Kambis Mashayekhi
University Heart center Bad Krozingen
Euro CTO Club 2017: Saturday 7h15-8h30
When am I prepared enough for myfirst retrograde approach ?

Situation in Europe
ESC – Guidelines on Myocardial Revascularisation 2014:
2

Single Operator K.M. (2013-2017)
931 CTO
(95,8% success)
430 single wire (46%)
J-CTO 1,5
Fluoro: 29min
96 Parallel wire / ADR (10,3%)
J-CTO 2,3
Fluoro: 62min
398 retrograde wire (43%)
J-CTO 2,8
Fluoro: 81min
7 data missing
Why do I need retrograde approach?1

Euro-CTO Registry 2013-2016
(n=7523, 32,3%retrograde)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Successrate
Successrate 2013-2016
Antegrade
ADR with CB
Retrograde
92,4%
83,4%85,0%
0
0.5
1
1.5
2
2.5
3
J-CTO
J-CTO Score 2013-2016
Antegrade
ADR with CB
Retrograde
1,87
2,49
2,76
K. Mashayekhi, EuroCTO Registry, TCT 2016

0.60%
1.30%
0.27%0.01%
0.83%
6.20%
0.41%0%
1.50%
4.70%
1.00%
0.16%
Tamponade PE withoutTamponade
PeriinterventionalInfarction
Procedural Death
Complications 2013-2016
Antegrade ADR with CB Retrograde
Am I ready to take the potential risk for
retrograde procedures?
K. Mashayekhi, EuroCTO Registry, TCT 2016
2

4,3
2,1
0,4
1,3
0,6 0,8
1,1
0,3 0,3 0,3 0,1 0,1
0
MACE
MI
Stroke
Pericard
iocente
sis
Re-PCI
Death
Com
plic
atio
n ra
te (%
)
Retrograde
Antegrade-only
PROspective Global REgiStry for the Study
of CTO interventions
MACCE in retrograde vs. antegrade-only CTO
Karmpaliotis et al. Circ Cardiovasc Interv 2016 Jun
n=539 J-CTO 3,1
n=762 J-CTO 2,5

Periprocedural ischaemia during CTO PCI:
Influence of the retrograde approach
Werner et al. Eurointervention 2014 Nov

