dr.s ramakrishnan - apidsc · s ramakrishnan md, dm, facc secretary csi t db & pcsi executive...
TRANSCRIPT

S Ramakrishnan MD, DM, FACC
•Secretary CSI – DB & PCSI
•Executive Editor, Indian Heart Journal
•Published 100 papers in indexed journals
•Awarded DP Basu award, Sujoy B Roy, Col Chopra awards, Best
paper awards at ACC, AEPC, APPCS, PCSI, CSI
Additional Professor of Cardiology
AIIMS, New Delhi
Evidence Based Selection of Statin: Case Based Approach
S RAMAKRISHNAN
ADDITIONAL PROF OF CARDIOLOGY
AIIMS, NEW DELHI

What has changed in ‘NEW’ guidelines?
Focus on ASCVD Risk Reduction
No Support For Use Of Specific LDL-C or Non-HDL
C Targets
Global Risk Assessment For Primary Prevention
Safety Recommendations Role of Biomarkers Fupture Updates

Siblings can have similar look but not the talent!
Drugs can have same structure and Mechanism of Action, but
not effects/ADRs!
ADR: Adverse Drug Reactions

So wait and think before prescribing statin to your patient

Four major statin benefit groups 6
Individuals with clinical ASCVD Primary elevations of LDL-C > 190
mg/dl
Diabetic patients aged 40-75 with LDL-C 70-189 mg/dl and without
clinical ASCVD
Individuals without ASCVD or diabetes aged 40-75 yr with LDL-C 70-189 mg/dl and with estimated
10-yr ASCVD risk > 7.5%

Case 1: 52-year-old with H/O ACS 1 year back. Smoker, no known risk factors. TC 210, TG 220, LDL 150, HDL 40
a. 1 mg Pitavastatin
b. 40 mg Atorvastatin
c. 10 mg Rosuvastatin
d. 20 mg Simvastatin
Has anything changed with ATP IV ?


Aim to Reduce RISK … not at Target levels

HIGH INTENSITY THERAPY MODERATE INTENSITY THERAPY
LOW INTENSITY THERAPY
Daily dose lowers LDL-C on average,by approximately ≥50%
Daily dose lowers LDL –C on average, by approximately 30-50%
Daily dose lowers LDL –C <30%
Atorvastatin (40) 80 mg Atorvastatin 10 (20) mg Simvastatin 10 mg
Rosuvastatin 20 (40) mg Rosuvastatin (5) 10 mg Pravastatin 10-20 mg
Simvastatin 20-40 mg Lovastatin 20 mg
Pravastatin 40 (80) mg Fluvastatin 20-40 mg
Lovastatin 40 mg Pitavastatin 1 mg
Fluvastatin XL 80 mg
Fluvastatin 40 mg bid
Pitavastatin 2-4 mg
ATP IV: Intensity of Statin Therapy

Major Secondary Prevention Studies On Statin

TNT: High Vs Low Dose Atorvastatin Primary Endpoint
22% risk reduction by 80 mg Vs 10 mg atorvastatin p<0.001
Waters DD et al. N Engl J Med 2005;352:1425-35
Primary Endpoint: Major cardiovascular event defined as coronary heart death (CHD),
nonfatal MI, resuscitated cardiac arrest, and fatal or nonfatal stroke
High dose atorvastatin is more effective for CV protection in stable IHD patients

Events Rates
RR Atorva 80 Prava 40
17% 1.9% 2.2%
18% 6.3% 7.7%
14% 12.2% 14.1%
16% 22.4%* 26.3%*
30 Days
90 Days
180 Days
End of Follow-up
PROVE IT TIMI 22: High Vs Moderate Intensity Statin : Primary Endpoint
Atorvastatin 80mg Better
0.5 0.75 1.0 1.25 1.5
Pravastatin 40mg Better *2-year event rates
High dose atorvastatin is more beneficial than moderate intensity statin for secondary prevention
Cannon CP et al. N Engl J Med 2004;350:1495-504

Time since randomization (years)
SPARCL Study : Primary End Point
*Adjusted
Fatal/ nonfatal stroke
(%)
0
0 1 2 3 4 5 6
16
12
8
4
16% RRR* HR 0.84 (0.71–0.99)
p=0.03
Placebo
Atorvastatin
NNT = 46 patients for 5 years
Primary outcome
SPARCL Investigators. N Engl J Med. 2006;355:549-59.
High dose atorvastatin reduces CV events in patients with stroke or TIA

Why No targets in Prevention?
ATP IV

Gi i g up the Goals…
▪ Many clinicians use targets such as LDL–C <70 mg/dL
▪ However, the RCT evidence clearly shows that ASCVD events are reduced by using the maximum tolerated statin intensity in those groups shown to benefit.
▪ After a comprehensive review, no RCTs were identified that titrated drug therapy to specific LDL–C or non-HDL–C goals to improve ASCVD outcomes.

