dua george systemic therapy for men with ... - duke university
TRANSCRIPT

Systemic Therapy for Men with Metastatic Prostate Cancer in 2018
Daniel George, MD Professor of Medicine and Surgery
Director of GU Oncology Duke Cancer Institute

Metastatic
Local Therapy
Castration Hormone Therapy
Tum
or V
olum
e an
d Ac
tivity
Sipuleucel-T
Time NONMETASTATIC
Asymptomatic Symptomatic
Docetaxel Cabazitaxel
Enzalutamide Radium-223
Natural History of Lethal Prostate Cancer and Treatment Options
Nonmetastatic
Abiraterone or Enzalutamide Radium-223
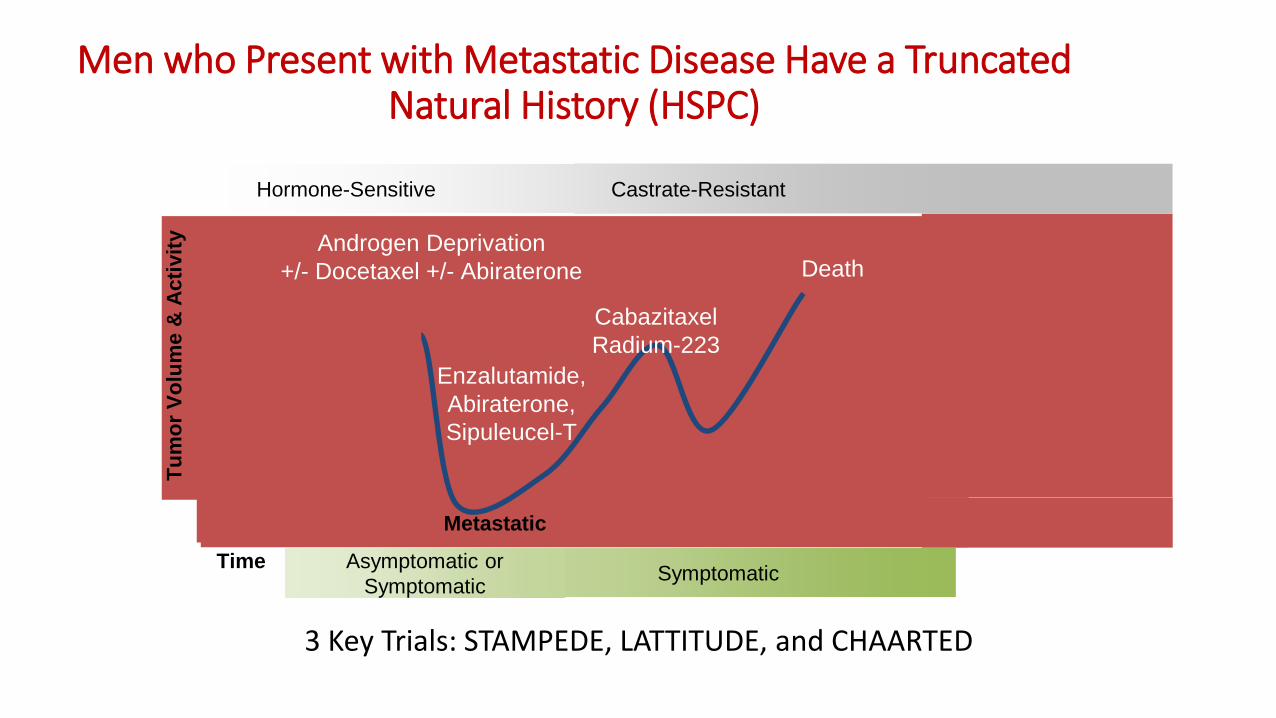
Men who Present with Metastatic Disease Have a Truncated Natural History (HSPC)
Symptomatic Time
Tum
or V
olum
e &
Act
ivity
