dr. rafn benediktsson the diagnosis of diabetes rests on glucose values * should be confirmed on a...
TRANSCRIPT

Dr. Rafn Benediktsson
The Diagnosis of Diabetes rests on Glucose Values
Fastings- glucose
2h s- glucose(75g OGTT)
Normal < 6,0 < 7,7
Impaired Fasting Glucose 6,1 – 6,9
Impaired Glucose Tolerance 7,8 – 11,0
Diabetes* > 7,0 > 11,1
* should be confirmed on a second occasion

Dr. Rafn Benediktsson
Type 2 Diabetes: DevelopmentType 2 Diabetes: Development
Adapted from Saltiel AR, Olefsky JM. Diabetes 1996;45:1661-1669.
Insulin resistance and declining insulin levels Insulin resistance and declining insulin levels with impaired glucose tolerancewith impaired glucose tolerance
Insulin resistance and declining insulin levels Insulin resistance and declining insulin levels with impaired glucose tolerancewith impaired glucose tolerance
Type 2 DiabetesType 2 Diabetes
Insulin resistanceInsulin resistanceInsulin resistanceInsulin resistance
Insulin resistance and hyperinsulinaemia with
normal glucose tolerance
Insulin resistance and hyperinsulinaemia with
normal glucose tolerance
Impaired Impaired -cell function-cell functionImpaired Impaired -cell function-cell function
Dr. Rafn Benediktsson
What is Insulin Resistance?What is Insulin Resistance?
• An impaired biological response to An impaired biological response to either exogenous or endogenous insulineither exogenous or endogenous insulin
• Biological responses could reflect:Biological responses could reflect:– metabolicmetabolic (CHO, lipid or protein metabolism) (CHO, lipid or protein metabolism)
and and – mitogenicmitogenic processes processes
(changes in growth, differentiation, DNA (changes in growth, differentiation, DNA synthesis, regulation of gene transcription)synthesis, regulation of gene transcription)
Anonymous. Diabetes Care 1998; 21:310-314.

Dr. Rafn Benediktsson
Insulin Resistance: Associated ConditionsInsulin Resistance: Associated Conditions
Atherosclerosis
Type 2 diabetesImpaired
glucose tolerance
Polycysticovarian syndrome
Obesity (central)
Dyslipidaemia Hypertension
Microalbuminuria
Hyperuricemia
Decreasedfibrinolytic activity
InsulinResistance
Dr. Rafn Benediktsson
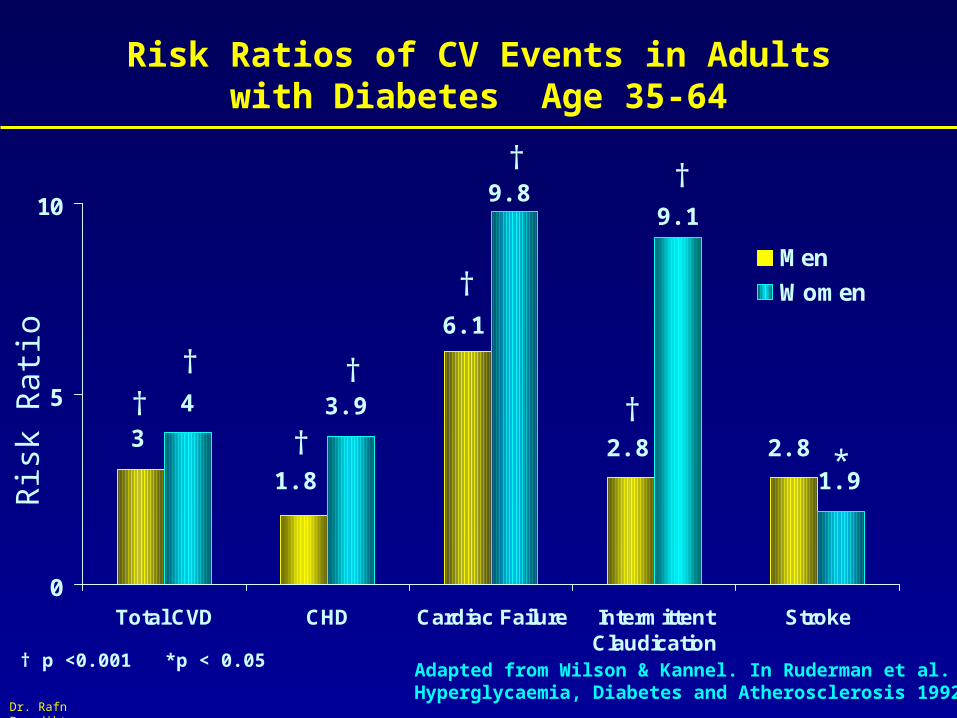
Risk Ratios of CV Events in Adultswith Diabetes Age 35-64
0
5
10
Total CVD CHD Cardiac Failure IntermittentClaudication
Stroke
Men
Women
3
1.8
6.1
2.8 2.8
4 3.9
9.89.1
1.9
Adapted from Wilson & Kannel. In Ruderman et al. Hyperglycaemia, Diabetes and Atherosclerosis 1992:21
†
†
†
†
†
†
*
††
† p <0.001 *p < 0.05
Ris
k R
ati o