No to Target based approach???
▪ There Is No Scientific Basis to Support Treating to LDL Targets
▪ The Safety of Treating to LDL Targets Has Never Been Proven
▪ Tailored Treatment Is a Simpler, Safer, More Effective, More Evidence-Based Approach

No to Target based approach???

Case 2; 55 year old diabetic female with no other risk factors – LDL C 125
Has anything changed with ATP IV ?
a. Should I start a Statin
b. Which one & what dose


ATP III- Risk Categories & Goals
▪ The foremost feature was the concept of risk assessment, both life time & short term – 10 years
▪ As per ATP-III guideline, the intensity of risk reduction intervention/s ust e at hed to a i di idual’s a solute risk as a fu da e tal
principle to prevention.

CARDS: Statin For Primary Prevention In T2DM
*Acute CHD event, coronary revascularization, stroke. RRR: Relative risk reduction
Colhoun HM et al. Lancet. 2004;364:685-696.
0
5
10
15
0 1 2 3 4 5 6
RRR=37% p=0.001
Cu
mu
lati
ve
in
cid
en
ce
of
ev
en
ts (
% o
f p
ati
en
ts)
127 events
83 events
Time (years)
Atorvastatin 10 mg (n=1428)
Placebo (n=1410)
median follow-up 3.9 years

22
25
21 21
0
5
10
15
20
25
30
Major CV event Coronary
revascularization
Stroke Major Vascular event
RR
R f
or
1 m
mo
l/L
red
uct
ion
of
LDL
Risk reduction per 40 mg/dl LDL reduction
Meta-analysis of statin studies in DM for primary prevention of CVD
Data from 18 686 DM patients Vs 71 370 without DM in 14 randomised trials of statins
Lancet 2008; 371: 117–25 CVD: Cardiovascular disease
Statin therapy can reduce CV events T2DM patients without CVD

ATP IV Primary prevention in patients with diabetes
Statins
Age
Diabetes LDLcholesterol
70-189 mg/dl
40-75 yrs
Moderate intensity statins
I A
High intensity statins
with risk >7.5%
IIa B
<40 yrs,
>75yrs
Balance between ASCVD benefits and
adverse effects
IIa C

Case 3: 60 year old male with LDL 195 No other risk factors
▪ Least controversial
Management
Evaluate for cause
Age>21 years LDL-C
>190mg/dl
primary
High dose statin
I B
Maximum tolerated
dose
I B
LDL-C reduction of atleast 50%
IIaB
secondary
Evaluate and treat
accordingly

STELLAR: Rosuvastatin reduce LDL-C better than all
other statins
-45.87
-52.34-54.96
-36.73
-42.57
-47.79-51.05
-20.13-24.29
-29.67-28.3
-34.98-38.81
-45.78
-70
-60
-50
-40
-30
-20
-10
010 20 40 80
Dose, mg
% c
ha
ng
e f
rom
ba
se
lin
e
Rosuvastatin (n = 156 - 160)Atorvastatin (n = 158 - 165)
Pravastatin (n = 158 - 165)Simvastatin (n = 161 - 164)
P < .001 vs comparators on a mg-to-mg basis.
Am J Cardiol 2003;92:152–160)
As Rosuvastatin causes maximum reduction in LDL-C among all the statins, it is preferable in those without
CVD, LDL-C > 190 mg/dl

▪ Mr C, A 58 years old man working in corporate office,
▪ K/C/o Hypertension 5 years. Smoker since 40 yrs (10 cigarettes/day)
▪ No H/o DM,IHD or CKD
▪ BP: 136/82 mm Hg, FPG: 98 mg/dl,
▪ eGFR: 101 mg/dl, S. Creatinine : 1.1 mg/dl Urine Protein: Nil, hsCRP: 3.9 mg/L
▪ TC:194 mg/dl, LDL:127mg/dl, HDL-C:31mg/dl, TG: 133 mg/dl
▪ He is on
▪ Olmesartan 40 mg 1 OD
Case 4: Non DM with risk factors

AHA Guidelines For Statin In Non-DM And Non-IHD Patients

Case 4: 10 years ASCVD risk: 21.7%
Moderate to high dose statin is required

Rosuvastatin 20 mg (N=8901)
MI Stroke
Unstable Angina
CVD Death CABG/PTCA
Randomized Double Blind Placebo Controlled Trial of Rosuvastatin in
the Prevention of CV Events In Individuals With Low LDL and high
hsCRP
4-week run-in
Ridker PM et al, Circulation 2003;108:2292-2297
No Prior CVD or DM Men >50, Women >60
LDL <130 mg/dL hsCRP >2 mg/L
Placebo (N=8901)
Follow up: 1.9 yrs
JUPITER study

