or prolonged hospitalisation for HIV related problems ** Once on ART programme, use Form Paed/HIV1: “Appointment and prescription Record for patients on ARV medicines”
If not eligible for ART use this checklist
Step Yes/No Date Done
1. Reason: social/medical (state reason: _________________________________________________ )
2. Caregiver advised that ART will eventually become necessary
3. Place for follow up identified (name site ____________________________ )
4. Caregiver informed of follow up site
5. Cotrimoxazole initiated (state date: _____________ )
6. Multivitamins initiated (state date: _____________ )
7. High dose Vitamin A given (state date: _____________ )
8. Dewormed (state date: _____________ )
9. Caregiver notified of next CD4 date (state date: _____________ )
10. Caregiver/Mother’s own CD4 count checked (enter result: _____________ )
11. Caregiver/Mother has ART Clinic booking for herself (state date: _____________ )
Comment:

Health: KwaZulu-Natal Form Reference Number: Paed/HIV1 Clinical Records: Paediatrics
Name:____________________________ Folder Number:__________________
Appointment and prescription record for patients on ARV medicines
Appointment Date MO initials
Pharm initials
Weight + Height CD4 Viral
Load Comment
Start treatment
First 2 week
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
10th month
11th month
12th month

Health: KwaZulu-Natal Form Reference Number: Paed/HIV1 Clinical Records: Paediatrics
Name:____________________________ Folder Number:__________________
Appointment Date MO initials
Pharm initials
Weight + Height CD4 Viral
Load Comment
2

Health: KwaZulu-Natal Form Reference Number: Paed/25 Clinical Records: Paediatrics
This is a PATIENT HELD Record
Chronic Rheumatic Heart Disease: Antibiotic Prophylaxis
Re: Name of Patient: _________________________________________ Folder Number_______________________
The above patient has Chronic Rheumatic Heart Disease. The first episode of Acute Rheumatic Fever was in _______________. S/he is left with the following cardiac problems:
1. ______________________________________ 2. ______________________________________
3. ______________________________________ 4. ______________________________________
S/he should receive continuous penicillin prophylaxis as per the schedule below at EXACTLY 4 week intervals. Please could you dispense according to the schedule below. Please refer the child to the doctor if s/he has symptoms. S/he also receives the following treatment:
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
Please also supply these at the 4 weekly intervals.
Sign: _________________________
Penilente (LA) 1,2 MU IMI at 4 weekly or PenVK 250mg-500mg per os bd (if oral used, also indicate date of issue and date of next collection)
Date Due Date Given Place Given Signature INR Warfarin Dose
Indications for antibiotic prophylaxis against Infective Endocarditis
All dental procedures, including cleaning by a dental hygienist Childbirth
Any instrumentation of the gastro-intestinal, urinary, genital or upper respiratory tracts
Dental procedures
Antibiotics No anaesthetic: Penicillin Allergic:
>10 years Amoxicillin3 grams <10 years Erythromycin 500 mg <10 years Amoxicillin 1,5 grams >10 years Erythromycin 1 gram
Anaesthetic:
Penicillin or Amoxicillin equivalent


Health: KwaZulu-Natal Form Reference Number: Paed/28 Clinical Records: Paediatrics
Chronic Rheumatic Heart Disease Follow Up Continuation Sheet
Name: __________________________________________ Folder No.: __________________________ Nearest Town: ________________________________ Nearest Clinic/Hospital: _______________________ (For monthly treatment)
Acute Rheumatic Fever Episode Date: _________________
Acute Rheumatic Fever Criteria (tick applicable) Evidence of preceding
Streptococcal infection Culture Rising ASOT Scarlet Fever None Unknown
Major Criteria Pancarditis Flitting Arthritis Chorea Erythema Marginatum
Subcutaneous nodules
Minor Criteria Long PR Interval Arthralgia Previous ARF/RHD Fever Raised
ESR/CRP/WCC
Date
Weight
Height
Pulse Rate
Blood Pressure
Prophylaxis letter checked
Effort tolerance/symptoms
CVS (anatomy & haemodynamics highlights)
CXR: CTR%
ECG: Chamber hypertrophy
Echo
IALCH last date/next date
Artificial Valve Candidate: y/n
Artificial Valve: y/n
INR/Warfarin
Medication
New Problems
Other Problems
Sign


Health: KwaZulu-Natal Form Reference Number: Paed/36 Clinical Records: Paediatrics
Children’s Coma Score Sheet: children under 4 years Name: ______________________ Folder Number: _________________
Date Time
Eye opening Spontaneously 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4
To verbal stimuli 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 To pain 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2
No eye response to pain 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 Best Motor Response
Obeys verbal command or moves normally 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 Localise pain or withdraws to touch 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
Withdraws from pain 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 Abnormal flexion to pain (decorticate) 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3
Abnormal extension to pain (decerebrate) 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 No motor response to pain 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Best Verbal Response Alert; babbles; coos; usual words and sentences 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
Less than usual ability and/or spontaneous irritable cry 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 Cries inappropriately 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3
Occasionally whimpers and/or moans 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 No verbal response to pain 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Total Suspected Phenobarb aetiology: Phenytoin Infection Benzodiazipine Trauma Opiate Seizures Thiopentone
Toxin Other CVA Pulse
Tumour BP Inborn error Respiratory rate
Other Left Pupil Right pupil
PTO for children 4 - 15 years

Health: KwaZulu-Natal Form Reference Number: Paed/24 Clinical Records: Paediatrics
Children’s Coma Score Sheet: children 4-15 years Name: ______________________ Folder Number: _________________
Date Time
Eye opening Spontaneously 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4
To verbal stimuli 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 To pain 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2
No eye response to pain 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 Best Motor Response
Obeys verbal command 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 6 Localise pain 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
Withdraws from pain 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 Abnormal flexion to pain (decorticate) 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3
Abnormal extension to pain (decerebrate) 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 No motor response to pain 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Best Verbal Response Orientated and converses 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5 5
Disorientated and converses 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 Inappropriate words 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3 3
Incomprehensible sounds 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 2 No verbal response to pain 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
Total Suspected Phenobarb aetiology: Phenytoin Infection Benzodiazipine Trauma Opiate Seizures Thiopentone
Toxin Other CVA Pulse
Tumour BP Inborn error Respiratory rate
Other Left Pupil Right pupil
PTO for children under 4 years

Health: KwaZulu-Natal Form Reference Number: Paed/27 Clinical Records: Paediatrics
Checklist for Documenting Brain Death
Name:__________________________ Date of Birth:__________ Folder No.:_________
I Diagnosis Cause of Coma
II Laboratory Information 1. Blood Glucose Date&Time
2. CNS Depressing Drugs
Drug and dose Date&Time
Blood Level Date&Time
3. Toxicology Screen
III Clinical Examination Examiner 1 Examiner 2 Date
Time
Temperature
Blood Pressure
No spontaneous movements: (including no decorticate or decerebrate posturing or shivering)
Cranial Nerves
1. Pupils fixed and dilated
2. No corneal reflexes
3. No doll’s eye movement when head turned
4. No eye movement when auditory canals irrigated with ice water for 1 minute (clear tympanic membranes)
5. No cough when trachea suctioned
5. No motor response in cranial nerve distribution to painful stimulation
Apnoea Test (on IPPV: 100% O2 for 5 min then turn off IPPV for 5 min)
1. pCO2 at end of test
2. O2 saturation at end of test
3. pH at end of test
IV Isotope brain scan (if available) Date&Time V Having considered the above findings we certify the death: Examiner 1 Examiner 2
Date
Time
Signed
Print Name
From Red Cross War Memorial Children’s Hospital, Cape Town


Health: KwaZulu-Natal Form Reference Number: Paed/32 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Burns chart for assessing total body surface area burnt Use this chart on every child admitted with burns
Date of burn: _____________ Agent: ________________ Time of burn: ____________ Date of assessment: _____________ Time of assessment: ____________ Name (print): _____________ Sign: ____________