Dr. Rafn Benediktsson
Drug Treatment in T2DM
Glucose (G)
Carbohydrate
GlucoseDIGESTIVE ENZYMES
Insulin(I)
I
I
I
II
I
I
I
G
G
G
G
G
G
G
GI
G
G
G
AcarboseReduces absorption
SulphonylureaRepaglinide
Stimulates pancreas
MetforminReduces hepatic glucose output
(? muscle / fat effects)
Insulin“Replaces” pancreas

Dr. Rafn Benediktsson
Lowering HbA1C Reduces Risk of Complications*
UKPDS. Lancet 1998; 352:837
*Percent risk reduction for 0.9% decrease in HbA1C
-40
-35
-30
-25
-20
-15
-10
-5
0
Re
du
cti
on
in
Ris
k (
%)
Any diabetesrelated endpoint
Microvascularendpoint
MI
Cataractextraction
Retinopathy
Albuminuria at12 years
-12
-25
-16
-24-21
-34
p=0.029
p=0.009
p=0.052
p=0.046p=0.015
p=0.00005

Dr. Rafn Benediktsson
UKPDS: Value of Good Blood Pressure Control in T2DM
0%
5%
10%
15%
20%
25%
0 3 6 9
Years from randomisation
Tight Blood Pressure Control (758)
Less Tight Blood Pressure Control (390)
risk reduction37% p=0.0092
Dr. Rafn Benediktsson
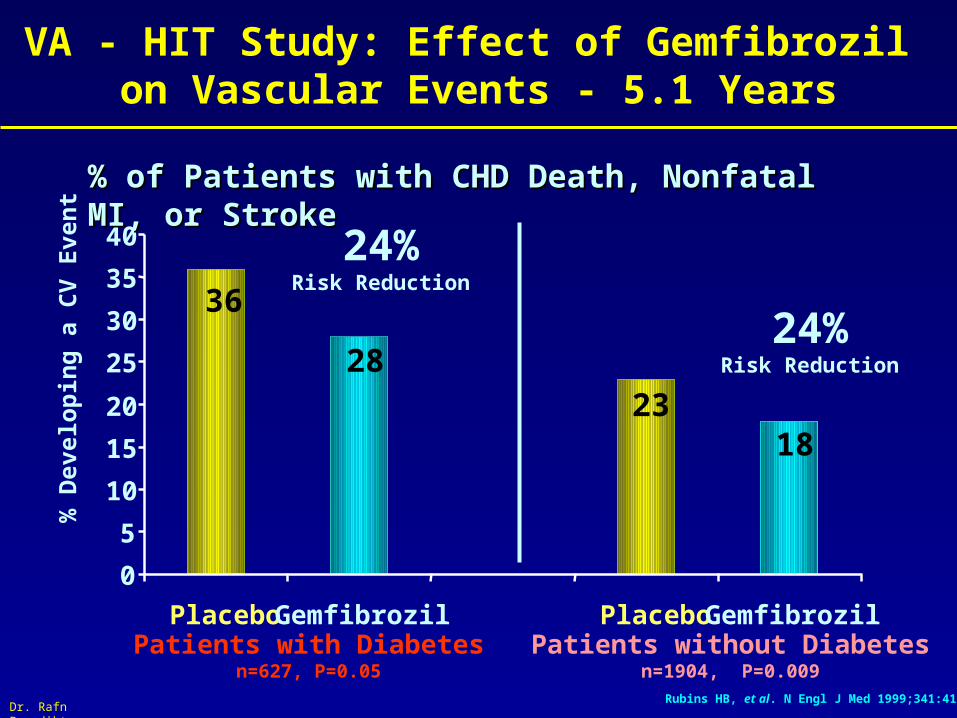
36
2823
18
0
5
10
15
20
25
30
35
40
Placebo Gemfibrozil Placebo GemfibrozilPatients with Diabetes
n=627, P=0.05Patients without Diabetes
n=1904, P=0.009
24%Risk Reduction
24%Risk Reduction
% of Patients with CHD Death, Nonfatal MI, or Stroke % of Patients with CHD Death, Nonfatal MI, or Stroke
VA - HIT Study: Effect of Gemfibrozil on Vascular Events - 5.1 Years
Rubins HB, et al. N Engl J Med 1999;341:410
% D
evel
op
ing
a C
V E
ven
t

