early indicators of autism spectrum disorders donald oswald, phd professor, department of psychiatry...
TRANSCRIPT

Early Indicators of Autism Spectrum Disorders
Donald Oswald, PhDProfessor, Department of PsychiatryVirginia Commonwealth University

Autistic Disorder – DSM-IV• Key Characteristics:
– Qualitative impairment in social interaction– Qualitative impairment in communication– Restricted repetitive and stereotyped
patterns of behavior, interests, and activities– Differences present prior to three years

Multisystem Developmental Disorder – DC:0-3R• Can be applied to children under two years of
age• Features are descriptive, not criterion-based• Does not require the range of relationship and
communication difficulties seen in Autistic Disorder
• Used as alternative to PDD-NOS in children under two years
» ZERO TO THREE. (2005). Diagnostic classification of mental health and developmental disorders of infancy and early childhood: Revised edition (DC:0-3R). Washington, DC: ZERO TO THREE Press.

Multisystem Developmental Disorder – DC:0-3R• Significant impairment in the ability to engage
in an emotional and social relationship with a primary caregiver (e.g., the child may appear avoidant or aimless but may evidence subtle, emergent forms of relating or relate quite warmly intermittently).
• Significant impairment in forming, maintaining, and/or developing preverbal gestural communication or verbal and nonverbal symbolic communication

Multisystem Developmental Disorder – DC:0-3R• Significant dysfunction in the processing
of visual, auditory, tactile, proprioceptive, and vestibular sensations, including hyperreactivity and hyporeactivity to sensory input.
• Significant dysfunction in motor planning (sequencing movements).

Etiology
• ASDs are – Biologically based neurodevelopmental
disorders– Highly heritable (recurrence risk is about 5 -
6 percent when there is an older sibling with an ASD)
– Not caused by emotionally distant parenting

Etiology
– Sometimes associated with a medical condition or known syndrome
• Fragile X• Tuberous Sclerosis• Phenylketonuria• Fetal alcohol syndrome• Angelman syndrome• Rett syndrome

Prevalence
• “. . . the best estimate of current prevalence of ASDs in Europe and North America is approximately 6 per 1000”
» Johnson et al., 2007
• Prevalence by type:– Autistic Disorder - 2.2 per 1000– Asperger’s Disorder - 1.0 per 1000– PDD-NOS - 3.3 per 1000
» Fombonne et al., 2006

Age at identification
• “the age at which a child was first identified by a health, education, or other community service provider as having an ASD. . .”– a clinical diagnosis noted in an abstracted
evaluation– eligibility for special education services under an
ASD category– an International Classification of Diseases, 9th
Edition, code for an ASD » Shattuck, P.T. et al., (2009). Timing of identification
among children with an autism spectrum disorder: Findings from a population-based surveillance study. Journal of the American Academy of Child and Adolescent Psychiatry, 48, 474-483
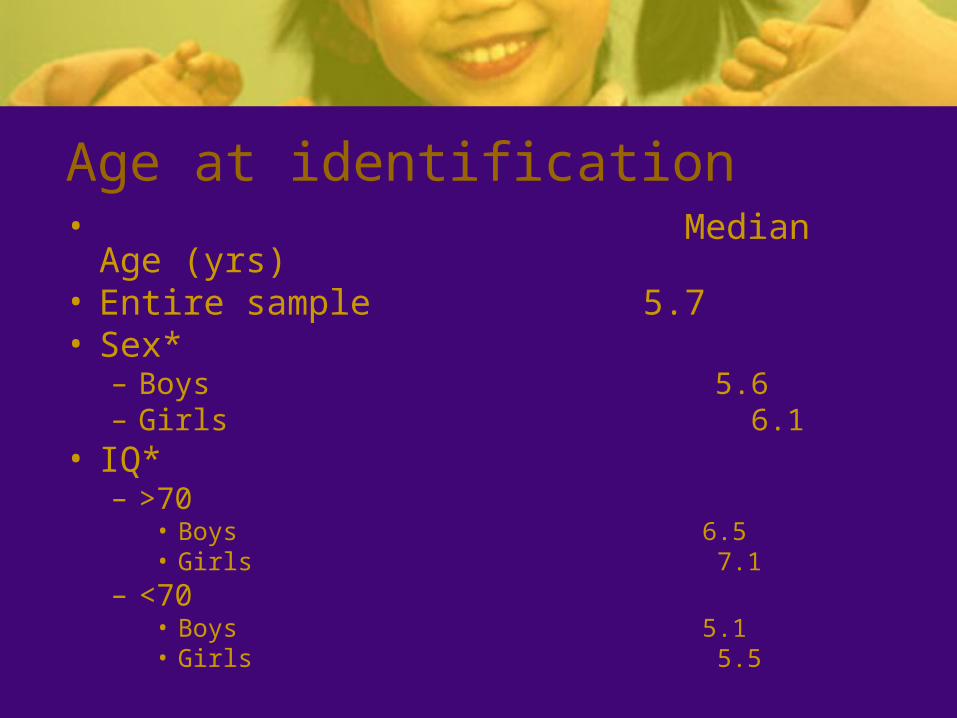
Age at identification• Median Age (yrs)• Entire sample 5.7• Sex*
– Boys 5.6– Girls 6.1
• IQ*– >70
• Boys 6.5• Girls 7.1
– <70• Boys 5.1• Girls 5.5

