dsm-5: practical overview of changes · • assigning dsm diagnosis provides direct access to...
TRANSCRIPT

DSM-5: Practical Overview of Changes
Faculty
Michael B. First, MD
Professor of Clinical PsychiatryColumbia UniversityNew York, New YorkAttending Physician
New York-Presbyterian HospitalNew York, New York
Faculty Disclosure
• Dr. First receives royalties from DSM-related publications
Learning Objectives
• Review the new organization structure of the Diagnostic and Statistical Manual of Mental Health Disorders, Fifth Edition (DSM-5)
• Explain the rationale, implications, and manifestations of the incorporation of a more dimensional approach to DSM-5
• Describe the background and practical implications of the forthcoming changeover from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) to ICD-10-CM codes
• Discuss the changes being made throughout the DSM-5, including their rationale and practical implications
• Identify the controversies surrounding some of the changes, including their pros and cons
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Health Disorders. Fifth Edition. Arlington, VA: American Psychiatric Association; 2013.
Value of Making a DSM Diagnosis
• Well-defined and reliable terminology facilitates communication among clinicians, administrators, lawyers, patients, and families
– Provides convenient short-hand when describing psychiatric presentations
• Assigning DSM diagnosis provides direct access to psychiatric literature about treatment, prognosis, etc
– Journal articles, practice guidelines, textbooks for the past 33 years have been geared to DSM definitions of mental disorders
• Facilitates assignment of diagnostic code for payment
Limitations of Making a DSM Diagnosis
• Most treatment decisions are geared to symptoms regardless of diagnosis (eg, psychosis)
• Diagnostic heterogeneity limits predictive power of diagnoses
• Diagnoses are not informative about etiology or pathophysiology
• High rates of NOS limit clinical utility in terms of communication and access to the literature
NOS = not otherwise specified.
Why a DSM-5 Is Needed
• Longest gap between DSMs ever
– DSM-IV criteria sets reflect research base circa 1993 (20-year gap)
– Text reflects research base circa 1999 (14-year gap)
• Need to coordinate with ICD-11 (to be published in 2017)
• Potential for DSM-5 to update definitions to reflect most recent research findings and to address identified weaknesses
Will DSM-5 Be More “Etiological” and/or Based on Objective Measures?
• The simple answer: No
• Genetics, neuroimaging, biological markers, etc will NOT be included in definitions of disorders in DSM-5/ICD-11
– Exception: polysomnography in sleep disorders and hypocretin in narcolepsy
• Problem is lack of diagnostic specificity on an individual patient level
– Tests able to identify clear differences between groups but not between individuals because of within group variability (ie, some non-affected people will have abnormal value on test that is higher than “affected” individuals)
Changes in Diagnostic Groupings (“Metastructure”)
• DSM-IV diagnostic classes mostly based on shared symptom presentation (eg, anxiety disorders)
• DSM-5 regrouping of disorders reflects 20 years of research on how the brain functions and interactions between genes and environment
– Groupings are based on putative common underlying factors (eg, internalizing vs externalizing) and underlying vulnerabilities
• Ordering of diagnostic groupings also reflects relationships among disorders
– eg, bipolar disorders following schizophrenia spectrum

DSM-5 “Metastructure”
DSM- 5
• Neurodevelopmental Disorders
– Includes Intellectual Disability, Global Developmental Delay, Autism Spectrum Disorder, Learning Disorders, Communication Disorders (including Social Pragmatic Communication Disorder), ADHD, Motor Disorders (Tics, Stereotyped Movement, Coordination)
• Schizophrenia Spectrum and Other Psychotic Disorders
– Includes Schizophrenia, Schizotypal PD, Schizoaffective, Brief Psychotic, Delusional Disorder, Substance-induced Psychotic Disorder, Psychotic Disorder due to AMC, Catatonia Associated with Another Mental Disorder, Catatonia due to AMC
DSM-IV
• Childhood Disorders
– Mental Retardation, Learning Disorders, Communication, PDD, Tic Disorders, part of Disruptive Behavior
• Schizophrenia and Other Psychotic Disorders
– Schizotypal in PD
ADHD = attention-deficit/hyperactivity disorder; AMC = another medical condition; PD = personality disorder; PDD = pervasive developmental disorder.