Health: KwaZulu-Natal Form Reference Number: Paed/29 Clinical Records: Paediatrics
Date: Monitoring & handover sheet for paediatric transfers
(to be completed by referring and receiving doctors starting at time of referral) Time: Patient Name: Date of Birth: DoA: DoT:
1) REFERRING AND RECEIVING INFORMATION
Hospital Ward Doctor Designation Contact number
Referring Junior:
Senior:
Receiving Junior:
Senior:
2) CAREGIVER INFORMATION Accompanying
caregiver: Relationship: Contact number:
3) NUTRITION
OWFA Normal UWFA Marasmus Kwashiorkor M-K Unknown Weight: _____kg
4) HIV
Laboratory test Negative Exposed Infected No result Not tested (but indicated)
Not tested (not indicated) Unknown
Clinical Stage I Stage II Stage III Stage IV Not staged (but indicated)
Not staged (not indicated) Unknown
ARV Current Ever Never (but indicated) Never (not indicated) Unknown
5) CURRENT CONDITION (CIRCLE APPLICABLE) TIME:
Vitals Temp: PR: RR: Sats: Airway Critical Narrow Normal
Breathing Needs IPPV Needs oxygen Hyperventilation Normal Circulation Shock (Cap refill > 3s) Hypovolaemia Hypervolaemia Normal
Consciousness (AVPU) Unconscious Response to Pain Response to Voice Alert Convulsions In hospital Before arrival Past Never Dehydration 10% 5% Oedema Normal
IMCI classification “Red” “Yellow” “Green” Infection SIRS (“toxic shock”) Needs IV agent Needs oral agent No
6) SIGNIFICANT BIOCHEMICAL PROBLEMS (CIRCLE APPLICABLE)
Hypoxia (Sats in air____) Hypoglycaemia pH < 7.2 K+ < 2.0 K+> 6 Na+<120 Na+> 150 Albumin < 20
7) REASON FOR TRANSFER OR NON-ACCEPTANCE
Accepted(circle applicable): YES NO ICD 10
Main diagnosis / problem:
Other diagnoses / problems:
Prognosis for survival: Excellent Good Indeterminate Guarded
Prognosis for normal outcome: Excellent Good Indeterminate Guarded
Main reason for transfer / non acceptance:
8) URGENT MANAGEMENT
Specific Rx (circle or state) Other Rx Airway ETT / oral airway / none Oxygen delivery:
Breathing IPPV / Bag / Spontaneous Oxygen monitoring: Circulation/Shock Intra-osseous / peripheral IV / central IV / none Volume expand:
Dehydration IV / Oral ½ DD / ORS: Consciousness Protect airway: Coma position:
Infection IV antibiotic stat: Steroid / antipyretic:
9) PAIN ASSESSMENT
No pain Mild pain Moderate pain Severe pain Analgesia plan:

Health: KwaZulu-Natal Form Reference Number: Paed/08 Clinical Records: Paediatrics
2007/06/26 2
10) ONGOING MONITORING AND RESPONSIBILITY WHILE AWAITING EMRS Name Rank Contact number
Doctor
Nurse
Time Temp Heart rate
Resp rate Sats Fi O2
O2 device
IV site secure
IV control device
IV rate AVPU score BP Gluc. Sign
On transfer
to ambulance
11) PROBLEMS ARISING AND THEIR PLANS WHILE AWAITING EMRS Problem Plan Discussed with Verified by
12) PATIENT TRANSPORT INFORMATION
Time accepted Receiving Hospital Doctor Rank Telephone Plan Sign
Time EMRS called EMRS Ops Centre Operator Designation Telephone Plan Sign
Time of EMRS arrival
Ambulance type Paramedic Designation Telephone Plan Sign
Time of departure, AND receiving
hospital notified
Receiving Hospital Doctor Rank Telephone Plan Sign
Time of arrival at receiving hospital Receiving Ward Doctor Rank Telephone Plan Sign
13) PATIENT HANDOVER
Handed over by Received by
Time Handover Point Name Designation Name Designation Sign
Referring hospital to EMRS
EMRS to receiving hospital
14) CAREGIVER PLAN
Name Relationship Contact number Breastfeeding Well/sick Plan for transport to receiving
hospital y/n
15) OUTCOME
Alive & not transferred
Died & not transferred
Died awaiting EMRS Died in transit
Died within 24 hours of transfer
Died beyond 24 hours of transfer
Alive and transferred back
to referring hospital
NB: this does not replace the usual referral letter containing ALL relevant clinical details; use the ‘Paediatric Discharge/Referral Letter’ proforma

Health: KwaZulu-Natal Form Reference Number: Paed/30 Clinical Records: Paediatrics
Paediatric in-transit monitoring sheet (to be used by EMRS personnel)
Patient Name: Date of Birth: Date: Time:
1) REFERRING AND RECEIVING INFORMATION
Hospital Ward Doctor Designation Contact number
Referring Junior:
Senior:
Receiving Junior:
Senior:
2) REASON FOR TRANSFER
ICD 10
Main diagnosis / problem:
Other diagnoses / problems:
Prognosis for survival: Excellent Good Indeterminate Guarded
Prognosis for normal outcome Excellent Good Indeterminate Guarded
Main reason for transfer:
3) PAIN ASSESSMENT
No pain Mild pain Moderate pain Severe pain
Analgesia plan:
4) ONGOING MONITORING AND RESPONSIBILITY IN TRANSIT Name Rank Contact number Sign
Paramedic/EVC
Assistant
Time Temp Heart rate
Resp rate Sats Fi O2
O2 device
IV site secure
IV control device
IV rate GCS BP Glucose Sign
In ambulance by EMRS
In ward by receiving
doctor
5) PROBLEMS ARISING AND PLANS IN TRANSIT
#1: #2:
Plan: Plan:
Discussed with: Discussed with:
6) PATIENT HANDOVER
Handover by Received by
Time Handover Point Name Designation Name Designation Sign
EMRS to receiving hospital
If further recording is required, or if problems were encountered, use space overleaf

Health: KwaZulu-Natal Form Reference Number: Paed/08 Clinical Records: Paediatrics
2007/06/08 2
Notes:
Problems encountered with the actual transfer:
Plan for reporting problems:

Health: KwaZulu-Natal Form Reference Number: Paed/23 Clinical Records: Paediatrics
Paediatric Discharge/Referral Letter Hospital: Date: Patient Name: Date of Birth: DOA: Age:
Address: Gender: Male / Female DOD:
OP Number: Ward:
IP Number: Doctor in charge:
Referred by: Healthworker Clinic Hospital Private Practice
Name: Self
Outcome: Alive Dead Transferred to another hospital:
Dear Colleague Thank you for receiving the above-named patient. The child was found to have the following problems:
1 (main diagnosis) ICD Code
4 ICD Code
2 5
3 6
At admission the weight was ________ kg and the nutritional status was:
Normal UWFA Kwashiorkor Marasmus Marasmic Kwashiorkor
The discharge weight was ________ kg
Perinatal History
HIV and TB
HIV Date Age (Child) Result Child Exposed /
Infected / Not infected Caregiver informed
(date) Mother’s serology
Child’s serology Initial PCR
Current CD4 ART Started
Clinical stage 1 2 3 4 Not staged Tuberculosis Contact: Skin test: CXR: Rx started:
Vaccinations
Up to Date Incomplete → action taken:
Social History
Qualifies for Grant: CSG / CDG / FCG Caregiver advised: Y / N Letter given: Y / N
Family History
Development
Normal Delayed → action taken:
Past Medical History

2007/06/26 2
Progress in the ward (document each problem, and its management and course, separately)
Prescription at discharge (drug AND dose)
1 4
2 5
3 6
Future plans and follow up arrangements (including for HIV) Problem Follow up date Follow up venue
Remarks
The Road to Health Chart was checked and updated Yes No Not present Yours sincerely
Sign: _______________________ Print/Stamp: _____________________ Date: _________________
Contact Number: ______________________