Developmental Screening
• Further evaluation is warranted if:– Does not babble or coo by 12 months– Does not gesture (point, wave, grasp) by 12
months– Does not say single words by 16 months– Does not say two-word phrases on his or her
own by 24 months– Has any loss of any language or social skill at
any age.– National Institute of Child Health and Human
Development (NICHD)

Screening and Early Identification• AAP Recommended Surveillance and
Screening Algorithm– Evaluate risk factors:
• Is there a sibling with autism spectrum disorders?• Are parents concerned?• Are other caregivers concerned?• Is physician concerned?
– If at least two risk factors present and child is at least 18 months old, administer ASD specific screening tool.
» Johnson et al., 2007

Screening and Early Identification• AAP Recommended Surveillance and
Screening Algorithm– Regardless of risk factors, administer ASD
specific screening tool at both the 18 month and 24 month visits.
» Johnson et al., 2007

Screening Instruments for ASD• Modified Checklist for Autism in Toddlers
• Social Communication Questionnaire
• These are parent-report instruments for screening purposes only (not diagnosis)

Modified Checklist for Autism in Toddlers (M-CHAT)
• M-CHAT – Expanded American version of the original CHAT– 23 questions using the original nine from the CHAT as its basis. – Goal: to improve the sensitivity of the CHAT and position it better
for an American audience.• Appropriate for children 18 - 24 months of age• Yes/no answers convert to pass/fail responses.• Child fails the checklist
– when 2 or more critical items are failed – OR when any three items are failed.
• Available at www.firstsigns.org/
Robins, D., Fein, D., Barton, M., & Green, J. (2001

M-CHAT critical items2. Does your child take an interest in other children? (No)7. Does your child ever use his/her index finger to point, to indicate interest
in something? (No)9. Does your child ever bring objects over to you (parent) to show you
something? (No)13. Does your child imitate you? (e.g., you make a face-will your child
imitate it?) (No)14. Does your child respond to his/her name when you call? (No)15. If you point at a toy across the room, does your child look at it? (No)

Social Communication Questionnaire
• A parent report screening measure for autism spectrum disorders (ASDs)
• Based on the Autism Diagnostic Interview-Revised (ADI-R).
• Use evaluated in an autism specialty clinic and a general preschool developmental clinic
» EAVES, WINGERT, HO, & MICKELSON, 2006

The Social Communication Questionnaire
– 40 items, Yes/No format– 10 minutes to complete– Appropriate for individuals whose CA is at least 4
years (possibly CA at least 2 years) and whose MA is at least 2 years
– Current and Lifetime forms; Lifetime generally used for diagnostic screening
– Lifetime score of 15 or greater indicates possible ASD, need for comprehensive evaluation

