dr. neeraj-presentation-23-des
TRANSCRIPT
Cardiology Top 5Cardiology Top 5
Top 5 recent advances in 2011 (which will impact our practice in 2012) Top 5 recent advances in 2011 (which will impact our practice in 2012)
Dr Neeraj BhallaChairman and HODDeptt of CardiologyBLK Super Specialty Hospital
Dr Neeraj BhallaChairman and HODDeptt of CardiologyBLK Super Specialty Hospital
Advancements in Anticoagulation
00
Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolism
Favourswarfarin
Favoursother treatment
Warfarin vs
Placebo1
20
Low-dose warfarin1
05 10 15
Aspirin1
Aspirin + clopidogrel2
Clinical Trials in Perspective
Error bars = 95 CI BID = twice daily
1 Adapted from Camm J ESC 2009 oral presentation 182 2Lip GYH Edwards SJ Thromb Res 2006118321-333
Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
AT antithrombin Ph phaseFibrin
IX
IXa
X
VIIIa
Thrombin
Fibrinogen
Direct factor Xa inhibitorsApixaban (Ph III ongoing)56
Rivaroxaban (Ph III completed)7
Edoxaban (Ph III ongoing)8
Betrixaban (Ph II ongoing)9
Va
Xa
II
AT
Direct thrombin inhibitors Dabigatran etexilate (Approved)10
AZD0837 (Ph II completed)11
Indirect factor Xa inhibitors Idraparinux (Ph III terminated)3
SSR 126517 (withdrawn 2009)4
Vitamin K antagonist Tecarfarin (Ph II completed)2
Tissue factorVIIa
New Oral Antiocoagulants
CommonPathway
IXX
TF VIIa
VIII
Xa
Thrombin
Fibrin
ThrombinActivity
InitiationPhase
AmplificationPropagation
Phase
PlateletSurface
XIIXI
Contact
Fibrinogen
Dabigatran2
etexilateDabigatran2
etexilate
Rivaroxaban1
ApixabanRivaroxaban1
Apixaban
WarfarinWarfarin
1 Mahaffey KW et al Presented at AHA 2010 Session LBCT02 21839 Available at httpsciencenewsmyamericanheartorgsessionslate_breakingshtmlrocket 2 Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Adapted from Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Advantage of Direct Thrombin Inhibitors (DTIs)
DTIs block both circulating and clot-bound thrombinThrombin generation
Clot-bound thrombin
Heparin
Conversion of fibrinogen to fibrin
DTIs dabigatran etexilate
Amplification
Anti-thrombin
DTIs dabigatran etexilate
DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Advancements in Anticoagulation
00
Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolism
Favourswarfarin
Favoursother treatment
Warfarin vs
Placebo1
20
Low-dose warfarin1
05 10 15
Aspirin1
Aspirin + clopidogrel2
Clinical Trials in Perspective
Error bars = 95 CI BID = twice daily
1 Adapted from Camm J ESC 2009 oral presentation 182 2Lip GYH Edwards SJ Thromb Res 2006118321-333
Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
AT antithrombin Ph phaseFibrin
IX
IXa
X
VIIIa
Thrombin
Fibrinogen
Direct factor Xa inhibitorsApixaban (Ph III ongoing)56
Rivaroxaban (Ph III completed)7
Edoxaban (Ph III ongoing)8
Betrixaban (Ph II ongoing)9
Va
Xa
II
AT
Direct thrombin inhibitors Dabigatran etexilate (Approved)10
AZD0837 (Ph II completed)11
Indirect factor Xa inhibitors Idraparinux (Ph III terminated)3
SSR 126517 (withdrawn 2009)4
Vitamin K antagonist Tecarfarin (Ph II completed)2
Tissue factorVIIa
New Oral Antiocoagulants
CommonPathway
IXX
TF VIIa
VIII
Xa
Thrombin
Fibrin
ThrombinActivity
InitiationPhase
AmplificationPropagation
Phase
PlateletSurface
XIIXI
Contact
Fibrinogen
Dabigatran2
etexilateDabigatran2
etexilate
Rivaroxaban1
ApixabanRivaroxaban1
Apixaban
WarfarinWarfarin
1 Mahaffey KW et al Presented at AHA 2010 Session LBCT02 21839 Available at httpsciencenewsmyamericanheartorgsessionslate_breakingshtmlrocket 2 Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Adapted from Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Advantage of Direct Thrombin Inhibitors (DTIs)
DTIs block both circulating and clot-bound thrombinThrombin generation
Clot-bound thrombin
Heparin
Conversion of fibrinogen to fibrin
DTIs dabigatran etexilate
Amplification
Anti-thrombin
DTIs dabigatran etexilate
DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

00
Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolism
Favourswarfarin
Favoursother treatment
Warfarin vs
Placebo1
20
Low-dose warfarin1
05 10 15
Aspirin1
Aspirin + clopidogrel2
Clinical Trials in Perspective
Error bars = 95 CI BID = twice daily
1 Adapted from Camm J ESC 2009 oral presentation 182 2Lip GYH Edwards SJ Thromb Res 2006118321-333
Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
AT antithrombin Ph phaseFibrin
IX
IXa
X
VIIIa
Thrombin
Fibrinogen
Direct factor Xa inhibitorsApixaban (Ph III ongoing)56
Rivaroxaban (Ph III completed)7
Edoxaban (Ph III ongoing)8
Betrixaban (Ph II ongoing)9
Va
Xa
II
AT
Direct thrombin inhibitors Dabigatran etexilate (Approved)10
AZD0837 (Ph II completed)11
Indirect factor Xa inhibitors Idraparinux (Ph III terminated)3
SSR 126517 (withdrawn 2009)4
Vitamin K antagonist Tecarfarin (Ph II completed)2
Tissue factorVIIa
New Oral Antiocoagulants
CommonPathway
IXX
TF VIIa
VIII
Xa
Thrombin
Fibrin
ThrombinActivity
InitiationPhase
AmplificationPropagation
Phase
PlateletSurface
XIIXI
Contact
Fibrinogen
Dabigatran2
etexilateDabigatran2
etexilate
Rivaroxaban1
ApixabanRivaroxaban1
Apixaban
WarfarinWarfarin
1 Mahaffey KW et al Presented at AHA 2010 Session LBCT02 21839 Available at httpsciencenewsmyamericanheartorgsessionslate_breakingshtmlrocket 2 Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Adapted from Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Advantage of Direct Thrombin Inhibitors (DTIs)
DTIs block both circulating and clot-bound thrombinThrombin generation
Clot-bound thrombin
Heparin
Conversion of fibrinogen to fibrin
DTIs dabigatran etexilate
Amplification
Anti-thrombin
DTIs dabigatran etexilate
DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
AT antithrombin Ph phaseFibrin
IX
IXa
X
VIIIa
Thrombin
Fibrinogen
Direct factor Xa inhibitorsApixaban (Ph III ongoing)56
Rivaroxaban (Ph III completed)7
Edoxaban (Ph III ongoing)8
Betrixaban (Ph II ongoing)9
Va
Xa
II
AT
Direct thrombin inhibitors Dabigatran etexilate (Approved)10
AZD0837 (Ph II completed)11
Indirect factor Xa inhibitors Idraparinux (Ph III terminated)3
SSR 126517 (withdrawn 2009)4
Vitamin K antagonist Tecarfarin (Ph II completed)2
Tissue factorVIIa
New Oral Antiocoagulants
CommonPathway
IXX
TF VIIa
VIII
Xa
Thrombin
Fibrin
ThrombinActivity
InitiationPhase
AmplificationPropagation
Phase
PlateletSurface
XIIXI
Contact
Fibrinogen
Dabigatran2
etexilateDabigatran2
etexilate
Rivaroxaban1
ApixabanRivaroxaban1
Apixaban
WarfarinWarfarin
1 Mahaffey KW et al Presented at AHA 2010 Session LBCT02 21839 Available at httpsciencenewsmyamericanheartorgsessionslate_breakingshtmlrocket 2 Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Adapted from Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Advantage of Direct Thrombin Inhibitors (DTIs)
DTIs block both circulating and clot-bound thrombinThrombin generation
Clot-bound thrombin
Heparin
Conversion of fibrinogen to fibrin
DTIs dabigatran etexilate
Amplification
Anti-thrombin
DTIs dabigatran etexilate
DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

New Oral Antiocoagulants
CommonPathway
IXX
TF VIIa
VIII
Xa
Thrombin
Fibrin
ThrombinActivity
InitiationPhase
AmplificationPropagation
Phase
PlateletSurface
XIIXI
Contact
Fibrinogen
Dabigatran2
etexilateDabigatran2
etexilate
Rivaroxaban1
ApixabanRivaroxaban1
Apixaban
WarfarinWarfarin
1 Mahaffey KW et al Presented at AHA 2010 Session LBCT02 21839 Available at httpsciencenewsmyamericanheartorgsessionslate_breakingshtmlrocket 2 Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Adapted from Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Advantage of Direct Thrombin Inhibitors (DTIs)
DTIs block both circulating and clot-bound thrombinThrombin generation
Clot-bound thrombin
Heparin
Conversion of fibrinogen to fibrin
DTIs dabigatran etexilate
Amplification
Anti-thrombin
DTIs dabigatran etexilate
DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Adapted from Eikelboom J et al J Am Coll Cardiol 20034170Sndash78S
Advantage of Direct Thrombin Inhibitors (DTIs)
DTIs block both circulating and clot-bound thrombinThrombin generation
Clot-bound thrombin
Heparin
Conversion of fibrinogen to fibrin
DTIs dabigatran etexilate
Amplification
Anti-thrombin
DTIs dabigatran etexilate
DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

