druj issues
TRANSCRIPT
PRESENTED BY:
DR . N. BENTHUNGO TUNGOEPOST GRADUATE
M.S(ORTHOPEDICS)
CENTRAL INSTITUTE OF ORTHOPEDICSVMMC & SAFDARJUNG HOSPITAL
NEW DELHI
DISTAL RADIO ULNAR JOINT(DRUJ) ISSUES AND MANAGEMENT


INTRODUCTION
The distal radioulnar joint (DRUJ) is a diarthrodial, synovial articulation that provides the distal link between the radius and the ulna and a pivot for pronation-supination .
Because the ulna and radius articular surfaces have different radii of curvature, the soft tissues play a substantia role in guiding and restraining the joint.
During forearm motion, the DRUJ moves synchronously with the proximal radioulnar joint, and any injury or deformity involving the radius or ulna can alter the function of both joints.
The DRUJ and ulnocarpal joint are also anatomically and functionally integrated, so that both are affected by traumatic and arthritic conditions.

BIOMECHANICS The normal arc of pronation and supination ranges among
individuals from 150 to 180 degrees. Additional rotation of up to 30 degrees occurs through the radiocarpal joint
During forearm rotation, translation occurs between the ulnar head and sigmoid notch, resulting in a combination of rolling and sliding movements at the articular surface.
when the unloaded forearm is in the neutral position, articular contact is maximal, reaching 60% of the available surface area. At the extremes of pronation and supination, there may be only 2 mm of articular contact at the rims of the notch (<10% of the articular surface area).
Translation can occur because the sigmoid notch is shallow, and its radius of curvature is 50% to 100% greater than that of the ulnar head.

In the transverse plane, the average sigmoid notch subtends an arc of approximately 50 degrees

Based on an anatomic study of 50 cadavers, four different sigmoid notch shapes were found: flat face (42%), ski slope (14%), “C” type (30%), and “S” type (14%)
NOTE: A flat sigmoid notch may be more prone to instability and less responsive to treatment by soft tissue repair alone
The ulna is the stable unit of the forearm and supports loads transmitted from the radius and carpus. The ulnar head serves as the articular seat for the sigmoid notch around which the radius rotates. The surface of the ulnar head that faces the sigmoid notch forms a slightly asymmetric, partial cylinder of about a 130-degree arc.


At the base of the ULNAR styloid and encompassing the geometric center of the head, is a shallow concavity called the fovea that is devoid of cartilage and replete with vascular foramina that supply vessels to the TFCC .
The fovea is the primary attachment site for the radioulnar and ulnocarpal ligaments.
The ulnar styloid is a continuation of the subcutaneous ridge of the ulna, projecting 2 to 6 mm distally. It provides an increased area for soft tissue attachments, including the extensor carpi ulnaris (ECU) tendon sheath and thesecondary attachments of the radioulnar ligaments.
Ulnar variance is the term used to relate the difference in lengths of the radius and ulna. Ulna plus (or positive) and ulna minus (or negative) describe the ulna as longer or shorter than the radius, respectively.
TFCC The TFCC, named by Palmer and Werner,is the most commonly used term
for the interconnected soft tissues that span and support the DRUJ and ulnocarpal articulations.
The primary functions of the TFCC are:
(1) extend the smooth articular surface of the distal radius to cover the ulnar head;
(2) transmit axial force across the ulnocarpal joint, while partially absorbing the load;
(3) provide a strong but flexible connection between the distal radius and ulna that allows forearm rotation; and
(4) support the ulnar portion of the carpus through connections to the ulna and the radius.
The TFCC/ articular disk extends from the ulnar edge of the lunate fossa at the distal rim of the sigmoid notch and blends peripherally with the radioulnar ligaments
The radioulnar ligaments(PALMAR AND DORSAL) are the principal stabilizers of the DRUJ. The ligaments extend from the palmar and dorsal distal margins of the sigmoid notch and converge in a triangular configuration to attach to the ulna. the palmar ligament prevents dorsal displacement in pronation, and the dorsal ligament restrains palmar displacement in supination.

TFCC ANATOMY

Because its skeletal architecture imparts minimal stability to the DRUJ, the soft tissues are the prime stabilizers.
Several soft tissue structures contribute to DRUJ stability, including the pronator quadratus, ECU, interosseous membrane (IOM), DRUJ capsule, articular disk/TFCC, and palmar and dorsal radioulnar ligaments.
Although multiple structures contribute to DRUJ stability, the TFCC is generally accepted as the primary static stabilizer in the transverse plane.