Social Communication Questionnaire
• Overall sensitivity was .71, the same for both clinics• Specificity was better for the preschool clinic (.62) than
for the autism clinic (.53) reflecting fewer false-positives in the former.
• The ‘‘hit rate’’ was 65% with 28% of the children with autism missed by the SCQ at a cutoff score of 15 (false negatives) and 38% of the nonautistic misidentified as having an ASD (false-positives).
» EAVES, WINGERT, HO, & MICKELSON, 2006

Screening Follow-up
• Refer for diagnostic evaluation – Developmental pediatrician– Specialty clinic
• If developmental delays present, refer for evaluation for Early Intervention services while awaiting diagnostic clarification

Practitioner Review: Diagnosis of autism spectrum disorder in 2- and 3-year-old children• Multidisciplinary diagnostic assessment
– detailed information on developmental history– parents' descriptions of the everyday behaviour
and activities of the child– direct assessment of the child's social
interaction style, including where possible with age peers
– formal assessment of communicative, intellectual and adaptive function
» Charman, T. & Baird, G. (2002). JOURNAL OF CHILD PSYCHOLOGY AND PSYCHIATRY, 43, 289

Practitioner Review (cont.)
• Clinical assessments need to concentrate on early non-verbal social communication behaviours that characterise children with ASD from the second year of life– social orienting– joint attention– Imitation– play – reciprocal affective behaviour.
Practitioner Review (cont.)
• The particular pattern of symptoms in a 2-year-old with ASD may differ from that seen at the more prototypic age of 4 or 5 years. – e.g., overt repetitive and stereotyped
behaviours may be less notable, although where these are seen alongside the social and communicative impairments they are highly indicative of ASD.
Practitioner Review (cont.)
• The use of standardised assessment instruments and the strict application of the DSM and ICD diagnostic criteria need to be employed with caution, as an expert clinical view has been shown to be more accurate.
• An important aspect of early diagnostic consultation is an open and straightforward approach to the negotiation of the diagnostic view with parents over time.

Autism Diagnostic Observation Schedule - Generic (ADOS-G)
• Developed by Catherine Lord, Michael Rutter, and Pamela DiLavore
• Structured play interview conducted with the child
• Designed to provide explicit presses for language and social behaviors that are challenging for children with autism

Key Behaviors Coded in Module One - Communication
• Frequency of vocalization directed to others
• Stereotyped / Idiosyncratic words or phrases
• Use of other’s body to communicate
• Pointing• Gestures

Key Behaviors Coded in Module One - Social
• Unusual eye contact• Facial expressions directed to
others• Shared enjoyment in interaction• Showing• Spontaneous initiation of joint
attention• Response to joint attention• Quality of social overtures

Key Behaviors Coded in Module One - Play
• Functional play with objects
• Imagination / Creativity

Key Behaviors Coded in Module One - Stereotyped Behaviors
• Unusual sensory interest in play material / person
• Hand and finger and other complex mannerisms
• Unusually repetitive interests or stereotyped behaviors

Key Behaviors Coded in Module Two: Communication
• Amount of social overtures• Stereotyped / idiosyncratic words or
phrases• Conversation• Pointing to express interest• Descriptive, conventional, instrumental
gestures

Key Behaviors Coded in Module Two: Social Interaction
• Unusual eye contact• Facial expressions directed to others• Spontaneous initiation of joint attention• Quality of social overtures• Quality of social response• Amount of reciprocal social communication• Overall quality of rapport

Key Behaviors Coded in Module Two: Play
• Imagination / Creativity (“flexible, creative use of objects in a representational manner . . . Use or description of figures or dolls as agents of action”)

Key Behaviors Coded in Module Two: Stereotyped Behaviors / Restricted Interests
• Unusual sensory interest in play material / person
• Hand and finger and other complex mannerisms
• Unusually repetitive interests or stereotyped behaviors
Principles of Good Practice
• Components of diagnostic evaluation– Diagnosis– rationale for the diagnosis– discussion of the implications of the child’s
strengths and challenges– treatment and education recommendations– follow-up to support the implementation of
the recommendations.

Principles of Good Practice
• Family-centered practice – including the parents as full partners in the
assessment team – communicating respect for their expertise and their
contribution to the assessment and treatment planning process.
• Transdisciplinary practice• Community collaboration