eae-clinical significance of valvulo-arterial …...impact of hypertension on the timing of symptom...
TRANSCRIPT

Clinical Significance of Valvulo-Arterial
Impedance in Aortic Valve Stenosis
Dr. Julien Magne, PhD
Sart Tilman Liège, BELGIUM

Conflict of Interest Disclosure
None

Valvulo-Arterial Impedance (Zva): Definition
Mechanical Impedance: a measure of how much a structure resists
motion when subjected to a given force.
In Aortic stenosis: Zva represents the cost in mmHg for each
systemic mL of blood indexed for body size pumped by the left
ventricle during systole.
Zva provides an estimate of the global LV hemodynamic load that
results from the summation of the valvular and vascular loads:
• stenosis severity
• volume flow rate
• body size
• systemic vascular resistance
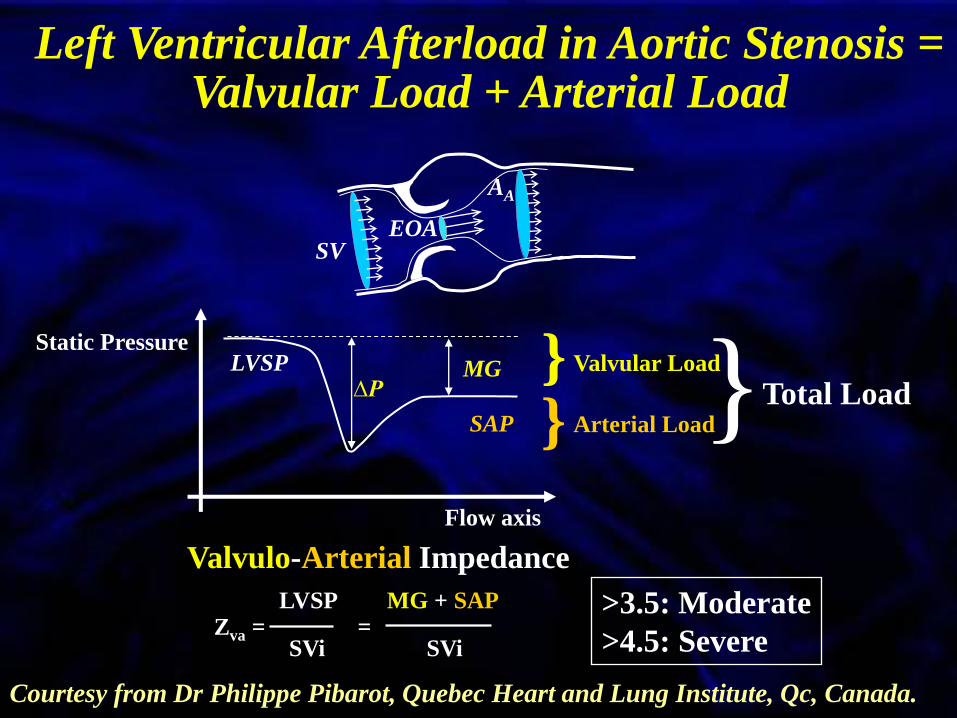
Static Pressure LVSP
SAP
∆P
MG
AA
Flow axis
Valvular Load
Arterial Load
EOA SV
} }
Valvulo-Arterial Impedance
Zva = = LVSP MG + SAP
SVi SVi
Left Ventricular Afterload in Aortic Stenosis = Valvular Load + Arterial Load
Courtesy from Dr Philippe Pibarot, Quebec Heart and Lung Institute, Qc, Canada.
} Total Load
>3.5: Moderate
>4.5: Severe

Impact of Hypertension on AS Severity
Little et al. Heart, 93:848-55. 2007 Mascherbauer et al.; Eur Heart J; 2008

Impact of Hypertension on the Timing of Symptom Onset in AS
193 patients with symptomatic AS
32% had concomitant HTN
Symptoms of AS develop
at lower degree of stenosis severity
in hypertensive patients, probably
because of the additional overload
due to hypertension.
0,6
0,65
0,7
0,75
0,8
0,85
0,9
AVA (cm2) at symptom onset
Antonini-Canterin et al.; Hypertension. 2003;41:1268-1272.
p=0.02
No
HTN
HTN

Zva
(m
mH
g.m
L-1
.m-2
)
2
3
4
5
6
7
Group 0 Group A Group ABGroup B
*†‡
**
Groups I II III IV (n=208) Moderate AS
Normal SAC
Moderate AS
Low SAC
Severe AS
Normal SAC
Severe AS
Low SAC
(n=77, 37%) (n=50, 24%) (n=45, 22%) (n=36, 17%)
Valvulo-Arterial Impedance (Global LV Afterload)
SAC= PP
SVi
Low SAC: 0.6
ZVA= SAP+MG
SVi
Briand, JACC, 46:291-296,2005
AS and Reduced Systemic Arterial Compliance: Impact on LV Afterload