Hormone-Sensitive Castrate-Resistant
Asymptomatic or Symptomatic
Death
Cabazitaxel Radium-223
Enzalutamide, Abiraterone, Sipuleucel-T
Androgen Deprivation +/- Docetaxel +/- Abiraterone
Metastatic
3 Key Trials: STAMPEDE, LATTITUDE, and CHAARTED
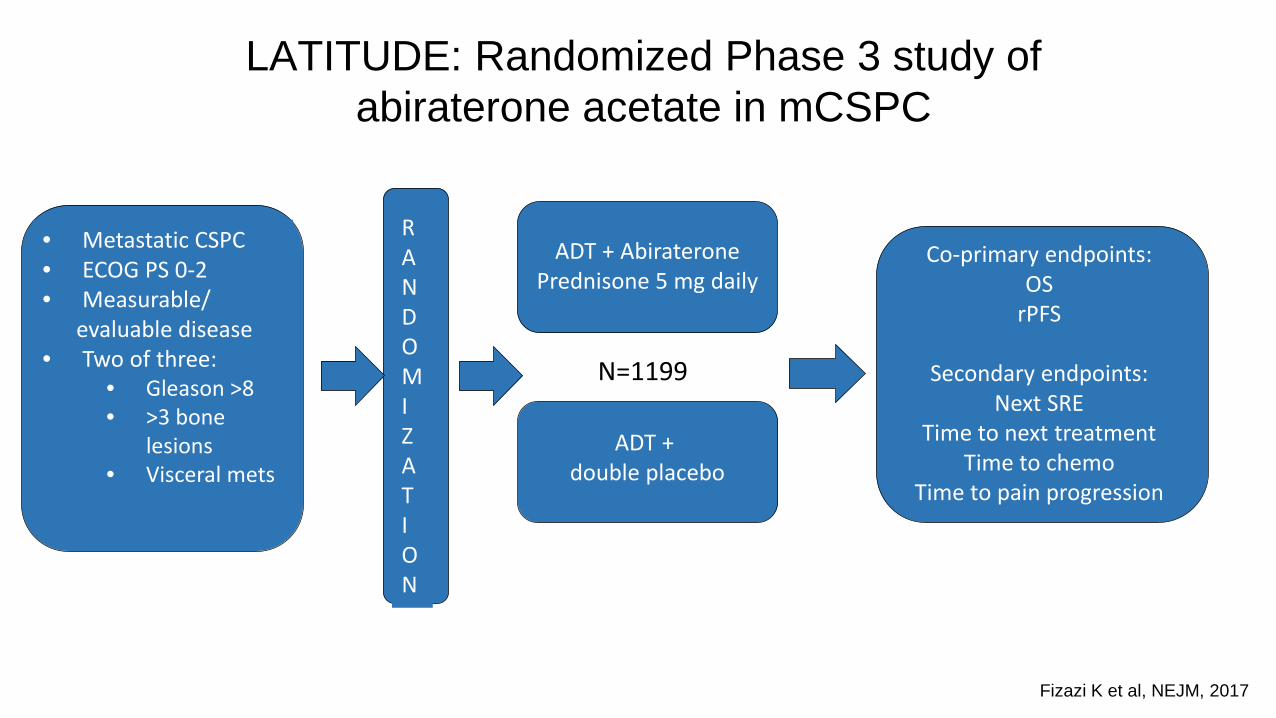
LATITUDE: Randomized Phase 3 study of abiraterone acetate in mCSPC
Fizazi K et al, NEJM, 2017
• Metastatic CSPC • ECOG PS 0-2 • Measurable/ evaluable disease • Two of three:
• Gleason >8 • >3 bone
lesions • Visceral mets
R A N D O M I Z A T I O N
ADT + Abiraterone Prednisone 5 mg daily
Co-primary endpoints: OS
rPFS
Secondary endpoints: Next SRE
Time to next treatment Time to chemo
Time to pain progression
ADT + double placebo
N=1199

