early childhood - bright futures · average of 41/2 to 61/2 pounds per year and grow ... during...
TRANSCRIPT
Early Childhood1–4
Years
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S
EARLY CHILDHOOD
33
During early childhood (ages 1 to 4), a
child’s world expands to include
friends, schoolmates, and others in the
community. The child’s physical, cog-
nitive, social, and emotional development are tight-
ly linked. For this reason, physical activity affects
not only the physical health of children but also
their overall health status.
Early childhood is divided into two stages: the
toddler stage, ages 1 to 2, and the young child stage,
ages 3 to 4. The toddler stage can be stressful for
parents as toddlers develop a sense of indepen-
dence. As they get older, children become more
interested in trying new activities.
Early childhood is a key period for promoting
physical activity. During these years, fundamental
motor skills, basic movement patterns that all chil-
dren tend to develop (e.g., walking, running, gallop-
ing, jumping, hopping, skipping, throwing, catching,
striking, kicking, balancing), begin to develop. If chil-
dren are encouraged to be physically active, these
skills can develop into advanced patterns of motor
coordination that can last a lifetime. Unfortunately,
many children barely acquire fundamental motor
skills and some will not develop advanced patterns of
motor coordination because they are not encouraged
to participate in physical activities that provide
opportunities to practice these skills.
Participation and instruction in various physi-
cal activities help children develop motor skills.
Although other factors (e.g., genetics) influence
whether a child will become an athlete, physical
activity in early childhood helps ensure that chil-
dren will have the motor skills they need through-
out life. Children will not develop motor skills
without intervention.
Children of this age usually play and explore;
however, many spend only 10 to 20 percent of their
time participating in gross motor physical activities,
which require whole-body participation (e.g., walk-
ing, running, climbing). Many children spend too
much time participating in sedentary behaviors
(e.g., watching television and videotapes, playing
computer games, playing with toys that do not
require the child to move).
Children benefit from physical activity in a
number of ways. Physical activity can
• Give children a feeling of accomplishment.
• Reduce the risk of certain diseases (e.g., coronary
heart disease, hypertension, colon cancer, dia-
betes mellitus), if children continue to be active
during adulthood.
• Promote mental health.
Growth and PhysicalDevelopment
A child’s birthweight quadruples by 2 years of
age. Between the ages of 2 and 5, children gain an
average of 41/2 to 6 1/2 pounds per year and grow
2 1/2 to 31/2 inches per year.
The child’s head and trunk size are large in pro-
portion to the rest of the body, making locomotion
more difficult. However, as the legs grow, the child
is able to move faster and more easily. Skeletal
growth is steady in early childhood, and noninten-
sive physical activity does not damage growing
EARLY CHILDHOOD • 1–4 YEARS
34
bones. Joints are flexible, and they get even more
flexible during this period.
During early childhood, other physical changes
take place that enhance the child’s ability to move
and participate in physical activity:
• Muscles continue to grow.
• The nervous system continues to develop.
• Vision and visual perception improve. (Chil-
dren’s vision does not fully mature before ages 6
or 7. Imprecise eye movements limit their ability
to track and judge the speed of moving objects.)
• Kinesthesia—the sense that detects body posi-
tion, weight, and movement of the muscles, ten-
dons, and joints—improves.
• Sense of balance improves.
• Cognition improves.
Healthy LifestylesEarly childhood is a key time for promoting
the development of motor skills and physical
activity behaviors. Most children are active but
may not have the opportunity to play and explore
because of space or safety concerns, or because
their parents do not encourage them to be physi-
cally active.
Children in early childhood should be encour-
aged to participate in physical activity. Simple
games such as “Simon Says,” chase, and tag are
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S
EARLY CHILDHOOD • 1–4 YEARS
35
appropriate. Physical activities (e.g., tumbling, gym-
nastics, dancing) tailored to the developmental
needs of children are also appropriate. Because most
children need to develop motor skills, they are not
ready for organized sports, which require visual acu-
ity, control, and balance.
Building PartnershipsPartnerships among health professionals, fami-
lies, and communities are essential for ensuring that
families receive guidance on physical activity.
Health professionals need to give parents the oppor-
tunity to discuss physical activity issues and con-
cerns affecting their children, and need to identify
and contact community resources to help parents
promote physical activity in their children.
