early childhood development programme evaluation report · 2014-05-23 · direct beneficiaryfor the...
TRANSCRIPT

EARLY CHILDHOOD DEVELOPMENT PROGRAMME EVALUATION REPORT

Early Childhood Development Programme evaluation report 1. Introduction The year 2012 marked a full five years that the FNB Fund has been a key player in the ECD sector. This journey started in 2006 with a position paper that was presented to the committee summarising the then-current context, policy imperatives, challenges and opportunities. In February 2007, Tshikululu Social Investments, on behalf of the FNB Fund, held a series of engagements; a significant one being a two-day workshop with the DG Murray Trust and Jim Joel Foundation and five other key ECD organisations to map out innovative projects that could be considered in order to address the challenges that were facing the ECD sector. This workshop outlined three critical issues that required attention, despite existing efforts of ECD service delivery and legislative frameworks: the low number of children accessing ECD services, aging leadership in the sector, and static ECD practitioner professional development. The discussions from the workshop and engagements with key players in the sector informed the ECD programme strategy paper that was tabled to the committee for approval in June 2007. The overarching goal of the ECD programme was to improve the quality of and increase access to the ECD services, and the following objectives were developed:
• To increase access to services, in particular striving for full national coverage across all provinces;
• To support the continued development and implementation of quality ECD initiatives; • To support community-based provision of services; and • To take cognisance of the need to replace aging leadership in the sector and actively support
mentorship and the transfer of skills between established and emerging organisations
Two years later (in June 2009), the programme objectives shifted and more emphasis was placed on improving the quality of ECD services. The Fund decided to channel more resources towards improving quality because government was funding access of ECD to children. In essence, the Fund’s ECD programme objectives of increasing access to ECD services had a stable implementation span of about two complete years; while improving the quality of ECD services enjoyed attention for about four years of implementation within the period under review (2007/8–2011/12). In order to critically asses whether the Fund through its intervention was meeting achieving its goal, a decision to evaluate the programme was made. The early childhood development (ECD) programme evaluation was conducted in October to December 2012, targeting the current ECD project partners; the ECD centres that benefitted from their services; the children accessing ECD services from these centres and their parents; and the ECD practitioners who received ECD level-4 training funded by the Fund. In addition, recommendations are provided to inform the ECD programme strategy for the next three years (2013–2015). This evaluation thus seeks to evaluate the effectiveness of these strategies of the ECD Programme in achieving the overarching goal of the programme. 1.1 Conceptual framework for evaluating the ECD Programme The fundamental questions underpinning this evaluation were:
• How effectively have the Fund’s ECD partners increased access to ECD services for children nationwide?
• How effectively have the Fund’s ECD partners improved the quality of ECD services through ECD practitioner training?

Figure 1: Conceptual framework of the evaluation
• How effectively have the Fund’s ECD partners capacitated emerging ECD centres to provide quality ECD services to children and ultimately address the ageing leadership issue in the sector?
A conceptual framework was developed in order to respond to these key questions. On a basic level, the objectives of the ECD programme were very straightforward and could be evaluated by counting the number of children that accessed ECD services (to determine whether access was increased), counting the number of practitioners that completed the training (to determine whether quality of ECD services was improved), and studying the emerging ECD centres and the milestones they have achieved (to determine if capacity had been built). However, assessing the success of the programme required more than just counting numbers. To determine the improvement of the quality of ECD services, ‘school readiness of children’ was adopted as a proxy indicator to measure quality. The argument is that if the quality of the ECD practitioner training is improved, the practitioners will help to improve the cognitive, intellectual, social and emotional development of children, and thus enable them to be ready to cope with the demanding needs of a formal primary school. Similarly, if partners help to improve access to quality ECD services or help to build the capacity of ECD centres, this should also lead to great school readiness for children. The evaluation team believed that the central logic of supporting the ECD sector, through the three key objectives, should result in children who are more prepared for formal schooling. The implication of stretching the programme objectives to include schools readiness may have been premature, as the ECD partners did not put systems in place to measure this indicator. Hence, the school readiness assessment results will highlight the conditions that enhance this objective and a list of recommended indicators to measure it, for consideration by the Fund in the next three-year programme strategy. 1.2 Evaluation methodology, sampling methodology, and ethics 1.2.1 Evaluation methodology The evaluation employed a rigourous qualitative data-collection approach. The data collection methods included:
• A document review of project partners’ annual reports from 2008 to 2011; • Collation of FNB Fund committee papers; • A literature review; • A self-administered semi-structured questionnaire completed by programme partners; • In-depth interviews with the managers of the Fund’s 21 partners1; • In-depth interviews with managers and practitioners of beneficiary ECD centres2; • Focus group discussions with the parents of the children attending beneficiary ECD centres; and • Assessments of school readiness with a selected number of grade R children in the centres that
directly3 or indirectly4 benefitted from the Fund’s ECD programme 1 An ECD project partner refers to an ECD organisation that is directly funded by the FNB Fund ECD Programme 2 A beneficiary ECD centre refers to an ECD centre that has benefitted from the services of the ECD project partners.

This approach to data collection helped to determine the effectiveness of the programme (and the FNB Fund’s investments) thus far, while simultaneously ensuring that the voices of direct or/and indirect beneficiaries of these services are heard. 1.2.2 Sampling methodology The evaluation adopted two sampling methods. A consensus sampling5 method was adopted to evaluate the ECD project partners, while a convenient sampling6 method was used for ECD practitioners, children, and parents. Consensus sampling was chosen for this study due to the different implementation approaches used by the ECD partners to deliver the practitioner training, access to ECD services and capacity building; while the convenient sampling used with the practitioners, children, and parents was dictated by the timing of the evaluation. In-depth interviews and focus groups were conducted with:
• Project managers and staff of the 21 ECD project partners; • 21 ECD managers and 25 ECD practitioners from beneficiary ECD centres
Six focus group discussions were held and facilitated with 54 caregivers of children accessing ECD services from beneficiary ECD centres and ECD project partners in Free State, Gauteng, Western Cape and KwaZulu-Natal.
School readiness assessments were conducted with forty-five children aged between five and six years old, at the six beneficiary ECD centres and one ECD partner in NorthWest; Eastern Cape and Free State. The assessment was administered by Dr Eunice van Deventer, an educational psychologist who worked with a team of evaluators from MTD Research Specialists. 1.2.3 Ethics Permission to conduct interviews with practitioners, project managers, and focus group participants was obtained from the Fund’s ECD partners and the evaluands7 themselves. Consent to conduct school readiness assessments with children was obtained from their caregivers. 1.3 Limitations The study was conducted towards the end of the year when the ECD partners were preparing for the year-end planning and reviews and the beneficiary ECD centres were preparing for graduations –dictating/resulting in only the practitioners, children and parents that could be available at such short notice participating in the evaluation. Because of the qualititative methods used to conduct the evaluation, the results cannot be generalised to all the practitioners, nor to the grade R children and parents that benefitted either directly or indirectly from the ECD services, as the views expressed during the evaluation, were unique to their context and experience of the services.
3 A direct beneficiary for the purposes of this report refers to a child that directly had access to ECD services offered by the ECD project partners. 4 An indirect beneficiary in this case refers to a child that accesses ECD services from an ECD centre whose practitioner has been trained by the ECD project partners. 5 Consensus sampling refers to a sampling technique that includes everyone. For the purposes of this evaluation we included every ECD partner that was still funded by the Fund. 6 Convenient sampling refers to a sampling technique that selected people based on their availability and accessibility 7 Evaluands refers to people participating in the programme evaluation.

