dvt prophylaxis in surgical patients - mc.vanderbilt.edu€¢ rogers and caprini score can be used...
TRANSCRIPT

Thromboprophylaxis in Surgical Patients
M. J. Osgood Summer School 2012

Background
• The problem: DVT and its sequelae • DVT: sequelae
– Pulmonary embolism (PE) – Post-thrombotic syndrome (PTS) – Pulmonary hypertension (PH)
• DVT, PE, and PTS are the most common preventable causes of in-hospital death
• DVT has 19% incidence in general surgery patients

Risk Factors for Venous Thromboembolism (VTE)
• Surgical patients uniformly manifest the Virchow Triad – Stasis (i.e. immobilization) – Endothelial injury (i.e. trauma, central venous
catheter placement) – Hypercoagulability (i.e. TF release, increased PAI-
1)

Additional VTE Risk Factors • Increased age • Malignancy • Immobilization • Trauma (esp. spinal cord injury) • Oral contraceptive use • Hormone replacement therapy • Pregnancy, esp. in puerperium • Neurologic disease (esp. extremity paralysis) • Inflammatory bowel disease, esp. active disease • Central venous catheter, transvenous pacemaker • May-Thurner syndrome • Paget-Schroetter syndrome • Cardiac dysfunction (maybe) • Obesity (maybe)
Hypercoagulable States • Antiphospholipid, anticardiolipin antibodies • Antithrombin III deficiency • Protein C/S deficiency • Factor V Leiden • Prothrombin gene 20210A mutation • Blood group non-O • Dysfibrinogenemia • Dysplasminogenemia • Hyperhomocystinemia • Reduced heparin cofactor II activity • Elevated levels of clotting factors (XI, IX, VII, VIII, X, II) • Elevated levels of PAI-1

Hypercoagulable States • Antiphospholipid antibodies • Antithrombin III deficiency • Protein C/S deficiency • Factor V Leiden = most common inherited thrombophilia • Prothrombin gene 20210A mutation • Blood group non-O • Dysfibrinogenemia • Dysplasminogenemia • Hyperhomocystinemia • Reduced heparin cofactor II activity • Elevated levels of clotting factors (XI, IX, VII, VIII, X, II) • Elevated levels of PAI-1
Hematologic syndromes conferring risk for VTE
• HIT • DIC • Antiphospholipid antibody syndrome • TTP • HUS • Myeloproliferative disorders

Diagnosis of DVT
• Physical exam – Pain, edema, erythema, tenderness, fever,
prominent superficial veins, Homan’s sign • Imaging
– Duplex ultrasound >> MRV, CTV >> Conventional venography
– Duplex: B-mode + spectral doppler venous incompressibility, flow abnormalities
– Duplex ultrasound is not useful for diagnosis of DVT proximal to inguinal ligament

