draft detailed newborn screening use case and resource guide advisory committee on heritable...
TRANSCRIPT

Draft Detailed Newborn Screening Draft Detailed Newborn Screening Use Case and Resource GuideUse Case and Resource Guide
Advisory Committee on Heritable Disorders in Advisory Committee on Heritable Disorders in Newborns and ChildrenNewborns and Children
Stephen M Downs MDStephen M Downs MDIndiana University School of MedicineIndiana University School of MedicineAHIC Personalized Healthcare WorkgroupAHIC Personalized Healthcare Workgroup
Alan E Zuckerman MD Alan E Zuckerman MD Georgetown University School of Medicine, consultant ONCGeorgetown University School of Medicine, consultant ONC
Oct 2, 2008Oct 2, 2008

Overview
• Dr Downs– New roles for Health Information Technology in Newborn
Screening• Dr Zuckerman
– Newborn Screening Draft Detailed Use Case– Next Steps for Completing the NBS Use Case– Supporting Implementation of the Use Case and deployment
of standards in state newborn screening programs • Dr Downs
– Resource Guide for Newborn Screening Draft Detailed Use Case
– Maintaining the Resource Guide for the NBS Use Case– Web application for viewing the NBS Resource Database
New Roles for HIT in Newborn Screening
Advisory Committee on Heritable Disorders in Newborns and Children
• 29 disorders
• Increase children identified 32% (4,370 to 6,439)
• Improve quality by improving the efficiency of identifying cases
• Rare disorders– May require regional expertise– Screening, diagnosis, and management– HRSA regional network of technical centers– Need for coordination
• Long term roles of NBS programs – Surveillance and tracking– Ensuring screening and follow-up for many rare disorders– Ensuring clinical care and management of complex disorders
• Rare & more common (e.g., cystic fibrosis)• Require different types of specialists
• Life-long clinical management.

