
What’stheenvironmentgottodowithit?
MichaelParry,MD,FACP,FIDSA,FSHEAThomasJayBradsell ChairofInfectiousDiseases,StamfordHospital
ProfessorofClinicalMedicine,ColumbiaUniversityCollegeofPhysiciansandSurgeons

GoldenRulesofInfectionPrevention
hand hygiene
environmentalhygiene
engineered processes of care

HandHygiene
Bundleimplementation(SSIprevention)• Pharmacologic
– Mechanicalbowelprep– Oralantibioticsthedaypriortosurgery(Correctdrugs,doses)– Prophylacticintravenousantibiotics(Appropriateselection,timing,re-
dosing,postoplimitation)• NonPharmacologic
– Preoperativeshowers– Appropriatehairclipping– Appropriateskinprep– Maintainbodytemperature– Postoperativeoxygenation– Laparoscopicwhenpossible
• Technical– Reduceintraoperativecontamination-- minimizespillage– Maintain“clean”areasseparatefromcontaminated– Changegloves,gowns,suction,bovie tip– Protectsuperficialwound– Recognizehighrisksituations-- Delayedprimaryclosure
• Systematic– Time-out– Checklist– Debriefingform– Quarterlydatareview


6
Contaminatedsurfaces
• 70%ofsurfacesincolonizedpatients’roomsarecontaminatedwithMRSAorVREorC.difficile.– Countertops– Bedrails– Equipment– Telephone,callbutton
• MorethanhalfthepatientswhobecamecolonizedwithMRSAafterenteringtheICUacquireastrainNOT presentonotherpatientsthereatthetime.
• Oncecaregiverstouchthesesurfaces,theirhandsorglovesarecontaminated.
Infection Control and Hospital Epidemiology (v. 9, 1997) 622-627.Infection Control and Hospital Epidemiology (v.20.2, 2006).
7
SurvivalofMulti-drug-resistantOrganismsintheEnvironment
• DurationofsurvivalofMRSAindryconditions– Plasticcharts=11days– Laminatedtabletop=12days– Clothcurtains=9days
• EnvironmentalsurvivalofVRE– Upholstery,furnitureandwallcoverings=7days
• SurvivalofClostridiumdifficile– Months
Huang et al, Infect Control Hosp Epidemiol 2006;27:1267-1269Lankford et al, Am J Infect Control2006;34:258-263

8
Contamination of Computer Keyboards
Beforecleaning
Aftercleaning
Keyboards,Telephones,Equipment–allharborStaph,Strep,andotherPathogens

9
Manypersonneldon’trealizewhentheyhavemicroorganismsontheirhands
Nurses,doctorsandotherhealthcareworkerscangetthousandsofbacteriaontheirhandsbydoingsimpletasks,like
• pullingpatientsupinbed• takingabloodpressureorpulse• touchingapatient’shand• rollingpatientsoverinbed• touchingthepatient’sgownorbedsheets• touchingequipmentlikebedsiderails,over-bedtables,IVpumps
Cultureplateshowinggrowthofbacteria24hoursafterhandplacedontheagarplate

10
RoleofasymptomaticcarriageofCdifficile inpatientsataLTCFRiggs,etal.ClevelandClinic,2007.
• 68asymptomaticpatientsinLTCF• 51%carriersofC.difficile
– 49%ofthesehadNAP-1strain
• Carriershadhighskin(61%)carriage– versus70%inCDIcases
• Carriershadhighenvironmental(59%)contamination– Versus70%inCDIcasesand20%innon-carriers
• PriorCDIandrecent(<3mo)antibioticusewasassociatedwithcarriage
• 20%ofcarriersdevelopedCDIover4mofollow-up

11
Wherearethegerms?

12
Wherearethegerms?

13

14
TheChallenge:tocreateaneffectiveenvironmentalhygieneprogram
• CleaningPolicies&Procedures– Everyone’sjob!– Dailycleaningandterminalcleaning– Hightouchsurfacesfocus– Equipmentcleaning– “Rollingstock”management– Unitcorecleaning
• Staffneededucationonanongoingbasis.• Checklistforroomcleaning• Roomturn-overtimeforanisolationpatienttakes
approximately45-60minutes.• Staffshouldberoutinelyevaluatedonperformance
– DirectandClandestineobservation

