dr.maninder ahuja director ahuja nursing home & infertility centre faridabad vice presindet...
TRANSCRIPT

DR.MANINDER AHUJADirector AHUJA NURSING HOME & INFERTILITY CENTREFARIDABAD
• VICE PRESINDET FOGSI• PRESIDENT ELECT INDIAN MENOPAUSE SOCIETY• DEPUTY SECRETARY GENERAL SAFOMS • BOOK “STEP BY STEP MANAGEMENT OF MENOPAUSE”• THREE CHAPTERS IN JEFFCAOTE BOOK OF GYNAECOLOGY
UPDATED IN 2008• CHAPTERS IN “ 3RD EDITION OF FOGSI’S Priciples& Practice Of
Obstetrics &Gynaecology for Post Graduates”• Three Chapters in “Operative Obst.&Gynaecology”editors dr.Randhir
Puri&Dr.Narendra Malhotra • Editor of Manual on “ Prevention of Cervical Cancer”
• DVD ON “PRESCRIPTION OF EXERCISE FROM ADOLESCENT
TO MENOPAUSE”• Dvd on “EXERCISE IN PREGNANCY”• EDUCATIONAL CD ON MENOPAUSE• PRESIDENT FARIDABAD OBST&GYNAE SOCIETY• CHAPTER SECRETARY INDIAN MENOPAUSE SOCIETY
(FARIDABAD)• CHAIRPERSON PUBLIC AWARENESS COMMITTEE OF IMS• CHAIRPERSON GERIATRIC GYNAECOLOGICAL COMMITTEE
OF FOGSI
04/19/231DR.Maninder Ahuja VP FOGSI

04/19/23DR.Maninder Ahuja VP FOGSI2
DVDs ONEXERCISE

Mid lifeNew Beginnings
North ZoneYuva FOGSI2 0 1 3
22nd Nov to 24th Nov Venue- Hotel Radisson Amritsar
04/19/233 DR.Maninder Ahuja VP FOGSI

04/19/23DR.Maninder Ahuja VP FOGSI4
SCREENING TESTS PRERUISITES
The ultimate proof of success of cervical screening is its ability to reduce the incidence of and deaths from cervical cancer in a cost-effective manner.
One of the prerequisites for effective screening is the availability of a suitable cervical screening test that has adequate sensitivity and specificity for detection of precancerous lesions and that yields reproducible results.
Such a test should be cheap, simple, and easy to apply; without side effects or complications; as painless as possible; and socio culturally acceptable.
R. Sankaranarayanana,T, L. Gaffikin , M. Jacobc , J. Sellorsd , S. Roblesea International Agency for Research on Cancer (IARC), 150 cours Albert Thomas, 69372 Lyon Cedex 08, France b JHPIEGO, Baltimore, MD, USAcEngenderHealth, New York, NY, USA dPATH (Program for Appropriate Technology in Health), Seattle, WA, USA e PAHO (Pan American Health Organization), Washington, DC, USA
04/19/23DR.Maninder Ahuja VP FOGSI5

EARLY DIAGNOSIS AND MANAGEMENT OF PRECANCEROUS LESIONS IS GOING
TO SAVE MANY LIVES!
Every seven min one woman is dying of cervical cancer in
India.
04/19/236 DR.Maninder Ahuja VP FOGSI
Mother and daughter dyad
Every seven minute one mother is dying of Cervical cancer !
04/19/237 DR.Maninder Ahuja VP FOGSI