Dr. Rafn Benediktsson
Drug Treatment in T2DM
Glucose (G)
Carbohydrate
GlucoseDIGESTIVEENZYMES
Insulin(I)
II
I
II
I
I
I
G
G
G
G
G
G
G
GI
G
G
G
AcarboseReduces absorption
SulphonylureaRepaglinide
Stimulates pancreas
MetforminReduces hepatic glucose output
(? muscle / fat effects)
Insulin“Replaces” pancreas
Thiazolidinediones(TZD)

Dr. Rafn Benediktsson
TZD = thiazolidinedionePPAR - RXR = nuclear receptorsTF = transcription factors
TZD: Mechanism of Insulin Sensitization
TZD
PPAR RXR
PPAR RXR
TZDTF
RNA
DNA
Protein– signalling– downstream events
RECEPTOR
INSULIN
Saltiel & Olefsky. Diabetes 1996;45:1661

Dr. Rafn Benediktsson

Dr. Rafn Benediktsson
Dr. Rafn Benediktsson
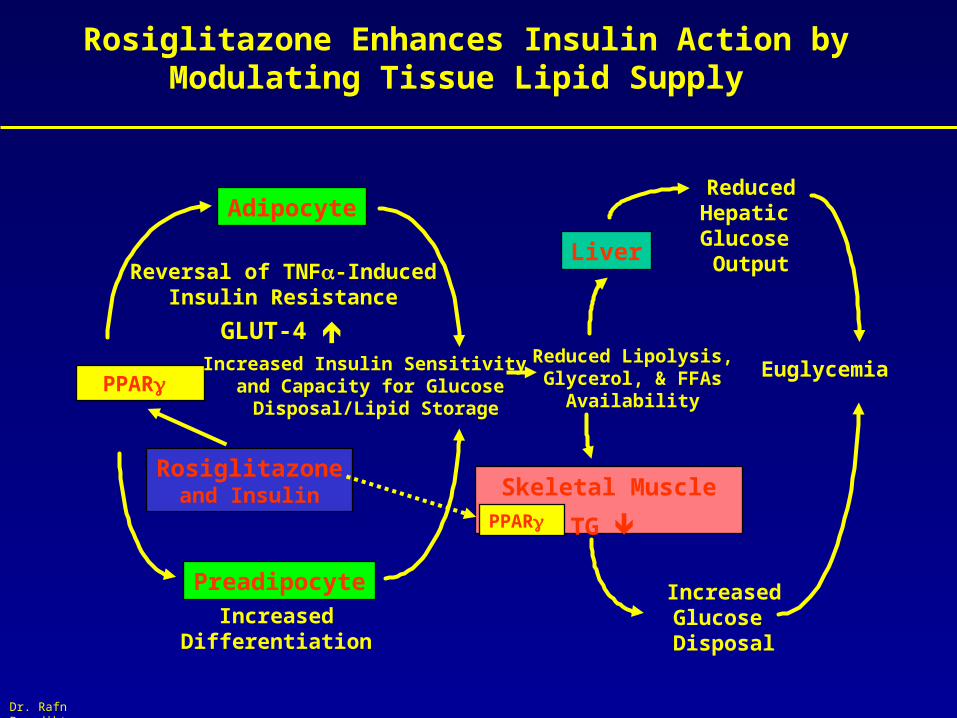
Rosiglitazone Enhances Insulin Action by Modulating Tissue Lipid Supply
Rosiglitazoneand Insulin
PPAR
Preadipocyte
Adipocyte
IncreasedDifferentiation
Reversal of TNF-InducedInsulin Resistance
Increased Insulin Sensitivity and Capacity for Glucose Disposal/Lipid Storage
Reduced Lipolysis, Glycerol, & FFAs
Availability
Skeletal Muscle
Liver
Euglycemia
IncreasedGlucose Disposal
ReducedHepatic Glucose Output
PPAR
GLUT-4
TG