2. Literature review ECD legislative frameworks The legislative cornerstones of the ECD sector in South Africa are the White Paper 5 on ECD, 2001; Guidelines for ECD, 2006; the National Integrated Plan for ECD, 2005–2010; and the National Programme of Action for Children. These documents aim to expand services to children from 0–9 years old in the following areas: health, nutrition, support and stimulation at the home, community-centre-based services, aftercare for school-going children, stimulation programmes including part-day programmes, and family education. While the ECD services that are operating in public schools are legislated under the jurisdiction of the Department of Education, those targeted by the Fund – the community-based centres and home-based programmes – are legislated under the Department of Social Development. Throughout the abovementioned documents a strong thrust is made towards the exploration of other approaches to ECD in order to expand services to children. These approaches include, among others, a host of home-based and centre-based programmes – a sector in which most of the access ECD partners supported by the Fund are playing. The national integrated plan (NIP 2005–2010) for ECD, which is currently under review, aims to integrate the efforts of the fragmented legislative frameworks and service delivery relating to ECD across all sectors of government, the not-for-profit sector, and communities in order to maximise its impact. In addition, the NIP identified a number of challenges which it aims to address through inter-sectoral collaboration between various government department and the community. These are:
• Limited access to ECD services; • Inequities in existing ECD provisioning; • Variable quality of ECD services; and • Lack of adequate human and financial resources in the ECD sector, both at national provincial
and local/district levels Socio-economic status in South Africa hinders the ability of children to enjoy the accessibility of ECD services Tulani University (2011:8) notes that while the ECD centres have experienced some notable successes, challenges remain in regard to providing ECD education to disadvantaged children throughout South Africa. These challenges relate to:
• Inconsistent programme attendance, especially among children whose families experience serious economic hardship or whose parents or caregivers are chronically ill. In other cases, children are enrolled in ECD programmes only a few months before they are to start primary school, with the expectation that the programme will be able to prepare them fully for grade R or grade one, despite insufficient time to do so. Raising awareness about the importance of ECD and implementing parent-centered programmes, as well as increasing the scope of existing parent-centered programmes, would help organisations reach more children.
• In rural and low-income communities ECD centres often struggle to find qualified ECD practitioners. There is also a common need for more resources for infrastructure, and for administrative support, which would better enable centers to obtain government registration, and relieve practitioners from the many administrative duties that interfere with their teaching time.
• For children who have cognitive or physical challenges, inadequate assessment and support were cited frequently. Many are unable to cope in a regular classroom setting without specialised assistance. Additional training on effective techniques for working with children who have cognitive or physical challenges would benefit these children and their teachers alike.
Dawes, Biersteker and Hendrick (2012:16) echoed the same sentiments in the evaluation study of the Ilifa Labantwana ECD Programme. The evaluation found that the consequences socio-economic status has on the development of children even before they reach school are dire. ‘Accordingly, because of the high levels of poverty in South Africa, by the time many South African children reach school, they have already been compromised by the consequences of poverty, notably malnourishment. Early stunting as a result of malnutrition compromises neurological development, and significantly impedes the ability of children to benefit from education’ (Dawes et al, 2012:16).

Is there a relationship between poor ECD centres’ infrastructure and resources and the quality of service offered? The study undertaken by the Departments of Basic Education and Social Development, and UNICEF (2011) concluded that poverty, poor infrastructure and lack of resources in ECD centres have a significant influence on the ability of the ECD centres to provide quality services to children. Most encouraging is that even in these dire situations, the ECD centres are doing their best to have well-organised playrooms with a daily programme. The study concludes that:
• Unregistered facilities more often provide low-quality services and often have inadequate infrastructure and unsafe classrooms. Reasons provided for not applying for registration were that they had just started recently, that they did not qualify (usually due to poor infrastructure), or even that they did not know about the grants and registration (an area that the FNB Fund is currently trying to address through its capacity-building objective);
• There is clearly room for improvement in service delivery, given the demonstrated importance of ECD in providing a solid foundation for children’s education. ECD principals at community-based facilities cite lack of resources, and specifically insufficient classrooms, playgrounds and toilet facilities, issues surrounding the security of children, lack of funding, shortages of qualified teachers and training, the lack of involvement of parents, and the poor and disadvantaged backgrounds of children as problems. Many of these items are most appropriately and effectively provided at the local level, and ideally by the municipality.
What is the long-term social return on investment in ECD services? The benefits associated with the ECD programme were revealed by the American Journal of Preventive Medicine (2003). The study compared children that attended ECD programmes and those that did not and found that ECD has life-long benefits, particularly cognitive benefits, and is a precursor for socio-economic and health gains. Some concrete relationships between ECD services and cognitive outcomes discovered were as follows:
• Students enrolled in ECD programmes demonstrated increases in academic achievement. • Student retention rates among students enrolled in ECD programmes were lower compared to
their counterparts. Retention in grades is highly predictive of failure to graduate from high school, and high school graduation is an important precursor to socio-economic well-being and improved health status.
• Moreover, ECD programmes were found to have a significant benefit for children with disabilities: ‘children placed in special education because of developmental delays, disabilities, or other learning difficulty demonstrated reduction in special education placement for students who had been enrolled in early childhood development programs’ (American Journal of Preventive Medicine, 2003).
Summary of key points from the literature
• Focus of the legislative frameworks continues to be expanding access to ECD services, improving the quality of practitioners, and improving the infrastructural and financial resources of the ECD services.
• There is inconsistent attendance of children in the ECD services due to parents’ economic hardship and chronic illnesses.
• The rural and low-income ECD centres are struggling to attract and retain qualified practitioners. • Unregistered facilities often provide low-quality services because of inadequate infrastructure and
unsafe facilities. • Consequences of poverty, mainly malnutrition, have dire effects on children’s development, even
before they reach school. • ECD has long-lasting benefits to children later in life such as student retention and academic
achievement.
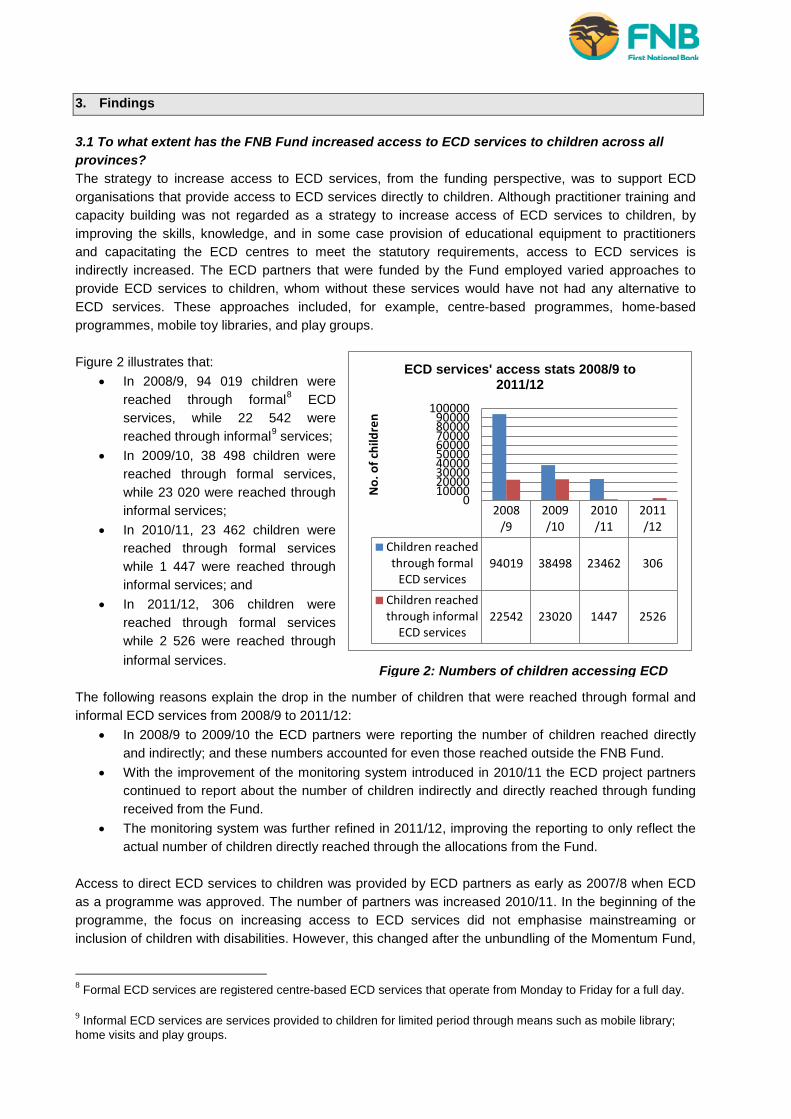
Figure 2: Numbers of children accessing ECD
2008/9
2009/10
2010/11
2011/12
Children reachedthrough formal
ECD services94019 38498 23462 306
Children reachedthrough informal
ECD services22542 23020 1447 2526
0100002000030000400005000060000700008000090000
100000
No.
of c
hild
ren
ECD services' access stats 2008/9 to 2011/12
3. Findings 3.1 To what extent has the FNB Fund increased access to ECD services to children across all provinces? The strategy to increase access to ECD services, from the funding perspective, was to support ECD organisations that provide access to ECD services directly to children. Although practitioner training and capacity building was not regarded as a strategy to increase access of ECD services to children, by improving the skills, knowledge, and in some case provision of educational equipment to practitioners and capacitating the ECD centres to meet the statutory requirements, access to ECD services is indirectly increased. The ECD partners that were funded by the Fund employed varied approaches to provide ECD services to children, whom without these services would have not had any alternative to ECD services. These approaches included, for example, centre-based programmes, home-based programmes, mobile toy libraries, and play groups. Figure 2 illustrates that:
• In 2008/9, 94 019 children were reached through formal8 ECD services, while 22 542 were reached through informal9 services;
• In 2009/10, 38 498 children were reached through formal services, while 23 020 were reached through informal services;
• In 2010/11, 23 462 children were reached through formal services while 1 447 were reached through informal services; and
• In 2011/12, 306 children were reached through formal services while 2 526 were reached through informal services.
The following reasons explain the drop in the number of children that were reached through formal and informal ECD services from 2008/9 to 2011/12:
• In 2008/9 to 2009/10 the ECD partners were reporting the number of children reached directly and indirectly; and these numbers accounted for even those reached outside the FNB Fund.
• With the improvement of the monitoring system introduced in 2010/11 the ECD project partners continued to report about the number of children indirectly and directly reached through funding received from the Fund.
• The monitoring system was further refined in 2011/12, improving the reporting to only reflect the actual number of children directly reached through the allocations from the Fund.
Access to direct ECD services to children was provided by ECD partners as early as 2007/8 when ECD as a programme was approved. The number of partners was increased 2010/11. In the beginning of the programme, the focus on increasing access to ECD services did not emphasise mainstreaming or inclusion of children with disabilities. However, this changed after the unbundling of the Momentum Fund,
8 Formal ECD services are registered centre-based ECD services that operate from Monday to Friday for a full day. 9 Informal ECD services are services provided to children for limited period through means such as mobile library; home visits and play groups.