DIRECT THROMBIN INHIBITORS
Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Dabigatran Etexilate
Potent and reversible oral DTI1 Inhibiting both c lo t b o u n d and fre e t h ro m b in 1
Predictable and consistent PK profile23 -Rapid onsetoffset of action2 (Peak plasma levels within 2 hours)A n t ic o a g u la t io n m o n it o r in g mdash N o t re q u ire d 4
Half-life 12ndash17 hours (twice-daily dosing)1
L o w d ru g ndash d ru g in t e ra c t io n s (not metabolised by CYP450 enzymes)15
No foodndashdrug interactionsDosing independent of meals or dietary restrictions6
6 5 bioavailability ~80 renal excretion
1 Pradaxa SmPC 2009 Connolly SJ et al N Engl J Med 20093611139-1151 2 Stangier J et al Clin Pharmacokinet 20082847ndash59 3 Stangier J Clin Pharmacokinet 200847285-295 4 Stangier J et al Br J Pharmacol 200764292ndash303 5 Blech S et al Drug Metab Dispos 200836386-399 6 Stangier J et al J Clin Pharmacol 200545555-563
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
RE-LY Largest AF Outcomes Trial
PROBE study design18113 patients randomised during 2 years 951 centres in 44 countries12
50 of enrolled patients naiumlve to previous oral anticoagulantMedian treatment duration 2 years
10
RE-LY Randomized Evaluation of Long-term anticoagulant therapy
ESC = European Society of Cardiology
1 Ezekowitz MD et al Am Heart J 2009157805ndash10 2 Connolly SJ et al N Engl J Med 20093611139ndash51
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
RE-LY Study Design
Primary objective to establish the noninferiority of dabigatran to warfarin Minimum 1 year follow-up maximum of 3 years and median of 2 years of follow-up
AF with ge1 risk factorAbsence of contraindications
R
Dabigatran110 mg BID
n = 6000
Warfarin1 mg 3 mg 5 mg
(INR 20ndash30)n = 6000
Dabigatran150 mg BID
n = 6000
Severe heart-valve disorder stroke le14 days or severe stroke le6 months before screening increased haemorrhage risk creatinine clearance lt30 mLmin active liver disease pregnancy BID = twice daily INR = international normalized ratio
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
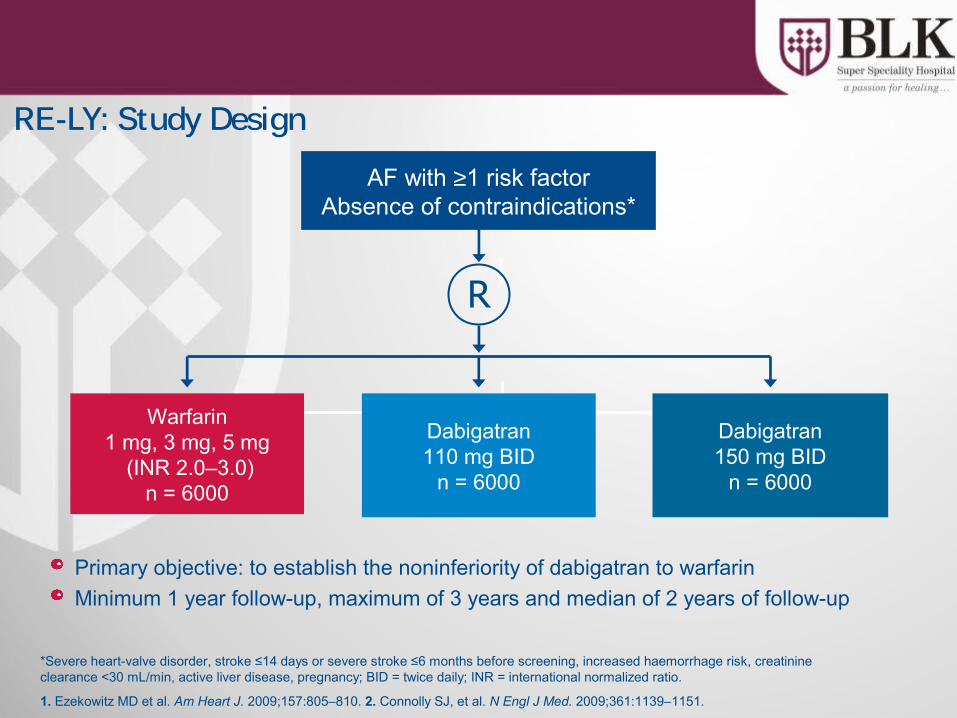
Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
1 Ezekowitz MD et al Am Heart J 2009157805ndash810 2 Connolly SJ et al N Engl J Med 20093611139ndash1151
Exclusion criteria
1 Severe heart-valve disorder2 Stroke within 14 days or severe stroke within 6 months before screening3 Any condition that increases the risk of haemorrhage4 Creatinine clearance lt30 mLmin5 Active liver disease6 Pregnancy
Inclusion criteria1 Documented AF2 One additional risk factor for stroke
bull History of previous stroke transient ischaemic attack or systemic embolismbull LVEF less than 40bull Symptomatic heart failure NYHA Class II or greaterbull Age of 75 years or morebull Age of 65 years or more and one of the following additional risk factors diabetes mellitus
coronary artery disease or hypertension
Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Data on file
Patients with Valvular Heart Disease were Included in RE-LY
DE 110 mg BIDn ()
DE 150 mg BIDn ()
Warfarinn ()
Totaln ()
Valvular heart disease 1288 (1000) 1353 (1000) 1303 (1000) 3944 (1000)
Aortic stenosis 152 (118) 163 (120) 156 (119) 471 (119)
Aortic regurgitation 264 (204) 281 (207) 272 (208) 817 (207)
Mitral stenosis 77 (59) 62 (45) 54 (41) 193 (48)
Mitral regurgitation 1035 (803) 1050 (776) 1016 (779) 3101 (786)
Other 470 (364) 496 (366) 492 (377) 1458 (369)
Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Incidence of Stroke or Systemic Embolism
RR 065 (95 CI 052ndash081)
Stro
kes
yste
mic
em
bolis
m (
yr)
Eventsn
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiority
Connolly SJ et al N Engl J Med 20103631875ndash1876
1836015 1346076 2026022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin00
03
06
09
12
15
18
154
111
171Plt001 (Sup)
Plt001 (NI)RR 090 (95 CI 074ndash110)
RRR35
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Phase III RE-LY Time to First Stroke or Systemic Embolism
BID twice daily NI non-inferiority RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
Years00 05 10 15 20 25
001
002
003
005
004
Cum
ulat
ive
haza
rd ra
tes
000
Warfarin
Dabigatran 110 mg BID
Dabigatran 150 mg BID
RR 090(95 CI 074ndash110)Plt001 (NI)P = 30 (Sup)
RR 065(95 CI 052ndash081)Plt001 (NI)Plt001 (Sup)
RRR35
Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Time to First Haemorrhagic Stroke
FDA Briefing Document Dabigatran etexilate 2010
Time from randomisation (months)
Cum
ulat
ive
haza
rd ra
tes
0015
0014
00130012
00110010
0009
00080007
00060005
0004
00030002
00010000
0 3 6 9 12 15 18 21 24 27 30 33 36 39
WarfarinDabigatran 110 mg BIDDabigatran 150 mg BI D
RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

RE-LY SAFETY RESULTS
150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

150 mg BID no Difference vs Warfarin for Major Bleeds
00
05
10
15
20
25
30
35
40
Maj
or b
leed
ing
(y
r)
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiorityConnolly SJ et al N Engl J Med 20103631875ndash1876
3426015 3996076 4216022
RR 080 (95 CI 070ndash093)
P = 003 (Sup) RR 093 (95 CI 081ndash107)
P = 32 (Sup)RRR20
287
332357
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
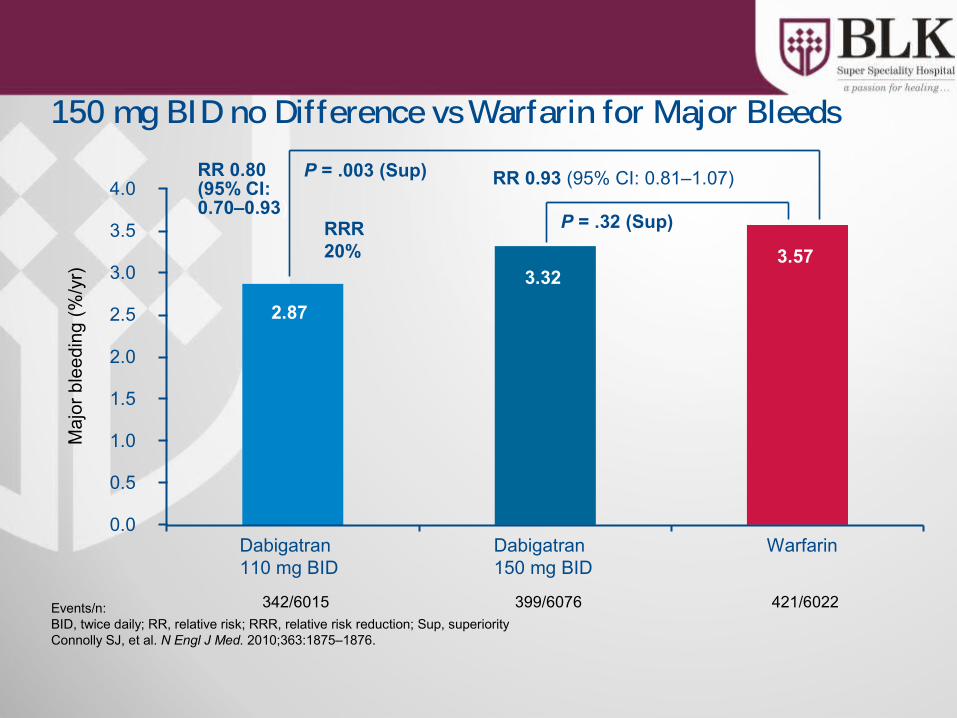
Error bars = 95 CI BID twice dailyConnolly SJ et al N Engl J Med 20103631875ndash1876
Dabigatran110 mg BIDvs warfarin
Dabigatran150 mg BIDvs warfarin
050 075 100 125 150
lt001
lt001
SuperiorityP value
30
lt001
Non-inferiorityP value
Hazard ratioM
argi
n =
146
Phase III RE-LY Risk of Stroke or Systemic Embolism
EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

EventsnBID twice daily RR relative risk RRR relative risk reduction Sup superiority
276015 386076 906022
Dabigatran110 mg BID
Dabigatran150 mg BID
Warfarin0
06
09
Intra
cran
ial b
leed
ing
(y
r)
08
07
05
04
03
02
01023
032
076
RR 030(95 CI 019ndash045)
Plt001 (Sup)RR 041 (95 CI 028ndash060)
Plt001 (Sup)
RRR70
RRR59
Significantly Lower Intracranial Bleeding with Dabigatran
Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Time to first event of
Annual rate
HR (95 CI) D110 D150
ICH stoke SEE 16 13
Life threatening bleed stroke SEE 2524
Major bleed stroke SEE 41 41
D150 Better D110 Better06 08 10 12
CRDAC meeting 92010FDA Beasley
Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
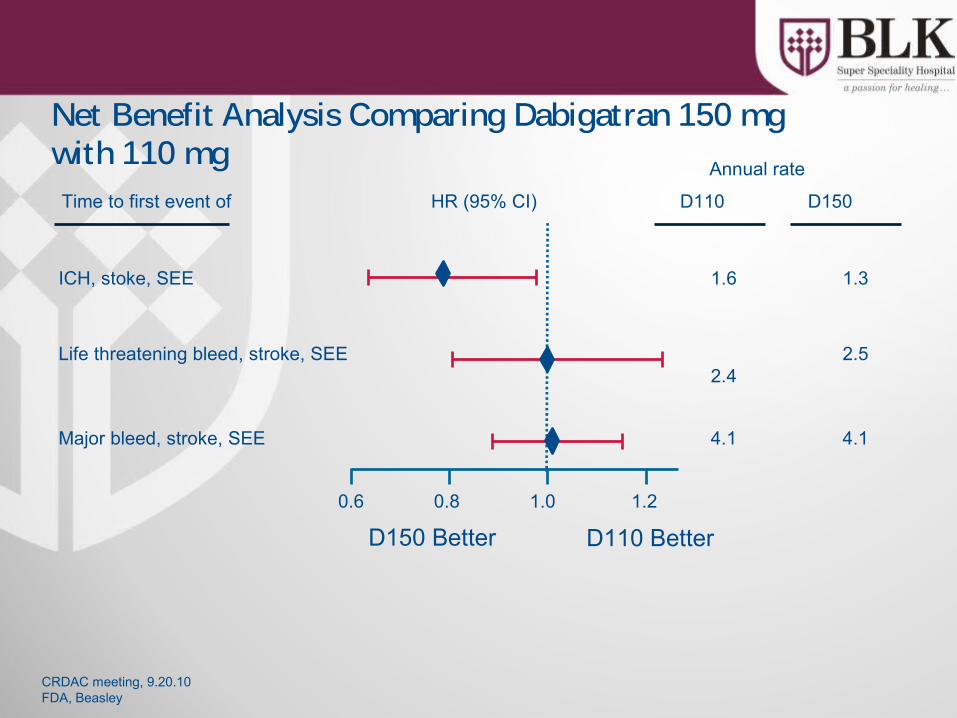
110 mg BID DosemdashWhich Patients
gt 75 years Patients with higher risk of bleeding includingndash Moderate renal impairment (30ndash50 mLmin CrCl)ndash P-glycoprotein-inhibitor co-medicationndash ASA NSAID clopidogrelndash Congenital coagulation disordersndash Active ulcerative GI diseaserecent GI bleedndash Recent intracranial haemorrhage
00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