15
ElementsoftheInterdisciplinaryCleaningandDisinfectionInitiative
• ProgramimplementedOctober,2005• Useofafluorescentmarkertodetect
surfacecleaning• Collaborativeevaluationofcleaningprocess• Nursingserviceperformedcleaning
assessments• Ongoingevaluationofeffectiveness
– Groupfeedbacktohousekeepingdepartmentatlarge
– Personalfeedbackonindividualperformancetomanager
• Incorporationintoperformancemanagementprocess

16
EnvironmentalSitesTesting
• Toiletseat• Toilethandle• Toilethandhold• Sink• Sinkfaucethandle• BRdoorknob• BRlightswitch• Telephone• TVcontrol/callswitch• Siderails• Traytable• Bedsidetable• Chairhandrail• Roomdoorknobs


18
EnvironmentalCleaningSHOverallProgress

Percentofsurfacescleaned
19
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
perc
ent c
lean
ed
Percent of surfaces cleaned 10/12 to 6/15
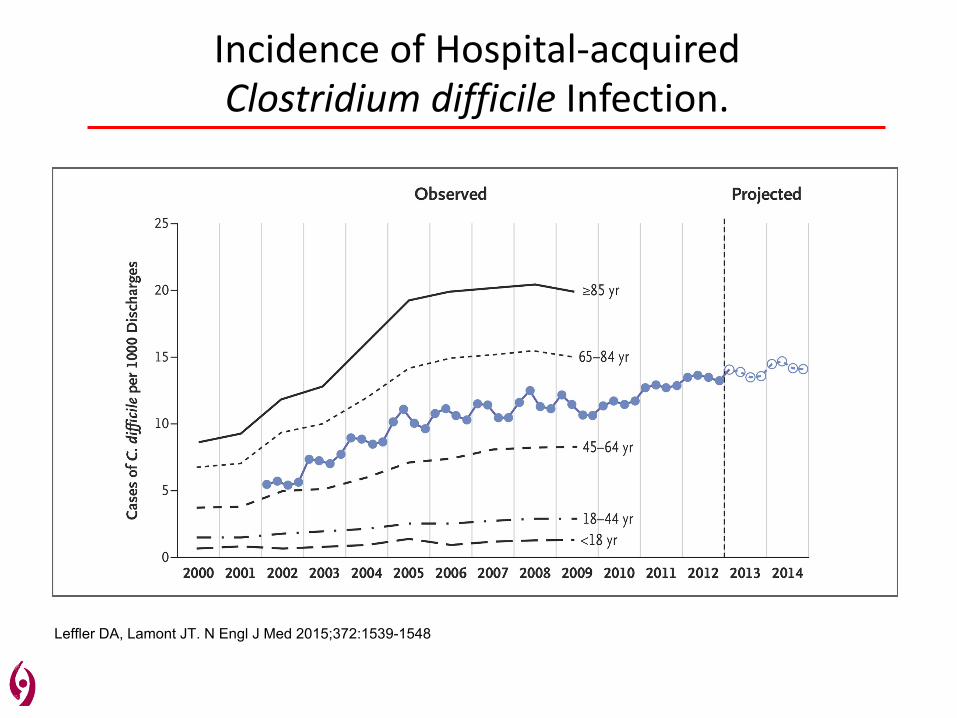
IncidenceofHospital-acquiredClostridiumdifficile Infection.
Leffler DA, Lamont JT. N Engl J Med 2015;372:1539-1548
DifficultiesincontrollingthespreadofC.difficile
• Highcommunityprevalence– especiallyLTAC(30-50%);SNF(10-20%);community(3-6%)
• Difficultypreventinginfectioninhighrisksettings– “incidentdensity”pressure– carriers+ill
• Hospital“onset”versushospital“acquisition”• Antibioticuseandthemicrobiome
– necessaryandunnecessary– breadthandlengthandtypeofrx
• Prevalenceofacidsuppressiontherapy– VAPprevention;otherordersets
• Prolongedfecalandskincarriage– Clinicallysuccessfultreatmentdoesn’teradicatethespore
• Frequentrecurrence– Treatment,ageandimmunocompetence dependent
• Persistenceofsporesintheenvironment– Resistancetogermicides– Patientingestion
21

