driver rehabilitation: reclaiming the road wesley perry, msbme, atp, cdrs cliff d. dedeaux, otr/l,...
TRANSCRIPT

Driver Rehabilitation: Reclaiming the Road
Wesley Perry, MSBME, ATP, CDRSCliff D. Dedeaux, OTR/L, ATP, CDRS
November 2006
Introduction
Wesley L. Perry, MSBME, ATP, CDRS
M.S., Biomedical EngineeringCertified Driver Rehabilitation Specialist (CDRS), 2000Assistive Technology Practitioner (ATP), 2005
Member ADED, The Association for Driver Rehabilitation Specialists
Dec. ’98 – present; Research Associate, T.K. Martin Center for Technology and Disability, Mississippi State University, responsibilities include coordinating the Center’s adaptive driving program.
Introduction
Cliff D. Dedeaux, OTR/L, ATP, CDRS
Occupational Therapist Registered (OTR), 2001Certified Driver Rehabilitation Specialist, 2005Assistive Technology Practitioner, 2005
March, ‘03 – present; Research Associate II, T.K. Martin Center for Technology and Disability, Mississippi State University, responsibilities include rehabilitation driving, seating & mobility, and Mississippi AgrAbility Project
“For people without disabilities, technology makes things easier; for people with disabilities, technology makes things possible” (IBM, 1991).
Agenda
• Introductions and overview• Transportation Information• Introduction to the driving
assessment process• Review of different vehicle
adaptations• General overview of Bioptic
Driving• Discussion
Workshop Goals
Upon completion the participant will be able:
• to list 3 components of the clinical assessment
• to list and describe at least 5 adaptive driving controls
• to describe general use of bioptics lenses for driving
Transportation Facts
• The United States is the most mobile society in the World
• People love the flexibility of such vehicles to travel where and when they want without having to schedule in advance, wait at stations, or endure other constraints
• America’s highways and roads are dominated by personal motor vehicles
• Over 95 percent of all US adult residents drive or ride in personal motor vehicles (Bureau of Transportation Statistics’ Omnibus Survey, 2002)
• The number of vehicles in the US is increasing at an annual rate of almost one and one-half times that of the total population.
• Most people travel to work in a privately owned vehicle (91%)

Personal Mobility
• Personal mobility is the key to true independence– Personal mobility in terms of assistive technology
includes:• Wheelchairs and• Accessible vehicles
• It has social, health, economic, and symbolic functions • Creates true urban and rural connections for everyone.
• Fundamental to opening the door to choices in so
many areas:– Increasing social, community, and vocational participation– Allowing choices about where one lives– Expands choices:
• Who provides medical, dental care, etc• Where to shop• What church to attend• So on and so on

People with disabilities spend their days overcoming barriers. Many find that using a private
vehicle is the essence of personal freedom
(The New York Times, September 20, 1998)
What is a driving evaluation?
• The driver assessment is a complete evaluation of an individual's potential to operate a motor vehicle independently.
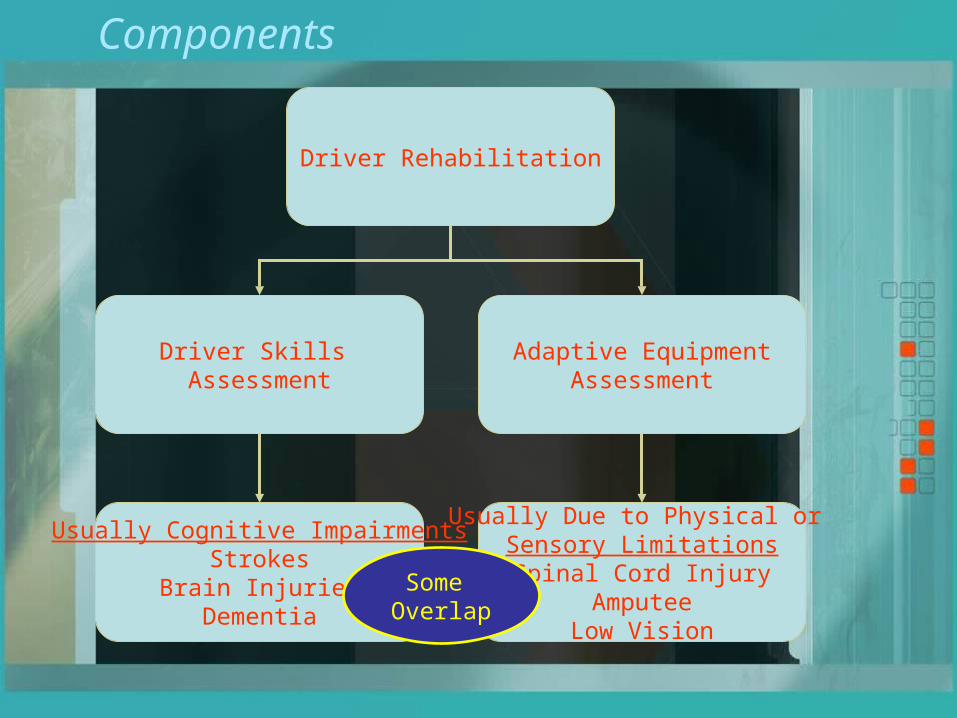
Driver Rehabilitation
Driver Skills Assessment
Adaptive EquipmentAssessment
Usually Cognitive ImpairmentsStrokes
Brain InjuriesDementia
Usually Due to Physical or Sensory LimitationsSpinal Cord Injury
AmputeeLow Vision
Some Overlap
Components

From Start to FinishReferral
Clinical Assessment
Behind-the-Wheel Assessment
Driver Training (as Needed)
Adaptive Equipment Prescription Supplied to
Referral Source
Final Inspection Entails Equipment Inspection and Fitting
Follow up Training in Client’s Vehicle

