early onset dementia key worker service - uowweb/@smah/@med/... · early onset dementia key worker...
TRANSCRIPT

Early Onset Dementia Key Worker Service
Working collaboratively with clients and family carers: A Practical guide to implementing the Goal Attainment Scale in
Younger Onset Dementia care services: Workbook activities
Associate Professor Victoria Traynor University of Wollongong
Draft Workbook September 2013

Draft Workbook Page 1 of 54
Contact details Victoria Traynor Associate Professor (Rehabilitation, Continuing, and Aged Care) & Associate Director, NSW/ACT Dementia Training Study Centre School of Nursing, Midwifery and Indigenous Health Faculty of Science, Medicine and Health Building 41 Room 209 University of Wollongong Wollongong NSW 2522 Australia Email: [email protected] Telephone: +61 2 4221 3471 (Administration Ex 3339) Fax: +61 2 4221 3137
GAS: YOD: Introduction August 2013 ([email protected])

Draft Workbook Page 1 of 54
Contents Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ..................................................................................................................... 1
Introduction ........................................................................................................................... 1
References ............................................................................................................................ 2
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ..................................................................................................................... 3
Aims ........................................................................................................................................ 3
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ..................................................................................................................... 4
1. What is unique about younger onset dementia? ....................................................... 4
Learning Activity 1: Part i: How do clients and their care partners experience younger onset dementia? .............................................................................................. 4
Learning Activity 1: Part ii: How do we identify and assess the needs of individuals and their informal carers/ family members living with younger onset dementia? . 4
Learning Activity 1: Part iii: What does it feel like to live with younger onset dementia? ......................................................................................................................... 5
References ............................................................................................................................ 6
Further reading ..................................................................................................................... 6
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ..................................................................................................................... 7
2. What is rehabilitation care? ............................................................................................ 7
Learning activity 2: Part i: Adopting a rehabilitation approach to dementia care 7
Rehabilitation: Is the Collaborative Recovery Model applicable in dementia care: 8
Collaborative Recovery Model: Guiding principles and main components .......... 8
Learning Activity 2: Part ii: Explaining the potential contribution of the Collaborative Recovery Model for Younger Onset Dementia .................................. 8
References .......................................................................................................................... 10
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ................................................................................................................... 11
3. Goal Attainment Scale: Development and its main components ......................... 11
Goal Attainment Scale: What is it? .................................................................................. 12
Learning Activity 3: Part i: Becoming familiar with GAS: Where do I start? ............ 12
Goal Attainment Scale: The main components ............................................................ 14
Goal Attainment Scale: How do I use the GAS? ....................................................... 14
GAS: YOD: Introduction August 2013 ([email protected])

Draft Workbook Page 2 of 54
How many goals? ........................................................................................................... 14
The GAS score ................................................................................................................. 14
How do we know what is an acceptable gaol attainment level? ......................... 16
Combining the GAS score with therapeutic measurements to evaluate goal attainment for a client ................................................................................................... 17
Learning Activity 3: Part ii: Learning about using the GAS from colleagues .......... 17
Learning Activity 3: Part iii: Locating research papers describing the use of the GAS ................................................................................................................................... 19
Adapting the GAS to increase its usability .................................................................. 21
Learning Activity 3: Part iv: Comparing GAS to GAS-Light Model ........................... 21
References .......................................................................................................................... 22
Further reading ................................................................................................................... 23
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ................................................................................................................... 24
4. Where has GAS been used in dementia care?......................................................... 24
References .......................................................................................................................... 25
Further reading ................................................................................................................... 25
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ................................................................................................................... 26
5. Developing, implementing and evaluating an action plan/ care plan using the GAS ...................................................................................................................................... 26
Learning Activity 5: Part i: Applying the GAS in practice: What is the research evidence that the GAS works for practitioners and clients?.................................... 26
Learning Activity 5: Part ii: Implementing the GAS in practice: Worked example using the Six-Step Guide ................................................................................................ 29
Learning Activity 5: Part iii: Developing SMART goals with the GAS ........................ 30
References .......................................................................................................................... 35
Further reading ................................................................................................................... 36
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ................................................................................................................... 37
6. Promoting the use of the GAS with colleagues ......................................................... 37
Learning Activity 6: Part i: Developing a one-page summary describing the implementation of the GAS .......................................................................................... 37
Learning Activity 6: Part ii: Developing a 3-5 PPT slides summarising the implementation of the GAS .......................................................................................... 37
Implementing collaboratively with clients and family carers: Goal Attainment Scale 38
GAS: YOD: Introduction August 2013 ([email protected])

Draft Workbook Page 3 of 54
Conclusion .......................................................................................................................... 38
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale ................................................................................................................... 39
References .......................................................................................................................... 39
Further reading ................................................................................................................... 40
Responses to Learning Activities .......................................................................................... 43
5. Developing, implementing and evaluating an action plan/ care plan using the GAS: Responses .................................................................................................................. 43
Learning Activity 5: Part i: Responses: Applying the GAS in practice: What is the research evidence that the GAS works for practitioners and clients? ................... 43
5. Developing, implementing and evaluating an action plan/ care plan using the GAS: Responses .................................................................................................................. 48
Learning Activity 5: Part ii: Applying the GAS in practice: What is the research evidence it works?: Responses ..................................................................................... 48
GAS: YOD: Introduction August 2013 ([email protected])
Draft Workbook Page 1 of 54
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
Introduction Welcome to this Module on the use of Goal Attainment Scale (GAS). Completing this Module is an integral activity for the implementation of the Younger Onset Dementia Key Worker initiative funded by the Australian Commonwealth Department of Health and Ageing and delivered by Alzheimer’s Australia. Implementing the use of the Goal Attainment Scale in your role as a Younger Onset Dementia Key Worker will enable you to deliver a range of the Key Results Areas/ Main Responsibilities listed in your Position Description (AA n.d. a) (Table 1).
Table 1: Ways in which using the Goal Attainment Scale will contribute to you fulfilling your role as a Younger Onset Dementia Key Worker
Extract from the Younger Onset Dementia Key Worker Position Description
“Providing direct support to people with younger onset dementia and their carers and families (‘client/s’)” • Being the primary or secondary contact for a client and their family/carer to
provide support at key transition periods throughout a client’s dementia journey using a person centred approach;
• Providing proactive follow up after diagnosis with information and support, carrying out needs assessment, goal setting (Goal Attainment Scale) and developing an individualised service and support plan;
• Developing ongoing relationships with clients and assisting them to develop plans and strategies to meet current and future needs;
• Providing client consultations in a range of settings, including community and in-home environments, telephone and over the internet; and
• Creating awareness of the needs of younger people with dementia and supporting the development of appropriate local service models in the area.
GAS: YOD: Introduction August 2013 ([email protected])
Draft Workbook Page 2 of 54
Extract from the Younger Onset Dementia Key Worker Position Description
“Key Performance Indicators”
• Individualised service and support plans developed for relevant clients; and
• Culturally appropriate strategies are implemented to address the needs of people with dementia and their carers from diverse cultural backgrounds, Aboriginal and Torres Strait Islander people and people in rural and remote areas.
“Skills, experience and knowledge required”
• Client assessment skills and ability to use these skills in a range of settings.
References
Alzheimer’s Australia (AA) n.d. a, Position Description: Younger Onset Dementia Key Worker AA, viewed 28/08/13 <http://www.fightdementia.org.au/common/files/NAT/20130316_NAT_PD_YODkeyWorker.pdf>
GAS: YOD: Introduction August 2013 ([email protected])
Draft Workbook Page 3 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
Aims
By the end of this Module you will be able to:
1. describe the unique aspects of younger onset dementia for those living with younger onset dementia and their informal carers/ family members;
2. understand an enabling approach to rehabilitation care;
3. explain how the Goal Attainment Scale was developed and its main components;
4. critically reflect on the effectiveness of the Goal Attainment Scale for contributing to the delivery of good dementia care;
5. demonstrate how the Goal Attainment Scale can be used to enable individuals and their informal carers/ family members living with younger onset dementia to set goals and evaluate the progress of attaining these goals; and
6. identify the next steps in implementing the use of the Goal Attainment Scale in your workplace.
GAS: YOD: Aims August 2013 ([email protected])