Periprocedural Myocardial Injury in Patients
Undergoing CTO-PCI : Role of Antegrade and
Retrograde Crossing Techniques
Toma et al, unpublished data 2017
antegrade; n=1447
19,4% PMIretrograde; n=462
44,2% PMI
PMI (elevation of cardiac troponin T [cTnT] >5 x 99th percentile of normal)
Do I have enough support in my hospital?
• Strong backing from the head of the department and the senior consultants
• Motivated and interested Cath-lab team, who believes, that the CTO - operator can handle complex PCI scenarios
• Support from a device company
• Do I need additional support from an experience retrograde CTO operator
3
Do I have enough resources for a retrograde
CTO program?
• Structural resources:– 2 Cath labs
– Institution with >500-750 PCI (50-75 CTO´s / year)
– Cardiac – MRI, Cardiac – CT-scan
• Personal resources:– Experienced internationalist
– CTO- days/week (extra time slots)
• Material and financial resources:– CTO wires, microcatheters, IVUS, rotablator, ACT-measurement
4
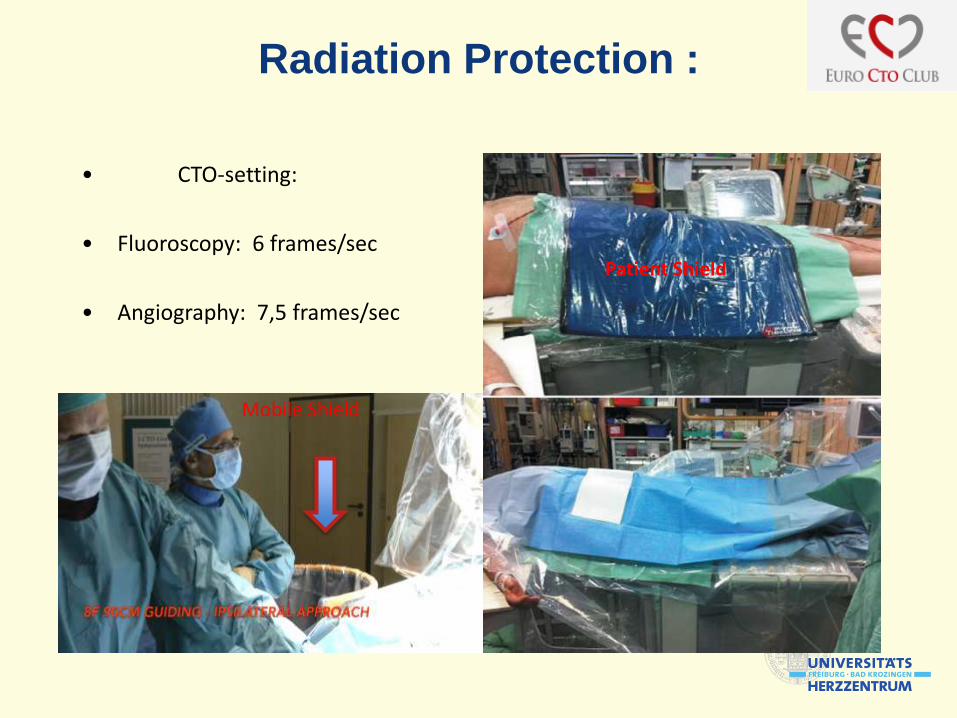
Radiation Protection :
• CTO-setting:
• Fluoroscopy: 6 frames/sec
• Angiography: 7,5 frames/sec
Distance to radiation sourceMobile Shield
Patient Shield
Personal Resources
Special requirements:
• Personality structure of the operator ambitious, persistent, mental force, interested in training activities, sharing experiences and open to communicate
• Enough experience in antegrade CTO PCI
• Knowledge about radiation protection
• Able to avoid, but also master complex emergency situations:
Emergency pericardiocentesis
Coiling, Embolization (fat, microspheres)
Experience in the technique of implanting a Cover-Stent (ping pong - guiding technique)
Am I really prepared for the first retrograde
procedures in my institution?
• Clear communication to the Cath lab team and colleges about what is going on today in the lab
• Do I need support from a device company or medical proctor?
Patients information
• „This procedure will take at least 2-3h !“
• 2 puncture sides
• Talk also about alternative options
• Radiation exposure
• Bladder catheter
5
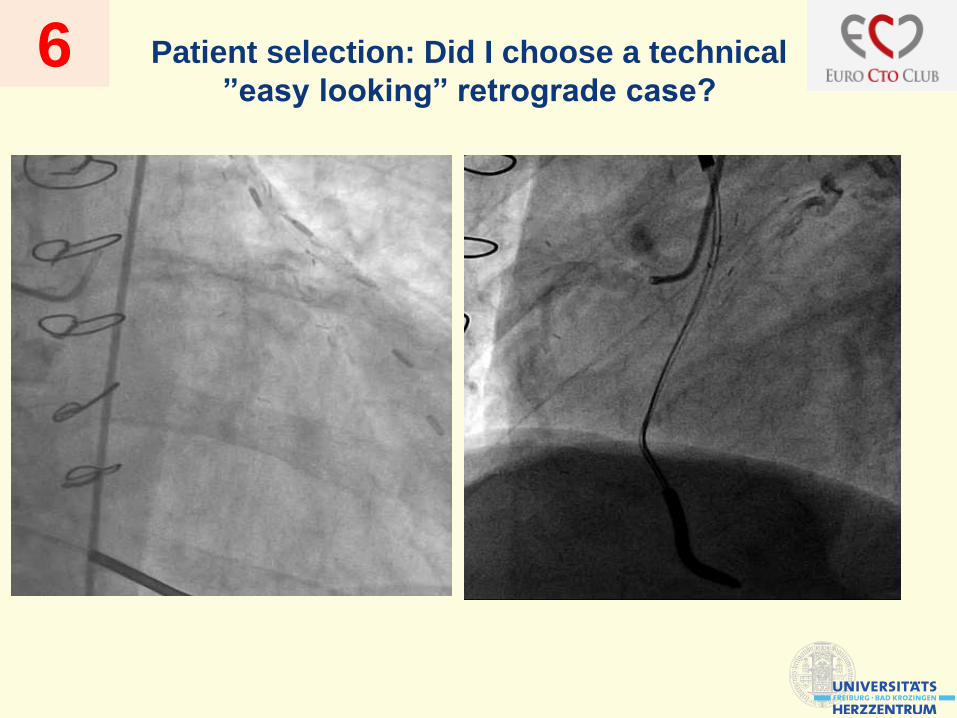
Patient selection: Did I choose a technical
”easy looking” retrograde case? 6

J-CTO 4 6 months follow up
Procedural time 302 min., fluoroscopic time 161 min, cumulative radiation dose 37096 uGym2 and amount of contrast was 200cc.
Is this the right patient to start with my first
retrograde CTO?

Do I know at which point in the
procedure I should change from
antegrade to retrograde?
7

x
x
x
x
x
2x
When to change to retrograde?

