dr michelle meiring mbchb, fcpaeds, mmed (paeds) hpca, pcssa, uct and the bigshoes foundation awacc...
TRANSCRIPT
Dr Michelle Meiring
MBChB, FCPaeds, MMED (Paeds)
HPCA, PCSSA, UCT and
The Bigshoes Foundation
AWACC Conference
Durban 02/10/2009

8 year old boy from rural KZNSent to Jhb by his granny to live with his uncle ( a
miner) to access “better health care”WHO Class IV 3 disease - CD4 < 1 (0,1%)His mother had died from HIV related illness but
had not disclosed to her family- ?one of the reasons for the child’s late first presentation
He had a 5 year old brother who he was very close to who was HIV negative
Worked up and started on HAART as an outpatient
TB excludedHad to be hospitalized for complications
Complications included malignant bowel obstruction secondary to Non-Hodgkins Lymphoma
Surgeons unable to offer surgery due to his poor general condition
Developed severe abdominal pain that paradoxically seemed to worsen with morphine
Fortunately the obstruction resolved with conservative therapy and he was prepared for chemotherapy
During chemo developed excruciating peripheral neuropathy that was difficult to control
Complications included malignant bowel obstruction secondary to Non-Hodgkins Lymphoma
Surgeons unable to offer surgery due to his poor general condition
Developed severe abdominal pain that paradoxically seemed to worsen with morphine
Fortunately the obstruction resolved with conservative therapy and he was prepared for chemotherapy
During chemo developed excruciating peripheral neuropathy that was difficult to control
Fortunately peripheral neuropathy resolved with treatment
Despite a stormy course of chemotherapy did well and went into remission
Discharged back into care of uncle in JhBSent back to live with granny in rural KZN by
uncleAlthough granny tried to keep up with his
treatment, she struggled to collect his meds and keep appointments esp as she was also looking after his 5 year old brother and other grandchildren
Unfortunately ended up defaulting on treatmentSent up by granny to uncle in JhB againArrived in a critically ill stateRelapsed NHLDecision made to “palliate”Referred to Hospice Soweto for terminal careDied peacefully after a visit with his gran and
brotherFamily received assistance to bury him back in
KZN from hospice

What did the Bigshoes JhB Paediatric Palliative care team and Hospice Soweto do for the child?

8 year old boy from rural KZNSent to Jhb by his granny to live with his uncle ( a
miner) to access “better health care”WHO Class IV 3 disease - CD4 < 1 (0,1%)His mother had died from HIV related illness but
had not disclosed to her family- ?one of the reasons for the child’s late first presentation
He had a 5 year old brother who he was very close to who was HIV negative
Worked up and started on HAART as an outpatient
TB excludedHad to be hospitalized for complications
Sibling
support
Bereavement
counseling

Complications included malignant bowel obstruction secondary to Non-Hodgkins Lymphoma
Surgeons unable to offer surgery due to his poor general condition
Developed severe abdominal pain that paradoxically seemed to worsen with morphine
Fortunately the obstruction resolved with conservative therapy and he was prepared for chemotherapy
During chemo developed excruciating peripheral neuropathy that was difficult to control
Explanatio
n
Expert pain
control
Expert advice on Mx
ofMalignant bowel
obstruction

Fortunately peripheral neuropathy resolved with treatment
Despite a stormy course of chemotherapy did well and went into remission
Discharged back into care of uncle in JhBSent back to live with granny in rural KZN by
uncleAlthough granny tried to keep up with his
treatment, she struggled to collect his meds and keep appointments esp as she was also looking after his 5 year old brother and other grandchildren
Advice on the Mx of severe
mucositis –
magic mouth
wash
HIV
Disclosure Counseling
Second line tre
atment
Including motivating for
gabapentin (neurontin)

Unfortunately ended up defaulting on treatmentSent up by granny to uncle in JhB againArrived in a critically ill stateRelapsed NHLDecision made to “palliate”Referred to Hospice Soweto for terminal careDied peacefully after a visit with his gran and
brotherFamily received assistance to bury him back in
KZN from hospice
Assistance with
decision making re
withdrawal of
therapy
Provision of
holistic term
inal
care in a more
conducive
environment
Funeral and
bereavement
support to family
Spiritual care
8 year old boy from rural KZNSent to Jhb by his granny to live with his uncle ( a
miner) to access “better health care”WHO Class IV 3 disease - CD4 < 1 (0,1%)His mother had died from HIV related illness but
had not disclosed to her family- ?one of the reasons for the child’s late first presentation
He had a 5 year old brother who he was very close to who was HIV negative
Worked up and started on HAART as an outpatient
TB excludedHad to be hospitalized for complications
Counselled mom on
her death bed about
disclosure and future
planning for her
children

