dr jane dickson - oxleas nhs foundation...
TRANSCRIPT
Dr Jane Dickson
Contents
• Local picture• Small update• New guidelines – interactions, quick-start,
missed pill• Chlamydia• HIV testing

Abortion rates in London
Greenwich
Bromley
Bexley


Teenage pregnancy rates in London
Greenwich
Bromley
Bexley

Levonelle
• Main mechanism of action is to delay ovulation - can’t do this if LH surge has begun
• 1.5mg up to 72 hours post UPSI or contraceptive failure
• Efficacy shown to 96 hours (96-120 hours unknown)
• Can be used > once per cycle (or even if another UPSI outside treatment window)

Taylor
• 14 years old• SI for first time at a party four days ago• LMP 13 days ago • Regular 28 day cycle• Brought in by cousin requesting Emergency
Contraception• Declines IUD


Introducing ellaOne▼®
• ellaOne® is an orally-active, synthetic, selective, progesterone receptor modulator which binds with high-affinity to the human progesterone receptor1
• ellaOne® is indicated for use ‘within 120 hours (five days) of unprotected sexual intercourse (UPSI) or contraceptive failure’1
• ellaOne®’s primary mode of action is to inhibit or delay ovulation1 SP*RM



LARC
• All women presenting for contraception should be advised about the availability of LARC
• All LARC more cost effective than COC at one year
• IUD/IUS/Implanon more cost effective at one year than depot
• Increasing LARC will reduce numbers of unintended pregnancy

LARC Suitability• Nullips• Breastfeeding• Post TOP• BMI>30• HIV• Diabetes• Migraine• Contraindication to estrogen

Have things changed?
2000/01 2008/09Pill 25 25Condom 21 25IUD 5 6Injection/Implant 3 4IUS 1 2Female Sterilisation 11 6Male Sterilisation 11 11

QOF
• Four points – Contraception register• Three points – All those on patch/COC
counselled about LARC• Three points – All those given emergency
contraception counselled about LARC
• Local and national enhanced services

How to increase LARC uptake
• Information• Access• Opportunity• Counselling• Management of side effects• Adequate training• Adequate funding

Request for contraception
Something toremember?
Oral (patch/ring)
Barriers
Something toforget?
Intrauterine method acceptable?
Yes
IUS(five years)
Lighter periods?
Heavier (regular) periods?
IUD(10 years)
No
Planning pregnancy?
Implant(three years)
Yes
Come every 12 weeks – likely amenorrhoea
YesNo
Depot (two years and review)
No


Lucy
• 15 years old• Implanon in situ four months• Has bled irregularly since insertion• Wants device removed


Bleeding problems with implant
• Rule out other causes of bleeding• If no contraindication to estrogen try COC, eg
Marvelon®• If contraindication try Cerazette®• Other things that can be tried include NSAIDs
and one week of doxycycline

UK MEC

Obesity and CHC
• BMI > 30 UK MEC 2
• BMI > 35 UK MEC 3
• BMI > 40 Gone
Headache
• If migraine with aura > five years ago – COC now a 3
• Migraine with aura – all other methods 1 or 2 (COC still a 4)
Smoking
• < 35 yrs UK MEC 2• > 35 and 15/day UK MEC
4• > 35 and < 15/day or
stopped <one year ago UK MEC 3
• >35 and stopped > one year ago UK MEC 2

IUDs
• Contraindicated in trophoblastic disease
• Only a 3 with fibroids/ uterine anomalies if the cavity is distorted
• Current PID/ CT only a 4 for insertion of device (safe to keep in if develop PID)
Caroline
• 17 years• Learning Disability• Heavy menstrual bleeding• Mother is a very senior nurse• Microgynon® made her sick• Loestrin® bled all the time• Had opted for IUS but became afraid and
changed her mind



Step up ProgestogenStep down Estrogen


Qlaira®
• Only COC licensed for heavy menstrual bleeding
• 88% reduction in median menstrual blood loss
• Reductions in blood loss are significant, rapid and sustained (Fraser IS et al. Poster at COGI 2010)


Missed Pill rules If have missed one pill, take next missed pill even if it means taking two in one day
If have missed more than one pill :1.Take last pill missed now2.Take the rest of the pack3.Condoms for seven days4.May need EC5.If last week of pack miss PFI

Tailored/extended Pill taking
• Continuous use of COC with breaks individually tailored for each woman
• Take pill until there is a bleed and then have a PFI (unlicensed)
• Suitable for women who have problems in PFI
• Women tend to develop a regular pattern• Requires time, effort and motivation!