Draft Workbook Page 4 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
1. What is unique about younger onset dementia?
Before learning about the Goal Attainment (GAS) Scale and how it can be implemented as part of your work role we invite you to undertake activities which will enable you to describe the unique aspects of younger onset dementia. These activities will help you later during the Module when you are invited to use the Goal Attainment Scale to identify and evaluate potential goals for individual living with younger onset dementia and their family carers.
Learning Activity 1: Part i: How do clients and their care partners experience younger onset dementia?
To start with, we ask you to watch the DoHA DVD ‘2 Young 4 Dementia’.
‘2 Young 4 Dementia’
Review the case studies and complete the workbook activities.
Learning Activity 1: Part ii: How do we identify and assess the needs of individuals and their informal carers/ family members living with younger onset dementia?
Next, we invite you to complete a 3 hour Module on Younger Onset Dementia. This Module includes a combination of information giving about younger onset dementia a range of interactive learning activities which will provide you with opportunities to develop your understanding about the unique aspects of younger onset dementia.
Visit the NSW/ACT Dementia Training Study Centre n.d. Dementia Education Online website and complete ‘Module 5: Younger Onset Dementia’: http://dementia.uow.edu.au/understandingdementiacare/module5/index.htm to complete the learning activities
GAS: YOD: What is Younger Onset Dementia August 2013 ([email protected])
Draft Workbook Page 5 of 1
Learning Activity 1: Part iii: What does it feel like to live with younger onset dementia?
We also invite you to review the following resource published by the Alzheimer’s Australia (2009) which includes 11 personal stories of men and women from across Australia living with younger onset dementia.
In our own words: A collection of very personal stories Younger Onset Dementia: A collection personal stories found at the following web page: http://www.fightdementia.org.au/common/files/NAT/20101027-Nat-YOD-InOurOwnWords.pdf
Select a story from the person living nearest you and consider how the person telling his/ her story can help you understand what it’s like to live with younger onset dementia.
Personal stories about living with younger onset dementia
What did learn from reading one of these stories?
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
GAS: YOD: What is Younger Onset Dementia August 2013 ([email protected])

Draft Workbook Page 6 of 1
References
Alzheimer’s Australia (AA) 2009, In our own words: a collection of very personal stories Younger Onset Dementia AA, viewed 17/09/13, <http://www.fightdementia.org.au/common/files/NAT/20101027-Nat-YOD-InOurOwnWords.pdf>
Alzheimer’s Australia (AA) ACT 2008, 2 Young 4 Dementia DVD Learning Resource and Workbook AA ACT, Canberra
NSW/ACT Dementia Training Study Centre n.d., Dementia Education Online: Module 5: Younger Onset Dementia University of Wollongong, viewed 28/08/13, <http://dementia.uow.edu.au/understandingdementiacare/module5/index.htm>
Further reading
Alzheimer’s Australia (AA) n.d b, Other resources, AA viewed 17/09/13, <http://www.fightdementia.org.au/services/further-reading-and-resources.aspx>
Alzheimer’s Australia (AA) n.d c, Younger Onset Dementia, AA viewed 17/09/13, <http://www.fightdementia.org.au/services/early-or-younger-onset-dementia.aspx>
Beaumont, H 2009, Losing Clive to younger onset dementia: one family's story, Jessica Kingsley, London.
Davies-Quarrell, V the ACE Club & Keady, J 2010, 'The ACE Approach: promoting well-being and peer support for younger people with dementia’, Journal of Mental Health Training, Education and Practice, vol. 5, no. 3, pp. 41-50.
Harris, PB & Keady, J 2009, ‘Selfhood in younger onset dementia: transitions and testimonies,’ Aging & Mental Health, vol. 13, no. 3, pp. 437-444.
Hodges, JR Gregory, C McKinnon, C Kelso, W Mioshi, E & Piguet O 2009, Quality Dementia Care Series: Younger Onset Dementia a practical guide Alzheimer’s Australia, viewed 17/09/13, <http://www.fightdementia.org.au/common/files/NAT/20090200_Nat_QDC_QDC5YODPracGuide.pdf>
Roach, P Keady, J Bee, P & Hope, K 2009, ‘Subjective experiences of younger people with dementia and their families: a review and implications for UK research, policy and practice attention’. Reviews in Clinical Gerontology, vol. 18, pp. 165-174.
GAS: YOD: What is Younger Onset Dementia August 2013 ([email protected])

Draft Workbook Page 7 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
2. What is rehabilitation care?
Colleagues in the UK who have developed tools and guidance for using the Goal Attainment Scale which is this focus of this module set the scene for us by explaining why the GAS is such a useful tool for practitioners working in rehabilitation care (Turner-Stokes, L n.d. a).
Measuring the effectiveness of rehabilitation care among older people, and specifically clients with a dementia, poses major problems due to the heterogeneity of the deficits and the desired outcomes of clients. Particularly at the level of disability (participation) goals are very much dependant on the individual lifestyles and aspirations of the clients. Standardised measures become increasingly difficult to apply.
For example For some clients, being able to move about independently in a wheelchair may be a triumph while for others this would mean failure.
Goal-setting has become a routine part of rehabilitation care and many multi-disciplinary approaches to clinical care. There is substantial literature which demonstrates its usefulness both as part of the communication and decision-making process, and as a person-centred outcome measure for rehabilitation(Turner-Stokes, L n.d. a ).
This purpose of this section is to demonstrate what approach to rehabilitation care is required in the first place to implement the Goal Attainment Scale in practice.
Learning activity 2: Part i: Adopting a rehabilitation approach to dementia care Competing definitions of rehabilitation exist, for example, some are mechanical and driven by a medical model of rehabilitation with a focus on reversing health problems and working towards helping the client regain previous levels of functioning prior to their health crisis:
GAS: YOD: Rehabilitation models August 2013 ([email protected])

Draft Workbook Page 8 of 1
The NSW Ministry of Health defined rehabilitation as the provision of care that aims to:
restore functional ability for a person who has experienced an illness or injury;
enable regaining function and self-sufficiency to the level prior to that illness or injury within the constraints of the medical prognosis for improvement; and
develop functional ability to compensate for deficits that cannot be medically reversed.
A survey of clinicians working in rehabilitation care within the NSW MoH endorsed this definition with 86% of clinicians stated their agreement with these components of rehabilitation care.
Clearly, in dementia care or when working with frail older people these aims are flawed and rehabilitation care needs to adopt a more open approach with a focus on improving quality of life and enabling a person to live as well as possible with a chronic health problem or a permanent disability.
An alternative definition was proposed by the Royal College of Nursing (2007) in the UK which is also relevant for practitioners working in multi-disciplinary teams:
enhancing and maintaining quality of life;
restoring physical, psychological and social functioning by recognising the health potential of the individual; and
preventing disease and illness.
(RCN, 2007; p. 4)
This model proposes a more enabling approach to rehabilitation care but we would suggest its emphasis remains on restoration which might not always be possible for individuals, particular older people, living with chronic conditions or a permanent disability. An alternative approach from mental health is therefore considered for the purposes of this Module.
Rehabilitation: Is the Collaborative Recovery Model applicable in dementia care:
Collaborative Recovery Model: Guiding principles and main components
Learning Activity 2: Part ii: Explaining the potential contribution of the Collaborative Recovery Model for Younger Onset Dementia
The Collaborative Recovery Model (CRM) reflects the values of or something known as ‘the recovery movement’ which was influenced by theory and practice from Positive Psychology, Psychosocial Rehabilitation Principles, Motivational Interviewing and Theories of Change (Oades et al. 2005).
The CRM focuses on supporting the autonomy of clients through the use of a strong working alliance between the practitioner and client.
GAS: YOD: Rehabilitation models August 2013 ([email protected])
Draft Workbook Page 9 of 1
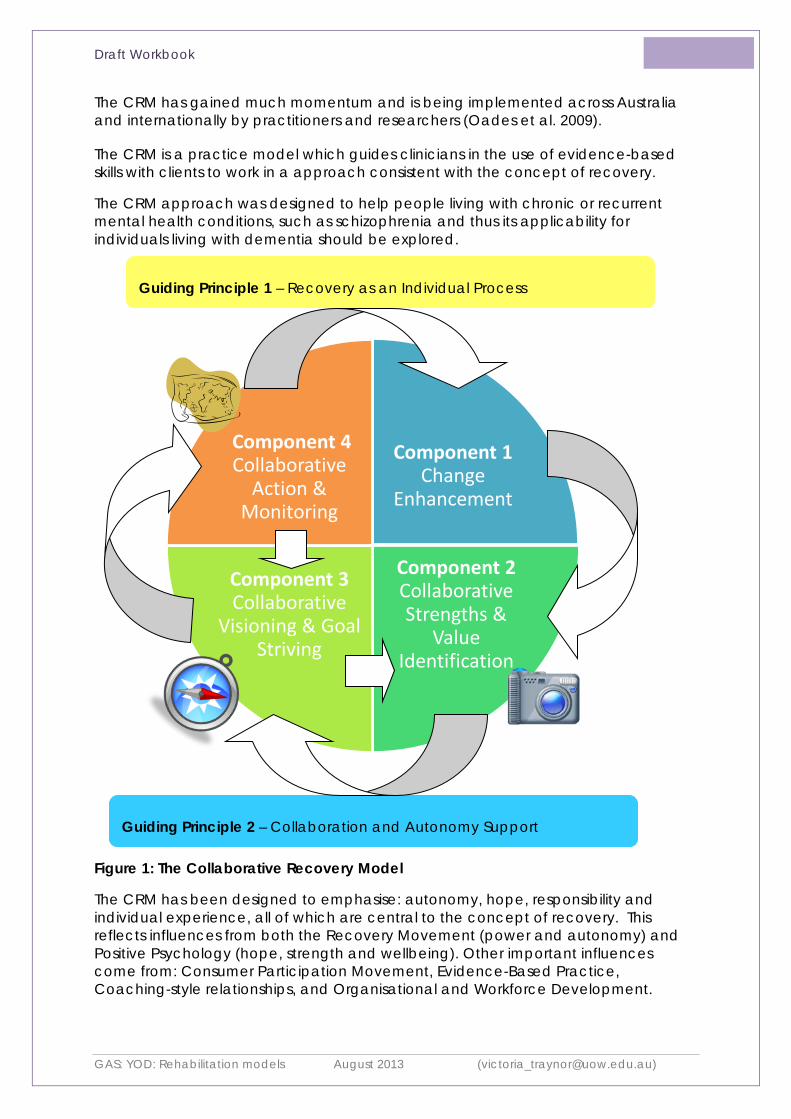
The CRM has gained much momentum and is being implemented across Australia and internationally by practitioners and researchers (Oades et al. 2009).
The CRM is a practice model which guides clinicians in the use of evidence-based skills with clients to work in a approach consistent with the concept of recovery.
The CRM approach was designed to help people living with chronic or recurrent mental health conditions, such as schizophrenia and thus its applicability for individuals living with dementia should be explored.
Figure 1: The Collaborative Recovery Model
The CRM has been designed to emphasise: autonomy, hope, responsibility and individual experience, all of which are central to the concept of recovery. This reflects influences from both the Recovery Movement (power and autonomy) and Positive Psychology (hope, strength and wellbeing). Other important influences come from: Consumer Participation Movement, Evidence-Based Practice, Coaching-style relationships, and Organisational and Workforce Development.
Component 1 Change
Enhancement
Component 2 Collaborative Strengths &
Value Identification
Component 3 Collaborative
Visioning & Goal Striving
Component 4 Collaborative
Action & Monitoring
Guiding Principle 1 – Recovery as an Individual Process
Guiding Principle 2 – Collaboration and Autonomy Support
GAS: YOD: Rehabilitation models August 2013 ([email protected])

