drugs affecting the gastrointestinal system - ssu affecting the gastrointestinal system antacids,...
TRANSCRIPT
Drugs Affecting the
Gastrointestinal
System
Antacids, Constipation,
Increasing gastrointestinal
motility
Cells of the Gastric Gland
• parietal cells:
• produce & secrete HCl
• primary site of action for many drugs
• chief cells:
• secrete pepsinogen [= a proenzyme]
• pepsinogen acid pepsin[ breaks
down proteins]
• mucoid cells:
• mucus-secreting cells
• purpose = protective mucous coat [HCl]
Hydrochloric Acid
• secreted by parietal cells
• maintains stomach pH at 1 to 4
• stimulants to secretion:
• large, fatty meals
• excessive amounts of ETOH
• emotional stress
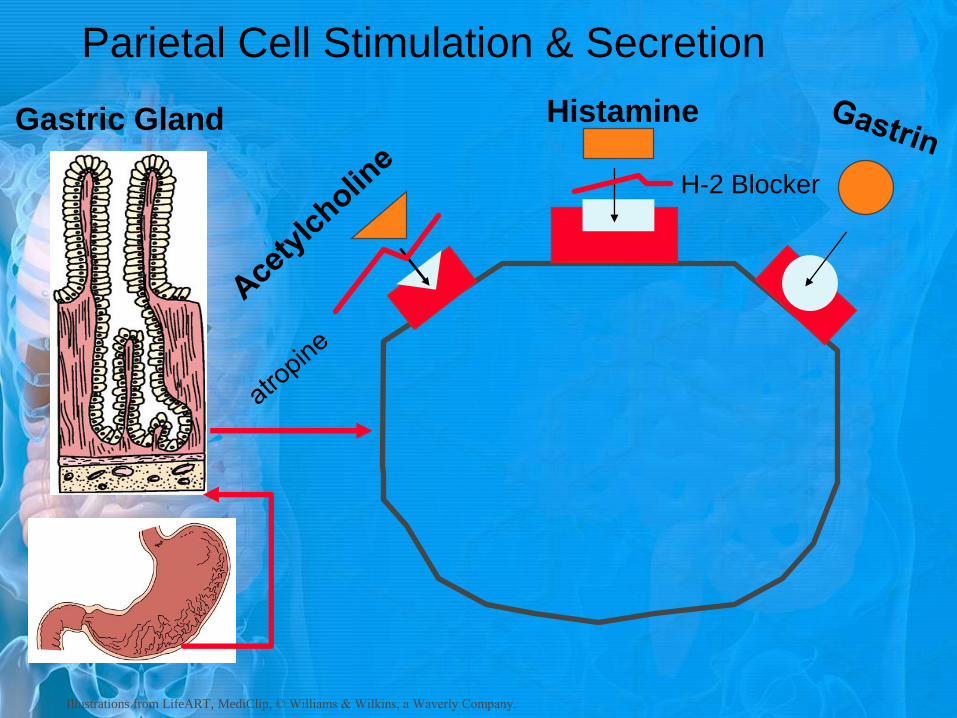
Parietal Cell Stimulation & Secretion
Histamine
H-2 Blocker
Gastric Gland
Illustrations from LifeART, MediClip, © Williams & Wilkins, a Waverly Company.
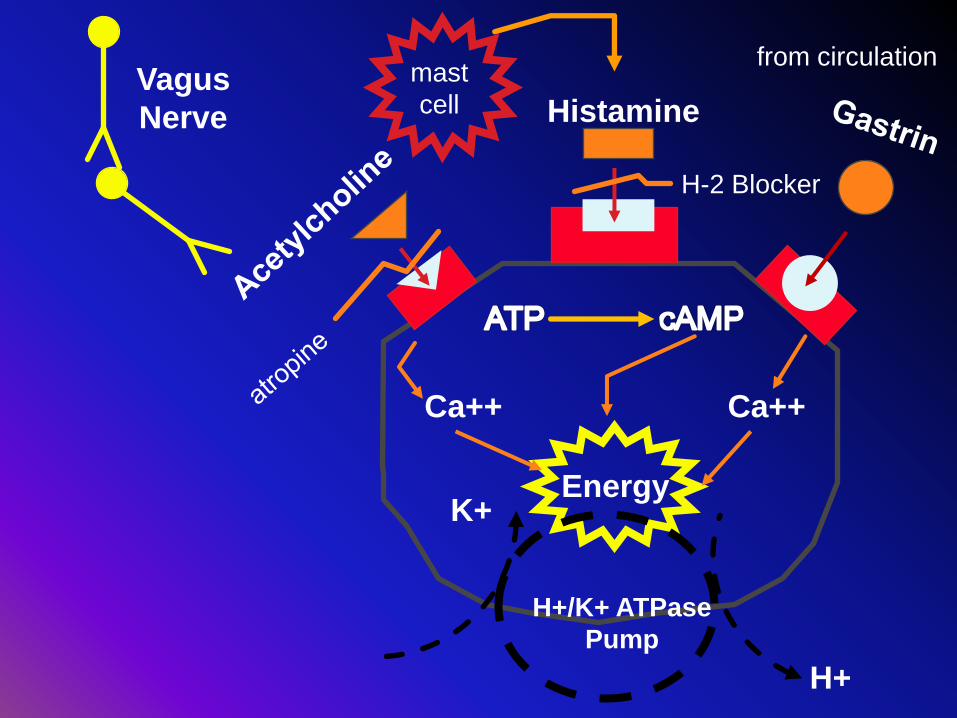
Histamine
H-2 Blocker
Ca++ Ca++
Energy
H+/K+ ATPase
Pump
H+
K+
mast
cell Vagus
Nerve
from circulation