The community can help promote physical
activity by providing programs that
• Encourage families to promote physical activity
in children.
• Teach families about physical and motor skill
development during early childhood.
• Give children the opportunity to be physically
active.
In addition, communities can provide (1)
affordable, skilled child care providers who promote
physical activity in children, (2) safe environments
for physical activity, and (3) support for families of
children with special health care needs.
Many children spend time with child care
providers or participate in Head Start or other
preschool programs that provide opportunities for
physical activity. Children in community programs
can be introduced to new activities and may try
them more readily if their peers seem to be enjoy-
ing them.
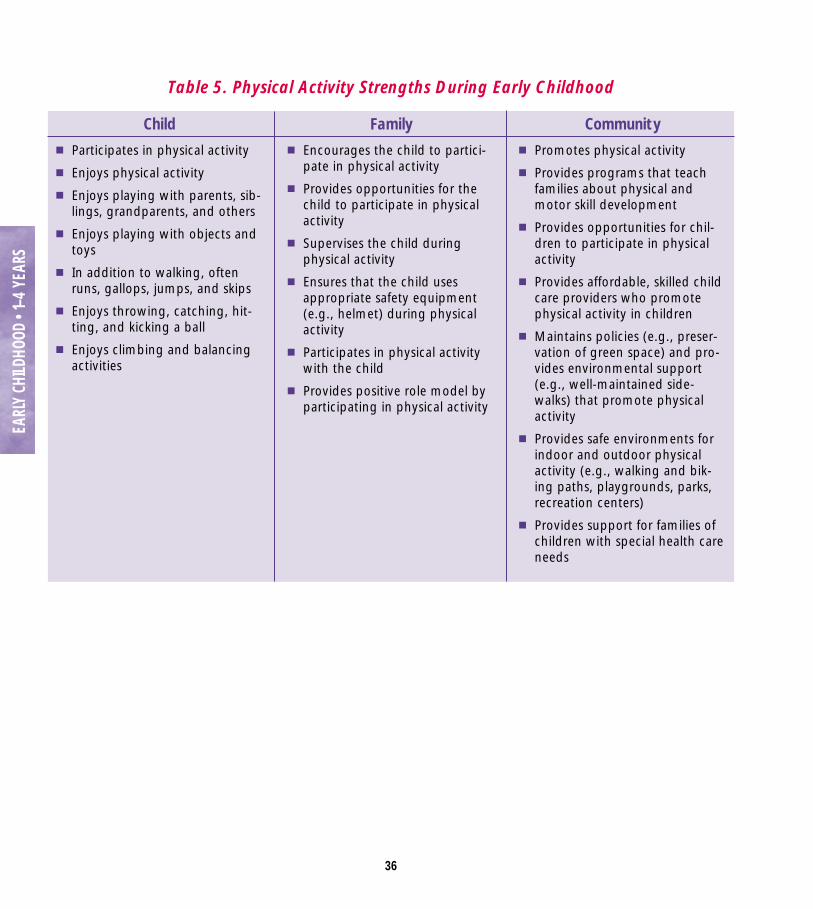
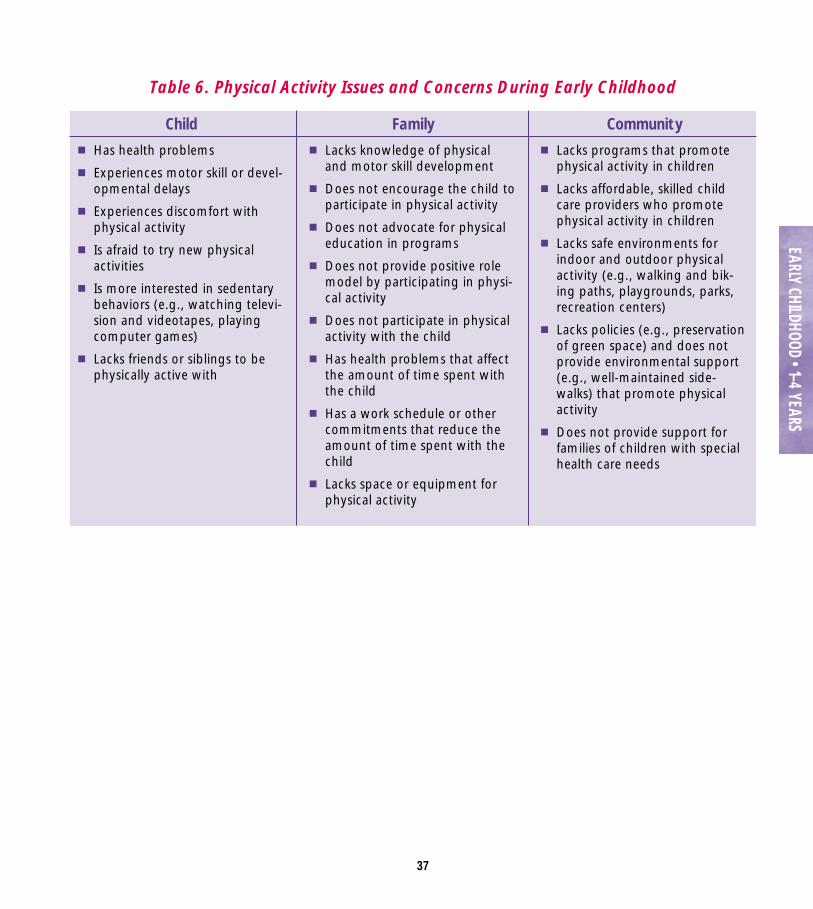
Strengths, and Issues andConcerns
During health supervision visits, health profes-
sionals should emphasize the physical activity
strengths of the child, family, and community
(Table 5) and address any physical activity issues
and concerns (Table 6).
36
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S
Table 5. Physical Activity Strengths During Early Childhood
Child■ Participates in physical activity
■ Enjoys physical activity
■ Enjoys playing with parents, sib-lings, grandparents, and others
■ Enjoys playing with objects andtoys
■ In addition to walking, oftenruns, gallops, jumps, and skips
■ Enjoys throwing, catching, hit-ting, and kicking a ball
■ Enjoys climbing and balancingactivities
Family■ Encourages the child to partici-
pate in physical activity
■ Provides opportunities for thechild to participate in physicalactivity
■ Supervises the child duringphysical activity
■ Ensures that the child usesappropriate safety equipment(e.g., helmet) during physicalactivity
■ Participates in physical activitywith the child
■ Provides positive role model byparticipating in physical activity
Community■ Promotes physical activity
■ Provides programs that teachfamilies about physical andmotor skill development
■ Provides opportunities for chil-dren to participate in physicalactivity
■ Provides affordable, skilled childcare providers who promotephysical activity in children