when a decision was taken to make this a cross-cutting area of the Foundation. ECD project partners were brought in to respond to this decision. The models of providing the ECD services to children are varied across all the seven current ECD project partners. While some partners provide full five-day centre-based ECD services to children, others only expose children to the ECD services through non centre-based models such as mobile toy libraries, home-visits, and play groups. The different models and frequency of exposure of children to the ECD services are discussed in the following section. The refinement of the reporting and monitoring system makes it difficult to conclude whether the Fund has increased access to ECD services to children as the statistics dropped from year to year, see Figure 2 above. What can be said though is that the Fund has expanded the access of ECD services to children who without the Fund would have not had access to any ECD services. Models used to increase access of ECD services to children Partner A Project description Partner A is addressing a critical need in the community of Greytown, KwaZulu-Natal, where without its services children would be roaming around the streets and therefore vulnerable to all sorts of abuse. Although the benefits of a three-hour session per day once a week would not compare to that of a full-day ECD service, this programme still addresses these children’s critical developmental needs, as they are exposed to rhymes/music, fantasy, and basic literacy and numeracy skills. Partner A trains community members who volunteer to provide home-visit play groups. Children walk to the different houses at which ECD services are provided every day – thus increasing their exposure to the services to four days a week instead of the intended three hours a week. Key characteristics and highlights
• Partner A provides access to ECD services to children aged one to five years through home visits
• The play groups are implemented by community members, referred to as ‘Umhambi’, trained by Partner A
• Three hours of ECD services are provided per week per household with no cost to caregivers of children.
• Given the resources available, the model is cost-effective as it requires less resources such as infrastructure, and the fact that the ‘Umhambi’ are community based and therefore require no travelling.
• The play group model offered by Partner A is very appropriate for an area of this kind where the majority of parents of the children benefitting from these services are unemployed and therefore would not be able to afford any fee-paying ECD services.
Key challenges • Parental involvement could be improved because parents do not currently attend the playgroups
as intended. • All the children attend the same play group regardless of age and as such, the benefit of age-
appropriate educational equipment is not maximised. • Partner A has no children with disabilities in their programme and they only trained two
caregivers with disabilities.

Partner B Project description Partner B is situated in Harare Township in Khayelitsha, Cape Town. It has an Outreach Programme and uses concrete extensions built around the communal taps to run a fully-fledged ECD service for three hours from Monday to Thursday while parents do their washing at the nearby tap. The programme was established in partnership with the local municipality. The programme is implemented by Family Community Motivators (FCM) and works with children aged nought to six to teach them the same curriculum that would be followed in a formal ECD centre. Children also receive a meal each day. Key characteristics and highlights
• This is the most interestingly innovative approach to an ECD service – a playgroup set-up by the communal taps built by the municipalities, within a community where resources are scarce and unemployment among the parents in the informal settlement is rife.
• The ECD services are provided for three hours per day from Monday to Thursday. On Tuesdays children spend three hours in the toy library situated opposite Partner B’s offices.
• No cost to parents.
Key challenges • ‘The presence of the a playgroup sparked conflicts between Partner B and the ECD Forum
because of its perceived threat to the financial sustainability of the fee-paying ECD centres in the community and this resulted in an agreement with Partner B not to erect any permanent structure’ (in-depth interview respondent, November 2012).
• During bad weather conditions, the playgroup cannot proceed and children have to be kept at home. Partner B is aware of this challenge and is putting plans in place to address it, but is stymied because of the agreement with the ECD Forum.
Partner C Project description Partner C helps ‘self-help’ groups (SHGs) to establish safe parks for their children in Grahamstown, Eastern Cape. SHGs are a concept similar to a township ‘stokvel’, where community groups save money and run a lending scheme to purchase material to start informal businesses that could have potential to grow. From this group, people, mostly women, who are passionate about ECD are selected by the group. Once the selection is complete, a basic assessment is conducted on the abilities, skills and knowledge of this group about child caring and ECD; this is followed by basic training in health, nutrition, and hygiene; basic ECD training: playroom set-up, stimulation activities and so forth. The selected group of women establish a formal ECD centre, referred to as a ‘safe park’. Partner C also works with the Centre for Social Development at the University of Rhodes, to train these practitioners in ECD level 4 training. Key characteristics and highlights
• Partner C works with a total of nine safe parks and provides mentorship, assists them with networking, formal registration with the DSD, and more importantly ensures that they provide an acceptable standard of ECD care.
• The number of children catered for varies from one safe park to the other. • The safe parks run a formal ECD service catering for children from 18 months to six years old.
Key challenges and lessons
• ‘Inclusion of children with disabilities was a critical challenge among the safe parks, with some centres resistant to enrol these children’ (interview respondent, 2012 November).
• In response to this challenge, the Partner C organised a week of practical training in 2012, which will continue in 2013.
• The programme does not include any fundraising skills.

• One key lesson that came out of this evaluation is that the intervention of this type cannot be achieved over a period of a year, and it requires more dedication and passion from the people involved. The capacity building goes beyond facilitating how to run the day-to-day ECD to group dynamics, community engagements, and continuous professional development of the practitioners in the safe parks.
Partner D Project description Partner D runs a fully-fledged mobile ECD centre with toilets and outdoor/indoor facilities to a total of five areas (three informal settlements and two farm areas in Bethlehem, Free State). The toy library has policies displayed on the walls, a daily programme and themes, safety and security measures, and is laid-out to be child-friendly. Partner D has obtained safe, secured and open isolated municipal spaces to park the toy library, where mobile toilets are also installed for that specific day for use by children. Partner D reaches a maximum of 20 children per area through the toy library. Although other ECD centres with stable infrastructures are available in some of these communities, high unemployment levels among these households do not allow them to enrol their children in these fee-paying ECD centres. Key characteristics and highlights
• A ‘toy library’ rotates between the five communities and is only accessible to children one day per week for about three hours; and children get meals.
• Community Motivators are volunteers, trained in ECD practitioner training Level 4 and community facilitation skills, who conduct home stimulation activities with children for the remaining 4 days of the week.
• ‘The Community Motivators address both the educational development and social matters (e.g. identifying children with disabilities and raising awareness to the families about the services available to them and their children; and identifying neglected children and problems that require social workers)’ Partner D manager, November 2012.
• According to caregivers, the toy library has improved children’s perceptual skills – they are able to cut; to sing; and have improved hygiene and tidiness. Moreover, children that have speech disabilities have improved their speech because of the assistance from the physiotherapist (focus group discussions, 2012 November).
• Mainstreaming or inclusion of children with disabilities is facilitated through the specialised skills of Partner D’s board members; a physiotherapist and educational psychologist. Both parents and practitioners have been trained to identify children with disabilities. The physiotherapist has developed a simple guide to stimulation activities to be conducted with children with disabilities.
Key challenges • The parents of children who access the services of the toy library felt that they would prefer to
have the toy library stationed in one community for a full five-day period to ensure that their children get used to a routine of getting up daily and going to an ECD facility.
• It was reported that some children feel anxious when the toy library is absent from their community and tend to follow it to the nearby community if it is within walking distance – this does pose a safety risk (focus-group participant, 2012 November).
Partner E Project description Partner E is dedicated to working with children with hearing disabilities. The approach of the project is to address the developmental needs of these children by providing them with hearing assistive devices and speech therapy that would enable them to hear and speak like any child without hearing loss.