DSM-5 “Metastructure” (continued)
DSM-5
• Bipolar and Related Disorders
– Includes Bipolar I, Bipolar II, Cyclothymic, Substance-Induced Bipolar, Bipolar due to AMC
• Depressive Disorders
– Includes MDD, Chronic Persistent Depressive Disorder, Disruptive Mood Dysregulation Disorder, Premenstrual DysphoricDisorder, Substance-induced, due to AMC
DSM-IV
• Mood Disorders
MDD = major depressive disorder.
DSM-5 “Metastructure” (continued)
DSM-5
• Anxiety Disorders– Includes Separation Anxiety, Selective
Mutism, Social Anxiety, Specific Phobia, Panic, Agoraphobia, GAD, Substance-induced Anxiety, Anxiety due to AMC
• Obsessive-Compulsive and Related Disorders
– Includes OCD, BDD, Hoarding, Trichotillomania, Excoriation Disorder, Substance-induced, due to AMC
• Trauma- and Stress-Related Disorders
– Includes PTSD, Acute Stress, Reactive Attachment, Disinhibited Social Engagement Disorder, Adjustment Disorders
DSM-IV
• Anxiety Disorders– Separation Anxiety within Childhood
– Reactive Attachment within Childhood
– Trichotillomania within Impulse Control
• Adjustment Disorders
BDD = body dysmorphic disorder; GAD = generalized anxiety disorder; OCD = obsessive-
compulsive disorder; PTSD = posttraumatic stress disorder.

DSM-5 “Metastructure” (continued)
DSM-5• Dissociative Disorders
– Includes Depersonalization/ Derealization, Dissociative Amnesia, DID
• Somatic Symptom Disorders– Includes Somatic Symptom Disorder
Illness Anxiety, Conversion Disorder, Factitious Disorder, PFAMC
• Feeding and Eating Disorders– Includes Anorexia, Bulimia, Binge-
Eating Disorder, Avoidant/Restrictive Food Intake, Pica, Rumination Disorder
• Elimination Disorders– Includes Enuresis, Encopresis
DSM-IV• Dissociative Disorders
• Somatoform Disorders
• Factitious Disorders
• Feeding Disorders
• Eating Disorders
• Elimination Disorders
– Formerly in Childhood
DID = dissociative identity disorder; PFAMC = psychological factors affecting medical condition.
DSM-5 “Metastructure” (continued)
DSM-5• Sleep/Wake Disorders
– Includes several new disorders from ICSD including REM Sleep Behavior, Restless Leg Syndrome
• Sexual Dysfunctions
– Includes Male Hypoactive Sexual Desire Disorder, Erectile Disorder, Early Ejaculation, Delayed Ejaculation, Female Sexual Interest/Arousal Disorder, Female Orgasmic Disorder Genito-Pelvic Pain/Penetration Disorder
• Gender Dysphoria
DSM-IV
• Sleep Disorders
• Sexual Dysfunctions (within Sexual Disorders)
• Gender Identity Disorder (within Sexual Disorders)
ICSD = International Classification of Sleep Disorders; REM = rapid eye movement.
DSM-5 “Metastructure” (continued)
DSM-5• Disruptive, Impulse Control,
and Conduct Disorders
– Includes ODD, Conduct Disorder, Antisocial PD, Pyromania, Kleptomania, IED
• Substance Use and Addictive Disorders
– Includes Substance Use, Substance-Induced, Intoxication, Withdrawal, Gambling Disorder
DSM-IV• Disruptive Behavior
– ODD, Conduct (in Childhood)
• Impulse Control Disorder
– Pyromania, Kleptomania, IED
• Antisocial PD
– In personality disorders
• Substance-Related Disorders
– Pathological Gambling in Impulse Control Disorders
IED = intermittent explosive disorder; ODD = oppositional defiant disorder.