Draft Workbook Page 10 of 1
The CRM acknowledges that change occurs at different rates for different people, and might involve several cycles through the different stages of change. The CRM also takes into account the motivational and cognitive capacities of the client and how these may act as barriers to the recovery process.
The CRM is composed of two guiding principles and four components.
The two guiding principles are:
1. Recovery as an Individual Process
2. Collaboration and Autonomy Support
The four components are:
1. Change Enhancement
2. Collaborative Strengths and Values Identification
3. Collaborative Visioning and Goal Striving
4. Collaborative Action and Monitoring
References
Oades, L Deane, F Crowe, T Lambert, WG Kavanagh, D & Lloyd, C 2005, ‘Collaborative recovery: an integrative model for working with individual who experience chronic and recurring mental illness’, Australasian Psychiatry, vol. 13, no. 3, pp.279–284.
Oades, L Crowe, TP & Nguyen, M 2009, ‘Leadership coaching transforming mental health systems from the inside out: person-centred strengths based coaching psychology’, International Coaching Review, vol. 4, no. 1, pp.25–36.
NSW Ministry of Health n.d., NSW Health Rehabilitation Redesign Project Final Report: Model of Care NSW MoH, viewed 28/08/13 <http://www.archi.net.au/documents/resources/models/rehab_redesign/rehabilitation-moc.pdf>
Royal College of Nursing (RCN) 2007, Maximising potential: the role of the nurse in supporting the rehabilitation of older people RCN, viewed 18/09/13, <http://www.rcn.org.uk/__data/assets/pdf_file/0003/109326/003186.pdf>
Turner-Stokes, L n.d. a, Goal Attainment Scaling (GAS) in rehabilitation: a practical guide King’s College London University of London and The North West London Hospitals NHS Trust, viewed 28/08/13 <http://www.csi.kcl.ac.uk/files/Goal%20Attainment%20Scaling%20in%20Rehabilitation%20%20a%20practical%20guide.pdf>
GAS: YOD: Rehabilitation models August 2013 ([email protected])