LATITUDE: Overall Survival
Fizazi K et al, NEJM, 2017
Median OS NR vs 34.7 months
Median PFS 33 mos vs 14.8 months

LATITUDE: Secondary Endpoints
Fizazi K et al, NEJM, 2017

OS benefit consistently favorable across subgroups
Presented By Karim Fizazi at 2017 ASCO Annual Meeting

Statistically significant improvement in all secondary end points
Presented By Karim Fizazi at 2017 ASCO Annual Meeting

Subsequent life-prolonging therapy for prostate cancer
Presented By Karim Fizazi at 2017 ASCO Annual Meeting

LATITUDE: Adverse Events
Fizazi K et al, NEJM, 2017
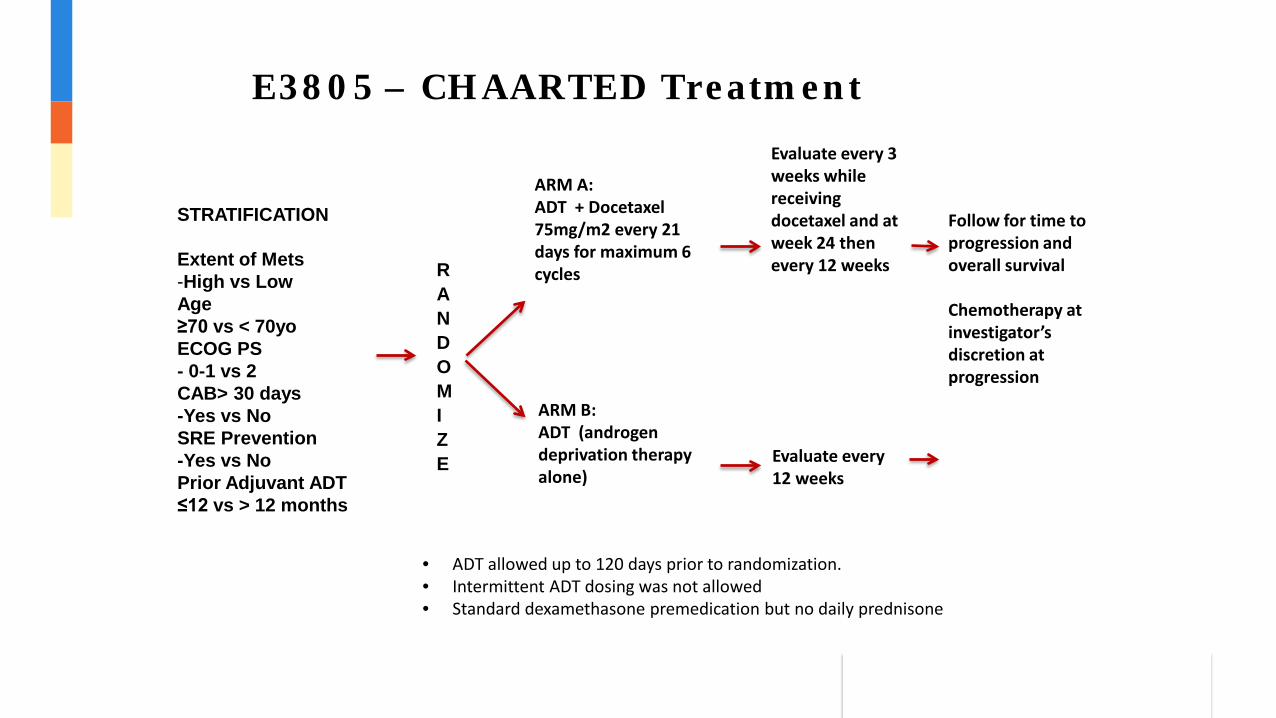
E3805 – CHAARTED Treatment