Key characteristics and highlights • It offers a formal ECD service to children with hearing disabilities aged 18 months to seven years,
operating from Monday to Friday. Children are provided with assistive devices and speech therapy to ultimately hear and communicate with others.
• Fees are R1 800 per month, and full scholarships are offered to under-privileged children. • Partner E also has an outreach programme which provides screening services to children at
clinics in townships in and around Tshwane, but this programme is not supported by the Fund. Key challenges and lessons
• The Fund invested in the programme, which mainly targets children from affluent communities; while the Partner E has another programme that reaches out to the communities in the peripheral areas of Pretoria to conduct screening and provide hearing devices to children.
• In future, the Fund could direct its funding towards the outreach programme of the Partner E, which raises awareness about disabilities and conducts diagnoses.
• Although Partner E provides accessible ECD services to children with disabilities, its presence within the Fund’s strategy to mainstream disability is questionable, as it caters specifically for children with disabilities from affluent households.
Partner F Project description FNB has funded centres situated in Craighall and Elsburg, Gauteng. Partner F provides a very good example of inclusion of children with disabilities in a mainstream ECD centre, as it caters for both children with disabilities and children without disabilities at its Craighall site. The inclusion concept from this centre exposes children to differences and inculcates a culture of acceptance and understanding. It offers formal ECD services to both children with disabilities and those without; which includes a grade R class for children who will be able to enrol in the mainstream schools. Key characteristics and highlights
• Partner F caters for children aged from 18 months to seven years old. In cases where children have severe disabilities, they are enrolled up until 10 years.
• A toy library is available for parents to borrow bags of educational toys during school holidays to help continue stimulating the children.
• The cost of ECD services is R1 300 per month, and bursaries are provided to children whose parents cannot afford to pay for the fees.
• Although the staff to children ratio does not meet the current requirement, Partner F has a group of unemployed parents that volunteer at the centre.
Key challenges
• Lack of parental training to enable the continuity of stimulation of children is a limitation and could have serious setbacks in the development of children with disabilities.
• There are staffing challenges reported by Partner F with the current caregiver per child ratio of 1:10 below the legally required one of 1:5. The insufficient staff members issue is crucial and should not be underestimated, especially for a centre that works with children with disabilities and those without, as it operates beyond its capacity and this could result in staff burnout and quality of service being compromised.
• One visit per week from an occupational therapist and physiotherapist is insufficient and the parents indicated that individual child attention is compromised due to time limitation.
Partner G Project description Partner G runs Family Outreach Programme in eight local areas of the Mopani district in Limpopo province. Partner G works with the local headmen in community forums and participates in community

meetings where awareness about the ECD services and challenges facing children is raised. It is from these meetings that parents volunteer to be recruited to implement the Family Outreach Programme. After the recruitment, parents based in these eight areas are trained to provide family outreach ECD services to children who do not access any sort of ECD service. The volunteers are mainly trained in childcare, hygiene, nutrition and basic childhood development skills. The workshop are continuous and even parents of children are encouraged to participate in order to teach them skills that will enable them to continue with childcare in the absence of the outreach volunteers. Once the volunteers complete the training, they are provided with a bag of toys to conduct home visits. Key characteristics and highlights
• Parents from the local communities volunteer and receive training to implement the Family Outreach Programme;
• 20 parents based in the communities were trained in 2011/12 to conduct home visits; • The volunteers conduct home visits with a bag of toys to stimulate children, one day per week.
Over and above, parents are also taught about hygiene, provided with seedlings to start vegetable gardens, and educated on how to use child-grants effectively.
• Approximately 240 children were reached in 2011/12 through the Family Outreach Programme and this has seen some improvement in child enrolment in the centre-based ECDs as a result.
Key challenges
• During ‘marula’ and ‘mopani worms’ pick-up season, very few children participate in the programme, as parents relocate to the farms to pick marula and mopani worms;
• There is high turnover among the volunteers implementing the Family Outreach Programme – and this meant that Partner G has had to conduct continuous training for new volunteers.
• Ideally, each community should have at least seven volunteers, which was not the case. • The volunteers do not receive any stipend and parents are also not expected to pay fees for the
service.
4.2 To what extent have the FNB Fund’s ECD partners improved the quality of the ECD services? The strategy of the FNB Fund to improve the quality of ECD services was to train ECD practitioners, in the belief that if practitioners are well trained and equipped with knowledge and skills to work with children, assuming that the infrastructure and other resources are in place to enhance this knowledge and skill, then the quality of ECD services will improve. To test this hypothesis, we used two methods. First, the evaluation team collected data on practitioner training that was conducted, including training content, duration and qualification levels, so as to confirm that practitioners had received training. Second, a school readiness assessment was conducted with forty-five children aged between five and six years old from seven beneficiary ECD centres. The intention of this assessment was to test the quality of ECD services received by the children from these centres as they are ready to enter primary schooling. The findings on the quality of the ECD services are presented below in the following sequence; first, the number of practitioners that have been trained, the training content, training duration and the qualification level; and second, the school readiness assessment results of the children from the seven beneficiary ECD centres that were assessed.
a) A geographic distribution of ECD project partners in the practitioner training space A total of 13 ECD project partners were implementing ECD practitioner training, mentorship and coaching in the Eastern Cape, Limpopo, Free State, North West, Northern Cape and Western Cape. Figure 3 below illustrates the geographic spread and the number of projects per province. The majority of ECD practitioner training took place in the Eastern Cape, followed by the Western Cape, Mpumalanga, North West, and Limpopo, with the Free State and Northern Cape having the fewest projects.

Figure 4: 2007 to 2011 ECD practitioner training stats
Figure 3: Geographic distribution of the ECD partners providing practitioner training
Similar to the access focus area, the delivery of practitioner training varied. Although the majority of ECD project partners are providing an accredited ECD practitioner training at Level 4, Project J and K are providing unaccredited training, which they feel is necessary as a result of government scrapping all the lower ECD practitioner training qualifications. The ECD project partners implementing practitioner training did so on a staggered timeframe. Seven ECD project partners started their work in 2007, one in 2008, one in 2009, and five in 2010. This is reflected in the statistics of the practitioners that have graduated from Level 4 ECD practitioner training.
b) Were the ECD practitioners trained and to what extent? Monitoring of the ECD programme has evolved over time since the beginning of the programme. ‘After the approval of the ECD programme strategy in 2007, a knowledge sharing workshop was held in 2008 with all the project partners to define the performance indicators that are appropriate to all the partners forreporting purposes. The first report on these performance indicators was received in 2009 and the same indicators were reported on again in 2010. In 2011 ECD project partners provided feedback indicating that the performance indicators are too many and some being irrelevant. A decision to refine the indicators into afew manageable ones and categorise them per focus area’ was subsequently made. (FNB Fund committee pack, 2011:44-45). The Fund has since seen improved data collection efforts that reflect the actual reach of the practitioner training component and the qualification levels of the trained practitioners. Figure 4 illustrates the number of ECD practitioners trained. The majority (1 026) were trained in Level 4, followed by those in Levels 1 and 2 (639); while a few were trained in Levels 5 and 6 (144) – a qualification equivalent to a National Diploma and a Bachelor’s degree respectively. It is clear that skills within the ECD sector have improved and this may yield direct personal benefits to individual