Moderate AS Severe AS
AS and Reduced Systemic Arterial Compliance:
Impact on LV Function
Norm
SAC
Low
SAC
Norm
SAC
Low
SAC
Briand, JACC, 46:291-296,2005
LV Diast. dysfunction
Zva≥4.5
OR=5.4, p<0.0001
LV Syst. dysfunction
Zva≥4.5
OR=4.2, p=0.001
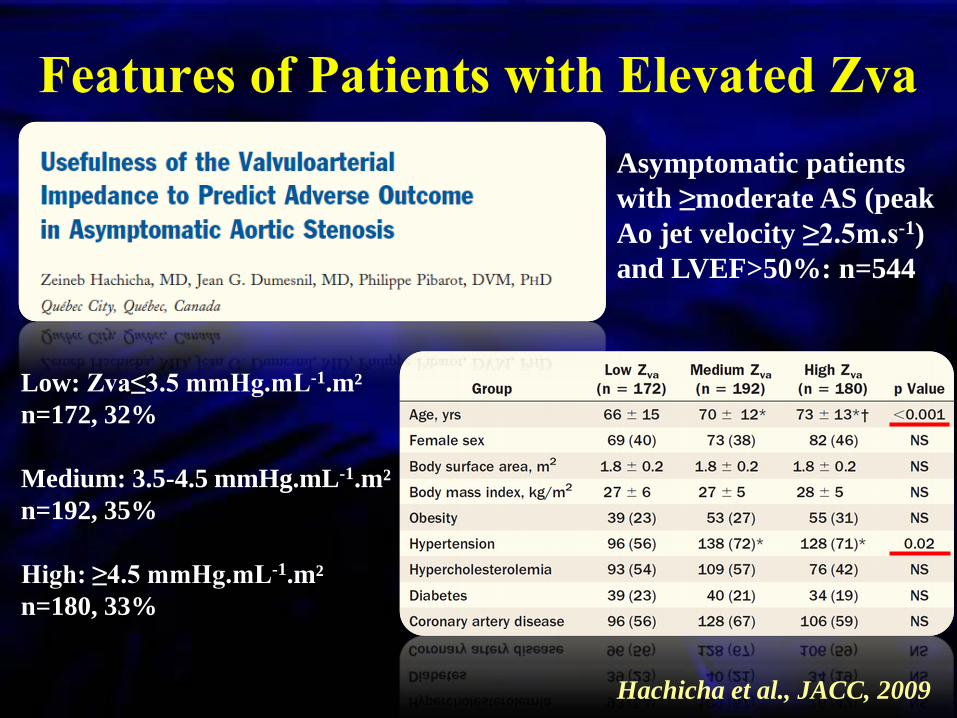
Features of Patients with Elevated Zva
Hachicha et al., JACC, 2009
Asymptomatic patients
with ≥moderate AS (peak
Ao jet velocity ≥2.5m.s-1)
and LVEF>50%: n=544
Low: Zva≤3.5 mmHg.mL-1.m²
n=172, 32%
Medium: 3.5-4.5 mmHg.mL-1.m²
n=192, 35%
High: ≥4.5 mmHg.mL-1.m²
n=180, 33%
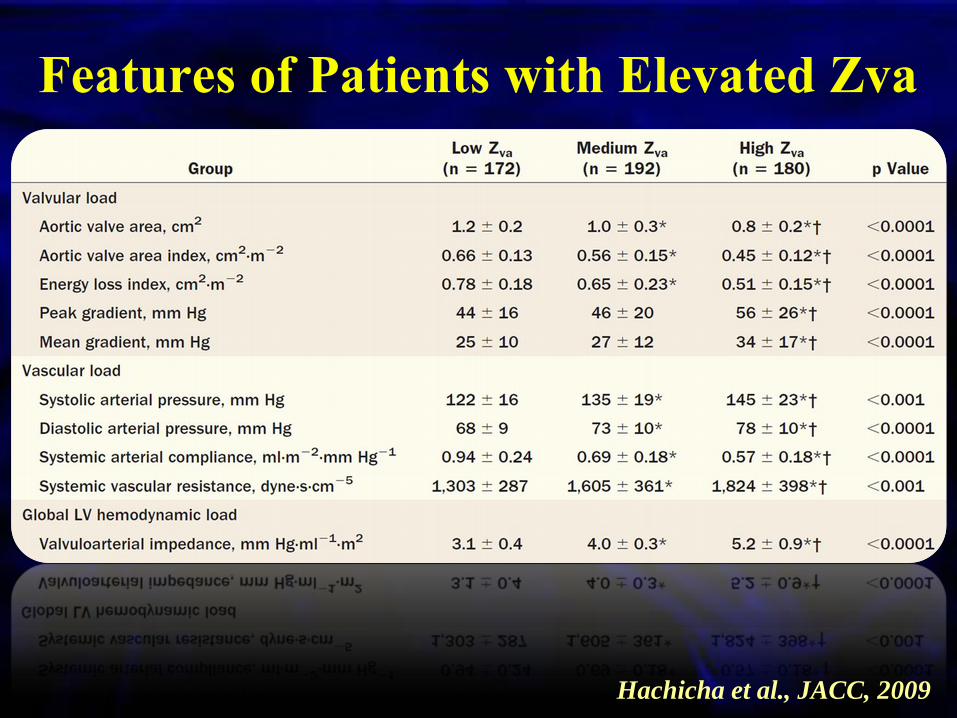