DSM-5 “Metastructure” (continued)
DSM-5
• Neurocognitive Disorders
– Includes Delirium, Major Neurocognitive Disorder, Mild Neurocognitive Disorder
• Personality Disorders
• Paraphilias
DSM-IV
• Delirium, Dementia, Amnesticand Other Cognitive Disorders
• Personality Disorders
• Paraphilias (within Sexual Disorder)
DSM-5 and Dimensions
“We have decided that one, if not the major, difference between DSM-IV and DSM-5 will be the more prominent
use of dimensional measures in DSM-5”
Regier DA, et al. Am J Psychiatry. 2009;166(6):645-650.
Dimensions vs Categories
• Although most patient data is dimensional (eg, blood pressure, laboratory values, severity of depression), all classification systems in medicine are categorical (eg, hypertension, MDD) reflecting nature of medical decisions
• Dimensions most useful for
– Documenting subthreshold symptoms
– Indicating and monitoring of disorder severity
– Communicating dimensional nature of syndromes

DSM-5 Moves Toward Dimensionality
• Combining categories with lower and higher severities into single broad categories with dimensional severity indicators
– Autistic Disorder (more severe) and Asperger’s disorder (less severe) combined into Autism Spectrum Disorder
– Substance Dependence (more severe) and Substance Abuse (less severe) combined into Substance Use Disorder
DSM-5 Moves Toward Dimensionality(continued)
• Reconceptualization of Neurocognitive Disorders on a dimensional continuum
– Major Neurocognitive Disorder: significant cognitive decline that interferes with independence in everyday activities
– Mild Neurocognitive Disorder: modest cognitive decline that does not interfere with capacity for independence but requires greater effort, compensatory strategies, or accommodation
DSM-5 Moves Toward Dimensionality(continued)
• Original plan for radical change in classification of personality disorders to a trait model dividing personality into 5 domains: Negative Affectivity, Detachment, Antagonism, Disinhibition, and Psychoticism
• Ultimately rejected because of concerns about complexity, validity, reliability, and clinical utility
• Placed in Section III (“Emerging Measures and Models”)

DSM-5 Moves Toward Dimensionality(continued)
• Original plan to include cross-cutting symptom measures, a disability scale, plus 150+ disorder severity measures as an official part of DSM-5
• With 2 exceptions (severity of intellectual disability, autism spectrum disorder), all were relegated to Section III
– Only 3 of these measures included in print version of DSM-5; remainder available for free in the on-line supplement (www.psych.org/dsm5)
– Although dimensions of psychosis symptom severity appear in Section III, severity ratings for psychotic disorders in Section II entails their use
Concerns About Adding Dimensional Measures to DSM-5
• No evidence that adding dimensions improves patient management or outcome
• No evidence for feasibility of use of dimensions in typical psychiatric settings
• None of proposed DSM-5 dimensions are codable and thus information cannot be indicated to payers
• Many are extremely complex (eg, 8 dimensions for psychosis, each rated 0 to 4)
• Could be co-opted by insurers to limit care (see GAF, Axis II)
GAF = Global Assessment of Functioning.
When Does DSM-5 Become “Official”?