00Hazard ratio
Meta-analysis of ischaemic stroke or systemic embolismFavourswarfarin
Favoursother treatment
Warfarin vs
Placebo
20
Low-dose warfarin
05 10 15
Aspirin
Ximelagatran
Dabigatran 150 mg BID
Aspirin + clopidogrel
Dabigatran 110 mg BID
RE-LY in Perspective
Error bars = 95 CI BID = twice daily
Adapted from Camm J ESC 2009 oral presentation 182 Lip GYH amp Edwards SJ Thromb Res 2006118321ndash33
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
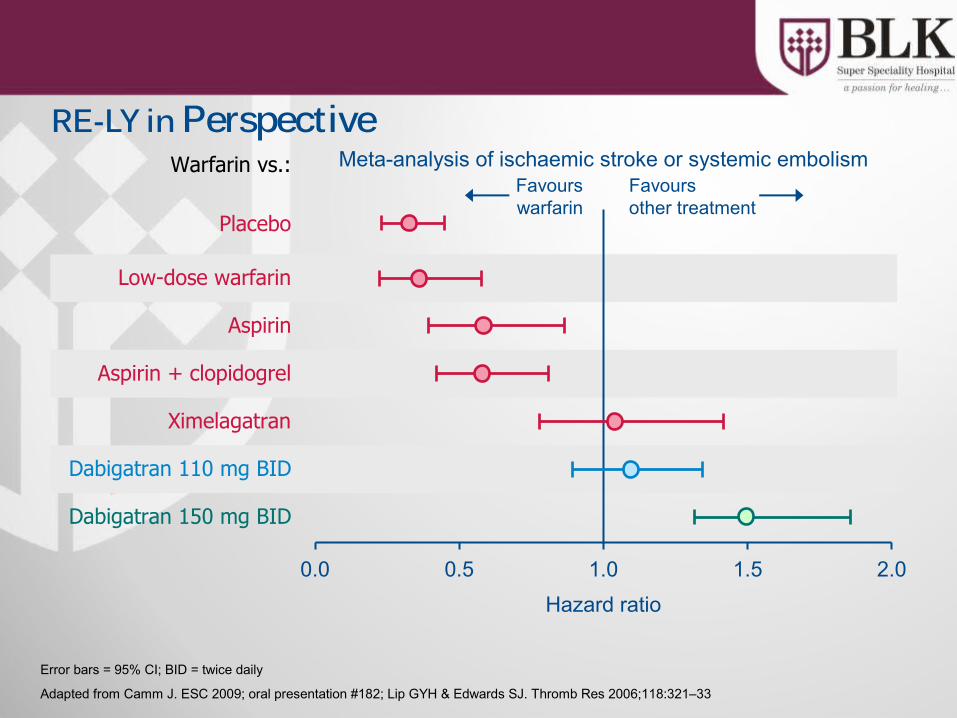
25
The Newer Anticoagulants on the Horizon
TrialDrug Dose Comparator N CHADS2
score
RE-LY Dabigatran 150 mg and 110 mg
BID
Warfarin(INR 20ndash30)
18000 gt0
ROCKET-AF56 Rivaroxaban 20 mgOD
Warfarin(INR 20ndash30)
14000 ge2
AVERROES34 Apixaban 5 mgBID
Aspirin (81ndash324 mg OD)
6000 ge1
ARISTOTLE12 Apixaban 5 mgBID
Warfarin(INR 20ndash30)
18000 ge1
ENGAGE-AF TIMI 487
Edoxaban 30 mg OD60 mg OD
Warfarin(INR 20ndash30)
16500 ge2
Adjusted based on renal function BID twice daily INR international normalised ratio OD once daily
Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
Dabigatran Rivaroxaban Apixaban
US Approved Submitted Submitted
Canada Approved Submitted Submitted
Europe Approved on August 4 2011
Submitted Submitted
Asia Pacific(Philippines Japan Indonesia Singapore Korea Malaysia)
Approved
Current as of June 10 2011AVERROES Trial
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
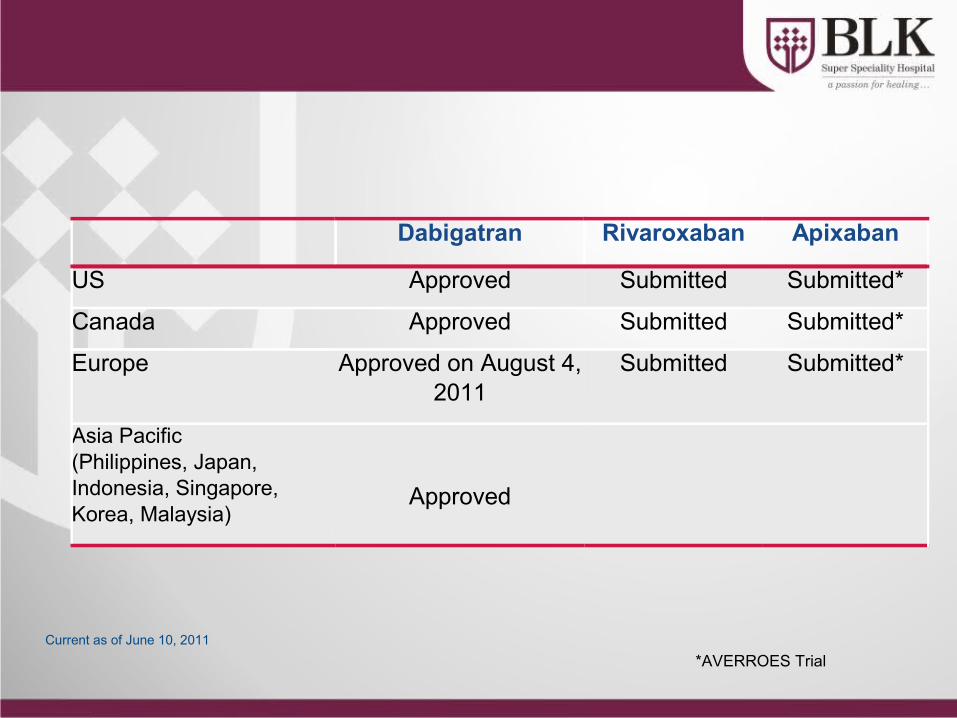
Dabigatran vs Warfarin RiskBenefit by Dose
Adapted from Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6
110 mg BID 150 mg BID
darr Haemorrhagic
stroke
darr Total amp life-threatening bleeds ICH
darrstrokesystemic embolism
darr Major bleeds
darr Vascular mortality
darr Ischaemic stroke
Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Conclusions
Dabigatran etexilate has been shown to concurrently reduce both thrombotic and haemorrhagic events Both doses of dabigatran provide different and complementary advantages over warfarinndash 150 mg BID has superior efficacy with similar bleedingndash 110 mg BID has significantly less bleedings with similar efficacyndash Similar net clinical benefit was seen between the two dabigatran doses
Dabigatran demonstrates high efficacy and safety in a variety of clinically relevant populations
BID = twice daily INR = international normalized ratio
Connolly SJ et al N Engl J Med 20093611139ndash51 Connolly SJ et al N Engl J Med 20103631875ndash6 Wallentin L et al Lancet 2010376975ndash83
TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

TicagrelorNew Antiplatelet Therapy
What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

What is it
bull Ticagrelor is an oral adenosine diphosphate antagonist which blocks ADP-induced platelet aggregation
bull Ticagrelor exhibits rapid onset and offset of action with reversible binding
bull Ticagrelor treatment is recommended for up to 12 months
When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

When should it be used
bull Ticagrelor is indicated for the prevention of atherothrombotic events (Cardiovascular death MI and stroke) in all patients with Acute Coronary Syndrome (ACS) regardless of mode of therapy Medical or Interventional vis a vis Prasugrel ( only approved for ACS undergoing PCI)
bull Based on PLATO trial latest ESC guideline give Class I A recommendation in ACS
Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Bioabsorbable stent
The 4th Stephellip
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Balloon Angioplasty
Bare metal Stent Drug Eluting Stent
Decade 1980s 1990s 2000s
Acute Success rate 70-85 gt95 gt95
Restenosis 40-45 20-30 lt10
Early Thrombosislt30 days
3-5 1-2 1-2
Late Thrombosisgt30 days
NA lt05 1
Very Late Thrombosis (gt1y)
NA asymp0 06per yr
Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Igaki- Tamai Bioabsorbable Stentbull Igaki- Tamai Bioabsorbable Stent (Igaki Medical Planning Company Kyoto
Japan) the first absorbable stent implanted in humans is constructed from Poly-L-Lactic acid (PLLA)
bull In the absorption process hydrolysis of bonds between repeating lactide units produce Lactic acid that enters Krebs cycle and is metabolized to Carbon di-oxide and water
bull Stent Design- Zig Zag helical coil with straight bridges
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
Bioabsorbable Magnesuim Stentbull The first bioabsorbable stent implanted in humans is the Magnesium alloy
stentbull This stent laser cut from tubular magnesium WE-43
(BiotronikBerlinGermany) has sinusoidal in-phase hoops linked by straight bridges
bull It is a Balloon expandable stent and absorption is by surface erosion such that the strut thickness is decreased as the stent is absorbed
REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

REVA Bioabsorbable Stentbull The REVA (Reva Medical Inc San Diego Calif) stent is constructed
from an absorable tyrosine-derived polycarbonate polymer that metabolizes to amino acids ethanol and carbon di-oxide
bull It is a balloon expandable with a slide and lock (ratchet) design
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
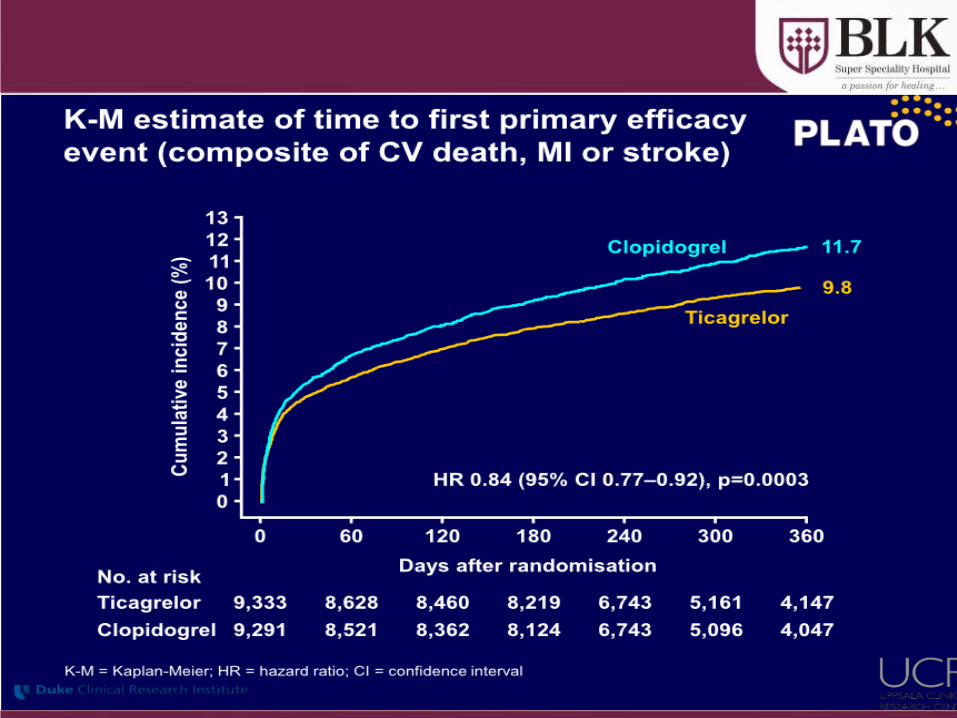
Bioabsorbable Therapeutics Stentbull The Bioabsorbable therapeutics stent (Bioabsorbable Therapeutics Inc
Menlo Park Calif) a fully bioabsorbable sirolimus-eluting stent that also releases salicylic acid
bull It has a polymer backbone that gives the stent the physical structure and a polymer coating that contains and controls the release of the anti-proliferative agent
bull During absorption the bonds between salicylic acid and linked molecules are hydrolyzed releasing the anti-inflammatory drug salicylic acid
BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