Features of Patients with Elevated Zva
Hachicha et al., JACC, 2009
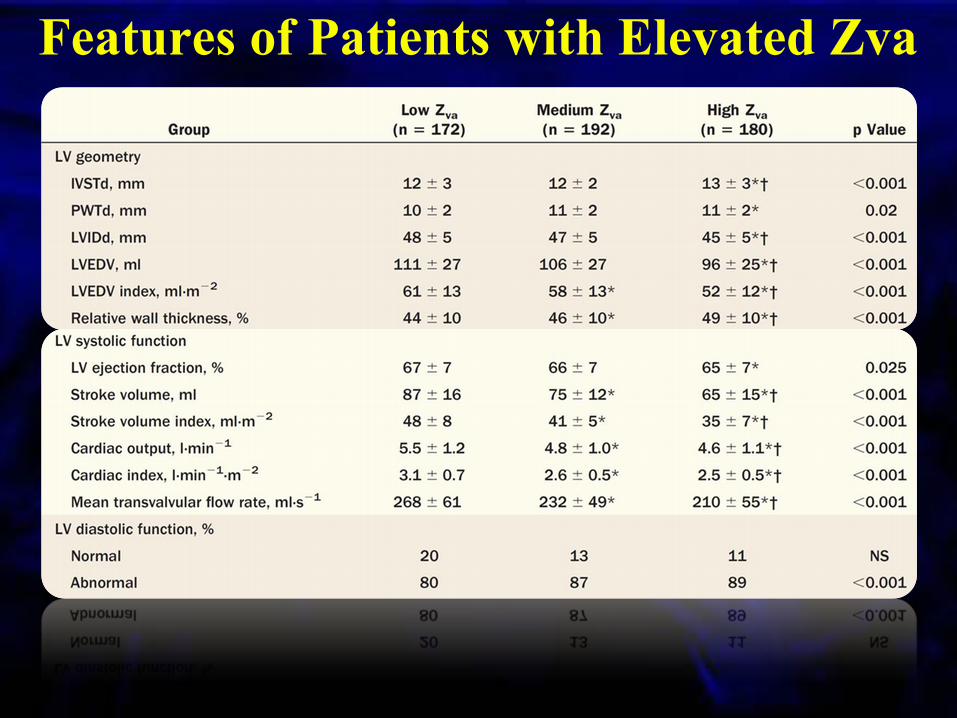
Features of Patients with Elevated Zva
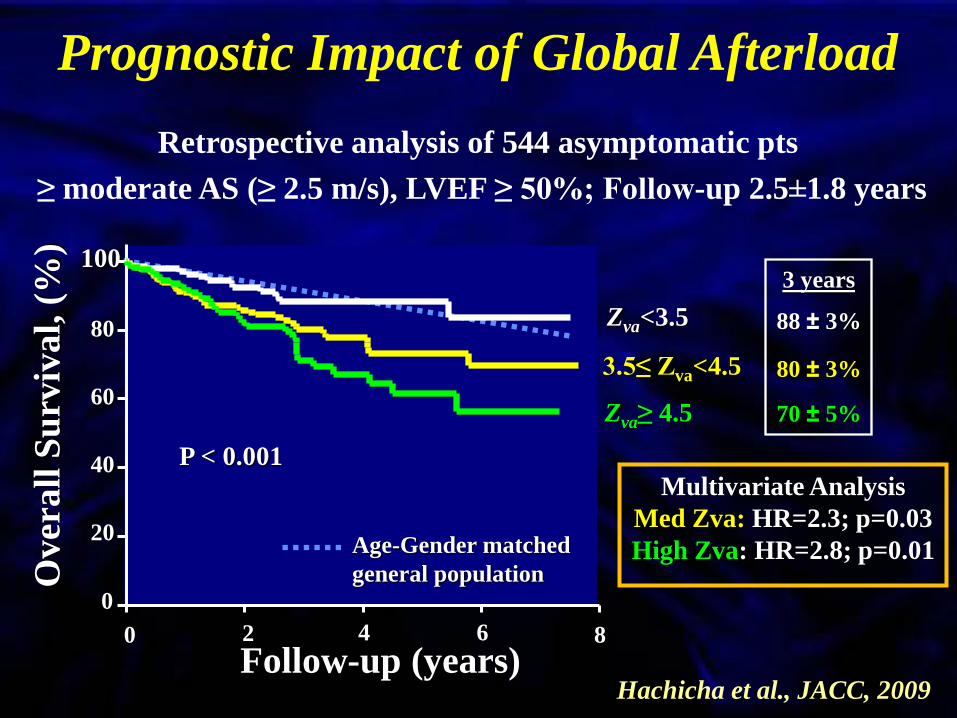
Retrospective analysis of 544 asymptomatic pts
≥ moderate AS (≥ 2.5 m/s), LVEF ≥ 50%; Follow-up 2.5±1.8 years
Prognostic Impact of Global Afterload
Follow-up (years)
Over
all
Su
rviv
al,
(%
)
Multivariate Analysis
Med Zva: HR=2.3; p=0.03
High Zva: HR=2.8; p=0.01
100
80
60
40
20
0
0 2 4 6 8
Zva<3.5
P < 0.001
3 years
88 ± 3%
80 ± 3%
70 ± 5%
3.5≤ Zva<4.5
Zva≥ 4.5
Age-Gender matched
general population
Hachicha et al., JACC, 2009