■ Maintains policies (e.g., preser-vation of green space) and pro-vides environmental support(e.g., well-maintained side-walks) that promote physicalactivity
■ Provides safe environments forindoor and outdoor physicalactivity (e.g., walking and bik-ing paths, playgrounds, parks,recreation centers)
■ Provides support for families ofchildren with special health careneeds
37
EARLY CHILDHOOD • 1–4 YEARS
Table 6. Physical Activity Issues and Concerns During Early Childhood
Child■ Has health problems
■ Experiences motor skill or devel-opmental delays
■ Experiences discomfort withphysical activity
■ Is afraid to try new physicalactivities
■ Is more interested in sedentarybehaviors (e.g., watching televi-sion and videotapes, playingcomputer games)
■ Lacks friends or siblings to bephysically active with
Family■ Lacks knowledge of physical
and motor skill development
■ Does not encourage the child toparticipate in physical activity
■ Does not advocate for physicaleducation in programs
■ Does not provide positive rolemodel by participating in physi-cal activity
■ Does not participate in physicalactivity with the child
■ Has health problems that affectthe amount of time spent withthe child
■ Has a work schedule or othercommitments that reduce theamount of time spent with thechild
■ Lacks space or equipment forphysical activity
Community■ Lacks programs that promote
physical activity in children
■ Lacks affordable, skilled childcare providers who promotephysical activity in children
■ Lacks safe environments forindoor and outdoor physicalactivity (e.g., walking and bik-ing paths, playgrounds, parks,recreation centers)
■ Lacks policies (e.g., preservationof green space) and does notprovide environmental support(e.g., well-maintained side-walks) that promote physicalactivity
■ Does not provide support forfamilies of children with specialhealth care needs
38
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S
A child’s level of physical activity should be
assessed as part of health supervision visits. (For
more information on health supervision, see Bright
Futures: Guidelines for Health Supervision of Infants,
Children, and Adolescents, listed under Suggested
Reading in this chapter.)
