dphn phllp ph. dufdcimages.uflib.ufl.edu/ca/00/40/01/44/00001/pdf.pdf · 2009-03-17 · ddn ftr,...
TRANSCRIPT

THE IMF, STRUCTURAL ADJUSTMENT AND HEALTHIN THE CARIBBEAN: A Comparison With Brazil
DAPHNE PHILLIPS Ph. D
Department of Sociology
The University of the West Indies
St Augustine, Trinidad
Trinidad and Tobago
West Indies
Paper prepared for the 18th Annual Conference of the Caribbean
Studies Association to be held in Kingston & Ocho Rios, Jamaica, May
24 -29, 1993.

THE IMF, STRUCTURAL ADJUSTMENT AND HEALTH
IN THE CARIBBEAN: A Comparison With Brazil
ABSTRACT
In this study, an assessment of the impact of Structural Adjustment
policies on the living conditions of people in the Caribbean is
undertaken through observation of the trends in employment,
income, education, nutrition, housing and water supply in the decade
of the 1980s. A comparative analysis is carried out on the effects of
similar policies on identical living conditions in Brazil in the
previous decade. The data show similar patterns of decline in living
conditions for the Caribbean in the 1980s as for Brazil in the 1970s.
For the Brazil study, through the use of multiple regression
techniques on survey data collected in 1990, the relative impact of
these living conditions on health is measured. The results show that
while nutrition has the greatest impact on health, all the other
influencing variables examined significantly affect the health
status of the people.
In conclusion, I argue that if declines in living conditions result in a
measurable decline-in health status, then the declines in these
conditions observed in the Caribbean in the 1980s have negatively
affected health. This negative effect on health is exacerbated
further by the simultaneous cuts in health spending and the gradual
privatisation of health care services observed in the Caribbean.

ACKNOWLEDGEMENTS
The survey data for Brazil used in this analysis were collected
in 1990 for a study funded by the Institute of Health,
Department of Health, Government of the State of Sao Paulo,
Brazil. The principal researchers were Raymond and Karen
Goldsteen of the University of Illinois at Urbana-Champaign. I
thank the Goldsteens for the use of these data.

THE IMF, STRUCTURAL ADJUSTMENT AND HEALTH
IN THE CARIBBEAN:
A Comparison With Brazil
Introduction / Review of the Literature
In the 1980s, the policies of the International Monetary Fund (IMF)
were introduced into developing countries on a large scale, as the
response of the core industrial countries and large international
banks to the massive balance of payments problems that were being
experienced by developing countries. The balance of payments crises
affecting many countries force them to turn to the IMF for loan
assistance.
The IMF was created at the end of the second World War as a result
of an international and monetary conference held at Bretton Woods,
New Hampshire in July 1944, to assist countries which experienced
temporary balance of payments problems as a result of destruction
brought about by the war. These were mainly European countries, and
the assistance provided was particularly generous in helping them to
rebuild their economies and societies. In the 1980s however, in the
wake of the massive balance of payments problems experienced in
developing member countries,
the IMF restructured its lending policies.
The new policies, called Structural Adjustment Policies, were very
much unlike the assistance given to European countries with balance
of payments problems at the end of the second World War. These
policies were punitive and destabilizing and led to declines in the
1

decision making capacity and relative autonomy of the local state.
These IMF policies of Structural Adjustment, which have been
compulsory for developing societies requiring loans for addressing
balance of payments problems, involved reduced public sector
spending and participation in economic activity, an increase in
exports, increased inflation, devaluation of the currency and the
introduction of measures to attract foreign capital.
In more specific detail, these measures have meant reductions in
government expenditure and the size of the public sector; an end to
the creation of new public enterprises and rationalization and
privatisation of those already in existence; higher interest rates to
discourage capital flight; removal of trade and exchange controls;
reduction of effective protection against imports; tax reform to
introduce a higher tax structure, and higher prices for agricultural
producers, especially exporters.
Liberalization of trade and the encouragement of exports are
important goals of the structural adjustment package. These are
brought about by the introduction of measures such as devaluation,
the establishment of quotas and quantitative restrictions, and the
introduction of a uniform external tariff rate. Other elements of the
package consist of an increase in producer prices, reduction of the
wage bill, wage freezes, declines in real wages and salaries, and
reduction or elimination of fringe benefits, labour welfare and other
protective measures. The insistence on privatisation of economic
activities has involved the closure or sale of state enterprises in
2

directly productive and financial sectors, the reduction or
elimination of state marketing agencies and a series of incentives
for foreign investors (Ghai,1991).
These policies are based on a number of assumptions: firstly, there
is the general assumption that excessive expenditure by the state,
particularly where it takes the form of introducing higher levels of
consumption, rather than production, should be reduced. Secondly,
reduction in state spending is assumed to be necessarily associated
with a reduction in wages; thirdly, it is assumed that the cuts in
wages and services will reduce imports. However, they also lead to
increases in the profits of the private sector since private
capitalists subsequently have to pay lower taxes and reduced labour
costs. Finally, the attempt to discourage direct controls over trade
is assumed to enhance the local economy, but this influences the
previous tendency to use the rate of exchange to favour local as
opposed to foreign producers (Brett,1983).
In an attempt to increase their exports, lesser developed countries
immediately confront the core capitalist countries which are
attempting to do the same thing; the latter have the advantage of
producing on a very large scale, selling to a huge home market as
well as controlling established markets abroad, having direct use of
highly trained work forces and research facilities and monopoly over
areas of technology and skills. Lesser developed countries cannot
compete effectively in these conditions.
3