Dr. Rafn Benediktsson
Effect of Pioglitazone on Insulin Resistance (HOMA R)
-12.4
30.3
-15
-5
5
15
25
35
Ch
ang
e (%
)
placebo (n=81)
pioglitazone 30 mg(n=96)
Baseline IR: placebo 10.1, pioglitazone 30 mg 9.8* p = 0.0002 vs baseline† p = 0.0001 vs placebo
Rosenstock I, et al. Diabetologia 2000;43(suppl 1):A738
30.3*
†

Dr. Rafn Benediktsson
Before After p-value
Body weight (kg) 82 85 < 0.01
Fat mass (kg) 24 29 < 0.01
Subcu fat area (cm2) 300 342 < 0.01
Visc fat area (cm2) 144 131 < 0.05
V/S ratio 0.59 0.44 < 0.01
Effect of Pioglitazone on Abdominal Fat Distribution
Miyazaki Y et al. Diabetes 2000;49(SI);A299.

Dr. Rafn Benediktsson
TRIPOD: Buchanan et al. Diabetes 2001;50(S2):A327
Placebo for 30 months
Troglitazone for 30 months
235 Latino womenwith GDMA
% w
ith d
iab
ete
s
0
4
8
12
16
20
Placebo Troglitazone
B Observ. for8 mo.: OGTT

Dr. Rafn Benediktsson
PCOS: Improvement in hirsutism by troglitazone
% change in F
G score
PBO TGZ150 TGZ300 TGZ600
-20-18-16-14-12-10-8-6-4-2024
Azziz et al JCEM 2001;86:1626
*

Dr. Rafn Benediktsson
LOCF* p0.05 vs. placebo
-13.6
4.6
9.5
1.62.1
11.5
1.2
- 15.1-20
-10
0
10
20 Glycaemic Non-Responders (45 mg)
Total Cohort (45 mg)
from placebo at 26 weeks
HDL Cholesterol LDL CholesterolTriglycerides Total Cholesterol
(%)
Baseline (mmol/L) 3.281.056.272.93
**
2.66 5.45 1.07 3.29
*
Effect of Pioglitazone on Serum Lipids Effect of Pioglitazone on Serum Lipids Effects by Glycaemic ResponseEffects by Glycaemic Response
Takeda Pharmaceuticals America, Inc., data on file, study 001

Dr. Rafn Benediktsson
Inflammation: Effect of rosiglitazone on CRP
-50
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
CR
P %
Ch
an
ge
fro
m b
as
elin
e a
t 2
6w
Placebo
Rosiglitazone
N = 357, treatment for 26 weeks
Greenberg et al @ EASD 2001

Dr. Rafn Benediktsson
PPAR activators inhibit migration of VSMC
0
50
100
PDGF
% o
f mig
ratio
n c
ompa
red
to P
DG
F-B
B
- + ++
5 µM
troglitazone
10 µM
Marx et al.; Circ Res 1998; 83: 1097-1103