Referrals
• Sources– Vocational Rehab/OSDP counselors– Worker’s Comp– School Systems– Veteran’s Administration– Doctor’s– Therapist
Clinical Assessment
• Information Intake– Valid driver’s license or Permit
• Ever suspended or revoked? If so, why?– Driving History
• Is the client currently driving (any close calls?)• If not, why and when was the last time?• In what type of traffic environment do they drive?• Any experience with adaptive equipment?• Found at fault for any wrecks? If so, reason?• Any traffic violations?
– Medical History• Where they have been and where are they now in recovery• Current medication? Any side effects?• Try to get the client to paint a picture of how they feel they
are doing; this gives good indication if they have grasp on current abilities and where they are in the recovery process
• Physical Evaluation– Range of motion (active and passive)– Strength available through AROM
Clinical Assessment Cont’d
• Visual Evaluation– Use screener to test:
• Visual acuity both and individual eyes• Color vision• Depth perception• Phoria (eyes working together)• Horizontal peripheral field
Clinical Assessment Cont’d
• Visual-Perceptual/Cognitive Evaluation – Reaction times– Figure ground– Short term memory– Figure completion– Visual attention, scanning, planning, and
sequencing– Visual processing speed– Divided and selective attention– Rapid decision making– Attention shifting– Etc.
Behind-the-Wheel Assessment
• Based on the clinical evaluation results, an in-vehicle evaluation is conducted to determine the type and level of adaptive driving equipment needed, and/or an on-road performance evaluation is conducted to determine a person's driving capabilities in a variety of traffic and roadway environments

Driver’s Training
• Based on the client’s performance during the initial evaluation
• Can vary from a few to several hours• Graded – based on skill level
Parking Lot
Subdivision
County/Country Roads
State Highways
Interstate
Town/City
Low Traffic/Speed
High Traffic/Speed
Little External Stimulus
Unlimited Stimulus
Equipment Prescription
• Mainly states type of equipment and where to install– An example for steering and gas/brake
controls could be as follows:Steering- Vehicle to have zero-effort steering installed- Tripin steering orthotic mounted at the 3 o’clock
position for right hand useAccelerator/brake controls- MPD Push/Ninety Pull Hand Controls with
offset handle and quad wrist support mounted for left hand use
- A brake rod extension may be needed to access a full brake; this will be determined at fitting

Final Fitting
• Conducted at vendor’s workshop• Determine that all prescribed equipment is
provided• Fit or mount equipment in best locations for
access (i.e., switch to be used by elbow, etc.)• Prior to completion, client demonstrates ability to
use equipment in driving environment

Training in Client’s Vehicle
• Usually performed in circumstances where a certain comfort level is desired in client’s vehicle prior to independent driving
• Passenger side training brake is temporarily installed for training purposes and removed at completion of training

Vehicle Types and Adaptive Driving
Equipment
Vehicle Types
• Sedans• SUVs• Minivans• Full-size vans• Trucks