BVS Everolimus-Eluting Bioabsorbable PLLA Stent
bull The BVS everolimus eluting stent (Abbott Vascular Santa Clara Calif)bull The stent has a bioabsorbable polymer backbone of PLLA with a polymer
coating of Poly-DL-lactide that contains and controls the release of the anti-proliferative drug everolimus
bull Stent Design- Revision10 has circumferential out of phase zig zag hoops linked either directly or by straight links Revision11 has circumferential in phase zig zag hoops linked by straight links
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
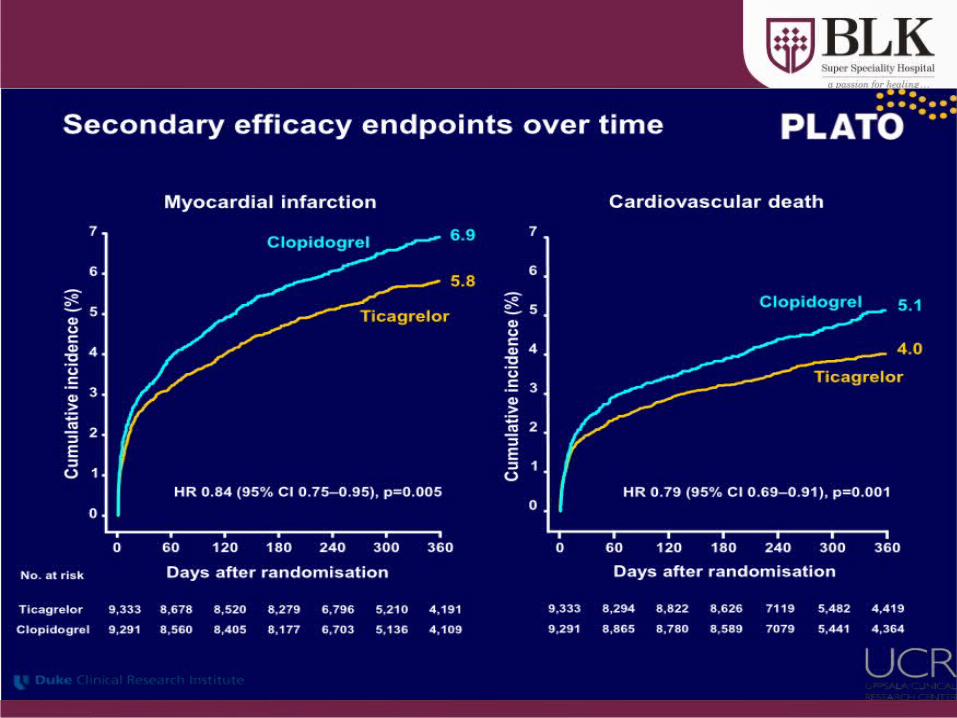
SE2935049 Rev B Information contained herein intended for healthcare professionals from outside the US only
Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
bull Restoration of epicardial coronary capacitance to coronary flow regulation
bull Restoration of shear stress modulation and flow mediated dilation vital for the direct coupling of coronary flow to metabolic demand
bull Minimize chronic flow separations (turbulence) and low endothelial shear stress (ESS) due to protruding struts and or vessel distortion
bull Abolition of stress ldquoshieldingrdquo and negative influences of endothelial and SM cell function
bull Reduce risk of late events or atheroprogression (all other factors controlled)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Poly Lactide - Hydrolysis
Lactide
PLAPLA
darr Molecular Weight
H2O
Hydrolysis
Mass Loss
Krebs Krebs CycleCycle
Mass Transport
CO2 + H2O
RO
RprimeOH2O+ R
ORprime
OHHO+
carboxylic acid alcohol
PLA ndash Poly Lactic Acid
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Bioresorbable Polymer ABSORBbull EverolimusPDLLA Matrix
Coatingbull Thin coating layerbull Amorphous (non-crystalline)bull 11 ratio of EverolimusPLA
matrixbull Conformal Coating 2-4 microm
thickbull Controlled drug release
bull PLLA Backbonebull Highly crystallinebull Provides device integritybull Processed for increased radial
strength
Polymer backbone
Drugpolymer matrix
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
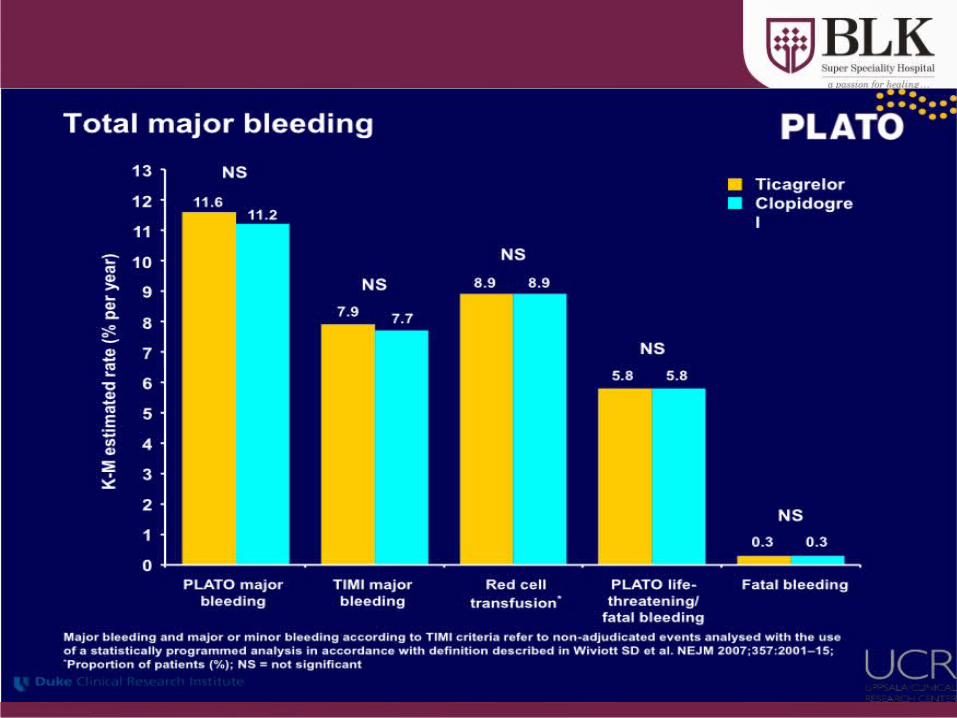
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
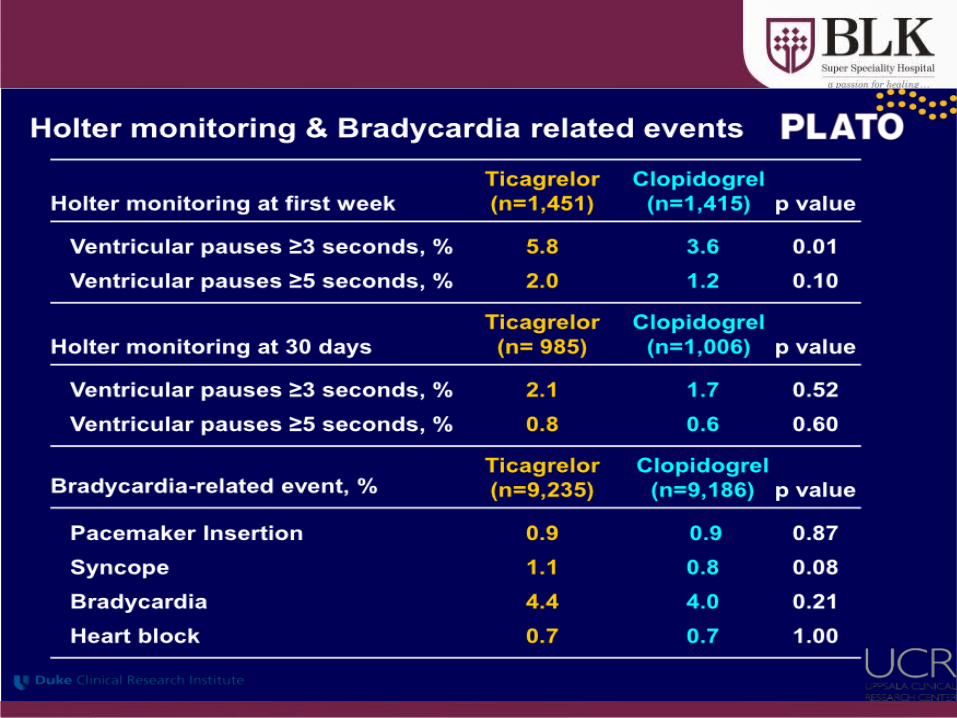
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
Clinical Study Design ndash Cohort ASingle
de-novo lesion30 mmn = 30
bull Sponsor Abbott Vascular
bull Prospective open label bull PI John Ormiston MD
Patrick Serruys MD PhD
bull DSMB J Tijssen PhD T Lefegravevre MD P Urban MD
bull CEC C Hanet MD D McClean MD V Umans MD
bull Angiographic and IVUS corelab Cardialysis (Rotterdam NL)
BVS Device
bull 30 x 12mm device
bull 6 sites EU NZRotterdam NL Patrick Serruys Krakow PL Dariusz Dudek Auckland NZ John Ormiston Aarhus DN Leif Thuesen Aalst BE Bernard de BruyneSt Denis F Bernard Chevalier
bull Post-procedure clopidogrel for 6 months aspirin for 5 years
(30 x 18mm device available after enrolment start and used in 2 patients)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C58
ABSORB Long term follow-up
ABSORB Cohort A Clinical Results at Each Phase Intent to TreatRESTORATION RESORPTION
Hierarchical 6 Months30 Patients
12 Months29 Patients
24 Months29 Patients
60 Months29 Patients
Ischemia Driven MACE 1 (33) 1 (34) 1 (34) 1 (34)
Cardiac Death 0 (00) 0 (00) 0 (00) 0 (00)
MI 1 (33) 1 (34) 1 (34) 1 (34)
Q-Wave MI 0 (00) 0 (00) 0 (00) 0 (00)
Non Q-Wave MI 1 (33) 1 (34) 1 (34) 1 (34)
Ischemia Driven TLR 0 (00) 0 (00) 0 (00) 0 (00)
by PCI 0 (00) 0 (00) 0 (00) 0 (0)
by CABG 0 (00) 0 (00) 0 (00) 0 (0)
Same patient ndash this patient also underwent a TLR not qualified as ID-TLR (DS = 42) One patient missed the 9 12 18 month and 2 3 and 4 year visits one patient died from a non-cardiac cause 706 days post procedure MACE ndash Composite endpoint comprised of cardiac death myocardial infarction (MI) and ischemia-driven target lesion revascularization (TLR) by PCI or CABG
5-Year Clinical Results
Serruys PW TCT 2011
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
59
ABSORB Scaffold Thrombosis Out to 5 Years
Thrombosis Results Through All Phases
Time Patients N
Acute (lt1 day) 0 (00) 30
Sub-Acute (1-30 days) 0 (00) 30
Late (gt30 days ndash 1 year) 0 (00) 29
Very Late (gt1 year) 0 (00) 29
Cohort A5-Year Clinical Results
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
69
75∆ 06
393-day HR093 [038224]
p=08678
B V S ( B 1 + B 2 )X V ( S P I + S P I I + S P I I I R C T )
MA
CE
(C
-De
ath
MI
ID-T
LR
)
00
50
100
150
200
250
T i m e P o s t I n d e x P r o c e d u r e ( M o n t h s )
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
XV Includes only patients with single 30 x 18mm stent
BVS Includes all patients
KM estimate of MACE rate in patients treated with BVS (Absorb Cohort B n=101) vs patients treated
with a single 3x 18 mm metallic EES (Spirit I+II+III n=227)
Patients at risk 0 days 37 days 194 days 284 days 365 days 393 days
BVS(B1+B2)101 99 96 96 95 94
XV(SPI+SPII+SPIII RCT)227 224 219 211 209 208
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
ABSORB Extendbull N = up to 1000 patients at up to 100 sites
(Europe Australia New Zealand)Device sizesndash 25 amp 3 x 18 amp 28 mm ndash Lesion length treatable le 28 mm
bull Clinical follow up onlyndash ID-MACE ID-TVF ID-TLR ID-TVR lsquostentrsquo
thrombosisndash 30 days 6 months and annually 1-3 years
(overlap of two 18 mm long devices also permitted)
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C 62
First ABSORB EXTEND Follow-up
Patient was treated with a metallic DES not ABSORB
6-Month Clinical Results in the first 200 patients
Abizaid A TCT 2011
ABSORB Extend Clinical Results ndash Intent to Treat
30 Days 6 Months
Non-hierarchical N = 200 N = 200
Cardiac Death (n) 0 05 (1)
Myocardial Infarction (n) 20 (4) 20 (4)
Q-wave MI 10 (2) 10 (2)
Non Q-wave MI 10 (2) 10 (2)
Ischemia driven TLR (n) 05 (1) 05 (1)
CABG 0 0
PCI 05 (1) 05 (1)
Hierarchical MACE (n) 20 (4) 25 (5)
Hierarchical TVF (n) 20 (4) 30 (6)
One additional ischemia driven non-TL TVR treated by CABG
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
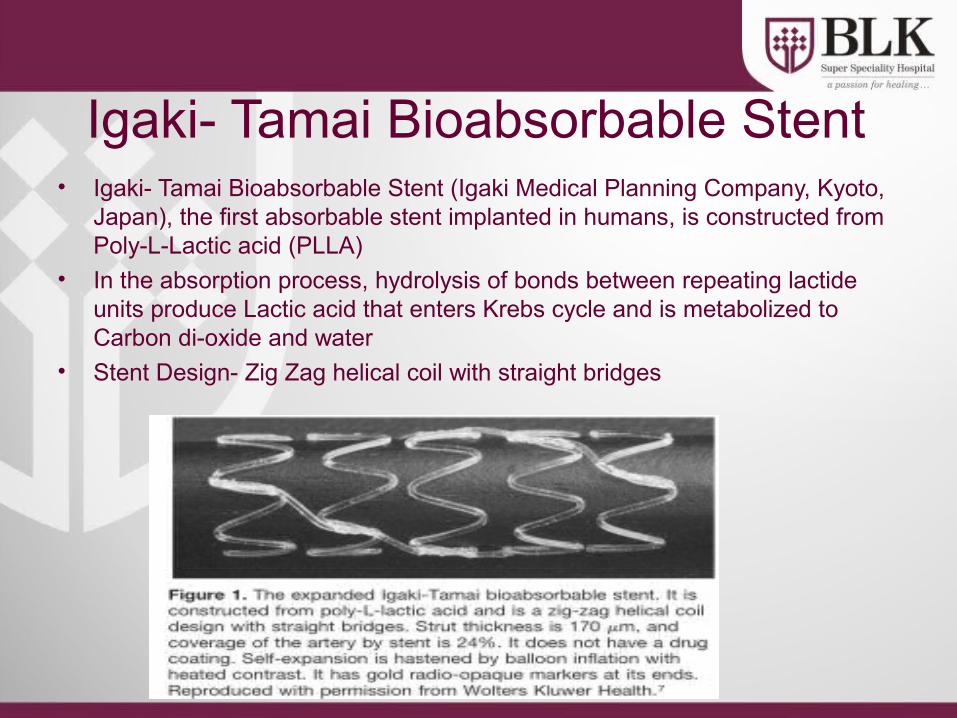
copy 2009 Abbott Laboratories
Pipeline product Currently in development at Abbott Vascular Not available for sale
SE 2928803 Rev C
So farhellipbull Bioabsorbable active stent keeps promise
ndash As good as DESndash Positive effect on late healing (vasoreactivity
conformability positive remodeling no trigger for neo-atherosclerosis)
bull A slow amp relatively long resorption process is necessary to obtain these results
bull Future trials are mandatory to evaluate the role of this technology
Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Trans-catheter Aortic Valve Implantation (TAVI)
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
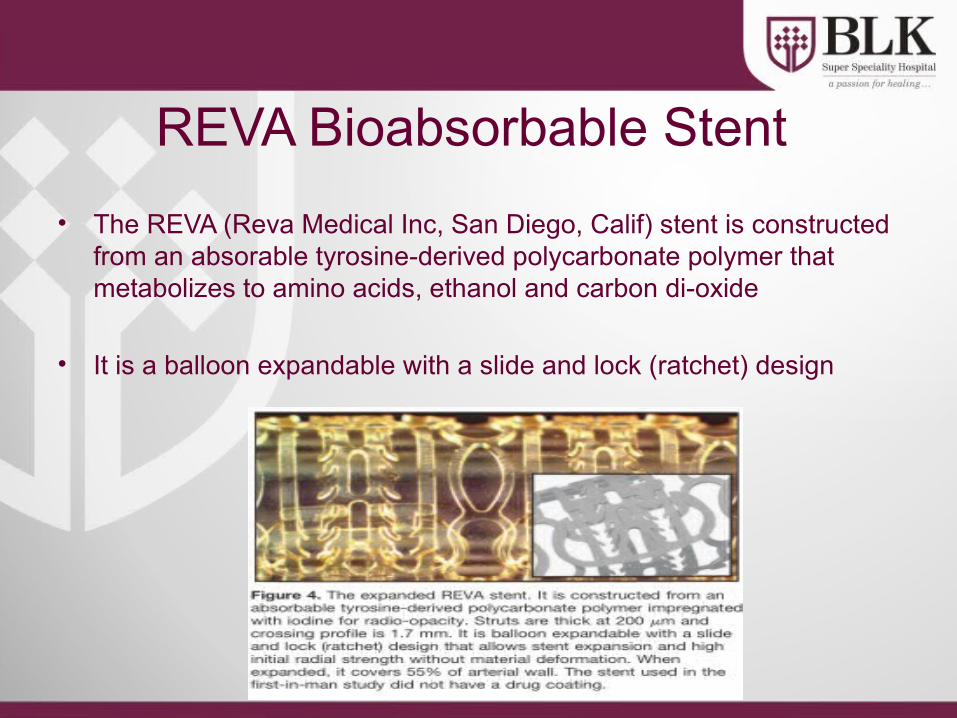
TAVIbull Potentially life-saving therapy for patients unsuitable for
conventional aortic valve replacementbull No longer regarded as experimentalbull At the end of 2009 c 8000 valves were implanted world-
widebull 2 major competitors
ndash Medtronic Core-Valvendash Edwards Sapien
bull 3 methods of implantationndash Trans-arteriallyndash Trans-apicallyndash Subclavian approach
ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