Quality Control and Research
• Extremely rare conditions• Natural history poorly understood• Therapeutic trials require multiple centers• Case definitions very state to state• Optimal screening cut-offs unknown• Uniform, consistent coding and electronic exchange of data
is critical– Lab with health department
– Health department (or lab) with clinician
– Health department with health department
– Health department with investigators
– Health department with government agencies
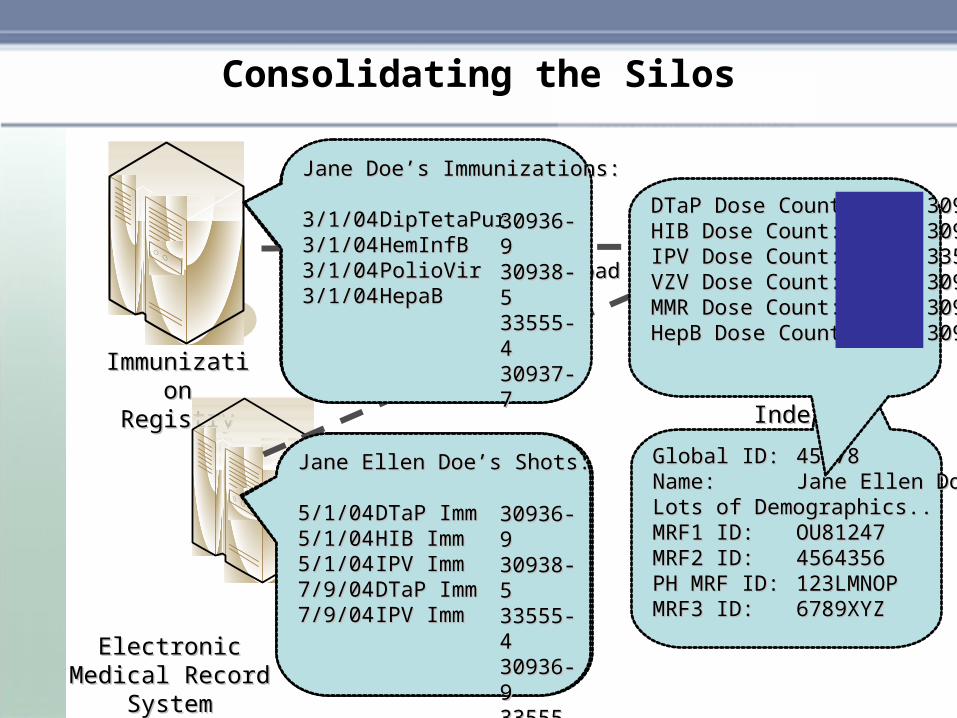
Consolidating the Silos
ImmunizatioImmunization Registryn Registry
Electronic Electronic Medical Record Medical Record
SystemSystem
Patient ID: 123LMNOPPatient ID: 123LMNOPName: Jane Doe Name: Jane Doe DOB: 01/01/04DOB: 01/01/04SSN: N/A SSN: N/A Address: 555 Johnson RoadAddress: 555 Johnson RoadCity: IndianapolisCity: IndianapolisState: IndianaState: IndianaZIP: 46202ZIP: 46202
Patient ID: 6789XYZPatient ID: 6789XYZName: Jane Ellen DoeName: Jane Ellen DoeDOB: 01/01/04DOB: 01/01/04SSN:123-45-6789SSN:123-45-6789Address: 555 Johnson Address: 555 Johnson RoadRoadCity: IndianapolisCity: IndianapolisState: IndianaState: IndianaZIP: 46202ZIP: 46202
Global Global Patient Patient IndexIndex
Concept Concept DictionaryDictionary
Global ID:Global ID: 4567845678Name: Name: Jane Ellen Doe Jane Ellen Doe Lots of Demographics..Lots of Demographics..MRF1 ID: MRF1 ID: OU81247OU81247MRF2 ID: MRF2 ID: 45643564564356PH MRF ID: PH MRF ID: 123LMNOP123LMNOPMRF3 ID:MRF3 ID: 6789XYZ6789XYZ
DTaP Dose Count:DTaP Dose Count: 30936-930936-9HIB Dose Count:HIB Dose Count: 30938-530938-5IPV Dose Count:IPV Dose Count: 33555-433555-4VZV Dose Count:VZV Dose Count: 30943-530943-5MMR Dose Count:MMR Dose Count: 30940-130940-1HepB Dose Count:HepB Dose Count: 30937-730937-7
Jane Doe’s Immunizations:Jane Doe’s Immunizations:
3/1/043/1/04 DipTetaPurDipTetaPur3/1/043/1/04 HemInfBHemInfB3/1/043/1/04 PolioVirPolioVir3/1/043/1/04 HepaBHepaB
Jane Ellen Doe’s Shots:Jane Ellen Doe’s Shots:
5/1/045/1/04 DTaP ImmDTaP Imm5/1/045/1/04 HIB ImmHIB Imm5/1/045/1/04 IPV ImmIPV Imm7/9/047/9/04 DTaP ImmDTaP Imm7/9/047/9/04 IPV ImmIPV Imm
30936-30936-9 9 30938-30938-5 5 33555-33555-4 4 30937-30937-77
30936-30936-9 9 30938-30938-5 5 33555-33555-4 4 30936-30936-9 9 33555-33555-44

Consolidating the Silos
ImmunizatioImmunization Registryn Registry
Electronic Electronic Medical Record Medical Record
SystemSystem
Global Global Patient Patient IndexIndex
Concept Concept DictionaryDictionary
St. St. Vincent Vincent
MRFMRF
Clarian Clarian MRFMRF
Wishard Wishard MRFMRF
Community MRFCommunity MRF
Public Public Health MRFHealth MRF
Global Global Patient Patient IndexIndex
IUMG MRFIUMG MRF
Concept Concept DictionaryDictionary