Placebo 251 / 8901
Rosuvastatin 142 / 8901
Risk Reduction: 44 %
0 1 2 3 4
0.0
0
0.0
2
0.0
4
0.0
6
0.0
8
Cu
mu
lati
ve
In
cid
en
ce
Follow-up (years)
Ridker PM et al, N Engl J Med 2008;359:2195-207
JUPITER :primary trial endpoint
In patients without DM and CVD, with high hs-CRP (>2
mg/dl), rosuvastatin significantly reduces CV events by 44%

▪ A sub analysis to evaluate CV benefits in patients who achieved LDL-C< 50mg/dl with rosuvastatin (n= 4154) Vs those on placebo
▪ Following benefits were seen those with LDL-C< 50 mg/dl vs those on placebo
JUPITER : LDL < 50 mg/Dl Provides Maximum CV Protection
65% Risk reduction in
Primary End Point
46% Risk reduction in
All Cause Mortality
J Am Coll Cardiol 2011;57:1666–75

▪ Olmesartan 40 mg OD
▪ Rosuvastatin 20 mg OD or Atorvastatin 40 mg OD
Final Therapy for Case 4
Case 5: 68-year-old lady Non DM & HTN, No ASCVD, Non Smoker TC 145, TG 200, LDL 88, HDL 42. 130/85 on treatment.
a. No Statins.
b. 40 mg Atorvastatin.
c. 80 mg Atorvastatin.
d. 40 mg Rosuvastatin.
e. 2 mg Pitavastatin.

Case 6: 42-year-old IT professional. Male Smoker, no known risk factors. TC 210, TG 220, LDL 150, HDL 40
a. Only life style management
b. 10 mg Atorvastatin
c. 20 mg Rosuvastatin
d. 10 mg Rosuvastatin + Fenofibrate

How do you decide ? ATP IV Guidelines
▪ Individuals without clinical ASCVD or diabetes
▪ 40 to 75 years of age
▪ LDL-C 70-189 mg/dL
▪ Estimated 10-year ASCVD risk of 7.5% or higher
Moderate- or high-intensity statin