On the other hand, in sectors where lesser developed countries do
have a competitive advantage, where cheap labour provides the
possibility of employment to larger sections of the populations such
as in textiles, the core industrial countries have tended to adopt
protective controls in order to defend jobs and capital investment in
those sectors (Brett,1983). In the textile sector in poor countries
therefore, jobs are not available to the extent to which this may
have been possible.
The rescheduling of debt and debt service as well as the granting of
new loans have been made contingent upon acceptance of the policy
package of structural adjustment measures outlined above, thereby
paving the way for a degree of external intervention in national
policy-making unprecedented in the post war period. The strong
insistence upon eliminating barriers to free trade in these
countries, as well as reducing the role of the state in the economy
has run directly against and counteracts the efforts of Latin
American, Caribbean and African governments to foster greater
national economic integration within a framework of protection for
local industry (Ghai,1991).
Research Questions
The questions posed in this paper are:
1. Have structural adjustment policies affected living conditions in
the Caribbean?
2. What are the effects of living conditions on health status?
4

3. What are the effects of Structural Adjustment policies on health
in the Caribbean?
Methodology
The methodology employed to answer these questions involves
firstly, a comparative analysis • between the effects of Structural
Adjustment policies on living conditions in the Caribbean, and the
effects of similar policies on living conditions in Brazil. Secondly,
I measure the effects of living conditions on health in Brazil (for
which recent survey data is available). Thirdly, I infer similar
effects of living conditions on health in the Caribbean. Finally I
argue that if Structural Adjustment policies have led to a decline in
living conditions, and living conditions have a noticeable and
measurable effect of health, then Structural Adjustment policies
have led to a decline in health status.
The living conditions used in this study are those of income,
employment, education and other social services.
Effects of Structural Adjustment on Living Conditions in
the Caribbean
Many sources clearly indicate a real decline in living conditions in
Latin America, the Caribbean and African countries since the
universal introduction of IMF structural adjustment policies in 1980
for peripheral capitalist countries.
5

Income
The following Table on economic changes in Latin America and the
Caribbean highlights declines in income and resources - from both
resource loss due to deterioration on the terms of trade and lower
levels of imports (both by volume and per capita measures)
coexisting with a huge effort to improve the volume of exports. The
overall conditions of living have nevertheless deteriorated.
Table 1 Changes in Economic Indicators. 1980 - 1988,
Latin America and the Caribbean
(Accumulated Percentages)
GDP per capita -6.6
Income per capita -16.0
(loss due to terms of trade) (-3.0)
(loss due to resource transfers) (-6.0)
Export volume +56.0
Export per capita +36.0
Import volume -13.0
Imports per capita -33.0
1978-1979 1987-1988
Ratio of interest payment to
exports of goods and services 16.7 -28.9
Resource transfers as percentage
of goods and services 22.5 -20.5
Rate of inflation (percentage) 46.0 336.0
6

Source : "The Crisis of the 1980s in Africa, Latin America and the
Caribbean : An Overview." D. Ghai and Cynthia Hewitt de Alcantara, in
The IMF And The South, D. Ghai (editor), Zed Books Ltd.,
London,1991.
Table 1 shows that income per capita declined by 16 percent
between 1980 and 1988 for Latin America and the Caribbean. At the
same time, inflation increased by 630 percent over the ten year
period 1978-1988. This means that there were declines in the
ability of people to provide the levels of food and other basic
necessities which they could have done prior to 1980.
It is evident from the Table that the deterioration in the terms of
trade contributed approximately 3 percent, and the shift in net
external resource inflows added another 6 percent to the 7 percent
decline in income per capita between 1980 and 1988. At the same
time, the volume of exports grew by 56 percent or 36 percent per
capita, while imports by volume declined by 13 percent or one third
on a per capita basis (Ghai & Hewitt de Alcantara, 1991). Despite
this huge sacrifice by the population, the ratio of interest payments
to exports of goods and services grew by over 100 percent -
reflecting an incremental worsening of living conditions.
By the end of 1989, in the Caribbean, the gross domestic product per
capita had fallen below the level it had attained 13 years before
(ECLAC , 1990, p. 11). The national economies lost momentum at
differing rates, as evidenced by a pronounced decline in the
7

coefficient of net investment, from almost 23 percent to 16.5
percent between 1980 and 1988 (ECLAC, 1990, P. 38). Latin America
and the Caribbean as a region had become net exporters of financial
resources. It was estimated that over the period 1980-1988,
accumulated net transfers, in which excessive indebtedness was a
deciding factor, reached more than US200 billion dollars (ECLAC,
1990, p. 47).
Employment
Other indicators of the crucial social situation are the increase in
unemployment, under-employment and self employment; the
increasing tendency for productive employment to move into the
'informal' economy with deterioration in the level and stability of
income, and increase in employment in small or family business and
in micro business many in the informal sector (UN Development
Fund). There was widespread deepening of poverty and especially
poverty. among females.
Social- Services
Public sector spending on all social services ( such as education,
health, housing and social security) declined in those territories
which had implemented Structural Adjustment policies before 1985
(such as Jamaica) but remained relatively constant or increased in
those countries which had not yet implemented these policies as
shown in Table 2.
8

