dr. amanj burhan specialist neurosurgeon 5/8/20151brain abscess
TRANSCRIPT
Dr. Amanj Burhan specialist Neurosurgeon
04/18/23 1Brain Abscess
• INCIDENCE:• ETIOLOGY• MICROBIOLOGY• PATHOGENESIS• CLINICAL PRESENTATION• DIAGNOSIS• MANAGEMENT• OUTCOME
04/18/23 2Brain Abscess

INCIDENCE
• Is 1-2% of SOL in brain (USA)• Is 8% (INDIA)• Decreased incidence (because of antibiotic
and improved life)• Lastly increased incidence because of
opportunistic infection in immune compromised patient .
04/18/23 3Brain Abscess

ETIOLOGY
1.Infection :
From PNS ,middle ear and mastoid
Characterized by solitary and located superficially
Infection spread by either direct or through veins(thrombophlibitis of
diploic vein)
PNS (frontal and temporal lobe )
Middle ear (temporal lobe)
mastoid (temporal lobe and cerebellum)
04/18/23 4Brain Abscess

2. Heamatogenous
•hematogenous dissemination microorganism from remote site of infection •The abscess are multiple and deeply located •Mostly located in the frontal and parietal lobe?•Primary foci include (skin pustule ,pulmonary infection , diverticulitis …etc.•In Cyanotic cong. Heart dis. Brain abscess is leading cause of mortality and morbidity •Most common type of CHD. Is TOF 50%•Brain abscess in CHD are generally solitary
04/18/23 5Brain Abscess

3. Penetrating trauma :
A. Penetrating trauma are seen occur soon or
after years from trauma.
Contaminated bone fragments and debris
provide anidus for infection
Bullet cause brain abscess or not ?
04/18/23 6Brain Abscess

B. Basal skull fracture with CSF leak and
meningitis cause post traumatic abscess
•Brain abscess from penetrating trauma is
preventable or not?
04/18/23 Brain Abscess 7
4.Previous craniotomyBecause of :
A. Introduce of M.O.at time of surgeryB. Spread of M.O. intracranialy through the woundC. Bone flap infection
5. Immune compromised person
04/18/23 8Brain Abscess
MICROBIOLOGY•Otogenic and dental infection caused by anaerobic organism •Sinusitis caused by staph aureus, aerobic streptococci • CHD caused by strep. SPP.•In immune deficiency caused by fungus •In AIDS by toxoplasma gondi •Incidence of –ve culture is 25-30%
04/18/23 9Brain Abscess

PATHOGENESIS AND HISTOPATHOLOGY OF BRAIN ABSCESS
• Preceding antibody formation there is an area of necrosis which is seeded by bacteria
• Brain abscess formation are 4 stages 1.stage I:early cerebritis (day 1 to day 3)
characterized by necrotic tissue ,local inflammatory response, marked edema This stage there is no demarcation between the lesion and surrounding brain
04/18/23 10Brain Abscess

2.stage two (late cerebritis)(day 4-10):
characterized by : pus , maximum edema
3.stage three (early encapsulation)(day10—13)
Capsule limits spread of infection
Capsule develops slowly in medial wall of abscess?
4.Stage four: late capsule stage ( day 14 and on )
04/18/23 11Brain Abscess

04/18/23 Brain Abscess 12
04/18/23 Brain Abscess 13

04/18/23 Brain Abscess 14

04/18/23 Brain Abscess 15
04/18/23 Brain Abscess 16
04/18/23 17Brain Abscess

• Symptoms : 1. Head ache ( 90 %) 2. Change in conscious level ( 60 %) 3. FND ( 60 %)
Parietal lobe : hemiparesis Temporal lobe : dysphasia Cerebellar : ataxia and nystagmus
4.Fever (more than 50 %) 5. Nausea and vomiting ( 50 %) 6. Seizure ( 50 %) 7.Papilledema and meningismus
04/18/23 Brain Abscess 18

Laboratory findings
1. WBC : normal or mild increase 2. ESR : increase in 90%3. CSF : not specific
1. Opening pressure 2. Protein 3. Glucose 4. Culture
04/18/23 Brain Abscess 19