Draft Workbook Page 11 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
3. Goal Attainment Scale: Development and its main components
In the 1960s, the Goal Attainment Scale (GAS) was developed to evaluate community mental health programmes. Its primary use was to demonstrate, numerically, to funding bodies the size of the positive effect of community mental health programmes on the health and well-being of clients living with mental health problems.
Over time, the use of the GAS has expanded widely. The GAS has been adopted to evaluate physical and general healthcare services, including hospital-based initiatives and is widely used by practitioners with individual clients and informal carers/ family members to evaluate their progress following the implementation of a therapeutic, community or healthcare intervention.
In summary, the GAS is now commonly used to evaluate:
(i) services against how they attain client-specific goals; and
(ii) longitudinal changes in an individual clients or a group of clients.
In particular, the GAS is effective in the following areas of health need:
Successful implementation of the GAS with population groups living with:
age-related changes;
chronic pain;
acquired brain injury; and
amputation.
(Turner-Stokes, n.d. a)
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 12 of 1
In addition, the GAS has been used across a range of care settings:
Successful implementation of the GAS in specialist healthcare services:
home based rehabilitation;
nursing homes; and
paediatric services.
(Bouwens, van Heugten & Verhey, 2008)
Goal Attainment Scale: What is it?
Put simply, the GAS is a numerical measurement method designed to monitor the achievement of goals of services and individuals. The GAS is a global outcome measure which takes account of the needs of individuals and their informal carers/ family members and was designed to provide a client/ family centred approach to evaluation.
In contrast to some medical assessment tools, the GAS takes into account the impact of health problems on everyday living tasks and focuses the attention of the practitioner on developing realistic attainable goals for clients and informal carers/ family carers regardless of how small the change might be considered from a medical evidence based perspective.
The GAS is an ideal tool for use by nurses, allied health and community care workers because it does not focus on medically reversible changes in the health status of clients and informal carers/ family members.
A research institute in London, the Cicely Saunders Institute has developed a web site with a range of resources which could be considered essential for any practitioner or service provider planning to implement the GAS:
Learning Activity 3: Part i: Becoming familiar with GAS: Where do I start?
The first activity for this part of the Module is an invitation to visit the following website and spend time reading, downloading and reviewing the resources included on the web pages:
Cicley Saunders Institute 2010a, GAS - Goal Attainment Scaling in Rehabilitation Institute King’s College London, University of London: http://www.csi.kcl.ac.uk/gas-tool
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 13 of 1
Importantly, GAS promotes the individualisation of goal setting to reflect the needs of each client and informal carer/ family member. In addition, a standardised measurement is used to monitor the attainment of the individual goals by each client attained using a summary formula which enables comparisons over time and across population/ client groups. There could also be comparisons of goal attainment within families if different members of a family select similar goals to work towards and attain.
The score created from the GAS is used by practitioners to demonstrate numerically to clients, informal carers/ family members and other members of the multi-disciplinary team changes in the progress of clients towards attainment of the goals they identify as a priority for promoting their health and well-being. Later in this section, you will be invited to review more specific details about how the GAS score is created.
What is particularly useful about the GAS score is that it is used to reflect the functional ability of clients and can be adapted for any level of health and domain of health. The GAS can be used to address all aspects of life as a whole and the goals for some older clients or clients living with chronic health problems might seem very small when compared to younger people recovery from an acute treatable problem.
Example of a client with a global health issue which would suit the use of the GAS for a small but significant and demanding goal for the client to attain.
An older woman, Amy, experienced a stroke and is living with long term disabilities as a result of the stroke. Amy wants to be able to make a cup of tea for her daughter when her daughter visits her at home. Attaining this goal will enhance Amy’s overall well-being and sense of connectedness in her family. Attaining this goal will require physical abilities, co-ordination skills and household adaptations and involve the support of an Occupational Therapist and Physiotherapist. Amy will negotiate with the practitioners to determine what level of goal attainment will be acceptable to Amy. This goal and the attainment level will be recorded in the GAS scoring sheet which will be re-visited to evaluate Amy’s progress over pre-determined time frames.
The GAS is a valuable tool for practitioners to use for monitoring the achievements of their day-to-day work with individual clients and population groups. In today’s healthcare environment in which there is an increased emphasis on a client-centred approach for population groups living with chronic health issues, including dementia, the numerical scores in the GAS enable practitioners to clearly and explicitly demonstrate their value for promoting the health and well-being of population groups living with chronic health issues.
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 14 of 1
Goal Attainment Scale: The main components
Goal Attainment Scale: How do I use the GAS?
The GAS method consists of a 6-step process which has been well documented by those who have used the GAS in a range of healthcare settings and with a wide range of clients, including dementia care (Figure 1).
How many goals?
The authors of the GAS and those who have written guidelines for using the GAS recommend an optimal number of goals which practitioners negotiate with clients to prioritise and work towards attaining.
A set of three goals is the optimal number of goals to be set when using the GAS.
The GAS score
A GAS scoring guide is used to monitor attainment of goals and evaluate the progress of an intervention.
Table 2: Goal Attainment Scale: Summary of the six step approach to identifying and evaluating individual goals (adapted from Better Evaluation 2012)
Level of Expected OUTCOME
3 months after the course
Rating
Behavioural statement of
EXPECTED OUTCOMES: - GOALS 1
Behavioural statement of
EXPECTED OUTCOMES:
- GOAL 2
Behavioural statement of
EXPECTED OUTCOMES:
- GOAL 3
MUCH MORE Than
EXPECTED +2
MORE than EXPEXTED +1
EXPECTED Outcome 0
LESS than EXPECTED -1
MUCH LESS than
EXPECTED
-2
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 15 of 1
Figure 1: Goal Attainment Scale: Summary of the six step approach to identifying and evaluating individual goals (adapted from Bouwens et al. 2008; p. 529-530)
Step 1
• Select goals (a minium of 3) that are relevant to the individual and/ or family caregiver. An interview is used by a clinician to identify needs and determine goals for those areas of need for which an intervention will be planned. To ensure reliable calculation, with the standard formula, a minimum of 3 goals is recommended.
Step 2 • Find an opportunity to weight the goals from the 'most important' to the 'least important' using a number between 1 and 10. If there is no
hierarchy in the importance of the goals according to the individual and/ or family member all weights for the goals are set at '1'.
Step 3 • A follow-up time is set before the start of the evaluation is determined. This is the pre-determined time when a clinician measures the
level of goal attainment.
Step 4 • The expected outcome, that is the goal, is set. Outcome levels are specified in observable terms in such a way that a lay person would be
able to score the follow-up guides. Levels do not overlap. The expected outcome is scored with ‘0’.
Step 5 • Complete other scale levels, using possible outcomes including much less than expected (–2), somewhat less than expected (–1),
somewhat better than expected (+1) and much better than expected (+2).
Step 6
• GAS baseline levels are noted on the follow-up guide. If a clinically relevant deterioration is plausible the description of the current status can be scored as ‘–1’, with the worsened state scored as ‘–2’. If the problem is at its worst the current level of functioning is scored as ‘–2’. Client receives an intervention and at the defined follow-up time (e.g. end of intervention) the client is scored at the attained level.
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 16 of 1
The Cecily Saunders Institute developed an Excel spread sheet into which practitioners can enter the GAS scores. A formula entered into the GAS Calculation Sheet generates the outcomes for the clients and informal carers/ family members with whom the practitioners are working (Figure 2).
Download the GAS Calculation Excel spread sheet:
Cicley Saunders Institute 2010b, GAS Calculation Sheet Institute King’s College London, University of London, http://www.csi.kcl.ac.uk/files/GAS%20calculation%20sheet.xls
Figure 2: GAS Calculation Sheet in Excel format (adapted from Cicley Saunders Institute 2010b)
Please note: You might need to find a colleague with experience of using Excel to provide some initial guidance for understanding how this Excel spread sheet can be used.
How do we know what is an acceptable gaol attainment level?
A GAS score at follow-up of 50 indicates that all predefined goals met the expected outcome at follow-up.
The overall GAS score at baseline and follow-up is calculated with a standard formula. When goals are weighted, this weight is inserted in this formula.
The hypothetical mean GAS score at follow-up is 50 (SD = 10). Consistently high or low follow-up scores indicate that goals were too easy (scores >50) or too difficult to attain (scores <50).
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 17 of 1
Combining the GAS score with therapeutic measurements to evaluate goal attainment for a client
The implementation of the GAS can be combined with any therapeutic/ clinical outcome measure which is relevant to the work you do with a client and informal carer/ family member. In Appendix 1 of the Turner-Stokes (n.d. a) ‘Practical Guide to Using the GAS’ a ‘Worked Example’ (p. 8-10) is provided for practitioners to see how the GAS can be used in combination with a therapeutic/ clinical outcome measure.
Goal: Experience less pain
A validated pain assessment scale, for example, the Abbey Pain Scale, can be used in conjunction with the GAS to provide supporting evidence, at any time, about how the client is working towards attaining a GAS goal. The practitioner works with the client and informal carer/ family member to determine what score on the Abbey Pain Scale would reflect the goal attainment of:
• ‘MUCH MORE Than EXPECTED (+2)’;
• ‘MORE than EXPEXTED (+1)’;
• ‘EXPECTED Outcome (0)’;
• ‘LESS than EXPECTED (-1)’; or
• ‘MUCH LESS than EXPECTED (-2)’.
In this way, there is a rigorous approach to monitoring the progress towards attaining the goal of ‘experience less pain’. Objective measurable changes provide supporting evidence about what effect a pain management intervention is having on the health and well-being of a client and informal carer/ family member and, more specifically, the level of this effect.
When you use the GAS you can select therapeutic/ clinical outcome measures which will be used to measure specific aspects of the work you undertake with individual and/ or groups of clients and carers/ family members to improve their health and well-being and demonstrate specifically levels of goal attainment.
You will have the opportunity to re-visit how therapeutic/ clinical outcome measures are combined with the GAS later in the Module when you are invited to develop undertake a real case study of Hugh and his family with younger onset dementia.
Learning Activity 3: Part ii: Learning about using the GAS from colleagues
To start with, we invite you to use your professional local, extended and virtual networks to find colleagues who have used the GAS in their work place.
We suggest you talk to colleagues during face-to-face meetings, make telephone contact, email or use ‘list serves’ to find colleagues who have used the GAS in their work roles.
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 18 of 1
Talking to colleagues is always a good place to start exploring a new model/ tool/ ways of working. When you consult your colleagues it is important that you use the opportunity to engage with them using a critical reflective dialogue.
Below are some suggestions for the type of questions you could use to structure the critical reflective dialogue you have with colleagues about the GAS and other aspects of your work when exploring other topics in the future.
When you talk to your colleagues ask them the following questions
ADVANTAGES OF GAS
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
DISADVANTAGES OF GAS
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
LESSONS LEARNT FOR USING GAS IN THE FUTURE
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 19 of 1
Using this structured approach to conversations with your colleagues provides you with the opportunity to further develop your critical thinking skills. These critical thinking skills are necessary for your client work as well as reviewing research papers of best practice evidence.
Learning Activity 3: Part iii: Locating research papers describing the use of the GAS
Use the library databases you are familiar with, or ask a colleague which library databases they would recommend, to locate two research papers describing the use of the GAS:
(i) services against how they attain client-specific goals; and
(ii) longitudinal changes in an individual clients or a group of clients.
a) Write down the references for these research papers in the box below
REFERENCES
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
b) Identify and write down the aims of the two research projects which you located and selected as examples of using the GAS as an evaluation approach.
AIMS
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 20 of 1
c) Consider your work role and identify what is similar and different to what you are required to do in the service where you work and what lessons you can learn from these two research papers for the service you provide.
SIMILARITIES TO MY WORK ROLE and SERVICES I DELIVER
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
DIFFERENCES TO MY WORK ROLE and SERVICES I DELIVER
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
LESSONS FOR MY WORK ROLE and SERVICES I DELIVER
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 21 of 1
Adapting the GAS to increase its usability
Colleagues at King’s College London University of London and The North West London Hospitals NHS Trust recently adapted the GAS and developed the GAS-Light Model (Turner-Stokes, n.d. b; p. 5). You are invited to compare the GAS and GAS-Light Model and consider which version is most suitable for your work role.
The GAS was adapted because Turner-Stokes (n.d. b) discovered that it had drawbacks which led to practitioners not using the GAS: (i) practitioners had ‘perceived negative connotations of the zero and minus scores’ required when using the GAS score and (ii) the score cannot account for a client ‘worsening’ after the implementation of an intervention (p. 5).
The main adaption in the GAS-Light Model was the creation of the verbal scoring system: ‘verbal non-numerical scores’ for (Turner-Stokes, n.d. b) (Table 3).
Table 3: GAS verbal non-numerical scoring using the GAS-Light model (adapted from Turner-Stokes, n.d. b; 5)
At Baseline With respect to the goal, what function does the client have?
Some function
No function (as bad as they could be)
At Outcome Was the goal achieved?
YES A lot more
A little more
As expected
No Partially achieved
No change
Got worse
Learning Activity 3: Part iv: Comparing GAS to GAS-Light Model
Review the material presented in this section and compare the original GAS and the Gas-Light Model
Identify the benefits of using the GAS in work role
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
GAS: YOD: Development and components August 2013 ([email protected])