STRATIFICATION Extent of Mets -High vs Low Age ≥70 vs < 70yo ECOG PS - 0-1 vs 2 CAB> 30 days -Yes vs No SRE Prevention -Yes vs No Prior Adjuvant ADT ≤12 vs > 12 months
RANDOMIZE
ARM A: ADT + Docetaxel 75mg/m2 every 21 days for maximum 6 cycles
ARM B: ADT (androgen deprivation therapy alone)
Evaluate every 3 weeks while receiving docetaxel and at week 24 then every 12 weeks
Evaluate every 12 weeks
Follow for time to progression and overall survival Chemotherapy at investigator’s discretion at progression
• ADT allowed up to 120 days prior to randomization. • Intermittent ADT dosing was not allowed • Standard dexamethasone premedication but no daily prednisone
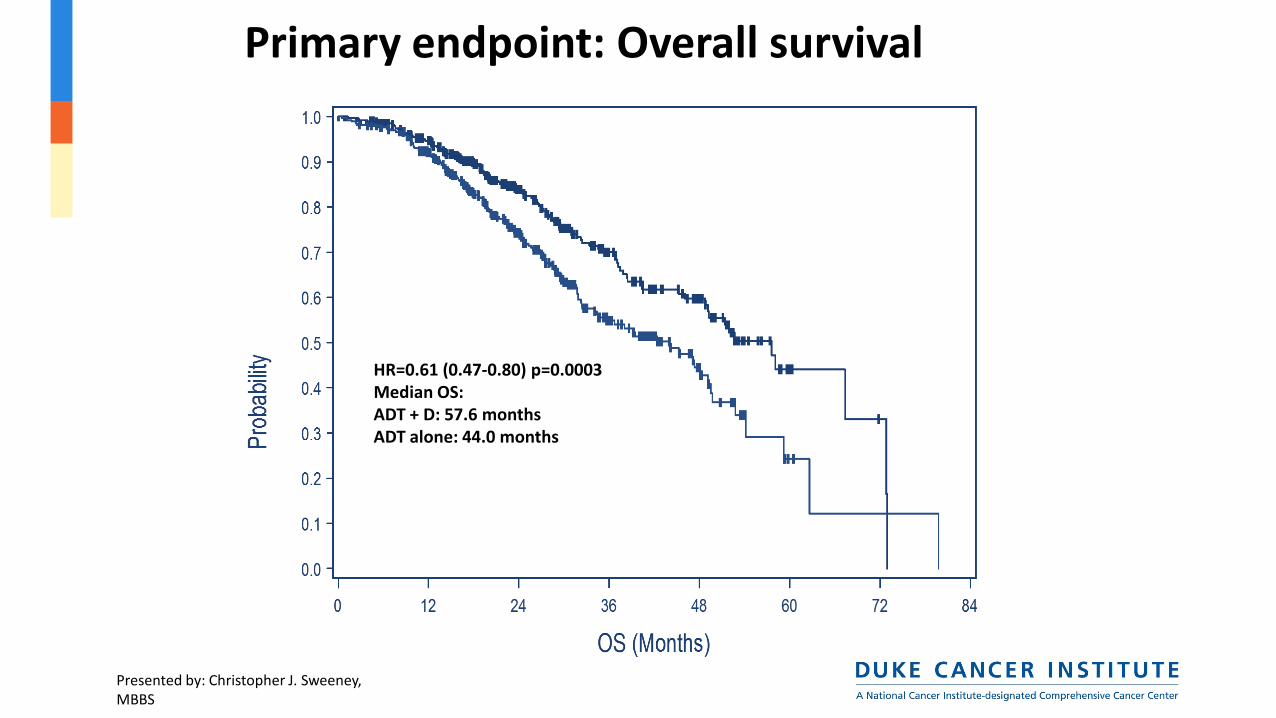
Primary endpoint: Overall survival
HR=0.61 (0.47-0.80) p=0.0003 Median OS: ADT + D: 57.6 months ADT alone: 44.0 months
Presented by: Christopher J. Sweeney, MBBS
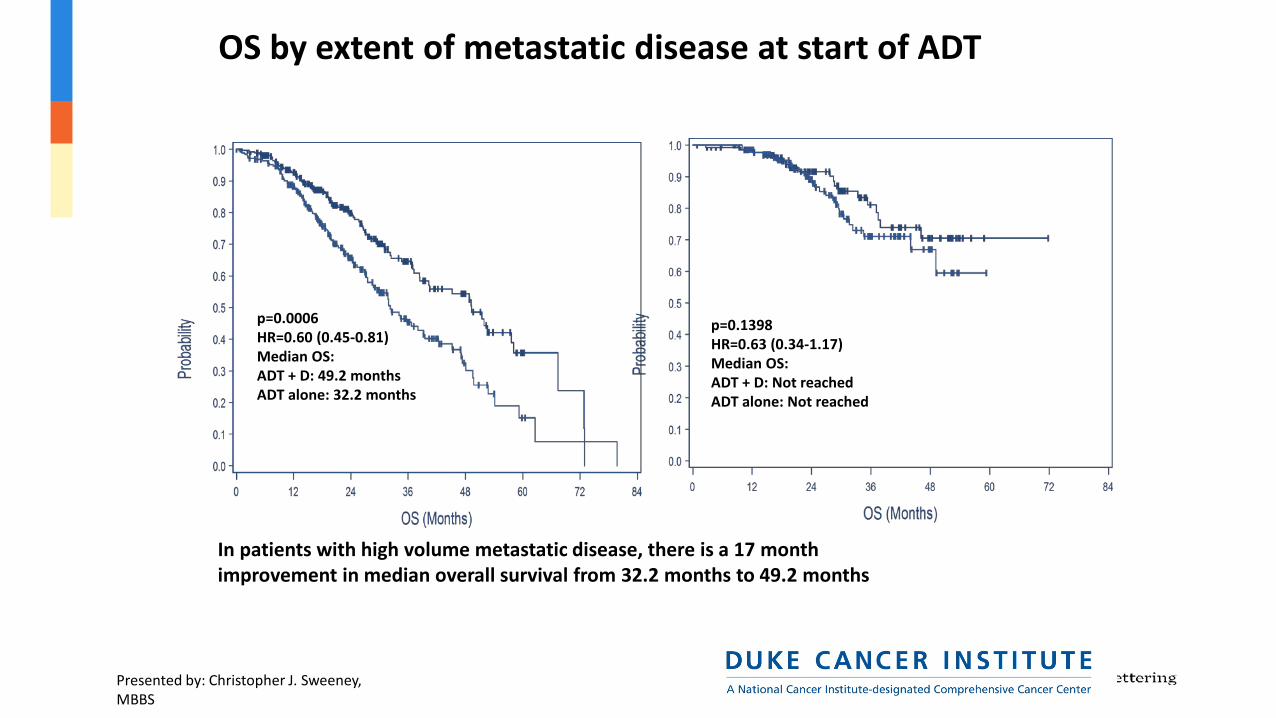
In patients with high volume metastatic disease, there is a 17 month improvement in median overall survival from 32.2 months to 49.2 months
OS by extent of metastatic disease at start of ADT High volume Low volume
p=0.0006 HR=0.60 (0.45-0.81) Median OS: ADT + D: 49.2 months ADT alone: 32.2 months
p=0.1398 HR=0.63 (0.34-1.17) Median OS: ADT + D: Not reached ADT alone: Not reached
Presented by: Christopher J. Sweeney, MBBS