Femoral vein DVT

Femoral vein confluence without DVT

Subclavian Vein Occlusion on Venogram

Right innominate vein occlusion on MRV


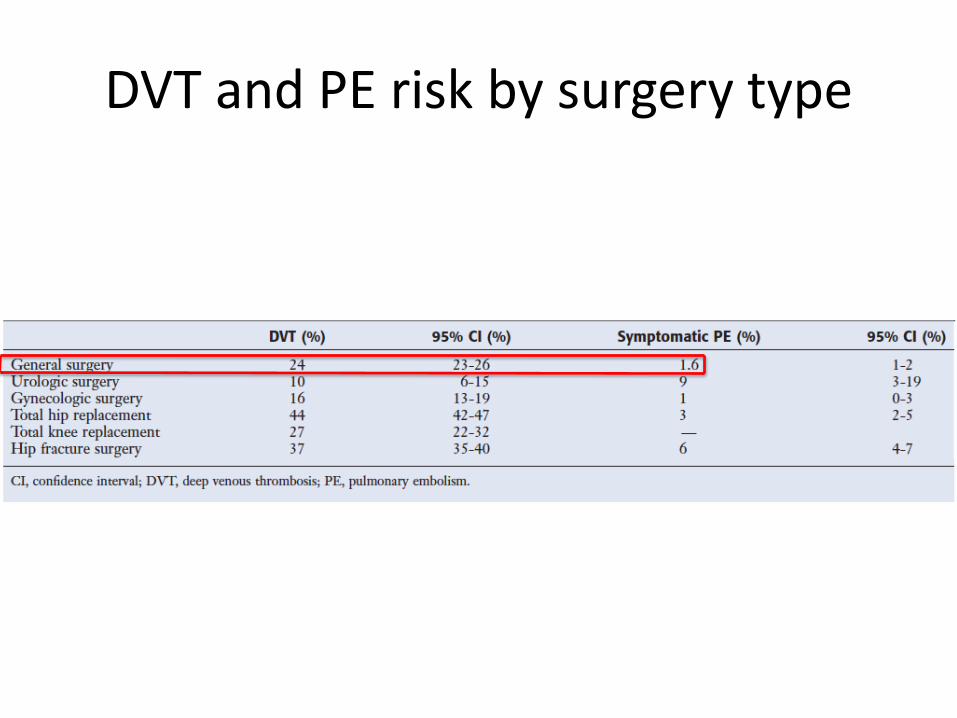
DVT and PE risk by surgery type

DVT Prophylaxis
• Goals: – Prevention of venous thromboembolism (VTE) and
sequelae – Prevention of postthrombotic syndrome (PTS) – Prevention of pulmonary embolism (PE)
• Forms of DVT prophylaxis: – Pharmacologic (UFH, LMWH, ASA, warfarin,
danaparoid, fondaparinux) – Mechanical (Intermittent pneumatic compression,
graduated compression stockings, venous foot pump)
Evidence: anticoagulant thromboprophylaxis in general surgery
• Unfractionated heparin (UFH) reduces risk of fatal PE by 66%
• Low-molecular weight heparin (LMWH) reduces risk of symptomatic venous thromboembolism by 80% in patients undergoing abdominal surgery
• Prophylactic anticoagulants reduce the risk of silent DVT by 30-70%
Evidence: mechanical thromboprophylaxis
• Compared with anticoagulants and ASA, mechanical methods of thromboprophylaxis have the advantage of not increasing bleeding
• These agents are effective in reducing thrombosis compared with no prophylaxis
• However, there is no compelling data establishing the efficacy of these agents in prevention of fatal PE
• Use is indicated in low-risk surgical patients
Thromboprophylaxis in general surgery
• Risk for VTE can be predicted using validated evidence-based scoring systems
• Rogers and Caprini score can be used to estimate VTE risk
• Decision regarding method of VTE prophylaxis needs to weigh bleeding risk versus risk of VTE
• Bleeding risk is very low for general surgery patients receiving most forms of pharmacologic thromboprophylaxis (<5%)