ldquoSurgical intervention should be performed promptly once evenhellip minor symptoms occurrdquo1
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)
1 CM Otto Valve Disease Timing of Aortic Valve Surgery Heart 2000
Chart Ross J Jr Braunwald E Aortic stenosis Circulation 196838 (Suppl 1)61-7
Valvular Aortic Stenosis in Adults(Average Course)
Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Mortality in Aortic Valve ReplacementMortality in Aortic Valve Replacement
Burr et al Annals Thor Surg 199560S264-269
n = 1984n = 1984
What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

What is the risk
bull Initial mortality approximately 10bull Improving
ndash Core valve May 2008 30 day mortality = 8 in first 1000 European implants
ndash Edwards May 2009 30 day mortality = 63 for TAVI and 103 for trans-apical in 1038 patients
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
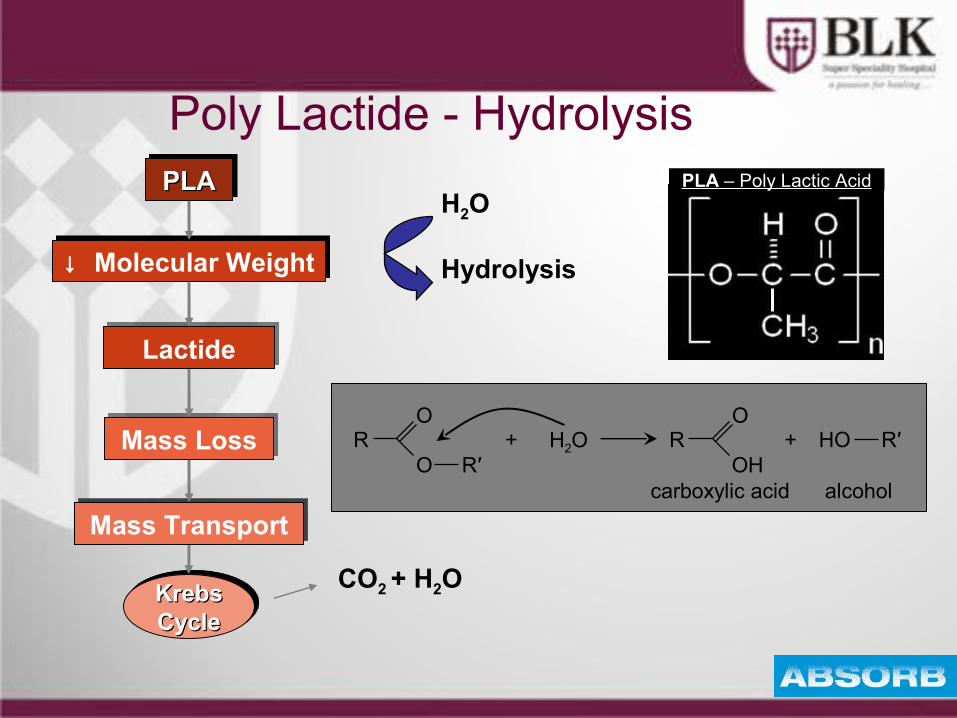
Landmark PARTNER TRAIL
Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Baseline Characteristicsof the patients and Echocardiographicfindings
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
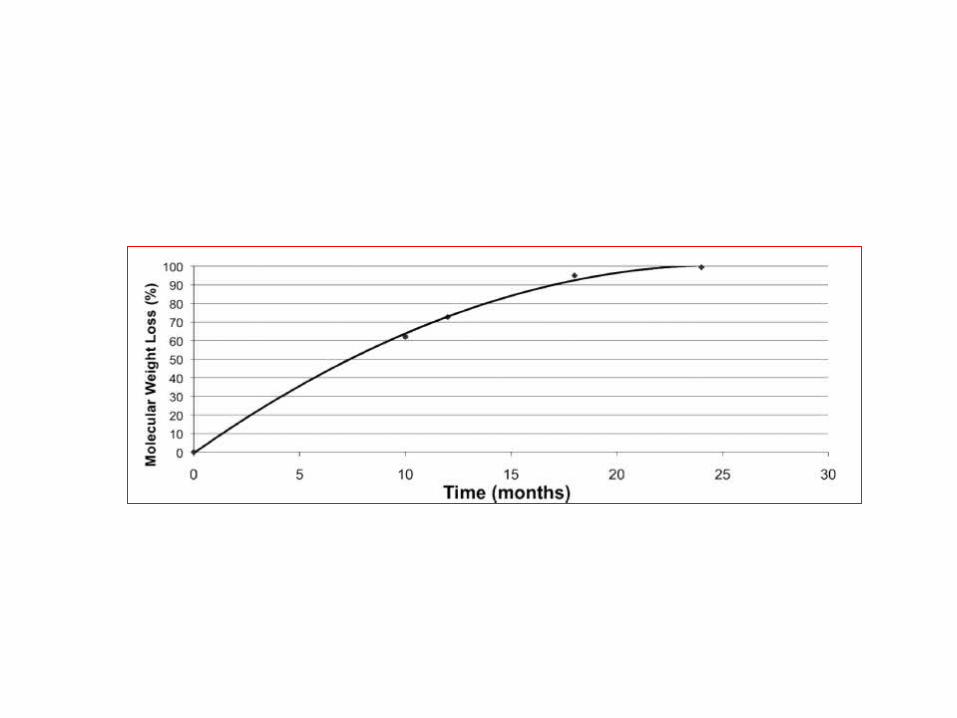
Primary End Point
Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Relative risk and95 Confidence Intervals are shown for the primaryend point of deathfrom any cause at1 year among patients randomly assigned toTAVI
Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Vitamin Da Novel Cardiovascular risk factor
Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Backgroundbull Vitamin D has been traditionally known as
anti-ricketic factor or sunshine vitaminbull Vitamin D is unique because it is synthesized
by the body and it functions as a hormonebull Besides its pivotal role in calcium homeostasis
and bone mineral metabolism evidences link Vitamin D with chronic diseases like Diabetes Hypertension Myopathic disorder infections autoimmune disorder and cancer
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
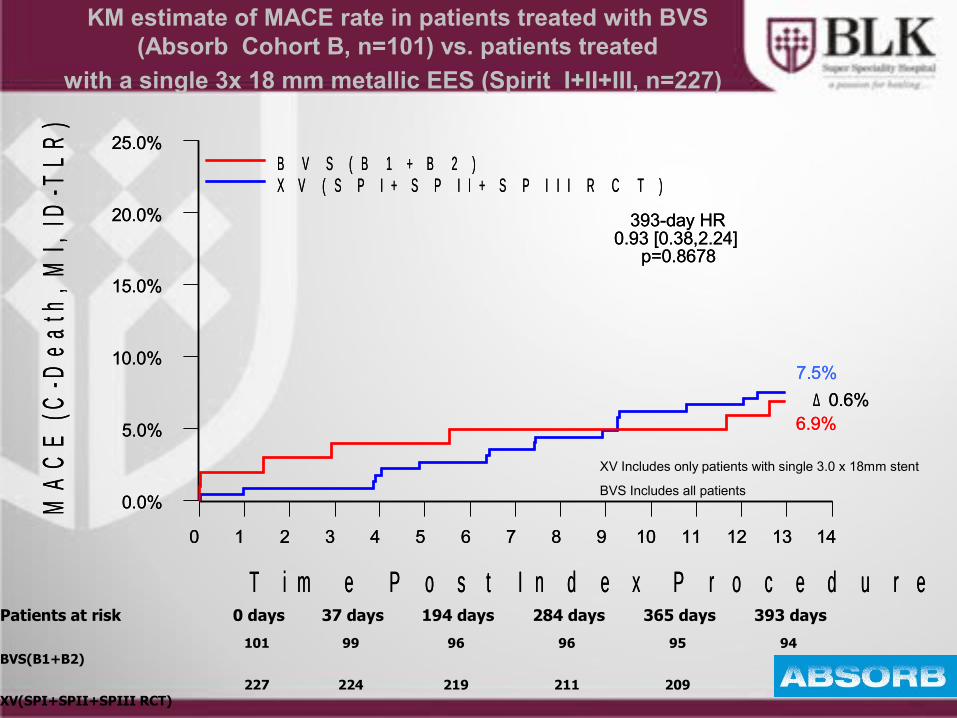
Different forms of Vitamin DCholecalciferol ndash
bull naturally occurring form bull made in large quantities in skin when
exposed to sunlight (UVB rays 290 - 310 nm)
bull Cholecalciferol transported to liver metabolized into calcidiol
Calcidiol (25-hydroxyvitamin D) ndashbull Prehormone storage form of vit D bull Serum 25(OH)D-reliable indicator of vit D
adequacy Tested routinely for vit D deficiency
Calcitriol (125- dihydroxyvitamin D) ndashbull made from calcidiol in kidneys and other
tissues
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
JAPI 2009 57 40-48
Vitamin D status in India
bull Vitamin D deficiency is epidemic in Indiabull Studies have documented low 25(OH)D level
in the Indian population despite abundant sunshine
bull Low dietary Vitamin D intake is also been documented
bull Prevalence varying from 50-100
Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Why does this happen
bull Dress codebull Changing lifestylesbull Urban- less sun exposurebull Avoiding the sunbull Sunscreensbull Dark skinbull Rural- less calciumVit D intake other risk factors obese drug intake malabsorption
Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Location N Study population Age (Yrs) 25(OH)D Unit
Delhi1 40 Indian Paramiltary forces - Men 20 ndash 30 184 + 53 ngml
Delhi1 50 Indian Paramiltary forces - Women
20 ndash 30 253 + 74 ngml
Delhi2 32 Rural Males 428 + 166 442 + 244 nmoll
Delhi2 32 Rural females 434 + 126 269 + 159 nmoll
1 Tandon N et al Natl Med J India 200316298-3022 Goswami R et al J Assoc Physicians India 200856755-57
Indian Studies Vitamin D status in Middle age group (20-45 years)
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
Diagnostic Criteria for Vit D deficiency
bull 25 (OH) is major circulatingstorage form of Vitamin D longer T12 than 125 (OH) Vit D
bull Measurement of 25(OH)D limited by methodological differences overcome by RIAbull Currently available assays ndash antibodies co-specific to both 25(OH)D2 and
25(OH)D3 terminology 25(OH)D assays usedbull Conversion ngmL to nmolL ndash multiply by 2496 bull nmolL to ngmL ndash divide by 2496
Condition nmoll ngml
Normal 75 ndash 80 30 -32
Insufficiency 20 ndash 75 8 -30
Deficiency lt 20 lt 8
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
Sources of Vitamin D in Indiabull Diet is a poor source ndash average Indian dietary
intake is low (lt100 IUd)bull Food supplementation with vitamin D is limitedbull Exposure to sunlight ndash a balance between
adequate exposure to increase serum vitamin D or increasing risk of skin cancer is required
bull Vitamin D supplements ndash 1000 IU (D3) or cod liver oil capsules 400 - 800 IU (D3 and vitamin A)
What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