Subitimale Wire(Confianza Pro)
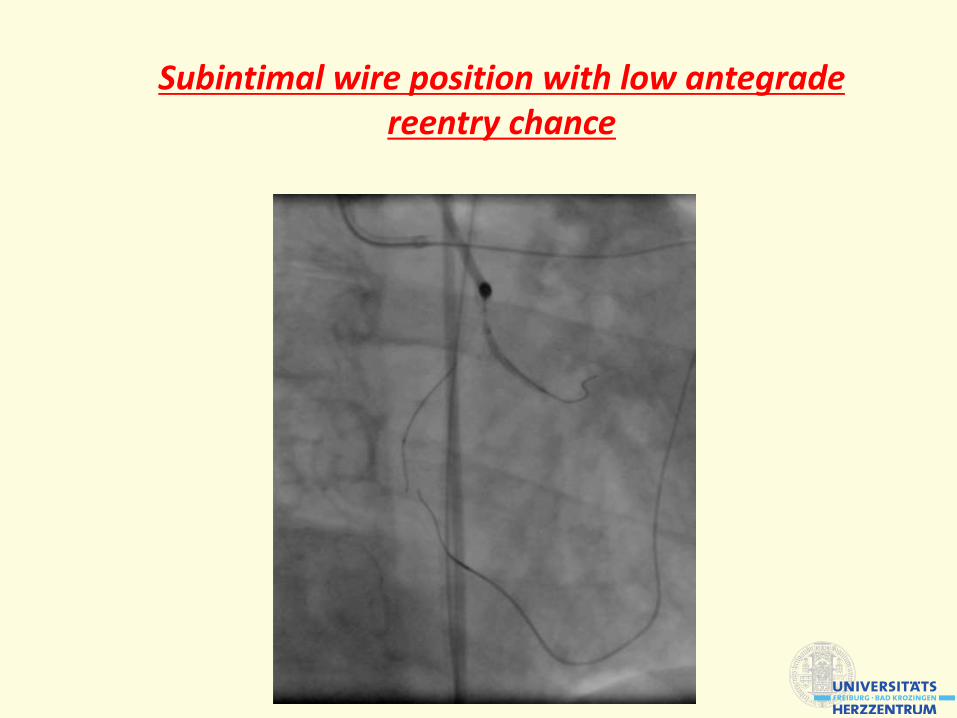
Subintimal wire position with low antegradereentry chance
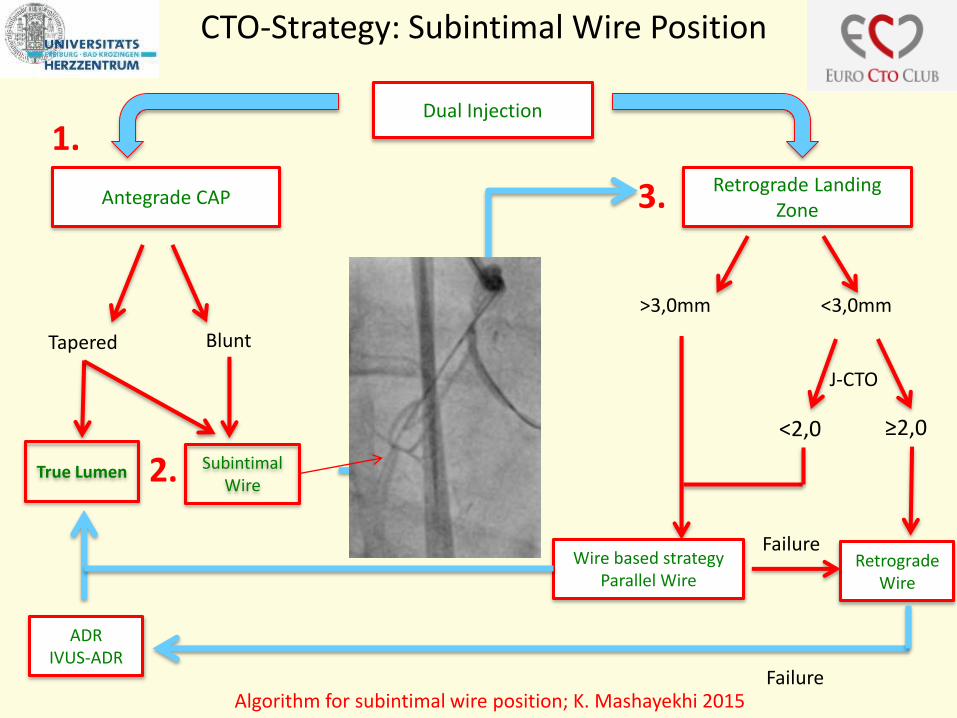
Dual Injection
Antegrade CAPRetrograde Landing
Zone
True Lumen SubintimalWire
Tapered Blunt
>3,0mm <3,0mm
J-CTO
<2,0 ≥2,0
Retrograde Wire
Wire based strategy Parallel Wire
ADRIVUS-ADR
Failure
Failure
1.
2.
3.
CTO-Strategy: Subintimal Wire Position
Algorithm for subintimal wire position; K. Mashayekhi 2015

