dysfunctional uterine bleeding ding ding m.d., ph.d. department of obstetrics & gynecology...
TRANSCRIPT
Dysfunctional Uterine Bleeding
Ding Ding M.D., Ph.D. Department of Obstetrics & Gynecology
Ob/Gyn Hospital
Fudan Unoversity
IntroductionDUB is defined as ABNORMAL uterine bleeding absence of demonstrable structural or organic pathology. It is usually with hormonal disturbances due to hypothalamic-pituitary-ovarian axis (HPOA) dysregulation.
Diagnosis must be made by exclusion.DUB occurs most often shortly after menarche and at the end of the reproductive years.
•20% of cases are adolescents•50% of cases in perimenopausal years
Introduction
Heavy menses, prolonged menses, or
frequent irregular bleeding are the most common complaints.
Up to 20% of women will experience irregular cycles in their lifetimes.
Normal Menstrual Cycle Follicular phase
14 days (varies)• Dominant follicle develop with greatest number of
granulosa cells and FSH receptors Ovulation
• 30-36 hours after LH surge Luteal phase
• LH surge to menses• Persists 14 days (constant)
Menses
Involution of corpus luteum
Decrease progesterone and estrogen
20-60 cc of dark blood containing endometrial tissue
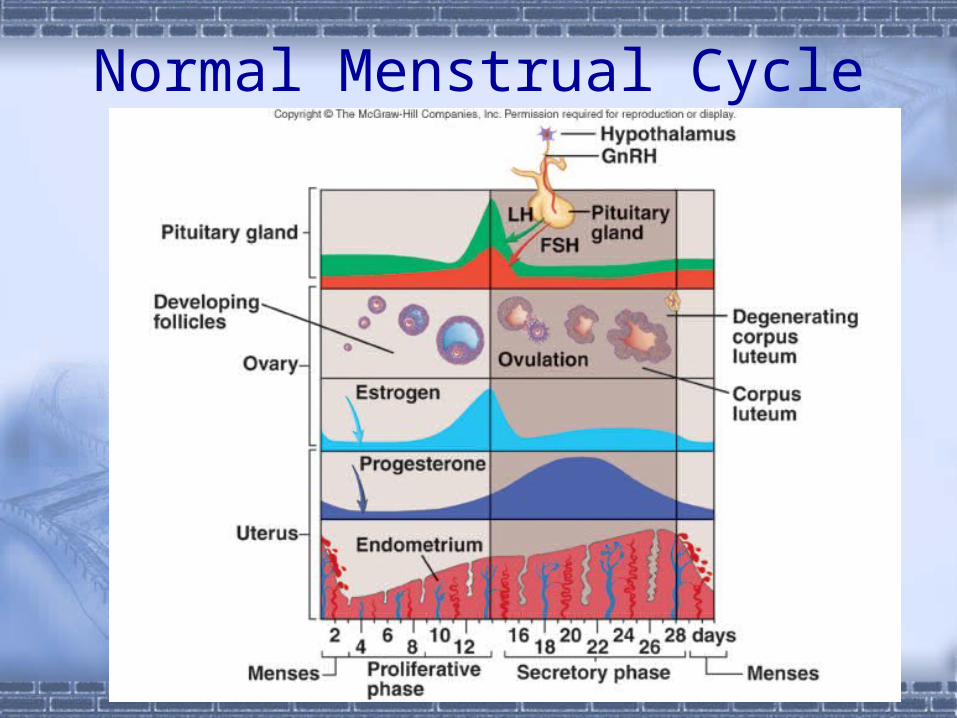
Normal Menstrual Cycle
Pathophysiology Two types: anovulatory and ovulatory
Most women with DUB do not ovulate (70-80%).• In theses women, there is continuous E2 production
without corpus luteum formation and progesterone production.
• Adolescent: 20%• Perimenopausal years: 50%
Ovulatory DUB occurs most commonly at the reproductive age.• 20-30% of DUB• Incidence in these patients may be as high as 10%
Anovulatory DUBEtiology
Psychological stress Body weight (obesity, anorexia, or a rapid change) Endocrine: In perimenopausal women, the mean length of the cycle is
shorter compared to younger women. Shortened follicular phase
Diminished capacity of follicles to secrete Estradiol Neoplasm, Drugs It may be otherwise idiopathic.