What is adequate supplementation What is adequate supplementation in the Indian context in the Indian context
Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Vitamin D conversion to 25(OH)D
bull 1000 IU per day of Vitamin D(3) on daily basis increases circulating 25(OH)D by 1ngml after 3 months
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
What is adequate supplementation in the Indian context
bull If typical serum 25 (OH)D level in Indians is 10 ngmlhellip
bull And if target serum 25 (OH)D level is 30 ngmlhellip
bull They would require about 2000 IUday
Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Down to the bone Medscape CME June 2007+ European Commission Opinion on tolerable upper intake levels of vit D 2002
Safety of Vitamin Dbull Doses of 5000-10000 IUday for 4-
5 months have not resulted in elevated serum or urinary calcium levels
bull Found to be safebull Upper tolerable limit of intake in
adults 2000 IUday
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
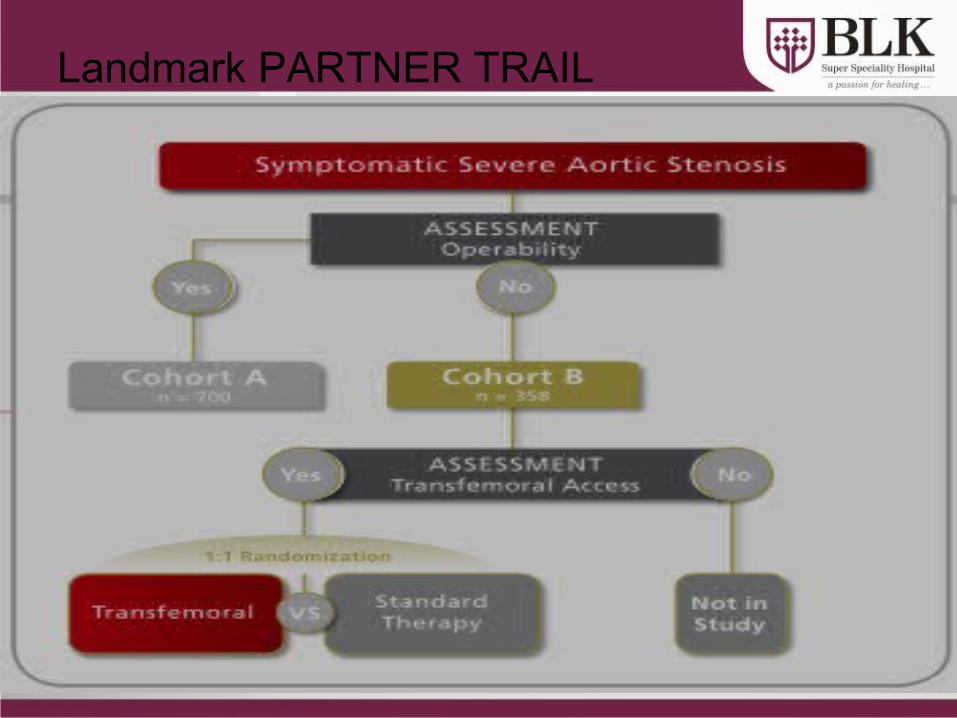
Curr Opin Clin Nutr Metab Care 200811(1)7ndash12
Vitamin D deficiency may be a contributor to the development of CVD potentially through
associations with diabetes or hypertension
Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
Low levels of vitamin D is found to be associated withbull Diabetes mellitusbull Metabolic syndromebull Obesitybull Hypertension bull Strokebull Congestive heart failure
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
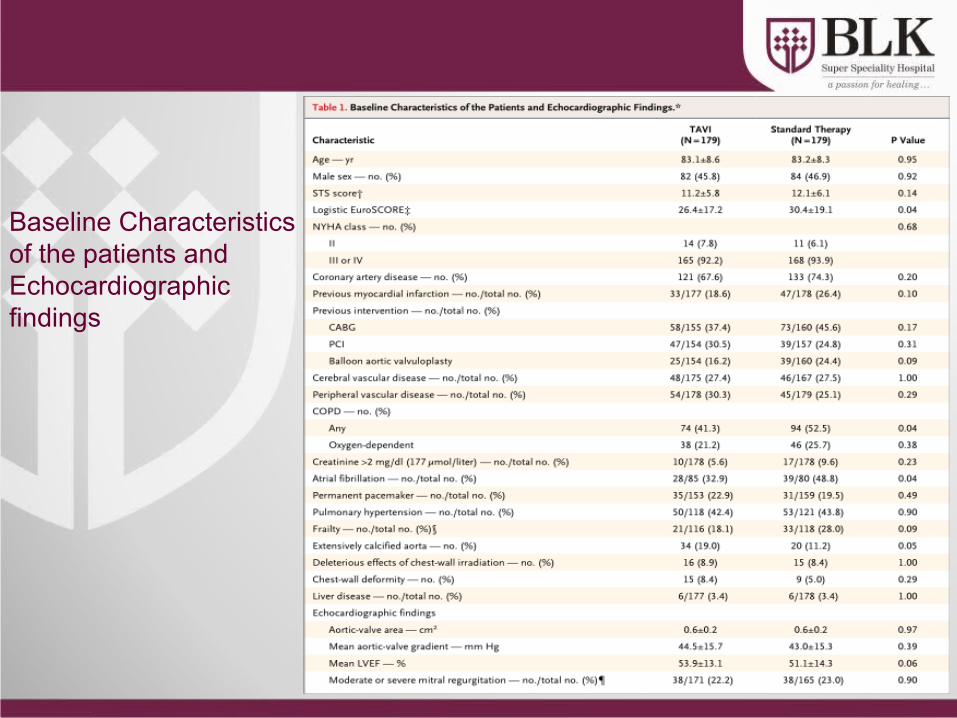
J Am Coll Cardiol 2008521949ndash1956
Vitamin D Deficiency
PTH
Atherosclerosis
Hypertension amp Hypertrophy Diabetes amp
Metabolic Syndrome
Adverse Cardiovascular Events
RAAS Inflammation
Insulin resistance+
Pancreatic Beta Cell Dysfunction
Potential Mechanisms for Diabetes amp CVDdue to Vitamin D Deficiency
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
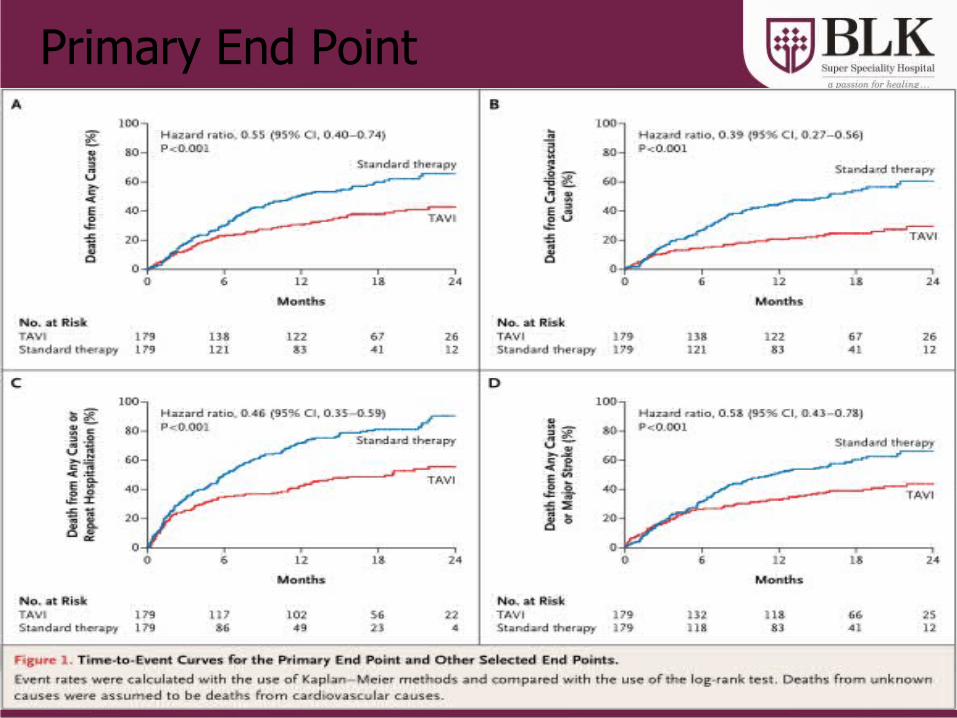
Role of Vit D in CVD CV risk factors
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
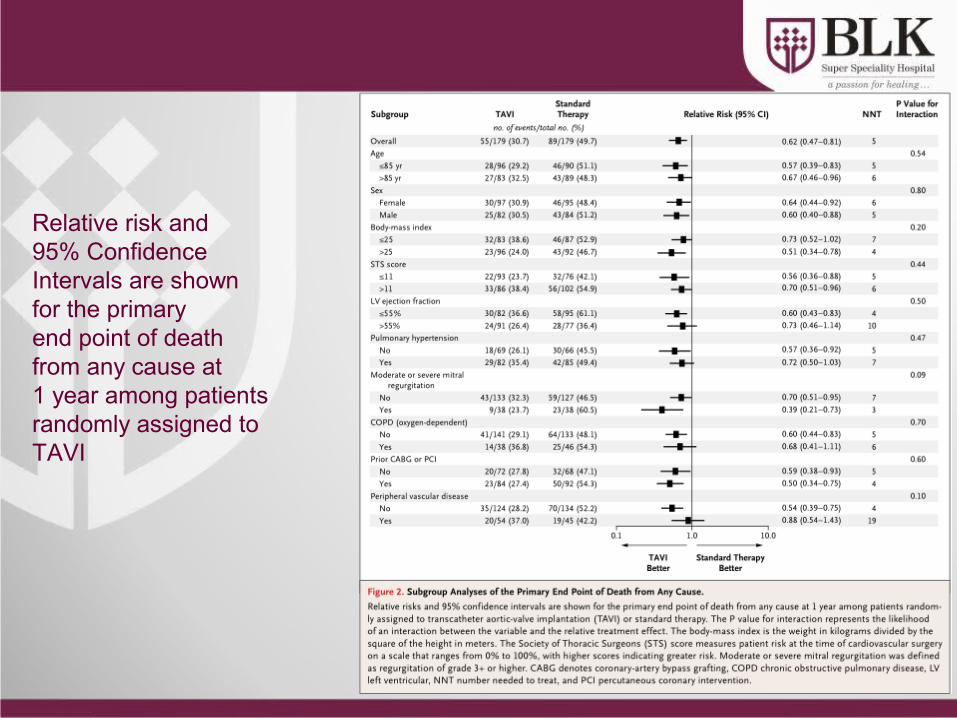
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Hypertension
bull Prospectively followed two cohortsndash Nursesrsquo Health Study ndash 1198 womenndash Health Professionals Follow-up Study ndash 613 men
bull Relative risk of hypertensionndash lt 15 ngmL vs gt 30 ngmL 25(OH)D ndash Men RR = 613ndash Women RR = 267
Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Hypertension
bull BP higher in winterbull BP higher with increasing latitudebull BP higher with darker skin pigmentationbull HTN pts given UV light treatments 3xweek for 6 weeks had Vit D level
increases of 162 and saw mild decreases in BPKrause et al Lancet 1998352(9129)709
bull Small doses of Vit D (800IU) for 8 weeks rarr decreased BP and pulse ratePfeifer et al J Clin Endocrinol Metab 200186(4)258
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
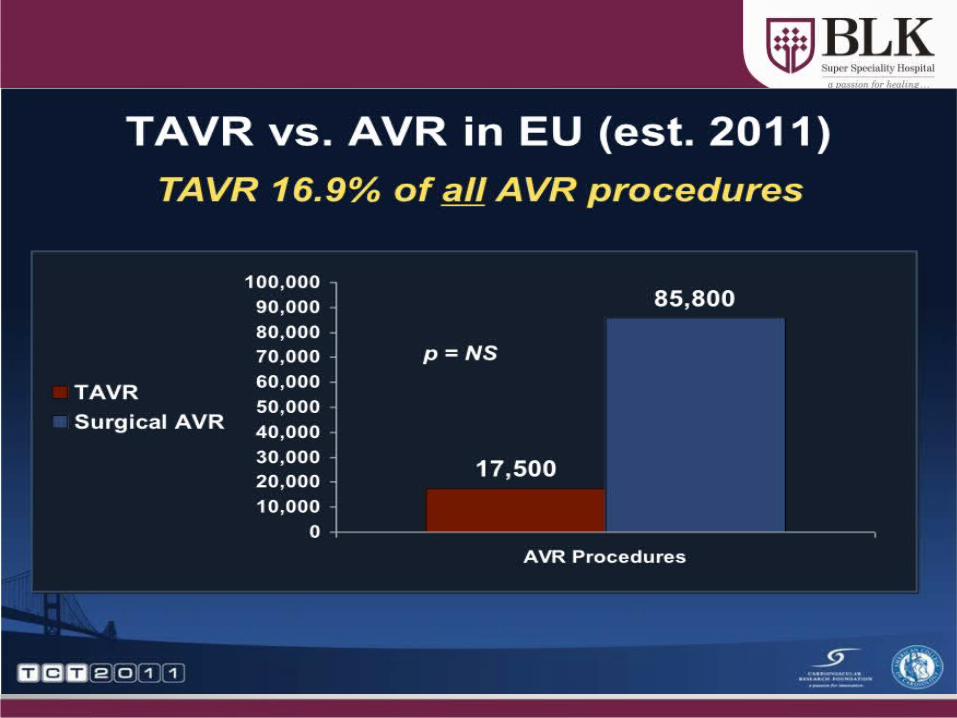
Wang et al Circulation 2008
Vitamin D deficiency and risk of CVD
bull 1739 Framingham study participants (MF)
bull Followed up for CV event-mean 54 yrs
bull 25(OH)D lt15 ngml vs gt15 ngml- RR162
bull Greater risk if 25(OH) D lt10 ngml
Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Giovannuci et al Arch Int Med 2008
25(OH)D and risk of MI in Men
bull Prospective 18225 men in Health Professionals follow up study 10 yr follow up
bull 25 (OH)D level lt15 ngml vs gt30 ngml- RR for MI 242
bull Greater risk even in the 15-30 ngml group ndash RR 143-16
Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Heart disease
bull MI risk doubles in pts with 25OHVitD levels lt34ngmlScragg et al Int J Epidemiol 199019(3)559
bull CHF pts have much lower 25OHVitD levels than controls
Zitterman et al J Am Coll Cardiol 200341105
bull Deaths from CAD more common in winterScragg Int J Epidemiol 198110(4)337
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
Mechanisms of Vit D in CVD prevention
bull Inhibition of vascular smooth muscle proliferation by an acute influx of Ca into the cells
bull Suppression of vascular calcification by uarrsing matrix Gla synthesis by chondrocytes amp vascular smooth muscle cells
bull Down-regulation of pro-inflammatory cytokines TNF-α and IL-6
bull Up-regulation of anti-inflammatory cytokines
bull Action of vit D as a negative endocrine regulator of the renin-angiotensin system
Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Polycystic Ovary SyndromeA study 120 untreated women with PCOS median age 28 yrs
ndash Low levels of vit D assoc with insulin resistance amp obesity ndash In all subjects conc of 25-OH-D inversely assoc with BMI body fat
HOMA-IR hyperinsulinemia amp levels of leptin while being positively assoc with HDL levels
bull Additional analysis found 25-OH-VD levels to be significantly correlated with SHBG and free androgen index
Hahn S Haselhorst U et al 2006 114(10) 577-583
Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Metabolic Syndromebull Third National Health amp Nutrition Examination Survey (NHANES III)
ndash 8421 men and non-pregnant women gt 20 yrs of age and had fasted gt 8 hrsbull Unadjusted prevalence of metabolic syndrome - 219bull After adjustments for known risk factors odds of metabolic syndrome decreased
progressively across increasing conc of 25(OH)Dbull Relative risk compared with bottom quintile of vitamin D level
ndash 2nd quintile ndash 085ndash 3rd quintile ndash 075ndash 4th quintile ndash 062ndash 5th quintile ndash 046
Ford et al 2005
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
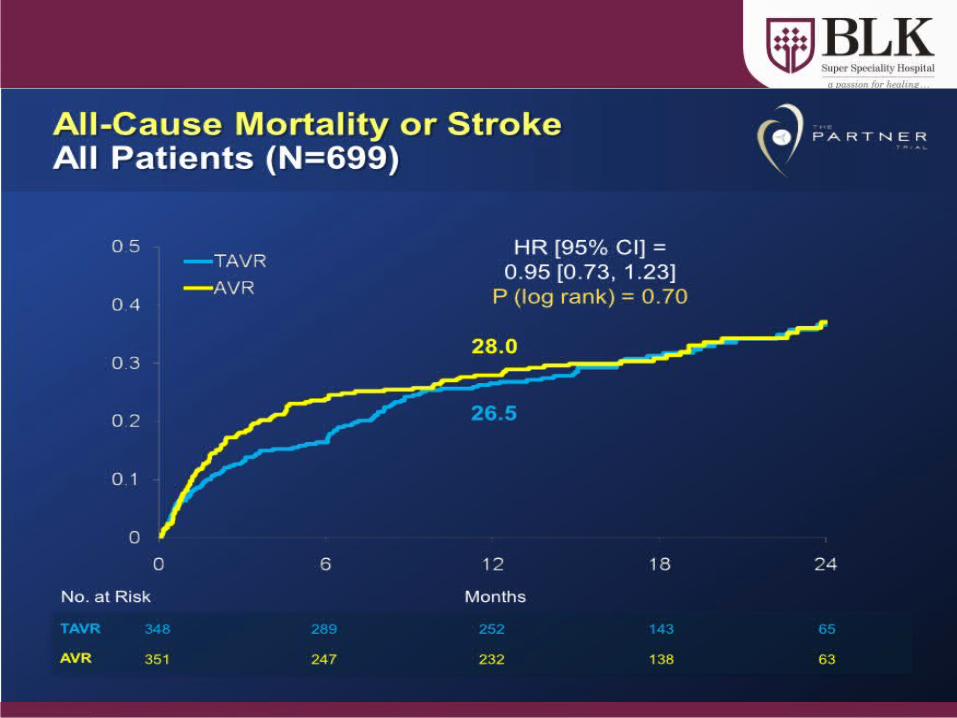
Vitamin D and ObesityObese subjects vs normal weight controls have
bull Lower serum 25OHD levelsbull Higher PTH and inconsistent results for
125(OH)2 D Liel et al Calcif Tissue Int 1988
Two possible explanationsbull Less sunlight exposurebull Decreased bioavailability of Vit D due to sequestration in
adipose tissue Wortsman et al Am J Clin Nutr 2000
bull Vit deficiency also associated with higher BMI and visceral adiposity
Cheng S et al Diabetes 2010
Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Overall high levels of Vit D are associated with a 43 reduction in cardiometabolic disorders
this finding applied to outcomes reported like CVD DM or MetS
Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis
Bolland MJ Grey A Avenell A Gamble GD Reid IR bullReanalysis of WHI CaD Study a seven year randomised placebo controlled trial of calcium and vitamin D (1g calcium and 400 IU vitamin D daily) in 36282 community dwelling postmenopausal women
RESULTS bullIn the 16718 women (46) who were not taking personal calcium supplements at randomisation the hazard ratios for cardiovascular events with calcium and vitamin D ranged from 113 to 122 (P = 005 for clinical myocardial infarction or stroke P = 004 for clinical myocardial infarction or revascularisation)
bullIn meta-analyses of three placebo controlled trials calcium and vitamin D increased the risk of myocardial infarction (relative risk 121 (95 confidence interval 101 to 144) P = 004) stroke (120 (100 to 143) P = 005) and the composite of myocardial infarction or stroke (116 (102 to 132) P = 002)
CONCLUSIONS bullCalcium supplements with or without vitamin D modestly increase the risk of cardiovascular events especially myocardial infarction A reassessment of the role of calcium supplements in osteoporosis management is warrantedBMJ 2011 Apr 19342d2040 doi 101136bmjd2040
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
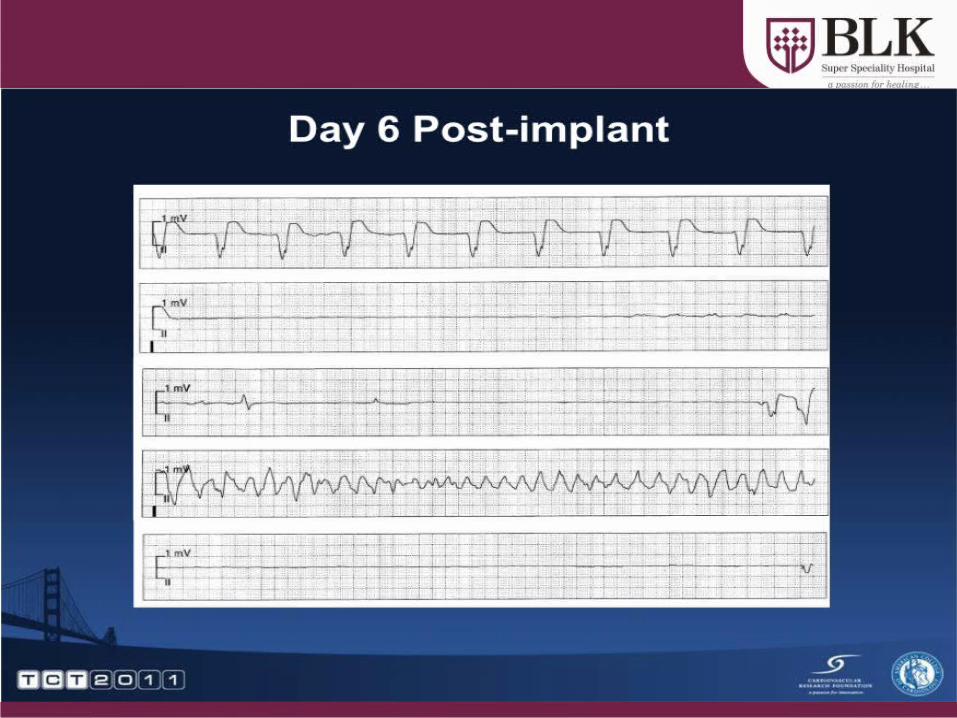
Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events
Wang L Manson JE Song Y Sesso HDbullFive prospective studies of patients receiving dialysis and 1 study involving a general population showed consistent reductions in cardiovascular disease (CVD) mortality among adults who received vitamin D supplements bullFour prospective studies of initially healthy persons found no differences in incidence of CVD between calcium supplement recipients and nonrecepients bullResults of secondary analyses in 8 randomized trials showed a slight but statistically nonsignificant reduction in CVD risk (pooled relative risk 090 [95 CI 077 to 105]) with vitamin D supplementation at moderate to high doses (approximately 1000 IUd) but not with calcium supplementation (pooled relative risk 114 [CI 092 to 141]) or a combination of vitamin D and calcium supplementation (pooled relative risk 104 [CI 092 to 118]) compared with placeboCONCLUSION bullEvidence from limited data suggests that vitamin D supplements at moderate to high doses may reduce CVD risk whereas calcium supplements seem to have minimal cardiovascular effects Further research is needed to elucidate the role of these supplements in CVD prevention
Ann Intern Med 2010 Mar 2152(5)315-23
bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