Health: KwaZulu-Natal Form Reference Number: Paed/38 Clinical Records: Paediatrics
P A E D I A T R I C R E C O R D A U D I T DATE: ___________________________ HOSPITAL: ___________________________ DATE OF PATIENT’S ADMISSION: ___________________________ PATIENT’S DIAGNOSIS: ___________________________
Check each document for the following:
Paediatric Patient Record A. PATIENT’S DETAILS: N/C P/C C COMMENTS Name and Initials recorded on very page Hospital number recorded on every page Date of birth recorded wherever indicated Name and contact details for primary care giver clearly recorded wherever indicated
C. DOCUMENTATION Standardised Paediatric Record Keeping system used Record compiled exactly according to policy Clinical notes, including referral letters, in chronological order Clinical notes, including referral letters are legible Identifiable name on every entry Cover page filled in Second page (background information) filled in Weight plotted on growth chart Results sheet filled in Signature on all results/reports of investigations e.g. bloods, x-rays, etc.
HIV testing and staging filled in Admission times recorded Consultation times recorded Appropriate history taken Appropriate clinical examination performed Requests of special diagnostic tests documented Details of medical findings leading to a diagnosis are recorded An assessment of the child’s problems is recorded A comprehensive problem list is recorded A plan is made for each problem Treatment prescribed, in notes, and on prescription sheets Intake (oral and IV when indicated) in notes and intake/output sheet Nursing orders are clearly documented Every consultation/clinical encounter with patient is recorded Every referral to other services is recorded clearly The findings and plans of other services involved in the patient’s care are clearly documented
Abbreviations are kept to a minimum or made clear

Last modified: 15 June 2007 For review: 2007 2
D. INFORMATION FOR PARENTS / CARE GIVER N/C P/C C COMMENTS Carer/child is informed of diagnoses and problems and this is documented
Carer/child is informed of management/treatment plan and this is documented
Carer/child is informed of prognosis and this is documented Patient and carer participate in decision-making relating to treatment, and same documented
Informed consent is obtained when necessary and this is documented
E. DISCHARGE OF PATIENTS Unresolved problems at discharge are clearly stated and documented Follow-up plans (including places and dates) for each problem are agreed with patients and carers by doctors prior to discharge and documented
Discharge medication (drugs and dosing) clearly documented in the discharge letter
Discharge summary in the paediatric patient record and a copy filed in the ward
Adequate Health Education is given to caregivers during hospitalisation and on discharge
GENERAL OVERVIEW / COMMENTS This paediatric patient record reflects quality medical care This paediatric patient record reflects comprehensive care The guideline on quality paediatric record keeping was followed If this was my own child, I would be happy with this clinical record Auditor’s name: ___________________________ Signature: _______________________ Outcome of audit Reported by: ____________________________________ Reported to: ____________________________________ Date: ____________________________________ Rating: Non-compliant (n/c) = 0 Partially compliant (p/c) = 1 Compliant (c) = 2

Health: KwaZulu-Natal Form Reference number: Paed/A Clinical Records: Paediatrics
Clinical Record Keeping in the Nursery
It is a good idea to standardise the structure for Neonatal Inpatient Folders, and for filing of non-current records.
An example, which REALLY works, follows.
All charts must be exactly the same (inside Ring Binders) Section (each section separated by a file divider) Healthworker responsible
1) Patient’s clinical notes Doctor
2) Doctor’s obs (results page, scoring sheets etc) Doctor
3) Nursing obs (“routine”, ventilator, phototherapy, etc) Nurse
4) Nursing Process Nurse
5) Intake/Output/Feeds Nurse
6) Prescription Doctor and Nurse to check all sheets every day
7) Road to Health Chart Doctor and Nurse to fill in relevant sections when appropriate
8) Miscellaneous “Clearing House” for anything awaiting filing (empty daily)
All charts are in chronological order Section Order
Baby’s clinical notes Front to Back
Doctor’s obs (results page, scoring sheets etc) Front to Back
Nursing obs (“routine”, ventilator, phototherapy, etc) Back to Front
Nursing Process Back to Front
Intake/Output/Feeds Back to Front
Prescription Back to Front
Important instructions Non-current pages are removed after one - two days
This applies to all sections except patient’s clinical notes Results must be entered on results page, signed by attending doctor and filed Each page should have patient’s name and hospital number Notes should be problem orientated and focussed If any change is made to the management of the patient, this change and the reason for the change must be
documented When “filing” non-current pages, use a paper binder and keep the pages in chronological order When “filing” non-current pages, bind like with like All the different kinds of pages (progress, prescription, intake/output, special observations etc.) used in your
unit/department should be standardised
Each Ward should have a “Gold Standard” folder to refer to for structuring folders, and to compare with during chart review meetings.


Health: KwaZulu-Natal Form Reference Number: Paed/B Clinical Records: Paediatrics
Using the Newborn Care Record
Using the Infant Care Record, and following these instructions for its use will immediately enable the improvement of the quality of care babies receive, and will make your looking after them more efficient
ALWAYS PRINT YOUR NAME CLEARLY Newborn Care Record: 1st page (ALL live births) 1. Birth attendant (midwife and/or doctor) to fill in all maternal and resuscitation details, marking where necessary the
appropriate response boxes. Where pregnancy, labour and/or delivery problems are noted, give detail on Page 3 in the space provided
2. The apgar scores should be transposed from the table on the back page 3. Birth attendant’s name MUST appear in the bottom right corner 4. When WR is positive, write in the titre in the space provided 5. When filling in the weight scale, start in the space provided between 36 and 37 degrees. Use weight gradations of
50 grams 6. The front page becomes the daily snapshot of the clinical course 7. When babies stay longer than 14 days, use the continuation weight/temperature chart, but start the weight scale in
the space provided between 34 and 35 degrees, and continue using weight gradations of 50 grams 8. The “Problem List” is to be filled in, as problems are identified (don’t use this space for clinical notes, or X-ray
registers e.t.c.). Start getting into the habit of entering the ICD 10 codes as well
2nd page (ALL live births) 1. Birth attendant to fill in information on previous pregnancies and on the placenta, and to complete the relevant
identification section 2. When urine or meconium are passed or when abnormalities are noted, these should be documented on the
“Examination check list” even if they are noted at a time prior to the formal First Examination 3. First examination table to be completed by the person performing the first examination. This should be done within
24 hours of delivery. Remember to print your name and sign
3rd page (only if problems - no matter how trivial - are encountered) 1. Insert the referral letter here if there is one 2. Details of abnormalities during pregnancy, labour and or/delivery to be documented in the space provided 3. Clinical “First Contact” notes start below this. Doctors AND nurses can use the same pages for clinical notes 4. List the significant problems on the front page as well 5. Clinical notes continue on page 5 (using a ‘ring-binder’)
4th page 1. Use the “Apgar Scoring Chart” to score all babies. Transpose the totals to the space provided on page 1.
Remember to print your name and sign 2. A 10 minute apgar need only be done if the baby needs ongoing resuscitation 3. On the “Discharge Check and Plan”, the “Unresolved Problems” list should only be completed at discharge
Continuation Pages 1. Number continuation pages starting from 5 2. Write patient registration details on each page, or use a sticker
Referring When referring or transferring baby to another facility, the Newborn Care Record or a photocopy thereof should travel with the baby (this makes writing a long referral letter unnecessary). Any additional information in a referral letter should be in duplicate, the original with the patient, and the copy in the folder as a clinical record kept in chronological order with the rest of the clinical notes.