Wheelchair Access for Minivans
Entervan lowered-floor minivan by The Braun Corporation
Vision conversion by Viewpoint Mobility
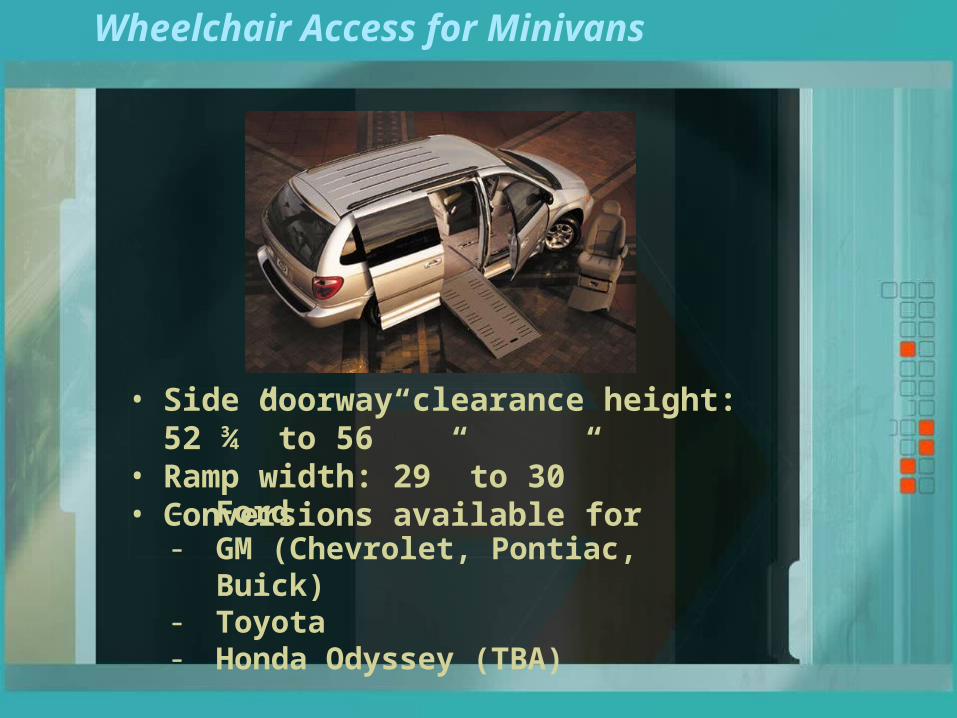
Wheelchair Access for Minivans
• Side doorway clearance height: 52 ¾” to 56”• Ramp width: 29” to 30”• Conversions available for
- Ford- GM (Chevrolet, Pontiac, Buick)- Toyota- Honda Odyssey (TBA)
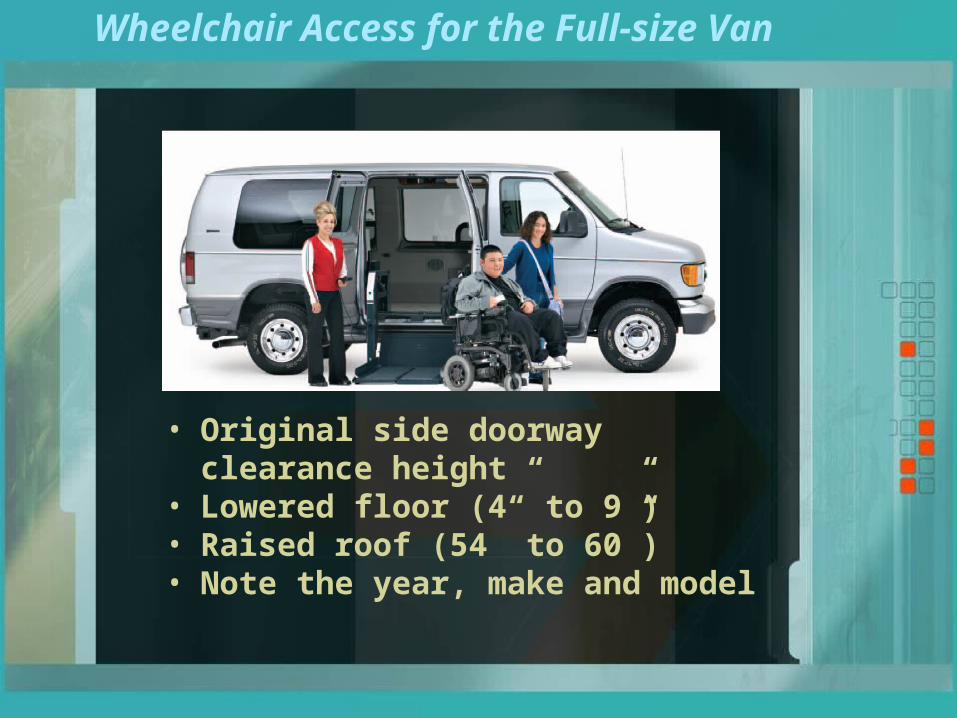
Wheelchair Access for the Full-size Van
• Original side doorway clearance height• Lowered floor (4” to 9”)• Raised roof (54” to 60”)• Note the year, make and model
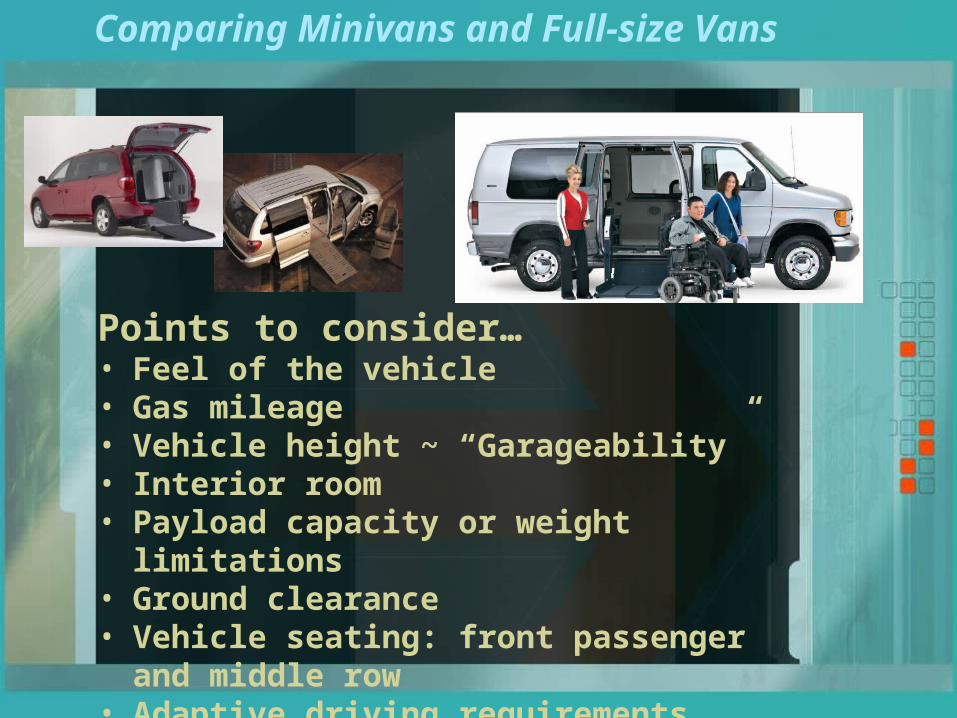
Comparing Minivans and Full-size Vans
Points to consider…• Feel of the vehicle• Gas mileage• Vehicle height ~ “Garageability”• Interior room• Payload capacity or weight limitations• Ground clearance• Vehicle seating: front passenger and middle row• Adaptive driving requirements
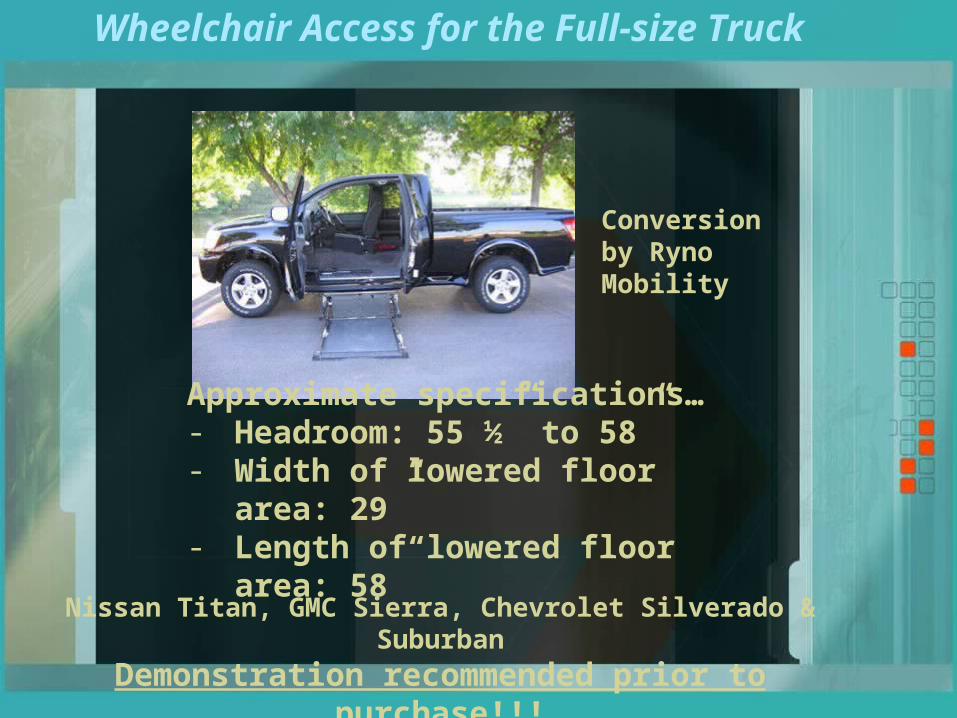
Nissan Titan, GMC Sierra, Chevrolet Silverado & Suburban
Demonstration recommended prior to purchase!!!
Conversion by Ryno Mobility
Approximate specifications…- Headroom: 55 ½” to 58”- Width of lowered floor area: 29”- Length of lowered floor area: 58”
Wheelchair Access for the Full-size Truck

Personal Access
Notched transfer board
EZ Transfer by Access Unlimited

Personal Access
Glide ‘N Go by Access Unlimited
TAS System by Bruno
Transfer Seat Base by VMI/Ricon