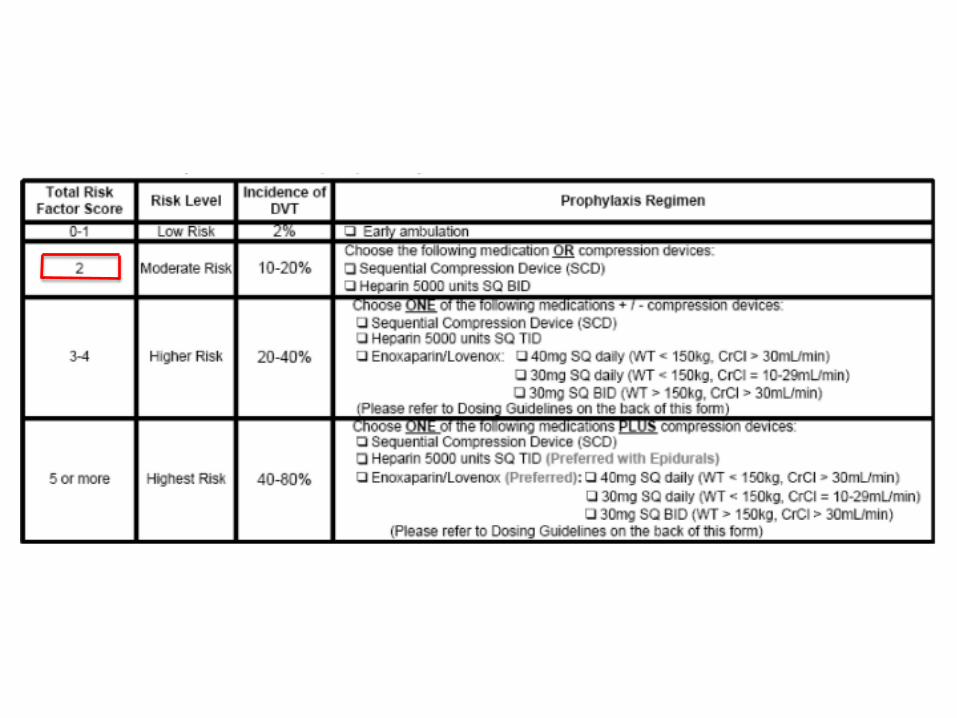
Caprini Score Model
DVT PROPHYLAXIS
QUIZ!!!!!
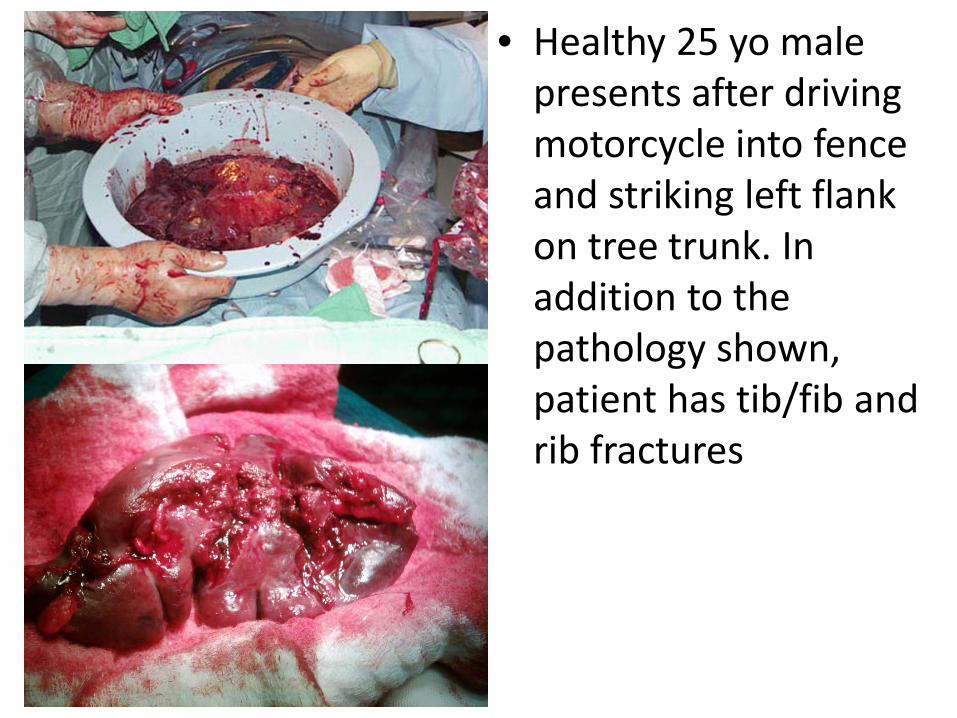
• Healthy 25 yo male presents after driving motorcycle into fence and striking left flank on tree trunk. In addition to the pathology shown, patient has tib/fib and rib fractures
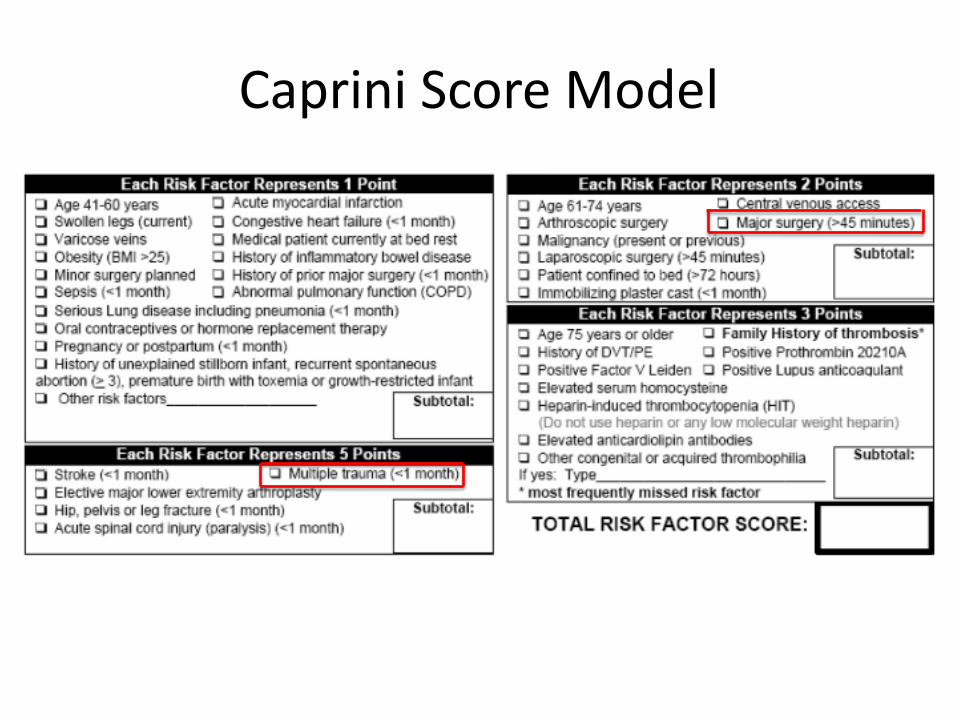
Caprini Score Model