Health professionals can begin by gathering
information about the child’s level of physical
activity. This can be accomplished by selectively
asking key interview questions (listed in this chap-
ter), which provide a useful starting point for iden-
tifying physical activity issues and concerns.
Health professionals can then use this chap-
ter’s screening and assessment guidelines, and
counseling guidelines, to provide families with
anticipatory guidance. Interview questions, screen-
ing and assessment, and counseling should be used
as appropriate and will vary from visit to visit,
child to child, and family to family.
Desired outcomes for the child, and the role of
the family, are presented to assist health profession-
als in promoting physical activity.
Interview QuestionsThe following questions are intended to be
used selectively to gather information, to address
the family’s issues and concerns, and to build
partnerships.
Do you have any concerns about Benita’s
development?
How often do you play with her?
What are some physical activities you do with
Ethan?
How often does he get a chance to run?
How often does Benita play with a ball?
How does her development compare to that of
your other children when they were her age?
How much television do you allow Ethan to
watch each day?
Is your neighborhood safe enough for him to
play outside?
Do you participate in physical activity? If so,
which ones?
Did you participate in physical activity when you
were a child?
EARLY CHILDHOOD PHYSICAL ACTIVITY SUPERVISION
EARLY CHILDHOOD • 1–4 YEARS
39
Screening and Assessment■ Measure the child’s length or height and weight,
and plot these on a standard growth chart (see
Tool H: CDC Growth Charts). Deviation from the
expected growth pattern (e.g., a major change in
growth percentiles on the chart) should be evalu-
ated. This may be normal or may indicate a
problem (e.g., difficulties with eating).
■ Assess the child’s visual acuity and eye move-
ment. Vision problems hinder the development
of motor-visual (hand-eye) coordination, an
important component of physical activity.
■ Assess the child’s coordination. Poor coordina-
tion may result from lack of physical activity or
other factors, or it may be a symptom of develop-
mental coordination disorder (DCD). If DCD is
suspected, refer the child for neurodevelopmen-
tal assessment. (See the Developmental Coordi-
nation Disorder chapter.)
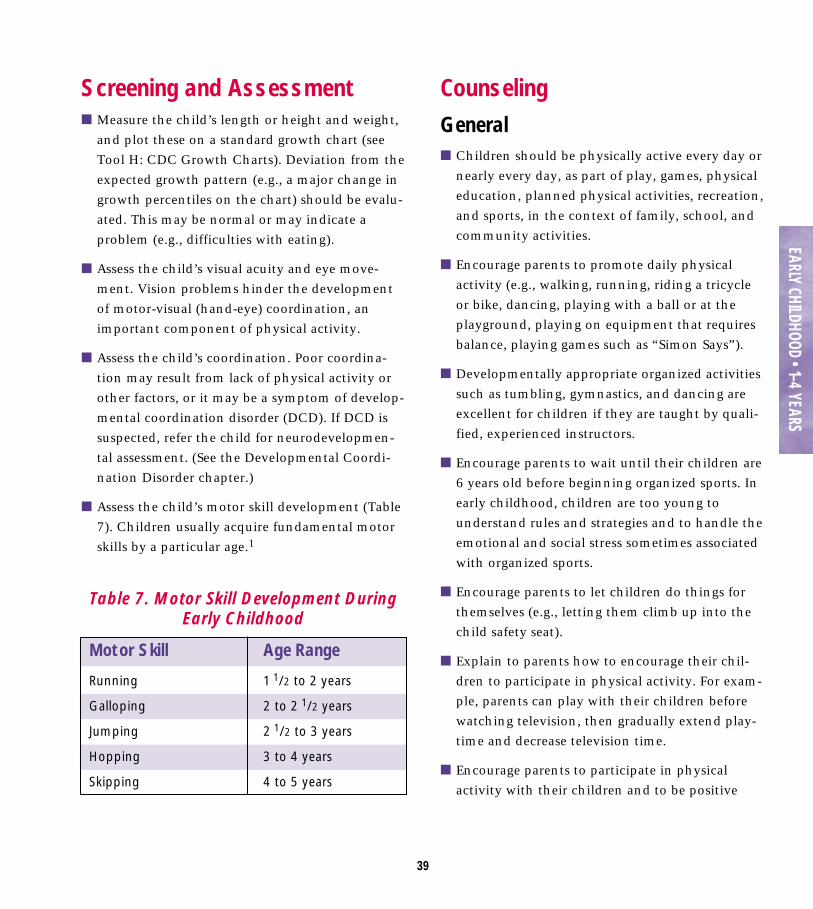
■ Assess the child’s motor skill development (Table
7). Children usually acquire fundamental motor
skills by a particular age.1
CounselingGeneral■ Children should be physically active every day or
nearly every day, as part of play, games, physical
education, planned physical activities, recreation,
and sports, in the context of family, school, and
community activities.