Manually operated wheelchair tiedowns
Q5001 System by Q-Straint
Some points to consider…• Availability of tiedown attachment points• Knowledge and ability for correct use
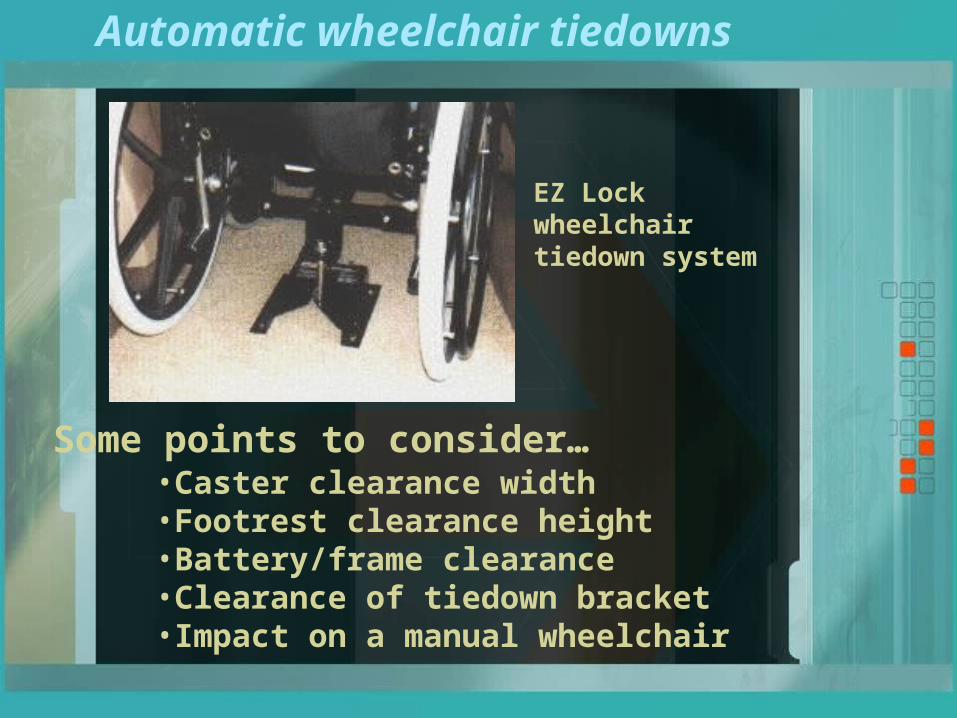
Automatic wheelchair tiedowns
EZ Lock wheelchair tiedown system
•Caster clearance width•Footrest clearance height•Battery/frame clearance•Clearance of tiedown bracket•Impact on a manual wheelchair
Some points to consider…
Primary Driving Controls
• Steering
• Accelerator
• Brake

Steering Controls
Column extensions and different-sized steering wheels
Products shown are by Drive-Master Corporation
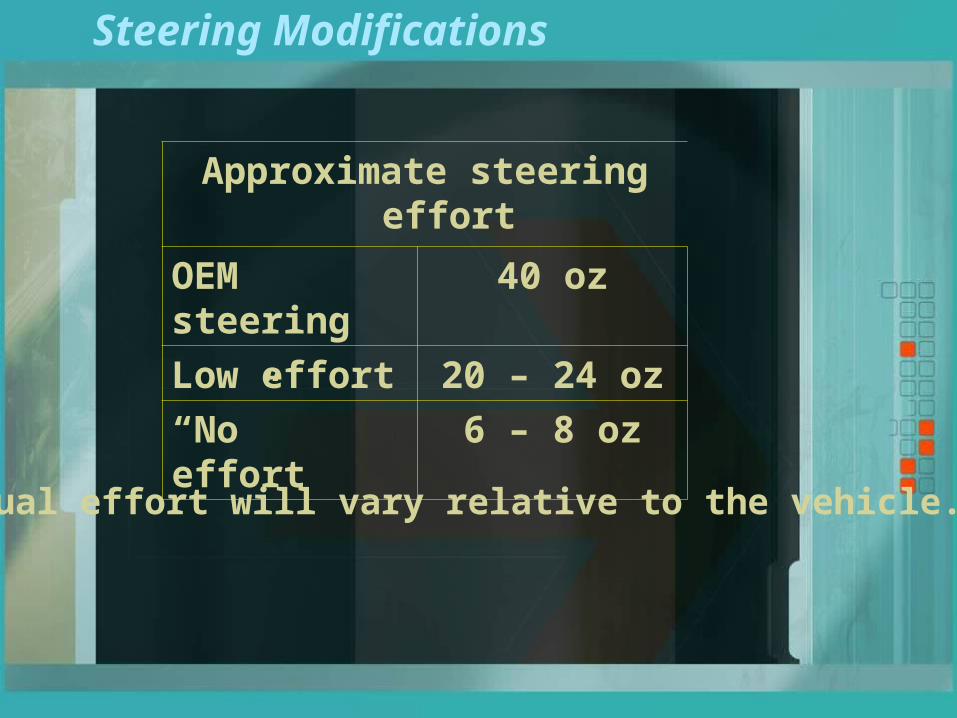
Steering Modifications
Approximate steering effort
OEM steering 40 oz
Low effort 20 – 24 oz
“No” effort 6 – 8 oz
Actual effort will vary relative to the vehicle.