14
Adding abiraterone acetate plus prednisolone (AAP) or docetaxel for patients (pts) with high-risk
prostate cancer (PCa) starting long-term androgen deprivation therapy (ADT):
directly randomised data from STAMPEDE
Matthew Sydes Statistician, Reader in Clinical Trials
MRC Clinical Trials Unit at UCL Institute of Clinical Trials and Methodology UCL, London, UK
Co-authors Malcolm D Mason, Melissa R Spears, Noel W Clarke, David P Dearnaley, Alastair WS Ritchie, J Martin Russell, Clare Gilson, Rob Jones, Johann S de Bono, Silke Gillessen, Robin Millman, Shaun Tolan, John Wagstaff, Simon Chowdhury, Jason Lester, Denise Sheehan, Joanna Gale, Mahesh KB Parmar and Nicholas D James and the STAMPEDE Investigators
Trial registration: NCT00268476

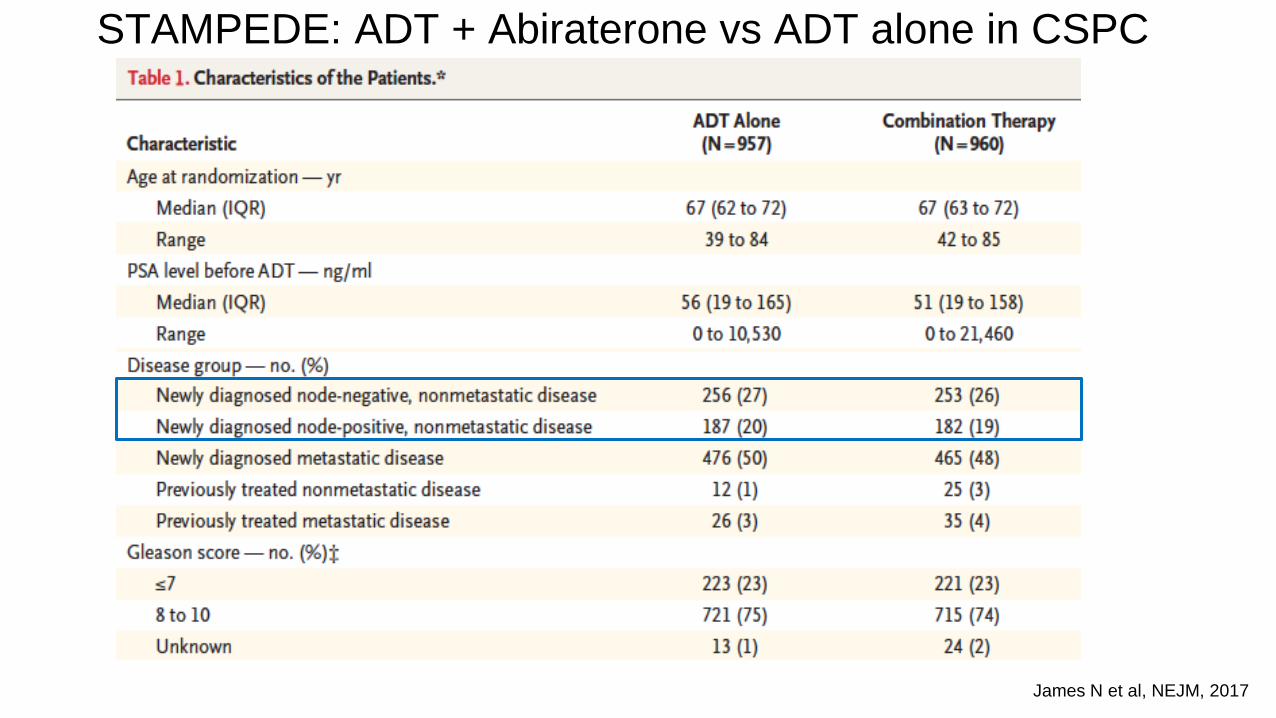
STAMPEDE: Multigroup study of prostate cancer in UK Analysis of ADT+ abiraterone vs ADT alone in CSPC
• WHO PS 0-2 • Histologic evidence of PCa • New diagnosis and
metastatic • OR high risk locally
advanced (2 of 3): • T3/T4 • Gleason 8-10 • PSA>40
• OR high risk relapse: • PSA>4 & PSADT<6
months • PSA>20 • <6 months ADT
R A N D O M I Z A T I O N
ADT + Abiraterone Prednisone
for 2 years or progression
Primary endpoint: OS
Secondary endpoints:
Time to next treatment Time to chemo
Time to pain progression ADT alone
N=1917
James N et al, NEJM, 2017