Zva in the SEAS trial
n=1 591 asymptomatic patients
with AS (67±10 yrs, 51% of
hypertensive, 39% of women
In patients with asymptomatic AS without diabetes or known CAD:
• LVEF generally preserved
• LV myocardial dysfunction: 33%
LV myocardial dysfunction:
• common in patients with increased Zva
• especially in the subgroup with low-flow AS
• more concentric LV geometry, LV hypertrophy, and male
Cramariuc et al. JACC CV Img, 2009

Peak aortic velocity ≥ 4.4 m.s-1
Zva ≥ 4.9 mmHg.ml-1.m-2
Longitudinal strain ≤ 15.9 %
Ind. LA area ≥ 12.2 cm2/m2
HR= 1.7, p=0.027
HR= 1.9, p=0.013
HR= 2.2, p=0.003
HR= 2.8, p=0.001
0 1 2 3 4 5
Hazard-ratio
6
Zva in Asymptomatic AS Prospective study: 163 patients with asymptomatic AS and
preserved LV function
Adjustment for gender, systemic arterial compliance, E-wave, E/A
ratio and response to exercise (abnormal vs. normal)
Lancellotti, Donal, Magne et al. Heart, 2010
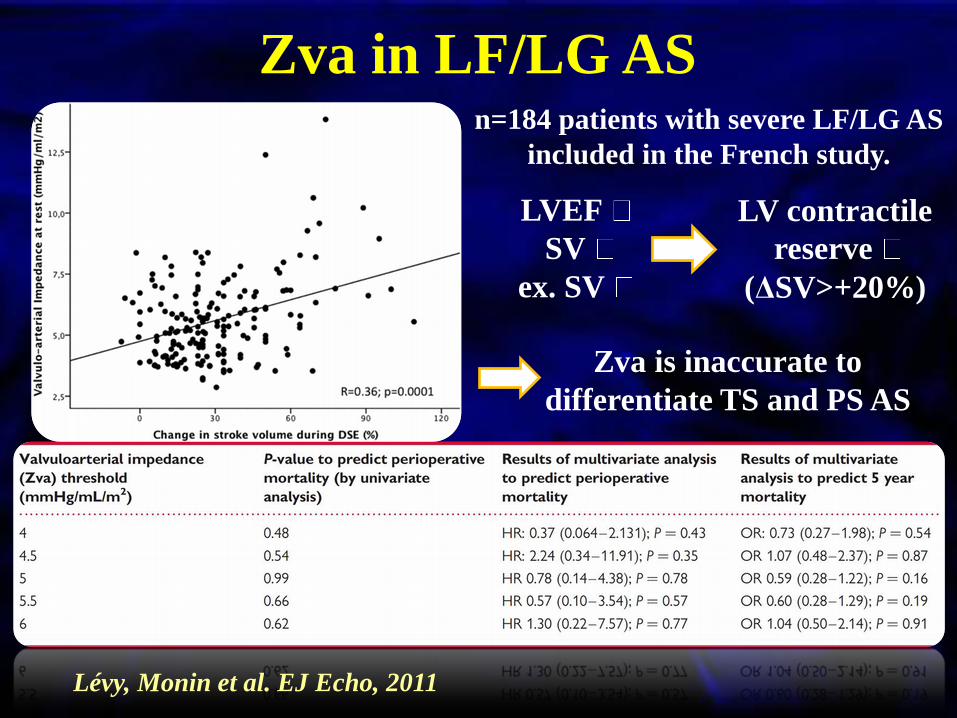
Zva in LF/LG AS n=184 patients with severe LF/LG AS
included in the French study.
Lévy, Monin et al. EJ Echo, 2011
LVEF
SV
ex. SV
LV contractile
reserve
(ΔSV>+20%)
Zva is inaccurate to
differentiate TS and PS AS
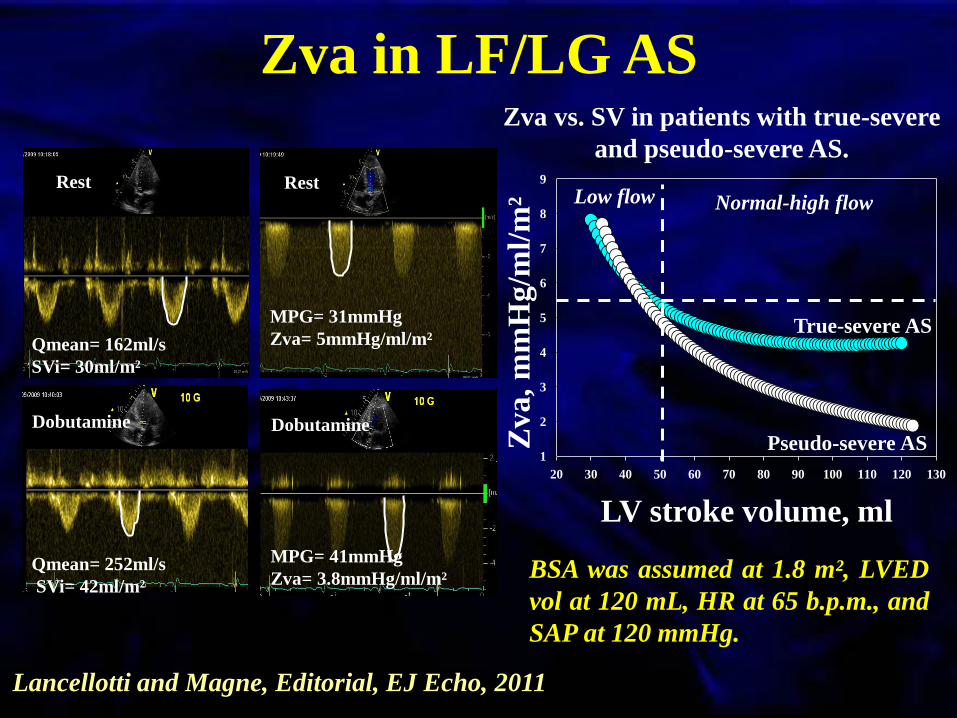
Zva in LF/LG AS
Rest
Qmean= 162ml/s
SVi= 30ml/m²
Rest
MPG= 31mmHg
Zva= 5mmHg/ml/m²
Dobutamine
Qmean= 252ml/s
SVi= 42ml/m²
Dobutamine
MPG= 41mmHg
Zva= 3.8mmHg/ml/m²
20 30 40 50 60 70 80 90 100 110 120 130
1
2
3
4
5
6
7
8
9
Zva
, m
mH
g/m
l/m
² LV stroke volume, ml
Pseudo-severe AS
True-severe AS
Low flow Normal-high flow
BSA was assumed at 1.8 m², LVED
vol at 120 mL, HR at 65 b.p.m., and
SAP at 120 mmHg.
Zva vs. SV in patients with true-severe
and pseudo-severe AS.
Lancellotti and Magne, Editorial, EJ Echo, 2011
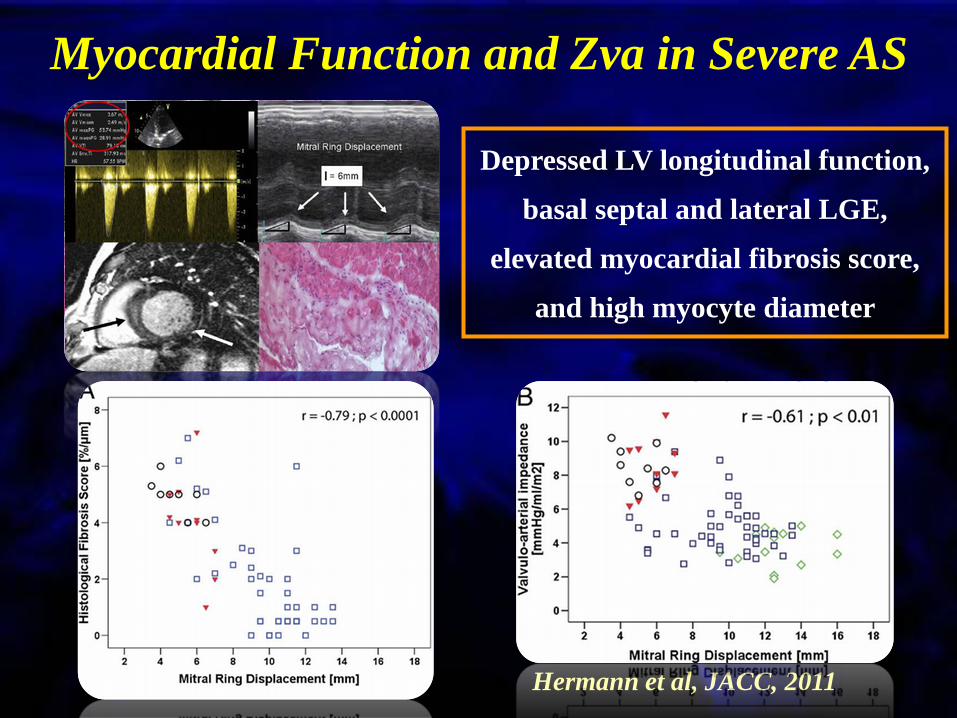
Myocardial Function and Zva in Severe AS
Depressed LV longitudinal function,
basal septal and lateral LGE,
elevated myocardial fibrosis score,
and high myocyte diameter
Hermann et al, JACC, 2011

Maximal Exercise Capacity and Zva
0
5
10
15
20
25
3021.5±4.8 21.2±5.1 20.6±5.3 20.3±5.3 20.2±5.3
18.8±5.8 17.6±5.7 15.6±5.3
14.0±5.9 12.3±6.0
p=0.079 p=0.014 p=0.007 p=0.008 p=0.006
VO
2 m
ax,
mL
/kg/m
in
Valvulo-Arterial Impedance (Zva), mmHg/mL/m²
Dulgheru et al. ESC meeting 2012