Dr. Rafn Benediktsson
Rosiglitazone inhibits the insulin-mediated increase in PAI-1 secretion in human subcutaneous adipocytes
30
40
50
60
70
80
90
100
110
0,1 1 10 100 1000
PA
I-1
secr
etio
n [
ng
/ml]
Insulin
Insulin + Rosi
CTRL
Insulin [nM]
Mcternan @ EASD 2001
Dr. Rafn Benediktsson
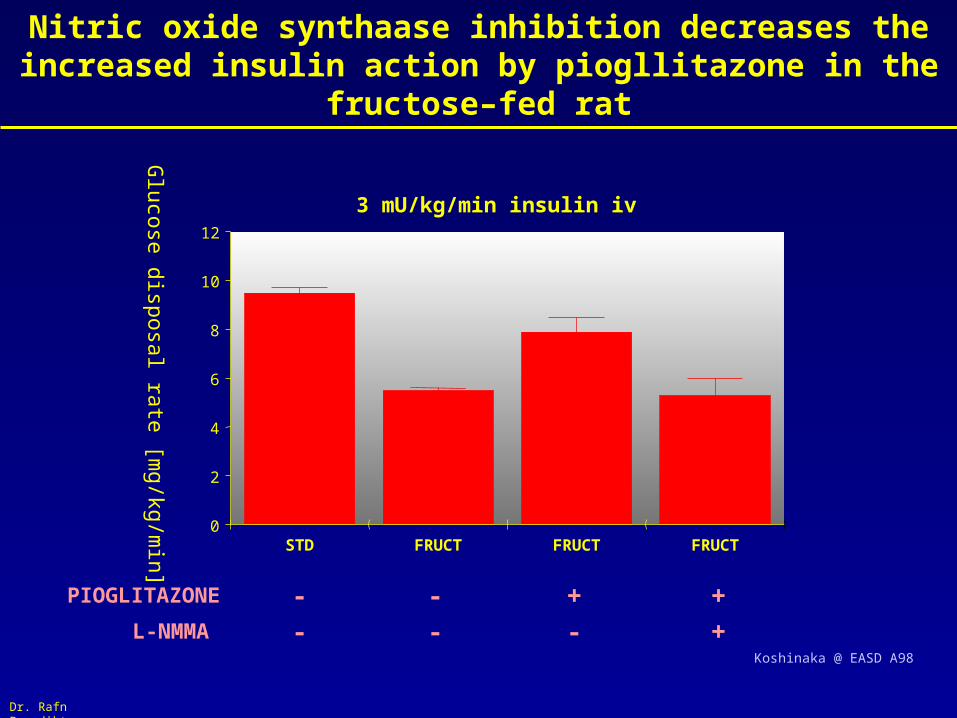
Nitric oxide synthaase inhibition decreases the increased insulin action by piogllitazone in the fructose–fed rat
3 mU/kg/min insulin iv
Glucose disposal rate [m
g/kg/min] 0
2
4
6
8
10
12
STD FRUCT FRUCT FRUCT
PIOGLITAZONE
L-NMMA ++ +-
--
- -Koshinaka @ EASD A98

Dr. Rafn Benediktsson
The ischaemic obese Zucker rat heart
0
0,2
0,4
0,6
0,8
1
1,2
Lean Rosi Lean
Obese RosiObese
Glu
co
se
up
tak
e
*
Sidell @ EASD 2001

Dr. Rafn Benediktsson
Rosiglitazone reduces atherosclerosis in ApoE KO mice
Benson et al @ EASD 2001

potential antiatherogenic effects
potentialproatherogenic effects
VCAM-1, endothelin
IL-6, prostaglandin,
COX-2
apoptosis Tissue factor, TNF-
ECs
SMCs
Mo / MØ
CXC chemokines,
endothelin, PAI-1ECs
SMCs
Mo / MØMMP-9; cytokines,
SR A,I-NOS
PAI-1
migration, MMP-9,
Ang-II-receptor
NO production
CD 36Foam cell formation
apoptosis
MCP-1, IL-8
PPAR
PPAR
ECs
SMCs
Mo / MØ
ECs
SMCs
Mo / MØ
TH-1 cytokines T-cells

Dr. Rafn Benediktsson
Niðurstaða
• Thiazolidinedione lyf eru leyfð á Íslandi sem meðferð við sykursýki
• Eingöngu sem viðbót við eitt annað per os blóðsykurlækkandi lyf
• TZD lyf ráðast að kjarna málsins – Insúlín viðnám – og þannig á ýmsa áhættuþætti hjarta og æðasjúkdóma
• In-vitro rannsóknir og dýratilraunir gefa vísbendingar um að TZD lyf geti hugsanlega tafið nýmyndun og framgang atherosclerosis
• Ekki eru til klínískar mannarannsóknir á áhrifum TZD á atherosclerosu eða dánartíðni !