■ Encourage parents to promote daily physical
activity (e.g., walking, running, riding a tricycle
or bike, dancing, playing with a ball or at the
playground, playing on equipment that requires
balance, playing games such as “Simon Says”).
■ Developmentally appropriate organized activities
such as tumbling, gymnastics, and dancing are
excellent for children if they are taught by quali-
fied, experienced instructors.
■ Encourage parents to wait until their children are
6 years old before beginning organized sports. In
early childhood, children are too young to
understand rules and strategies and to handle the
emotional and social stress sometimes associated
with organized sports.
■ Encourage parents to let children do things for
themselves (e.g., letting them climb up into the
child safety seat).
■ Explain to parents how to encourage their chil-
dren to participate in physical activity. For exam-
ple, parents can play with their children before
watching television, then gradually extend play-
time and decrease television time.
■ Encourage parents to participate in physical
activity with their children and to be positive
Table 7. Motor Skill Development DuringEarly Childhood
Motor Skill
Running
Galloping
Jumping
Hopping
Skipping
Age Range
1 1/2 to 2 years
2 to 2 1/2 years
2 1/2 to 3 years
3 to 4 years
4 to 5 years
40
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S
role models by participating in physical activity
themselves.
■ Discuss with parents the importance of using
child care providers who promote physical activi-
ty and have the space and equipment for it.
Physical Development■ Children do not develop catching, throwing, and
kicking skills by a specific age. However, if chil-
dren have not attempted any of these activities
by age 4, they may have difficulties keeping up
with their peers.
■ Tell parents that organized sports, which require
visual acuity, control, and balance, are inappro-
priate for children less than 6 years old because
they need time to develop their motor skills.
Injury Prevention■ Emphasize that children should be supervised
when they participate in physical activity.
■ Emphasize the importance of safety equipment
(e.g., helmets, goggles) when children participate
in physical activity. (See the Injury chapter.)
■ Emphasize the importance of reducing children’s
exposure to sunlight while playing outdoors and
thus their risk of developing skin cancer. Recom-
mend that parents practice preventive strategies
such as (1) applying a broad-spectrum sunscreen
with a sun protection factor (SPF) rating of 15 or
greater to children’s exposed skin 30 minutes
before they go outdoors, (2) reapplying sunscreen
every 2 hours, and (3) ensuring that children
wear broad-spectrum child-sized sunglasses and
brimmed hats and clothing that protect the skin
as much as possible.
Safety■ If the safety of the environment or neighborhood
is a concern, help parents find other settings for
physical activity (e.g., Boys and Girls Clubs of
America, recreation centers, churches and other
places of worship).
■ Remind parents that children can do many activ-
ities indoors with soft equipment that can be
used in tight spaces (e.g., playing tag or hide-and-
seek, tossing a ball, crawling through an obstacle
course).