• 45 yo F with elevated serum calcium, elevated PTH, and imaging study shown to the left

Caprini Score Model

• 38 yo F with DM type II, metabolic syndrome, and morbid obesity has failed conventional weight loss programs

Caprini Score Model

Pharmacologic Thromboprophylaxis: Considerations
• LMWH – More expensive – Longer half life, less
frequent dosing – Contraindicated in
renal failure – Lower risk of HIT
• UFH – Less expensive – Shorter half life – Can use in renal failure – Greater safety in pts
with epidural catheters – Higher risk of HIT
LMWH and UFH have similar efficacy in thromboprophylaxis in general surgery patients

Administration of pharmacologic thromboprophylaxis
• UFH – Initiate 1-2 hours prior to induction of general
anesthesia – TID dosing superior to BID dosing
• If pharmacologic thromboprophylaxis is indicated, continue until hospital discharge or at least 7 days postoperatively
• Certain populations require extended thromboprophylaxis for 4 weeks (i.e. major cancer surgery, SCI, history of VTE) (Grade 1B)
DVT: Treatment
• Immediate systemic anticoagulation = standard therapy – Therapeutic anticoagulation with UFH infusion or
LMWH (1 mg/kg BID) – VKA (i.e. warfarin)
• Delay in initiation of therapeutic anticoagulation >24 hrs is associated with increased rate of VTE
DVT: duration of treatment?
• 30% of patients develop recurrent DVT within 10 years of initial DVT
• Risk factors for recurrent DVT: – Older age – Obesity – Malignant neoplasm – Extremity paresis
IVC Filter Placement: Indications
• Complication of anticoagulation • Contraindication to anticoagulation (i.e.
excessive bleeding risk) • Failure of anticoagulation • Free-floating thrombus > 5 cm • High risk of PE

New trends in DVT management
• Recently there has been increased recognition of increased incidence of PTS with anticoagulation alone
• Early thrombus removal strategies have been advocated – Good functional capacity, ambulatory patients
with first episode of ileofemoral DVT <14 days and low bleeding risk (Grade 2C)
– Limb-threatening ischemia (phlegmasia cerulea dolens) (Grade 1A)