Draft Workbook Page 22 of 1
Identify barriers to using the original GAS
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
Identify reasons why the GAS-Light model would suit the work you do with clients and informal carers/ family members
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
…………………………………………………………………………………………………………..
References
Better Evaluation 2012, Goal Attainment Scale Better Evaluation viewed 17/09/13 <http://betterevaluation.org/evaluation-options/GoalAttainmentScales>
Bouwens, SFM van Heugten, CM & Verhey, FRJ 2008, ‘Review of Goal Attainment Scaling as a Useful Outcome Measure in Psychogeriatric Patients with Cognitive Disorders’, Dementia Geriatric and Cognitive Disorders, vol. 26, pp. 528–540.
Cicley Saunders Institute 2010a, GAS - Goal Attainment Scaling in Rehabilitation Institute King’s College London, University of London, viewed 28/08/13, <http://www.csi.kcl.ac.uk/gas-tool>
GAS: YOD: Development and components August 2013 ([email protected])
Draft Workbook Page 23 of 1
Cicley Saunders Institute 2010b, GAS Calculation Sheet Institute King’s College London, University of London, viewed 28/08/13, <http://www.csi.kcl.ac.uk/files/GAS%20calculation%20sheet.xls>
Turner-Stokes, L n.d. a, Goal Attainment Scaling (GAS) in rehabilitation: a practical guide King’s College London University of London and The North West London Hospitals NHS Trust, viewed 28/08/13 <http://www.csi.kcl.ac.uk/files/Goal%20Attainment%20Scaling%20in%20Rehabilitation%20%20a%20practical%20guide.pdf>
Turner-Stokes, L n.d. b, Goal Attainment Scaling (GAS) in rehabilitation: the GAS-Light model King’s College London University of London and The North West London Hospitals NHS Trust, viewed 28/08/13 <http://www.csi.kcl.ac.uk/gas-tool>
Further reading
Bravo, G Dubois, MF & Roy PM 2005, ‘Using Goal Attainment Scaling to improve the quality of long-term care: a group-randomized trial’, International Journal of Qualitative Health Care, vol. 17, pp. 511–519.
Fisher, K 2008, ‘Assessing clinically meaningful change following a programme for managing chronic pain’. Clinical Rehabilitation, vol. 22, pp. 252–259.
Hurn, J Kneebone, I & Cropley, M 2006, ‘Goal setting as an outcome measure: a systematic review’. Clinical Rehabilitation vol. 20, no. 9, pp. 756-72.
Kiresuk, T & Sherman, RE 1968 ‘Goal Attainment Scaling: a general method for evaluating comprehensive community mental health programs’, Community Mental Health Journal, vol. 4, pp. 443–453.
Yau, DCN Lam, MCC Lung, MKW Chow, AYH Yung, NSY Chui, TY, et al. 2002, ‘Outcome focused nursing practice in geriatric day-rehabilitation service: facilitating elderly patients to achieve therapeutic goals’, Hong Kong Nursing Journal, vol. 38, pp. 33–38.
GAS: YOD: Development and components August 2013 ([email protected])
Draft Workbook Page 24 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
4. Where has GAS been used in dementia care?
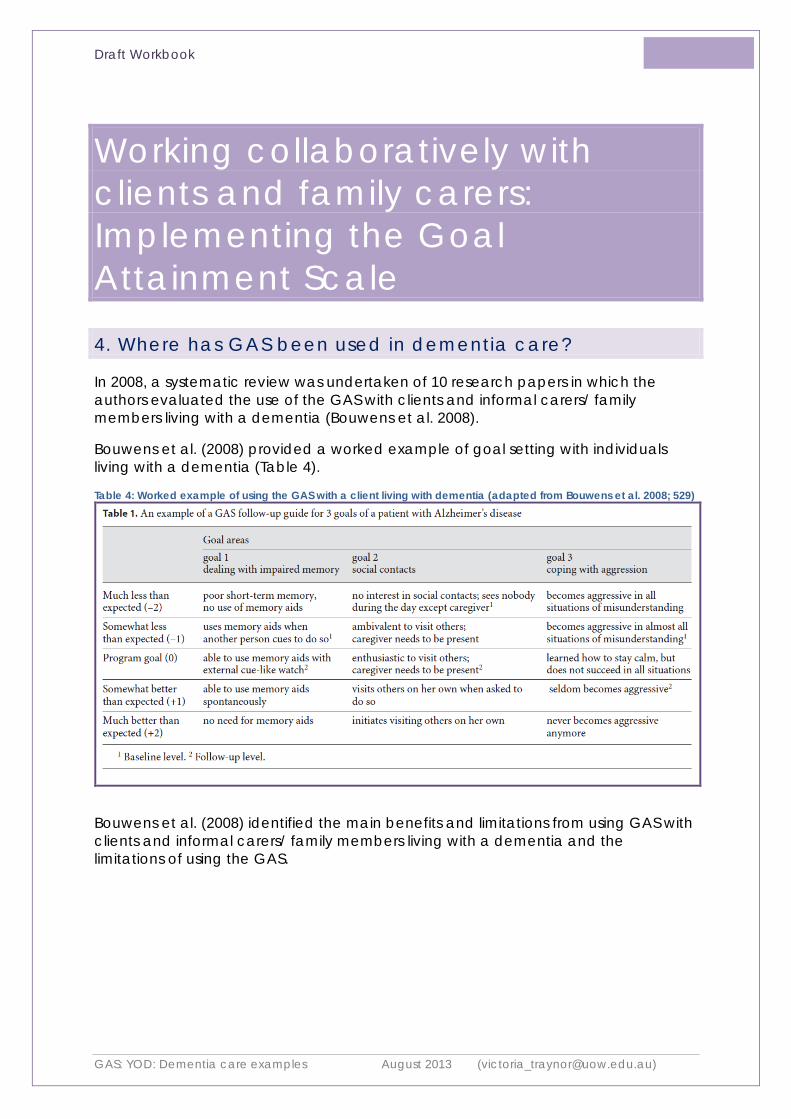
In 2008, a systematic review was undertaken of 10 research papers in which the authors evaluated the use of the GAS with clients and informal carers/ family members living with a dementia (Bouwens et al. 2008).
Bouwens et al. (2008) provided a worked example of goal setting with individuals living with a dementia (Table 4).
Table 4: Worked example of using the GAS with a client living with dementia (adapted from Bouwens et al. 2008; 529)
Bouwens et al. (2008) identified the main benefits and limitations from using GAS with clients and informal carers/ family members living with a dementia and the limitations of using the GAS.
GAS: YOD: Dementia care examples August 2013 ([email protected])

Draft Workbook Page 25 of 1
Advantages of GAS in dementia care
• A wide range of domains were selected by the authors of the 10 papers in which the GAS was used in dementia care(p. 535 column 1), including:
o cognition; o instrumental activities of daily life/ self care; o mood; o behaviour; or o mood.
• The information generated from the GAS is particularly useful when used in conjunction with traditional standard dementia care outcome measures because the GAS provides information which cannot be generated from these tools, for example:
o ADAS-cog (p. 537 column 2).
• The GAS requires practitioners to proactively involve clients and informal carers/ family members in setting goals. Therefore, using the GAS reduces the risk that clients and informal carers/ family members be excluded from goal setting activities and deciding the order in which interventions be implemented (p. 534 column 2 and p. 537 column 2).
• The GAS inevitably involves discussions with different members of the multi-disciplinary team and discussions about how different practitioners will contribute towards attaining the goals the client and informal carers/ family members identify as their priorities.
Limitations of GAS in dementia care
• The review demonstrated that in 8 out of the 10 studies practitioners identified more than the optimal 3 goals (p. 534 column 1). It is clear from this review that practitioners need clearer guidelines about observing the recommendation in the GAS literature that only 3 goals be set with clients and informal carers/ family members.
• Completing the GAS can take up to 30 minutes compared to the 3-5 minutes it can take to complete dementia-specific assessment tools, for example, the Mini Mental State Examination (MMSE) (p. 537 column 2).
References
Bouwens, SFM van Heugten, CM & Verhey, FRJ 2008, ‘Review of Goal Attainment Scaling as a Useful Outcome Measure in Psychogeriatric Patients with Cognitive Disorders’, Dementia Geriatric and Cognitive Disorders, vol. 26, pp. 528–540.
Further reading
Rockwood, K Fay, S & Jarrett, P 2007, ‘Asp E: effect of galantamine on verbal repetition in AD: a secondary analysis of the VISTA trial’, Neurology, vol. 68, pp. 1116–1121.
GAS: YOD: Dementia care examples August 2013 ([email protected])