Fortunately peripheral neuropathy resolved with treatment
Despite a stormy course of chemotherapy did well and went into remission
Discharged back into care of uncle in JhBSent back to live with granny in rural KZN by
uncleAlthough granny tried to keep up with his
treatment, she struggled to collect his meds and keep appointments esp as she was also looking after his 5 year old brother and other grandchildren
Home based care
and
HAART supervisio
n
Orphan care and
support
AND IT’S ROLE IN PAEDIATRIC HIV MANAGEMENT
WHO Definition:Palliative care for children represents a special,
albeit closely related field to adult palliative care. PPC is the active total care of the child's
body, mind and spirit, and also involves giving support to the family.
It begins when illness is diagnosed, and continues regardless of whether or not a child receives treatment directed at the disease.

WHO Definition continued:Health providers must evaluate and alleviate a child’s
physical, psychological and social distress.Effective palliative care requires a broad
multidisciplinary approach that includes the family and makes use of available community resources; it can be successfully implemented even if resources are limited.
It can be provided in tertiary care facilities, in community health centres and even in children's own homes.
WHO Definition:Palliative care for children represents a special,
albeit closely related field to adult palliative care. PPC is the active total care of the child's
body, mind and spirit, and also involves giving support to the family.
It begins when illness is diagnosed, and continues regardless of whether or not a child receives treatment directed at the disease.
PASSIVE
LIMITED TO
TERMINAL
CARE
THE ANTITHESIS OF
ACTIVE TREATMENT
(EG HAART)
WHO Definition continued:Health providers must evaluate and alleviate a child’s
physical, psychological and social distress.Effective palliative care requires a broad
multidisciplinary approach that includes the family and makes use of available community resources; it can be successfully implemented even if resources are limited.
It can be provided in tertiary care facilities, in community health centres and even in children's own homes.
TOO EXPENSIVE
LIMITED TO
HOSPICES
ONLY

Figure 1 Traditional palliative care services model
DIAGNOSIS
ACTIVE AGGRESSIVE
INTENT
PALLIATIVE INTENT BEREAVEME
NT
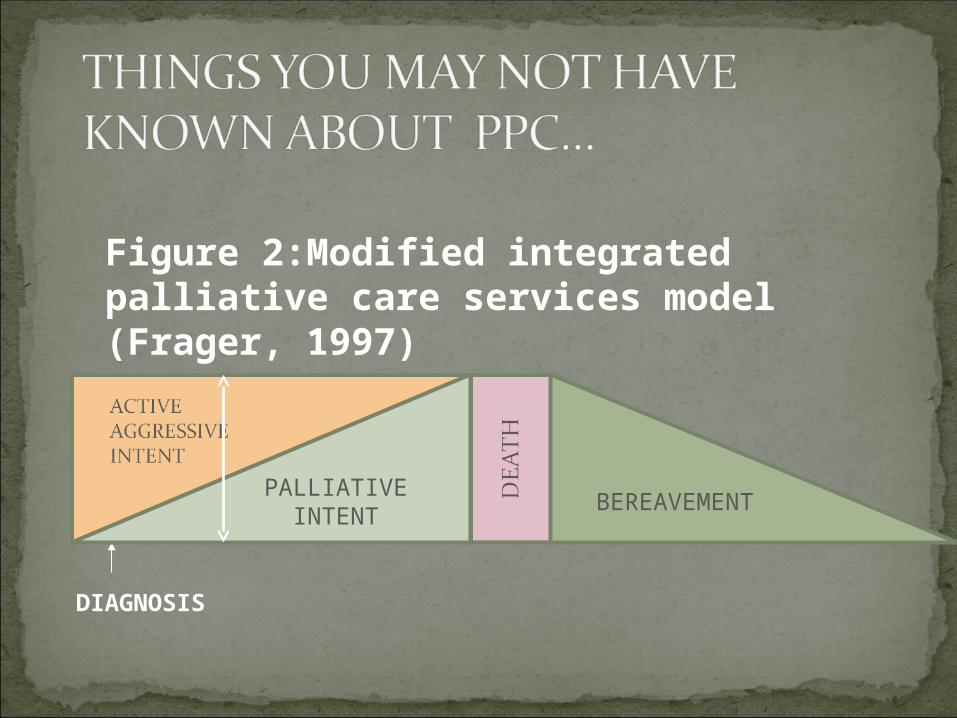
DIAGNOSIS
PALLIATIVE INTENT
BEREAVEMENT
Figure 2:Modified integrated palliative care services model (Frager, 1997)