BANG!
Marilyn
• Age 35• Has developed post herpetic neuralgia and is
prescribed carbamazepine for four weeks• Takes COC and doesn’t want to switch the
method• What should she be advised?

Short term enzyme inducers
• Continue COC• Can tricycle and reduce PFI to 4/7• Use additional precautions whilst taking the
enzyme inducer and for four weeks afterwards

Long term Enzyme inducers• If long term use of enzyme inducers is
needed and the woman wishes to continue her COC, then she should be given 50mcg EE (minimum)
• Use a tricycling or extended regime with four days PFI
• If women on enzyme inducers get BTB, this may indicate low EE levels
• Dose of EE can be increased to a maximum of 70mcg

Not ‘reasonably certain’
• Can quick-start if woman likely to be at continued risk of pregnancy and woman expresses wish to start contraception immediately
• Acceptable for CHC (not Dianette), POP, Implant
• Not acceptable for IUD unless criteria for emergency IUD are met
• Injection only if potential risks explained

‘Bridging’
• Quick starting a method immediately after emergency contraception with the view of switching to a different method when pregnancy has been excluded
• 2-3x increased risk of pregnancy in women who go on to have other UPSI in the same cycle that EC has been given compared to those who abstain
Additional Precautions
• After POEC – seven days for CHC, Implant, Injection (nine days for Qlaira )
• After UPA EC – 14 days for CHC, Implant, Injection (16 days for Qlaira )

Contraception for women over the age of 40
• Risks of pregnancy – death, Downs, miscarriage, diabetes, placenta praevia, abruption, preterm delivery, LBW and perinatal mortality
• STIs• Menopause


Can stop contraception
• Two years after menopause if age < 50 or one year after menopause age > 50
• At age 55• Stop CHC and injectable age 50 and switch
to a different method
Use of IUD/IUS in older women
• IUD – If >40 years can keep until no longer need contraception
• IUS- If >45 years and amenorrhoeic can keep until no longer need contraception (if bleeding can be kept for seven years)


Aim of CSP
• Early detection of chlamydia• Treatment of asymptomatic infection• Reduction in sequelae and onward
transmission of chlamydia
• Screen annually or when change partner
Beware missed diagnosis