Subintimale Wire
(Confianza Pro)
Subintimal wire position with low antegradereentry chance

Do I know how to use a septal dilatator?
Thanks to Nicolas Boudou for the invitation to the great JIF - CTO in Toulouse 2016
8
Subintimal wire position with low antegradereentry chance

Do I understand the principals of revers CART?
9
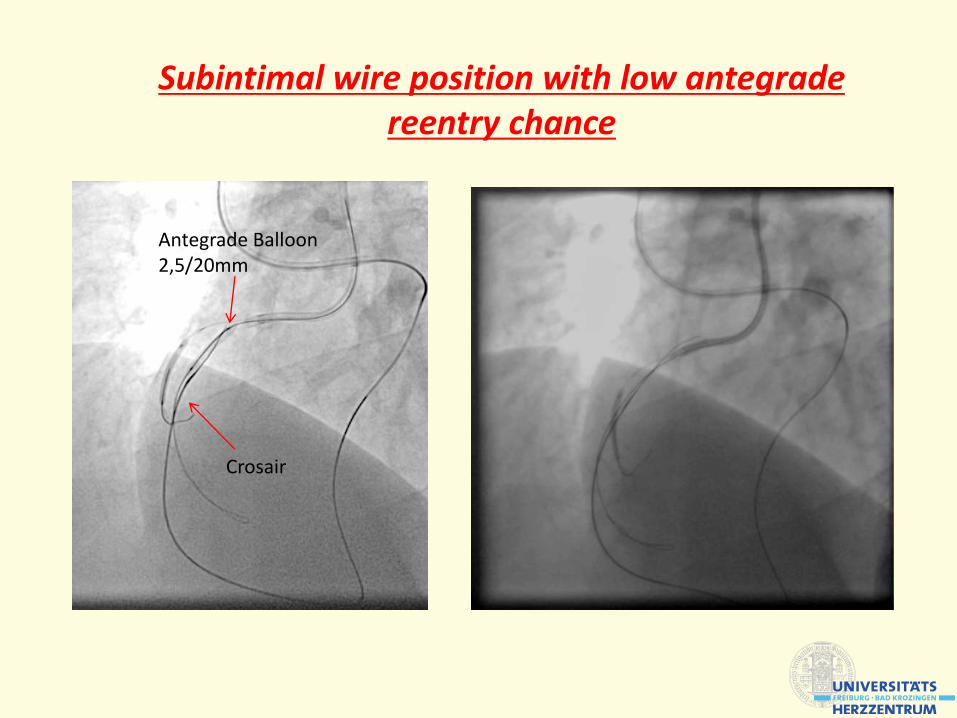
Antegrade Balloon2,5/20mm
Crosair
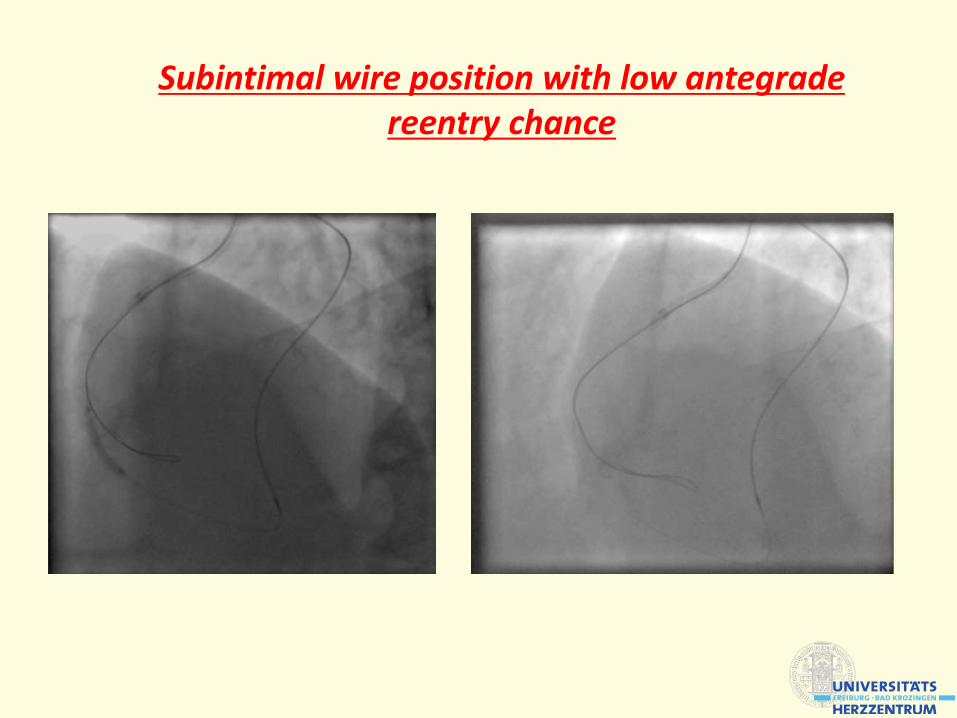
Subintimal wire position with low antegradereentry chance