Management
• Therapy is aimed at • Healing the ulcer • Preventing recurrence
• Drug therapy has several major thrusts
• Raising gastric pH • antacids • Inhibitors of acid secretion
• H2 antagonists • Proton pump inhibitors
• Mucosal protection • H Pylori eradication
• The predominant causes of peptic ulcer disease are H pylori
infection and use of NSAIDs accounting for 48% and 24% of cases, respectively.

Antacids
• Neutralize gastric pH
• Largely replaced in recent years by other drugs
• Used for fast relief of gastric discomfort, often in combination with other therapies
• Onset: 5-15 minutes
• Duration: 2 hours
• must be used repeatedly to reduce acidity
Antacids • Formulations: chewable tablets, liquids
• liquids are more effective
• Formulations of aluminum, magnesium and
calcium, often combinations are made
MOA Antacids • Do nothing to stop overproduction of acid
• Promote gastric mucosal defenses by:
• stimulating mucus,
• prostaglandins, and
• bicarbonate secretion from the gastric
glands

Effects of Antacids • raising pH 1.3 to 1.6
• acid in gastric juices 50% neutralized
• raising pH 1.3 to 2.3
• reduction of acid by 90%
• reduces pain assoc. with acid-release
Therapeutic Uses • Heart burn
• DU
• GU
Doses: 1 -2 tablespoon 1-3 hours after meals
(140 -156 mEq)
Side Effects • Minimal and depend upon compound
• May be unpleasant or chalky tasting
• flavors are better tolerated
• magnesium:
• Diarrhea, in RF causes CNS toxicity
• aluminum & calcium
• constipation
Drug Interactions
• Four basic mechanisms • chelation:
• binding or inactivation of another drug
• chemical inactivation:
• produces insoluble complexes
• increased stomach pH:
• increases absorption of basic drugs
• decreases absorption of acidic drugs
• increased urinary pH
• increases excretion of acidic drugs
• decreases excretion of basic drugs

Cimetidine
Ranitidine
Famotidine
Nizatidine
H2 Antagonists • Histamine type 2 receptor [H2] competitive
antagonist
• prototypical acid secretory antagonists
• Reduce, but not abolish acid secretion
• one of most frequently Rx’d drugs
MOA
• 2 mechanism: • Competitively block the histamine (H2)
receptor of acid-producing parietal cells
• Also up to 90% inhibition of vagal
stimulated and gastrin stimulated acid
secretion
Therapeutic Effects
• Proven effective: • PUD = gastric & duodenal ulcer
• Gastroesophageal reflux disease [GERD]
• Upper GI bleed [GIB]
• May be effective: • Prevention of stress ulcers
• Peptic esophagitis
• Less potent than PPIs but still suppress acid by 60- 70% over 24 hrs
• Complete inhibition has not been shown.

• 70-85% of patients with DU respond in 4-6 weeks and 87% to 94% after 8 weeks.
• Suppression of acid secretion during night.
• 60-80% of patients with GU respond in 6-8 weeks.
• It is used in half of usual dose to prevent recurrence of ulcer.