Table 2 Social Service Spendingl Caribbean - 1980 - 1985
Country
(Percentage of all spending)
1983 1984 19851980 1981 1982
Bahamas 7.1 7.7 7.9 8.2 7.8 7.7
Barbados 16.3 16.6 14.3 13.8 14.9 15.6
DominicanRepublic 5.4 5.5 3.2 3.1 2.9 2.7
Guyana 11.6 14.1 16.5 15.6 14.4 16.2
Haiti 2.2 2.3 2.8 2.3 2.3 2.2
Jamaica 14.0 15.5 14.4 13.8 10.4 9.5
Trinfrobago 8.8 9.2 12.2 13.1 13.7 14.0
Venezuela 8.3 9.4 10.0 9.8 9.4 9.8
1. Including education, health, housing, social security and othersocial services.
Source : Modified from Bank of International Development,Washington. D.C. 1988. Cited in ECLAC, 1989.
Education
Table 3 shows that, with the exception of Trinidad and Tobago,
spending on education declined for all territories for which data is
available by 1987 when many more countries had implemented
Structural Adjustment policies.
9

Table 3 Education. Public Sector Spending as a Percentage of all Spending1981 - 1987 (Percentages)
Country 1981 1982 1983 1984 1985 1986 1987
Bahamas 4.1 4.2 4.4 3.9 3.8 3.9 n.a
Barbados 7.0 5.9 5.7 6.3 6.4 5.8 5.9
Dominican Rep. 2.2 1.9 1.8 1.7 1.5 1.4 n.a
Haiti 1.1 1.2 1.1 1.0 1.0 n.a n.a
Jamaica 7.2 7.2 7.3 5.7 5.3 n.a n.a
Trinidad/Tobago 2.4 4.1 4.3 4.7 4.9 5.5 5.6
Venezuela 5.1 4.6 5.0 4.3 4.9 4.5 n.a
Source : Modified from Bank of International Development,Washington. D.C. 1988. Cited in ECLAC, 1989.
Although the level of spending on education in Trinidad and Tobago
did not decline up to 1987, Table 4 shows that there was no
improvement in the percentage of students completing secondary
education in 1986 as compared with 1975, while Table 5 shows a
decline in young persons with tertiary education in Trinidad and
Tobago, Jamaica and Guyana in 1981 as compared with 1975. The
trend indicates that by the 1990s the percentage of persons exposed
to education at all levels is lower than in the 1970s for all
territories.

Table 4 English Speaking Caribbean. Secondary EducationCompleted
1975 - 1986 (Percentage of school age)
Country 1975 1981 1986
Barbados (11-16) 73 84 93
Guyana (12-17) 54 60 n.a
Jamaica 58 60 58
Trinidad/Tobago (12-16) 51 72 50
Source : UNESCO Statistical Year book, 1986. Cited in ECLAC, 1989.
Table 5 English Speaking Caribbean. Tertiary Education By Sex 1975 -
1981(Percentages, ages 20-24)
Country 1975 1981FemaleTotal Male Female Total Male
Barbados 10 n.a n.a 18.7 n.a n.a
Guyana 3.8 5.0 2.7 2.8 3.1 2.5
Jamaica 6.7 n.a n.a 6.0 n.a n.a
Trinidad/Tobago 5.1 6.0 4.2 4.8 5.8 3.8
Source : UNESCO Statistical Year book, 1986. Cited in ECLAC, 1989.
Health Expenditure
In addition to the decline in living conditions of employment,
income, social infrastructure, education and housing, which were
11