BLOOD AND VASCULAR SUPPLY OF TFCC
Its vascular supply is primarily via the anterior interosseous artery and ulnar artery.
Vascular penetration into the disk extends only to its outer 15%, leaving the central portion essentially avascular.
Similar to its vascular distribution, the neural supply of the TFCC excludes the central portion of the disk.
The volar and ulnar portions of the TFCC receive innervation from the ulnar nerve, and the dorsal portion receives innervation from the posterior interosseous nerve.
PHYSICAL EXAMINATION
Symptoms are due to instability, stiffness, or degeneration,
Tenderness in the soft depression between the flexorcarpi ulnaris (FCU) tendon, ulnar styloid, and triquetrum is suggestive of a TFCC injury.
Decreased motion and crepitus during pronation-supination are signs of DRUJ arthritis, which may be accentuated by manually compressing the joint.
Increased anteroposterior translation of the ulna on the radius during passive manipulation is evidence of DRUJ instability.

IMAGING A standard posteroanterior radiograph (neutral forearm rotation) is taken with the
shoulder abducted 90 degrees, the elbow flexed 90 degrees, the forearm and palm flat on the cassette, and the wrist in neutral flexion-extension and neutral radioulnar deviation.
Measure the Ulnar Variance
The standard lateral radiograph is taken with the shoulder at the patient’s side (0 degrees abduction), the elbow flexed 90 degrees, and the wrist in a neutral position. An accurate view is marked by the palmar surface of the pisiform visualized midway between the palmar surfaces of the distal pole of the scaphoid and the capitate (the so-called SPC lateral).
Evidence of DRUJ instability can be accentuated in a lateral stress view in which the patient holds a 5-lb weight with the forearm in pronation and the x-ray beam is directed “cross-table.”
Semisupinated and semipronated views better show the rims of the sigmoid notch and the dorsal and volar aspects of the ulnar head and are useful to evaluate for fractures and arthritis.



Imaging: CT
Several measurement methods have been used to assess DRUJ instability, including use of dorsal and palmar radioulnar lines described by Mino and associates,
1. epicenter and congruency methods proposed by Wechsler and colleagues,
2. radioulnar ratio described by Lo and co-workers


IMAGING : MRI
More useful in the diagnosis of TFCC tears, with improved sensitivity, specificity, and accuracy in addition to making anatomic measurements and assessing stability.


Other imaging modalities
Arthrography: used less frequently
Scintigraphy: It is most useful in diagnosing ulnar impaction syndrome, in which the ulnar head, lunate, and triquetrum show increased uptake consistent with chronic inflammation in the bone and soft tissues.
Arthroscopy: Arthroscopy is sensitive for identifying traumatic TFCC tears or
degeneration in the central portion of the disk, chondromalacia, and ulnocarpal ligament injuries.
A lax or hypermobile TFCC under direct probing—the socalled trampoline effect—is indicative of an unstable TFCC.Arthrography

TFCC LESIONSPALMER CLASSIFICATIONTraumatic TFCC Lesions: Mostly due to
acute rotational injury to the forearm, a combined axial load and distraction injury to the ulnar border of the forearm, or a fall on the pronated outstretched hand.
Degenerative TFCC Lesions: due to chronic, excessive loading through the ulnocarpal joint and are a component of ulnar impaction syndrome.

Palmer classification
Palmer Class 1-A tear/ central perforation
Signs and Symptoms:
ulnar-sided wrist pain that is aggravated by power grip, especially with ulnar deviation or forearm rotation. It is a relatively common injury that produces pain and clicking.
Does not cause DRUJ instability and does not require acute treatment.
This tear is confined to the disk, located 2 to 3 mm ulnar to its radial attachment, and oriented volar to dorsal.
MANAGEMENT: These tears should initially be managed conservatively by rest, immobilization, anti-
inflammatory medications, and corticosteroid injection, but patients with ulnar-neutral wrists and especially patients with ulnarpositive wrists are less likely to respond to conservative management.
Arthroscopic débridement is the preferred treatment for traumatic TFCC tears when symptoms persist .
PALMER CLASS 1-B TEAR Partial or complete avulsion of the TFCC from its ulnar
attachments, with or without an ulnar styloid fracture . DRUJ instability may or may not be present.
SIGNS AND SYMPTOMS: similar to a class 1A tear, but a click is usually absent, and tenderness is more
ulnar, with point tenderness directly volar to the ulnar styloid. This site overlies the fovea, and tenderness located here has been termed the fovea sign
MANAGEMENT:
CONSERVATIVE: treated initially by above-elbow immobilization for 4 to 6 weeks with the forearm in neutral rotation with subsequent hand therapy.
Arthroscopic repair or Open repair(in chronic cases especially if there is an ulnar styloid nonunion)

Palmer class 1C Tears
Partial or complete tear of the ulnocarpal Ligaments, either within their substance or at their attachments to the lunate and triquetrum.
These injuries can occur in combination with class 1B tears or lunotriquetral ligament tears or both.
They are reported much less frequently than other TFCC injuries, probably because they are more difficult to diagnose and perhaps because they heal more reliably owing to their good vascular supply
The most obvious sign of injury is a volar “sag” of the carpus relative to the ulnar head, analogous to the “caput ulnae” syndrome in rheumatoid arthritis.
There is little published literature concerning treatment of these injuries.
Generally, these injuries should be managed conservatively, unless mechanical instability is present