Health: KwaZulu-Natal Form reference number: Paed/01 Clinical Records: Paediatrics
Page 1
MOTHER Baby’s Name: Baby’s Number: Birthweight (g)
Name:
Gender: ♂ / ♀ Address: Length (cm)
Folder Number:
Age: Grav: Para: Date of Birth: (use sticker when available)
COH (cm)
Pregnancy Received ANC: ⓎⓃTime of birth NVD Breech Assisted C/S LMP (mm/yy) / EDD /
Date
VDRL/WR: ⊕ ⊖
Titre:1/ Rx X 3: ⓎⓃPCV/Hb
Blood Group: Antibodies: ⓎⓃTSB
Hypertension/PIH: ⓎⓃ Diabetes: ⓎⓃPhototherapy
TB: ⓎⓃ Cardiac: ⓎⓃWeight(g) ℃ m e m e m e m e m e m e m e m e m e m e m e m e m e m e Epilepsy: ⓎⓃ APH: ⓎⓃ
Alcohol: ⓎⓃ Smoker: ⓎⓃ40 Labour Induced: �� ROM: hrs
1st Stage: hrs 2nd Stage: mins
Pyrexia: ⓎⓃ AB’s: ⓎⓃ
39 Analgesia: ⓎⓃ Foetal distress: ⓎⓃBABY
Apgar:1min 5 min 10 min
Resuscitation 38
MSL: ⓎⓃ SuctionedⓎⓃAction: None: ⓎⓃ Oxygen: ⓎⓃ
Mask ventilation: ⓎⓃ ETT+IPPV: ⓎⓃ37 Drugs:
‘Distress’ Indicators: TSR: (mins)
Cord pH: Cord BE:
36 Cord Blood
Group: Coombs: ⊕ ⊖ WR: ⊕ ⊖Gestational Age Estimate: weeks
US: weeks Scored: weeks35 AGA UGA OGA
MTCT: Mother ⊕ /⊖ /? Breast / Formula
Mother NVP: Ⓨ/Ⓝ/?/na Baby NVP: Ⓨ/Ⓝ/?/na
34 Problem List ICD
Antibiotic 1
Antibiotic 2
% Oxygen
IPPV / CPAP
Other:
Feed
s
IV (ml/hr)
ml/kg/day
Birth Attendant Print: Sign:
Age (day) Put to breast in LW? Ⓨ Ⓝ

Page 2
First Examination (mark the appropriate block) Previous Pregnancy Appearance Well Sick Dysmorphic Year Abnormalities
Temperature 36-37 °C Hypothermic Hyperthermic 1.
Nutrition Well nourished Obese Wasted 2.
Odour Normal Offensive 3.
Behaviour Responsive Lethargic Irritable Jittery 4.
Colour Pink Blue Plethoric Pale Jaundice 5.
Apex bpm 120-160 /min Tachycardia Bradycardia Murmur Placenta Breast/Nipples Normal Wide-spaced Engorged Discharging Accessory Weight:
Resp. rate 40-60 /min Fast Slow Irregular Appearance:
Chest movement Symmetrical Asymmetrical Shallow Clots:
Recession Absent Costal Sternal Number of Cord vessels:
Breath sounds Quiet Grunting Noisy Cord knots:
Abdomen Normal Distended Scaphoid Large liver Large spleen Recorded by (print):
Umbilicus Normal Moist Flare Bleeding Mec. stained Vitamin K given
Femoral pulses Present Absent Site Date:
Genitalia: Male Testes down Undescended Hydrocoele Inguinal hernia Hypospadias Print name: Sign:
Genitalia: Female Normal Ambiguous Eye prophylaxis given Date:
Urine Passed Not passed Print name: Sign:
Anus Patent Imperforate Identification Meconium Passed Not passed At Birth Date:
Hips Normal Dislocated Dislocatable Midwife (print): Sign:
Legs Normal Not moving Asymmetrical Witness (print): Sign:
Feet position Normal Posit. deformity Clubbed Mother (print): Sign:
Toes Normal Polydactyly Syndactyly (or) Mother’s Thumbprint
Arms Normal Not moving Asymmetrical
Palmar creases Normal Single
Fingers Normal Polydactyly Syndactyly
Grasp reflex Present & equal Weak Absent
Moro reflex Present & equal Asymmetrical Weak Absent Nursery Date
Clavicles Intact Fracture Brought by (print): Sign:
Suck reflex Present Weak Absent Received by (print): Sign
Mouth Normal Smooth philtrim Cleft lip Ward Date:
Palate Intact Cleft hard Cleft soft Brought by (print): Sign:
Tongue Normal Large Protruding Received by (print): Sign
Chin Normal Small Mother (print): Sign:
Face Symmetrical Asymmetrical Abnormal (or) Mother’s Thumbprint
Nose Patent Blocked
Eyes Normal Small Large Slanting Infected
Ears Normal Abnormal Low position
Neck Normal Swellings Webbed
Back Normal Meningocoele Sacral dimple Hair tuft Scoliosis Footprint Head shape Normal Asymmetrical Caput Haematoma Trauma
Fontanelles Normal Bulging Large Third Sunken
Sutures Mobile Overriding Widened Fused
Muscle tone Normal Hypotonic Hypertonic Skin Intact Bruising Rash Purpura
Cry Normal Hoarse High-pitched Weak Absent
Assessment:
Assessed by (print name): Sign:
Date: Time:

Page 3 Clinical notes are continued on page 5
Date Abnormalities in Current Pregnancy and Labour Print name
Date Time First Contact Notes Print name

Page 4
Apgar Scoring Chart (circle appropriate number, an accurate score is essential) Assessment 1 Minute 5 Minutes 10 Minutes
None 0 0 0 Heart rate Less than 100 1 1 1
More than 100 2 2 2 Absent 0 0 0
Respiration Weak/Irregular 1 1 1 Good/Cries 2 2 2 Central Cyanosis 0 0 0
Colour Peripheral Cyanosis 1 1 1 Peripherally Pink 2 2 2 Limp 0 0 0
Tone Some Flexion 1 1 1 Active/Well Flexed 2 2 2 None 0 0 0
Response to stimulation Some Response 1 1 1 Good Response 2 2 2
Total Score /10 /10 /10
Scored by: Print name Sign Date
Pre-discharge Checklist
Checked by: Pint Name: Sign: Date:
Feeding well y n Breast fed y n Eyes normal y n Jaundice y n
Cord infection y n Cord stump normal y n Meconium passed y n Urine passed y n
BCG given y n Polio given y n Health Education given: Buttock care y n Infant feeding y n
Cord care y n General hygiene y n RTHC filled in y n RTHC instruction y n Birth registration done y n
Unresolved problems at discharge Plan at discharge (include Rx)
1.
2.
3.
4.
5.
Follow up place: Follow Up date:
PMTCT site: PMTCT date:
Discharged by (Print Name): Sign: Designation:
Discharged to (Print Name): Sign: Relationship:
Identified by ID: (or) Thumbprint
Abbreviations: ANC=antenatal care, (g)=grams, (cm)=centimetres, COH=circumference of head, Grav=gravida, Para=parity, EDD=estimated date of delivery, PMTCT=mother to child transmission prevention, VDRL=syphilis serology, TB=tuberculosis, APH=antepartum haemorrhage, MSL=meconium stained liquor, ETT+IPPV=endotracheal tube plus ventilation, TSR=time to spontaneous respiration, Cord pH=acidity of cord blood, Cord BE=base excess of cord blood, ICD=international classification of disease, PCV=packed cell volume, TSB=total serum bilirubin, IPPV=intermittent positive pressure ventilation, CPAP=continuous positive airways pressure, IV=intravenous, ml/kg/day=millilitres per kilogram per day, LW=labour ward, Resp.=respiration, Posit.=Positional, BCG=TB vaccine, RTHC=road to health card, (mm/yy)=month/year, NVP=nevirapine (or alternative), PMTCT=prevention of mother to child transmission, AGA/UGA/OGA=appropriate/underweight/overweight for gestational age
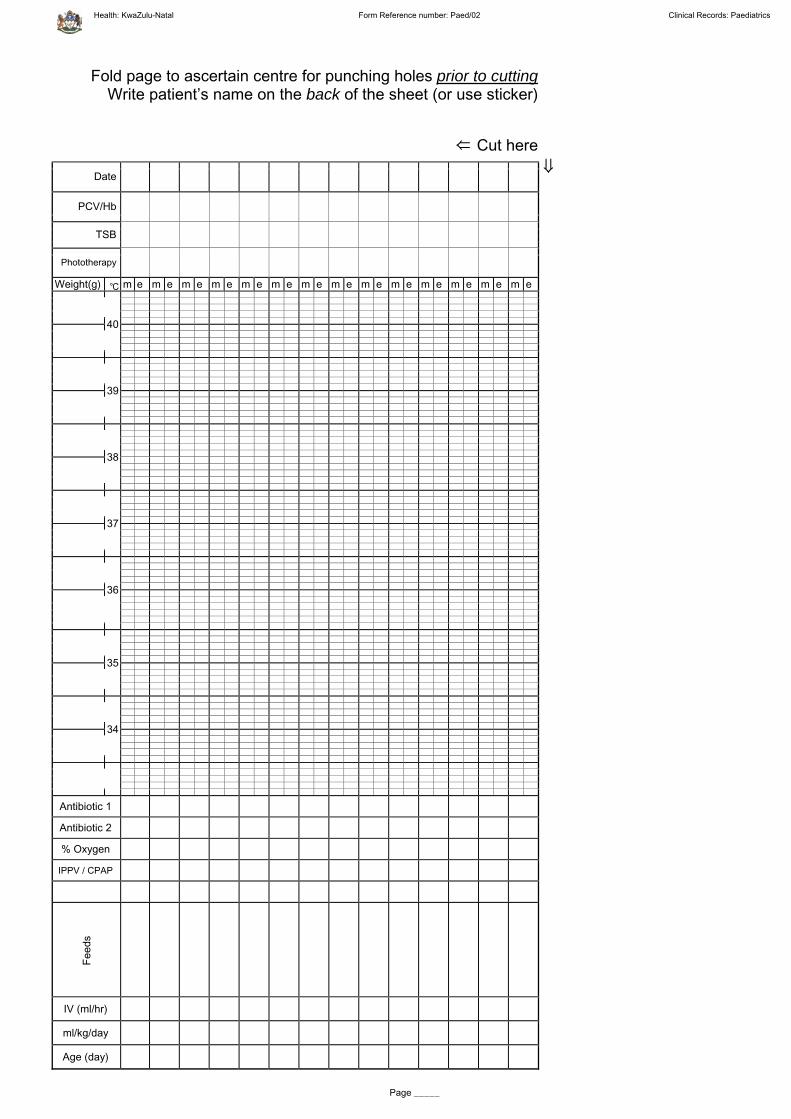
Health: KwaZulu-Natal Form Reference number: Paed/02 Clinical Records: Paediatrics
Page _____
Fold page to ascertain centre for punching holes prior to cuttingWrite patient’s name on the back of the sheet (or use sticker)
⇐ Cut here
Date
PCV/Hb
TSB
Phototherapy
Weight(g) ℃ m e m e m e m e m e m e m e m e m e m e m e m e m e m e
40
39
38
37
36
35
34
Antibiotic 1
Antibiotic 2
% Oxygen
IPPV / CPAP
Fee
ds
IV (ml/hr)
ml/kg/day
Age (day)
⇓