brought about by the IMF conditionalities since 1980 in the
Caribbean, there have been specific cuts in health spending by the
governments in areas such as public health provision and health care
services which have simultaneously tended to become privatized,
costly, and outside the reach of large sections of the populations
whose living conditions have further declined. For selected Latin
American and Caribbean countries, the following Table represents
the actual cuts in health spending between 1980 and 1984 in
percentage levels.
Table 6 Cuts in Health Expenditure. 1980-1984 (cumulative).
Latin America and Caribbean
Health Expenditure Cuts
Bolivia -77.0*
Guatemala -58.3
Dominican Republic -46.5
Surinam -44.2**
El Salvador -32.4
Chile -23.8
Barbados -21.3
Jamaica -18.5
Costa Rica -16.5 *Until 1982
Honduras -15.2 **Until 1983
Argentina -13.9
Uruguay -13.4
Source: UNICEF, Adjustment With A Human Face, Vol.1, Clarendon
Press, Oxford, 1987, p 76; cited in Roddick,1988, p.98.
12
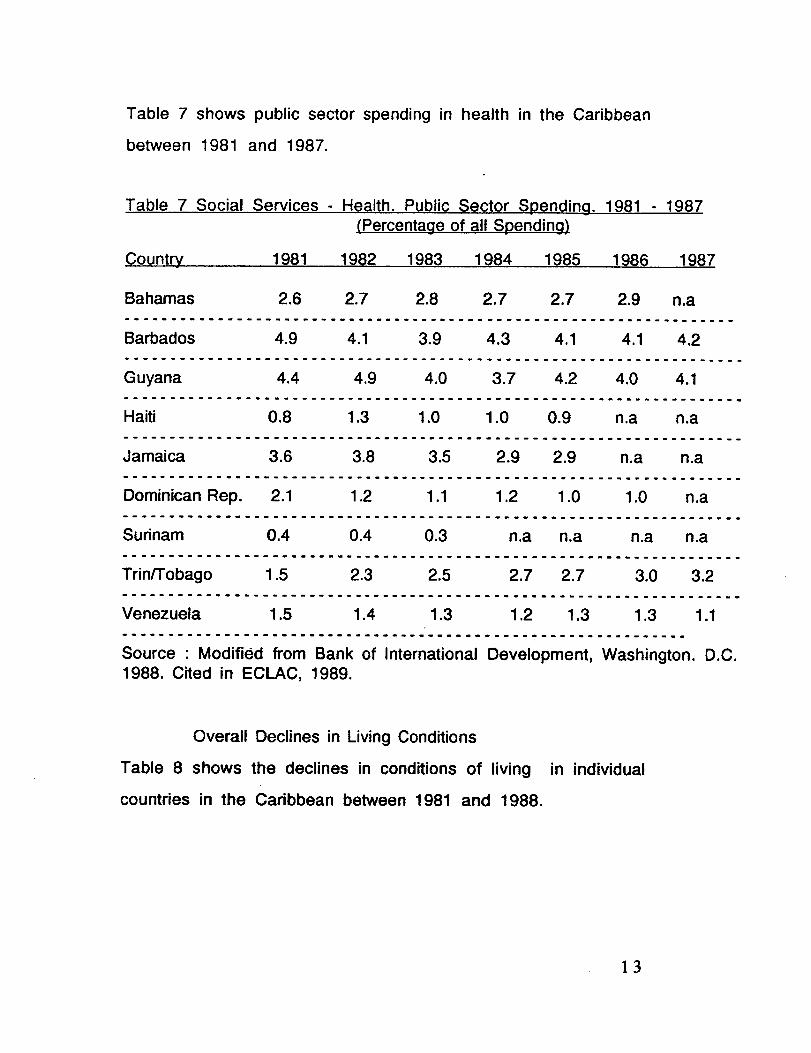
Table 7 shows public sector spending in health in the Caribbean
between 1981 and 1987.
Table 7 Social Services - Health. Public Sector Spending. 1981 - 1987(Percentage of all Spending)
Country 1981 1982 1983 1984 1985 1986 1987
Bahamas 2.6 2.7 2.8 2.7 2.7 2.9 n.a
Barbados 4.9 4.1 3.9 4.3 4.1 4.1 4.2
Guyana 4.4 4.9 4.0 3.7 4.2 4.0 4.1
Haiti 0.8 1.3 1.0 1.0 0.9 n.a n.a
Jamaica 3.6 3.8 3.5 2.9 2.9 n.a n.a
Dominican Rep. 2.1 1.2 1.1 1.2 1.0 1.0 n.a
Surinam 0.4 0.4 0.3 n.a n.a n.a n.a
Trinfrobago 1.5 2.3 2.5 2.7 2.7 3.0 3.2
Venezuela 1.5 1.4 1.3 1.2 1.3 1.3 1.1
Source : Modified from Bank of International Development, Washington. D.C.1988. Cited in ECLAC, 1989.
Overall Declines in Living Conditions
Table 8 shows the declines in conditions of living in individual
countries in the Caribbean between 1981 and 1988.

Table 8 Changes in Conditions of Living - Caribbean Countries - 1981-1988
(Each year over previous year)
1986 1987 1988 1981-88Country 1982 1983 1984 1985
Barbados -5.2 0.0 3.2 0.6 4.8 1.4 2.1 4.3
Cuba 3.3 4.3 6.5 3.9 0.3 -4.7 1.0 33.1
Dominican Rep. -1.1 2.5 2.0 -4.1 0.8 5.5 -1.3 -1.4
Guyana -12.6 -11.7 0.3 -0.8 -1.6 -1.1 n.a. n.a.
Haiti -5.2 -1.2 -1.4 -1.3 -1.3 -2.4 -6.8 -21.7
Jamaica -1.5 -0.4 -2.2 -6.9 1.0 4.1 1.4 -2.8
Trinidad/Tobago* -1.2 -15.0 -6.4 -3.3 -5.3 -8.1 -5.5 -38.6
L. A. & CaribbeanExcluding Cuba -3.5 -4.7 1.4 1.4 1.6 0.3 -1.5 -6.6
*Oil exporting country
Source : Modified from ECLAC, Cepal, 1988.
By 1988, only Barbados and Cuba had not experienced overall
reductions in conditions of living. Trinidad and Tobago experienced
the most severe declines in the region. Coexisting with declines in
the general conditions of living was an increase in consumer prices
for basic goods and services. Table 9 gives yearly increases in
consumer prices in selected Caribbean countries and the overall
increases for Latin America and the Caribbean. These coexisted with
reductions in incomes and represent another indication of the
declines in living conditions.