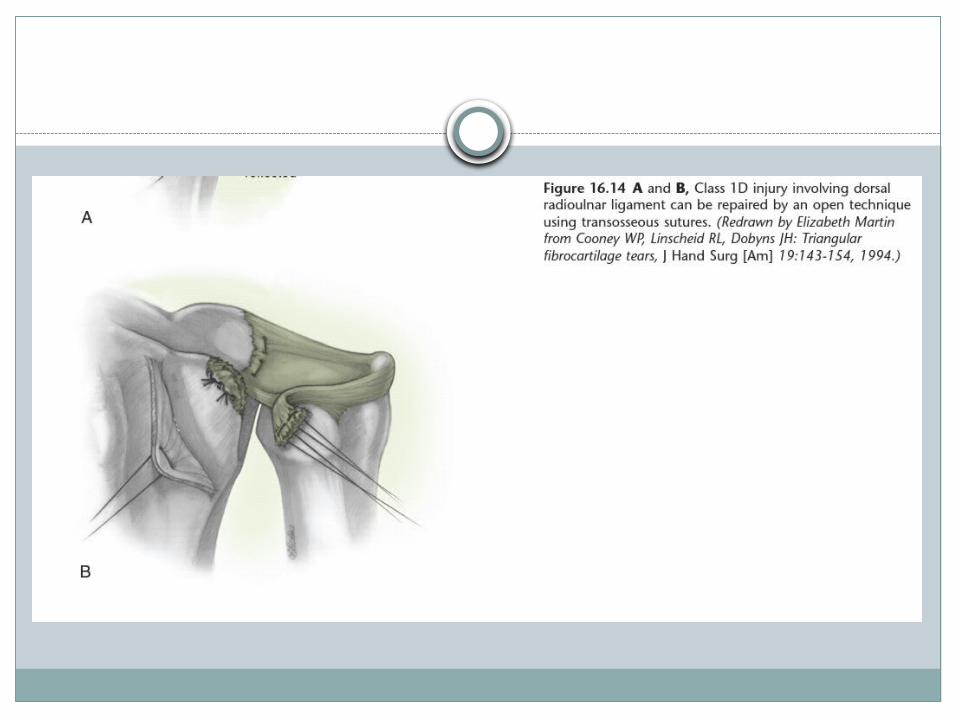
PALMER CLASS 1D TEARS
Partial or complete traumatic avulsion of the TFCC from the radius, with or without a bone fragment, and may involve one or both radioulnar ligaments
TREATMENT: frequently associated with a distal radius fracture and
usually respond to accurate fracture reduction of the radius
Cooney’s repair using an open technique through a dorsal approach



Cooney’s repair

ACUTE DISTAL RADIOULNARJOINT INSTABILITY
Causes: DRUJ dislocation: dorsal more common than volar Distal radius fracture/Galaezzi Ulnar styloid fractures
The radioulnar ligaments can tolerate no more than 5 to 7 mm of radial shortening before one or both ligaments tear.
In most cases, the secondary stabilizers of the DRUJ, including the IOM, ECU subsheath, ulnocarpal ligaments, and lunotriquetral interosseous ligament, maintain sufficient stability during healing to result in a stable joint.
Fracture reduction and maintenance of alignment of the radius are the most important factors to allow stable healing of the disrupted DRUJ