Endometrial Hyperplasia
Chronic anovulatory, persistently elevated estrogen levels, uninterrupted by progesterone
Proliferative Disorder: earliest pathology Simple Hyperplasia: 1% will develop EM cancer
Complex Hyperplasia: 3%
Atypical Hyperplasia: precarcinoma
15% will develop EM cancer
In fact, 17-51% cases are associated with EM cancer
Ovulatory DUB
Luteal phase insufficiency• Shortened menstrual interval(24-26d)• Not easy to conceive baby• Recurrent first-trimester abortionIrregular shedding of endometrium• Prolonged involution of corpus luteum• 5-6th day during menses of the
menstrual cycle, the secretory phase endometrium was still seen
Differential Diagnosis Organic • Reproductive tract cancer• Endometrial cancer• Cervical cancer • Less frequently:
vaginal, vulvar, fallopian tube cancers estrogen secreting ovarian tumors
• granulosa-theca cell tumors
• Systemic Disease: Coagulation disorders, liver • Ectopic pregnancy, abortion or trophoblastic disease• Pelvic infections
“You must exclude all organic causes first!”
Evaluation History
• Onset, frequency, duration, cyclic vs.acyclic, severity• Pain, change from menstrual pattern (calendar)• Age, parity, marital status, sexual hx, contraception• medications, pregnancies• symptoms of pregnancy and reproductive tract
disease
Physical Exam• pelvic exam• pap smear
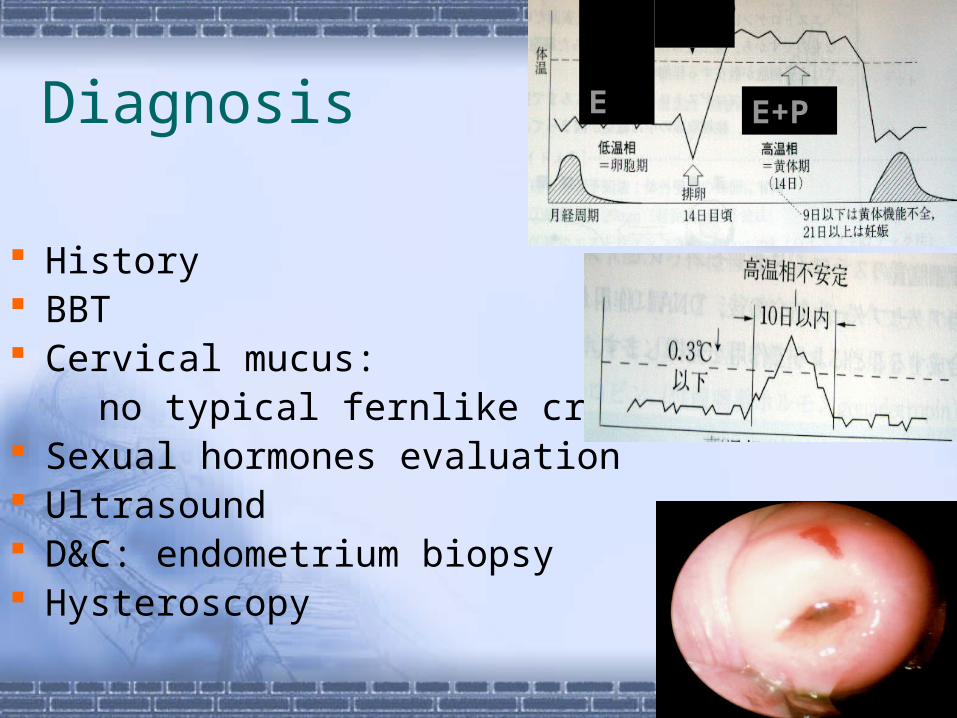
Diagnosis
History BBT Cervical mucus: no typical fernlike crystal Sexual hormones evaluation Ultrasound D&C: endometrium biopsy Hysteroscopy
E
E+P
Treatment Goals of DUB
Adolescent• Control bleeding• Regulate menstrual cycle• Induce ovulationReproductive age• Stimulate follicle development• Promote corpus luteum function• Induce ovulationPerimenopausal• Control bleeding, reduce volume• Regulate menstrual cycle• Prevent endometrial cancer
Treatment of DUB
Medical management before Surgical• effective methods include:
estrogens, progestins, or both antifibrinolytic agents danazol GnRH agonists
Treatment of DUB Acute bleeding
• Estrogen therapy High dose estrogens: adolescent Oral conjugated estrogens
• 10mg a day in four divided doses• treat for 21 to 25 days• medroxyprogesterone acetate, 10 mg per day for the
last 7 days of the treatment• if bleeding not controlled, consider organic cause
OR• 25 mg IV every 4 to 12 hours for 24 hours, then
switch to oral treatment as above.
• Bleeding usually diminishes within 24 hours
Treatment of DUB Recurrent bleeding episodes
• Sequential therapy: Estrodial+Progesterone
estrodial 1.25mg/d*21d , last 10d add MPA 10mg/d
• combination OCP’s one tablet per day for 21 days
• intermittent progesterone therapy medroxyprogesterone acetate, 10mg per day, for the first
10 days of each month higher doses and longer therapy my be tried if no initial
response prolonged use of high doses is associated with fatigue,
mood swings, weight gain, lipid changes
Treatment of DUB Recurrent bleeding episodes
(continued)• Progesterone releasing IUD (Mirena)
avoids side effects must be reinserted annually Levonorgestrel IUD
• 80% reduction of blood loss at 3 months
• 100% reduction at 1 year
• found to be superior to antifibrinolytic agents and prostaglandin synthetase inhibitors
Treatment of DUB Immature hypothalamic-pituitary axis
• progestin therapy by itself for 10 days every month or every other month until full maturity of the axis provides effective therapy.