practitioners, as the training and the qualification can open doors to new opportunities. In addition, skilled ECD practitioners will ultimately result in the improvement of classroom practice. This figures illustrate a contribution by the Fund to the practitioner training that improved the quality of the labour force – a sector mainly dominated by unskilled women.
c) Has the quality of ECD services improved, as a result of training ECD practitioners? To determine whether the quality of ECD services has improved as a result of the practitioner training, the evaluation could not rely on counting the number of ECD practitioners trained, but used a proxy indicator – school readiness – to answer this question. The results of the school readiness assessment are discussed in section D of this report. This section reflects on the training models used by the different project partners, and the challenges and strengths of these models. Although the ECD project partners used varied models to implement the ECD practitioner training, a matrix that assesses the effectiveness of each of the project partners that are delivering this service was developed. The intention of this matrix is to identify the effective practitioner training models. The matrix is based on six categories that have a strong influence on the quality of ECD practitioners produced:
• Type of training; • Training model; • Duration of training; • Mentoring and support mechanism; • Innovation; and • Evidence of knowledge application
The matrix consists of indicators and a weighting score across the six categories. These categories are scored with ratings ranging from 1 to 4 or from 0 to 3 in other instances. A mean value from the six categories is then calculated, which then determines the effectiveness of each ECD partner overall. The mean value across the six categories is 3.3. The projects were categorised as either highly effective, moderately effective, or ineffective depending on their mean value. The description of these values and categorisation is as follows:
• ECD partners with a mean score ranging from 3.3 to 2.6 across all the six categories are classified as highly effective, represented by a green robot;
• The ECD partners with a mean score ranging from 2.5 to 2.1 across all the six categories are classified as moderately effective, represented by an orage robot; while
• The ECD partners with a mean score below 2 across all the six categories are classified ineffective, represented by a red robot.
The effective ECD project partners are those that could also be referred to as ‘centres of excellence’ –they do extraordinary things beyond just delivering practitioner training content. While those that are regarded as moderately effective are still able to honour their grant contract with the Fund by training practitioners, no extraordinary activities are implemented. However, these partners do have pockets of excellence in certain components of the practitioner training but still have room for improvement in other areas. The ECD partners that are ineffective have several areas that require improvement across most of the areas being rated. These partners would require serious attention to improve their services in order to add more value to the beneficiary ECD centres that they serve. Table 2 illustrates that the Fund had a total of seven ECD partners that fall within the category of centres of excellence, three moderately effective ECD partners, and three ineffective partners. Some ECD partners, for example, have the advantage of infrastructure where they are able to have demonstration and modelling playrooms as part of the training. All the seven centres have introduced some innovation, such as hosting awards ceremonies.

In addition, they equip ECD practitioners with skills to make educational equipment from waste material and have rallied local companies to provide them with waste material and in return they distribute the waste to the beneficiary ECD centres to continue making the equipment. They have also developed ECD practitioner training manuals based on the context of their communities and thought leadership within their sector. The innovative nature of these centres has also been witnessed in the beneficiary ECD centres that were visited during the evaluation. They all reflect strong examples of good ECD practice. It is noteworthy that some project partners might have been disadvantaged in their assessment into these categories, as they are new to the programme and as such the evaluation only covered one complete year of their work. The assumption is that with time, these partners might have done better,as they have proposed to work with the same cohort of beneficiary ECD centres over the funding period. Some factors that the evaluation team found to have a critical influence on the quality of ECD services, over and above the ECD practitioners being trained and qualified, were the socio-economic status of families of the children, poor or lack of infrastructure, and lack of furnishings, sanitation, water and electricity. These are the factors that are beyond the control of the ECD project partners funded by the Fund, and yet they ultimately help to determine the quality of ECD services children receive. In cases where the lack of funds (i.e. no subsidy from DSD, and non-payment of fees by parents) persisted, some of the practitioners closed doors and left to find employment elsewhere using the qualification they had acquired. Even in the ECD centres where some basic resources and infrastructure existed, poverty proved to have the potential to undermine the gains that children make during the period they spent in the ECD centre. Malnutrition, which has a direct link to poverty, has been reported by the practitioners to be rife among their children. According to one ECD practitioner (November 2012 interview) during the school year children would have a normal weight as they get daily meals from the ECD; however, the children come back from school holidays having lost weight – this has an implication for children’s developmental growth. Observed evidence from the highly effective ECD project partners Of the beneficiary ECD centres that were observed during evaluation visits, the following could be pointed to as key success areas:
• Daily programme and theme-based activities are in place in most of the beneficiary centres; • Policy guidelines are in place; • Playrooms are child-friendly; • Educational equipment is made from waste material, which enhances the development of
numeracy and language (and saves costs); and • Assessment portfolios of children are kept
Observed evidence from the moderately effective ECD project partners:
• No innovation is introduced on training methods; and • Although some have intense support systems, they still provide short courses. Evidence of
knowledge application from the beneficiary ECD centres was very limited when compared to expected standards.
Observed evidence from ineffective ECD project partners:
• Some ECD project partners do not have adequate mentoring and aftercare support for the practitioners once they leave the training;
• Some project partners that run a further education and training (FET) model while some provide training even to practitioners who do not work in an ECD centre, and as such do not have any place to practice what they have learnt; this disadvantages them, particularly when the quality of practice is assessed.

• In light of financial sustainability, although some project partners have intense mentoring and support, their lack of innovation to teach practitioners about making educational toys is a challenge, as they rely only on purchased equipment.

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand
Foundation and should be treated as such.
Table 2: Effectiveness matrix for ECD practitioner training models What are the conditions that enhance or hamper the quality of ECD services? As noted in the previous section, we have found that irrespective of whether the beneficiary ECD practitioner has been trained through an accredited or non-accredited ECD training, the challenges that determine the successful application of their skills were similar.
These challenges can be summarised as follows:
1. High levels of poverty and unemployment have a direct impact on the quality of ECD services, as parents cannot afford to contribute towards the running cost of the ECD centres.
2. Lack of and poor infrastructure sanitation, water and lights. First, this is a barrier to successful registration and eligibility for accessing subsidies from the DSD. Second, children are not able to perform activities that develop them optimally to achieve expected developmental outcomes. For example, children are cramped into one playroom, which influences the age-appropriate activities that should be done with these children; or they do not have adequate space to practice activities that improve their perceptual skills, such as colouring, drawing and cutting.
3. Without the financial contribution of parents and subsidy from DSD, practitioners opt to look for ‘greener pastures’ as they do not receive any remuneration. 4. Point 1 and 2 greatly affect the ability of practitioners to deliver a quality service
Project Type of training
Training model
Training duration
Mentoring and support Innovation Evidence of
application Total score
1 Project A 3 3 4 2 3 4 3.17 2 Project B 3 3 4 2 3 3 3.00 3 Project C
3 3 3 2 3 4 3.00
4 Project D 3 2 4 3 2 4 3.00 5 Project E 3 2 4 3 2 4 3.00 6 Project F 3 2 4 2 2.3 3 2.72 7 Project G 3 2 4 2 2 3 2.67 8 Project H 3 2.5 4 1 2 2.5 2.50 9 Project I 3 2 3 2.6 0 2.3 2.15
10 Project J 3 2 2 2 0 3 2.00 11 Project K 2 2 2 3 0 2.5 1.92 12 Project L 3 1.5 3 1 0 1 1.58 13 Project M 2 1 4 0 0 1.5 1.42