Evaluation
An acute dislocation usually produces an obvious deformity with the ulnar head locked over a rim of the sigmoid notch.
Local tenderness, swelling, and limited motion are the characteristic findings on presentation.
Deep tenderness along the IOM and swelling or pain at the proximal radioulnar joint may indicate a concomitant Essex-Lopresti injury.
Instability after reduction is marked by increased translation of the ulnar head in neutral forearm rotation and may be present in supination or pronation depending on the injured soft tissue stabilizers.
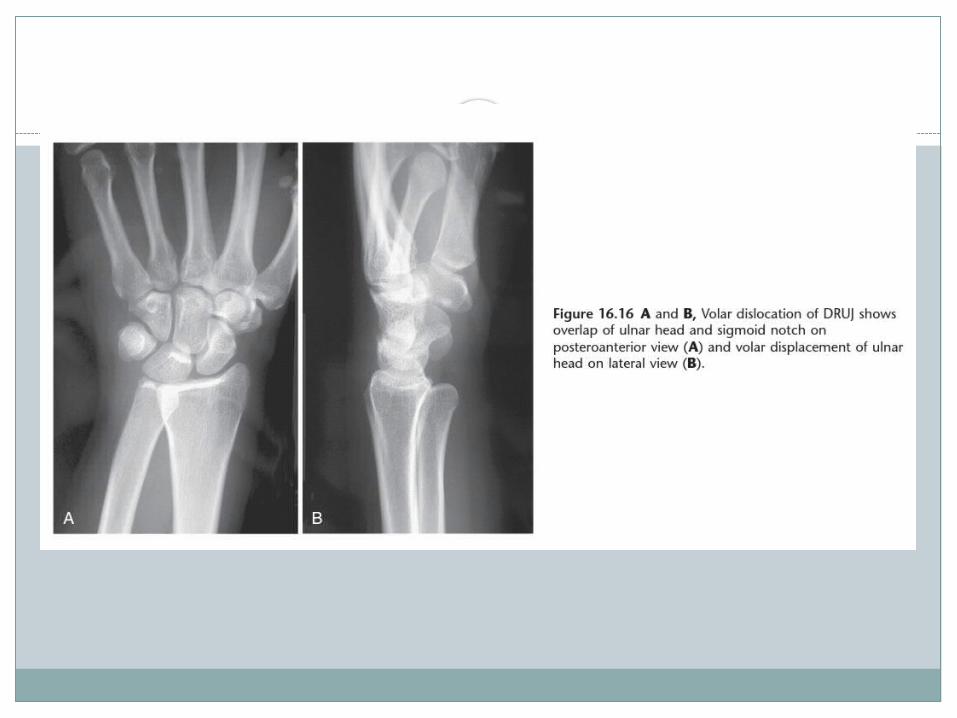
Simple Dislocations of DRUJ
Isolated dorsal DRUJ dislocation is more common than palmar dislocation.
Management: gentle pressure is applied over the ulnar head while the radius is
rotated toward the prominent ulna. After reduction, the joint should be tested over the full range of forearm rotation to determine the stable arc. Typically, a dorsal dislocation is most stable in supination, and a palmar dislocation is most stable in pronation.
If the joint is stable only in extreme pronation or supination, additional treatment should be considered, such as radioulnar pinning in the position of greatest stability or TFCC repair.
If the joint is stable in an acceptable position of forearm rotation, it is treated with an above-elbow cast in this position for 3 to 4 weeks followed by use of a well-molded short arm cast for 2 to 3 weeks

Ulnar Styloid Fractures and Nonunions
Frykman reported that ulnar styloid fractures occurred in approximately 61% of distal radius Fractures.
Fractures through the styloid base, especially when displaced, are associated with a higher risk of DRUJ instability. Fixation of the styloid restores DRUJ stability, provided that the TFCC is not otherwise damaged.
Indications OF ULNAR STYLOID FRACTURE FIXATION: Isolated displaced fracture through base of styloid, associated with unstable DRUJ, Persistent DRUJ instability after accurate reduction of radius fracture
Contraindications: Small fragment through its tip ,Nondisplaced fracture without DRUJ instability
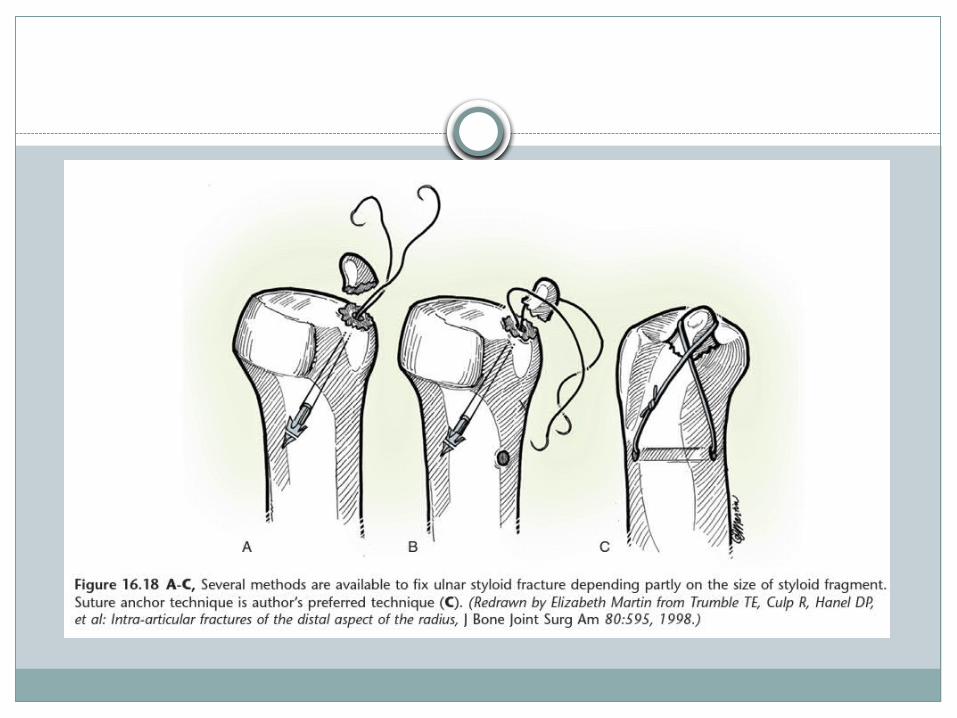
METHODS OF FIXATION: fixation of the ulnar Styloid fracture , including Kirschner wires, tension
band wiring, compression screw, variable-pitch headless screws, mini-fragment plates, and suture anchors
Symptomatic nonunion of the ulnar styloid is an uncommon problem that is usually best treated by simple subperiosteal excision. If the fragment is large, and the TFCC is unstable, the periphery of the TFCC is repaired to the styloid base after fragment excision with transosseous sutures