HL7 and Coding Standards
OBX|15|CWE|2^Endocrine Disorders^L||107^Borderline >48Hrs <1500^L^OH-C-03-002^THE SCREEN FOR CONGENITAL ADRENAL HYPERPLASIA IS ABNORMAL. FURTHER FOLLOW-UP IS NECESSARY TO EVALUATE THIS INFANT.^L||< 50 ng/ml|A||||||20070727040000
This is an observation
The observation name is “Endocrine Disorders” with a local code
The observation value is “Borderline >48Hrs <1500”
Local code OH-C-03-002
LOINC: Logical Observation Identifiers Names and Codes
• Most clinical labs use HL7, but idiosyncratic codes for tests• LOINC codes are universal identifiers for laboratory and other
clinical observations • Facilitate the exchange and pooling of results• Definition of a LOINC Codes includes:
– Component (or analyte name) — e.g. potassium, hemoglobin– Property— e.g. mass concentration, enzyme activity
(catalytic rate)– Timing - i.e. an observation at a moment of time, or
integrated over an extended duration of time — e.g. 24-hour urine
– Sample — e.g. urine; blood; blood spot– Scale — e.g. quantitative (a true measurement) ordinal (a
ranked set of options), nominal (e.g. E. coli; Staphylococcus aureus), or narrative (e.g. dictation results from xrays)
– Method used to produce the result or other observation
Newborn Screening Draft Detailed Use Case
11
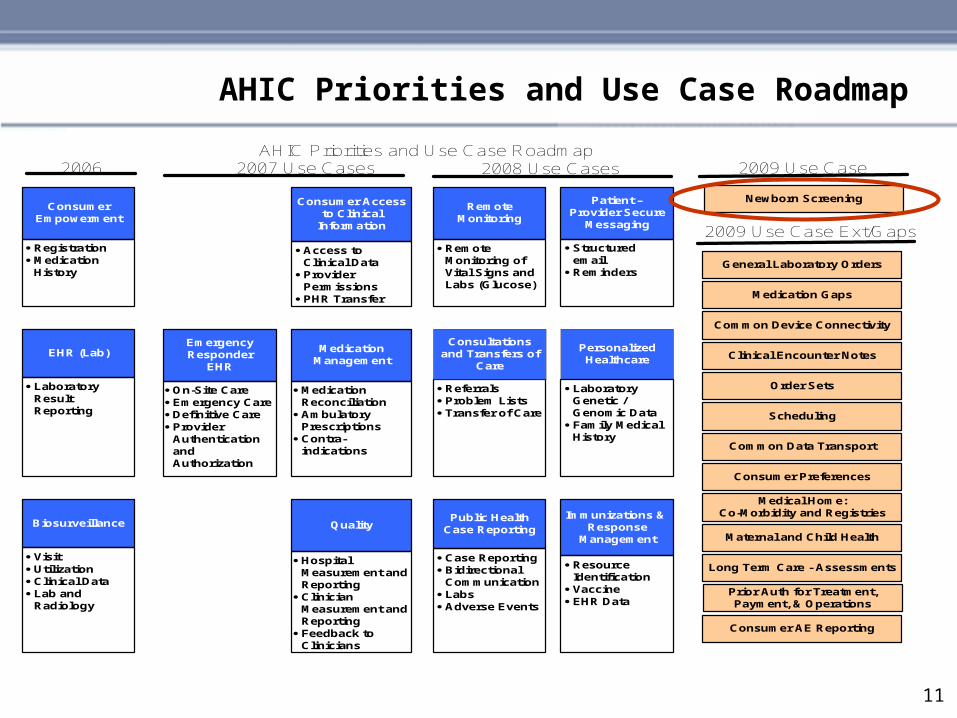
AHIC Priorities and Use Case Roadmap
2006 2007 Use Cases
Consumer Empowerment
· Registration· Medication
History
AHIC Priorities and Use Case Roadmap
Consumer Access to Clinical
Information
· Access to Clinical Data
· Provider Permissions
· PHR Transfer
Medication Management
· Medication Reconciliation
· Ambulatory Prescriptions
· Contra-indications
EHR (Lab)
· Laboratory Result Reporting
Emergency Responder
EHR
· On-Site Care· Emergency Care· Definitive Care· Provider
Authentication and Authorization
Patient – Provider Secure
Messaging
· Structured email
· Reminders
· Referrals· Problem Lists· Transfer of Care
Personalized Healthcare
· Laboratory Genetic / Genomic Data
· Family Medical History
2008 Use Cases
Quality
· Hospital Measurement and Reporting
· Clinician Measurement and Reporting
· Feedback to Clinicians
Biosurveillance
· Visit· Utilization· Clinical Data· Lab and
Radiology
Public HealthCase Reporting
· Case Reporting· Bidirectional
Communication· Labs· Adverse Events
Immunizations & Response
Management
· Resource Identification
· Vaccine· EHR Data
RemoteMonitoring
· Remote Monitoring of Vital Signs and Labs (Glucose)
2009 Use Case
Medical Home:Co-Morbidity and Registries
Maternal and Child Health
Prior Auth for Treatment, Payment, & Operations
Long Term Care - Assessments
Consumer AE Reporting
Consultations and Transfers of
Care
General Laboratory Orders
Medication Gaps
Common Device Connectivity
Order Sets
Consumer Preferences
Common Data Transport
Clinical Encounter Notes
Newborn Screening
2009 Use Case Ext/Gaps
Scheduling