Testing is easy

0
5,000
10,000
15,000
20,000
25,000
MSM Heterosexualmen born in
Africa
Heterosexualwomen born in
Africa
Heterosexualmen bornelsewhere
including UK
Heterosexualwomen bornelsewhere
including UK
IDU men IDU women
Estim
ated
num
ber o
f per
sons
livi
ng w
ith H
IV
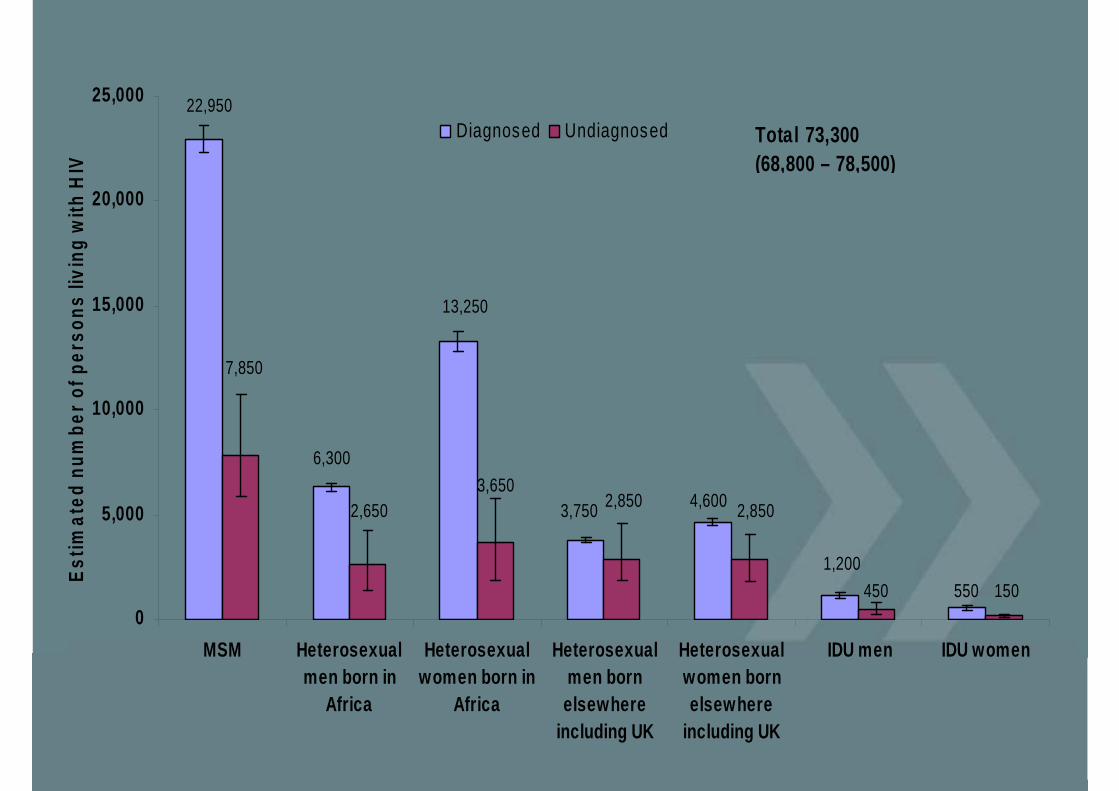
Diagnosed Undiagnosed
550
13,250
Total 73,300(68,800 – 78,500)
22,950
2,650
6,3003,650
3,750 2,850 4,600 2,850
1,200450 150
7,850

Routine HIV testing
• Part of normal diagnostic process• Increased uptake• Reduces stigma• Avoids death and serious illness (earlier Dx)• Reduces onward transmission
Who should have a ‘routine’ test?
• All attending specific services, eg sexual health, antenatal, TOP, drug services, TB/Hepatitis B/C
• Where HIV enters differential diagnosis• Groups at higher risk - MSM, African• Where diagnosed population prevalence > 2
in 1000 – GP registration/hospital admission/blood test