Cervical cancer screening –Indian perspective
India is a diverse country with varied scenarios
A uniform strategy can not be implemented75% of population is in rural or low resource
setting25% of population is in urban high resource
settingAny new program needs to be integrated in
the existing healthcare services
AOGIN guidelines04/19/238 DR.Maninder Ahuja VP FOGSI
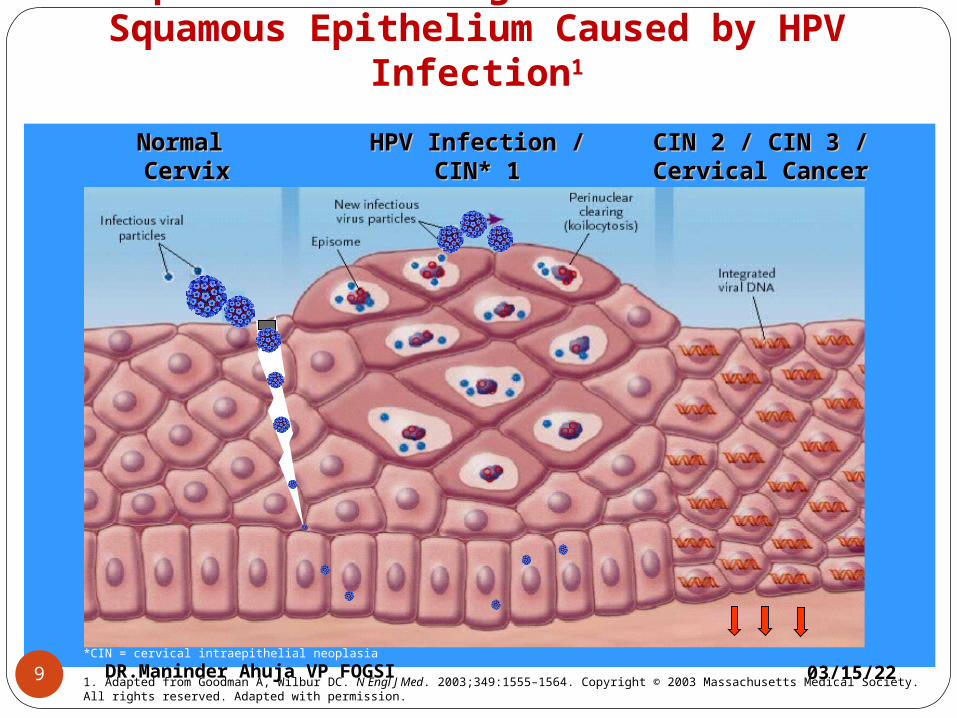
Spectrum of Changes in Cervical Squamous Epithelium Caused by HPV
Infection1
Normal Normal CervixCervix
HPV Infection /HPV Infection /CIN* 1CIN* 1
CIN 2 / CIN 3 /CIN 2 / CIN 3 /Cervical CancerCervical Cancer
*CIN = cervical intraepithelial neoplasia
1. Adapted from Goodman A, Wilbur DC. N Engl J Med. 2003;349:1555–1564. Copyright © 2003 Massachusetts Medical Society. All rights reserved. Adapted with permission.
04/19/239 DR.Maninder Ahuja VP FOGSI

FOR DEVELOPMENT OF PRECANCEROUS LESIONS
OF CXWe need infection with HPVPersistence of virusLeads to precancerous lesionsIf they don’t clear then invasive cancerThere is no viremia of natural infectionIt is only from local tissue changes that
we can diagnose premalignant lesionsSo screening involves exfoliated cells
from TZ, from endocervical glands, and HPV DNA Presenct in tissue
04/19/23DR.Maninder Ahuja VP FOGSI10

04/19/2311 DR.Maninder Ahuja VP FOGSI

Screening methods available
VISUAL INSPECTION: VIA and VILLI (subjective visual inspection with acetic acid &lugol’s iodine
Cytology : Pap Smear, LBC (Liquid based cytology)
HPV DNA Test: High Risk HPV DNA Test / HPV Typing
Follow up with colposcopy or directed biopsy or treat with ablative methods or excisional methods
04/19/2312 DR.Maninder Ahuja VP FOGSI