12
Purpose of AHIC Use Cases
Use Cases• Used to describe the high-level needs of many
– systems– stakeholder organizations– and individuals.
• Based on the priorities expressed by AHIC work groups; they describe– scenarios– perspectives– information flows– events– actions– needs– barriers– and sample datasets that may apply to the multiple
organizations participating in these areas.

13
• Integrate the results from screening in all six clinical domains – metabolic, hearing, endocrine, hemoglobin, pulmonary/genetic, congenital infections, and other into a single comprehensive report.
• Complete a newborn screening consultation and referral document that includes all of the initial screening results, adds and tracks confirmatory testing and referrals, and identifies all providers and all relevant encounters.
• Report to public health includes the sharing of de-identified data in the initial screening and the consultation and referral reports with the public health and clinical research community as well as individual case reporting to registries and local service providers
• Address consumer need to receive educational material regarding the screening and/or a suspected or confirmed condition, and provide additional information and/or specimens
NBS Use Case Scope –The AHIC Request
14
The Perspectives define the parties who exchange information
• Consumer• Ordering Clinician• Pediatric Clinician• Testing Facility • Testing Laboratory• Audiology services• Public Health• Information Exchange• Other Data Users
Newborn Screening - Perspectives
15
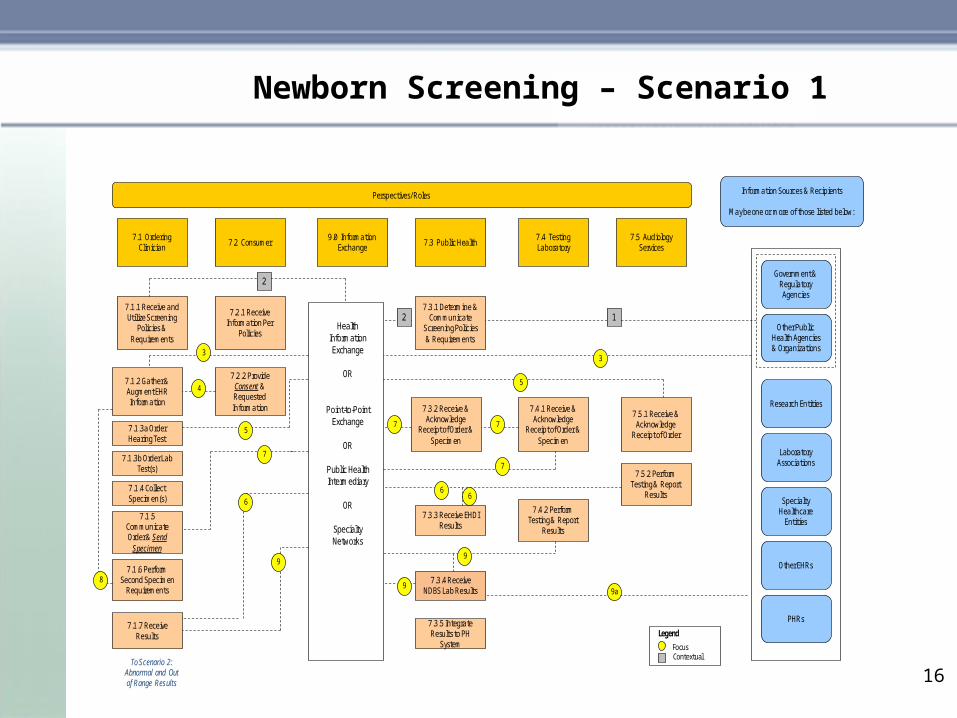
This scenario covers initial screening testing, both for Newborn Dried Blood Spot (NDBS) and Early Hearing Detection and Intervention (EHDI) and ends with the reporting of results, either within normal limits, or notification of the need for confirmatory testing if results are outside of normal limits.
• Includes pre-screening education and consent process
• Includes data collection as part of the ordering process
• Includes decisions for the need for second or repeat screening tests
• Includes routing results to the appropriate clinician caring for the child
• Includes closing the orders loop to acknowledge review of the results
Scenario 1 – Ordering and Resulting
16
Newborn Screening – Scenario 1
Contextual
Perspectives/ Roles
Health Information Exchange
OR
Point-to-PointExchange
OR
Public Health Intermediary
OR
Specialty Networks
Specialty Healthcare
Entities
Government & Regulatory Agencies
Other EHRs
Information Sources & Recipients
May be one or more of those listed below:
Research Entities
PHRs
Laboratory Associations
Other Public Health Agencies & Organizations
7.1 Ordering Clinician
7.1.1 Receive and Utilize Screening
Policies & Requirements
7.2 Consumer
7.2.1 Receive Information Per
Policies
7.3 Public Health
7.3.1 Determine & Communicate
Screening Policies & Requirements
7.4 Testing Laboratory
7.4.1 Receive & Acknowledge
Receipt of Order & Specimen
7.5 Audiology Services
7.5.1 Receive & Acknowledge
Receipt of Order
9.0 Information Exchange
7.1.2 Gather & Augment EHR Information
7.2.2 Provide Consent & Requested Information
4
33
7.1.3a Order Hearing Test
7.1.4 Collect Specimen(s)
7.1.5 Communicate Order & Send
Specimen
7.1.6 Perform Second Specimen
Requirements
7.3.2 Receive & Acknowledge
Receipt of Order & Specimen
7 7
7.4.2 Perform Testing & Report
Results
7.5.2 Perform Testing & Report
Results
7.1.7 Receive Results
8
7.3.3 Receive EHDI Results
9a
To Scenario 2: Abnormal and Out of Range Results
12
2
9
7.3.5 Integrate Results to PH
System Focus
Legend
7.1.3b Order Lab Test(s)
6
6
7
7.3.4 Receive NDBS Lab Results
6
9
5
5
7
9