22
PersistenceofC.difficileDuringandAfterTreatment
0
10
20
30
40
50
60
70
80
90
100
Prior to treatment Day 3 of treatment Resolution of diarrhea
End of treatment 1-6 weeks after treatment
Perc
ent P
ositi
ve
Percentage of positive cultures for C. difficile before, during, and after treatment
Stool Skin Environment
Wafa Al Nassir, et al. Cleveland VA. ICHE, 2010




26
StamfordHospital-acquiredC.difficile

27

C.difficile bundle• Environmentalcleaningprogram• Bleach/peracetic acidprogram• Dailyandterminalcleaning• IsolationforCdiff
– GownandGlove– Soapandwater– Durationofhospitalization
• Rapiddetection– PCR– Isolatefordiarrhea– Readmissionflag
• Dedicatedequipment– Yellowstethoscopes;disposableBPcuffs,thermometers,etc– Norectaltemperatures
• Treatmentinitiatives– vancomycinandfidaxomycin• PPIreductioninitiative• Antibioticstewardshipprogram• Fecaltransplantationprogram• NewHospitalinitiatives

TheNewStamfordHospital




Whathelpisonthehorizon?
• Antimicrobialsurfaceengineering– Copper,silver– Nanotechnology– Fabrics(curtains,scrubs,linens)
• UVlightandotherlighttechnologies• Aerosols• Focusonthemicrobiome
– Fecaltransplantation– Syntheticstool– Alternativetreatmentmodalities
• Focusontheimmunesystem– Monoclonalantibodies– Immunization

MicrobialLoadonEnvironmentalSurfaces:TheRelationshipBetweenReducedEnvironmentalContaminationandReductionofHealthcare-AssociatedInfections(TheBETRDisinfectionStudy)
IDWEEKAbstract262,2016
WILLIAMRUTALA,etalUniversityofNorthCarolinaHealthCare,ChapelHill,NC
Background:Disinfectionofnoncriticalenvironmentalsurfacesandequipmentisanessentialcomponentofinfectionpreventionassurfacesmaycontributetocross-transmissionofepidemiologicallyimportantpathogens(EIPs).
Results: Enhanceddisinfectioninterventions(i.e.,Quat/UV,Bleach,Bleach/UV)weresignificantlysuperiortoaQuat aloneinreducingEIPs.
Conclusion:Comparisonofthebeststrategywiththeworststrategy(i.e.,Quat vsQuat/UVorBleach/UV)revealedthatareductionof>90%inEIPsledtoa35%decreaseinsubsequentpatientcolonization/infection.Ourdatademonstratedthatadecreaseinroomcontaminationwasassociatedwithadecreaseinsubsequentpatientcolonization/infection.

AntimicrobialActivityofaContinuousVisibleLightDisinfectionSystem
IDWEEKAbstract267,2016
WILLIAMRUTALAandDANIELSEXTON,etal.UniversityofNorthCarolina,ChapelHill,NCandDukeUniversityMedicalCenter,Durham,NC
Background:Anoverheadlightfixturetechnology,whichcontinuouslyandsafelydisinfectstheenvironmentwasassessedtodeterminetheeffectivenessforthereductionofEIP. Thistechnologycreatesanarrowbandwidthofhigh-intensityvisiblebluelightwithapeakoutputof405nmthatgeneratesreactiveoxygenspeciesandkillsmicroorganisms.
Results:Theseresultsdemonstratedthatthe405nmlightinactivatedthreevegetativebacteria(MRSA,VRE,MDRA)onsurfaceswithcontacttimesof1-96hr.Statisticaldifferences(p<0.05)wereobservedusingbluelightforVREat24hr,forMRSAat3-7hr,forMDRAat5-24hr,andforC.difficile sporesat5hrand72hr.Theinactivationwasmoresignificantwhenthesurfaceirradiancewasincreasedbyaddingthebluelight.
Conclusion: Highintensitylighttechnologycouldbeconsideredforseveralhealthcaredecontaminationapplications