Draft Workbook Page 26 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
5. Developing, implementing and evaluating an action plan/ care plan using the GAS
We will now provide you with an opportunity to describe how you would develop, implement and evaluate an action plan/ care plan using the GAS with clients and informal carers/ family members living with a dementia.
Learning Activity 5: Part i: Applying the GAS in practice: What is the research evidence that the GAS works for practitioners and clients?
Before you complete this activity, we invite you to critically review a study evaluating the practical use of the GAS with clients living with acquired brain injury who receive cognitive rehabilitation. The purpose of you completing this critical review is to provide a clinical example of evaluating the role of GAS in the work of clinicians which simulates what will be expected of you in your clinical role.
Read and critically review the following paper
Bouwens, SFM van Heugten, CM & Verhey, FRJ 2009, ‘The practical use of goal attainment scaling for people with acquired brain injury who receive cognitive rehabilitation’, Clinical Rehabilitation, vol. 23, pp. 310–320.
Question Response
1. The authors claim that this study has a sample as large as only one other study evaluating the use of the GAS.
a. What was the total sample size at the end of the six months of this study?
b. What was the drop-out rate for this study?
c. For what reasons did clients drop out from this study?
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 27 of 1
d. Who were the authors of the study which recruited a similarly large sample size?
e. What was the year and the journal where this previous study was published?
2. The number of goals set using the GAS has an impact on its effectiveness.
a. What was the mean number of goals completed with clients for this study?
b. How does this number compare with the recommended number of goals to be set with clients.
3. The authors timed the length of time it took clients to identify their goals with practitioners.
a. What was the mean length of time it took to identify goals?
b. When it took longer than 30 minutes to set goals what the reasons for this?
c. Consider the implications of Question 3b for your work role of these findings and your implementation of the use of the GAS.
4. The authors report on the mean goal attainment levels for the clients who participated in this study.
At six months what was the percentage level of attainment for the client goals?
5. The practitioners used telephone calls to set goals with clients.
a. What were consequences of using telephone calls to set goals with clients.
b. Consider what impact these findings will have on whether you use telephone calls with clients and informal carers/ family members to set goals.
6. The authors reported a concern that clients might report socially desirable answers when goal attainment is reviewed (p. 317 column 1).
GAS: YOD: Implementation August 2013 ([email protected])
Draft Workbook Page 28 of 1
Consider the consequences of this when setting goals with your clients.
7. In some cases the informal carer/ family member contributed to helping the client setting goals (p. 316 column 1 and p. 317 column 2).
Explain how the findings from this research could provide you with insights into what it will be like to use the GAS with your clients and informal carers/ family members.
8. In the abstract the authors state that having a depressive illness has an impact on whether the use of the GAS is effective.
a. How many clients in this study did the authors find with depressive illness?
b. What is the significance of this finding for your work?
c. Use the library databases to locate one other research paper in which the GAS is implemented with or at least includes clients with a depressive illness.
9. The authors state that the GAS should not be used on its own but in conjunction with other measures of therapeutic effect (p. 317 column 2) and that specific objective measures are also required to measure the gaol attainment alongside the GAS scores, for example, the distance a client can walk following an intervention (p. 317 column 1).
a. Where in this Module is this approach discussed.
b. What examples from your practice can you think of which will require you to use another assessment tool/ additional criteria to evaluate the outcome of
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 29 of 1
Learning Activity 5: Part ii: Implementing the GAS in practice: Worked example using the Six-Step Guide
First of all, re-visit the Six-Step Guide from earlier in the Module (Figure 1, p. 15).
Next, re-visit the NSW/ACT Dementia Training Study Centre n.d., Dementia Education Online ‘Module 5: Younger Onset Dementia’ Section iv: ‘Service Provision for Younger Onset Dementia’ Activity 4 (http://dementia.uow.edu.au/understandingdementiacare/module5/service.html)
Watch the video prepared by Max Larkin and Emily Boardway about their father, Dr Hugh Larkin. The video explains how Hugh’s family continue to connect with him.
Use the Six-Step GAS Guide to develop goals for Hugh and his family.
1. Goal setting i. As you are watch the film of Hugh and his family consider the goals they
would each set for themselves:
Hugh
Hugh’s wife
Hugh’s sons
Hugh’s daughters
ii. List as many goals for Hugh and his family as you can think of.
iii. Next, select only 3 of these goals. Make the selection by imagining the conversations and negotiations you would have with Hugh and his family to select only 3 goals. Select 3 goals for (i) Hugh and 3 goals for (ii) one member of Hugh’s family (you will write a total of 6 goals).
2. Weight the (i) 3 goals for Hugh and the (ii) 3 goals for a family member.
3. Identify the initial timeframe and follow-up time which (i) Hugh and (ii) the family member will work towards attaining each of their 3 goals.
4. Identify the ‘Behavioural Outcome Statement’ for each of these 3 goals for (i) Hugh and (ii) one family member.
5. Step Five cannot be undertaken as part of this Learning Activity because it involves the evaluation phase and documenting the GAS scores at the agreed timeframe. At this time, the levels at which the goals were attained is agreed with the client and informal carer/ family member and a numerical GAS score is recorded in the Excel GAS Calculation Sheet (Figure 2, p. 16).
6. In your clinical work, Step 5 is repeated at an agreed follow-up time and again the progress towards attaining goals is agreed by the client and informal carers/ family members and recorded using the GAS score on the Excel GAS Calculation Sheet (Figure 2, p. 16).
GAS: YOD: Implementation August 2013 ([email protected])
Draft Workbook Page 30 of 1
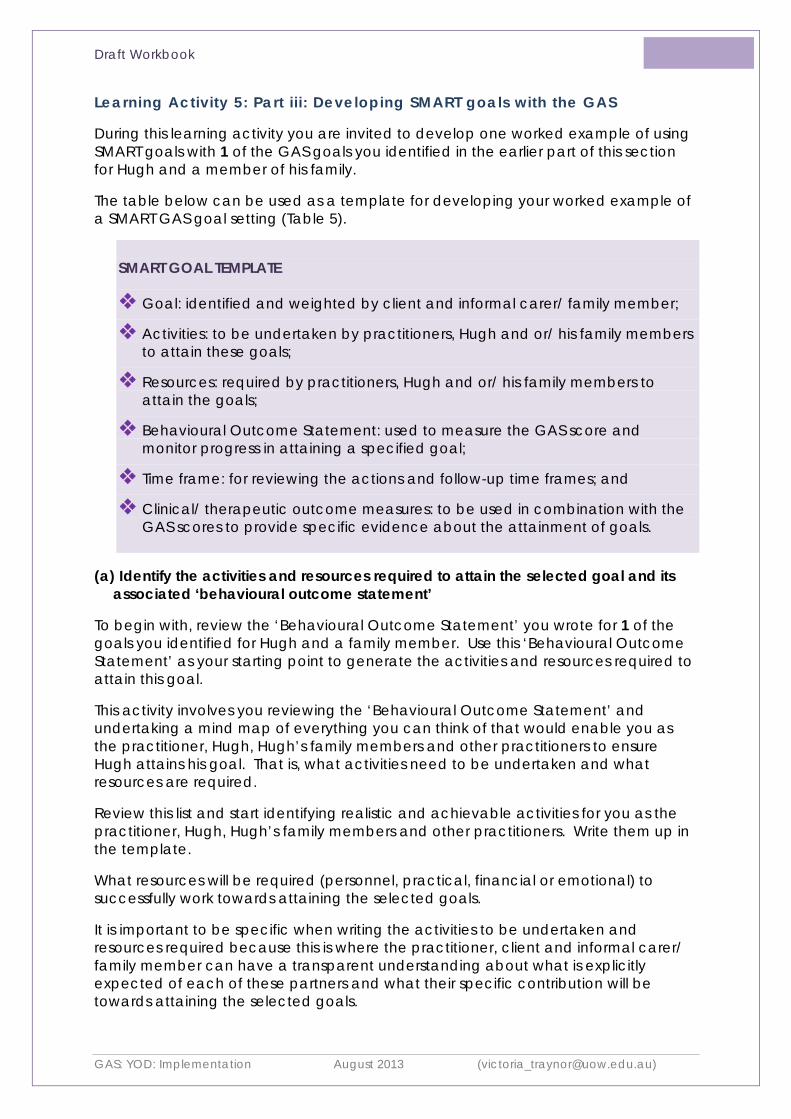
Learning Activity 5: Part iii: Developing SMART goals with the GAS
During this learning activity you are invited to develop one worked example of using SMART goals with 1 of the GAS goals you identified in the earlier part of this section for Hugh and a member of his family.
The table below can be used as a template for developing your worked example of a SMART GAS goal setting (Table 5).
SMART GOAL TEMPLATE
Goal: identified and weighted by client and informal carer/ family member;
Activities: to be undertaken by practitioners, Hugh and or/ his family members to attain these goals;
Resources: required by practitioners, Hugh and or/ his family members to attain the goals;
Behavioural Outcome Statement: used to measure the GAS score and monitor progress in attaining a specified goal;
Time frame: for reviewing the actions and follow-up time frames; and
Clinical/ therapeutic outcome measures: to be used in combination with the GAS scores to provide specific evidence about the attainment of goals.
(a) Identify the activities and resources required to attain the selected goal and its associated ‘behavioural outcome statement’
To begin with, review the ‘Behavioural Outcome Statement’ you wrote for 1 of the goals you identified for Hugh and a family member. Use this ‘Behavioural Outcome Statement’ as your starting point to generate the activities and resources required to attain this goal.
This activity involves you reviewing the ‘Behavioural Outcome Statement’ and undertaking a mind map of everything you can think of that would enable you as the practitioner, Hugh, Hugh’s family members and other practitioners to ensure Hugh attains his goal. That is, what activities need to be undertaken and what resources are required.
Review this list and start identifying realistic and achievable activities for you as the practitioner, Hugh, Hugh’s family members and other practitioners. Write them up in the template.
What resources will be required (personnel, practical, financial or emotional) to successfully work towards attaining the selected goals.
It is important to be specific when writing the activities to be undertaken and resources required because this is where the practitioner, client and informal carer/ family member can have a transparent understanding about what is explicitly expected of each of these partners and what their specific contribution will be towards attaining the selected goals.
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 31 of 1 Table 5: Summary of how SMART Goals to be achieved and progress monitored Goal Activity/
Therapeutic Intervention (undertaken by Key Worker(s), client, family member or other practitioner)
Resources Behavioural Outcome of Goal Statement
Clients’ or carers’ criteria/ Assessment Tools/ Clinical/ Therapeutic Outcome Measure
Review Dates/ Time frame
Hugh’s goals
1.
2.
3.
Wife’s goals
1.
2.
3.
Children’s goals 1.
2.
3.
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 32 of 1
(b) Identify clinical/ therapeutic outcome measures which could be used in combination with the GAS score to monitor progress towards attainment of the goals
Lastly, you are invited to select clinical/ therapeutic outcome measures which you will use in combination with the GAS to monitor more specifically the progress of the client or informal carer/ family carer towards attaining their selected goal.
The use of these clinical/ therapeutic outcome measures can make the selection of the GAS score easier and more meaningful for practitioners, clients and informal carers/ family members.
Clinical/ therapeutic outcome measure: Carer burden using the Zarit Burden Interview
The Zarit Burden Interview is a validated tool used to assess the level of carer burden for carers of individuals living with a dementia. The Zarit Burden Interview is a 22 Likert item tool which generates scores ranging from 0-88 (no burden to the highest level of burden).
One way of ensuring the GAS score is used rigorously is to ask Hugh’s wife what level of burden she would consider realistic to work towards attaining in the proceeding month. Her current score is 78. She decides to aim towards to reducing her burden to a score of 68.
You can work in advance with Hugh’s wife to decide what the Zarit Burden Interview scores would reflect the GAS score attainments:
• 58: MUCH MORE Than EXPECTED (+2);
• 63: MORE than EXPEXTED (+1);
• 68: EXPECTED Outcome (0);
• 72: LESS than EXPECTED (-1); or
• 75: MUCH LESS than EXPECTED (-2).
In this way, there is a rigorous approach to monitoring the progress towards attaining the goal of ‘reduced carer burden’. Objective measurable changes provide supporting evidence about what the specific effects your carer stress relief intervention will have on Hugh’s wife’s level of carer burden.
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 33 of 1
We invite you to review the 1 goal you have selected to develop into a worked example and list the clinical/ therapeutic outcome measures you could use in combination with the GAS goal.
Clinical/ therapeutic outcome measures to be used in combination with the GAS goals
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
………………………………………………………………………………………………
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 34 of 1
Below are lists of clinical/ therapeutic outcome measures which you could use in your role to monitor the progress of the client and informal carer/ family member in attaining their GAS goal.
Clients’ criteria/ assessment tools/ Clinical/ therapeutic outcome measures
• Qualitative o Client or family carer identified specific outcomes o A conversation o Narrative o Client/ carer outcome o Diary (completed by client, family carer and/ or staff)
(recording/ counting events as they occur) • Quantitative
o Depression - Cornell Depression Scale - Geriatric Depression Scale (GDS)
o Dementia specific - Abbey Pain Scale - Algase Wandering Scale (AWS) - Cohen Mansfield Agitation Inventory (CMAI) - DEM QoL/ DEMQol Proxy - Dewing Wandering Assessment Tool - Neuropsychiatry Inventory (NPI) - Pain Assessment In Advanced Dementia (PAINAD) scale - Psychogeriatric Assessment Scale (PAS)
o QoL – QOLAD/ o Physical Health Assessment o Physical activity assessment scales o Social networking scale o Well being scale – nominate a validated scale or create a
scale using a Likert scale using numbers or images to distinguish different levels
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 35 of 1
Care partner/ family member providing most day-to-day or with most responsibility/ power of attorney or official guardian criteria/
Carer criteria/ assessment tools/ Clinical/ therapeutic outcome measures
• Qualitative o Client or family carer identified specific outcomes o Diary (completed by client, family carer and/ or staff)
(recording/ counting events as they occur) • Quantitative
o Geriatric Depression Scale (GDS) (if family member over 55 years)
o Aged-appropriate depression scale o Physical Health Assessment o Zarit Burden Scale o Specific anxiety scale o Self-efficacy assessment o Social networking scale
Children’s or dependant’s criteria/ assessment tools
• Qualitative o Client or family carer identified specific outcomes
• Quantitative o Aged-appropriate depression scale o Aged-appropriate anxiety scale
References
Bouwens, SFM van Heugten, CM & Verhey, FRJ 2009, ‘The practical use of goal attainment scaling for people with acquired brain injury who receive cognitive rehabilitation’, Clinical Rehabilitation, vol. 23, pp. 310–320.
NSW/ACT Dementia Training Study Centre n.d., Dementia Education Online: Module 5: Younger Onset Dementia University of Wollongong, viewed 28/08/13, <http://dementia.uow.edu.au/understandingdementiacare/module5/service.html>
GAS: YOD: Implementation August 2013 ([email protected])
Draft Workbook Page 36 of 1
Further reading
Bovend’Eerdt, TJH Botell, RE & Wade, DT 2009, ‘Writing SMART rehabilitation goals and achieving goal attainment scaling: a practical guide’, Clinical Rehabilitation, vol. 23, pp. 352–361
Department of Health and Ageing (DoHA) 2012, Behaviour Management: a good practice guide: Managing Behavioural and Psychological Symptoms of Dementia DoHA viewed 18/09/13, <http://www.dementiaresearch.org.au/images/dcrc/output-files/328-2012_dbmas_bpsd_guidelines_guide.pdf>
Department of Health and Ageing (DoHA) 2007, Dementia Outcomes Suite DoHA viewed 18/09/13, <http://www.dementia-assessment.com.au/>
NSW Ministry of Health (NSW MoH) 2013, Assessment and Management of People with Behavioural and Psychological Symptoms of Dementia (BPSD) A Handbook for NSW Health Clinicians NSW MoH, viewed 18/09/13,<http://www.health.nsw.gov.au/dementia/Publications/assessment-mgmt-people-bpsd.pdf>
GAS: YOD: Implementation August 2013 ([email protected])