Health: KwaZulu-Natal Form Reference number: Paed/03 Clinical Records: Paediatrics
Name: __________________________ Folder Number: _______________________
PAGE _____
Date&Time Problem Clinical Notes Investigation Management

Health: KwaZulu-Natal Form Reference number: Paed/03 Clinical Records: Paediatrics
Name: __________________________ Folder Number: _______________________
PAGE _____
Date&Time Problem Clinical Notes Investigation Management

Health: KwaZulu-Natal Form Reference number: Paed/04 Clinical Records: Paediatrics
Name: ______________________________ Folder Number: _______________________ Date of Birth: ______________
Dubowitz/Ballard Exam for Gestational Age Physical Maturity -1 0 1 2 3 4 5
Skin Sticky, friable, transparent
Gelatinous red, translucent
Smooth pink, visible veins
Superficial peeling and/or rash, few veins
Cracking, pale areas, rare
veins
Parchment, deep cracking,
no vessels
Leathery, cracked, wrinkled
Lanugo None Sparse Abundant Thinning Bald areas Mostly bald
Plantar Creases
Heel-toe 40-50 mm = -1,
Heel-toe >50 mm, no creases Faint red marks
Anterior transverse crease
only
Creases over anterior 2/3
Creases over entire sole
Breast Imperceptible Barely perceptible
Flat areola, no bud
Stippled areola, 1-2 mm bud
Raised areola, 3-4 mm bud
Full areola, 5-10 mm bud
Eye & Ear Lids fused, loosely = -1, tightly = -2
Lids open, pinna flat, stays
folded
Slightly curved pinna, soft with
slow recoil
Well-curved pinna, soft but ready recoil
Formed and firm, with
instant recoil
Thick cartilage, ear stiff
Genitals, male
Scrotum flat, smooth
Scrotum empty, faint rugae
Testes in upper cannal, rare
rugae
Testes descending, few
rugae
Testes down, good rugae
Testes pendulous, deep
rugae
Genitals, female
Clitoris prominent, labia flat
Prominent clitoris, small labia minora
Prominent clitoris,
enlarging minora
Majora and minora equally
prominent
Majora large, minora small
Majora cover clitoris and
minora
Physical Score: ________
Neuromuscular Maturity
Neuromuscular Score: _______
Total Score: _______ Maturity Rating: _______
Maturity Rating Add up the individual Physical and Neuromuscular maturity scores for the twelve categories, then obtain the estimated gestational age from the table below.
Total Score
Gestational Age, Weeks
-10 20 -5 22 0 24 5 26 10 28 15 30 20 32 25 34 30 36 35 38 40 40 45 42 50 44
Plot weight on the growth chart overleaf, then decide on:
OGA AGA UGA (overweight for gestational age) (appropriate for gestational age) (underweight for gestational age)
Last modified: 08 June 2007 For review: 2009

Health: KwaZulu-Natal Form Reference number: Paed/04 Clinical Records: Paediatrics
Last modified: 08 June 2007 For review: 2009

Health: KwaZulu-Natal Form Reference number: Paed/05 Clinical Records: Paediatrics
Hypoxic Ischaemic Encephalopathy Score Sheet Name: ______________________ Folder Number: _________________
Date of Birth: _______________
Sco re at D e
Sign 0 1 2 3 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Tone Normal Hyper Hypo Flaccid
LOC Normal Staring Lethargic Comatose
Fits None <3/day >2/day
Posture Normal Fisting Frog-like Decerebrate
Moro Normal Partial Absent
Grasp Normal Poor Absent
Suck Normal Poor Absent +/-bites
Respiration Normal Hyper Apnoea IPPV
Fontanelle Normal Full Tense
Comment on labour, delivery, resuscitation Total
Phenobarb
Magnesium
Clonazepam
Midazolam
Valium
Other


Health: KwaZulu-Natal Form Reference Number: Paed/34 Clinical Records: Paediatrics
Neonatal Jaundice Monitoring Chart: Phototherapy
Name: Folder No:
Date of birth: Time of birth:
Birthweight: Gestation:
Baby’s Blood Group: Baby’s Coomb’s: Mother’s Blood Group
U s e “ E x c h a n g e T r a n s f u s i o n ” c h a r t o ve r l e a f i f E X C H AN G E T R AN S F U S I O N i s a p o s s i b i l i t y
PHOTOTHERAPYWESTERN CAPE 2006 CONSENSUS GUIDELINES In presence of risk factors use one line lower (the gestation below) until <1000g.
If gestational age is accurate, rather use gestational age (weeks) instead of body weight
Start intensive phototherapy when the TSB is ≥ the line accordinStart intensive phototherapy when the TSB is ≥ the line according to gestation or weight.g to gestation or weight.
Infants under phototherapy : Check the TSB 12 – 24 hly but if TSB >30 μmol/L above the line , check TSB 4 – 6hly.STOP phototherapy :If TSB > 50 μmol/L below the line. Recheck TSB in 12 – 24hr.
340320300280260240220200180160140120100
806040200
Micr
o mo
l / L
TSB
(tota
l ser
um b
ilirub
in)
Time (age of baby in hours)6h 12h 24h 36h 48h 60h 72h 84h 96h 108h 120h
XXX XX X X
X
X38+ wks or 3000+g35 – 37w6d or 2500 – 2999g34 – 34w6d or 2000 – 2499g32 – 33w6d or 1500 – 1999g30 – 31w6d or 1250 – 1499g28 – 29w6d or 1000 – 1249g<28w or <1000gX
Infants > 12 hours old with TSB level below threshold, repeat TSB level as follows: 1- 20μmol/L below line:repeat TSB in 6hrs or start phototherapy and rept TSB in 12- 24hrs,21 - 50 μmol/L below line: repeat TSB in 12 – 24hrs, >50 μmol/L below line: rept TSB until it is falling and/or until jaundice is clinically resolving