Steering Controls
Foot Steering System by Drive-Master Corporation

Steering Controls
Digital SteeringPictured is the AEVIT W-Series by EMC
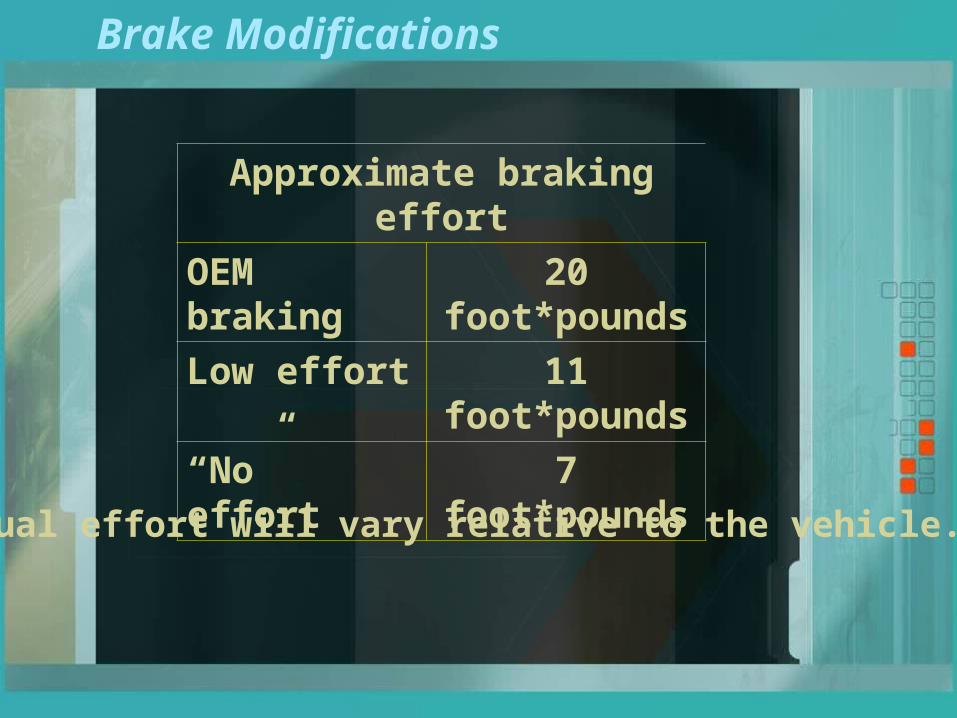
Brake Modifications
Approximate braking effort
OEM braking 20 foot*pounds
Low effort 11 foot*pounds
“No” effort 7 foot*pounds
Actual effort will vary relative to the vehicle.
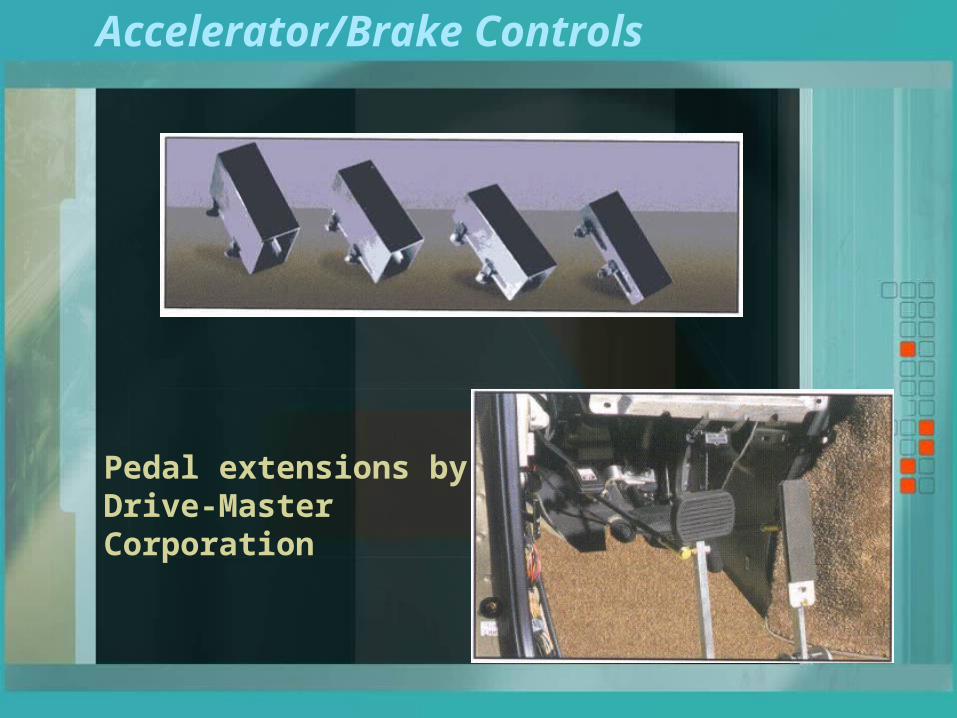
Accelerator/Brake Controls
Pedal extensions byDrive-Master Corporation

Accelerator Controls
Left Foot Accelerator Pedal by FujiAuto
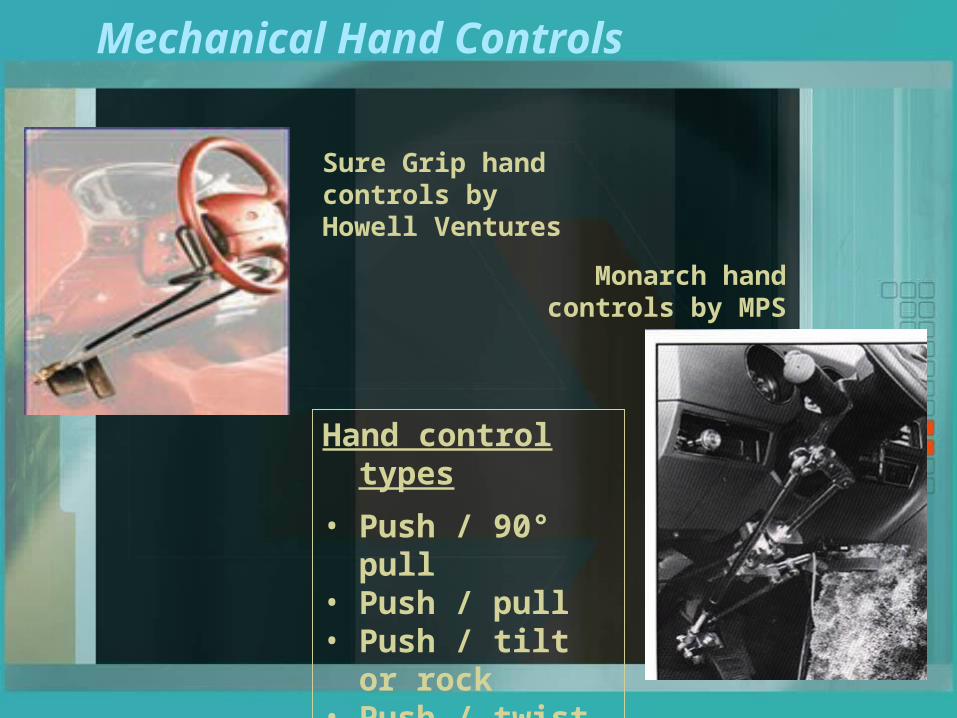
Mechanical Hand Controls
Monarch hand controls by MPS
Sure Grip hand controls by Howell Ventures
Hand control types
• Push / 90° pull• Push / pull• Push / tilt or rock• Push / twist