The New CV Risk Assessment Calculator
▪ Previously used Framingham risk score - inadequate
▪ “deri atio in an exclusively White sample population and the limited scope of the outcome
▪ Based on data collected from several large, racially & geographically diverse, modern NHLBI sponsored studies, including ARC, CARDIA, Framingham study.
▪ Includes
▪ Smoking status
▪ Diabetes
▪ Systolic BP & treatment status
▪ Total & HDL cholesterol
▪ Age
▪ Gender
▪ Race
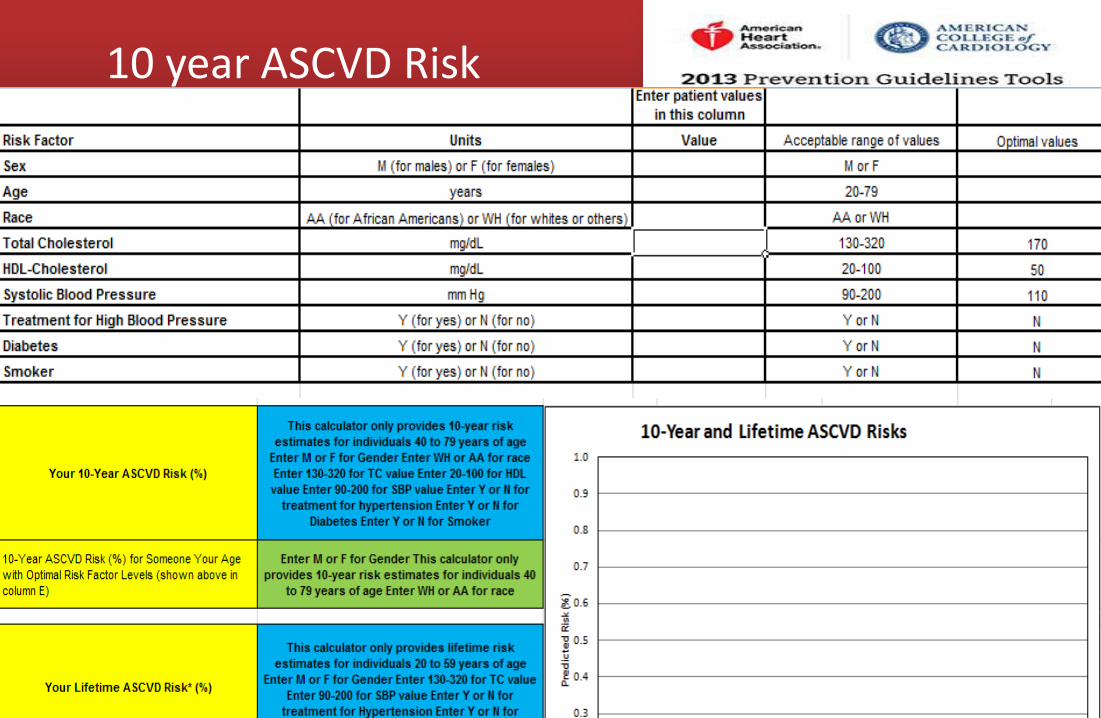
10 year ASCVD Risk
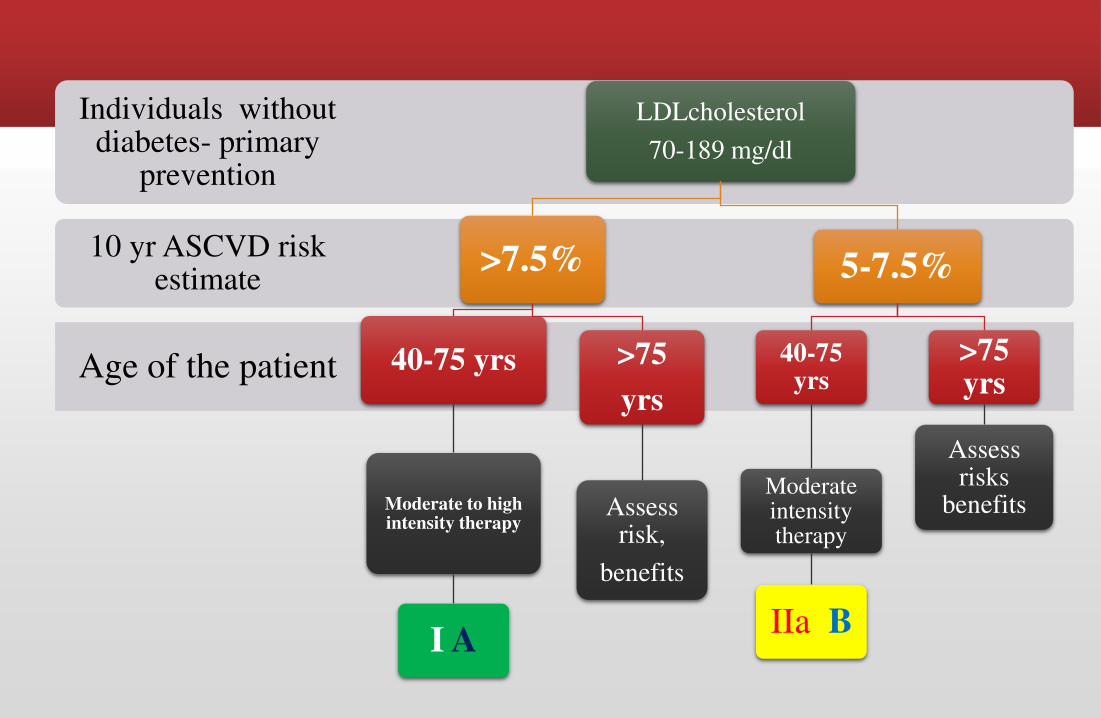
Age of the patient
10 yr ASCVD risk estimate
Individuals without diabetes- primary
prevention
LDLcholesterol
70-189 mg/dl
>7.5%
40-75 yrs
Moderate to high intensity therapy
I A
>75
yrs
Assess risk,
benefits
5-7.5%
40-75 yrs
Moderate intensity therapy
IIa B
>75 yrs
Assess risks
benefits

Case 5: 68-year-old lady Non DM & HTN, No ASCVD, Non Smoker TC 145, TG 200, LDL 88, HDL 42. 130/85 on treatment.
a. No Statins.
b. 40 mg Atorvastatin.
c. 80 mg Atorvastatin.
d. 40 mg Rosuvastatin.
e. 2 mg Pitavastatin.
ASCVD Risk 10%
Case 6: 42-year-old IT professional. Male Smoker, no known risk factors. TC 210, TG 220, LDL 150, HDL 40
a. Only life style management
b. 10 mg Atorvastatin
c. 20 mg Rosuvastatin
d. 10 mg Rosuvastatin + Fenofibrate
ASCVD Risk 5.7%

Additional Risk Markers?
▪ Primary LDL–C ≥ g/dL
▪ Other evidence of genetic hyperlipidemias,
▪ Family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative,
▪ High-sensitivity C-reactive protein >2 mg/L,
▪ CAC s ore ≥ Agatston u its or ≥ per e tile for age, sex, a d ethnicity,
▪ Ankle-brachial index <0.9, or
▪ Elevated lifetime risk of ASCVD