Side Effects
• Cimetidine:
• Overall low < 3%
• Headache, dizziness, confusion, rash, liver
& kidney impairment, muscle cramp, fever
• Impotence, increased prolactin, &
gynecomastia
• Dosage: qid or at hs
• Ranitidine:
• Headache, arrhythmia, confusion
• Dosage: bid or at hs
Drug Interactions
• Cimetidine:
• Decrease the activity of cytochrome
P450
• Ranitidine
• Inhibits CYP450 , 4- 10 times less than
cimetidine.
• Concurrent use with omeprazole
decreases its effect
• Cigarette decreases their effects

Anticholenergics
• Clidinium, Dicyclomine, Glycopyrrolate,
Propanthelene, Pirenzepine
• Decreases the effect of Ach on the parietal
cells
• Therapeutic Uses:
• Not a mainstay of therapy
• Should not be used in GERD
• Side effects:
• Blurred vision, dry mouth, tachycardia, urinary
retention, constipation
Omeprazole
Rabeprazole
Pantoprazole
Lansoprazole
Esomeprazole

H+/K+ATPase = site of action
Final common step in acid production
Acetylc
holine
Histamine Gastrin
atro
pine
H-2 Blocker
ATP cAMP
Ca++Ca++
Energy
H+/K+ ATPase
Pump
H+
K+
mast
cellVagus
Nerve
from circulation
MOA Proton Pump Inhibitors
• convert in to their active form in the acidic
environment (Activated only when pH
decreases below 4)
• irreversibly bind to H+/K+ATPase
• prevent H+ ion production & secretion
• block all acid secretion = achlorhydria
• to return to normal must synthesize new
H+/K+ ATPase
• Delayed effect

• should be administered approximately 1 hour
before a meal
• have a short serum half-life
• concentrated and activated near their site of
action
• have a long duration of action.

Therapeutic Effects
• GERD • Drug of choice
• PUD • recurrent [Helicobacter pylori]
• Better than H2 antagonists
• Erosive esophagitis
• Zollinger-Ellison syndrome [ZE]
• NSAID associated ulcers
• Prevention of Rebleeding from Peptic
Ulcers
• Prevention of stress related mucosal
bleeding
Dosage: 20 mg qd for 4- 8 weeks Most effective after a prolonged fast when large amounts of active proton pumps are present (i.e. breakfast)
PPIs provide superior acid suppression, healing
rates, and symptom relief vs H2 blockers and
heal 95% of duodenal ulcers and 80% to 90% of
gastric ulcers by 4 weeks
Side Effects & Interactions • Side effects: (mild) nausea, headache,
diarrhea, constipation, flatulence,
hypergastrinemia ECL hypeplasia
• May affect absorption of other drug
• May decrease calcium absorption or
osteoclast, which may lead to hip fracture.
• nosocomial pneumonia

Sucralfate • cytoprotective agent
• once comes in contact with acid in stomach
• dissociate into aluminum hydroxide &
sulfate anions
• attracted to and bind to the base of ulcers &
erosions
• forms a protective barrier over the base of
this area
• binds to exposed proteins of ulcers
• limits pepsin’s proteolytic action here
• Prevents H+ reflux
• Increases production of PGs and
bicarbonate secretion
Sucralfate • Uses: gastric, duodenal and oral ulcers, GI
bleed, stress ulcer prevention
• Minimal absorption
• Dosing: 1 g qid, 1 hr before meals & hs on
empty stomach