STAMPEDE: SOC+AAP vs SOC+DocP
ESMO 2017
Recruitment: Nov-2011 to Mar-2013 Reported: ESMO 2017 Published: (paper in development)
Patients: 189 SOC+DocP 377 SOC+AAP 566 patients randomised
contemporaneously to either research arm
Underpowered but the only head-to-head data Last year of recruitment to “abiraterone comparison” overlap with a question of radiotherapy to the prostate in men with M1 disease
Sydes et al ESMO 2017
James N et al, NEJM, 2017
STAMPEDE: ADT + Abiraterone vs ADT alone in CSPC

STAMPEDE – OS (primary endpoint) (n=1,776) • 61% M1; 15% N1M0; 24% N0M0; median follow-up: 43 mo
HR=0.78 (95% CI: 0.66-0.93)
P=0.006
Time from randomization (months)
Ove
rall
surv
ival
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 60 72 84
SOC by Kaplan Meier SOC + DOC by Kaplan Meier SOC by flexible parametric model SOC + DOC by flexible parametric model
SOC Median 71 mo
SOC + DOC Median 81 mo
James, ND et al. Lancet. 2016;387:1163-77.

HR 0.61 (0.49-0.75)
HR 0.75 (0.48 -1.18)
STAMPEDE: ADT+ Abiraterone vs ADT alone in CSPC
James N et al, NEJM, 2017
HR 0.63 95% CI 0.52 to 0.76 P-value 0.00000115
(n=1,917)

HR 0.31 (0.26-0.37)
HR 0.21 (0.15-0.31)
STAMPEDE: ADT+ Abiraterone vs ADT alone in CSPC
James N et al, NEJM, 2017

Failure-free survival [driven by PSA failure]
HR (95%CI) P-val Interactn test
All 0.51 (0.39 to 0.67) <0.001
M0 0.34 (0.16 to 0.69) 0.003 0.17
M1 0.56 (0.42 to 0.75) <0.001
SOC+AAP
SOC+DocP
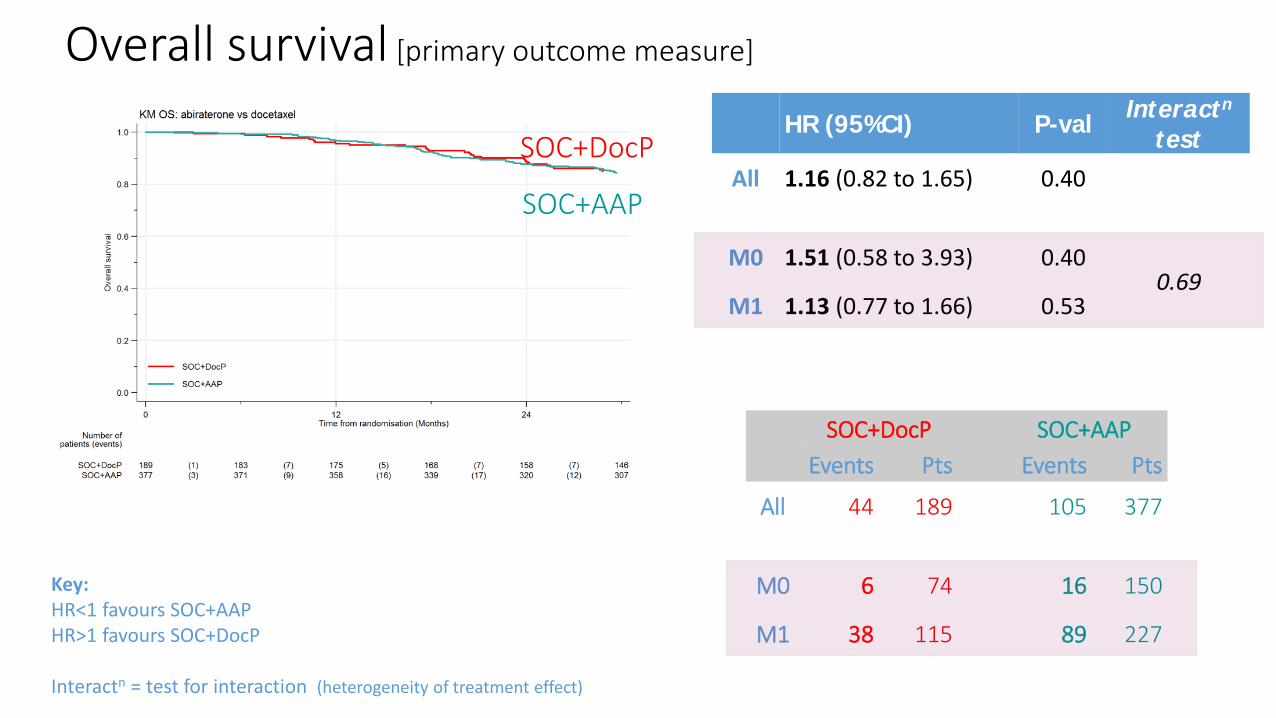
Key: HR<1 favours SOC+AAP HR>1 favours SOC+DocP Interactn = test for interaction (heterogeneity of treatment effect)
SOC+DocP SOC+AAP Events Pts Events Pts
All 97 189 122 377
M0 18 74 13 150
M1 79 115 109 227
HR (95%CI) P-val Interactn test
All 1.16 (0.82 to 1.65) 0.40
M0 1.51 (0.58 to 3.93) 0.40 0.69
M1 1.13 (0.77 to 1.66) 0.53
Key: HR<1 favours SOC+AAP HR>1 favours SOC+DocP Interactn = test for interaction (heterogeneity of treatment effect)
SOC+DocP SOC+AAP Events Pts Events Pts
All 44 189 105 377
M0 6 74 16 150
M1 38 115 89 227
SOC+AAP
SOC+DocP
Overall survival [primary outcome measure]