Blood pressure should be routinely measured in the echo lab.
and Zva calculated
High Zva in AS patients is an accurate marker of advanced
stage of the disease and is associated with reduced maximal
exercise capacity
High Zva is associated with poor mid- and long-term outcome,
even in asymptomatic patients
In patients with severe asymptomatic AS and high Zva, follow-
up could be shorten and exercise test and/or exercise echo should
be recommended
Conclusion

DON’T MISS
5-8 December 2012
MAICC – Athens, Greece
Abstract submission deadline
31 May
Early bird registration
30 September

Thank you for your
attention.
“In these matters the only certainty is
that nothing is certain.”
Pliny The Elder, 23 AD-79 AD

“Severe” AS with Low Gradient and
Low LVEF
AVA 1.0 cm2
Mean gradient 30-40 mmHg
LVEF 40%
Approximately 5-10% of AS population
High risk patients:
3-year survival 50-60%
If operated (AVR): operative mortality: 8-30%
Sténose Aortique
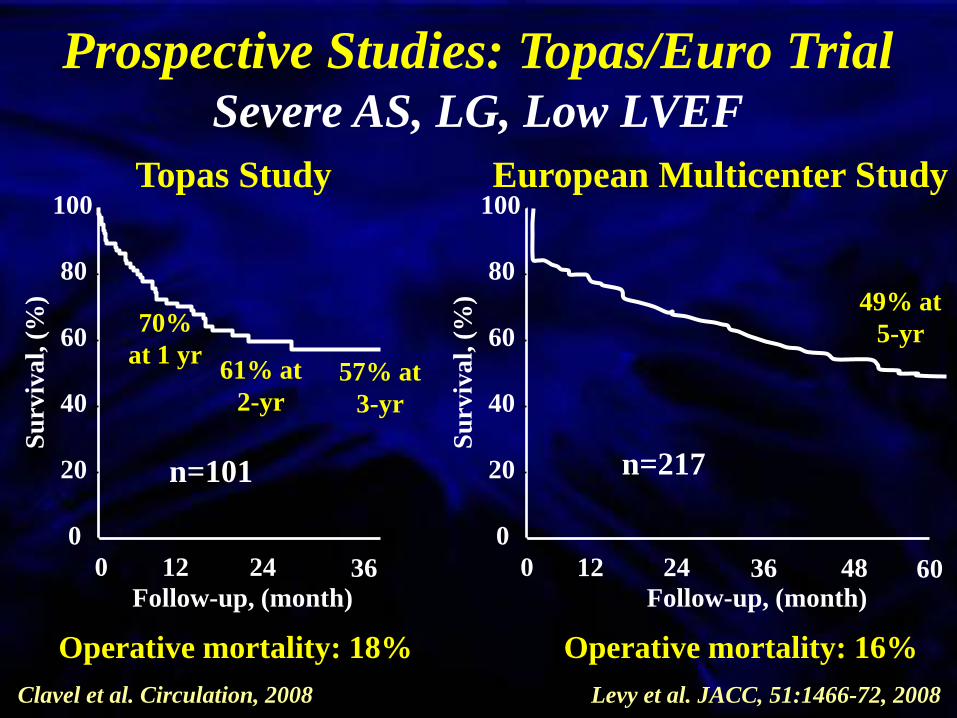
Prospective Studies: Topas/Euro Trial Severe AS, LG, Low LVEF
Follow-up, (month)
Su
rviv
al,
(%
)
0 12 24
0
20
40
60
80
100
36
70%
at 1 yr 61% at
2-yr
57% at
3-yr
Operative mortality: 18%
Follow-up, (month)
Su
rviv
al,
(%
)
0
20
40
60
80
100
0 12 24 36 48 60
Operative mortality: 16%
49% at
5-yr
Topas Study European Multicenter Study
Levy et al. JACC, 51:1466-72, 2008
n=101 n=217
Clavel et al. Circulation, 2008
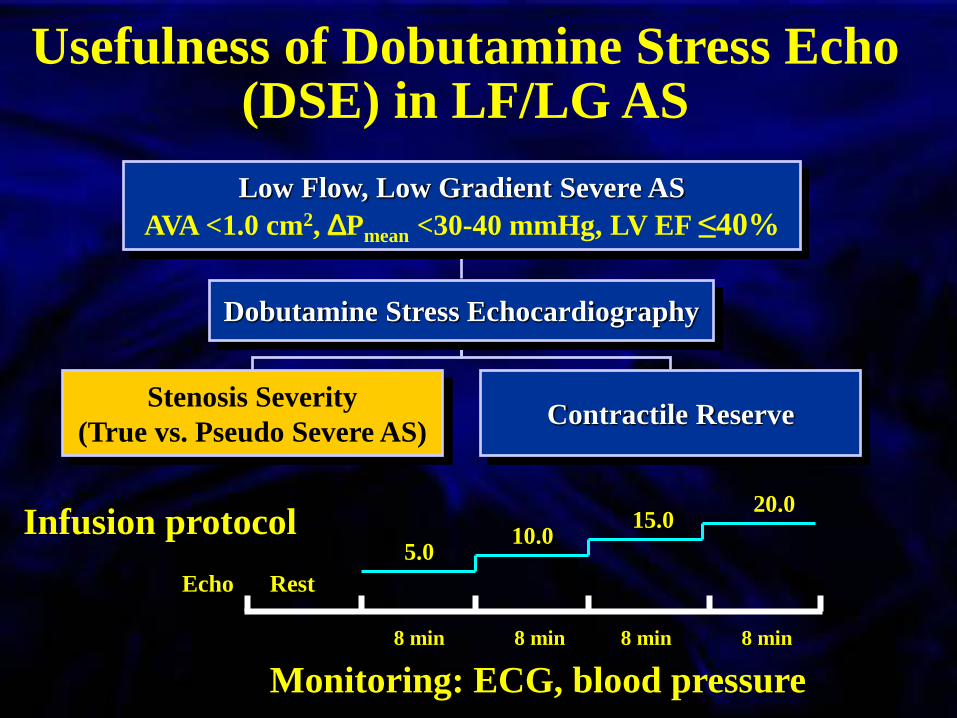
Usefulness of Dobutamine Stress Echo (DSE) in LF/LG AS
Echo Rest
10.0 5.0
20.0 15.0
8 min 8 min 8 min 8 min
Monitoring: ECG, blood pressure
Infusion protocol
Low Flow, Low Gradient Severe AS
AVA <1.0 cm2, DPmean <30-40 mmHg, LV EF ≤40%
Dobutamine Stress Echocardiography
Stenosis Severity
(True vs. Pseudo Severe AS) Contractile Reserve