41
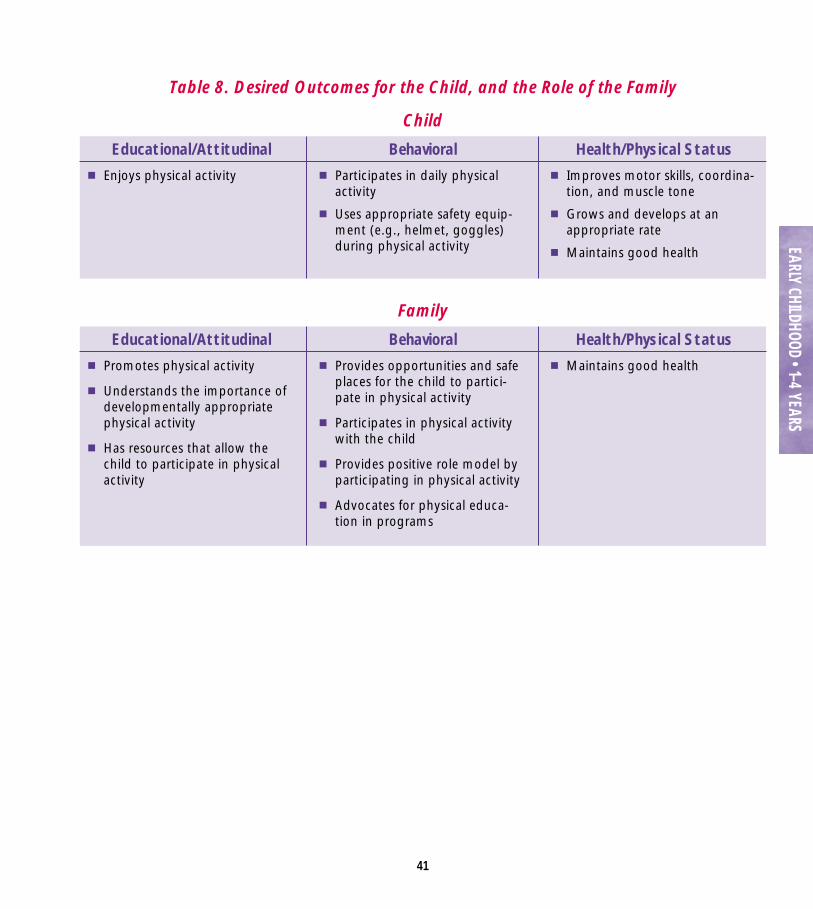
Educational/Attitudinal■ Enjoys physical activity
Behavioral■ Participates in daily physical
activity
■ Uses appropriate safety equip-ment (e.g., helmet, goggles)during physical activity
Health/Physical Status■ Improves motor skills, coordina-
tion, and muscle tone
■ Grows and develops at anappropriate rate
■ Maintains good health
Table 8. Desired Outcomes for the Child, and the Role of the Family
Child
Educational/Attitudinal■ Promotes physical activity
■ Understands the importance ofdevelopmentally appropriatephysical activity
■ Has resources that allow thechild to participate in physicalactivity
Behavioral■ Provides opportunities and safe
places for the child to partici-pate in physical activity
■ Participates in physical activitywith the child
■ Provides positive role model byparticipating in physical activity
■ Advocates for physical educa-tion in programs
Health/Physical Status■ Maintains good health
Family
EARLY CHILDHOOD • 1–4 YEARS

42
Reference1. Gabbard CP. 1999. Lifelong Motor Development (3rd
ed.). Needham Heights, MA: Allyn and Bacon.
Suggested ReadingAssociation of State and Territorial Directors of Health
Promotion and Public Health Education. 1997. Howto Promote Physical Activity in Your Community (2nded.). Washington, DC: Association of State and Terri-torial Directors of Health Promotion and PublicHealth Education.
Clark JE. 1994. Motor development. In RamachandranVS, ed., Encyclopedia of Human Behavior (pp. 245–255).San Diego, CA: Academic Press.
Clements RL, Lee M. 1998. Parent’s Guide to Physical Play.New York, NY: American Association for the Child’sRight to Play.
Gabbard CP. 1999. Lifelong Motor Development (3rd ed.).Needham Heights, MA: Allyn and Bacon.
Green M, Palfrey JS, eds. 2000. Bright Futures: Guidelinesfor Health Supervision of Infants, Children, and Adoles-cents (2nd ed.). Arlington, VA: National Center forEducation in Maternal and Child Health.
Hammett CT. 1992. Movement Activities for Early Child-hood. Champaign, IL: Human Kinetics.
Haywood KM. 1993. Life Span Motor Development. Cham-paign, IL: Human Kinetics.
Malina RM, Bouchard C. 1991. Growth, Maturation andPhysical Activity. Champaign, IL: Human Kinetics.