Name:________________________ Folder No:___________________
Neonatal Jaundice Monitoring Chart: Exchange Transfusion
EXCHANGE TRANSFUSIONWESTERN CAPE 2006 CONSENSUS GUIDELINES
In presence of sepsis, haemolysis, acidosis, or asphyxia, use one line lower (gestation below) until <1000g
If gestational age is accurate, rather use gestational age (weeks) than body weight
Note: 1. Infants who present with TSB above threshold should have Exchange done if the TSB is not expected to be below the threshold after 6 hrs of intensive phototherapy.
2. Immediate Exchange is recommended if signs of bilirubin encephalopathy and usually also if TSB is >85 μmol/L above threshold at presentation
3. Exchange if TSB continues to rise >17 μmol/L/hour with intensive phototherapy
Time (age of baby in hours) 6h 12h 24h 36h 48h 60h 72h 84h 96h 108h 120h
450440430420410400390380370360350340330320310300290280270260250240230220210200190180
Micro
mol
/ L T
SB (t
otal s
erum
biliru
bin)
38+ wks or 3000+g35 – 37w6d or 2500 – 2999g34 – 34w6d or 2000 – 2499g32 – 33w6d or 1500 – 1999g30 – 31w6d or 1250 – 1499g28 – 29w6d or 1000 – 1249g<28w or <1000g
XX X XX X X
X
X X
X
R e c o r d a l l T S B ’ s , H b / P C V ’ s , p h o t o t h e r a p y , b a b y ’ s g r o u p a n d C o o m b ’ s , a n d m o t h e r ’ s g r o u p i n t h e d e s i g n a t e d p l a c e s o n t h e “ N e w b o r n C a r e R e c o r d ” ( F o r m P a e d / 0 1 )
2

Health: KwaZulu-Natal Form Reference number: Paed/06 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Basic Neonatal Care Nursing Observations: ______ hourly
Date Time Incubator Tº Baby Tº Glucose * Oxygen:
y/n** Pulse Rate Sats (%) Blood
Pressure Active and responsive:
y/n
Buttocks clean and dry: y/n
Mouth Care Cord care Eye care Skin care
Old strapping removed:
y/n
Drip site OK: y/n
Sign
* If baby’s glucose is less than 2.5mmol/l, use hypoglycaemia monitoring sheet
** If baby is on oxygen, use oxygen monitoring sheet
PAGE ___

Health: KwaZulu-Natal Form Reference number: Paed/06 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Basic Neonatal Care Nursing Observations: ______ hourly
Date Time Incubator Tº Baby Tº Glucose * Oxygen:
y/n** Pulse Rate Sats (%) Blood
Pressure Active and responsive:
y/n
Buttocks clean and dry: y/n
Mouth Care Cord care Eye care Skin care
Old strapping removed:
y/n
Drip site OK: y/n
Sign
* If baby’s glucose is less than 2.5mmol/l, use hypoglycaemia monitoring sheet
** If baby is on oxygen, use oxygen monitoring sheet
PAGE ___

Health: KwaZulu-Natal Form Reference Number: Paed/26 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
KMC Daily Score Sheet Date
Date of birth: KMC start date: Day
Feeding choice: Breast / Formula PMTCT: yes / no Weight
Score 0 1 2 Intermittent (I)or Continuous (C) I/C
Breast fed Score here for exclusive breast feeding
Mom's milk production None Not enough Enough Must score 2 before discharge
Positioning at breast Needs help Some help needed No help needed
Baby's ability to suckle at breast Tube fed Breast AND cup or tube Mainly breast
Formula fed Score here for formula feeding Knowledge of formula preparation & cleaning No knowledge Some knowledge Good knowledge Must score 2 before
discharge
Positioning for feed Depends on nurse Needs some help No help needed Must score 2 before discharge
Baby's ability to cup/ bottle feed Tube fed Cup and tube Takes all feeds well by cup /
bottle
Score here all babies
Socio-economic support No family help or support Occasional help / support Good support system Name support person:
Confidence in handling baby (changing/bathing) Always needs assistance Occasionally needs
assistance No help needed
Baby's weight gain / day 0 - 10 g/day 10 - 20 g/day 20 - 30 g/day Must score 1 or 2 for a few days
Confidence in giving of vitamin and iron drops No confidence Some confidence Fully confident
Mother's knowledge of KMC Little knowledge Some knowledge Knowledgeable
Acceptance & application of KMC Does not accept / apply Partially accepts or applies Fully accepts or applies Applies KMC on own
initiative
Confidence in caring for baby at home Does not feel sure / able Feels slightly sure / able Feels confident
Ready for discharge when the score is 19 or more Tota l
Adapted from Groote Schuur Hospital and Kalafong KMC Unit
PAGE ___

Health: KwaZulu-Natal Form Reference Number: Paed/26 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
KMC Daily Score Sheet Date
Date of birth: KMC start date: Day
Feeding choice: Breast / Formula PMTCT: yes / no Weight
Score 0 1 2 Intermittent (I)or Continuous (C) I/C
Breast fed Score here for exclusive breast feeding
Mom's milk production None Not enough Enough Must score 2 before discharge
Positioning at breast Needs help Some help needed No help needed
Baby's ability to suckle at breast Tube fed Breast AND cup or tube Mainly breast
Formula fed Score here for formula feeding Knowledge of formula preparation & cleaning No knowledge Some knowledge Good knowledge Must score 2 before
discharge
Positioning for feed Depends on nurse Needs some help No help needed Must score 2 before discharge
Baby's ability to cup/ bottle feed Tube fed Cup and tube Takes all feeds well by cup /
bottle
Score here all babies
Socio-economic support No family help or support Occasional help / support Good support system Name support person:
Confidence in handling baby (changing/bathing) Always needs assistance Occasionally needs
assistance No help needed
Baby's weight gain / day 0 - 10 g/day 10 - 20 g/day 20 - 30 g/day Must score 1 or 2 for a few days
Confidence in giving of vitamin and iron drops No confidence Some confidence Fully confident
Mother's knowledge of KMC Little knowledge Some knowledge Knowledgeable
Acceptance & application of KMC Does not accept / apply Partially accepts or applies Fully accepts or applies Applies KMC on own
initiative
Confidence in caring for baby at home Does not feel sure / able Feels slightly sure / able Feels confident
Ready for discharge when the score is 19 or more Tota l
Adapted from Groote Schuur Hospital and Kalafong KMC Unit

Health: KwaZulu-Natal Form reference number: Paed/31 Clinical Records: Paediatrics
Date: Monitoring & handover sheet for neonatal transfers
(to be completed by referring and receiving doctors starting at time of referral) Time: MOTHER Baby’s Name: Baby’s Number: Birthweight (g)
Name:
Gender: ♂ / ♀ Address: Length (cm)
Folder Number:
Age: Grav: Para: Date of Birth (use sticker when available)
COH (cm)
Pregnancy Received ANC: ⓎⓃTime of birth NVD Breech Assisted C/S LMP (mm/yy) / EDD /
Date VDRL/WR: ⊕ ⊖
Titre:1/ Rx X 3: ⓎⓃPCV/Hb
Blood Group: Antibodies: ⓎⓃTSB
Hypertension/PIH: ⓎⓃ Diabetes: ⓎⓃPhototherapy TB: ⓎⓃ Cardiac: ⓎⓃ
Epilepsy: ⓎⓃ APH: ⓎⓃ
Alcohol: ⓎⓃ Smoker: ⓎⓃ
Labour Induced: ⓎⓃ ROM: hrs
Con
tact
No
Con
tact
No
1st Stage: hrs 2nd Stage: mins
Pyrexia: ⓎⓃ AB’s: ⓎⓃ
Analgesia: ⓎⓃ Foetal distress: ⓎⓃ
BABY
Apgar:1min 5 min 10 minDes
igna
tion
Des
igna
tion
Resuscitation
MSL: ⓎⓃ SuctionedⓎⓃ
Action: None: ⓎⓃ Oxygen: ⓎⓃ
Mask ventilation: ⓎⓃ ETT+IPPV: ⓎⓃDoc
tor
Doc
tor
Drugs:
‘Distress’ Indicators: TSR: (mins)
Plan
:
Plan
:
Plan
:
Plan
:
Plan
:
Plan
:
Plan
:
Cord pH: Cord BE:
Cord Blood
NO
NO
NO
NO
NO
NO
NO
Group: Coombs: ⊕ ⊖ WR: ⊕ ⊖Hos
pita
l
Hos
pita
l
Gestational Age Estimate: weeks
YE
S
YE
S
YE
S
YE
S
YE
S
YE
S
YE
S
US: weeks Scored: weeks
AGA UGA OGA
MTCT: Mother ⊕ /⊖ /? Breast / Formula Ref
errin
g:
Rec
eivi
ng:
Acc
epte
d
Acc
epte
d
Acc
epte
d
Acc
epte
d
Acc
epte
d
Acc
epte
d
Acc
epte
d
Mother NVP: Ⓨ/Ⓝ/?/na Baby NVP: Ⓨ/Ⓝ/?/na
Antibiotic 1 Problem List
Antibiotic 2 #1:
% Oxygen Plan:
IPPV / CPAP
#2:
Plan:
Feed
s
IV (ml/hr) #3:
ml/kg/day Plan:
Age (day)
Once accepted for transfer, and transport arranged, continue overleaf