• Answer: Never
– The only official coding system is ICD-9-CM (until October 1, 2015, when it will be ICD-10-CM)
– DSM-5 can be used immediately and will produce legal codes now (and after October 1, 2015)
– For most clinicians, its use is voluntary. One can meet legal requirements by using ICD-9-CM/ICD-10-CM codes
– Some institutions may require use of DSM-5 and may establish a mandatory implementation date
– Generally advantageous to use DSM-5 in order to maintain effective communication with the vast majority of clinicians who will be using it
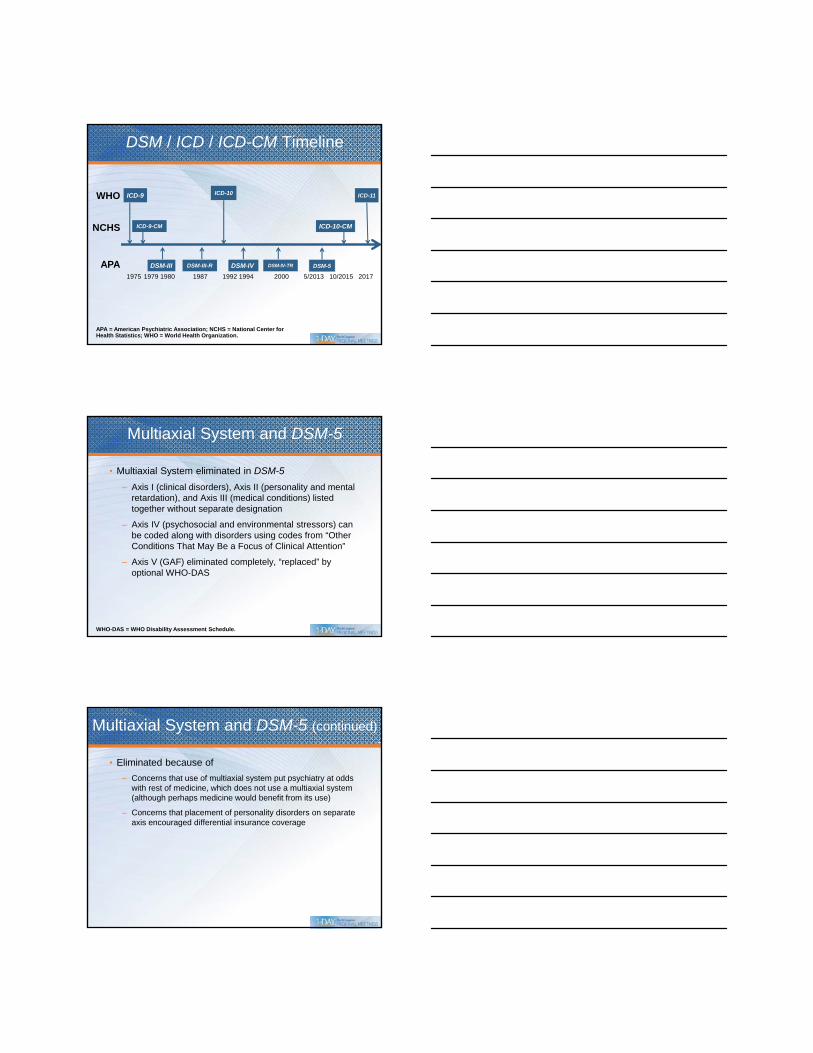
DSM / ICD / ICD-CM Timeline
1975 1979 1980 1987 1992 1994 2000 5/2013 10/2015 2017
ICD-9-CM ICD-10-CM
DSM-III DSM-III-R DSM-IV
ICD-10
DSM-IV-TR DSM-5
ICD-11ICD-9
APA = American Psychiatric Association; NCHS = National Center for Health Statistics; WHO = World Health Organization.
WHO
NCHS
APA
Multiaxial System and DSM-5
• Multiaxial System eliminated in DSM-5
– Axis I (clinical disorders), Axis II (personality and mental retardation), and Axis III (medical conditions) listed together without separate designation
– Axis IV (psychosocial and environmental stressors) can be coded along with disorders using codes from “Other Conditions That May Be a Focus of Clinical Attention”
– Axis V (GAF) eliminated completely, “replaced” by optional WHO-DAS
WHO-DAS = WHO Disability Assessment Schedule.