bull Very few foods in nature contain vitamin D The flesh of fatty fish (such as salmon tuna and mackerel) and fish liver oils are among the best sources [111] Small amounts of vitamin D are found in beef liver cheese and egg yolks Vitamin D in these foods is primarily in the form of vitamin D3 and its metabolite 25(OH)D3 [12] Some mushrooms provide vitamin D2 in variable amounts [1314] Mushrooms with enhanced levels of vitamin D2 from being exposed to ultraviolet light under controlled conditions are also available
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
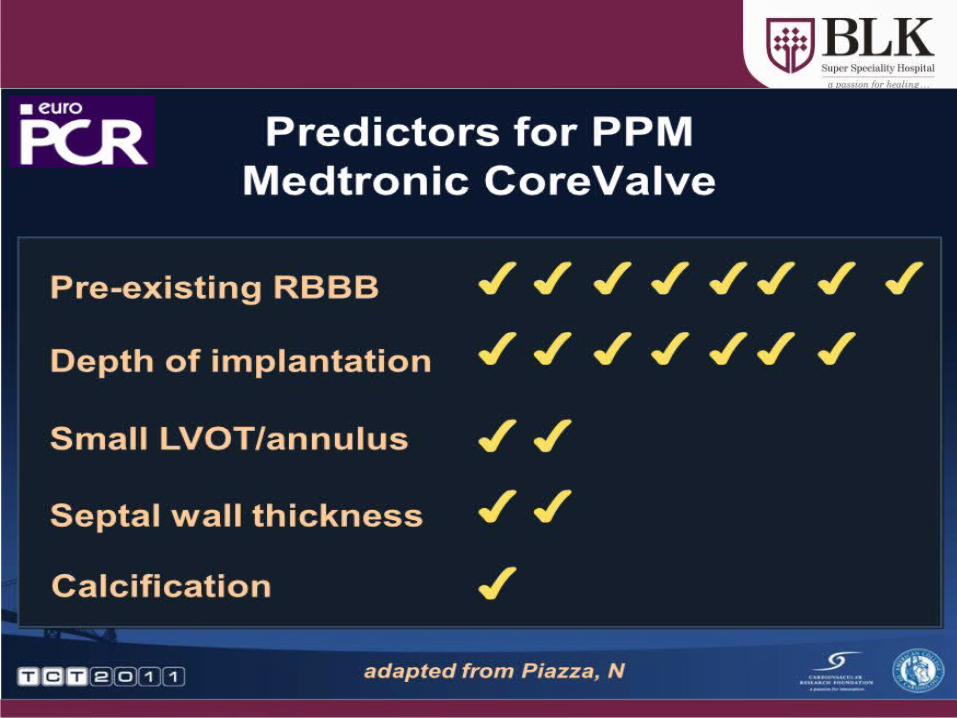
ButhellipWhat is the recommendation from
bull For most people daily Vitamin D supplementation is necessary particularly through the winter months
bull A daily amount of 800-1000IU per day will satisfy bodyrsquos basic requirement and higher doses are needed to correct deficiency
bull Leading advocates recommends 5000 IU per day for 2ndash3 months then obtain a 25-hydroxyvitamin D test and adjust dosage so that blood levels are between 50ndash80 ngmL (or 125ndash200 nML) year-round usually a minimum of 2000 IU a day 132
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
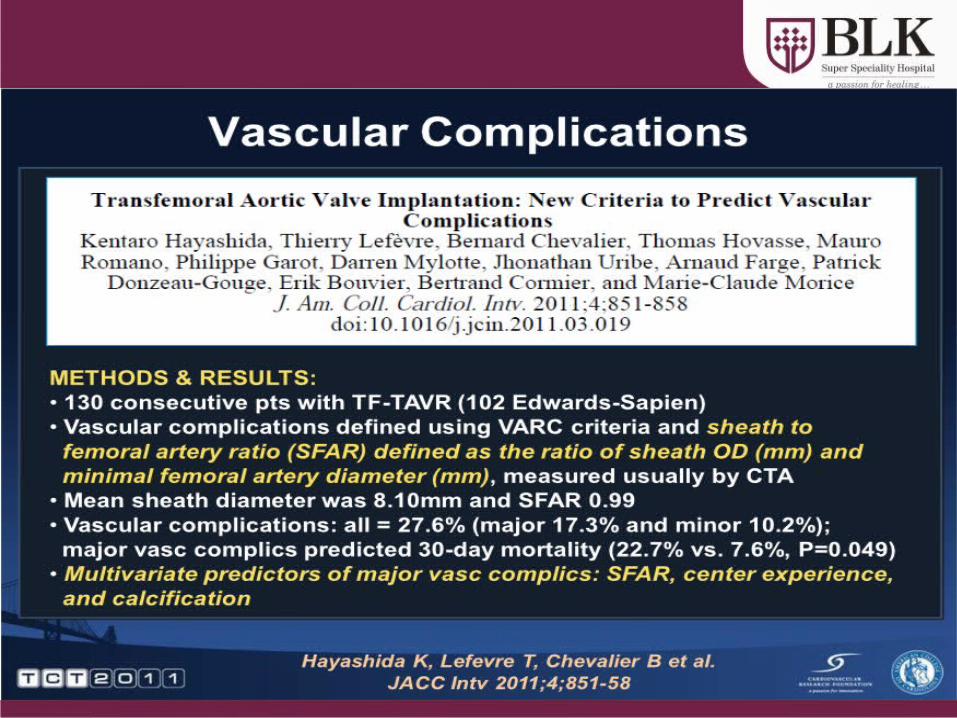
Preventive Measures1
Direct exposure to sunlight at least 30
minutesday Good dietary calcium intake
Supplementation to lactating
mothers
Artificial fortification
of infant food products
Making physical training to children in the schools
compulsory daily
Preventive use of sun screens
Outdoor activities of the
elderly and aged
J Assoc Physicians India 2009 Jan5740-48133
Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Vitamin D
Glucose Metabolismbull Increased insulin secretionbull Increased insulin sensitivitybull Increased glucose uptakebull Expression of insulin receptor
Endothelial amp Cardiovascular Protection
bull Suppression of RASSbull Control of inflammationbull Inhibition of smooth muscle cellbull Proliferation
Nephroprotectionbull Decreased inflammationbull Antiproteinuric effectbull Suppression of renin AT II
AT 1Rbull Decreased NF-αB activation
Vitamin D amp Spectrum of Vascular Protection
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-
NIH Recommendations of Vit D
Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Dawson-Hughes HeaneyHolick LipsMeunier ampVieth Osteoporosis Int 16713-7162005
How much Vitamin D Do We Need
bull ldquoFor five of the six authors the minimum desirable 25(OH)D concentration clusters between 70 and 80 nmolLrdquo (28-32 ngml)
ldquoThis requires~1000 IUdayrdquo
Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