Low Flow Low Flow High Flow High Flow
True Severe AS Pseudo Severe AS
True Severe AS vs. Pseudo Severe AS ?
∆P
AVA

Risk Stratification in LF/LG Severe AS, Low LVEF
Levy et al. JACC, 51:1466-72, 2008

Clavel et al. Circulation, 2008
Risk Stratification in LF/LG Severe AS, Low LVEF

Dobutamine Sress Echo
SV ≥ 20 %
Contractile Reserve No Contractile Reserve
SV < 20 %
AVR? MEDICAL?
AVR CABG
ΔP>30-40 AVA≤1.0
Pseudo Severe AS
MEDICAL
ΔP≤30-40 AVA>1.0
True Severe AS Indeterminate
ΔP<30-40 AVA≤1.0
ΔP<30-40 AVA≤1.0

Follow-up, (month)
Su
rviv
al,
(%
)
0
20
40
60
80
100
0 12 24 36 48 60
Su
rviv
al,
(%
) 0
20
40
60
80
100
Follow-up, (month)
0 12 24 36 48 60
AVR AVR
Medical Medical
54±7%
13±7%
65±11%
11±7%
p=0.0001 p=0.019
Whole Cohort (n=81) Matched Cohort (n=42)
Ouctome after AVR in Patients without
Contractile Reserve
Tribouilloy et al. JACC, 2009 Operative Mortality: 22%
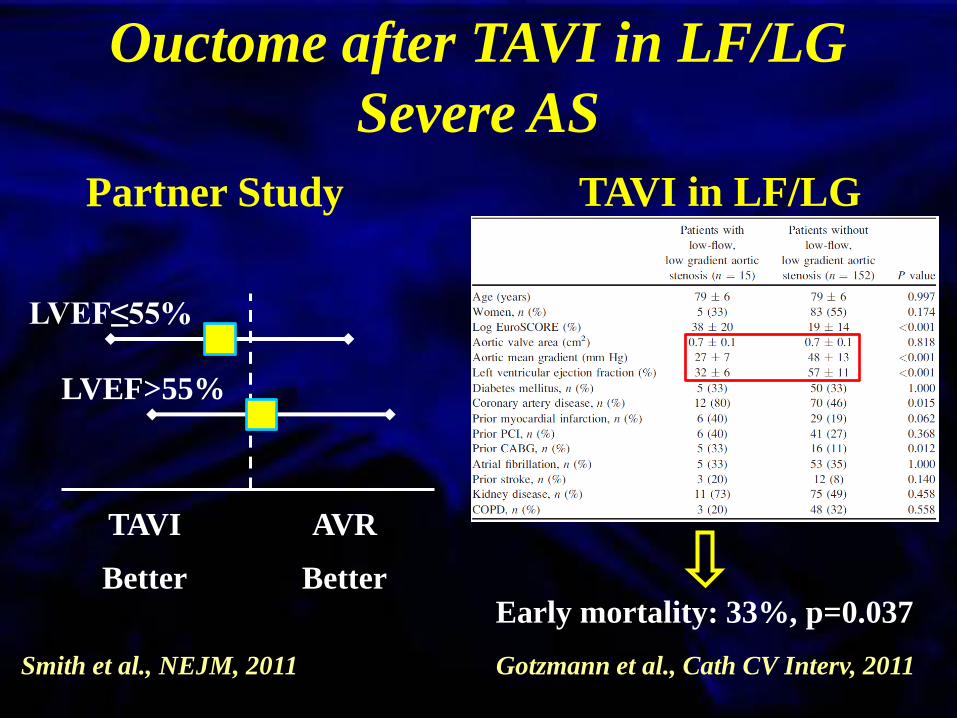
Ouctome after TAVI in LF/LG
Severe AS
Partner Study
TAVI
Better
AVR
Better
LVEF≤55%
LVEF>55%
Smith et al., NEJM, 2011
TAVI in LF/LG
Early mortality: 33%, p=0.037
Gotzmann et al., Cath CV Interv, 2011