AA Failure free survival in M0 subgroup
status
Mets
Overall
M1
M0
FFS/N
SOC-only
393/502
142/455
FFS/N
SOC+AAP
210/500
38/460
(95% CI)
Haz. Ratio
0.29 (0.25, 0.34)
0.31 (0.26, 0.37)
0.21 (0.15, 0.31)
Favours: abiraterone SOC-only
.2 .4 .6 .8 1 1.2 1.4
SOC vs SOC+AAP
No difference in M0N0 for: OS MFS Based on n=530 underpowered subsets for N0 M0 and n=384 subset for N+M0
Is radiotherapy planned?
RT plannedNo RT planned
110/396425/561
24/396224/564 0.023
0.18 (0.12, 0.28)0.31 (0.26, 0.36)
Overall
0.29 (0.25, 0.34)
Favours: abiraterone SOC-only
.2 .4 .6 .8 1 1.2 1.4
James N et al LBA34 ESMO 2017

Safety population SOC+DocP SOC+AAP Patients included in adverse event analysis 172 (91%) 373 (>99%)
Grade 1+ AE 172 (100%) 370 (99%) Grade 3+ AE 86 (50%) 180 (48%)
Grade 3+ AEs by category (incl. expected AEs) Endocrine disorder (incl. hot flashes, impotence) 15 (9%) 49 (13%) Febrile neutropenia 29 (17%) 3 (1%) Neutropenia 22 (13%) 4 (1%) Musculoskeletal disorder: 9 (5%) 33 (9%) Cardiovascular disorder (incl. hypertension, MI, cardiac dysrhythmia): 6 (3%) 32 (9%) Gastrointestinal disorder: 9 (5%) 28 (8%) Hepatic disorder (incl. increased AST, increased ALT): 1 (1%) 32 (9%) General disorder (incl. fatigue, oedema): 18 (10%) 21 (6%) Respiratory disorder (incl. breathlessness): 12 (7%) 11 (3%) Renal disorder 5 (3%) 20 (5%) Lab abnormalities (incl. hypokalaemia): 9 (5%) 11 (3%)
Adverse events

Phase 3 Ongoing Combination Therapy Trials in HSPC
25
Study Identifier Study Drugs Pts (N) Primary End Point
Status/Read Out
LATITUDE NCT01715285 ADT ± AA 1209 rPFS, OS ASCO 2017
STAMPEDE (Arm G) NCT00268476 ADT ± AA 1800 OS LBA ASCO 2017
PEACE-1 NCT01957436 ADT ± DOC vs
ADT + AA ± DOC (± local RT)
916 PFS, OS Recruiting/2020
STAMPEDE (Arm J) NCT00268476 ADT ± AA + ENZ* 1800 OS Closed-will report in 2-
3 yrs
SWOG-1216 NCT01809691 ADT + TAK-700 vs
ADT + BIC 1304 OS Recruiting/2027
ENZAMET NCT02446405 ADT + ENZ vs ADT + antiandrogen 1100 OS Recruiting/2020
TITAN NCT02489318 ADT ± APA (ARN 509) 1000 rPFS, OS Recruiting/ 2021
ARCHES NCT02677896 ADT (+docetaxel in selected cases) ± ENZ* 1100 rPFS Recruiting/ 2021
ARASENS NCT02799602 ADT + DOC ± ODM-201 1300 OS Recruiting/2022
*Includes upfront Doc Modified from and courtesy of K. Fizazi

Summary
• ADT alone is suboptimal for mHSPC • Abiraterone is preferred in most patients because of tolerance and
lower SAE rates of fever/neutropenia. Docetaxel may be preferable for cost and shorter course of treatment.
• Remaining questions under study: • Is combination of AAP and Docetaxel better? • Is there a role for consolidative primary treatment? • Is there a role for SBRT in oligometastatic patients?