Draft Workbook Page 37 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
6. Promoting the use of the GAS with colleagues
Congratulations for progressing through this module and learning about how to implement the GAS in your work role.
The final activity involves developing resources which you can use to teach new team members how to use the GAS and promote its use to other teams unfamiliar with GAS.
Learning Activity 6: Part i: Developing a one-page summary describing the implementation of the GAS
Make contact with a colleague in a different team and work together to draft the content for a one-page summary of implementing the GAS. This one-page summary will be provided to new team members as part of their induction programme so that they can start to learn how to use the GAS in their work.
Learning Activity 6: Part ii: Developing a 3-5 PPT slides summarising the implementation of the GAS
Make contact with another colleague in a different team and work together to draft the content for a 3-5 PPT summary of implementing the GAS. This summary will be used to promote the use of the GAS in other teams. Ensure you use the notes page of the PPT slides for recording the content of the presentation so that other colleagues can also use the presentation.
GAS: YOD: Future strategies August 2013 ([email protected])
Draft Workbook Page 38 of 1
Implementing collaboratively with clients and family carers: Goal Attainment Scale
Conclusion
Well done on completing this Module. After completing this Module and the learning activities which make up this Module you have developed your competence (knowledge, skills and attitudes) in using the GAS. More specifically you:
1. identified the unique aspects of younger onset dementia for those living with younger onset dementia and their informal carers/ family members;
2. understand an enabling approach to rehabilitation care;
3. explained how the Goal Attainment Scale was developed and its main components;
4. critically reflected on the effectiveness of the Goal Attainment Scale for contributing to the delivery of good dementia care;
5. practised using the Goal Attainment Scale to enable individuals and their informal carers/ family members living with younger onset dementia to set goals and evaluate the progress of attaining these goals; and
6. identify the next steps in implementing the use of the Goal Attainment Scale in your workplace.
GAS: YOD: Conclusion August 2013 ([email protected])