SEVERE AS PRESERVED LV FUNCTION
(AVAi ≤ 0.6 cm²/m²) (LVEF ≥ 50%)
331 patients (65%)
SVI > 35ml/m²
Normal Flow (NF) Group
181 patients (35%)
SVI ≤ 35ml/m²
Paradoxical Low Flow
(PLF) Group
n=512
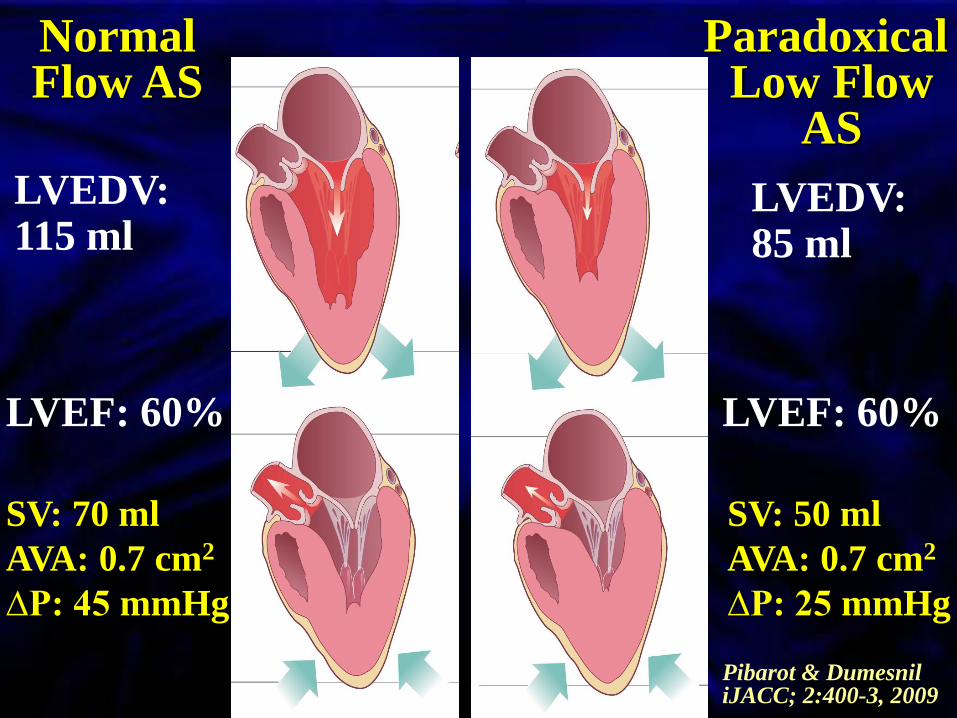
SV: 50 ml
AVA: 0.7 cm2
∆P: 25 mmHg
Normal Flow AS
LVEF: 60%
SV: 70 ml
AVA: 0.7 cm2
∆P: 45 mmHg
LVEDV: 115 ml
LVEF: 60%
Paradoxical Low Flow
AS
LVEDV: 85 ml
Pibarot & Dumesnil iJACC; 2:400-3, 2009
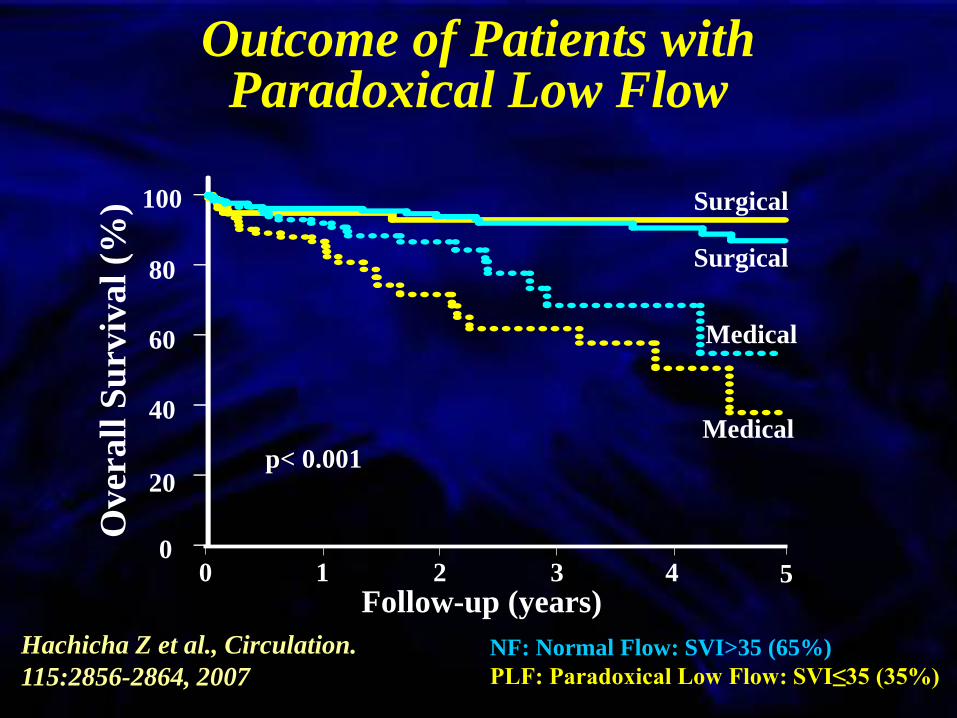
Outcome of Patients with Paradoxical Low Flow
Hachicha Z et al., Circulation.
115:2856-2864, 2007
Over
all
Su
rviv
al
(%)
NF: Normal Flow: SVI>35 (65%)
PLF: Paradoxical Low Flow: SVI≤35 (35%)
Follow-up (years) 0 1 2 3 4 5
0
20
40
60
80
100
p< 0.001
Surgical
Surgical
Medical
Medical

Hachicha
2006
Echo
(512 pts)
Barasch
2006
Echo
(215 pts)
Lancellotti
2010
Echo
(173 pts)
Cramariuc
2009
Echo
(1591 pts)
Minners
2010
Echo
(333 pts)
Minners
2010
Cath
(333 pts)
Jander
2011
Echo
(1525 pts)
Adda
2012
Echo
(340 pts)
Lancellotti
2012
Echo
(150 pts)
Asympt.
Prevalence of PLF/LG Severe AS
≈ 5-15% of Severe AS
Pre
vale
nce
, %

Echo Features of Paradoxical
LF/LG Severe AS
The Aortic Valve:
AVA< 1.0 cm2 AVAi < 0.6 cm2/m2
Severely thickened/calcified valve
Mean gradient <40 mmHg
Valvulo-arterial impedance > 4.5 mmHg.ml-1.m-2
The Left Ventricle
EDD<47 mm EDV< 55 mL/m2
RWT ratio > 0.50
Impaired LV filling
LVEF > 50%
GLS < 16% GRS < 30%
SVi < 35 mL/m2

Advanced Echo Features of
Paradoxical LF/LG Severe AS
-30
-25
-20
-15
-10
-5
0
LV
Str
ain
, %
0
10
20
30
40
50
60
70
NF/HG
NF/LG LF/HG
LF/LG
Radial
GLS LS base
LS mid
LS apex Circ
Adda et al, Circulation CV Img, 2012
LV
Str
ain
, %