Trapped retrograde wire
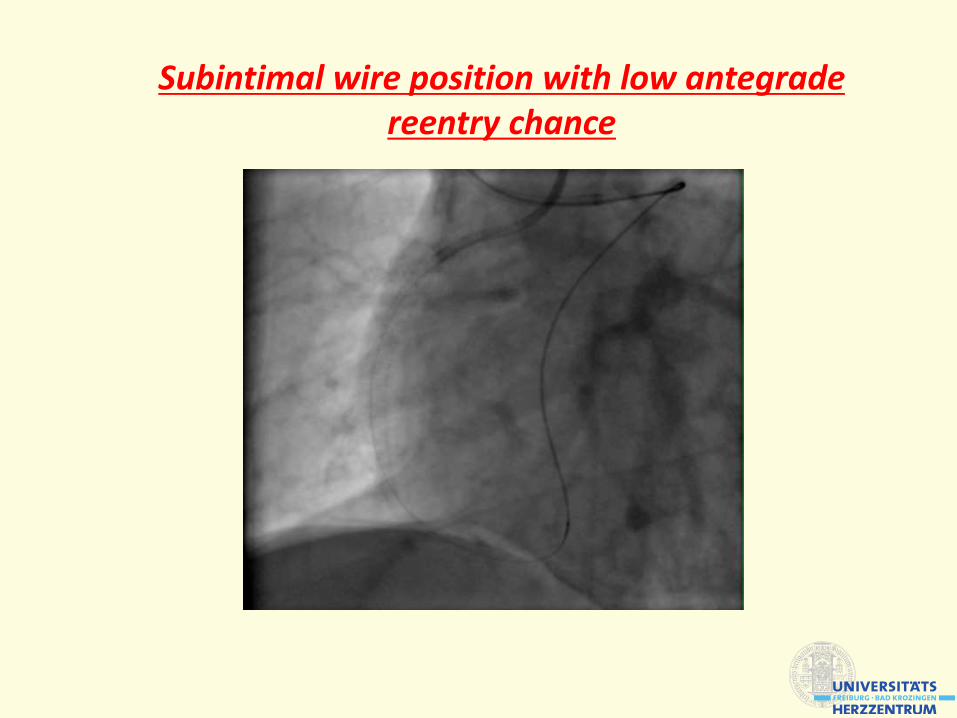
Subintimal wire position with low antegradereentry chance
Subintimal wire position with low antegradereentry chance
Subintimal wire position with low antegradereentry chance
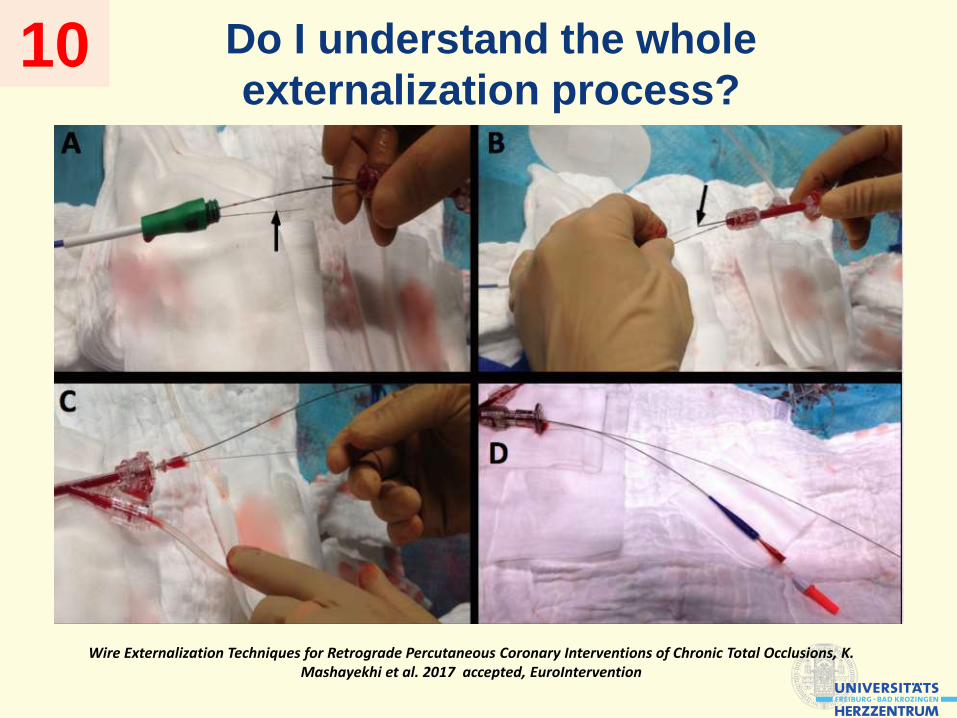
Do I understand the whole
externalization process?10
Wire Externalization Techniques for Retrograde Percutaneous Coronary Interventions of Chronic Total Occlusions, K. Mashayekhi et al. 2017 accepted, EuroIntervention