Table 9 Changes in Consumer Prices - Caribbean - 1980-1988 (From December to December)
Country 1980 1981 1982 1983 1984 1985 1986 1987 1988
Barbados 16.1 12.3 6.9 6.5 5.1 2.4 0.5 6.3 4.3
Dominican Rep. 4.6 7.3 7.2 7.7 38.1 28.4 6.5 25.0 57.3
Guyana
8.5 29.0 19.3 9.6 n.a n.a n.a n.a n.a
Haiti 15.6 16.4 4.9 11.2 5.4 17.4 -11.4 -4.1 8.3
Jamaica 28.6 4.8 7.0 16.7 31.2 23.9 10.4 8.4 7.7
Trin./Tobago 16.6 11.6 10.8 16.4 14.1 6.6 9.9 8.3 6.0
Venezuela 19.6 11.0 7.3 7.0 18.3 5.7 12.3 40.3 31.2 LA&Carib. 56.0 57.5 84.6 130.8 184.8 274.7 198.9 ?? 427.8
Source : Modified from ECLAC, Cepal, 1988. Cited in ECLAC, 1989
Summary / The commonwealth Caribbean
In the Commonwealth Caribbean, Thomas (1991) has shown that the
meaning and application of the crisis has affected the following
conditions, among others, in the region:
- a worsening distribution of income, wealth and access to
productive resources;
- massive, persistent and increasing unemployment and growing
under-employment, especially in those countries where structural
adjustment policies have been introduced;
- inadequate social services, especially social security provisions
for the unemployed, aged and infirm;
15

- massive flight of capital and heavy turnover of assets in the region;
- a weakened trade union movement in the face of increasing
unemployment, declining living standards and widespread poverty;
- the penetration of foreign media, values and culture into the region,
symbolized by the 'satellite dish' culture found in every island, no
matter how small;
- the massive depletion in several countries of social infrastructure,
especially internal transport and power supplies etc.
Source: Adapted from "The Economic Crisis and the Commonwealth
Caribbean: Impact and Response." C. Thomas, in The IMF And The
South. D. Ghai (Editor), Zed Books Ltd., London, 1991.
The application of structural adjustment policies had a decidedly
regressive effect and its social costs fell most notably on the
working class and the middle income sector to increase the extent
of poverty. By 1988, 170 million inhabitants of Latin America and
the Caribbean, representing more than 40 percent of its population,
live in conditions of poverty, unable to satisfy their basic needs
(PAHO, 1990).
Modernization Policies and Declines in living Conditions in Brazil
In Brazil, during the 1964-1985 modernization effort, the military
government introduced policies which emphasized privatisation of
public enterprises, reduction in spending on social services such as
health and education; reduction in public subsidies to specific
groups in the population, removal of trade protection for local goods,
16

tax increases and other similar policies which contributed to
declines in living conditions and impoverishment of the population.
It is clear that policies similar to those introduced in Brazil by the
military government in the modernization period, which contributed
to declines in living conditions of the population, have been
introduced in several 'developing' countries through the mandatory
Structural Adjustment policies of the IMF. The type of modernization
policies implemented in Brazil, which overwhelmingly benefitted US
firms, would not have been possible without a strong, coercive,
military government (Horn, 1985). There is much evidence that this
administration was put in place through the active collaboration of
the US military and government forces to benefit US investment and
profitability in Brazil. (Black, 1977). Structural Adjustment policies
now replace military governments like that of Brazil between 1964-
1985.
This process, among others, enhanced US economic advantage and
effectively led to the denationalization of the economy and the
transfer of former Brazilian sources of production to foreign
control. According to the Journal do Brazil in 1970, foreign
enterprise controlled 72 percent of capital goods, 78 percent of
durable consumer goods, and 52 percent of non-durable consumer
goods, and foreign capital controlled 70.2 percent of the country's
679 largest businesses.
Simultaneously, there was an increase in public utility rates
through the removal of government subsidies so that the costs of
17

transportation, electricity, water etc. were higher for the ordinary
citizen; there was indexing of bonds and loans to housing loans,
savings deposits, savings and loan associations and corporate debts
which made it more costly for the ordinary person to live, as well
as for local business to thrive. In addition, investment banks were
encouraged and there was the creation of special funds which
functioned as adjuncts of the government development bank.
According to Baer (1989) a large portion of the resources of these
official credit institutions were provided by a system of forced
savings whose burden was borne to a large extent by the working
classes. They were used to finance, for example, the sale of small
and medium sized Brazilian public firms or to finance the
acquisition of capital goods (Baer,1989). Hence public funds were
used to sell public property to the private sector. Foreign (more so
US) firms were best placed to take advantage of these special
arrangements.
Between 1968 and 1974 the average annual rate of growth of the
GDP in Brazil surged to 11.3 percent, up from an average of 3.7
percent in the 1962 to 1967 period (Baer,1989; Furtado,1978;
Black,1977). Industry was the leading sector expanding at yearly
rates of 12.6 percent and, within manufacturing, transport
equipment, machinery and electrical equipment were expanding
fastest, unlike the traditional industries of textiles, clothing and
food products (Baer,1989).
18