MPD Hand Controls on Utility Vehicles
Big Country Cub Cadet
John Deere Gator Golf Cart
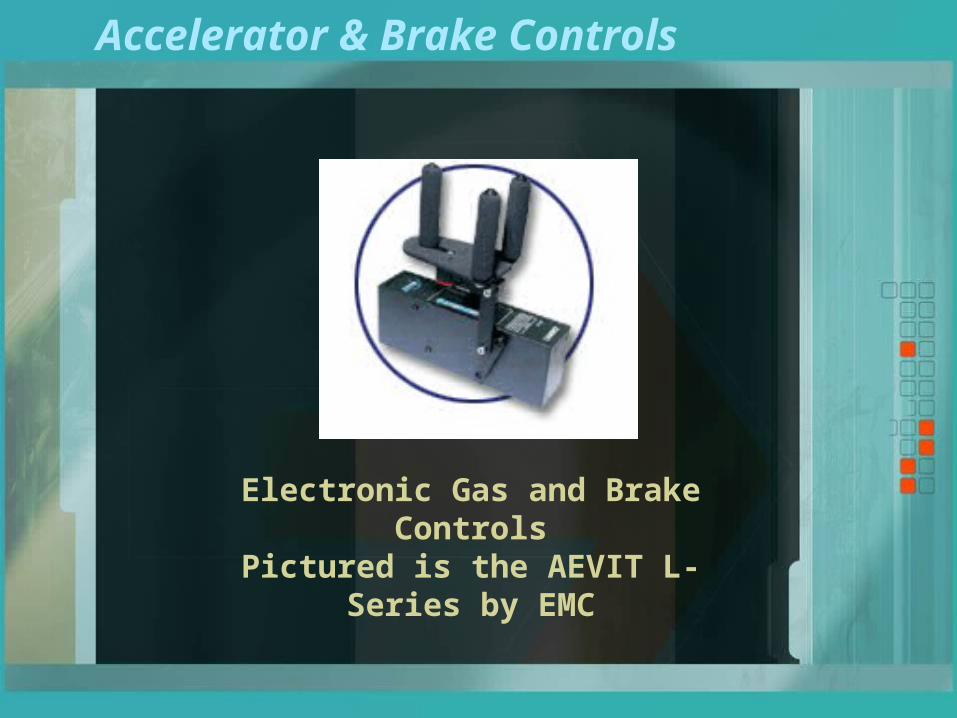
Accelerator & Brake Controls
Electronic Gas and Brake ControlsPictured is the AEVIT L-Series by EMC
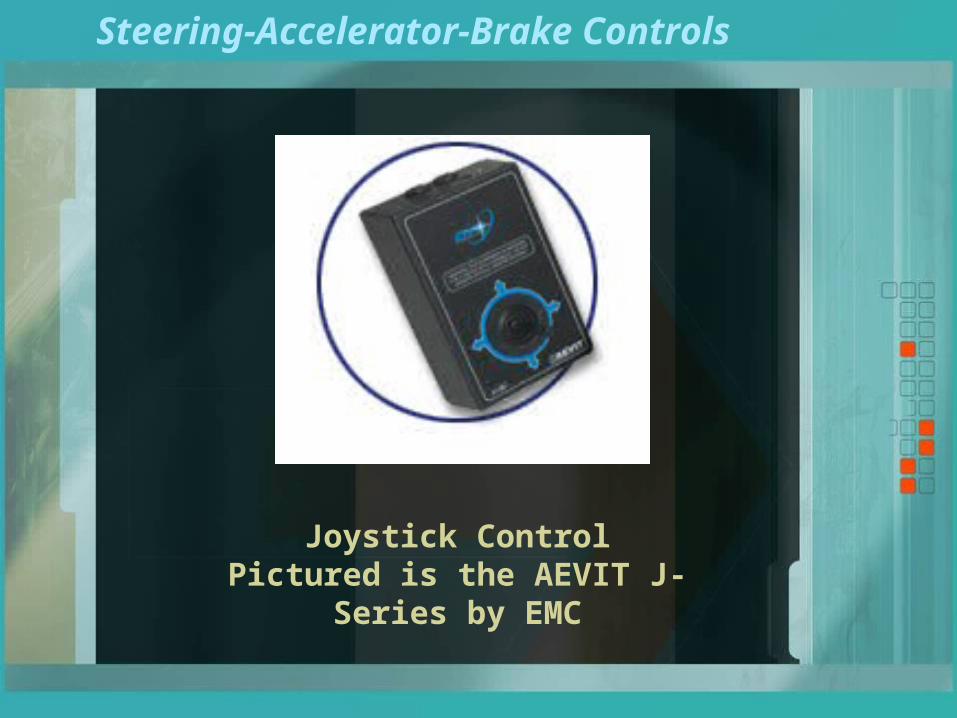
Steering-Accelerator-Brake Controls
Joystick ControlPictured is the AEVIT J-Series by EMC

Steering-Accelerator-Brake Controls
Scott Driving System by dSI
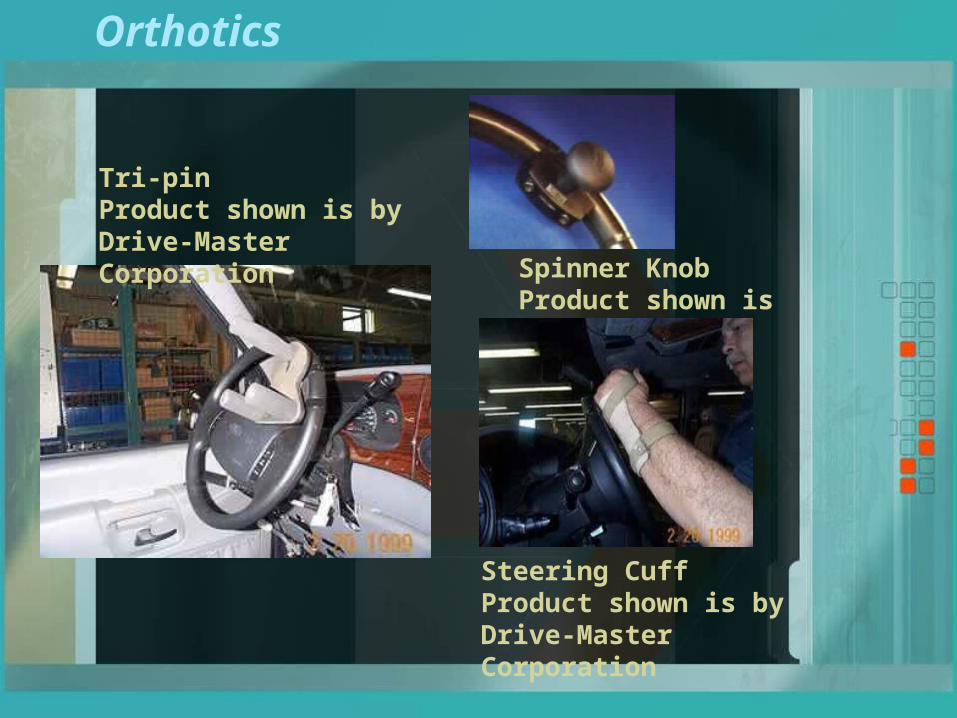
Orthotics
Tri-pinProduct shown is by Drive-Master Corporation
Spinner KnobProduct shown is by DSI
Steering CuffProduct shown is by Drive-Master Corporation

Secondary Controls
• Turn signals• Horn• Lights/Dimmer switch• Gear shifter• Park Brake• Etc.