Why 7.5?
ATP IV


Paris computer games store. In fact, the floor is
absolutely flat

The results of HPS led to the widespread concept that there are benefits of statin
therapy in high-risk individuals regardless of baseline cholesterol levels.
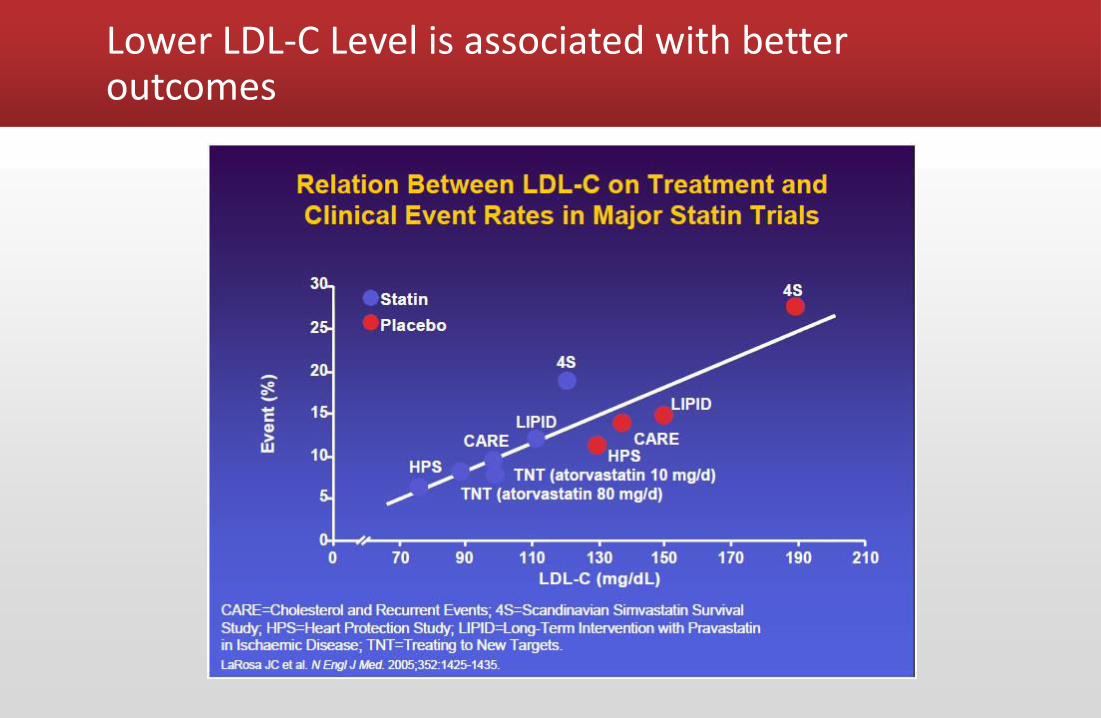
Lower LDL-C Level is associated with better outcomes

2012 Redefining the risk threshold for primary prevention

2012
▪ Reduction of LDL with a statin reduced the risk of major vascular events (RR 0・79, per 1 mmol/L reduction), largely irrespective of age, sex, baseline LDL cholesterol or previous vascular disease, and of vascular and all-cause mortality.
▪ In individuals with 5-year risk of major vascular events lower than 10%, each 1 mmol/L reduction in LDL cholesterol produced an absolute reduction in major vascular events of about 11 per 1000 over 5 years.
▪ This benefit greatly exceeds any known hazards of statin therapy.
Lancet 2012; 380: 581–90

Effects on major coronary events, strokes, coronary revascularisation procedures, and major vascular events per 1·0 mmol/L reduction in LDL cholesterol at different levels of risk
▪ Lancet 2012; 380: 581–90

Statin can it be Satin?
Number needed to harm – New onset diabetes – 120 - 450
Muscle problems – 5-10%

Why Statin for estimated risk of > 7.5?

Case 7a. 52-year-old lady. Euthyroid TC 212, TG 300, LDL123, HDL 68
a. Statin + Fenofibric acid.
b. No treatment (only LSM).
c. Niacin.
d. Fish oil.
ASCVD Risk 1.1%

Case 7b: 44-year-old male TC 220, TG 580, LDL 111, No other risk factors
a. Fenofibrate
b. Rosuvastatin
c. Statin + Fenofibrate.
d. Niacin.

ATP III- Non-HDL Cholesterol
▪ Established the concept of non-HDL-C as a secondary target for therapy in patients with TG greater than 200 mg/dL
▪ The non-HDL-C encompasses all atherogenic lipoproteins, including not just LDL but also VLDL and IDL.
▪ Thus, after focusing initially on lowering the LDL-C or if the LDL-C cannot be determined, one should use the non-HDL-C as a secondary target for therapy.
▪ The recommended targets for non-HDL-C are 30 mg/dL higher than the LDL-C targets
JAMA 2001;285:2486– 9 .