Part of the increase in the GDP was due to the rise in taxes, both
direct and indirect, which the military government had instituted
from the time of its capture of political office in 1964. Many
accounts claim that taxes contributed approximately 10 to 25
percent of the GDP between 1964 and 1977, the period of the
'economic miracle' in Brazil. This was accompanied by expansions in
foreign trade, especially with the US, and diversification of its
commodity export structure (Furtado,1978; Black,1977; Baer, 1989).
There is extensive documentary evidence of the extreme coercive
rule of this military apparatus in Brazil which facilitated
unprecedented economic growth for (US) firms operating in the
economy at the same time as it created massive poverty among the
ordinary people. One account claims that "more than half of Brazil's
140 million people live in poverty; 40 million are thought to live in
"absolute misery" without adequate food, shelter or health care; and
every year death claims nearly 260,000 babies before their first
birthday" (The Progressive, Sept.1990).
Effects of Brazil's modernization policies on living conditions
The living conditions examined here are those of employment,
income, education, nutrition, water/indoor plumbing, housing and
public health.
Employment.
Prior to 1964, Brazil was agrarian; over 60 percent of the population
of Brazil gained their income through agriculture (Baer,1983). This
has changed dramatically since the late 1960s and by 1985 only 15
19

percent of the population was engaged in full time agriculture
(Baer,1989). The loss of agricultural employment was not replaced
by factory or service jobs because capital investment in industry did
little to expand employment, and in many cases, technology has
eliminated jobs. In 1972, 20 percent of the labour force was listed
as unemployed, and another 35 percent as underemployed
(Black,1977:.243) compared to 10 percent unemployment before
1964 (Black,1977: 241).
Income
The incomes of the majority of the population in Brazil fell
substantially with modernization (Baer,1989: 64; Black,1977:239). One
study reported that every decile of the population, except the top one,
experienced a relative loss of income since 1964; another showed that
the 45 million at the bottom of the society had the same income in
aggregate at the end of the decade as the 900,000 at the top
(Greenwood,1973:. 12). Other sources claim that the poorest 80 percent
received only 27.5 percent of national income in 1970 compared to 35
percent in 1960 while the richest 5 percent increased its share from 44
percent to 50 percent (Burns,1972:17-20).
Urban labour suffered the greatest loss in income and status since
1964 (Black,1977: 243). Horn (1985: 49) quotes a survey conducted
in Sao Paulo which indicated that a worker earning the minimum
wage had to work more than twice as long in 1974 as in 1966 to
purchase the same staple commodities.
20

Education
The availability of education rose only marginally during the latest
modernization period. In 1960, 35 percent of the population had no
formal schooling, while in 1980, 33 percent of the population had no
formal education, a fall of only two percent. In 1960, 57 percent of
the population had between 1 to 4 years of schooling while in 1980,
45 percent had between 1 to 4 years schooling. In 1960, 7.5 percent
of the population had between 5 and 11 years of schooling and in
1980, 17 percent had between 5 to 11 years of schooling.
In relation to higher education, in 1960, under 1 percent of the
population had over twelve years of education and in 1980, 5
percent had 12 years and over (Baklanoff,1969:124-135, IBGE,
1983:12-14). Therefore, while primary education among the
poor actually declined, secondary education increased only
marginally, and specialist education rose fairly rapidly and
was free for the enrollees who were typically from the
wealthy class.
More than a quarter of all public spending on education went to
higher education as late as 1983, and only half to primary education.
Total public spending per student in higher education, where the
benefits accrue overwhelmingly to higher income groups, was about
18 times that in secondary and primary education (United Nations
Development Program Report,1990: 58). In primary education, the
percentage of grade one enrollment not completing primary school
21

was 78 in 1983 (UNDP Report, 1990:75). Many of these children were
out on the streets 'making a living'.
Nutrition
In 1974, at the height of the economic boom, there was a 'crisis' in
health in Brazil, a component of which was a rise in infant mortality
related to malnutrition (Wood,1982). In 1959, an adult in the city of
Sao Paulo could purchase the 'essential ration', a government
established minimum of calories, proteins and vitamins required by
an adult for one month, with 27.1 percent of the minimum wage. By
1974, the same purchase required 68.1 percent of the wage. In
April,1981, 80.7 percent of the wage was needed to buy the
essential ration (Horn,1985: 53). The Institute Of Nutrition of the
Federal University of Rio de Janeiro reported in 1982 that a family
of 4 required more than Cr 6,000 (US$75.00) above the minimum
wage to purchase the minimum diet recommended by the World
Health Organization.
Water/Indoor plumbing
In relation to water and sanitation, there was only marginal
improvement. The 1960 census showed that 41.8 percent of urban
households and 1.4 percent of rural households had water
connections. In 1970, the figures were 55 percent and 2.5 percent
respectively. In 1975, 5 percent of rural homes had adequate
sewerage installations and 5 percent had piped water to the interior.
In urban zones, chemical and industrial hazardous wastes pollute the
streams where favelados (inhabitants of urban slums) bathe and
22

wash their laundry because they have no indoor plumbing (Horn,1985:
55).
Housing
The process of modernization marginalized rural peasants and
intensified the swelling of urban ghettoes with recent migrants
from the rural areas seeking employment. The favelas thus created
or enlarged were typically characterized by poor housing in
overcrowded facilities, as well as by the absence of pipe borne
water, public sanitation, sewerage disposal, electrification and
other public amenities. In 1985, claims Horn, 25 million children -
one in every three - lived on the streets.
The rapid urbanization that occurred with the modernization process
in the society, concentrated large numbers of people in favelas and
corticos , the latter of which are collective dwellings which are
usually large old houses divided up into tiny cubicles, one for each
family. Up to 40 or 50 families share one bathroom, cooking and
washing facilities (Dimenstein,1991). These living arrangements,
and those of the favelas, are notorious for overcrowding and poor
sanitation and encourage epidemics and diarrhoeal diseases.
Public Health Provisions
Government expenditure on public health fell by 30 percent in real
terms between 1967 and 1971 (Black,1977: 241) at the same time
that the mortality rate in Brazil from tuberculosis was the highest
in the hemisphere. While the public health budget declined, and the
health of the poor deteriorated, private, hospital oriented treatment
23