Myocardial Function in Paradoxical LF/LG Severe AS
Characterized by similar
LVEF and AVA but lower
MPG and LV SV
Weidemann, Hermann et al, Circ, 2009
Depressed LV longitudinal
function, basal septal and
lateral LGE, elevated
myocardial fibrosis score, and
high myocyte diameter
Hermann et al, JACC, 2011
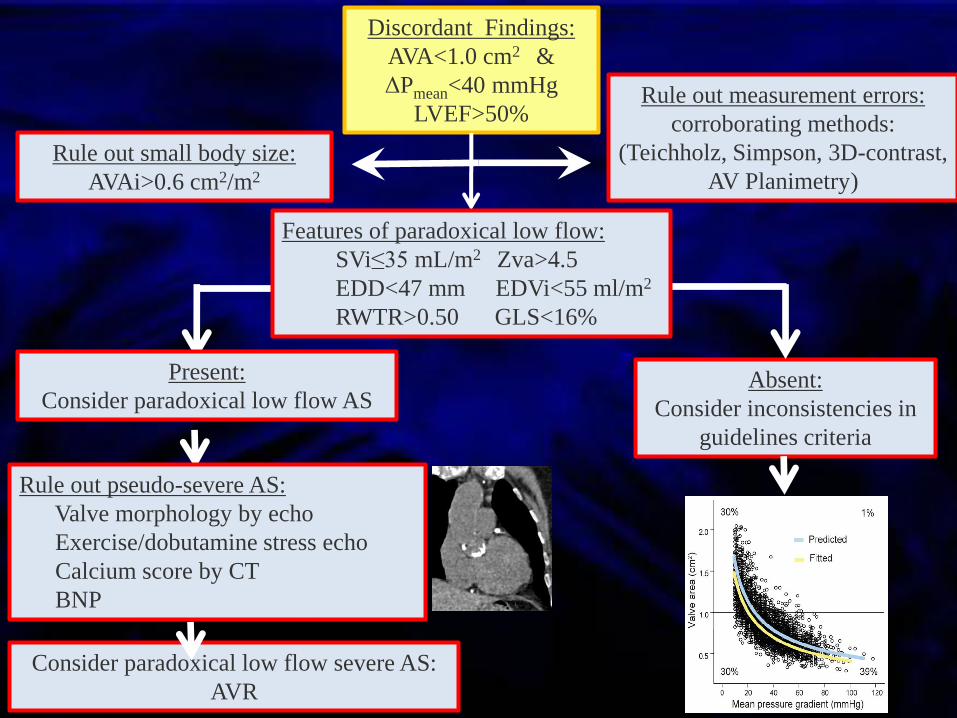
Absent:
Consider inconsistencies in
guidelines criteria
Rule out measurement errors:
corroborating methods:
(Teichholz, Simpson, 3D-contrast,
AV Planimetry)
Rule out small body size:
AVAi>0.6 cm2/m2
Discordant Findings:
AVA<1.0 cm2 &
ΔPmean<40 mmHg
LVEF>50%
Consider paradoxical low flow severe AS:
AVR
Rule out pseudo-severe AS:
Valve morphology by echo
Exercise/dobutamine stress echo
Calcium score by CT
BNP
Present:
Consider paradoxical low flow AS
Features of paradoxical low flow:
SVi≤35 mL/m2 Zva>4.5
EDD<47 mm EDVi<55 ml/m2
RWTR>0.50 GLS<16%

Outcome of Paradoxical LF/LG
Severe AS
SEAS trial
n=1 873
LVEF≥55%
n=1 525
LG Severe AS
n= 435, 29%
Severe AS
n= 35, 2%
Mod. AS
n= 184, 12%
Jander et al, Circulation, 2011

Outcome of Paradoxical LF/LG
Severe AS
Su
rviv
al,
(%
)
0
20
40
60
80
100
Follow-up, (month)
0 12 24 36 48 60
Su
rviv
al,
(%
)
0
20
60
80
100
Follow-up, (month)
0 12 24 36 48 60
p=0.48
40
p=0.64
Aortic Valve Events Major CV Events
Jander et al, Circulation, 2011
Moderate AS
Severe LG AS
Severe AS

Outcome of Paradoxical LF/LG
Jander et al, Circulation, 2011
SV= LVEFxLVED vol 77.1 82.9
BSA: 1.83m² vs. 1.94m²
SVi: 42.1 vs. 42.7 mL/m²
AVA: 0.99 vs. 1.01 cm²
AVAi: 0.54 vs 0.52 cm²/m²
Similar AS severity,
similar outcome!
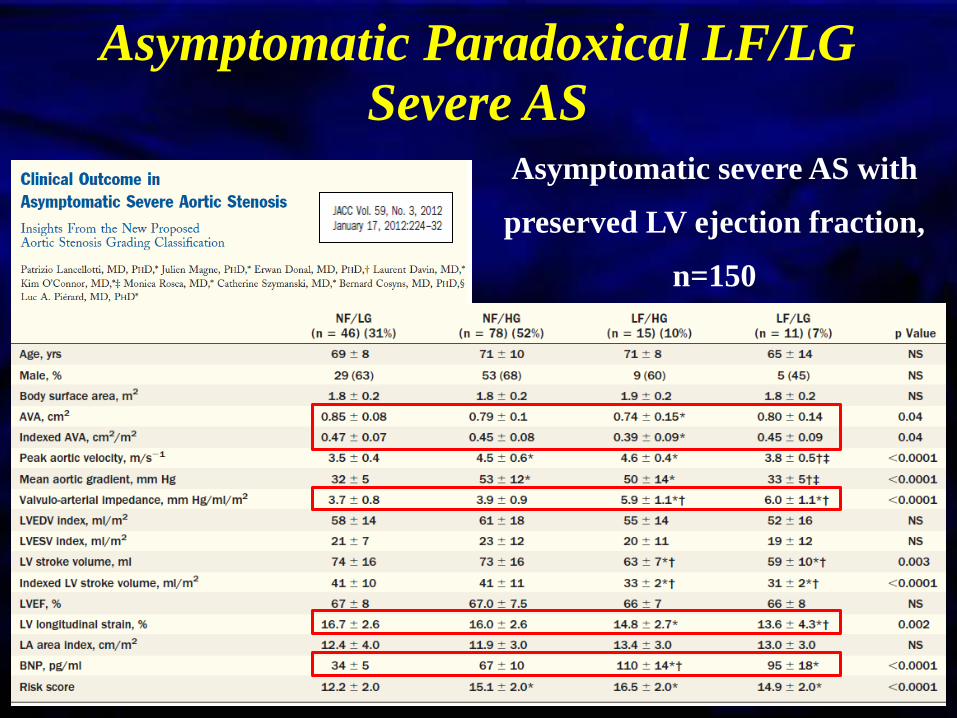
Asymptomatic Paradoxical LF/LG
Severe AS
Asymptomatic severe AS with
preserved LV ejection fraction,
n=150

Asymptomatic Paradoxical LF/LG
Severe AS
Follow-up, months
Ad
just
ed i
nci
den
ce o
f ca
rdia
c e
ven
ts, %
p=0.009 LF/LG group
NF/LG group
NF/HG group
LF/HG group
Key Messages The presence of a moderately increased transvalvular
gradient (<40 mmHg) does not exclude the presence of a
severe AS, even in patients with preserved LVEF
DSE is very useful for the management of LF/LG AS
Paradoxical LF/LG entity is found in 5-15% of AS
patients and is often associated with more advanced
stage of the disease and worse prognosis, even in
asymptomatic patients
It is important to recognize this entity so we do not deny
surgery to a symptomatic patient with small AVA and
LG

Thank you for your
attention.
“In these matters the only certainty is
that nothing is certain.”
Pliny The Elder, 23 AD-79 AD

DON’T MISS
5-8 December 2012
MAICC – Athens, Greece
Abstract submission deadline
31 May
Early bird registration
30 September
Thank you for your
attention.
“In these matters the only certainty is
that nothing is certain.”
Pliny The Elder, 23 AD-79 AD