What ATP IV says?
With few exceptions, use of lipid-modifying drugs other than statins is discouraged.
Non-statin lipid lowering drugs (Ezitimibe, Fibrates, Niacin, Efastenol, Sterols) have no evidence of CV protection

The New CV Risk Assessment Cal ulator…. Good, Bad or Ugly?
▪ It was derived from five population-based cohorts of African Americans and non-Hispanic whites and relies heavily on age and sex to determine ASCVD risk while ignoring other important factors such as family history.
▪ Several leading researchers have suggested that it overestimated the CV risk
▪ They applied the new risk algorithm in three large scale primary prevention studies- Women health study, Physician health study, women health initiative observational study and found that the new scoring system overestimated risk by 75-150%
▪ The new risk algorithm can not be applied to Asian population as the Asian population were not adequately represented in the studies used to develop the new algorithm



Case 8: 35 year old, Hypertensive patient TC 180, LDL 108, HDL 45
No recommendations

Individuals 21-39 years and >75 years age???
▪ No primary prevention RCT data were available for individuals 21 to 39 years of age and few data were available for individuals >75 years of age.
▪ Therefore, in adults with LDL–C <190 mg/dL who are not otherwise identified in a statin benefit group, clinician knowledge, experience and skill, and patient preferences, all contribute to the decision to initiate statin therapy in these individuals
▪ Future RCTs will be needed to determine the optimal age at which to initiate statin therapy to reduce ASCVD risk, as well as to determine the optimum duration of statin therapy.

Statins in Heart Failure, Hemodialysis patients

Common practical questions
▪When should I repeat a lipid profile
▪ Should I get a CPK done prior to high dose statin
▪ Should I get a LFT done
▪What if LDL < 40 on FU

ATP IV: Safety recommendations of statins
NHLBI ACC/AHA
COR
LOE
1.Creatine Kinase, routinely not needed A III no benefiit A
2.Baseline CK in pts at risk of events E IIa C
3.Baseline ALT before initiating statins B I B
4.Decreasing the statin dose,if 2 consecutive
values of LDL-C <40 mg/dl.
C IIb C
5.Simvastatin at 80 mg daily harmful B III harm A
6.New onset diabetes on statin therapy,
continue statins
B I B
7.If muscle symtpoms
develop,discontinue,use again
E II a C
8.Confusional state,see secondary causes E II b C

Safety considerations
Patient groups that may influence statin safety
• Impaired renal or hepatic function
• History of previous statin intolerance of muscle disorders
• Concomitant use of drugs affecting statin metabolism
• History of hemorrhagic stroke
• Age > 75 yr
• Asian race

▪ Mrs F, a 62 years old woman presented in OPD
▪ She is K/c/o HT since 15 years, DM since 6 years and CKD since 2 years
▪ BP: 128/78 mm Hg. FPG: 149 mg/dl, PPBG: 201 mg/dl
▪ TC: 204 mg/dl, LDL: 126 mg/dl, TG: 160 mg/dl, HDL: 47 mg/dl
▪ S. creatinine 1.8 mg/dl, eGFR: 67 mg/dl
▪ She is on
▪ Antidaibetic
▪ Tab Voglibose 0.2 mg 1 TDS
▪ Tab Telmisartan 80 mg + Amlodipine 5 mg 1 OD
▪ Tab Aspirin 75 mg 1 OD
Case 9: Chronic Kidney Disease

2013 KDIGO Guidelines For Lipid Management In CKD
KDIGO Kidney Disease: Improving Global Outcomes

▪ Atorvastatin: No dose adjustment required
▪ Rosuvastatin: In patients severe CKD with creatinine clearance < 30
ml/min (not on hemodialysis), Maximum dose: 10 mg/day
▪ Pitavastatin: in patients with moderate/severe CKD (GFR: 15-59
ml/min) Maximum dose: 2 mg/day,
Dose of statins in patients with CKD
GFR: Glomerular Filtration Rate

▪ A meta-analysis of 11 studies including 21,295 CKD patients (14,202 not on dialysis)
▪ Following were benefits of statin therapy (P < 0.05 for all)
▪ 36% relative risk reduction in all cause death
▪ 31% relative risk reduction in CV death
▪ 45% relative risk reduction in CV events
▪ 34% relative risk reduction in stroke
Benefit Of Statin In CKD Patients (Not On Dialysis): A Meta-analysis
Pharmacological Research 2013 ;72:35– 44

de Zeeuw D. 2010European Renal Association-European Dialysis and Transplant Association Congress; June 27, 2010; Munich, Germany.
Atorvastatin vs Rosuvastatin for renal
function PLANET I:
Adverse event
Rosuvastatin
10 mg/day
(n = 116)
Rosuvastatin 40
mg/day
(n = 123)
Atorvastatin 80
mg/day
(n = 110) p
Any renal
adverse event
7.8 9.8 4.5 NS
Acute renal failure 0.0 4.1 0.9 <0.05
Serum creatinine
doubling
0.0 4.9 0.0 <0.01
Serum creatinine
doubling or acute
renal failure
0.0 7.3 0.9 <0.01
Atorvastatin is safer than rosuvastatin in DM patients
with proteinuria