04/19/23DR.Maninder Ahuja VP FOGSI13
When to start screening?
Till What Age?
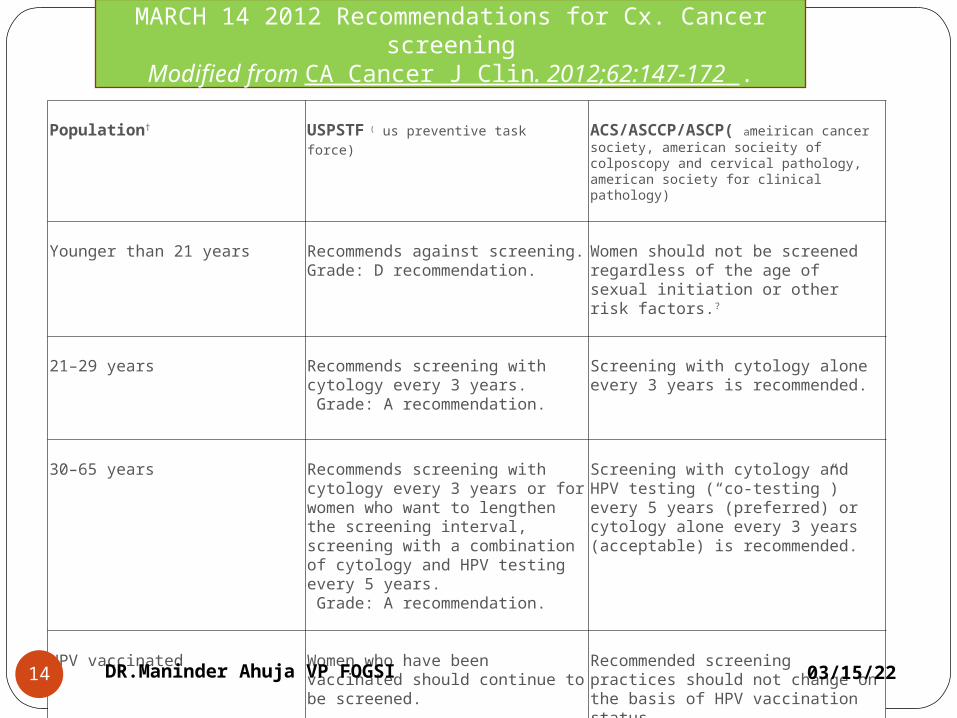
Population†
USPSTF ( us preventive task force) ACS/ASCCP/ASCP( ameirican cancer
society, american socieity of colposcopy and cervical pathology, american society for clinical pathology)
Younger than 21 years
Recommends against screening.Grade: D recommendation.
Women should not be screened regardless of the age of sexual initiation or other risk factors.?
21–29 years
Recommends screening with cytology every 3 years. Grade: A recommendation.
Screening with cytology alone every 3 years is recommended.
30–65 years
Recommends screening with cytology every 3 years or for women who want to lengthen the screening interval, screening with a combination of cytology and HPV testing every 5 years. Grade: A recommendation.
Screening with cytology and HPV testing (“co-testing”) every 5 years (preferred) or cytology alone every 3 years (acceptable) is recommended.
HPV vaccinated
Women who have been vaccinated should continue to be screened.
Recommended screening practices should not change on the basis of HPV vaccination status.
MARCH 14 2012 Recommendations for Cx. Cancer screening
Modified from CA Cancer J Clin. 2012;62:147-172 .
04/19/2314 DR.Maninder Ahuja VP FOGSI

Older than 65 years
Recommends against screening women who have had adequate prior screening¶ and are not otherwise at high risk for cervical cancer. Grade: D recommendation.
Women with evidence of adequate negative prior screening¶ and no history of CIN2+ within the last 20 years should not be screened. Screening should not be resumed for any reason, even if a woman reports having a new sexual partner.
After hysterectomy
Recommends against screening in women who have had a hysterectomy with removal of the cervix and who do not have a history of a high-grade precancerous lesion (ie, CIN 2 or 3) or cervical cancer.Grade: D recommendation
Women of any age following a hysterectomy with removal of the cervix who have no history of CIN2+ should not be screened for vaginal cancer. Evidence of adequate negative prior screening is not required. Screening should not be resumed for any reason, including if a woman reports having a new sexual partner.
high-risk populations who may need more intensive or alternative screenin.
These special populations include women 1) with a history of cervical cancer, 2) who were exposed in utero to diethylstilbestrol (DES), and 3) who are immune-compromised (eg, infection with human immunodeficiency virus).
04/19/2315DR.Maninder Ahuja VP FOGSI