Multiaxial System and DSM-5 (continued)
• Eliminated because of
– Concerns that use of multiaxial system put psychiatry at odds with rest of medicine, which does not use a multiaxial system (although perhaps medicine would benefit from its use)
– Concerns that placement of personality disorders on separate axis encouraged differential insurance coverage
Case Example: DSM-IV vs DSM-5
• 35-year-old homeless male with 13-year history of schizophrenia, type 2 diabetes, and recurrent hospitalizations for exacerbation of psychotic symptoms is brought to emergency room by police because of violent behavior related to hearing voices
• He also has a childhood history of conduct disorder with a pattern of antisocial behavior that has persisted into adulthood
DSM-IV Coding Using Multiaxial System
• Axis I: 295.30 Schizophrenia, Paranoid Type
• Axis II: 301.7 Antisocial Personality Disorder
• Axis III: 250.00 diabetes, type 2
• Axis IV: Homelessness
• Axis V: GAF = 25
DSM-5 Coding
• DSM-5: 295.90 Schizophrenia, multiple episodes, currently in acute episode, delusions present and severe, hallucinations present and severe, absent disorganized speech, abnormal psychomotor behavior and negative symptoms; 250.00 diabetes, type 2; 301.7 Antisocial Personality Disorder; V60.0 homelessness
WHO-DAS
• World Health Organization Disability Assessment Schedule 2.0
• Included in Section III; no evidence for its validity or clinical utility in mental health settings
• 36-item measure that assesses disability in adults age 18 years and older
• Self-report; if individual is impaired, knowledgeable informant can complete the proxy-administered version
WHO-DAS (continued)
• Individual asked to rate how much difficulty he or she has had in specific areas of functioning over the past 30 days
• 6 domains assessed:
– Understanding and communicating
– Getting around
– Self-care
– Getting along with people
– Life activities
– Participation in society
WHO-DAS (continued)
• Examples of items
– From Participation in Society domain: “In the past 30 days, how much of a problem did you have joining in community activities (for example, festivities, religious, or other activities) in the same way as anyone else can?”
– From Self-care domain: “In the past 30 days, how much of a problem did you have washing your whole body?”
– From Getting Around domain: “In the past 30 days, how much of a problem did you have standing for long periods, such as 30 minutes?”
Need for NOS Categories
• To cover the many presentations that do not fit into the precise diagnostic boundaries of the specific DSM-5disorders
• To cover situations in which the clinician does not have sufficient information to make a specific DSM-5diagnosis (eg, emergency room settings)
• To cover situations in which the clinician is uncertain whether a psychiatric presentation is primary, substance-induced, or due to AMC
Problem with NOS Categories
• Primary goal of DSM is to facilitate communication
• NOS categories communicate that the presentation is predominated by a particular symptom (eg, Psychotic Disorder NOS, Depressive Disorder NOS) but provides no other diagnostic information
NOS Split into 2 Categories in DSM-5
______ Disorder NOS
Other Specified _____ Disorder
Unspecified
_____ Disorder

Other Specified _____ Disorder
• For presentations in which the clinician has fully characterized the presentation but does not meet full criteria for existing disorders or for syndromes not included in the DSM-5
• Clinician writes in the reason why criteria are not met, eg, “Other Specified Bipolar Disorder, Short-duration hypomanic episodes (2-3 days) and major depressive episodes,” “Other Specified Feeding or Eating Disorder, Night Eating Syndrome”
Other Specified _____ Disorder (continued)
• Many Other Specified categories provide a numbered list of examples
– “Examples of presentations that can be specified using the ‘other specified’ designation include the following”
• Clinician can also write in the reason if not included among examples
• Problem: provides quasi-legitimacy with potential forensic implications to categories which are not accepted in DSM-5 as valid categories (eg, Attenuated Psychosis Syndrome listed as example)
Autism Spectrum Disorder
• Combined 5 DSM-IV categories: Autistic Disorder, Asperger’s Disorder, Childhood Disintegrative Disorder, Rett’s Disorder, and Pervasive Developmental Disorder NOS
• Reflects dimensional nature of autism
• Evidence that Asperger’s is simply milder form of Autism rather than distinct condition (eg, relatives of Asperger’s have increased risk of both Asperger’s and Autistic Disorder)
Autism Spectrum Disorder (continued)
• Persistent deficits in social communication and social interaction (ALL)
– Deficits in social-emotional reciprocity
– Deficits in non-verbal communication
– Deficits in developing and maintaining relationships
• Restricted repetitive behaviors or interests (2 of 4)– Stereotyped behavior or speech
– Need for sameness and routines
– Abnormal fixations or restricted interests
– Hyper- or hypo-reactivity to sensory input
• Spectrum of severity provided (“ranging from…”)
Autism Spectrum Disorder Controversies
• Loss of Asperger’s as a distinct category– Rare example of destigmatized category (“Aspies” who
claim Einstein had Asperger’s)
– Concern about being put into same boat as more ill Autistic patients
• Increase in requirement in social communications domain (2 of 4 in DSM-IV vs 3 of 3 in DSM-5) led to concern about false negatives
• Note added– “Individuals with a well-established DSM-IV diagnosis of
autistic disorder, Asperger’s disorder, or pervasive developmental disorder NOS should be given the diagnosis of autism spectrum disorder.”