Health: KwaZulu-Natal Form reference number: Paed/31 Clinical Records: Paediatrics
1) Ongoing monitoring and responsibility while awaiting EMRS Name Rank Contact number
Doctor
Nurse
Time Temp Heart rate
Resp rate Sats Fi O2
O2 device
IV site secure
IV control device
IV rate AVPU BP Glucose Sign
On transfer
to ambulance
2) Problems arising while awaiting EMRS, and their plans Problem Plan Discussed with Verified by
3) Patient Transport information
Time accepted Receiving Hospital Doctor Rank Telephone Plan Sign
Time EMRS called EMRS Ops Centre Operator Designation Telephone Plan Sign
Time of EMRS arrival Ambulance type Paramedic Designation Telephone Plan Sign
Time at departure, AND receiving
hospital notified
Receiving Hospital Doctor Rank Telephone Plan Sign
Time of arrival at receiving hospital Receiving Ward Doctor Rank Telephone Plan Sign
4) Patient Handover
Handed over by Received by
Time Handover Point Name Designation Name Designation Sign
Referring hospital to EMRS
EMRS to receiving hospital
5) Caregiver Plan
Name Relationship Contact number Breastfeeding Well/sick Plan for transport to receiving
hospital y/n
6) Outcome
Alive & not transferred
Died & not transferred
Died awaiting EMRS Died in transit Died within 24
hours of transfer Died beyond 24
hours of transfer
Alive and transferred back
to referring hospital
NB: this does not replace the usual referral letter containing ALL relevant clinical details: Use the ‘Neonatal Discharge/Referral Letter ’ proforma, and copy the ‘Newborn Care Record’

Health: KwaZulu-Natal Form reference number: Paed/39 Clinical Records: Paediatrics
Page 1
Neonatal Discharge/Referral Letter MOTHER Baby’s Name: Baby’s Number: Gender:
♂ / ♀ Birth weight (g)
Name: Place of birth: Address: Length (cm)
Folder Number:
Age: Grav: Para: Date of birth: (use sticker when available)
COH (cm)
Pregnancy Received ANC: ⓎⓃTime of birth NVD Breech Assisted C/S LMP (mm/yy) / EDD /
History, examination and management VDRL/WR: ⊕ ⊖
Titre:1/ Rx X 3: ⓎⓃ
Blood Group: Antibodies: ⓎⓃ
Hypertension/PIH: ⓎⓃ Diabetes: ⓎⓃ TB: ⓎⓃ Cardiac: ⓎⓃ Epilepsy: ⓎⓃ APH: ⓎⓃ Alcohol: ⓎⓃ Smoker: ⓎⓃ Labour Induced: �� ROM: hrs 1st Stage: hrs 2nd Stage: mins
Pyrexia: ⓎⓃ AB’s: ⓎⓃ Analgesia: ⓎⓃ Foetal distress: ⓎⓃ BABY
Apgar:1min 5 min 10 min
Resuscitation MSL: ⓎⓃ SuctionedⓎⓃ Action: None: ⓎⓃ Oxygen: ⓎⓃ
Mask ventilation: ⓎⓃ
ETT+IPPV: ⃞ ETT+IPPV: ⓎⓃ
Drugs:
‘Distress’ Indicators: TSR: (mins)
Cord pH: Cord BE:
Cord Blood
Group: Coombs: ⊕ ⊖ WR: ⊕ ⊖ Gestational Age Estimate: weeks
US: weeks Scored: weeks
AGA UGA OGA
MTCT: Mother ⊕ /⊖ /? Breast / Formula
Mother NVP: Ⓨ/Ⓝ/?/na Baby NVP: Ⓨ/Ⓝ/?/na
Problem List ICD 10

Feeding (type and amount) at discharge
Immunisations
Relevant investigation results
Investigation Date Result FBC U&E
Cultures TORCH screen
HIV Ultrasound head
Other
Prescription at discharge/referral (drug AND dose) 1 52 6 3 7 4 8 Futures plans and follow up arrangements
Problem Follow up date Follow up venue
PMTCT follow up (if applicable) PMTCT site: PMTCT date: Baby assessed for ARV’s: N/A Yes No Referred to ARV Clinic Mother assessed for ARV’s N/A Yes No Referred to ARV Clinic Remarks
The Road to Health Chart was updated and given to caregiver Yes No Not present Birth Registration was done Yes No Yours sincerely Sign:___________________________ Print/Stamp:________________________ Date: ____________ Contact number: _______________________________
Page 2

Health: KwaZulu-Natal Form Reference Number: Paed/37 Clinical Records: Paediatrics
N E O N A T A L R E C O R D A U D I T DATE: ___________________________ HOSPITAL: ___________________________ DATE OF PATIENT’S ADMISSION: ___________________________ PATIENT’S DIAGNOSIS: ___________________________
Check each document for the following A. Patient’s details N/C P/C C COMMENTS Name and initials Hospital number
Ward
B. Name of consultant on patient’s notes
C. Documentation
1) Standardised Neonatal Record Keeping system used
2) Time of admission
3) Time of examination
4) Maternal ANC history
5) Maternal intrapartum history
6) Neonatal resuscitation details
7) PMTCT details (test, nevirapine, feeding choice)
8) Neonatal assessment details
9) Gestational age and anthropometry assessed and plotted
10) Medical examination with details of medical findings leading to diagnosis
11) Clear problem list
12) Clear plan for each problem
13) Request for special investigations
14) Results of special investigations in results sheet
15) Signature on all results of special investigations
16) Medication prescribed in notes & on prescription sheets
17) Feeds calculated and prescribed
18) Daily notes written using the problem oriented approach
19) Weight plotted correctly daily
20) Notes legible & in chronological order
21) Legible signature with pager no., date and time on every entry
22) Record of consultation with other paramedical services

Last modified: 15 June 2007 For review: 2009 2
N/C P/C C COMMENTS D. INFORMATION FOR PARENTS / CARE GIVER
1) Fully informed of findings & same documented
2) Parents participate in decision making relating to treatment and same documented
3) Informed consent for interventional procedures
E. DISCHARGE OF PATIENTS
1) Follow up plan recorded
2) Discharge medicines clearly prescribed (including dose)
3) Discharge summary/referral letter present in case sheet
4) RTHC filled in correctly and completely
GENERAL OVERVIEW / COMMENTS
1) Do patient’s records reflect high quality medical care?
2) Do records present a total picture of this patient?
3) Were other team members involved in the patients care and was this documented? e.g. Social Worker
4) Were hospital policies followed?
5) Was adequate Health Education given to parents during hospitalisation / on discharge
Auditors name: ___________________________ Signature: _______________________ Outcome of audit Reported by : ____________________________________ Reported to : ____________________________________ Date : ____________________________________ Rating: Non-compliant (n/c) = 0 Partially compliant (p/c) = 1 Compliant (c) = 2