17
This scenario covers the diagnostic work up for an out of range (or abnormal) screening test either from the NDBS or the EHDI.
• Includes confirmatory testing• Includes collection of family history• Includes audiology evaluation of hearing loss• May include emergency treatment• Includes case reporting to the health department• Includes consultations and referrals• Includes referrals for other support services such as
dietary or early educational interventions• Includes sharing de-identified data• Includes bidirectional communication and educational
materials
Scenario 2 – Abnormal and Out of Range Results

18
Newborn Screening – Scenario 2
ContextualFocus
Legend
Perspectives/ Roles
Health Information Exchange
OR
Point-to-PointExchange
OR
Public Health Intermediary
OR
Specialty Networks
Specialty Healthcare
Entities
Government & Regulatory Agencies
Other EHRs
Information Sources & Recipients
May be one or more of those listed below:
Research Entities
PHRs
Laboratory Associations
Other Public Health Agencies & Organizations
8.1 Pediatric Clinician
8.1.1 Receive Abnormal or Out of Range Results and
Educational Materials
8.2 Consumer
8.2.1 Provide Detailed Family
History
8.3 Public Health
8.3.2 Receive Detailed Family
History
8.4 Laboratory
8.4.1 Receive & Acknowledge
Receipt of Order & Specimen
8.5 Audiology Services
8.5.1 Receive & Acknowledge
Receipt of Order
9.0 Information Exchange
8.1.2 Gather Detailed Family
History
8.2.2 Provide Confirmatory NDBS
8.1.3 Order Repeat Specimen and
Confirmatory Test(s)
8.1.4 Collect Specimen(s)
8.1.5 Communicate Order & Send
Specimen
8.3.3 Receive Confirmatory Order
Information
13
8.4.2 Perform Testing & Report
Results
8.5.2 Perform Testing & Report
Results
148.16 Receive
Results
Public Health Case Reporting Detailed Use Case March 21, 2008
14
15
8.2.3 Confirmatory EHDI testing
8.1.7 Public Health Case Reporting
10
10a
8.3.1 Collect and Distribute Disorder
Information
12
12
15
10b
8.2.4 Receive Clinical Interventions
and Support Services
8.3.5 Conduct Long Term Follow-up
8.18 Request Referral & Place
Intervention Orders
Personalized Health Care and Consultations and Transfers of Care Detailed Use Cases March 21, 2008
13
12
11
8.3.4 Request Referral & Place
Intervention Orders

