dr. madhu karna consultant pediatric ophthalmologist
TRANSCRIPT

Mystery of the Brown pupil
Dr. Madhu KarnaConsultant Pediatric Ophthalmologist

Presentation
• 8 year old boy with progressive DOV LE • h/o Hit with a nib of a pen for which he was
operated LE 8 months agoO/E Left eye• Vn - perception of light• CCC + Central corneal edema + brown pupil • adherent leucoma INQ + iridodialysis at 6 o’clock • IOP - 60mm HgRight Eye - 6/6, normal eye

Brown Pupil with Flat AC with INQ corneal scar

B scan vitreous clear, retina on, flat AC

D/D
• Anteriorly subluxated lens with posterior pigment epithelium with Malignant Glaucoma
• Iris pigment epithelial /Ciliary body tumor with pupillary block glaucoma (rare in children)

• IOP reduced with topical, oral antiglaucoma medication and intravenous mannitol
• Post Mannitol - AT LE 48/ 56 mm Hg• Post second Mannitol next day – 13/19 mm
Hg

Traumatic corneal opacity with vascularisation

An iris cyst was unveiled!

AC reforming superiorly, convex cyst surface

Lens seen on dilation - clear

Central adherent iris tissue and cyst

Cyst with iris pigment epithelium

Superior AC well formed

Iris Cyst and Iris tissue in visual axis

Management
• Iris cyst excision in toto recommended – with broad iridectomy
• 3rd Mannitol given – 11 mm Hg AT• Managed with a novel approach of minimally
invasive cyst aspiration and chemical ablation of cyst epithelium with absolute alcohol
Postoperatively
• progressive retraction of cyst• IOP – 40 mm Hg immediate postop• IV Mannitol given• IOP came down to 24 mm Hg• Vision improved to 6/24
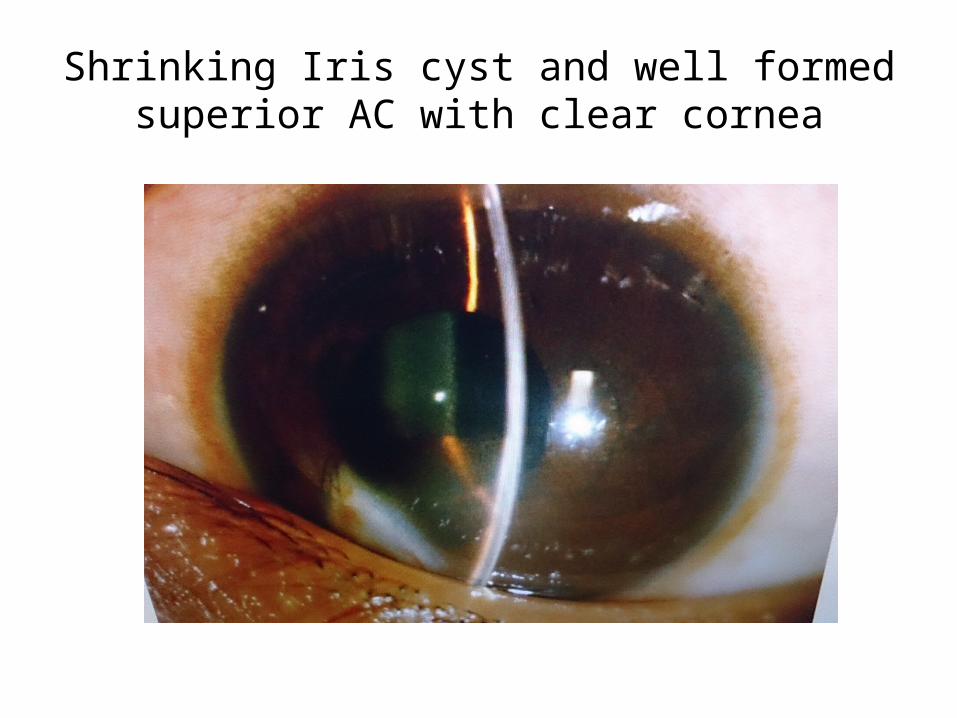
Shrinking Iris cyst and well formed superior AC with clear cornea

PAS nasally

PAS inferotemporally

Shrinking cyst surface inferocentrally

Postop day 6 – shrinking cyst, partly adherent to lens

Shrinking cyst and reducing PAS, inferior corneal edema

Fundus – normal disc and retina, tortuous temporal vessels

At 2 weeks postop
• On Prednisolone , Homatropine, NaCl, Betoxalol, Moxifloxacin, Dorzolamide Drops and Acetazolamide
• Vision – 6/24 with Refn -2.25 x 100 (6/9)• IOP – 14 mm Hg• Fundus – Normal