Do I understand the whole
externalization process?
• Be able to handle complex PCI scenarios (complex bifurcations,
calcified lesions, rotablation)
• Enough experience in basic antegrade techniques (trapping,
parallel wire, MC usage)
• Strong backing from the hole team
• Personal, material and structural resources (2 cathlabs)
• Special knowledge of retrograde techniques
• Support from a high volume CTO (-mentor)
When am I prepared enough for my first
retrograde approach ?

Thank you!
Thank you for your attention!
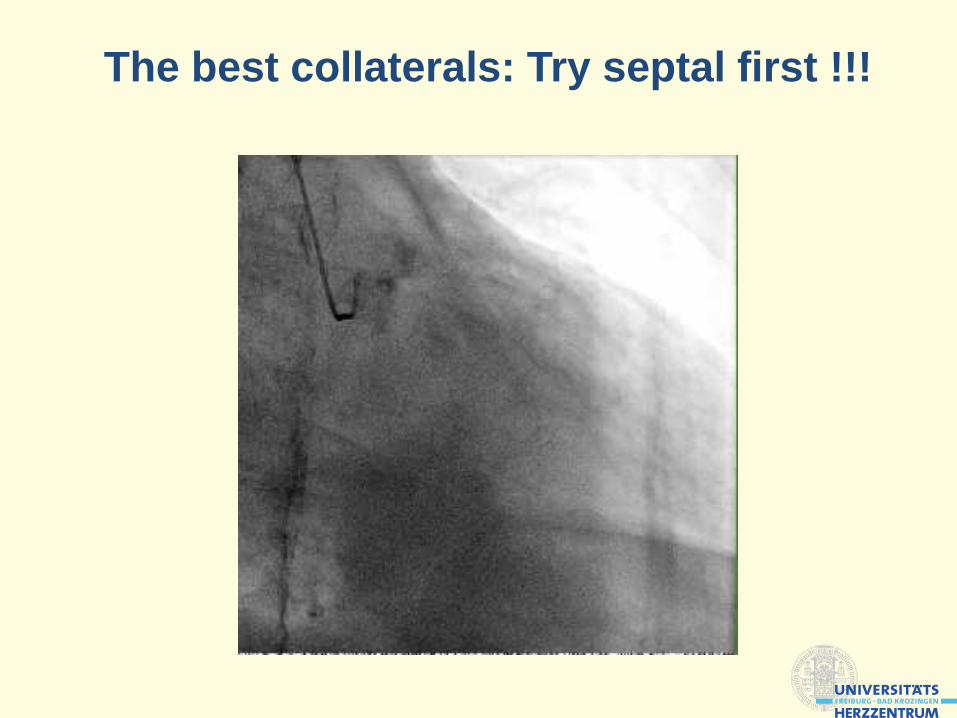
The best collaterals: Try septal first !!!
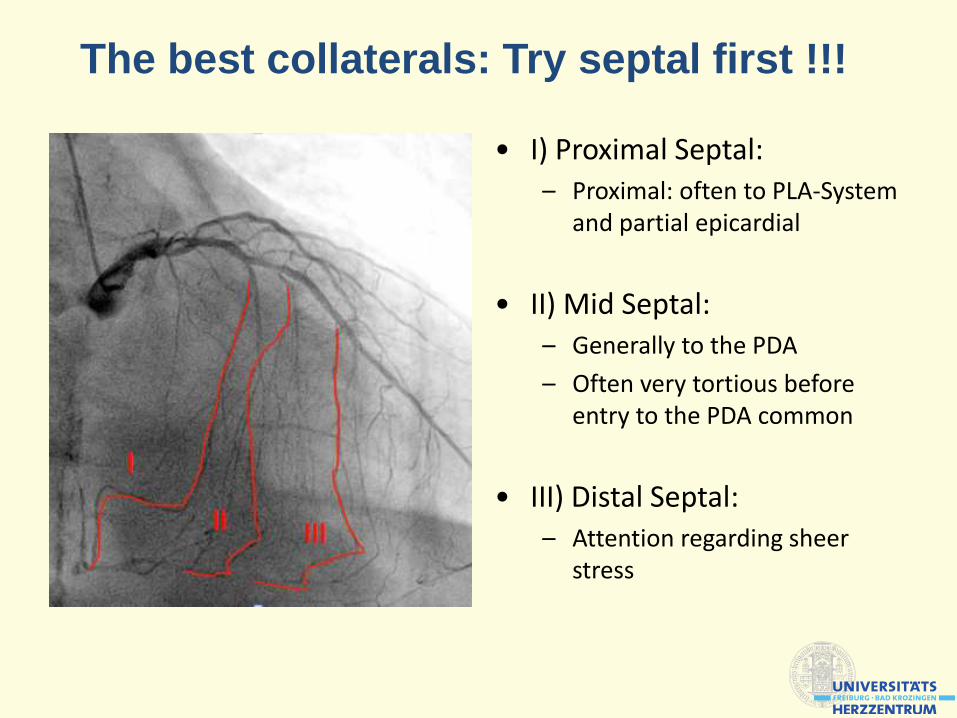
• I) Proximal Septal:– Proximal: often to PLA-System
and partial epicardial
• II) Mid Septal:– Generally to the PDA
– Often very tortious before entry to the PDA common
• III) Distal Septal:– Attention regarding sheer
stress
The best collaterals: Try septal first !!!
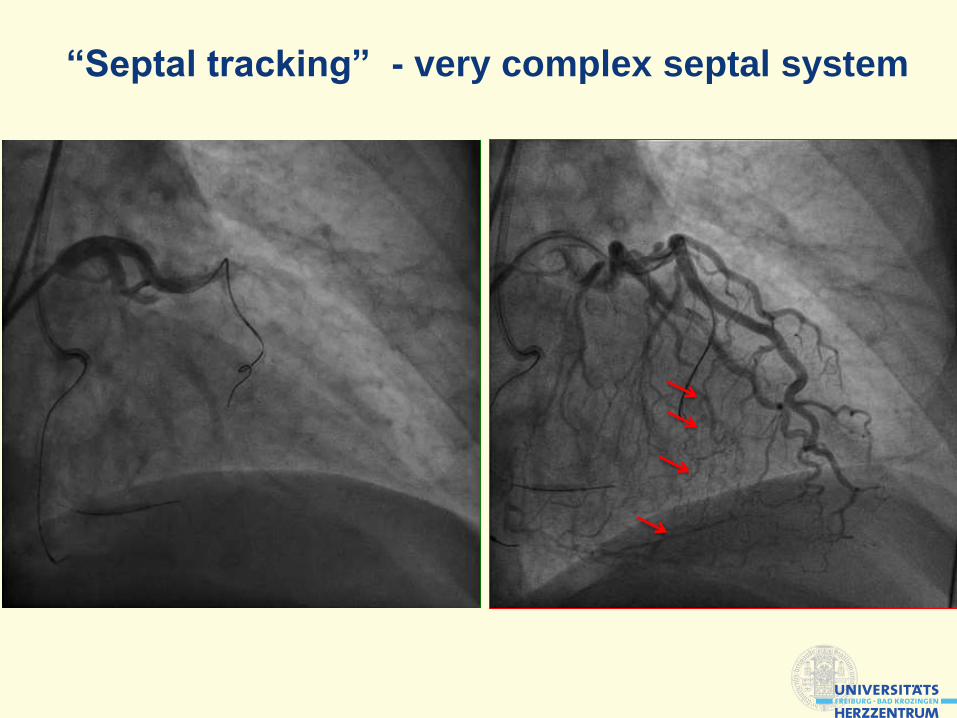
“Septal tracking” - very complex septal system