19
Datasets defined as part of the use case will standardize data exchange– Birth History– Newborn Information Required for Screening Order– Analytes and Conditions– Hearing Screenings– Date of Newborn Screening– Date of Diagnosis and Final Diagnosis– Date and Type of Referral– Date of Enrollment and Type of Treatment Plan/Services
• There is a need to report both the clinical conditions identified and the quantitative analytes measured on newborn screening
• There is also a need to standardize terminology and coding through the Resource Guide for NBS Draft Detailed Use Case
Data Set Considerations

20
• Instructions
– URL = http://www.hhs.gov/healthit/usecases/.
– Instructions for providing feedback are included on the web page
– Please provide feedback by Friday, 10/17/08
– Please identify Organization, Contact Name, and Contact Information in feedback response.
– Please provide references to relevant Extension/Gap sections when submitting feedback.
• For General Questions, Comments, or Communications [email protected]
• Additional Opportunities for Participation:
– Within feedback comments, please indicate willingness to be contacted for potential follow-up discussions, and/or:
– Please feel free to suggest potential subject matter experts (including contact information)
– Please feel free to send relevant reference documents and/or information
Public Feedback Instructions

Next Steps to Complete the Use Case
• A final detailed use case will be completed in December
• The Health Information Technology Standards Panel HITSP will develop an Interoperability Specification for Newborn Screening
• HL7 is developing an Implementation Guide for Newborn Screening Laboratory Results Reporting that will be essential to the work of HITSP
• The Resource Guide for the NBS Use Case will provide terminology and codes
• After the Standards are accepted and recognized by the Secretary of HHS, they must be implemented by NBS Programs

Implementing the NBS Use Case
• It is essential to begin now to generate interest in implementing the newborn screening use case nationwide
• The use case will enable direct reporting of NBS results into EHR, but only if Health Department and Screening Laboratories implement the standards developed for the use case – software enhancements are needed
• Because of limited rates of EHR adoption, web access to reports will also be part of the use case
• De-identified data will be available for program monitoring, national reporting, and research
• The Use Case is a work order or statement of requirements for standards, it is the beginning of a long process

Resource Guide for Newborn Screening
Draft Detailed Use Case
Resource Guide for Newborn Screening Draft Detailed Use Case
• A listing of codes and coding standards appropriate for the entities that are important to newborn screening
• Conditions– MIM (Mendelian Inheritance in Man)– SNOMED (Systematized Nomenclature of Medicine)– EC (Enzyme Commission, International Union of
Biochemistry and Molecular Biology)– ACMG (American College of Medical Genetics
• Analytes & clinical screening results (EHDI)– LOINC– Includes key sums and ratios
• Mappings– Analyte to condition– Condition to analyte