You don’t have to die to get out of a paediatric palliative care programme
ACT CLASSIFICATION OF PPC CONDITIONSACT 1: Life threatening conditions that can be
cured but where treatment may fail (eg ALL,Malnutrition)
ACT 2: Life limiting conditions associated with premature death but which are manageable due to available treatments (HIV on HAART)
ACT 3: Non-curable conditions where treatment is exclusively supportive (eg IEM)
ACT 4: Non-progressive life limiting conditions associated with disability

It will not become obsolete!
PA
LL
IAT
IVE
TR
EA
TM
EN
T
ACTIVE TREATMENT
AZT : 1986
HAART: 1996
IRIS, RESISTANCE, DRUG TOXCICITIESMDR TB, XDR TB8O’s
90’s2000….

Still 60% of patients requiring HAART in SA not accessing this
Still 1000 people dying from HIV in SA every day
Increasing numbers of patients with IRISARV side effectsTreatment failures secondary to resistanceIncreasing number of orphans nearly 2
millionThe need for palliative care is great!

HAART is the most powerful palliative care drug around!
It does not cure the patientBy addressing the root cause of distressing
symptoms- immunocompromise – opportunistic infections
Improves quantity of lifeImproves quality of lifeDecreases hospitalisationsRestores hope!!
Pain in children with HIV/AIDS is a multifactorial, biologically complex problem associated with diminished quality of life and increased mortality (PACTG 219)
Pain in advanced HIV can be more complex than pain in children with cancer
Pain in cancer is more often related to treatment and procedures than the cancer itself
Pain in HIV is more commonly related to the disease and its complications

INCIDENCE OF PAIN IN HIV:Adult studies: 40 – 60% depending on stage
of HIVPaediatric studies: fewer than adults
Varies from 21-59%National Cancer Institute NIH:1996 (pre-
HAART): 59%Paediatric late outcomes study (PACTG-
219):2002 patients on HAART: 59%
WHAT CAUSES PAIN IN CHILDREN WITH HIV?HIV itself: peripheral neuropathy, cardiomyopathy,
myositis, arthritis, osteonecrosis of the hipGp 120: activates NMDA receptors on excitatory
neuronsHIV infected children are oversensitized to pain as a
result of neuronal damage during developmentAnimal data suggests that exposure to noxious stimuli
during development of the nociceptive neuronal circuitry (the pain pathway) results in a permanent rewiring of the central nervous system.
WHAT CAUSES PAIN IN CHILDREN WITH HIV?HIV itself: peripheral neuropathy, cardiomyopathy,
myositis, arthritis, osteonecrosis of the hipGp 120: activates NMDA receptors on excitatory
neuronsHIV infected children are oversensitized to pain as a
result of neuronal damage during developmentAnimal data suggests that exposure to noxious stimuli
during development of the nociceptive neuronal circuitry (the pain pathway) results in a permanent rewiring of the central nervous system.

WHAT CAUSES PAIN IN CHILDREN WITH HIV?
Secondary and opportunistic infections: Lymphadenitis Parotitis Oral and oesophageal thrush Apthous ulcers Pneumonia Osteomyelitis, Meningitis: bacterial, tuberculous MAC infection, Herpes Zoster Sinusitis UTI Impetigo

What causes pain in children with HIV?Repeated painful proceduresHIV monitoring, diagnostic (esp LP), thoracocentesisChildren do not get used to repeated painful
proceduresPain may worsen with each procedure as a result of
considerable anticipatory anxiety from previous experiences
Untreated pain esp in the newborn period causes lifelong decrease in pain threshold through neural rewiring
Pain is more than just remembered, it changes the brain!
What causes pain in children with HIV?Toxcicities and adverse drug reactions:
d4T and EFZTB RX: INH: peripheral neuropathyChemotherapy: vincristine, cispaltin, etoposide,
inteferon
WHAT CAUSES PAIN IN CHILDREN WITH HIV?
NON-AIDS conditions:Same things that cause pain in children
without HIVDental diseaseMigraine tension headachesTrauma