POST-TRAUMATIC (CHRONIC) DISTALRADIOULNAR JOINT INSTABILITY
CAUSES: isolated trauma to the DRUJ fractures of the distal radius and ulna Madelung deformity unsuccessful attempts to repair the TFCC, inflammatory arthritis.
DRUJ instability after a distal radius or forearm malunion usually manifests as loss of forearm rotation, prominence of the ulnar head, and ulnar-sided wrist pain.
Complaints are caused by a combination of effects of the malunion on the radiocarpal joint, ulnocarpal joint, and DRUJ.

Management:
Conservative: less preferred/poor outcomes
Surgical: Restoration of stability and a full, painless arc of motion are the
goals of surgical treatment for a post-traumatic unstable DRUJ. In established DRUJ instability without malunion or arthritis, the
ideal surgical option is late repair of the TFCC. A soft tissue reconstructive procedure is indicated when the TFCC is
irreparable and the sigmoid notch is competent. Fixation of a basilar fracture of the ulnar styloid alone in chronic
instability is usually ineffective because the soft tissues are attenuated
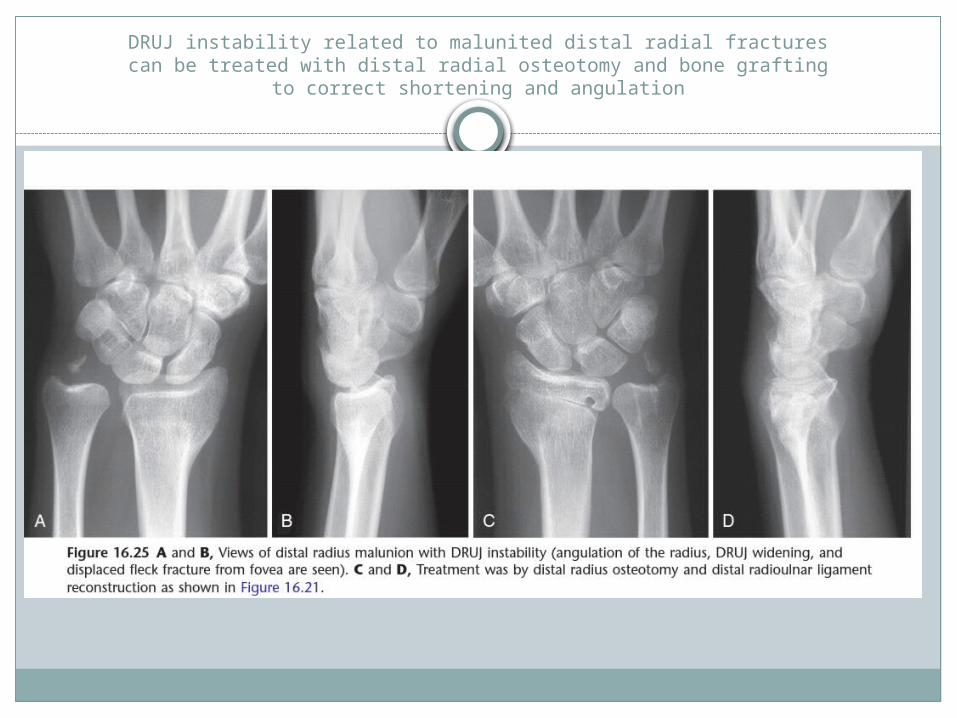
DRUJ instability related to malunited distal radial fracturescan be treated with distal radial osteotomy and bone grafting
to correct shortening and angulation


Adams identified three categoriesof soft tissue reconstruction for chronic DRUJ instability
Soft tissue Reconstructive techniques can be classified into three categories:
(1) a direct radioulnar tether that is extrinsic to the joint,
(2) an indirect radioulnar link via an ulnocarpal sling or a tenodesis,
(3) reconstruction of the distal radioulnar ligaments