WHO Guidelines for screening cancer cervix
•New programmes should start screening women aged 30 years or more, and include younger women only when the highest-risk group has been covered.
•Existing organized programmes should not include women less than 25 years of age in their target populations.
•If a woman can be screened only once in her lifetime, the best age is between 35 and 45 years.
contd……
04/19/2316 DR.Maninder Ahuja VP FOGSI

Contd….
•For women over 50 years, a five-year screening interval is appropriate.• In the age group 25-49 years, a three-year interval can be considered if resources are available.•Annual screening is not recommended at any age.• Screening is not necessary for women over 65 years, provided the last two previous smears were negative. 04/19/2317 DR.Maninder Ahuja VP FOGSI

04/19/2318 DR.Maninder Ahuja VP FOGSI

What is critical for Pap smear:
•Accurate sampling.
•Adequate preservation.
•Complete evaluation.
•Meaningful interpretation.
04/19/2319 DR.Maninder Ahuja VP FOGSI

WHEN?8th – 12th DAY OF MC
CERVICAL MUCUS IS ABUNDANT
EXT. OS IS WIDE OPEN
NO RECENT CERVICAL EXAM. / EXPLORATION / NO VAGINAL EXAM. WITH A LUBRICANT.
04/19/2320 DR.Maninder Ahuja VP FOGSI
Instruments and Materials Required
Sterile Cusco’s speculum
Good light source
Pair of gloves
Ayre’s spatula / endocervical brush
Glass Slides / pencil
Coplin’s Jar
95% ethly alcohol
Cytology form
04/19/2321 DR.Maninder Ahuja VP FOGSI

collection devices Plastic or wooden Ayre’s spatula
Cervix brush
Plastic broom
Ordinary wooden tongue blade
Cotton swab not to be used
04/19/2322 DR.Maninder Ahuja VP FOGSI

SAMPLING DEVICES
04/19/2323 DR.Maninder Ahuja VP FOGSI
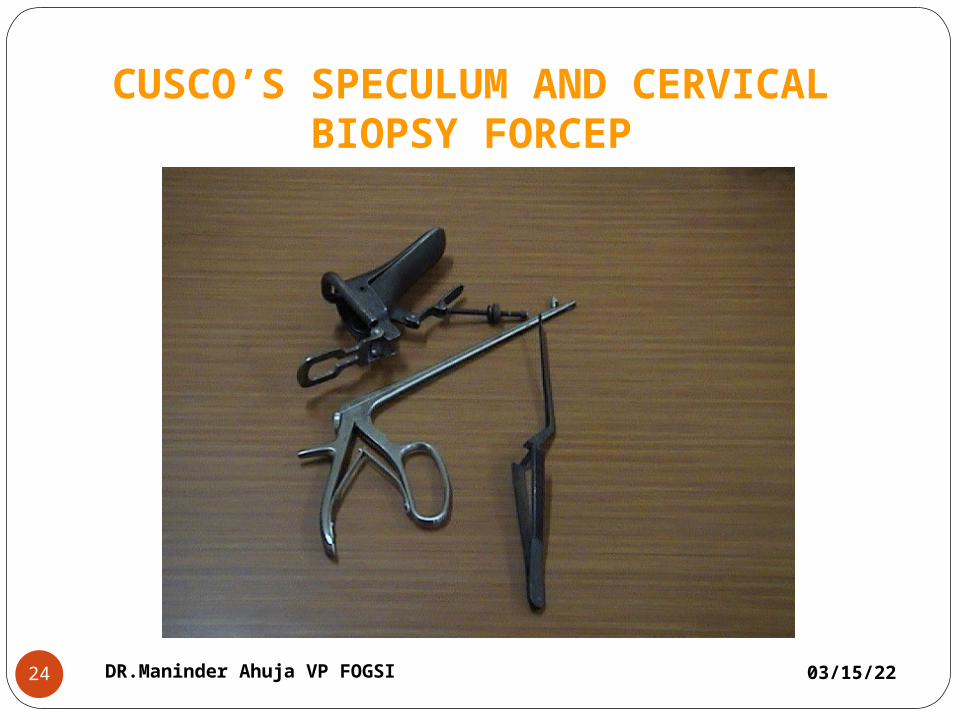
CUSCO’S SPECULUM AND CERVICAL BIOPSY FORCEP
04/19/2324 DR.Maninder Ahuja VP FOGSI