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
Mainstreaming or inclusion of children with disabilities within the practitioner training component
• Mainstreaming or inclusion of children with disabilities proved to be a challenge in most beneficiary ECD centres. The ECD practitioner NQF Level 4 training does not have sufficient detail to help prepare the ECD practitioners to work practically with children with disabilities. The content of the NQF Level 4 training is limited to information about the rights and admission policies that will ensure that these children are not discriminated against. Other than this, actual inclusion in practice is left up to the ECD project partners to capacitate ECD practitioners.
• Although there were efforts from ECD project partners to work with children with disabilities within their own ECD centre (that is not funded by the Fund), the practitioners from the beneficiary ECD centres indicated a great need for practical training that will enable them to identify children with disabilities and identify appropriate stimulation activities. Similar challenges were echoed by other partners that without the specialised skills of a physiotherapist it is not easy to diagnose whether a child has a disability, and therefore to design the activities that will benefit this category of children.
• The ECD centres are not wheelchair friendly.
d) How school ready are the children when leaving the ECD centres? One piece of legislation that has critical implications and the potential to undermine school readiness assessments is the South African Schools Act, section 5, as amended, 2002. The admission age policy as stated in the Act compels learners to be in grade 1 by the year they turn seven. However, the policy permits learners that are age five turning six by 30 June in the year of admission, to be admitted to grade 1. Accordingly, practitioners cannot hold back children that they feel have not yet demonstrated or achieved their age-appropriate developmental outcomes. Although the intention of this legislation is good, in the current education system, where there is no integration or collaboration between the Foundation phase and grade R community-based centres, learners who require support fall through the cracks because of lack of continuity and communication between their previous teachers and the current ones. Although school-readiness assessments have been criticised for their biases towards western cultures, they still provide some basic data from which to identify learning development gaps in the auditory, emotional, perceptual and cognitive abilities of children. Furthermore, the recently revised school readiness assessment, released in 2012, was adapted to the South African context to consider cultural issues. The remaining debates are more moral than content-based, where the argument is that children should not be tested based on a standardised tests because their conditions and the quality of ECD services they receive is varied. This argument is unfortunate because tests such as the Annual National Assessments (ANA) and the National Senior Certificate (NCS) use the standardised tests irrespective of the conditions of the schools and socio-economic status of the families of these children. For this evaluation, the educational psychologist worked very closely with ECD practitioners from the beneficiary ECD centres on the interpretations of exercises to eliminate the influence of English language barriers on the performance of children on these assessments. The evaluation revealed the following: School readiness assessment results Early childhood is the most rapid developmental stage in a child’s life. Children develop at their own individual pace physically, cognitively, emotionally, and socially. The ability of children to develop and learn can, however, be improved through stimulation programmes, focusing on various skills in order to prepare them to advance to grade R.

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
Seven ECD centres were visited and an average group of five children aged between five and six years old were selected for school readiness assessments per centre. The school readiness assessments were conducted by a qualified educational psychologist using the Optima School Readiness Assessment tool. The assessments were based on the following categories:
i. Visual perception ii. Auditory perception iii. Spatial/number concept iv. Social and emotional development v. Gross and fine motor coordination
Description of categories
i. Visual perception Visual perception is not only the ability to see, but is also the ability of the brain to interpret visual stimuli. The following aspects constitute visual perception:
• Visual discrimination – ability of the child to identify and interpret similarities and differences in visual images.
• Perception of geometric shapes • Foreground/background perception – ability to identify important detail based on contrast and
competing visual information such as known objects, shapes and colours against a different background.
• Gestalt perception – ability to see an object whose parts are in dynamic interrelation with each other and forms a whole or a unit.
• Visual memory – ability of the child to recall /remember visual images perceived on a short term and long term basis.
ii. Auditory perception Auditory perception is the ability of the child to make contact with the world of sound and to make sense of what the ears hear. The following aspects constitute auditory perception:
• Auditory discrimination – ability of the child to identify and interpret similarities and differences in sounds.
• Intense listening – ability to focus on a specific sound or word; • Auditory foreground/background perception – ability of the child to listen and concentrate on
the teacher’s instructions, directions, requests or communication despite of other environmental noises and disturbances;
• Auditory analysis – ability of the child to identify smaller sounds or parts in a word. • Picture riddles – ability of the child to interpret more complex information and sentences.
iii. Spatial orientation and number concept
Spatial orientation is the relation of the child with an object in space and the physical surroundings. The following aspects were assessed:
• Sense of direction – ability to perceive and identify direction and spatial orientation. • Laterality – awareness and ability of the child to identify the right and left sides of the body. • Midline crossing – the midline is an imaginary line that separates the body in half vertically,
thus dividing the body in two halves. Crossing the midline is the child’s ability to move a part of the body (e.g. right hand touching left foot) into the space of the other part of the body.
• Number concept – refers to the knowledge of the names of numbers, being able to count objects and identifying the difference between groups with a different number of objects;
• Number concept – represents a knowledge of quantities and proportions such as equal, less-than and greater-than and leads to a better understanding of the child’s surroundings.
iv. Social-emotional development This refers to the child’s development and awareness of their sense of self and being of an individual

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
person. This includes the understanding of their own emotions and feelings which also include the people around them.
v. Motor coordination • Gross motor coordination involves the larger muscles in the body, including the arms and the
legs. Movements that require gross motor coordination include walking, running skipping and many others. These movements require strength, muscle tone, postural control, balance, movement quality and range of movement.
• Fine motor coordination involves the smaller muscles of the body such as the toes and fingers in coordination with the eyes. Dexterity in movement is of importance when drawing lines in a confined space such as mazes and writing patterns which prepares the child for writing.
In order to determine whether or not the children were ready for school, they were qualitatively assessed in all the five categories (Table 2). Each category has a maximum score of one. In order to be considered ‘ready for school’, the children were required to achieve the maximum score of five across all the categories. Table 2: Scoring of school readiness categories
Category Assessed aspects Maximum score Description
Visual perception
• Visual discrimination • Perception of geometric shapes • Foreground/background
perception • Gestalt perception. • Visual memory
1
Each of the five aspects has a proportional score of 0.2 or 1/5.
Auditory perception
• Auditory discrimination • Auditory
foreground/background perception
• Auditory analysis • Picture riddles
1
Each of the four aspects has a proportional score of 0.25 or 1/4.
Spatial orientation and number concept
• Sense of direction • Laterality • Midline crossing • Number concept
1
Each of the four aspects has a proportional score of 0.25 or 1/4.
Social-emotional development
• Self-awareness 1
Motor coordination • Gross motor • Fine motor 1
Each of the two aspects has a proportional score of 0.5 or 1/2.
Based on the scoring:
• The ECD partners with an overall score above 3 have children that are generally ready for school and are highlighted in green;
• The ECD partners with an overall score below 3 have children who are generally not yet ready for school and are highlighted in red; and
• The red flags within each category indicate where performance by the children was very poor and requires urgent attention.

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the
FirstRand Foundation and should be treated as such.
The assessment indicated that the basic visual and auditory perception of the assessed children was generally satisfactory (see Table 3 below). The social and emotional maturation of the assessed children was satisfactory. However, the assessment indicated that more advanced visual and auditory perception, visual-motor integration and fine motor coordination skills require attention.
Table 3: School readiness assessment results Coordinating organisation
ECD centre Number of children
assessed
Visual perceptio
n
Auditory perception
Spatial/number concept
Social/emotional
development
Fine motor skills
Overall score
Organisation A
Pre-school A 5 0.6 0.5 0.5
1 0
2.6
Pre-school B 5 0.6 0.75 1 1
0 3.35
Organisation B Pre-school C 10 0.6 0.75 1 1 0
3.35
Organisation C Pre-school D 5 0.4
1 0.25
1 0
2.65
Organisation D Pre-school E 7 0.8 0.75 0.75 1 0
3.3
Organisation E Pre-school F 6 0.2
1 0.25
1 0
2.45
Organisation F Pre-school G 7 0.8 1 0.75 1 0
3.55