At 8 weeks postop
• On Prednisolone, Dorzolamide, NaCl• Vn LE 6/9• IOP – 13 mm Hg• Cyst shrunken, mild corneal edema inferiorly• Endothelial count - RE 3301, LE 1676

17 weeks postopVn 6/6 P, IOP – 13 mm Hg
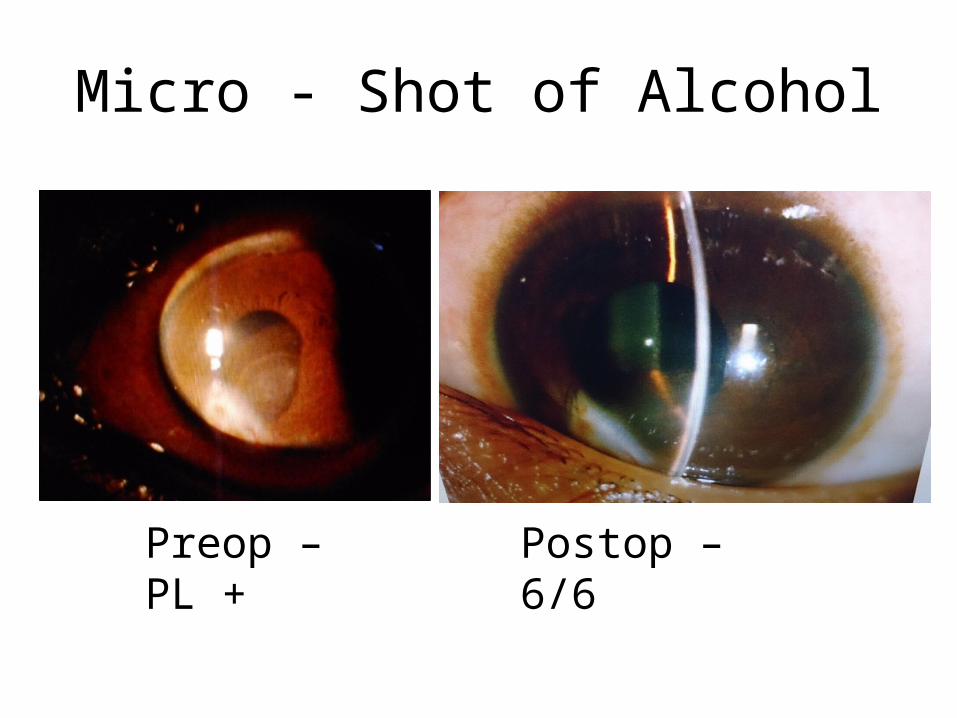
Micro - Shot of Alcohol
Preop – PL + Postop – 6/6


P Rishi, E Rishi, J Biswas, K Nandi, Clinical and histopathological features of posttraumatic iris cyst, IJO. 2008; 56(6): 518-521
• all cysts underwent total excision with/without iridocyclectomy. Additional surgical procedures like lensectomy, vitrectomy, penetrating keratoplasty and intraocular (IOL) removal
• 60% had good visual outcome• uncontrolled glaucoma and graft failure in the rest
Behrouzi Z, Khodadoust A. Epithelial iris cyst treatment with intracystic ethanol irrigation Ophthalmology. 2003 Aug;110(8):1601-5.
• 93 cysts resolved after the first irrigation, 3 after the second irrigation and 2 after the third irrigation and 1 case did not respond after third irrigation
• Intraocular pressure (IOP) normalized in 11 out of 21 cases who had IOP>20 mmHg before ETOH irrigation

C Shields, S Arepalli, E B. Lally, S E. Lally, J Shields. Iris Stromal Cyst Management With Absolute Alcohol–Induced Sclerosis in 16 Patients. JAMA
Ophthalmol. 2014;132(6):703-708.
• Aspiration with 30-g needle on 3-way T-extension into a 3-mL syringe, foll. by immediate infusion of abs. alcohol from a separate 1-mL syringe through the other arm of the T-extension with subsequent alcohol aspiration
• Microscopically monitored aspiration and absolute alcohol–induced sclerosis of iris stromal cysts is safe and effective, with cyst involution obtained in 93% (14 of 15) of patients.

Iris pigment epithelial cysts
Peripheral
Mid Zonal
Pupillary

Free floating Pig Epith cyst
Secondary Epith downgrowth cyst

Thank you for your kind attention