• Side effects: constipation, sleepiness,
hypophosphatemia
• Drug interaction: decreases absorption of
many drugs and fat soluble vitamins
Bismuth subcitrate
• Coats ulcer at low pH
• Assists H Pylori eradication
• Causes black tongue and stool
• Must be taken at least half an hour before meals
• Bismuth based preparations have more adverse effects, and also ~85% success.
However cheapest. • Bismuth, metronidazole and tetracycline,
and a proton pump inhibitor for 2 weeks
H Pylori eradication
regimens
• Clarithromycin based quadruple therapy has
highest eradication rate (~95%)
• Omeprazole (any PPI), clarithromycin,
amoxicillin and metronidazole, all twice
daily for a week
• Non-clarithromycin based regimens: cheaper,
but lower eradication rate (~85%)
• Omeprazole (or high dose ranitidine),
amoxicillin and metronidazole for 2 weeks
Eradication of H pylori reduces the incidence of peptic ulcer disease recurrence, from 67% to 6% for DU and from 59% to 4% for GU. Continue PPIs after 6 weeks of triple therapy, especially if ulcer is >1 cm.
• Bulk-formers
• Osmotic laxatives
• Stool softeners
• Stimulant Laxatives
Laxatives
Bulk-forming Laxatives
• Psyllium, bran, etc.
• Swells in water to form gel that increases
bulk and softens stool, increase peristalsis
– Similar to the action of dietary fiber
• Useful in chronic constipation, and in irritable
bowel syndrome
• Onset: 12-24 hrs
• Powder needs reconstitution in at
least 8 oz (1 glass) water or juice
• Drink 6-8 glasses of water
Osmotic laxatives
• Increase colonic fluid retention
• Nonabsorbable
• Stimulate peristalsis
• Include two types:
– Nonabsorbable Sugars
– Nonabsorbable salts
Nonabsorbable Sugars
• Lactulose – In the colon hydrolyzes to lactic acid, formic acid, and
acetic acid
– Onset: 24-48 hr
• Sorbital – Side effects: flatulence, abdominal bloating, diarrhea
• Polyethylene Glycol
- does not produce significant cramps or flatus.
Nonabsorbable salts
Milk of Magnesia, Magnesium oxide
• Used in simple constipation & postop
• Onset: 0.5-3 hours
• Use cautiously in renal impairment
– Potential for hypermagnesemia due to reduced
excretion
Stool softeners
• Docusate , Paraffin (Mineral oil), Glycerin
• Reduce surface tension in the bowel increasing water absorption into stool
• Onset: 6-8 hrs
• Side effects:
– (rare) GI pain, cramping, rash, decrease absorption of fat soluble vitamins
• Administer with adequate fluids
Stimulant Laxatives
• May stimulate myenteric plexus
• Increase intestinal peristaltic motility and secretion
• Onset: 2-6 hours
• Potent, may cause watery stools, cramping
• Often used for preprocedure bowel preps, postop
• Side effects: abdominal discomfort,
nausea, cramps

Castor oil
• Besides irritation, it has surfactant
activity
• It may acts through inhibition of Na+/k+
ATPase, cAMp, PGs

Bisacodyl (Dulcolax)
• inhibition of Na+/k+ ATPase, cAMp,
PGs
• Tablets
– Onset: 6-12 hrs
• Suppository
– Onset: 15-60 minutes
• Used in conjunction with PEG

Senokot (senna)
• Natural, obtained from dried cassia leaflets
• Used for simple constipation, postop, other
• Onset: 6-12 hours (up to 24)
Drugs promoting
gastrointestinal motility
Time to empty half of liquid is half an hour
and to empty solids is 2 hours
Factors that delay the gastric emptying:
Neuropathy, myopathy, electrolyte disturbances, gastroenteritis, anticholenergics, TCA, levodopa, β agonists
Factors that enhance the gastric emptying:
Metoclopramide, Cisapride, Domperidone, cholinomimetics

Metoclopramide Mechanism:
CNS: D2 antagonist
Peripheral: cholinergic agonist, dopamine antagonist, 5-HT4 agonist, 5-HT3 blocker, sensitize intestinal smooth muscles to the Ach
Increases gastric contractions, gastric emptying and peristaltic movement, raises pressure of lower esophageal sphincter
block dopamine D2 receptors in the CTZ of the medulla, resulting in potent anti N/V

Indications:
1. Decreases gastric emptying time
2. GERD
3. Nausea
4. Before induction of anesthesia
5. Facilitates small bowel intubation
6. Increases lactation
Side effects
Insomnia, fatigue, restlessness,
unordinary weakness
Galactorrhea, menstrual disorders
Extraperimedial side effects: parkinson,
dystonic reactions, akatesia, tardive
dyskenesia
Especially in elders and youngsters
Drug Interactions
Increases the effect of CNS depressant
Increases the EP side effects of
haloperidol, phenothiazines,
thioxanthins
Antimuscarinics neutralize the effects
of metoclopramide

Other drugs Domperidone
Like metoclopramide except it does not
enter the CNS
Cisapride
No effect on DA, activation of 5-HT4 and Ach
Causes fatal ventricular arrhythmia,
diarrhea
Cholinergic agonists
Increase the effect of metoclopramide
Erythromycin
Prokinetic activity