Schizophrenia Changes
• Diagnosis narrowed by excluding cases that met criteria for DSM-IV Schizophrenia
– Cases of disorganized or catatonic behavior AND negative symptoms (in DSM-5, delusions, hallucinations, or disorganized speech are required)
– Cases of bizarre delusions or certain kinds of auditory hallucinations (eg, running commentary) without other symptoms (in DSM-5, need 2 out of 5)

Schizophrenia Changes (continued)
• Subtypes, some dating back to turn of the century, are eliminated
– Paranoid Schizophrenia
– Catatonic Schizophrenia
– Disorganized Schizophrenia
– Undifferentiated Schizophrenia
– Residual Schizophrenia
• Not actually “types;” patients often change types over time
• Catatonia still can be indicated as a specifier
Severity Profile of Current Schizophrenia Symptoms
• Severity rated by quantitative assessment or primary symptoms of psychosis (ie, delusions, hallucinations, disorganized speech, abnormal psychomotor behavior, and negative symptoms)
• Rated for current severity (at its most severe point in the past 7 days) on a 5-point scale from 0 (not present) to 4 (present and severe)
• Each psychotic disorder (including substance-induced and psychotic disorder due to AMC) include these specifiers
Examples: Current Severity Rating for Delusion and Disorganized Speech
Domain Absent EquivocalPresent but
MildPresent and
ModeratePresent and
Severe
II. Delusions
0 1 = severity or duration not sufficient to be considered psychosis
2 = little pressure to act upon delusional beliefs, not very bothered by delusions
3 = some pressure to act upon beliefs, or is somewhat bothered by beliefs
4 = severe pressure to act upon beliefs, or is very bothered by beliefs
III. Disorganized Speech
0 1 = severity or duration not sufficient to be considered dis-organization
2 = some difficulty following speech
3 = speech often difficult to follow
4 = speech almost impossible to follow
Bipolar and Related Disorders
• Reduction of false positives
– Criterion A for mania and hypomania will require both mood disturbance (euphoric, elevated, or irritable mood) plus increase in activity or energy
– Mood disturbance must be present for most of the day, nearly every day during 4-day period (for hypomania) or 7-day period (for mania)
Elimination of Mixed Episode
• “With Mixed Features” specifier available for Manic, Hypomanic, and Major Depressive Episodes
– Manic or Hypomanic Episode with Mixed Features: 3+ depressive symptoms for majority of days
– Major Depressive Episode with Mixed Features: 3+ manic symptoms for majority of days (however, if full criteria for manic met, then Manic Episode with Mixed Features)
“Anxious Distress” Specifier
• Anxiety comorbidity associated with worse outcome (eg, increased suicidality, more difficult to manage)
• Anxious symptoms for majority of days: feeling keyed up, restless, difficulty concentrating, fear that something awful might happen, fear of losing control
• Severity:
– Mild = 2 Sxs
– Moderate = 3
– Moderate-Severe = 4-5
– Severe = 4-5 with motor agitation

Disruptive Mood Dysregulation Disorder
• Intended to provide diagnostic home for children with severe frequent temper outbursts on top of a baseline of angry, irritable mood
• Because of irritability and mood reactivity, misdiagnosed as juvenile bipolar disorder and inappropriately treated
• Since 95% also meet criteria for ODD, comorbid diagnosis not given
Disruptive Mood DysregulationDisorder Controversies
• Pros:
– Meet clinical need for children who require treatment; only applicable DSM-IV category was ODD; does not capture the severity of this condition
– Provides visible alternative to juvenile bipolar
• Cons:
– Replacing one category that encourages antipsychotic use with another that is likely to (“mood dysregulation”)
– Limited empirical support, all from a single research center
Premenstrual Dysphoric Disorder
• “Promoted” from appendix where it has lived since DSM-III-R (1987)
– Marked affective lability, irritability or anger or interpersonal conflicts, depressed mood or anxiety in week before onset of menses, improve after onset, minimal or absent in week post-menses
– Additional symptoms (eg, lethargy, appetite, sleep changes) for a total of 5
– Must be present for most cycles in previous year
– Not merely exacerbation of existing disorder
– Must cause clinically significant distress
– Should be confirmed by prospective daily ratings for 2 cycles

Premenstrual Dysphoric Disorder (continued)
• Most controversial diagnosis in DSM-III-R and DSM-IV
– Benefits of recognition and treatment vs stigmatizing women
• Little controversy in DSM-5; perhaps due to FDA-approved treatments
FDA = US Food and Drug Administration.