▪ A meta-analysis of 5 clinical trials head to head comparing atorvastatin vs rosuvastatin
Atorvastatin Vs Rosuvastatin For Proteinuria: A Meta-analysis
Atorvastatin is better than rosuvastatin for reduction in
proteinuria
Circ J 2012;76:1259-66

Effect of pitavastatin on eGFR in CKD patients with
baseline eGFR<60 ml/min
J Atheroscler Thromb 2010;17:601-609 CKD: Chronic Kidney disease,
eGFR: estimated Glomerular Filtration Rate
Pitavastatin improves renal function in CKD patients with
eGFR< 60 ml/min

Effect of 12 Weeks of Pitavastatin Therapy On Proteinuria
**p< 0.01
Am J Cardiol 2011;107:1644 –1649
Pitavastatin significantly reduced proteinuria in dyslipidemic patients
within 12 weeks

▪ Tab Metformin 500 mg 1 BD
▪ Tab Glimepiride 1 mg 1 OD
▪ Tab Voglibose 0.2 mg 1 TDS
▪ Tab Telmisartan 80 mg + Amlodipine 5 mg 1 OD
▪ Tab Aspirin 75 mg 1 OD
▪ Patient can be treated with 10 mg atorvastatin or 2 mg pitavastatin
Final therapy of Case 9

▪ Mr G, 53 old man working as engineer, presented for follow up for hypertension
▪ K/c/o Hypertension since 6 years, No H/o DM, IHD
▪ Smoker since 30 years, 10 bidis/day,
▪ Obese, Weight: 85 kg BMI: 28 kg/m2
▪ BP: 138/82 mm Hg, FPG: 116 mg/dl, HbA1c: 6.3%
▪ TC: 210 mg/dl, LDL-C: 138 mg/dl, TG: 167 mg/dl and HDL: 38 mg/dl
▪ He is on Ramipril 10 mg 1 OD and Amlodipine 5 mg 1 OD
Case 10: Impaired Glucose Tolerance Patient

Statin increases risk of new DM by 13%
▪ A meta-analysis has shown that with statin therapy, risk of new onset of diabetes is increased by 13%
FDA Drug Safety Communication: Important safety label changes to cholesterol-lowering statin drugs
Increases in HbA1c and fasting serum glucose levels have been reported with statin use

LIVES : Pitavastatin does not increase HbA1c in DM patients even at 2 yrs
Expert Opin Pharmacother. 2010;11(5):817–828.
Long term pitavastatin therapy does not affect glycemic
control in DM patients
▪ A prospective randomized, controlled trial
▪ 1,269 individuals with impaired glucose tolerance (IGT)
randomized to either pitavastatin (lifestyle modification and
pitavastatin [1-2 mg/day]) or control group (lifestyle modification
only)
▪ Pitavastatin significantly reduced new onset of DM [the hazard ratio
0.82 (p=0.041)]
J PREDICT : Pitavastatin In IGT Patients
ADA 2013, Late breaking abstract No. 61-LB
J-PREDICT-Japan Prevention Trial of Diabetes by Pitavastatin in Patients with Impaired Glucose Tolerance study