McCall RM, Craft DH. 2000. Moving with a Purpose: Devel-oping Programs for Preschoolers of All Abilities. Cham-paign, IL: Human Kinetics.
Payne VG, Isaacs LD. 1998. Human Motor Development: ALifespan Approach. Mountain View, CA: Mayfield Pub-lishing.
Pellegrini AD, Smith PK. 1998. Physical activity play: Thenature and function of a neglected aspect of play.Child Development 69(3):577–598.
Rowland T. 1990. Exercise and Children’s Health. Cham-paign, IL: Human Kinetics.
Sanders SW. 1992. Designing Preschool Movement Programs.Champaign, IL: Human Kinetics.
Torbert M, Schneider LB. 1993. Follow Me Too: A Hand-book of Movement Activities for Three- to Five-Year-Olds.Menlo Park, CA: Addison Wesley.
U.S. Department of Health and Human Services; U.S.Department of Education. 2000. Promoting BetterHealth for Young People Through Physical Activity andSports: A Report to the President from the Secretary ofHealth and Human Services and the Secretary of Educa-tion. Atlanta, GA: U.S. Department of Health andHuman Services.
Virgilio SJ. 1997. Fitness Education for Children: A TeamApproach. Champaign, IL: Human Kinetics.
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S
43
Why Isn’t Charlie DevelopingMotor Skills?
Charlie Spooner, a quiet 4-year-old boy, and hismother are going to see Dr.
Higgs, the family physician. Dr.Higgs notices that Charlie iscontent to sit in a chair and gazeat whomever is speaking. He hasno interest in getting up andlooking around or playing withthe toys in the room. Charlie’smother is concerned that Charlieis lagging behind his sister inmotor skill development.
Dr. Higgs reassures Charlie’smother that boys usually takelonger than girls to developmotor skills. Dr. Higgs discoversthat Charlie and his sister go todifferent child care providers.Charlie’s provider does notpromote physical activity, andthe children are allowed to spendhours watching television andplaying with toys that do notrequire much physical activity.On the weekends, Charlie’sparents run and bike; however,they place him in a stroller orbike seat. Charlie’s mother andfather wonder why their childdoes not seem interested inrunning or learning how to ride a bike.
Dr. Higgs explains thatCharlie needs the opportunity totry out various activities that areappropriate for his skill level. Dr.Higgs suggests that rather thanfocusing on running and biking,Charlie’s parents shouldencourage him to try otheractivities (e.g., playing with aball, climbing, jumping) and tomake these activities fun. Dr.Higgs also provides twoadditional suggestions: (1) chang-ing child care providers to onewho promotes physical activityand (2) allowing Charlie toparticipate in organized, super-vised activities (e.g., gymnasticsprograms, play groups). Charlie’smother agrees to give thesesuggestions a try.
EARLY CHILDHOOD • 1–4 YEARS
Dr. Higgs explains
that Charlie needs the
opportunity to try out
various activities that
are appropriate for his
skill level.

FREQUENTLY ASKED QUESTIONS ABOUT PHYSICAL ACTIVITY IN EARLY CHILDHOOD
44
■ How can I help my 3-year-old learn newskills, such as throwing a ball?
Children go through stages as they learn some-thing new, whether it’s learning to feed them-selves or to coordinate their arms and legs. Somechildren learn more quickly than others. Somemay need extra help from an adult. All childrenneed practice when they are learning new skills,just like adults do.
■ What physical activities are appropriatefor my child?
Physical activities (for example, running, jump-ing, climbing, and throwing, catching, or hittinga ball) and simple games (for example, “SimonSays,” chase, and tag) are appropriate for chil-dren. Your child can also participate in develop-mentally appropriate organized activities (forexample, tumbling, gymnastics, and dancing).Children less than 6 years old do not have themotor skills, or mental and emotional capabili-ties, to participate in organized sports.
■ How often should my child participate inphysical activity?
Your child will benefit most from daily physicalactivity. Children tend to be active in spurts andknow when they need to rest.
■ My neighborhood isn’t very safe. How can my child be active if he can’t playoutdoors?
Community organizations, recreation centers,and churches and other places of worship pro-vide opportunities for children to participate inphysical activity. Work with community leadersto ensure that your child has safe places for par-ticipating in physical activity (for example, walk-ing and biking paths, playgrounds, parks, andrecreation centers). Also, your child can do manyactivities at home such as hopping, dancing,playing tag or hide-and-seek, tossing a ball, orcrawling through an obstacle course.