Health: KwaZulu-Natal Form Reference Number: Paed/16 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Investigations Chemistry & Haematology
Date
Time
Renal Function Sodium
Potassium
Chloride
Bicarbonate
Urea
Creatinine
Liver Function Total Protein
Albumin
Total Bili/Conj Bili
ALP
GGT
ALT
LDH
INR
“CMP” Ca/Corrected
Magnesium
Phosphate
Haematology WCC
N%
L%
Hb
MCV
Platelets
Retics
PTT
Acid/Base & Blood Gasses Date
Time
FiO2
pH
pCO2
pO2
Base Excess
SBC
PAGE ___

Health: KwaZulu-Natal Form Reference Number: Paed/16 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Cultures
Date Test Result
Serology
Date Test Result
Radiology
Date Image
Other
Date Test Result
Test Date Age (Child) Result Child Exposed / Infected /
Not infected Caregiver informed
Mother Rapid
Mother Elisa
Child Rapid
Child ELISA
First PCR
First CD4
PAGE ___

Health: KwaZulu-Natal Form reference number: Paed/17 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Acid Base and Blood Gasses
Date Time Site FiO2 Sats Mode Vent Rate
Baby Rate IP/EP MAP TV IT pH pCO2 pO2 BE SBC Treatment Sign
PAGE ___

Health: KwaZulu-Natal Form reference number: Paed/17 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Acid Base and Blood Gasses
Date Time Site FiO2 Sats Mode Vent Rate
Baby Rate IP/EP MAP TV IT pH pCO2 pO2 BE SBC Treatment Sign
PAGE ___

Health: KwaZulu-Natal Form Reference Number: Paed/18 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Oxygen Delivery and Saturation Monitoring Chart
Date Time
Face mask/ head
box FiO2 (%)
Face mask / head
box flow (l/min)
Nasal cath O2
flow (l/min)
Resp rate
(bpm)
Pulse rate
(bpm)
O2 saturation
(%)
Nebs
____ hrly Steps taken to get sats
normal Sign

Health: KwaZulu-Natal Form Reference Number: Paed/18 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
Oxygen Delivery and Saturation Monitoring Chart
Date Time
Face mask/ head
box FiO2 (%)
Face mask / head
box flow (l/min)
Nasal cath O2
flow (l/min)
Resp rate
(bpm)
Pulse rate
(bpm)
O2 saturation
(%)
Nebs
____ hrly Steps taken to get sats
normal Sign

Health: KwaZulu-Natal Form Reference number: Paed/19 Clinical Records: Paediatrics
Name: ____________________
Folder Number: ______________
Page ___
Hypoglycaemia Management Chart
Date Time Glucometer (mmol/l)
Action taken to get blood glucose normal
Next G’meter (time)
PRINT name

Health: KwaZulu-Natal Form Reference number: Paed/19 Clinical Records: Paediatrics
Name: ____________________
Folder Number: ______________
Page ___
Hypoglycaemia Management Chart
Date Time Glucometer (mmol/l)
Action taken to get blood glucose normal
Next G’meter (time)
PRINT name

Health: KwaZulu-Natal Form Reference Number: Paed/20 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
Hourly Ventilator and CPAP Nursing Observations
Date Time FiO2 Sats (%) Pulse rate
Probe changed Humidifier full Water trap
empty ETT Secure Suction ___ hourly Saline lavage Secretions:
Amount Secretions: Appearance Sign

Health: KwaZulu-Natal Form Reference Number: Paed/20 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
Hourly Ventilator and CPAP Nursing Observations
Date Time FiO2 Sats (%) Pulse rate
Probe changed Humidifier full Water trap
empty ETT secure Suction ___ hourly Saline lavage Secretions:
Amount Secretions: Appearance Sign

Health: KwaZulu-Natal Form Reference Number: Paed/21 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
Intake Output Chart for Patients on Intravenous Fluids & Orals Age: _____ Weight: _____kg Date: ________________ Intravenous Intake Oral Intake Total in
Time Doctor’s Order Sign Time Doctor’s Order Sign Total out
Insensible loss
Balance
Output
Time Set Up
Type of fluid Amount Rate Time
Completed Subtotal/ carried Total Sign Time Type of
feed Amount How Given Sign Stool Vomit /
Aspirate Urine Other:
_______ Sign
08:00 09:00 10:00 11:00 12:00 13:00 14:00 15:00 16:00 17:00 18:00 19:00 20:00 21:00 22:00 23:00 24:00 01:00 02:00 03:00 04:00 05:00 06:00 07:00
To carry Total IV Total
oral Totals out

Health: KwaZulu-Natal Form Reference Number: Paed/21 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
Intake Output Chart for Patients on Intravenous Fluids & Orals Age: _____ Weight: _____kg Date:________________ Intravenous Intake Oral Intake Total in
Time Doctor’s Order Sign Time Doctor’s Order Sign Total out
Insensible loss
Balance
Output
Time Set Up
Type of fluid Amount Rate Time
Completed Subtotal/ carried Total Sign Time Type of
feed Amount How Given Sign Stool Vomit /
Aspirate Urine Other:
_______ Sign
08:00 09:00 10:00 11:00 12:00 13:00 14:00 15:00 16:00 17:00 18:00 19:00 20:00 21:00 22:00 23:00 24:00 01:00 02:00 03:00 04:00 05:00 06:00 07:00
To carry Total IV Total
oral Totals out

Health: KwaZulu-Natal Form Reference Number: Paed/22 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
Intake Output Chart for Patients on Orals Only Age: _____ Weight: _____kg Date:____________
Oral Intake Total in
Date Time Doctor’s Order Sign Total out
Insensible loss
Balance
Output
Time Type of feed Amount How Given Sign Stool Vomit Urine
Other: _______ Sign
If patient is on IV fluids, do not use this chart.

Health: KwaZulu-Natal Form Reference Number: Paed/22 Clinical Records: Paediatrics
Name:________________________ Folder No:___________________
PAGE ___
Intake Output Chart for Patients on Orals Only Age: _____ Weight: _____kg Date:______________
Oral Intake Total in
Date Time Doctor’s Order Sign Total out
Insensible loss
Balance
Output
Time Type of feed Amount How Given Sign Stool Vomit Urine
Other: _______ Sign
If patient is on IV fluids, do not use this chart.

Health: KwaZulu-Natal Form Reference Number: Paed/33 Clinical Records: Paediatrics
Letter in support of grant application
Institution: _____________________ Ward: ____________________ Date: ________________
To: The Welfare Officer Department of Welfare Dear Madam/Sir Re: Assistance with grant application Caregiver name: _____________________________ ID Number: ____________________________________
Child’s name: _____________________________ ID Number: ____________________________________
Kindly assist the bearer(s) with their social grant application(s). For processing the application, I have also asked the caregiver to be in possession of the indicated documentation:
Grant Eligibility criteria (circle applicable) Documents required
Old age pension ♂ > 65 years / ♀ > 60 years 1) Proof of income and assets of applicant and his/her
spouse
Child support grant
Household income: Urban < R800 pm; Rural/Informal < R1100 pm
1) Proof of income of primary care giver and his/her spouse
2) Proof that the applicant is the primary care giver of the child
Foster care grant De facto caregiver is not a parent; child must be placed in Foster Care by the Children’s Court
1) Proof of income of the foster child 2) Proof of regular school attendance 3) An order of the Children’s Court
Care dependency grant Child is severely handicapped
1) Proof of income of the applicant and his/her spouse as well as the child
2) Medical report in respect of the child
Social relief of distress Needs immediate help in order to survive
1) ID documents or birth certificates of all children 2) Proof of income and assets 3) Proof of efforts to get maintenance (letter from
Maintenance Court) 4) Proof that family has no money
In addition, I have advised that the following documents are required for ALL types of grant applications:
Document 13 digit barcode ID document of caregiver
Child’s birth certificate
Proof of caregiver’s marital status
On presentation of this letter to you, kindly supply the bearer with a receipt acknowledging the application, indicating the date of the application as well as your name, telephone number, and office.
Batho pele thanks
Sign: ___________________ Print Name: __________________ Stamp: ____________________
Contact number: ___________________