GreenwichBromley
Bexley
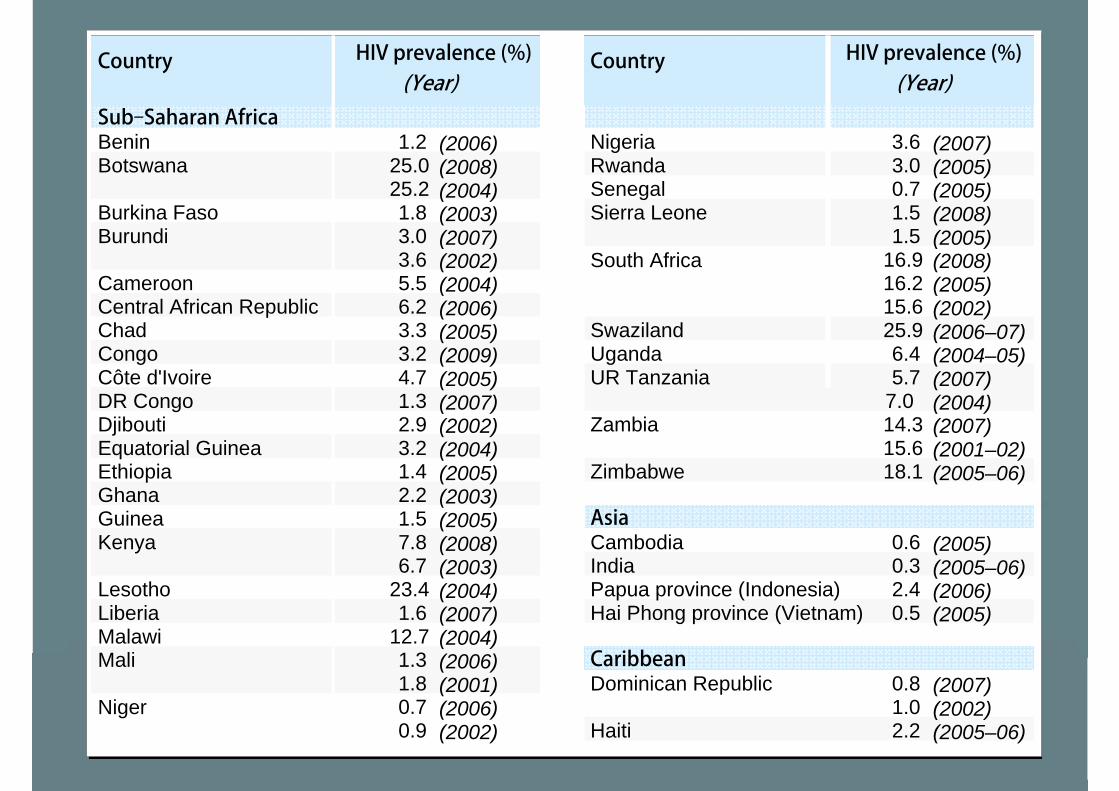
Country
Sub–Saharan AfricaBeninBotswana
Burkina FasoBurundi
Cameroon Central African RepublicChadCongoCôte d'IvoireDR CongoDjiboutiEquatorial GuineaEthiopia Ghana GuineaKenya
Lesotho Liberia MalawiMali
Niger
1.2 (2006)25.0 (2008)25.2 (2004)1.8 (2003)3.0 (2007)3.6 (2002)5.5 (2004)6.2 (2006)3.3 (2005)3.2 (2009)4.7 (2005)1.3 (2007)2.9 (2002)3.2 (2004)1.4 (2005)2.2 (2003)1.5 (2005)7.8 (2008)6.7 (2003)
23.4 (2004)1.6 (2007)
12.7 (2004)1.3 (2006)1.8 (2001)0.7 (2006)0.9 (2002)
HIV prevalence (%)(Year)
Country
NigeriaRwanda Senegal Sierra Leone
South Africa
Swaziland Uganda UR Tanzania
Zambia
Zimbabwe
AsiaCambodia IndiaPapua province (Indonesia)Hai Phong province (Vietnam)
CaribbeanDominican Republic
Haiti
3.6 (2007)3.0 (2005)0.7 (2005)1.5 (2008)1.5 (2005)
16.9 (2008)16.2 (2005)15.6 (2002)25.9 (2006–07)6.4 (2004–05)5.7 (2007)
7.0 (2004)14.3 (2007)15.6 (2001–02)18.1 (2005–06)
0.6 (2005)0.3 (2005–06)2.4 (2006)0.5 (2005)
0.8 (2007)1.0 (2002)2.2 (2005–06)
HIV prevalence (%)(Year)
Barriers
Patients• Fear of disease• Confidentiality• Insurance• Immigration issues• Stigma• Fear of prosecution
Clinicians• Embarrassment• Lack of time• Perceived lack of
skills• Patient won’t cope• Patient doesn’t
consider risk

Alice
• 37 year old South African• No SI seven years• Moved to UK four years previously• Recurrent herpes and candida




Upcoming GP Masterclass dates for your diary
Tuesday 24 April 2012Theme: mental health – cognitive behavioural therapy (to be confirmed)
Wednesday 4 July 2012Theme: cardiology (to be confirmed)
Wednesday 3 October 2012Theme: to be advised