Soft tissue Reconstructive techniques
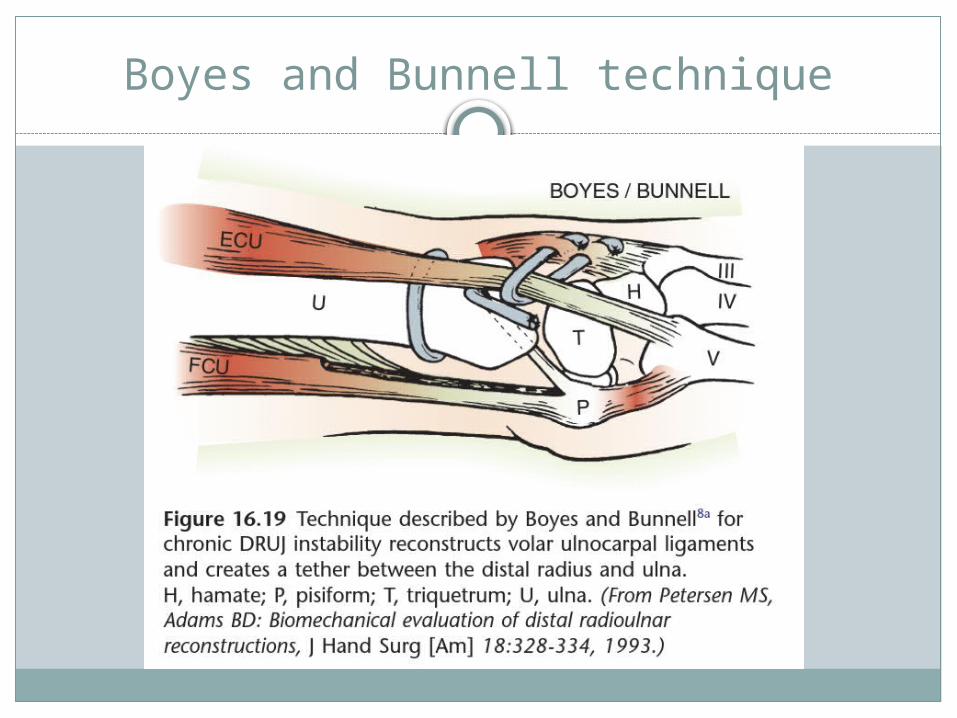
1. Boyes and Bunnell:-reconstructs volar ulnocarpal ligaments and creates a
tether between the distal radius and ulna).
2. Hui and Linscheid:-reconstructs volar ulnocarpal ligament using strip of FCU tendon.
3. Johnston Jones and Sanders:-reconstruction of both radioulnar ligaments with a palmaris tendon graft
Boyes and Bunnell technique

Hui and Linscheid technique

Johnston Jones and Sanders technique

Sigmoid notch osteoplasty
To improve the mechanical buttressing effect of the rim of the sigmoid notch, an osteoplasty can be considered as an isolated procedure or to complement a ligament reconstruction.
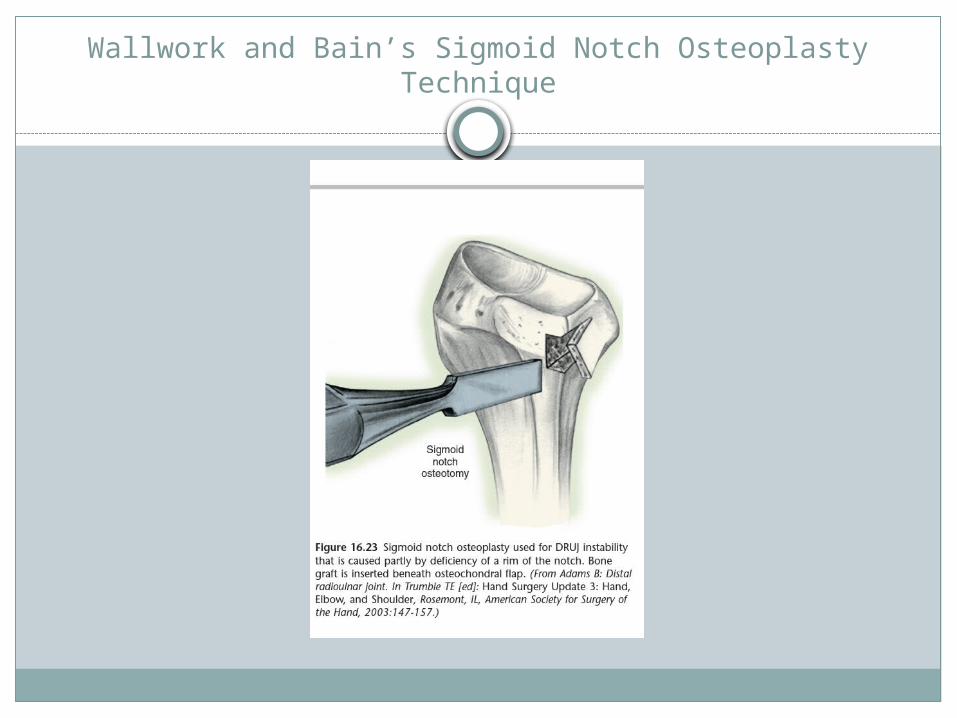
Wallwork and Bain’s Sigmoid Notch Osteoplasty Technique