of the sick advanced fairly rapidly (Horn,1985: 51-52; Banta,1986:
366). From 1960 to 1980, the Ministry Of Health saw its share of the
federal Budget fall from 5.87 percent to 1.13 percent. It reached its
lowest point with a 0.09 percent share in 1974. In other words, at
the height of the economic miracle, the state often spent less than 2
percent of its budget on public health (Horn, 1985: 62).
Effects of Living Conditions on Health in Brazil
The following analysis measures the relative effects of living
conditions on health in Brazil. Data from a sample of 457 men and
women gathered in 1990 are used. The indices of health status
employed were 'symptoms of disease' and 'poor functioning'. These
are regressed (in two steps) separately on five aspects of living
conditions : education, income employment, indoor plumbing,
nutrition and lack of crowding in households. Age , sex and marital
status are used as control variables.
24

Table 10 Regression of Symptoms of Disease on SociodemographicCharacteristics and Living Conditions
Step One
B
Step Two
(s.e.of b) (s.e. of b)
Education -.013*** -.171 -.009** -.121
(.004) (.004)
Unmarried .018 .029 .026 .027
(.046) (.045)
Age 1.68 .004 .002 .047
(.002) (.002)
Female .119*** .157 .098** .112
(.040) (.039)
Income -10.8* -.105 -6.39 -.062(5.26) (5.07)
Employed -.006 -.021 -.004 -.016
(.015) (.015)
Indoor -.218*** -.145
Plumbing (.071)
Nutrition -.173**** -.201(.041)
Lack of -.046** -.107
crowding (.021)
Constant 1.49**** 2.05 **"
R2 .089 .176
*p< .05, **p< .01, ***p< .001, ****p< .0001 (1 tailed tests). N = 416.
25

Table 10 shows that having adequate nutrition is the ultimate and the
most important factor in reducing symptoms of disease (Beta = -.201). It
is the major factor through which education and income translate into
good health. Having indoor plumbing (Beta = -.145) and lack of crowding in
homes (Beta = -.107) also reduce symptoms of disease. It is important to
note that employment among this population does not reduce the
probability of having symptoms of disease.
Education significantly reduces illness (Beta = -.171), although its
significance is reduced (Beta = -.121) by its effects on adequate
nutrition, plumbing and lack of crowding in the home, all of which
reduce the probability of having symptoms of disease. When
nutrition, lack of crowding and indoor plumbing are controlled for,
the importance of income is greatly reduced and becomes
insignificant.
Being female is consistently significant in increasing symptoms of
disease; (Beta = .157) the significance is only slightly reduced (Beta
= .112) through the effect of being female on other factors, such as
the probability of having adequate nutrition, indoor plumbing and
living in uncrowded homes. Women have higher rates of morbidity
than men.
The following Table 11 illustrates the effects of sociodemographic
factors and living conditions on poor functioning.

Table 11 Regression of Poor Functioning on Sociodemographic
Characteristics and Living Conditions
Education
Unmarried
Step Oneb
(s.e.of b)-.002(.002).017(.026)
B-.051
.032
Step Twob
(s.e.of b)-8.873(.002).021
(.026)
B-.020
.039
Age .003 ** .107 .003** .132
(.001) (.001)
Female -.023 -.052 -.036 -.081
(.024) (.023)
Income -5.54* -.094 -3.55 - .060
(3.04) (3.00)
Employed -.026** -.161 -.026 ** -.158
(.009) (.009)
Indoor -.052 -.060
Plumbing (.042)
Nutrition -.099**" -.196(.025)
Lack of crowding -.018 -.070(.013)
Constant 1.06 **** 1.29 **"
R2 .071 .123
*p< .05 , **p< .01, ***p< .001, ****p< .0001 (1 tailed tests). N=418
Step one of Table 11 shows that being employed and having a high
income significantly reduces the probability of poor functioning.
Education is not significant in reducing poor functioning.
27

Income has an effect through the extent to which it can be converted
into nutrition. Of all the factors considered, adequate nutrition is
the most significant in reducing poor functioning (beta = -.196). The
significance of employment does not change when nutrition, indoor
plumbing and lack of crowding are controlled for. This means that
work itself is highly significant in reducing poor functioning.
Alternately, poor functioning interferes with employment.
Summary/ Brazil
It is clear that the effects of the modernization process, assisted by
the military government in Brazil have had a deteriorating impact on
living conditions and on health for all but the wealthy. Living
conditions, particularly nutrition levels, have the greatest impact on
health. The negative effects on health that are brought about by a
decline in living conditions of employment, income, education,
nutrition, indoor plumbing and housing conditions, are not
compensated for by the sophistication of the health care system, the
nature of the medical technology, the potency of the drugs nor the
skills of the medical experts.
Effects of Living Conditions on Health In the Caribbean
It can be safely assumed that living conditions impact on health for
the people of the Caribbean in the same way that they do for Brazil.
Adequate nutrition has the greatest impact, while employment,
income, education, adequate housing and water supply (among
others) also significantly affect health status.
28