WHAT CAUSES PAIN IN CHILDREN WITH HIV?
Psychosocial stressors – emotional painLiving with a chronic illnessPovertyLong period of hospitalisation, maternal
separationPotential or actual loss of a parentClinical depressionBeing teasedNormal anxieties of childhood
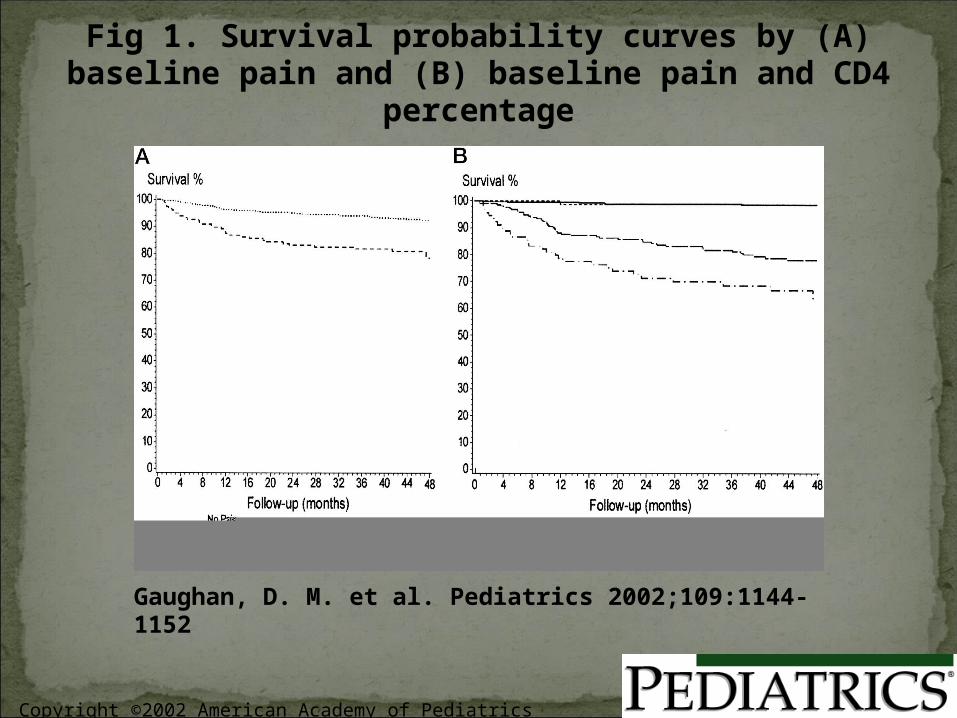
Untreated acute pain is responsible for considerable morbidity and even mortality
HIV infected children with pain were 5X more likely to die than patients without
Untreated acute pain can lead to chronic painUntreated acute pain can reset the pain
threshold for the rest of the child’s life
Copyright ©2002 American Academy of Pediatrics
Gaughan, D. M. et al. Pediatrics 2002;109:1144-1152
Fig 1. Survival probability curves by (A) baseline pain and (B) baseline pain and CD4 percentage

The story of Jeffrey Lawson: Born 198526 week prem weighing 750 gmsHad a PDA ligation at 2 weeks of lifeProcedure (included a mini thoracotomy)
lasted 1 ½ hoursFollowing the surgery… things started going
wrongNumerous electrolyte disturbances and other
signs of catabolismDeveloped an intra-ventricular haemorrage
and died a few weeks post op

Mom decided to investigateDiscovered the PDA ligation had been done
under pancuronium onlyThe anaesthetist had not given any analgesia
as she thought he was too sick (BP too low)During surgery BP and pulse increased
considerably
Catabolic reactions noted post op were secondary to stress response from pain
Untreated pain had been the trigger leading to his death
Public outcry when her letters were published in the Washington Post
1 year later AAP issued a policy statement recommending analgesia in newborns including prems
Recent studies suggest HIV infected children may be more sensitive to morphine than non-HIV infected children and that increases should be made more gradually
Sometimes accept side effects if they are less severe than the pain and especially if tolerance will develop in a few days (esp: drowsiness, nausea and vomiting)
Treat side effects with anti-emetics, laxatives if necessary
Palliative care developed out of the modern hospice movement
Dame Cecily Saunders started the first adult hospice St Christopher’s Hospice in London in 1967
First Children’s Hospice was opened in Oxford (UK) in 1982
First hospital based PPC service started at St Mary’s Hospital in New York in 1985,GOSH followed in 1986
Palliative Medicine became recognised as a full medical speciality in the UK in 1989 under the Royal College of Physicians

Rapidly developing speciality in paediatrics worldwide
2 academic chairs in PPC in GermanyRecently created chair in GOSH (UK)Increasing evidence base in paediatric pain
and its managementStill need increasing evidence base for drugs
used to treat non pain syndromes (many still used off code esp in children < 2 years)
TOWARDS EXCELLENCE WITHOUT APOLOGY!!!
ANY QUESTIONS?