Older perimenopausal women• cyclic progestin therapy
prevents development of endometrial hyperplasia
• low dose OCP’s healthy non-smokers, free of vascular disease
Treatment of DUB Other options
• inhibitors of fibrinolysis EACA (epsilon-aminocaproic acid) AMCA (tranexamic acid) PABA (para-aminomethybenzoic acid)
• use limited by side effects nausea, dizziness diarrhea, headaches abdominal pain allergic manifestations
Treatment of DUB
Danazol: perimenopausal women• androgenic steroid
200mg and 400 mg daily doses for 12 weeks studied
200mg dose as effective as 400 mg androgenic side effects: weight gain, acne
• side effects minimized with 200mg dose
100 mg not effective, expensive
Treatment of DUB
GnRH agonists• treatment results in medical menopause• blood loss returns to pretreatment levels when
discontinued• treatment usually reserved for women with
ovulatory DUB that fail other medical therapy and desire future fertility
• 3 months later, use add back therapy to prevent bone loss secondary to marked hypoestrogenism
Treatment of DUB
Surgical Treatment• Dilation and Curettage
quickest way to stop bleeding in patients who are hypovolemic
appropriate in older women (>35)to exclude malignancy but is inferior to hysteroscopy
follow with medroxyprogesterone acetate or OCP’s to prevent recurrence
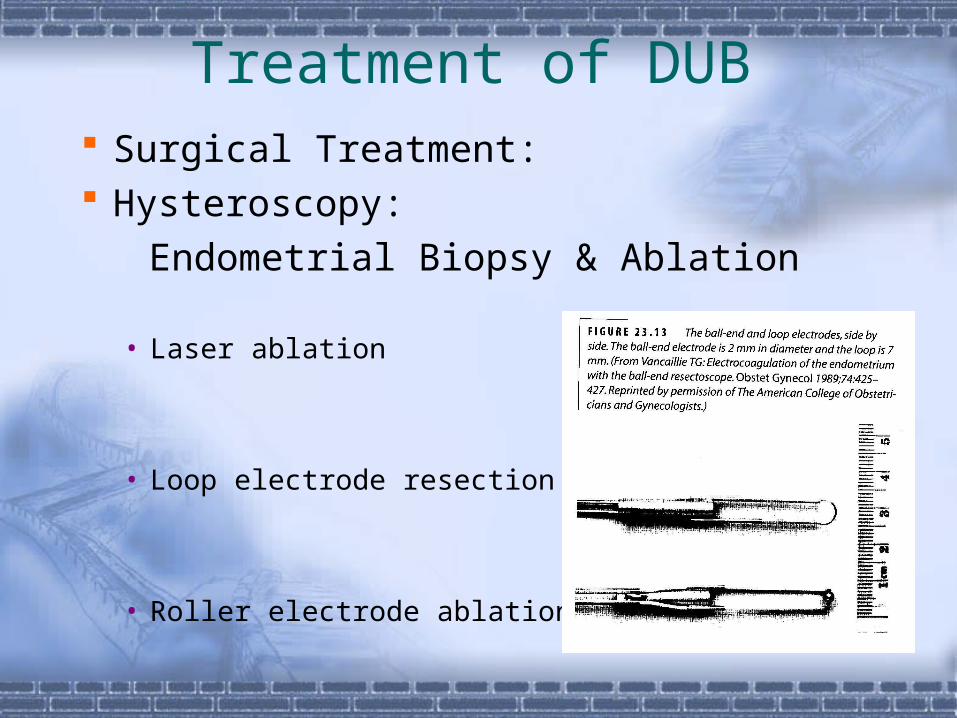
Treatment of DUB Surgical Treatment: Hysteroscopy:
Endometrial Biopsy & Ablation
• Laser ablation
• Loop electrode resection
• Roller electrode ablation
Treatment of DUB
Surgical Treatment• Hysterectomy• Indication:
elder and no demands on bearing babies
atypical hyperplasia or EM cancer
Case presentation1
15 y.o. girl menarche 13 y.o. Heavy bleeding for 10 days Hb 105g/L, WBC & plt normal
Following examination?
Diagnosis?
Management?
Case presentation2
50 y.o. woman, 1-0-1-1 Heavy bleeding for 8 days Urine HCG(-) Ultrasound: endometrium 12mm, ovaries(-) TCT: normal (two months ago)
Following examination?
Diagnosis?
Management?