epimyocardiale collateral crossing
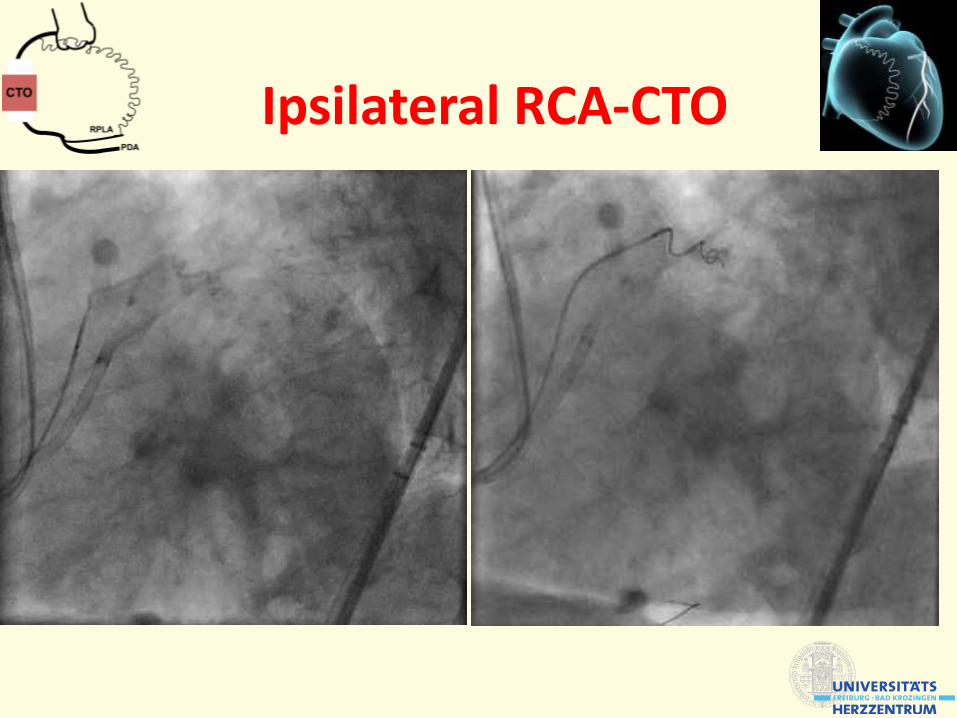
Ipsilateral RCA-CTO
Ipsilateral RCA-CTO Stuttgart Heart-LIVE 2015