A deterioration in health status of the population in the Caribbean is
implied in the reduction in living standards which have accompanied
accommodation to the structural adjustment policies mandated by
the IMF. This has been complicated by a reduction in health
expenditure of enormous proportions. The deteriorating effects on
health brought about by the lowering of living conditions among
populations already vulnerable to poor health, have been worsened by
direct reductions in health spending, thus exacerbating a potential
health crisis. Women and children are more vulnerable to poor health.
According to PAHO (1992) document, the fact that women are
concentrated in the informal sector of the economy means that, in
terms of impact on health, their average workdays are longer than
those of men, that they have less paid vacation and sick leave, that
they have less access to health services and the benefits of social
security and their jobs are less stable and certain. This situation,
especially in the case of female heads of households can contribute
to high levels of morbidity.
In relation to mortality the phenomenon of excess female mortality
in early childhood had been noted in 13 Latin American countries and
7 Caribbean countries. In Trinidad and Tobago, excess female
mortality is present for the total group of children under 5, and also
occurring basically in children under 1 year. This was considered to
be a warning sign for the probable existence of and important social
problem, discrimination against girls (Waldron 1987: 209).
29

Conclusions
The international economic policies of the 1960s, which were
designed to further incorporate peripheral countries into the
international capitalist economic system, were expressed as
'modernization' policies. They ultimately functioned for the
economic benefit of multinational firms and core capitalist
countries. Peripheral countries which strongly embraced these
policies, such as Brazil and other Latin American countries, have
depended on military governments whose policies made it possible
for the modernization programme to succeed for multinational firms
and small groups of local elite on the one hand. On the other hand,
these policies have marginalized and further impoverished large
sections of the populations whose health status have rapidly
declined.
The implementation of modernization policies and debates about
modernization are no longer aggressively disputed; they have been
replaced by a whole new ball game, though with similar motive, of
means to handle the international indebtedness of peripheral
countries (which has historical causation) in the new context of
OPEC, the energy crisis, and the concomitant debt crisis which
climaxed in 1982.
In this regard, emphasis on foreign controlled industrialization has
been enlarged, internationalized and enhanced by the dictates of
Structural Adjustment policies which apply to all peripheral
countries needing international funding from any source. The
30

mandatory privatisation of all economic activity, the opening up of
economies to the forces of the market, the compulsory decline of
state financial activity and political decision making, the
deterioration of social infrastructure, the decline in the terms of
trade, among other policies mandated by the IMF, have massively
enhanced multinational advantage in poor countries. They have
simultaneously undermined living conditions in the areas of
employment, income levels, nutrition, education, housing and public
health. These, together with reductions in direct health
spending,have contributed to a decline in health in peripheral
countries from which the Caribbean has not escaped. The IMF and
Structural Adjustment policies, on the basis of the evidence
presented in this paper, are associated with worsening of the health
status of the people in the Caribbean.
31

References
Baer, Werner The Brazilian Economy : Growth and Development.
Prager, New York, 1983.
Baer, Werner The Brazilian Economy : Growth and Development.
Prager, New York, 1989.
Baklanoff, Eric The Shaping of Modern Brazil. Louisana State University
Press, Baton Rouge, 1969.
Beckles, Gloria 'The Health of Women in the English Speaking
Caribbean.' Pan American Health Organization, World Health Organization,
May, 1992.
Black, Jan K. United States Penetration of Brazil. University of
Pensylvania Press, 1977.
Brett, E. A. 'The IMF's View of the World.' In Martin Honeywell (Ed) The
Poverty Brookers : The IMF and Latin America. Latin American Bureau
Ltd., London, 1983.
Burns, B. "Brazil : 'The Imitative Society.' Tne Nation, 215: 17-20, 1972
Dimenstein, Gilberto Brazil : War on Children. Latin American Bureau
Ltd., 1991.
Economic Commission for Latin America and the Caribbean
Transformacion Productiva Con Equidad. Santiago de Chile, 1990
Economic Commission for Latin America and the Caribbean/
United Nations Dynamics of Social Deterioration in Latin America and
the Caribbean in the 1980s. LC/G. 1557.
Furtado, Celso The Economic Growth of Brazil. University of California
Press, 1965.

Ghai, Dharam (Ed) The IMF and the South: The Social Impact of Crisis
and Adjustment.. Zed Books Ltd., London, 1991.
Ghai, D. & Hewitt, C. 'The Crisis of the 1980s in Africa, Latin America
and the Caribbean.' In Ghai, D. (Ed) The IMF and the South: The Social
Impact of Crisis and Adjustment. Zed Books Ltd., London, 1991.
Greenwood, L. 'Brazil Bishops Rap Economic Miracle.' Washington Post,
pp.12-14, May 22, 1973.
Horn, James 'Brazil: The Health Care Model of the Milirtary Modernizers
and Technocrats.' International Journal of Health Services, Vol. 15, No.1:
47-67, 1985.
Pan American Health Organization Epidemiological Profile of
Women's Health in the Region of the Americas. Regional Program on
Women, March, 1990.
Roddick, Jackie The Dance of Millions : Latin America and the Debt
Crisis. Latin American Bureau Ltd., London, 1988.
Thomas, Clive 'The Economic Crisis and the Commonwealth Caribbean :
Impact and Response.' In Ghai, D. (Ed) The IMF and the South: The Social
Impact of Crisis and Adjustment. Zed Books Ltd., London, 1991.
United Nations Development Program Human Development Report,
1990.
Wood, C. H. "The Political Economy of Infant Mortality in Sao Paulo,
Brazil. International Journal of Health Services 12 (2) : 215-229, 1982.