Example of Conditions

Example of Analytes
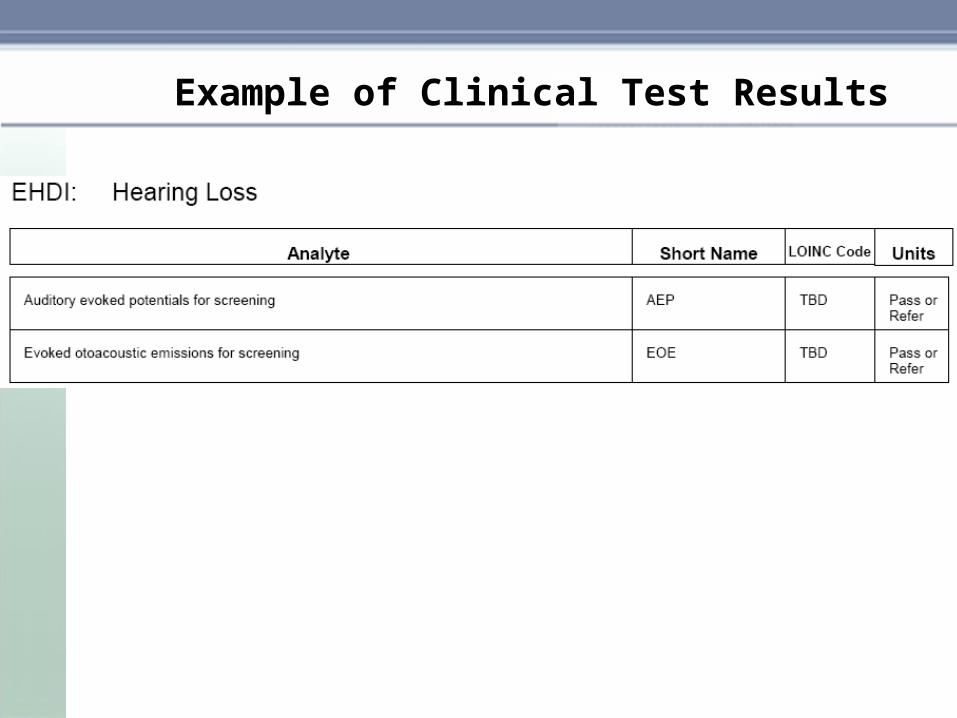
Example of Clinical Test Results
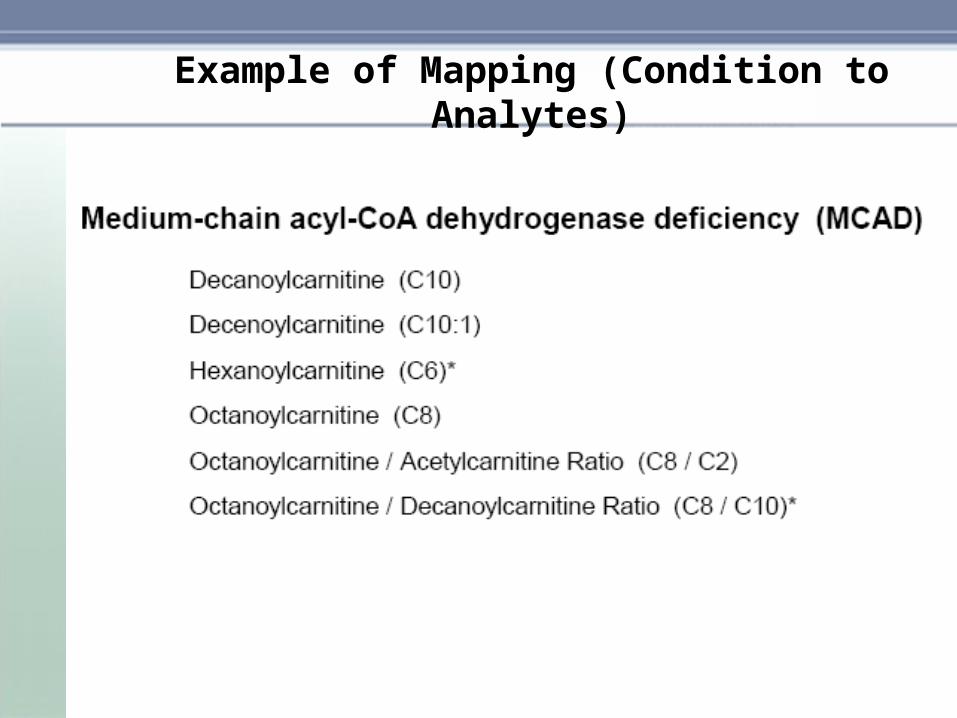
Example of Mapping (Condition to Analytes)

Demonstration of Web Version of the Newborn Screening Resource
Database
Temporary Developmental Locationhttp://transparency.cit.nih.gov/
screening
Maintaining the NBS Resource Guide
• The Resource Guide for the Newborn Screening Use Case is a work in progress that will require additional work to complete now, and on-going work to keep it current and complete.
• A revised version will be prepared to accompany the final detailed used case that will be published in December 2008
• As new tests and new methods of screening are developed, and as new codes are created, they must be added to the resource guide
• Web access to the resource guide will facilitate collection of comments and use by laboratories
• The scope of the resource guide could expand to include more genomic information and links to other databases
• We need to find a home for the resource guide as the AHIC Workgroups are completing their work

Comments and Discussion
• Affirming the need for new roles for Health Information Technology in Newborn Screening
• Comments on the Draft Detailed Use Case– Stakeholders and perspectives– Barriers and privacy issues– Scenario 1 – initial screening– Scenario 2 – confirmatory testing
• Comments on the NBS Resource Guide and other dataset issues• Plans for Assisting Implementation of the NBS Use Case
– Role of the ACHDNC• Plans for Maintaining and distributing the resource guide
– Role of the ACHDNC