04/19/2325 DR.Maninder Ahuja VP FOGSI

• Cervix is visualized using a Cusco’s speculum
• Obscuring elements like blood or mucus is gently removed
• The long arm of the spatula or mid part of the brush is inserted into the cervical canal and is gently rotated 360o so that the entire TZ is sampled.
• The device is removed and the material obtained is immediately transferred onto a numbered glass slide taking care to cover 75% of the surface area and on one side only.
• The slide is immediately put into a coplin jar containing the fixative 95% ethanol. Alternatively use spray fixative at a distance of 12 inches, to avoid disrupting the cells.
• Fixation time: Atleast 30 minutes.
How to take a Conventional pap Smear
04/19/23 27DR.Maninder Ahuja VP FOGSI
Option 1 Option 2 Option 3
No.
No.
No.
04/19/2328 DR.Maninder Ahuja VP FOGSI

04/19/23DR.Maninder Ahuja VP FOGSI29
It is better to have two slides one with brush and one with spatula

04/19/2330 DR.Maninder Ahuja VP FOGSI
Preservative
95% ethinyl Alcohol or 80% Isopropanol

Collection of Liquid based Cytology Samples
The cervex brush is used to collect the sample and the manufacturer’s instructions are to be followed.Rotated 5-9times
Central bristles inserted into cervical canal and lateral bristles fully bend against Ectocervix
No smear needs to be prepared and the entire sample collected by the brush is transported to the laboratory in the fixative vial after proper labelling
04/19/23 31DR.Maninder Ahuja VP FOGSI

SAMPLE COLLECTION PROCEDURE – LIQUID BASED CYTOLOGY
04/19/2332 DR.Maninder Ahuja VP FOGSI

SAMPLE COLLECTION - HPV HR HYBRID CAPTURE 2
04/19/2333 DR.Maninder Ahuja VP FOGSI
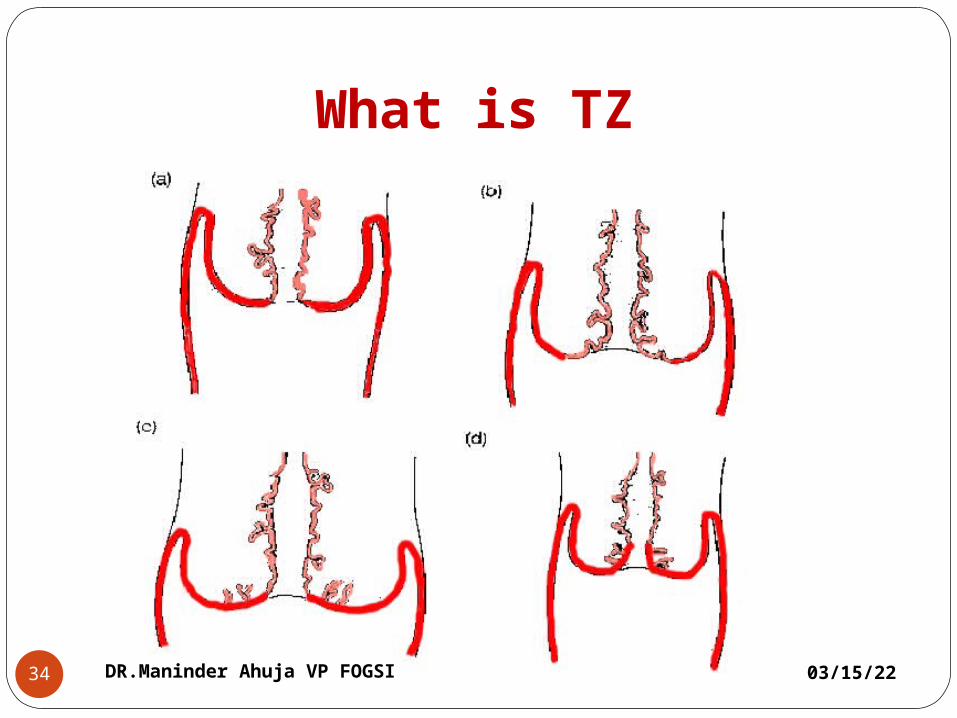
What is TZ
04/19/2334 DR.Maninder Ahuja VP FOGSI
Comparison Of LBC and PAP
CONVENTIONAL SMEAR
Heterogeneous Graphic cell
localization 300-500 k cells/slide Variable fixation Thick uneven groups need frequent
focusing Dirty background Variable preservation
LIQUID BASED SMEARHomogeneous Random cell
presentation 50-70 k cells/slide Uniform fixation Uniform thin layerNot single cell
monolayers Clean background Well preserved cells
04/19/2335 DR.Maninder Ahuja VP FOGSI