■ Why is my daughter afraid of playing onplayground equipment?
Be patient, and try holding on to her when she ison the equipment. If this doesn’t work, try tofind other activities that do not frighten her.
■ My son is lagging behind my daughter inmotor skill development even though mydaughter is a year younger. Why?
Boys often take longer than girls to developmotor skills. However, once boys learn a skill,they usually perform it as well as girls. Boys tendto perform better than girls in activities requiringstrength (for example, throwing), and girls tendto perform better in activities requiring balanceand fine motor skills (for example, tap dancing).
EARL
Y CH
ILDHO
OD •
1–4
YEAR
S

45
■ Should I enroll my child in a gymnasticsor dancing class?
Classes taught by qualified and experiencedinstructors can be excellent for children. Alwayscheck on instructors’ qualifications, and observethe classes as much as possible.
■ Our child care provider does not encour-age physical activity. What should I do?
Talk to your child care provider and encourageher to incorporate physical activity into the day.If lack of space or equipment is the problem,work with her to come up with creative ideas toprovide physical activity opportunities for thechildren. If this is not possible, consider chang-ing child care providers to one who promotesphysical activity.
Resources for FamiliesSee Tool F: Physical Activity Resources for con-
tact information on national organizations that can
provide information on physical activity. State and
local departments of public health and education
and local libraries are additional sources of
information.
Centers for Disease Control and Prevention, NationalCenter for Chronic Disease Prevention and HealthPromotion. 1999. Promoting Physical Activity: A Guidefor Community Action. Champaign, IL: Human Kinetics.
Cooper KH. 1999. Fit Kids! The Complete Shape-Up Programfor Birth Through High School. Nashville, TN: Broad-man and Holman Publishers.
Corbin CB, Pangrazi RP. 1998. Physical Activity for Chil-dren: A Statement of Guidelines. Reston, VA: NationalAssociation for Sport and Physical Education.
Institute for Research and Education HealthSystem Min-nesota, Health Education Center. 1996. Building YourActivity Pyramid. Minneapolis, MN: Institute forResearch and Education HealthSystem Minnesota,Health Education Center.
Kalish S. 1995. Your Child’s Fitness: Practical Advice for Par-ents. Champaign, IL: Human Kinetics.
Katzman CS, McCary R, Kidushim-Allen D. 1993. HelpingYour Child Be Healthy and Fit with Activities for ChildrenAged 4 Through 11. Washington, DC: U.S. Departmentof Education, Office of Educational Research andImprovement.
Koch T, Kamberg M. 1997. Cabin Fever Relievers: Hundredsof Games, Activities, and Crafts for Creative Indoor Fun.St. Paul, MN: Redleaf Press.
Kranowitz CS. 1995. 101 Activities for Kids in Tight Spaces.New York, NY: St. Martin’s Press.
Landy J, Burridge K. 1997. 50 Simple Things You Can Do toRaise a Child Who Is Physically Fit. New York, NY:Macmillan.
EARLY CHILDHOOD • 1–4 YEARS

46
National Association for Sport and Physical Education.1999. Help Your Child Achieve a Fit and HealthyLifestyle. Reston, VA: National Association for Sportand Physical Education.
National Association for Sport and Physical Education.1994. Developmentally Appropriate Practice for YoungChildren, Ages 3–5. Reston, VA: National Associationfor Sport and Physical Education.
National Institutes of Health, National Heart, Lung, andBlood Institute. 1995. Asthma and Physical Activity inthe School: Making a Difference. Bethesda, MD: Nation-al Institutes of Health, National Heart, Lung, andBlood Institute.
President’s Council on Physical Fitness and Sports. 1992.Kids in Action: Fitness for Children. Washington, DC:President’s Council on Physical Fitness and Sports.
Shisler J, Killingsworth R, Schmid T. 1999. Kidswalk-to-School: A Guide for Community Action to Promote Chil-dren Walking to School. Atlanta, GA: Centers forDisease Control and Prevention, National Center forChronic Disease Prevention and Health Promotion.EA
RLY
CHILD
HOOD
• 1–
4 YE
ARS