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
Based on the scores in Table 3, none of the ECD centres have children who are ready in all the assessed categories. However, Pre-school B, C, E and F attained encouraging scores. Children at Pre-school A, D and G require a lot of attention to be school ready. The poor performance of the children could be attributed to many factors, including the large number of children per centre, which makes it difficult for practitioners to give the children the necessary attention. Some of the centres do not have appropriate space, play surfaces, equipment or play materials to develop the various maturation and developmental skills necessary to prepare them for school. Most of the centres lack adequate financial resources to improve their play and learning environments for the benefit of the children. 4.3 To what extent has the Fund supported the mentoring and transfer of skills between established and emerging ECD centres? The capacity building and mentoring of emerging ECD centres was a strategic objective of the ECD programme since inception, but funding was only set aside for this objective in 2009. An amount of R1 000 000 was allocated towards capacity building in 2007. The purpose for this strategic objective was to provide training and support to emerging ECD centres on accessing grants and resources from different stakeholders. The motivation for this focus area was stated as follows: ‘this section is specifically geared towards building capacity of emerging organisations. However, it does so in a risk averse and developmentally informed way by suggesting that existing, established ECD centres be funded to provide mentorship to other smaller ECD centres in their vicinities. The idea is to support existing initiatives where organisations are ’trying to help’ emerging groups but find it difficult as it strains their resources. Grants in this category would be made to the established ECD centres on receipt of their proposals of how they believe they could add capacity and transfer skills to emerging ones.’ (FNB Fund pack, June 2007) As noted above, the capacity building and mentoring of emerging ECD centres was a strategic objective of the programme from the outset, but the objective was only implemented in 2011 when the Fund approved funding to for a pilot programme for capacity building and mentoring. A partner received a multi-year grant in 2010 towards training of practitioners and parents, skills development of governing body members, provision of educational equipment, monitoring and evaluation, and assistance with the registration of ECD centres in Gugulethu. However, this grant was not classified as capacity building and mentoring, but should have been, as its work is exactly what the Fund wanted to achieve with this objective. A slight shift of the objective was noted; instead of funding established ECD organisations to mentor emerging ones, the Fund provided funding to NPOs to capacitate the emerging ECD centres. Currently, the FNB Fund supports these two organisations, focusing on capacity building and mentoring for emerging ECD centres in the community. Below, we discuss the capacity building models employed by these ECD centres, the duration of support, the actual outcomes achieved thus far, challenges, and lessons. Capacity building model Although both organisations are working in the same field with the same expected outcomes, they have different approaches to their capacity building interventions. The anticipated outcome for the capacity building intervention is to have ECD centres registered with the relevant government departments, which will ultimately enable these centres to apply for a subsidy. Project N capacity building model Project N has designed a capacity building model that responds to the needs of the community in relation to ECD. The programme is not accredited, but it addresses the basic needs of the emerging ECD centre. Project N works in partnership with the DSD with the intention of getting the centres to comply with legislation and successfully complete the registration process (as such, the DSD registration checklist is used as one of the success indicators).

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
The FNB Fund has supported the implementation of Project N’s programme in KwaThema, supporting 20 ECD centres in the area. The programme offers training, on-site support and mentoring, and provision of educational equipment. The programme spans a period of 3–5 years depending on the availability of funds. The programme is packaged as shown in Table 4 below. The first year is dedicated to relationship building with critical stakeholders and the assessment of the ECD centres to determine needs and prioritise. The second year of capacity building involves training and in-service support of these emerging ECD centres. The training consists of four modules and targets ECD centre principals specifically. The third year is committed to mentoring and support of the centres and addresses registration of centres with the DSD as places of partial care. To date, Project N has completed the training of all four modules of four to five days a week each, and all the ECD centres have policies in place, meeting the minimum requirements of standard of care and in the process of registration. Although there are very few emerging ECD centres that have finalised their registration, and it does not seem like all 20 centres will be able to do so at the end of the third year, there seems to be evidence that the model works well in helping emerging ECD centres to provide a quality service. This was evident when we visited Padisong ECD centre in KwaThema. The centre is running in a backyard with very limited space. Based on the feedback and the record that was seen, the centre had never seen the value of developing policy and keeping records for finances, children and staff. It was only after the training that the principal started keeping records and filing things properly. Although the policies are still outstanding, she now has an idea of what is needed and there is commitment to start working on the policies in 2013. Table 4: Capacity building package of the Project N Trust
Year 1 (2010) Year 2 (2011) Year 3 (2012) Building relationship with different stakeholders including the ECD forum in the area and DSD, municipality and clinics. Conduct an assessment for each ECD centre to determine individual centre needs. The assessment also covers educational profile of the staff in the ECD centres, the environment and resources.
Training and in-service support of the principals of ECD centres; and three site support visits after each training module. Module 1: Duration of three days on the basic set-up of the playrooms Module 2: Duration of four days on policies required in the ECD centre Module 3: Duration of four days on role clarity between the board of directors, executive management and staff. Module 4: Duration of three days on planning, Ad hoc trainings are also provided and range from Acts relevant to the sector, disability and ECD, and new developments in the sector.
Support and mentoring to ensure that the ECD centre is registered and meets all the standards of providing quality service to children Project N Trust also selects ECD practitioners that are referred to organisations that provide ECD practitioner training Level 4.
Key highlights After visiting two of the centres that are part of the CARE training, it is concluded that the training is designed at the level of the participants and it is on the right track to achieve its objectives. None of the participants have formal or accredited practitioner training, but their centres are providing services that are in line with the ECD legislation. This is a clear sign that the model works. The organisation is able to create an opportunity for further learning for those who are able to achieve more than what they offer. From last year’s group, Project N Trust has selected eight practitioners who have matric and referred them to enrol in the ECD practitioner training Level 4. Having an Project N Trust
The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
field worker based in the community was stated as an advantage for the ECD centres that participate in the capacity building programme because of easy access to advice and support. Key challenges The biggest obstacle with most non-compliant ECD centres that affects their registration is infrastructure. For example, most centres cannot afford to build separate ablution facilities for boys and girls, as required. This requirement is a major one standing on the way of most emerging ECD centres to register as a place of care and apply for the care subsidy with the DSD. Another challenge, raised by one of the practitioners interviewed was that the generation gap between the training participants is problematic: ‘the training pace is slow to accommodate the elders and it becomes cumbersome for the youngsters’ (interview respondent, November 2012). Lessons learned
• The community-based model of capacity building works well, as it tends to focus on the needs of the particular community; and
• Mentoring and support is a very important component that leads to the success of the programme
Project O Project O is contracted to provide holistic services to ECD centres, and this includes training of practitioners and parents; skills development of governing body members; provision of educational equipment; monitoring and evaluation; and assistance with the registration of ECD centres in Gugulethu, Western Cape. The training for ECD principals and their governing bodies was discussed during the evaluation. The organisation reported that during the first year of funding, the grant was used for practitioner training, but the training was stopped when the department of basic education set up ECD training centres in the Western Cape. However, there was no clear communication from Project O informing the Fund about their decision to discontinue practitioner training. In fact, the report submitted by Project O in July 2012 reported that 249 practitioners and 842 parents were trained. Similar contradictory information was conveyed during the evaluation visit, as the information that was shared by Project O staff in the interviews could not be confirmed by the beneficiary ECD centres’ principals. The organisation has reported that funding from the Fund is supporting 30 ECD centres per annum in Gugulethu. Accordingly, the emerging ECD centres were selected in partnership with the DSD. Project O reported that it approached the DSD with a proposal to capacitate unregistered ECD centres. This is a new programme that replaced the discontinued practitioner training funded by the Fund. The programme is designed to run for a year, which means that within a three-year funding period, Project O would have capacitated a total of 90 unregistered ECD centres in Gugulethu. The organisation has reported that almost 15 out of 60 emerging ECD centres have completed the registration with the DSD, whereas the project reports provide contradicting statistics of nine out 45 ECD centres that completed the registration, and only five centres that are receiving a subsidy. Although there is no clearly articulated capacity building model, the capacity building programme is designed to provide training for the ECD centres’ principals and their governing bodies (which includes everyone in the committee). Project O provides four Saturday trainings that cover the following topics:
• Financial management; • Governance; • HR management; and • Leadership

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
Project O reported that when funding has a provision of equipment, it does provide two days of training on the use of equipment. It was also reported that support visits are implemented to observe how the learning is applied in the centres and that these visits normally lasts for two hours per centre. As indicated above, there have been mixed messages on what exactly was offered to the centres in terms of training, as the two centres that were visited by the evaluation team could not provide sufficient evidence. The visit to an ECD, which has been reported as one of the successful ECD centres in the programme, revealed that the staff has attended three workshops focusing on fundraising, governance and policy development. During those workshops, only one board member attended fundraising and governance training. The principal indicated that she had an invitation for two representatives but that the other one could not make it. The ECD centre appears to be a well-managed ECD centre, but it is not possible to tell if the success is owed to Project O or to the fact that the principal has level 4 training. At the second centre, the principal indicated that on the three occasions that she attended training the chairman, treasurer and secretary of the board were present. However, the ECD centre could not produce any records to prove that they have implemented what they have learned from the capacity building training. The only thing that could be seen was a policy document displayed on the wall. Key challenges The duration of training workshops and the on-site support provided will need to be reviewed if Project O is serious about getting participating ECD centres to a level where they could provide quality ECD services to children. Currently, the workshops span one day, which is followed by a two-hour visit. Given the inefficiency of the DSD, the level of support provided by Project O to these ECD centres is unlikely to help them achieve registration and subsidisation. 4. Concluding summary and recommendation 4.1 Concluding summary Access to early childhood development services Increasing accessibility of ECD services to children in South Africa remains a critical challenge. The majority of children from poor households, informal settlements and farming areas are still without access to these services. This may be due to the fact that there are no ECD centres in their vicinity, or that households cannot afford to pay the fees. High unemployment rates and inward-migrations from the periphery to cities are some of the factors for continued lack of access to ECD services. Moreover, there is a shortage of public ECD centres to allow for universal access to these services. Despite these challenges, corporate funding has ensured the access of ECD services to an increasing numbers of children – children who would have no exposure to ECD services without the funding. The ECD project partners have delivered ECD services to children, although with varying degrees of quality and frequency. In order to respond to a dichotomy of scarce resources and lack of access of ECD services to children, ECD project partners have designed innovative mechanisms of delivery, such as mobile libraries, training community motivators, family outreach programme, and using spaces surrounding communal taps to ensure that children have access to ECD services. These efforts, without doubt, should be applauded for using assets in these communities and contextualising their service offering to respond to local needs. Practitioner training The Fund has contributed towards the professional development of the ECD sector through practitioner training. There has been an increase in the number of practitioners that have received the ECD

