dr guy andry, m. moreau, i.el moussaoui, e. willemse, m. quiriny, a. digonnet université libre de...
TRANSCRIPT

Dr Guy ANDRY, M. MOREAU, I.EL MOUSSAOUI, E. WILLEMSE, M. QUIRINY, A. DIGONNET
Université Libre de Bruxelles, Brussels

Despite all the methods to evaluate and to
predict postoperative hypocalcemia, no
consensus exists on the role of routine
calcium and/or Vit. D following thyroid surgery
MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Hypocalcemia is the most frequent complication after total thyroidectomy
Transient: 9 to 50 %Permanent: 0.5 to 13% (→ 33 %)
MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Patients and methods
Patients were prospectively registered from January 2006 till December 2009.
Calcemia (phosphoremia) pre and postopPth levels
After the first blood sample (2 to 3 hours postop.): calcium gluconate 2 g/l of perfusion if calcemia ≤ 8.2 mg/dl
Symptoms and signs of hypocalcemia registered

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Patients and methods
From postop day 1 to day 2 (discharged): pth, calcemia, phosphoremia
Treatment for Ca < 8.0 mg/dl for 8.0 < Ca < 8.3 mg/dl
- 1 g calcium carbonate TID - 1g calcium BID
- Alfacalcidiol 1 mcg/day - Alfacalcidiol 1 mcg/day
0.5 mcg/day
Day 6 to 10 (outpatient clinic): pth, calcemia, phosphoremia and OH-vitD, TSH; T4L, …

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Materials & methods
Pth level and calcemia : between 5th and 10th
day postop, after 1 month, 3 months, 6 to 9 months,
1 year; 1/yr thereafter if prolonged hypocalcemia

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Results (1)
(near) total thyroïdectomy (or totalisation): 537 pts from Jan 2006 till
Dec 2009 (421:W; 116:M)Mean age: 51 yrs (12-82)Selective neck dissection (mainly central compartment: 63 pts)Cancer: 81 pts (72 PTC, 5 MTC, 4 follicular)Multinodular goiter: 415 (50 with throiditis)Basedow : 2912 pts (benigh adenomas, follicular nodule, …)

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Results (2)
43.4% (n=233) developped a transient hypocalcema3.91% (n=21) developped a 1 year hypocalcemia3.17% (n=17) prolonged hypocalcemia 4 PTS had a PTH normal level 15, 23, 32, 39 pg/ml but maintained calcemic supplements to avoid symptoms
MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
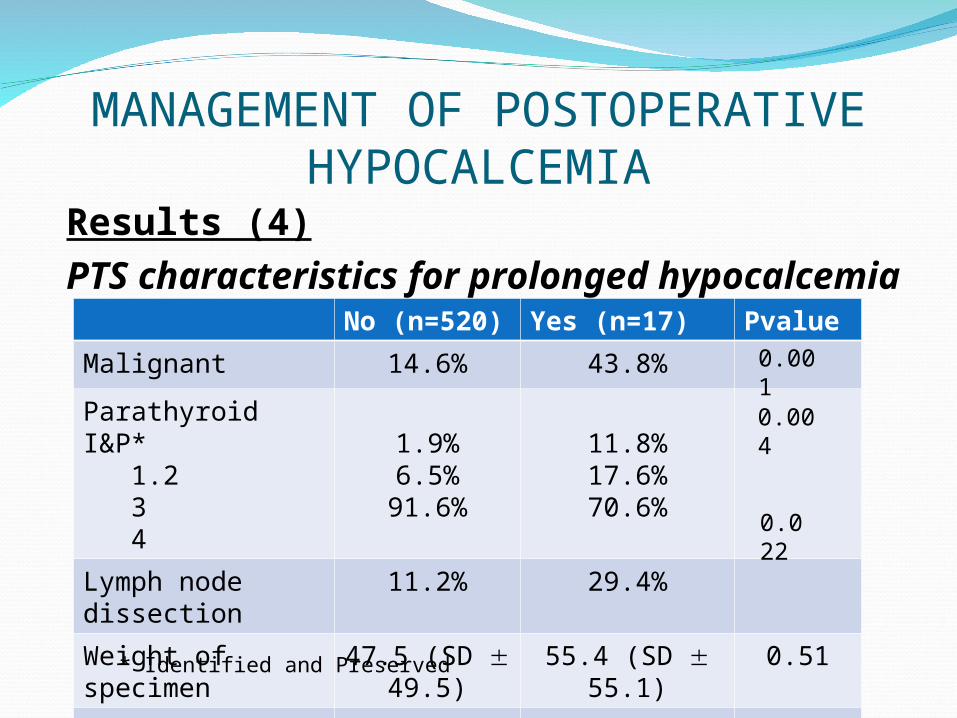
Results (4)PTS characteristics for prolonged hypocalcemia
No (n=520)
Yes (n=17) Pvalue
Malignant 14.6% 43.8%
Parathyroid I&P* 1.2 3 4
1.9%6.5%
91.6%
11.8%17.6%70.6%
Lymph node dissection
11.2% 29.4%
Weight of specimen
47.5 (SD 49.5)
55.4 (SD 55.1)
0.51
Hosp stay (d) 4.08 (SD 0.79)
4.2 (SD 0.84)
0.79
* Identified and Preserved
0.001
0.022
0.004