Secondary Controls
Quad Key Turner by MPD
Right Hand Turn Lever by MPD
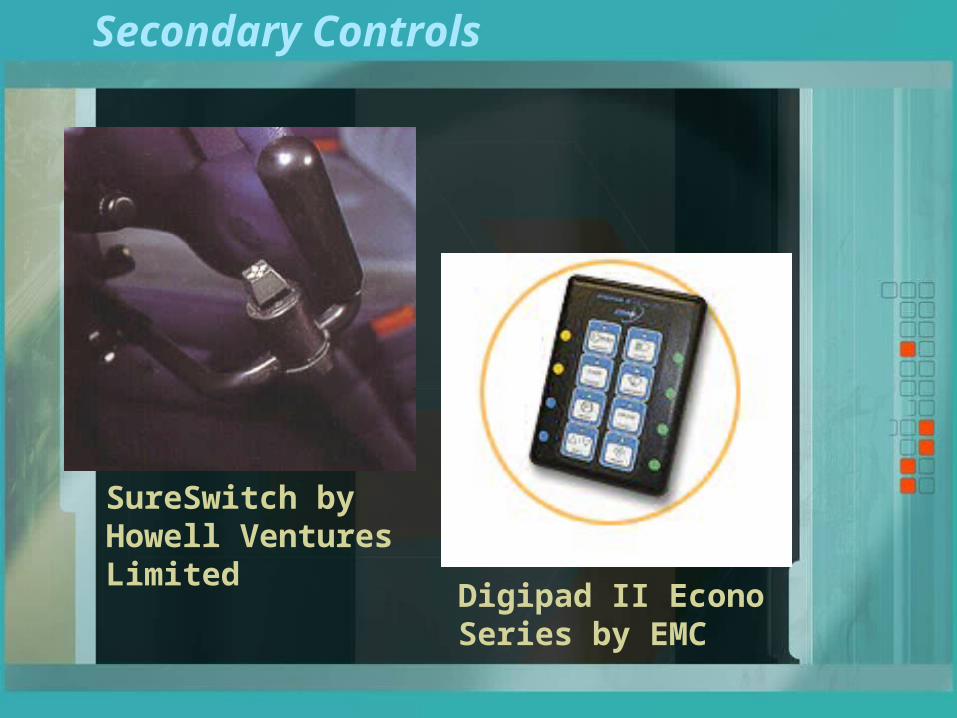
Secondary Controls
SureSwitch by Howell Ventures Limited
Digipad II Econo Series by EMC

Secondary Controls
Remote switch options
• Scanning
• Voice recognition
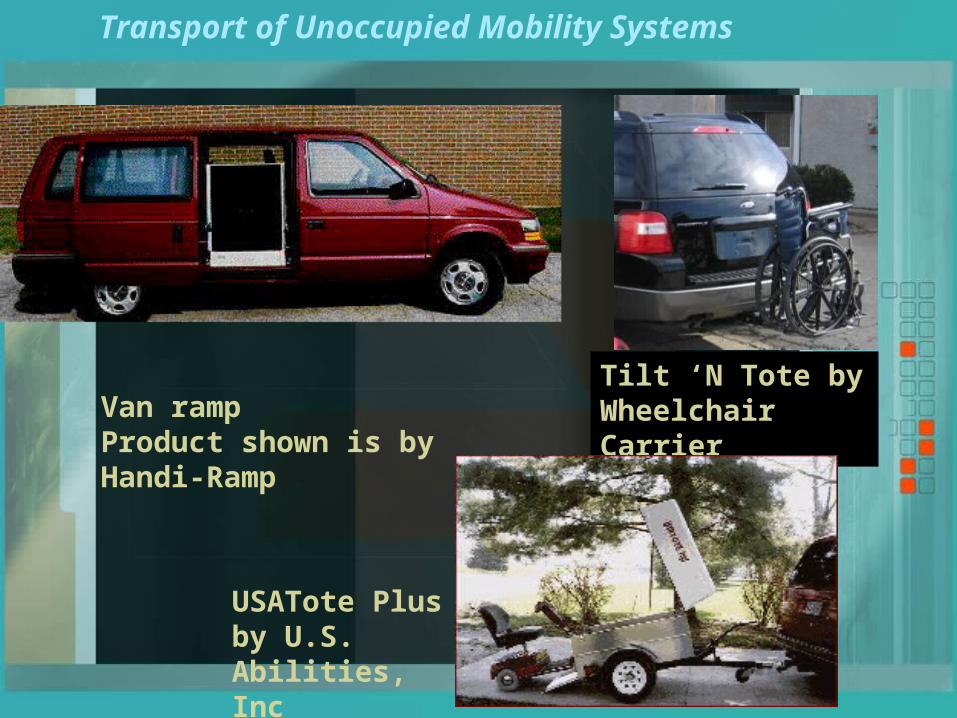
Transport of Unoccupied Mobility Systems
Van rampProduct shown is by Handi-Ramp
Tilt ‘N Tote by Wheelchair Carrier
USATote Plus by U.S. Abilities, Inc