Euro-CTO-Club Registry - Successful strategy
10/2013-10/2016
7523CTO-PCIs
2429 (32,3%)Retrograde Attempts
5094 (67,7%)Antegrade Attempts
2,76 J-CTO-Score83,4% Successrate
1,87 J-CTO-Score
92,4% Successrate
241 (3,2%)ADR with CrossBoss
2,49 J-CTO-Score
85,0 % Successrate
K. Mashayekhi, EuroCTO Registry, TCT 2016

Final Successful Strategy
The Hybrid Algorithm for Treating CTOs in Europe:
The RECHARGE Registry
Joren Maeremans et al., JACC 2016 Nov.
1253 CTO Attempts
AWE
623 (58%)
ADR
192 (18%)
RWE/RDR
260 (24%)

PROspective Global REgiStry for the Study
of CTO interventions
49.00%
23.80%
27.10%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Antegrade wiring Antegrade dissection/re-entry Retrograde
Antegrade wiring Antegrade dissection/re-entry Retrograde
Successful techniques in 1810 lesions
01/2012 – 06/2016
Data from Manos Brilakis 2016

The Hybrid Algorithm for Treating CTOs in Europe:
The RECHARGE Registry
Joren Maeremans et al., JACC 2016 Nov.

PROspective Global REgiStry for the Study
of CTO interventions
J-CTO-Score Validation and Successful Crossing Strategy
Christopoulos et al, Circ Cardiovasc Interv. 2015 Jul
n=650 lesions

CTO-Setting retrograde Approach (rad./fem.)
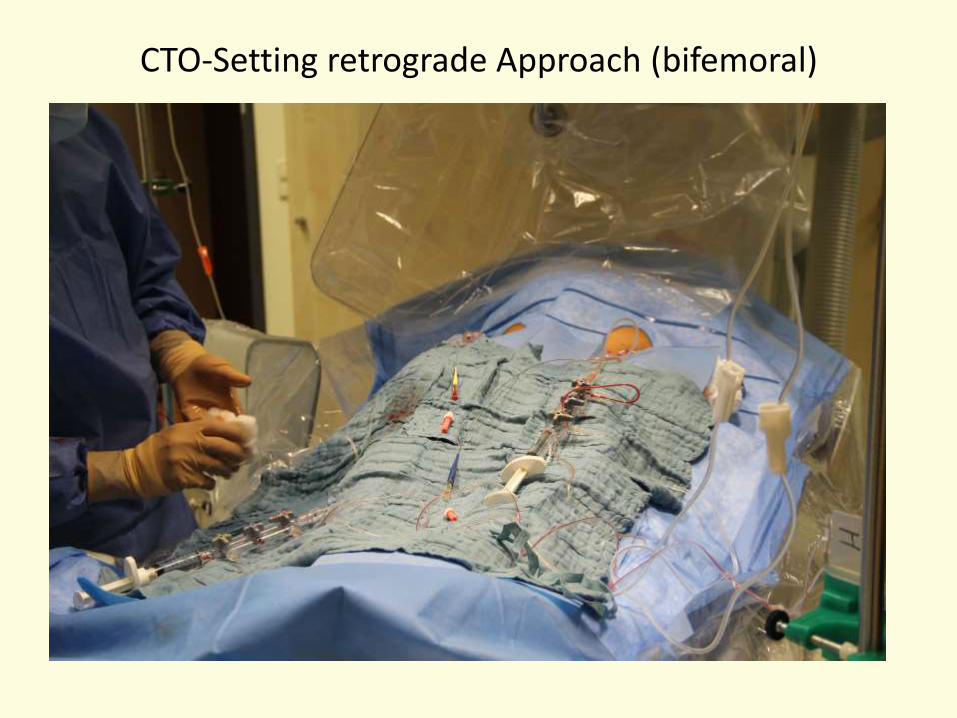
CTO-Setting retrograde Approach (bifemoral)