Hermansdorfer and Kleinman found reattachment of the TFCC effective for minimal subluxation.
The reports of Bach et al. and of Scheker et al. suggested that tenodesis augmentation of TFCC repair with extensor carpi ulnaris (Bach) or tendon graft reconstruction through radioulnar drill holes (Scheker) helped to stabilize the DRUJ.
Adams emphasized the importance of reconstruction of the distal radioulnar ligaments to restore DRUJ stability and to preserve DRUJ motion

In patients with posttraumaticDRUJ instability, Adams and Berger found that anatomicalreconstruction of the distal radioulnar ligaments restored
stability, preserved motion, and relieved pain
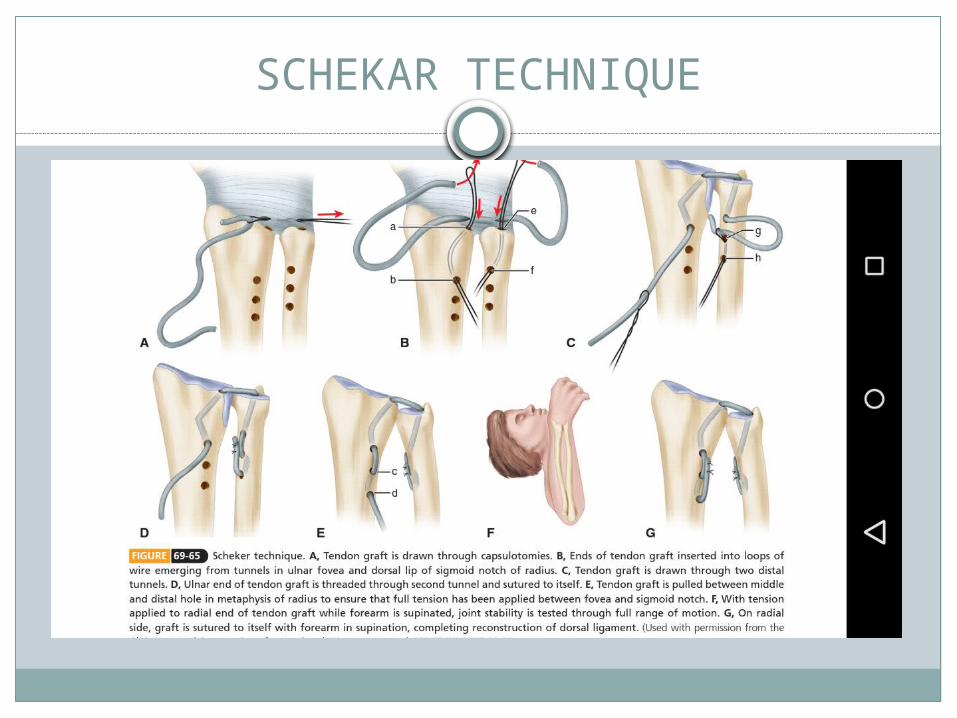
SCHEKAR TECHNIQUE

ULNAR IMPACTION-ABUTMENT AND DISTALRADIOULNAR JOINT ARTHRITIS
Patients with acquired or developmental ulnar-positive variation may develop degenerative changes in the triangular fibrocartilage, ulnar head, articular surfaces of the lunate and triquetrum, and lunotriquetral interosseous ligament.
Symptoms: ulnar wrist pain aggravated by ulnar deviation with forearm rotation
CAUSES of Positive ulnar variation: may be a normal finding Madelung deformity. Shortening of the radius after fracture radial head fracture-dislocation with interosseous membrane injury (Essex-
Lopresti), traumatic growth arrest of the distal radius

MANAGEMENT
CONSERVATIVE: activity modification, splinting,oral medications, and injections of corticosteroids.
SURGICAL: Arthroscopic joint débridement, open or arthroscopic distal ulnar resection, and ulnar shortening osteotomy

ULNAR SHORTENING OSTEOTOMY(CHUN AND PALMER))