Correlation between different terminologies
Dysplasia terminology(reagar,1953)
Original CIN terminology(richart,1968)
TBS(SIL) terminology,1991
Modified CIN terminology
normal normal With in normal limis.Benign cellular changes
normal
Atypia Koilocytic atypia,flat condyloma without epithelial changes
ASCUS/AGUS/LSIL
Low grade CIN
Mild dysplasia or mild dyskaryosis
CIN-1 LSIL Low grade CIN
Moderate dysplasia or moderate dyskaryosis
CIN-2 HSIL High grade CIN
Severe dysplasia or severe dyskaryosis
CIN-3 HSIL High grade CIN
Carcinoma in situ
CIN-3 HSIL High grade CIN
Invasive carcinoma
Invasive Invasive Invasive
04/19/2336 DR.Maninder Ahuja VP FOGSI

Screening test
Sensitivity Specificity characteristics
Cytology Low to moderate44-78%
high 91-96% Requires health based infrastructure,laboratory , training, subjective
HPV DNA High(66-100%) Moderate (61-90%)
Lab based, objective,repruducible, expensive
Visual inspection
Low technology, low cost ,linkage to immediate treatment
VIA Moderate 67-79%
Low 49-86% Suitable for low resource settings
VILLI Moderate high 78-98%
Moderate 73-93%
Properties and charactristics of different screening methods
04/19/2337 DR.Maninder Ahuja VP FOGSI

Poor-Moderate Sensitivity of Poor-Moderate Sensitivity of CytologyCytology
04/19/2338 DR.Maninder Ahuja VP FOGSI

Sensitivity of a single HPV test
04/19/2339 DR.Maninder Ahuja VP FOGSI

Cyto. Dx & Associated High Grade Lesions
Incidence CIN 2/3 Invasive Ca
ASC-CU 2.5 to 5.0% 5-10% <0.1%
LSIL 1.5 to 2.0% 15-30% 0.1-0.2%
HSIL 0.5 % 70% 1-2%
Glandular abnormalities: Colposcopy+ ECC is recommended
04/19/2340 DR.Maninder Ahuja VP FOGSI
Disadvantages of CytologySensitivity of single smear is 51% & specificity is 98%.
Expensive, Requires infrastructure and training2/3rd of false negatives are due to errors of sampling. 40-50% cancers in cases screened within 5 years . 15-42% fail to obtain evaluation. 10-18% are never notified.
04/19/2341 DR.Maninder Ahuja VP FOGSI