Transport of Unoccupied Mobility Systems
Products shown are by Bruno Independent Living Aids
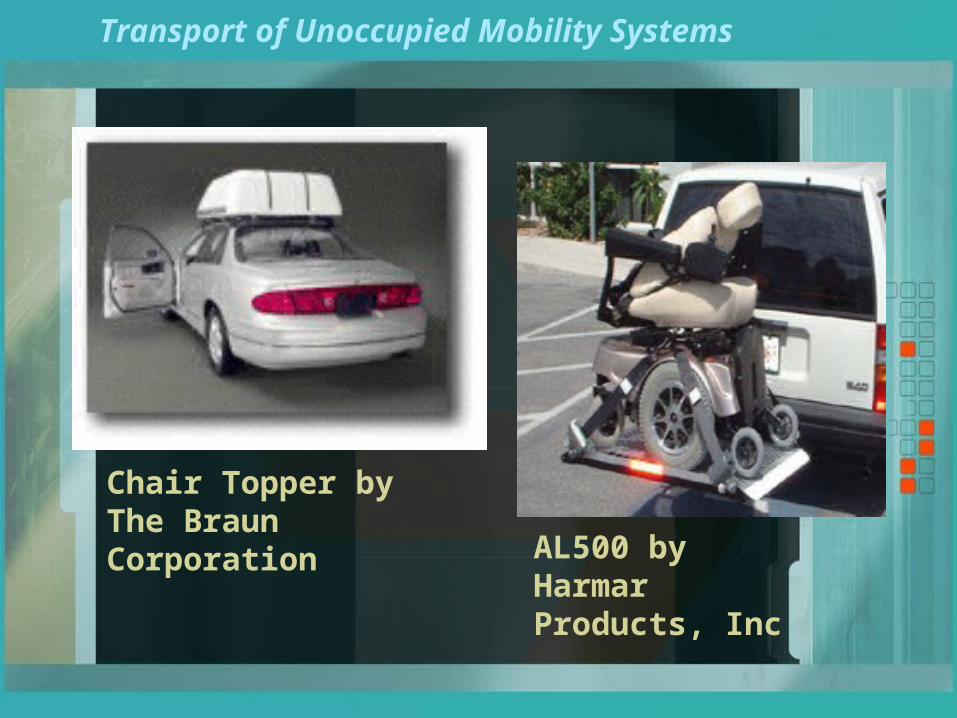
Transport of Unoccupied Mobility Systems
AL500 by Harmar Products, Inc
Chair Topper byThe Braun Corporation

Products shown are by Bruno Independent Living Aids
Transport of Unoccupied Mobility Systems

Driving With Bioptic Lenses
Bioptic Driving
The Premise…Vision is the primary sensory input for
driving…
…but acuity is only one aspect of vision
Bioptic lenses applied to the Driving Task
• Central vision vs. Visual field
• Fine detail vs. Gross vision
Bioptic Driving
Common Misconceptions
• Bioptics are not a “cure” for low vision
• Bioptics are not for constant use when driving

General eligibility criteria
• Distance acuity – best corrected with conventional lenses
• Acuity using bioptic lenses• Nature of vision diagnosis – expected changes
in vision• Visual field (including central vision)• Head, neck and eye movement• Maximum lens power• Training…both in the use of the bioptic lens
and for driving
Training in the use of the Bioptic Lens
Recommended by Mississippi Dept. of Public Safety• Tracking/Saccades• Spotting• Visual Memory• Peripheral Awareness
Orientation and Mobility Training• General use of bioptic lenses for the everyday
environment• Use in the driving environment
– Judging speed & distance– Use of mirrors– Critical object/hazard awareness– Maintaining peripheral awareness

The Assessment Procedure
• Interview
- Medical and driving history
• Active ROM & strength
• Reaction times
• Passenger in-vehicle
• Behind-the-wheel assessment
The Training Procedure
• Classroom-based driver education
- AAA Driver Ed series
- Rules of the road
• Behind-the-wheel training - Minimum training time
- Progression from low to high complexity
- Exposure to multiple driving conditions
- May include local training
Scope of License
The Driver License remains valid while the Licensee drives through other States.
However, if the Licensee moves to a different State, then they fall under the Driver Licensure Guidelines specific to that particular State.

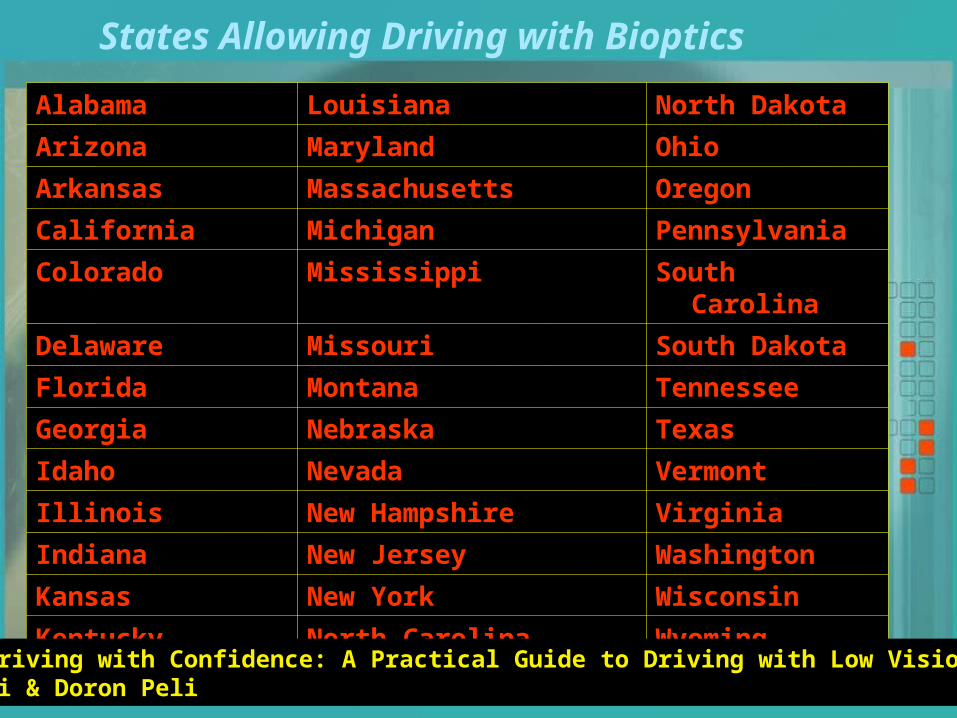
States Allowing Driving with Bioptics
Alabama Louisiana North Dakota
Arizona Maryland Ohio
Arkansas Massachusetts Oregon
California Michigan Pennsylvania
Colorado Mississippi South Carolina
Delaware Missouri South Dakota
Florida Montana Tennessee
Georgia Nebraska Texas
Idaho Nevada Vermont
Illinois New Hampshire Virginia
Indiana New Jersey Washington
Kansas New York Wisconsin
Kentucky North Carolina Wyoming
Ref: Driving with Confidence: A Practical Guide to Driving with Low Vision by Eli & Doron Peli
Resources
The Association for Driver Rehabilitation Specialists (ADED)www.driver-ed.org
National Mobility Equipment Dealers Associationwww.nmeda.org
Bioptic driving…www.nhtsa.dot.gov/people/injury/olddrive/OlderDriversBook/pages/Mississippi.html
www.lowvisioncare.com/visionlaws.htm
www.biopticdriving.org

Contact Information
T.K. Martin Center for Technology and Disability
Box 9736
Mississippi State, MS 39762
Phone: 662-325-1028