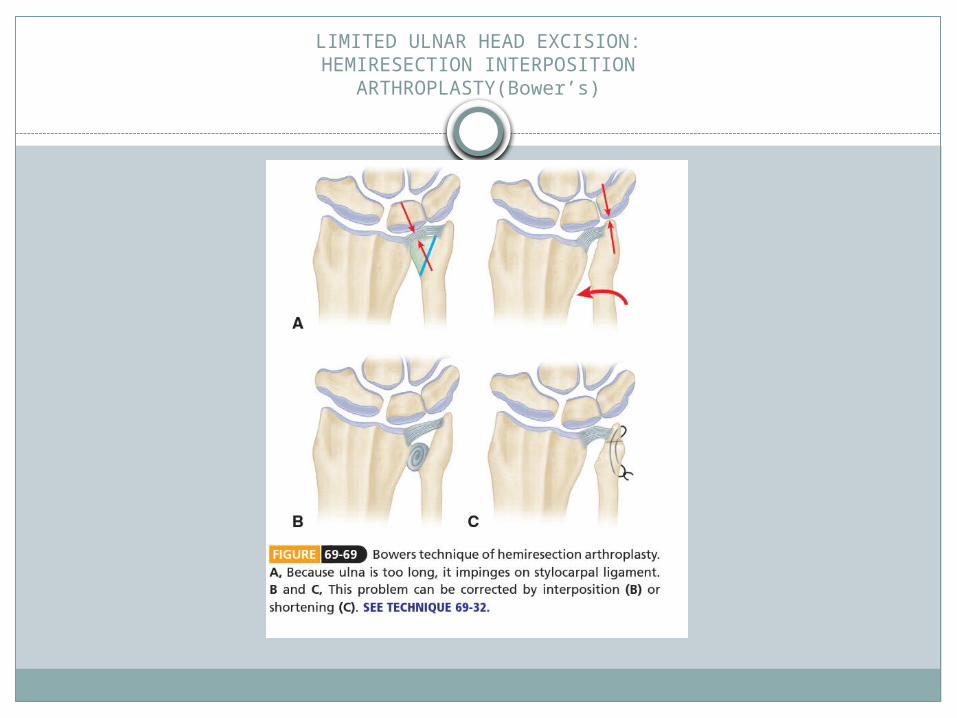
LIMITED ULNAR HEAD EXCISION:HEMIRESECTION INTERPOSITION
ARTHROPLASTY(Bower’s)
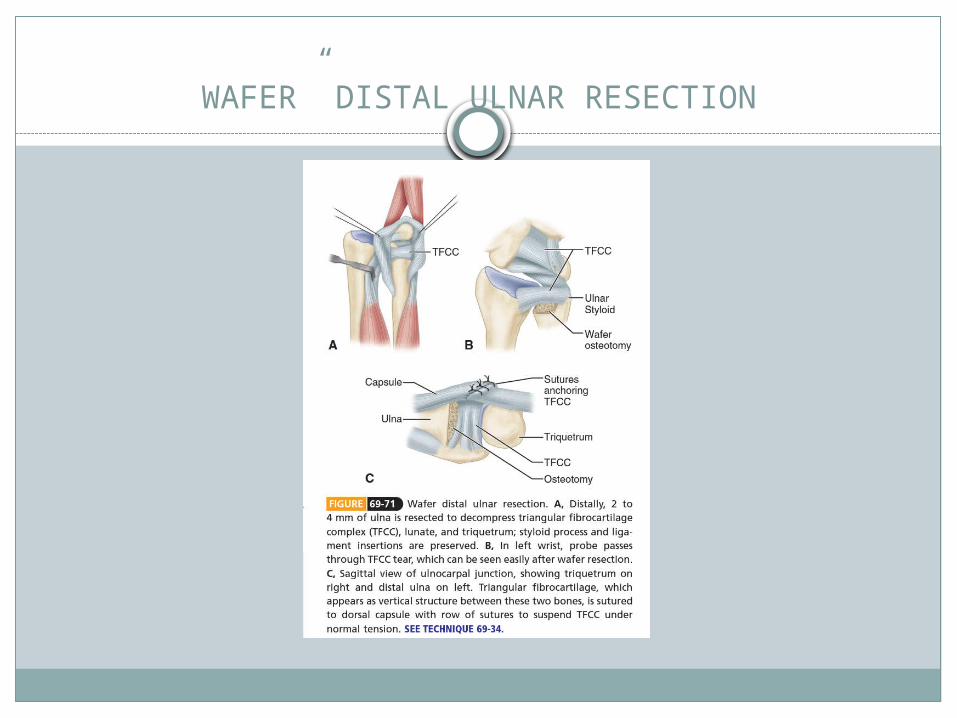
WAFER” DISTAL ULNAR RESECTION

Sauve Kapandji’s procedure
1. Resection of a portion of distal ulna shaft andfusion of ulnar head to radius.
2. Maintains function of TFCC & maintains normal anatomic configuration of wrist.
3. Should not be performed with ulnar variance positive unless ulna shortened as part of procedure

DISTAL RADIOULNAR ARTHRODESIS WITH DISTAL ULNAR PSEUDARTHROSIS (BALDWIN; SAUVÉ-KAPANDJI; LAUENSTEIN)

Distal Ulnar Resection(Darrach Procedure)
The general indication for a distal ulnar resection is any condition that causes incongruity or arthritis of the DRUJ, with resultant pain or stiffness.
The procedure is particularly effective in a low-demand patient with an incongruous or degenerative sigmoid notch owing to the sequelae of an intra-articular fracture.
COMPLICATIONS: Increased ulno-carpal translocation Decreased grip strength Unstable rotation of radio carpal joint

THANK YOUDR. BEN