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Results (6)Sensibility, specificity, ODDS ratio of hypocalcemia hypoPTH to predict « definitive » hypocalcemia
Ca: calcemia; PTH: level of « intact » on ice; 4 hrs: 4 hours postop; J1 to x: J postop 1 to x
Sensitivity
Specificity ODD1 ratio
Pvalue
Ca 4 hrs < 8 mg/dlCa J1 < 8 mg/dlCa J5-20 < 8 mg/dlCa J30 < 8 mg/dl
17.65%70.60%92.30%31.30%
90.3%64.7%94.3%98.3%
24.4
196.125.6
0.280.0029
< 0.0001<0.000
1
PTH 4 hrs < 15 pg/mlPTH J1 < 15 pg/mlPTH J5-20 < 15 pg/mlPTH J30 < 15 pg/ml
100%100%90%
63.6%
62.4%56.4%68.5%92.2%
∞∞
19.620.7
<.0001<.0001<.0001<.0001
MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Discussion (1)
Hypocalcemia postop J5-20: < 8 mg/dl (sens: 92.3%; specif : 94.3%)
Hypo PTH level postop < 15 pg/ml
are predictive of definitive hypocalcemia
ROC curve was constructed PTH early < 9 pg/ml is predictive of definitive hypocalcemia:
100% sensitivity76% specificity ODDS ratio ∞ p < 0.0001

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Discussion (2)
Late recovery of normal parathormone activity
Among 21 PTS with prolonged hypocalcemia
4 showed normal calcemia and PTH levels after 4, 5, 6 and 7 yrs (4 parathyroids respected during the operation; 2 M, 2W; 3 MN Goiters, 1 Basedow)

MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA
Role of postoperative vitamin D and/or
calcium routine supplementation in preventing hypocalcemia after thyroidectomy:
a systematic review and meta-analysis
A. Alhefdhi et al, The Oncologist 2013;18:539-542

Role of postoperative vitamin D and/or calcium routine supplementation in preventing hypocalcemia after
thyroidectomy: a systematic review and meta-analysis (1)
Out of 1180 studies on hypocalcemia post T thyroidectomy9 studies responding to the strength of recommendation taxonomy grading system (SORT)*
* Ebell M.H. 2004, J. Am. Board Fam. Pract.
N = 2285 PTSSymptomatic
hypocalcemia (%)
22 PTS : vit D only580 PTS : Ca++ only
792 PTS : vit D + Ca++
891 PTS : no
4.6 %14 %14 %
20.5 %
After A. ALHEFHI & al 2013

Conclusion
Systematic assays of iPTH at 4 hrs Ca++ between D5-20
are a good indicators of prolonged, hypoparathyroidism
hypocalcemia.
Immediate postop administration of IV Ca++ gluconate (2 g/l) followed at D1-2 by calcidial 1 mg and calcium carbonate (1 to 6 g tailorized by Ca++ levels) prevent the stress of symptomatic hypocalcemic.
MANAGEMENT OF POSTOPERATIVE HYPOCALCEMIA