Conclusions
bull Vitamin deficiency is common in Indiabull There is need to improve vitamin D status
through increased sun exposure food fortification supplements
bull Vitamin D may have beneficial effects on in prevention of Diabetes other CVD risk factors and CVD events
bull Need for further research regarding extra skeletal effects of Vitamin D
- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-

- Slide 1
- Slide 2
- Advancements in Anticoagulation
- Clinical Trials in Perspective
- Targets for Novel Antithrombotic Agents in the Coagulation Cascade1
- New Oral Antiocoagulants
- Advantage of Direct Thrombin Inhibitors (DTIs)
- DIRECT THROMBIN INHIBITORS
- Dabigatran Etexilate
- RE-LY Largest AF Outcomes Trial
- RE-LY Study Design
- Patients with Valvular Heart Disease (Haemodynamically Stable) were Included in RE-LY
- Patients with Valvular Heart Disease were Included in RE-LY
- Incidence of Stroke or Systemic Embolism
- Phase III RE-LY Risk of Stroke or Systemic Embolism
- Phase III RE-LY Time to First Stroke or Systemic Embolism
- Time to First Haemorrhagic Stroke
- RE-LY SAFETY RESULTS
- 150 mg BID no Difference vs Warfarin for Major Bleeds
- Slide 20
- Significantly Lower Intracranial Bleeding with Dabigatran
- Net Benefit Analysis Comparing Dabigatran 150 mg with 110 mg
- 110 mg BID DosemdashWhich Patients
- RE-LY in Perspective
- The Newer Anticoagulants on the Horizon
- Direct Thrombin and Factor Xa Inhibitors (DTIs) Approval for Stroke Prevention in AF
- Dabigatran vs Warfarin RiskBenefit by Dose
- Conclusions
- Slide 29
- Slide 30
- What is it
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- When should it be used
- Bioabsorbable stent The 4th Stephellip
- Slide 47
- Igaki- Tamai Bioabsorbable Stent
- Bioabsorbable Magnesuim Stent
- REVA Bioabsorbable Stent
- Bioabsorbable Therapeutics Stent
- BVS Everolimus-Eluting Bioabsorbable PLLA Stent
- Potential Long Term Advantages of ldquoRemovingrdquo a Rigid Coronary Stent
- Poly Lactide - Hydrolysis
- Bioresorbable Polymer ABSORB
- Slide 56
- Clinical Study Design ndash Cohort A
- ABSORB Long term follow-up
- ABSORB Scaffold Thrombosis Out to 5 Years
- Slide 60
- ABSORB Extend
- First ABSORB EXTEND Follow-up
- So farhellip
- Trans-catheter Aortic Valve Implantation (TAVI)
- TAVI
- Slide 66
- Slide 67
- What is the risk
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
- Slide 75
- Slide 76
- Slide 77
- Slide 78
- Slide 79
- Slide 80
- Slide 81
- Slide 82
- Slide 83
- Slide 84
- Slide 85
- Slide 86
- Slide 87
- Slide 88
- Slide 89
- Slide 90
- Slide 91
- Slide 92
- Slide 93
- Slide 94
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Slide 99
- Slide 100
- Slide 101
- Slide 102
- Vitamin D a Novel Cardiovascular risk factor
- Background
- Different forms of Vitamin D
- Vitamin D status in India
- Why does this happen
- Indian Studies Vitamin D status in Middle age group (20-45 years)
- Diagnostic Criteria for Vit D deficiency
- Sources of Vitamin D in India
- Slide 111
- Vitamin D conversion to 25(OH)D
- What is adequate supplementation in the Indian context
- Safety of Vitamin D
- Low Vitamin D A Potential Risk factor for CVD and Type 2 DM
- Potential Mechanisms for Diabetes amp CVD due to Vitamin D Deficiency
- Slide 117
- How much Vitamin D Do We Need
- Hypertension
- Slide 120
- Vitamin D deficiency and risk of CVD
- 25(OH)D and risk of MI in Men
- Heart disease
- Mechanisms of Vit D in CVD prevention
- Polycystic Ovary Syndrome
- Metabolic Syndrome
- Vitamin D and Obesity
- Slide 128
- Calcium supplements with or without vitamin D and risk of cardiovascular events reanalysis of the Womens Health Initiative and meta-analysis Bolland MJ Grey A Avenell A Gamble GD Reid IR
- Systematic review Vitamin D and calcium supplementation in prevention of cardiovascular events Wang L Manson JE Song Y Sesso HD
- Slide 131
- Buthellip What is the recommendation from
- Preventive Measures1
- Vitamin D amp Spectrum of Vascular Protection
- NIH Recommendations of Vit D
- Slide 136
- Conclusions
- Slide 138
-