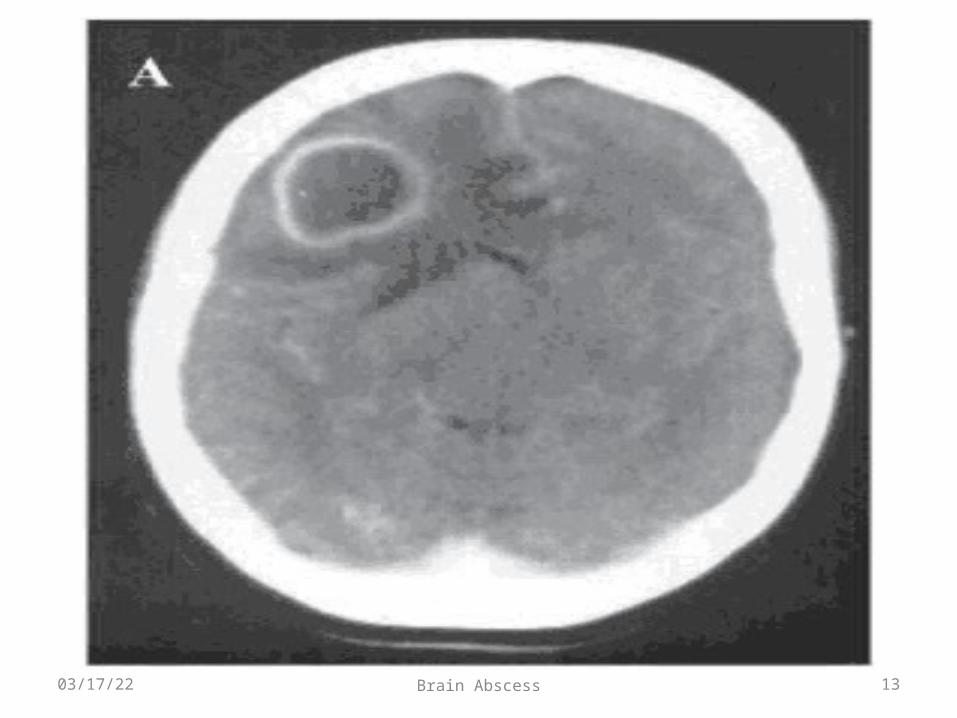
4. radiological characteristic of brain abscess1.Brain CTS with contrast
• ring enhancement • Multi loculation • Multiplicity• Finding of gas
04/18/23 Brain Abscess 20
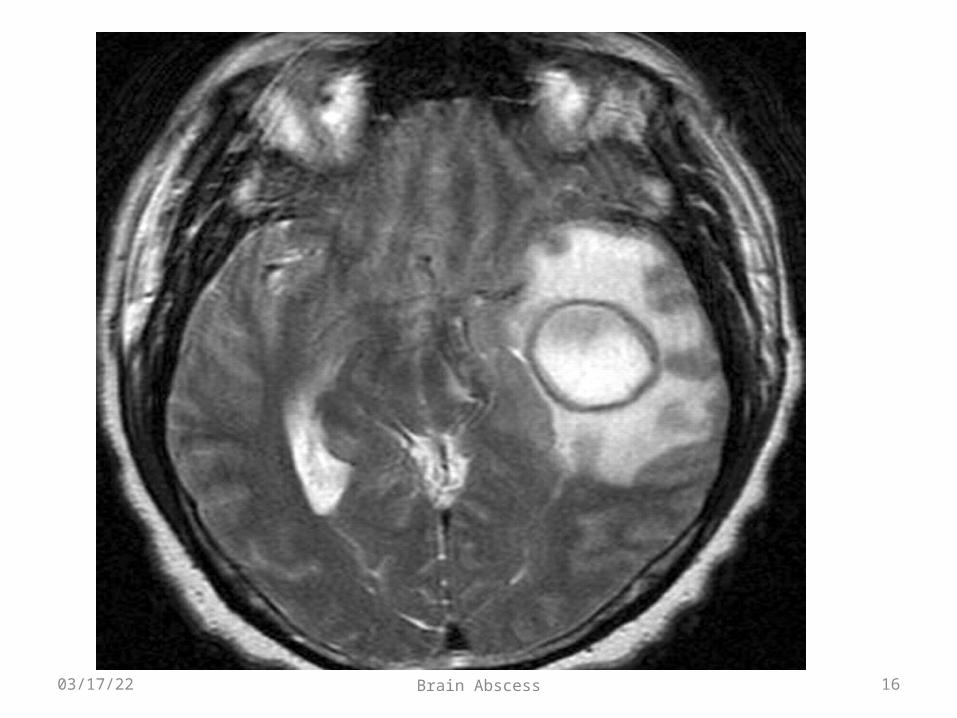
• MRI : • T1 :
• necrotic center ( hypointence) • Capsule ( hyperintence)• Edema ( hypointence)
• T2 :• necrotic center ( hyperintence) • Capsule ( hypointence)• Edema ( hyperintence
04/18/23 Brain Abscess 21

Management
1. Antibiotic therapy : • Antibiotic is mandatory and should given • Antibiotics depends on C/S• Imperial treatment depend on the etiology
– Sinusitis : ( penicillin + metronidazole )– Otitis : ( penicillin + metronidazole + 3rd generation cephalosporin)– Metastatic abscess :(metronidazole + 3rd generation cephalosporin)– Post traumatic abscess ( vancomycin)
04/18/23 Brain Abscess 22

• Advantage of antibiotic therapy • Small size • Deep seated •Multiple
04/18/23 Brain Abscess 23

2. Aspiration : •Advantages : 1.Confirm diagnosis 2.Remove of purulent material 3.Provide environment for antibiotics to work4.Provide immediate relief of IICP•Stereotactic guided aspiration
04/18/23 Brain Abscess 24

04/18/23 Brain Abscess 25
3.Excision of brain abscess •Advantages
1.Traumatic abscess ( contain foreign body and bone fragment )2.Fungal abscess 3.Gas containing abscess
•Disadvantages
04/18/23 Brain Abscess 26

Follow up •CT weekly during antibiotic therapy•And then monthly CT •2-3 week decrease size of abscess •3-4 months complete resolution of abscess• 6-9 months no residual contrast enhancement
04/18/23 Brain Abscess 27
Outcome of abscess :
Mortality influenced by ( herniation , rupture of
abscess to the ventricle , clinical course of
the patient, type of abscess, neurological
state of patient at time of diagnosis)
04/18/23 Brain Abscess 28

1. Long term morbidity : ( seizure , FND, Cognitive dysfunction)
2. Recurrence: ( 5-10%) causes ( inadequate antibiotic therapy, incorrect choice of AB, presence of foreign body , failure to eradicate source of the abscess)
04/18/23 Brain Abscess 29

04/18/23 Brain Abscess 30