Hoarding Disorder
• Hoarding occurs in 2% to 5% of the population and can lead to substantial distress and disability, as well as serious public health consequences
• Most cases do not meet criteria for OCD or OCPD
– Difficulty parting with possessions due to perceived need to save them and distress associated with act of discarding them
– Results in cluttered active living areas, compromising their intended use
OCPD = obsessive-compulsive personality disorder.
New Eating/Feeding Disorders
• Avoidant/Restrictive Food Intake Disorder
– Eating or feeding disturbance leading to persistent failure to meet energy or nutritional needs
– Examples include lack of interest in eating or food, avoidance of foods based on sensory characteristics, concerns about aversive consequences
• Binge-Eating Disorder (formerly in appendix)
– Binge eating without compensatory behavior
– Accompanied by other symptoms such as eating until uncomfortably full or when not hungry and feeling disgusted, guilty, or depressed
– Once a week for 3 months

Substance-Related and Addictive Disorders
DSM-5 Substance Use (2 of 11)
• Larger amounts taken than intended
• Persistent desire to cut down or control use
• Great deal of time to obtain, use, or recover
• Craving or strong desire to use
• Failure to fulfill role obligations
• Use despite social/interpersonal problems
• Activities given up or reduced
• Use where physically hazardous
• Use despite physical/psychological problem
• Tolerance
• Withdrawal
DSM-IV Dependence/Abuse
• Dependence (3)
• Dependence (4)
• Dependence (5)
• Not in DSM-IV
• Abuse (1)
• Abuse (4)
• Dependence (6)
• Abuse (2)
• Dependence (7)
• Dependence (1)
• Dependence (2)
Neurocognitive Disorders
• Major Neurocognitive Disorder
– Subsumes DSM-IV dementia and amnestic disorder
– Evidence of significant cognitive decline based on concern of individual, informant, or clinician AND substantial impairment in cognitive performance preferably documented by neuropsychological testing
– Severe enough to interfere with independence
– At a minimum, requires assistance with complex ADLs
ADLs = activities of daily living.
Neurocognitive Disorders (continued)
• Mild Neurocognitive Disorder
– Evidence of modest cognitive decline based on concern of individual, informant, or clinician AND modest impairment in cognitive performance preferably documented by neuropsychological testing
– NOT severe enough to interfere with capacity for independence
– Complex ADLs preserved but may require greater effort or compensatory strategies

Diagnosing Neurocognitive Disorders
• Determine whether cognitive impairment is major (“significant”) or mild (“modest”)
• Determine etiological factor
• Determine level of certainty regarding etiology, ie, “probable” or “possible” (only applies to some etiological causes)
• Indicate if “with behavioral disturbance,” eg, psychotic symptoms, mood disturbance, agitation, apathy, or other behavioral symptoms
Living Document: DSM-5.x
• Rather than revising the entire DSM at certain intervals, sections will be revised and updated depending on scientific advances
– For example, if biomarker is found for a diagnosis of Alzheimer’s disease, then that section only might be revised
• Might reduce profusion of small changes that are inevitable with current method (ie, temptation for workgroup members to leave their mark)
Summary
• DSM-5 revision characterized by many small changes reflecting new empirical evidence rather than paradigm shift
• Most significant change is reorganization of disorder groupings
• Original plan to add dimensions not implemented; instead dimensional measures included in Section III
Q&A Session