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
practitioner training over the years in NQF levels 1 to 6, and this has changed the face of the sector, mainly dominated by unskilled women. The findings of this evaluation have revealed that while the Fund’s ECD project partners have been effective in delivering ECD practitioner training, with some ‘going the extra mile’ in relation to programme implementation, training has not universally translated into ‘school ready children’, at least from the ECD partners that participated in the school readiness assessment. While the training of practitioners is not the only piece of the puzzle to improve school readiness of children, there were some issues that have the potential to influence classroom practice, given the varying methods of how the ECD practitioner training is delivered. School readiness assessments The poor performance of the children on the school readiness assessment could be attributed to the following factors:
• High numbers of children per centre which make it difficult for practitioners to give the children necessary attention.
• Some of the centres do not have the appropriate space, play surfaces, equipment or play material to develop the various maturation and developmental skills necessary to prepare them for school.
• In some of the centres, practitioners with lower than NQF level 4 qualification are teaching grade R classes.
• Most of the centres particularly lack adequate financial resources to improve play and learning environments for the benefit of the children.
Capacity building Capacity building of emerging ECD centres has been one of the strategic objectives of the Fund since 2007. However, when the evaluation tracked implementation, it revealed that the actual implementation of this strategic component only started in 2012, when funding towards Project N Trust was approved. This suggests a need to improve the management and monitoring of strategy implementation. Project N Trust was found to be implementing a more intensive and successful support programme than PROJECT O, which offers very limited on-site support. Mainstreaming or inclusion of children with disabilities To date, mainstreaming of disability within the programme has consisted of making grants to organisations that work specifically with children with disabilities. Little has been done to encourage or support the inclusion of children with disabilities, with the exception of funding towards a disability inclusion workshop that was approved by the Fund in September 2012 (outside of the period covered by this evaluation). However, the majority of ECD project partners have reported that they require support in ensuring that the inclusion of children with disability becomes a reality. 4.2 Recommendations Given the multi-faceted challenges of the ECD sector that affect access to and improved quality of ECD services, the Fund should consider an integrated approach to ECD. This approach will ensure that the Fund is able to address the multiple challenges of access and quality of ECD services for the children. The following option could be explored in trying to provide an integrated approach to ECD:
• Fund projects that provide a series of service package that increase or expand access to ECD services, train practitioners, and capacitate the ECD centres that require assistance to comply with legislative requirements;
Further recommendations on the focus areas that were evaluated are as follows:

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
Access: • A clear definition of what access is and its standards should be developed – this will assist to
develop a criteria for selecting partner organisations; and • The expansion of access should be channelled towards children that come from disadvantaged
households who do not afford to pay for ECD services. Practitioner training
• Clearly defined minimum guidelines for mentoring and support should be developed; • Support only the accredited practitioner training; and • The curriculum of the ECD practitioner training should cover school readiness to enable
practitioners to prepare children to be ready for school. Capacity building
• A clear definition of what capacity building entails should be developed; • Clearly defined outcomes of capacity building intervention should be developed; and • Clearly defined guidelines should be developed for the NGO partners implementing capacity on
the selection of the beneficiary ECD centres that have the potential to achieve the outcomes of capacity building.
Mainstreaming disability • Mainstreaming disability should be a cross-cutting area of the Fund’s focus areas; and • Explore ways to continue the momentum on the activities already implemented in the ECD
Programme, such as the training of the trainers on inclusion of people with disabilities, and expand them to other levels of the ECD centres.
School readiness indicators The following indicators are proposed in order to assist the Fund to track school readiness of children participating in its programme:
Category Indicator
Visual perception
• % of children recognising basic shapes • % of children who can recognise and name colours of objects • % of children able to recall visual images perceived on a short-term and long-term
basis
Auditory perception • % of children almost always recognising the relationships between letters and
sounds • % of children with the ability to listen to and carry out instructions independently
Spatial orientation and number concept
• % of children who can count and use numbers to describe and compare • % of children who can make comparisons based on length, weight, and size of
objects • % of children who can use objects in play, experimenting with materials, building
blocks and puzzles
Social-emotional development
• % of children who often or very often exhibit positive social behaviors when interacting with their peers
• % of children able to play and take turns in cooperative activities with their peers • % of children who can speak, understand language and are able to express
themselves • % of children who can name their body parts spontaneously • % of children with the ability to concentrate and focus on tasks
Motor coordination
• % of children who can hold and control a pencil and cut with a scissors • % of children who can draw a line between parallel lines • % of children who can bounce or catch a ball • % of children who can run, jump or climb with good balance

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand Foundation and should be treated as such.
List of references
1. Department of Education, 2001 ‘Education White paper 5 on Early Childhood Education’, Department Education South Africa
2. UNICEF & World Health Organisation, 2012 ‘Early Childhood Development and disability discussion paper’, World Health Organisation
3. Department of Social Development, 2006 ‘Guideline for Early Childhood Services’, Department of Social Development South Africa
4. Laurie M. Anderson, PhD, MPH, Carolynne Shinn, MS, Mindy T. Fullilove, MD, Susan C. Scrimshaw, PhD, Jonathan E. Fielding, MD, MPH, MBA, Jacques Normand, PhD, Vilma G. Carande-Kulis, PhD, MS, and the Task Force on Community Preventive Services, 2003 ‘The Effectiveness of Early Childhood Development Programs, Headstart’, American Journal of Preventive Medicine
5. Kristin Neudorf, Tonya R. Thurman, & Tory M. Taylor, 2011 ‘A case study of Interventions Promoting Early Childhood Development in South Africa’, Tulani University
6. Andrew Dawes,Linda Biersteker and Lynn Hendricks, 2012, ‘Towards integrated Early Childhood Development, ‘An evaluation of the Sobambisana Initiative’, Ilifa Labantwana, Cape Town, South Africa

The above information as set out in papers prepared for the Trustees of the FirstRand Foundation and FirstRand Trust by Tshikululu Social Investments is confidential internal property of the FirstRand
Foundation and should be treated as such.
Annexure A: ECD practitioner training effectiveness matrix Categories Indicators Weight Type of training Unstructured and informal 1 Structured and informal or accredited with no clear assessment standards in place 2 Structured and informal with assessment standards in place 3 Accredited with assessment standards in place 3 Training model Theory based with no practice 1 Mixed methods: theory and practice integrated 2 Training, practice and coupled with playroom demonstration and modelling 3 Duration Short courses spanning few days 1 Short courses spanning 1 to 3 months 2 A structured course spanning 12 to 14 months 3 A structured course spanning 18 to 24 months 4 Mentoring and support No mentoring and support 0 Mentoring and support exist but limited to 1 to 3 on-site support visits 1 Mentoring and support exist but limited to 4 to 5 on-site support visits 2 Intensive mentoring and support (above 5 on-site support visits) 3
Innovation The training model relies on traditional reliance on provision of equipment or no there is no reference to the use of current assets to supplement the resources 0
The training model provides theory of how the assets in the surroundings can be used to complement the learning 1
The training model equip the practitioners to make educational equipment from waste material - available resources in their surrounding; contextualise the service to the community 2
A combination of asset based model; competitions and awards for the best practice ECDs; publish training manual 3
Evidence of application The knowledge and skills not applied to standard 1 There is evidence of application of the knowledge and skills by practitioners but to a limited extent 2 There is evidence of the application of the skills and knowledge without innovation 3 There is evidence of the application of the skills and knowledge with innovation 4 Average weighting