J PREDICT : Pitavastatin In IGT Patients
Atherosclerosis Supplements 2015;161:1–27
J PREDICT - Japan PREvention Trial of Diabetes
by Pitavastatin in Patients with Impaired GluCose Tolerance
J PREDICT study - Lifestyle modification plus 1–2 mg/day of
pitavastatin significantly reduced the cumulative incidence of
T2DM (by 18%) in 1,269 high-risk patients with impaired glucose tolerance,
compared to lifestyle modifications alone
18%
NOD – New onset Diabetes
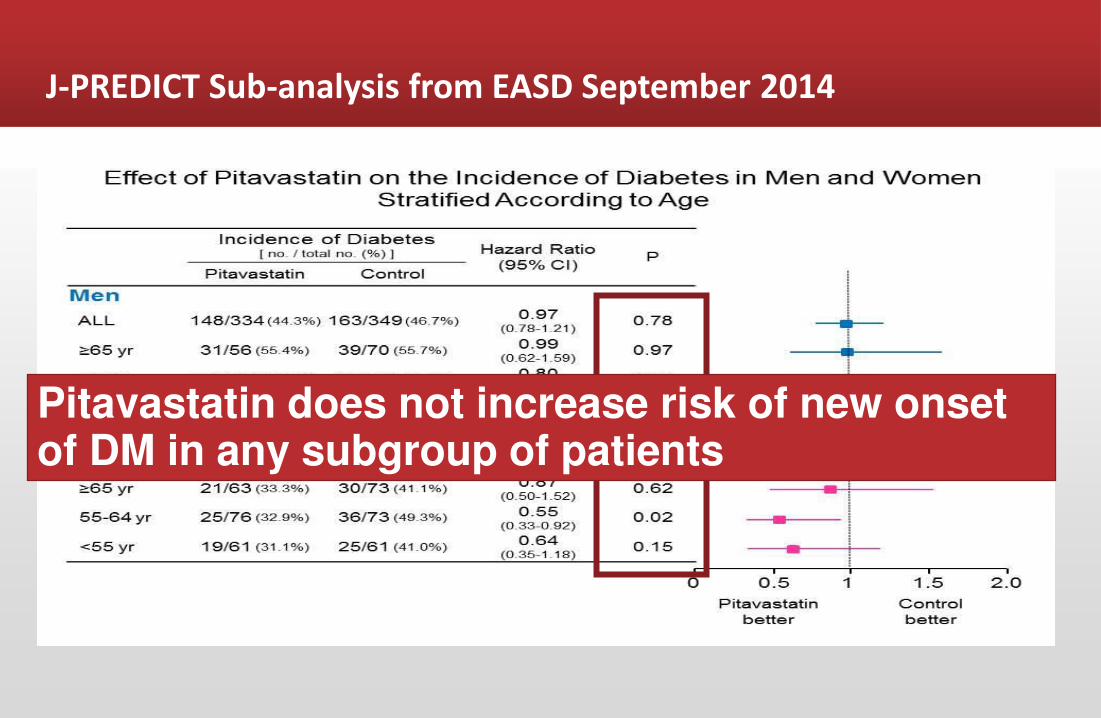
J-PREDICT Sub-analysis from EASD September 2014
Pitavastatin does not increase risk of new onset of DM in any subgroup of patients

▪ Mr I, a 41 years old person presented in OPD for follow up
▪ He is K/c/o Dyslipidemia since 6 months
▪ No H/o HT, DM IHD or other diseases
▪ FPG: 85mg/dl, PPPG: 138 mg/dl BP:
▪ He is not on any medication. He was prescribed Rosuvastatin 10 mg before 6 months, stopped after 1 month due to severe myalgia
▪ TC: 250 mg/dl, LDL-C: 161 mg/dl, TG: 130 mg/dl, HDL: 38 mg/dl
Case 11: Statin intolerant patient

▪ In Florida, USA, 152 patients intolerant to > 2 previous statins due to myopathy (average 2.7 statins) were placed on pitavastatin therapy.
▪ Percentage (%) of patients tolerating pitavastatin and achieving NCEP ATP-III LDL-C goal non-HDL-C goal were measured
▪ 104 patients (76%) patients tolerated pitavastatin therapy and continued it for > 6 months
▪ 87% of patients with intermediate CV risk achieved their NCEP-ATP III LDL-C goals with pitavastatin therapy
Pitavastatin For Statin Intolerant Patients
Journal of Clinical Lipidology 2012: 6(3) : 274

LDL
cholesterol
>190 mg/dl
Pt had CAD, HTN,smoker,not
on statins
Age 45 yrs
Start Statins to the maximum tolerated dose
Age 75 yrs
Assess risk,benefits
Pt diabetic,no CAD,
ASCVDrisk >7.5%
High intensity statins
Pt not diabetic,
noCAD
Evaluate secondary causes
High dose statin
therapy
70-189 mg/dl
Pt CAD
Statins
Pt diabetic
Moderat dose
statins
Pt no h/o CAD,
DM2,
risk <7.5%
Assess risk,
benefits
Pt having CKD
No EBT for statins
Summarizing ATP IV

Worth the ait….???
No Target
Only Statins
Based on RCTs

2004.. BE MORE AGGRESSIVE!!

2013 Revolution (Stavolution) of ATP IV STATIN THERAPY IS BENEFICIAL IN HIGH-RISK PATIENTS VIRTUALLY REGARDLESS OF THE BASELINE LDL-C LEVEL

So, how to select a statin finally?
Patient’s Profile Preferred Statin
Secondary prevention of CVD Atorvastatin
Primary prevention of CVD for DM and high risk patients Atorvastatin/
Rosuvastatin
Primary prevention of CVD without DM and high hsCRP (> 2 mg/dl) Rosuvastatin
Difficult to achieve LDL-C goal Atorvastatin/
Rosuvastatin
Acute Coronary Syndrome/PCI Atorvastatin/Rosuvasta
tin
For patients with CKD Atorvastatin/
Pitavastatin*
Patients with IGT Pitavastatin
Statin intolerance Try Pitavastatin
*If eGFR > 15 ml/min

Thank You