ReducedHealthcareAssociatedInfectionsinanAcuteCareCommunityHospitalusingaCombinationofSelf-DisinfectingCopper-ImpregnatedCompositeHardSurfacesandLinens
IDWEEKAbstract263,2016
COSTISIFRI,MD,KYLEENFIELD,MDandGENEBURKEMD.UniversityofVirginiaHealthSystemandSentaraHealthcare,Norfolk,VA
Background:Effortstodecreaseenvironmentalbioburden areassociatedwithreducedtransmissionofmicrobialpathogensanddevelopmentofHAIs.Copperoxidehaspotentbiocidal activity.Herewereporttheresultstrialofacopperoxide-impregnatedcompositeproductincorporatedintohospitalcountertops,moldedsurfaces,patientgownsandlinens.
Results:Thestudywasconductedovera25.5-monthtimeperiod.HAIratesobtainedfromthecopper-containingnewtower(72beds;14,479patient-days)andtheunmodifiedhospitalwing(84beds;19,177patient-days)werecomparedtothosefromthebaselineperiod(204beds;46,391patient-days).Thenewtowerhad78%(P=.023)fewerhealthcare-associatedinfectionsduetoMDROsorC.difficile ,83%(P=.048)fewercasesofC.difficile infection,and68%(P=.252)fewerinfectionsduetoMDROsrelativetothebaselineperiod.Nochangesinratesofhealthcare-associatedinfectionswereobservedintheunmodifiedhospitalwing.
Conclusion:Copperoxide-impregnatedcompositehardsurfacesandlinensmaybeusefultechnologiestopreventhealthcare-associatedinfectionsintheacutecarehospitalsetting.

TheAntisepticScrubContaminationandTransmission(ASCOT)TrialtoDeterminetheImpactofAntiseptic-
ImpregnatedScrubsonHealthcareWorkerContaminationIDWEEKAbstract1351,2016
DEVERICKANDERSON,MDetal.DukeInfectionControlOutreachNetwork,DukeUniversityMedicalCenter,Durham,NC
Background:HCPclothingbecomescontaminatedduringpatientcareandcanserveasavectorforsubsequenttransmission. Antimicrobial-impregnatedclothingmayreducecontamination,butclinicaldataarelacking.
Methods:Scrubsimpregnatedwith(1)acomplexelementcompoundwithasilver-alloy,or(2)anorganosilane-basedquaternaryammoniumandahydrophobicfluoroacrylate copolymeremulsion,werecomparedtotostandardcotton-polyscrubsduringclinicalcare
Results:167uniquepatientsreceivedcarefrom40nursesubjectsover120individualshifts.2,185cultureswereobtainedfromHCPclothing,455frompatients,and2,919frompatients’environments. Themedianunadjustedincreasesincontaminationweresimilaramongscrubtypes.ScrubtypewasnotassociatedwithadecreaseinHCPclothingcontamination.
Conclusion:Antimicrobial-impregnatedscrubsdidnotleadtodecreasedcontaminationofnursesclothing.

AreAntimicrobialCurtainsasCleanasYouThink?IDWEEKAbstract260,2016
SHELASRIAR,MD,etal.MedicalCollegeofWisconsin,Milwaukee,WI,
Background:Weaimedtodeterminethedegreeofbacterialcontaminationonantimicrobialcurtainswithinourmedicalintensivecareunit(ICU).
Results:Wefoundthatoutof20curtains,95%(n=19)showedbacterialgrowth.Outofthe10doorcurtains50%(n=5)showedGram-negativebacilliand100%(n=10)hadGram-positiveorganisms.Outofthe10commodecurtains,10%(n=1)showedGram-negativeorganismsand90%(n=9)hadGram-positiveorganisms
Conclusion:Antimicrobialcurtainsarecontaminatedwithpathogenicorganisms;therefore,theyshouldbethoroughlydisinfected,exchanged,ortotallyforegoneinbetweenpatients.

Thankyou!
Questions?