Draft Workbook Page 39 of 1
Working collaboratively with clients and family carers: Implementing the Goal Attainment Scale
References
Alzheimer’s Australia (AA) 2009, In our own words: a collection of very personal stories Younger Onset Dementia AA, viewed 17/09/13, <http://www.fightdementia.org.au/common/files/NAT/20101027-Nat-YOD-InOurOwnWords.pdf>
Alzheimer’s Australia (AA) ACT 2008, 2 Young 4 Dementia DVD Learning Resource and Workbook AA ACT, Canberra
Alzheimer’s Australia (AA) n.d. a, Position Description: Younger Onset Dementia Key Worker AA, viewed 28/08/13 <http://www.fightdementia.org.au/common/files/NAT/20130316_NAT_PD_YODkeyWorker.pdf>
Better Evaluation 2012, Goal Attainment Scale Better Evaluation viewed 17/09/13 <http://betterevaluation.org/evaluation-options/GoalAttainmentScales>
Bouwens, SFM van Heugten, CM & Verhey, FRJ 2008, ‘Review of Goal Attainment Scaling as a Useful Outcome Measure in Psychogeriatric Patients with Cognitive Disorders’, Dementia Geriatric and Cognitive Disorders, vol. 26, pp. 528–540.
Bouwens, SFM van Heugten, CM & Verhey, FRJ 2009, ‘The practical use of goal attainment scaling for people with acquired brain injury who receive cognitive rehabilitation’, Clinical Rehabilitation, vol. 23, pp. 310–320.
Cicley Saunders Institute 2010a, GAS - Goal Attainment Scaling in Rehabilitation Institute King’s College London, University of London, viewed 28/08/13, <http://www.csi.kcl.ac.uk/gas-tool>
Cicley Saunders Institute 2010b, GAS Calculation Sheet Institute King’s College London, University of London, viewed 28/08/13, <http://www.csi.kcl.ac.uk/files/GAS%20calculation%20sheet.xls>
NSW Ministry of Health n.d., NSW Health Rehabilitation Redesign Project Final Report: Model of Care NSW MoH, viewed 28/08/13
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])

Draft Workbook Page 40 of 1
<http://www.archi.net.au/documents/resources/models/rehab_redesign/rehabilitation-moc.pdf>
NSW/ACT Dementia Training Study Centre n.d., Dementia Education Online: Module 5: Younger Onset Dementia University of Wollongong, viewed 28/08/13, <http://dementia.uow.edu.au/understandingdementiacare/module5/index.htm>
Oades, L Crowe, TP & Nguyen, M 2009, ‘Leadership coaching transforming mental health systems from the inside out: person-centred strengths based coaching psychology’, International Coaching Review, vol. 4, no. 1, pp.25–36.
Oades, L Deane, F Crowe, T Lambert, WG Kavanagh, D & Lloyd, C 2005, ‘Collaborative recovery: an integrative model for working with individual who experience chronic and recurring mental illness’, Australasian Psychiatry, vol. 13, no. 3, pp.279–284.
Royal College of Nursing (RCN) 2007, Maximising potential: the role of the nurse in supporting the rehabilitation of older people RCN, viewed 18/09/13, <http://www.rcn.org.uk/__data/assets/pdf_file/0003/109326/003186.pdf>
Turner-Stokes, L n.d. a, Goal Attainment Scaling (GAS) in rehabilitation: a practical guide King’s College London University of London and The North West London Hospitals NHS Trust, viewed 28/08/13 <http://www.csi.kcl.ac.uk/files/Goal%20Attainment%20Scaling%20in%20Rehabilitation%20%20a%20practical%20guide.pdf>
Turner-Stokes, L n.d. b, Goal Attainment Scaling (GAS) in rehabilitation: the GAS-Light model King’s College London University of London and The North West London Hospitals NHS Trust, viewed 28/08/13 <http://www.csi.kcl.ac.uk/gas-tool>
Further reading
Alzheimer’s Australia (AA) n.d b, Other resources, AA viewed 17/09/13, <http://www.fightdementia.org.au/services/further-reading-and-resources.aspx>
Alzheimer’s Australia (AA) n.d c, Younger Onset Dementia, AA viewed 17/09/13, <http://www.fightdementia.org.au/services/early-or-younger-onset-dementia.aspx>
Ashford, S & Turner-Stokes, L 2006, ‘Evaluation of goal attainment in management of spasticity with botulinum toxin: use of Goal Attainment Scaling to demonstrate functional gains’, Physiotherapy Research International, vol. 11, pp. 14-23.
Beaumont, H 2009, Losing Clive to younger onset dementia: one family's story, Jessica Kingsley, London.
Bovend’Eerdt, TJH Botell, RE & Wade, DT 2009, ‘Writing SMART rehabilitation goals and achieving goal attainment scaling: a practical guide’, Clinical Rehabilitation, vol. 23, pp. 352–361
Bravo, G Dubois, MF & Roy PM 2005, ‘Using Goal Attainment Scaling to improve the quality of long-term care: a group-randomized trial’, International Journal of Qualitative Health Care, vol. 17, pp. 511–519.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])
Draft Workbook Page 41 of 1
Davies-Quarrell, V the ACE Club & Keady, J 2010, 'The ACE Approach: promoting well-being and peer support for younger people with dementia’, Journal of Mental Health Training, Education and Practice, vol. 5, no. 3, pp. 41-50.
Department of Health and Ageing (DoHA) 2007, Dementia Outcomes Suite DoHA viewed 18/09/13, <http://www.dementia-assessment.com.au/>
Department of Health and Ageing (DoHA) 2012, Behaviour Management: a good practice guide: Managing Behavioural and Psychological Symptoms of Dementia DoHA viewed 18/09/13, <http://www.dementiaresearch.org.au/images/dcrc/output-files/328-2012_dbmas_bpsd_guidelines_guide.pdf>
Fisher, K 2008, ‘Assessing clinically meaningful change following a programme for managing chronic pain’. Clinical Rehabilitation vol. 22, pp. 252–259.
Harris, PB & Keady, J 2009, ‘Selfhood in younger onset dementia: Transitions and testimonies,’ Aging & Mental Health, vol. 13, no. 3, pp. 437-444.
Hodges, JR Gregory, C McKinnon, C Kelso, W Mioshi, E & Piguet O 2009, Quality Dementia Care Series: Younger Onset Dementia a practical guide Alzheimer’s Australia, viewed 17/09/13, <http://www.fightdementia.org.au/common/files/NAT/20090200_Nat_QDC_QDC5YODPracGuide.pdf>
Hurn, J Kneebone, I & Cropley, M 2006, ‘Goal setting as an outcome measure: A systematic review’. Clinical Rehabilitation vol. 20, no. 9, pp. 756-72.
Khan, F Pallant, JF & Turner-Stokes, L 2008, ‘Use of Goal Attainment Scaling (GAS) in rehabilitation for persons with Multiple Sclerosis’, Archives of Physical Medicine and Rehabilitation, vol. 89, no. 4, pp. 652-9.
Kiresuk, T & Sherman, RE 1968 ‘Goal Attainment Scaling: a general method for evaluating comprehensive community mental health programs’, Community Mental Health Journal, vol. 4, pp. 443–453.
NSW Ministry of Health (NSW MoH) 2013, Assessment and Management of People with Behavioural and Psychological Symptoms of Dementia (BPSD) A Handbook for NSW Health Clinicians NSW MoH, viewed 18/09/13,<http://www.health.nsw.gov.au/dementia/Publications/assessment-mgmt-people-bpsd.pdf>
Roach, P Keady, J Bee, P & Hope, K 2009, ‘Subjective experiences of younger people with dementia and their families: A review and implications for UK research, policy and practice attention’. Reviews in Clinical Gerontology, vol. 18, pp. 165-174.
Rockwood, K Fay, S & Jarrett, P 2007, ‘Asp E: effect of galantamine on verbal repetition in AD: a secondary analysis of the VISTA trial’, Neurology, vol. 68, pp. 1116–1121.
Schölzel-Dorenbosa, CJM Meeuwsenb, EJ & Rikkert, MGMO 2010, ‘Integrating unmet needs into dementia health-related quality of life research and care: Introduction of the Hierarchy Model of Needs in Dementia’, Aging & Mental Health, vol. 14, no. 1, pp. 113–119.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])

Draft Workbook Page 42 of 1
Turner-Stokes, L Baguley, I De Graff, S McCrory, P Katrak, P Davies, L & Hughes, A ‘Goal attainment scaling in the evaluation of treatment of upper limb spasticity with botulinum toxin: a secondary analysis from a double blind placebo controlled randomised clinical trial’, Journal of Rehabilitation Medicine, vol. 42, no. 1, pp. 81-9, doi: 10.2340/16501977-0474.
Yau, DCN Lam, MCC Lung, MKW Chow, AYH Yung, NSY Chui, TY, et al. 2002, ‘Outcome focused nursing practice in geriatric day-rehabilitation service: facilitating elderly patients to achieve therapeutic goals’, Hong Kong Nursing Journal vol. 38, pp. 33–38.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])

Draft Workbook Page 43 of 1
Responses to Learning Activities
5. Developing, implementing and evaluating an action plan/ care plan using the GAS: Responses
Learning Activity 5: Part i: Responses: Applying the GAS in practice: What is the research evidence that the GAS works for practitioners and clients?
Responses (Learning Activity 5: Part i) Question Response
1. The authors claim that this study has a sample as large as only one other study evaluating the use of the GAS.
a. What was the total sample size at the end of the six months of this study?
40 clients (p. 315 column 2)
b. What was the drop-out rate for this study? 17% (48 started the study p. 315 column 2)
c. For what reasons did clients drop out from this study? Not fully reported in the paper
d. Who were the authors of the study which recruited a similarly large sample size?
Rockwood et al. (p. 316 column 2)
e. What was the year and the journal where this previous study was published?
Reference 15 1997 published in Journal of Clinical Epidemiology (p. 318 column 2)
2. The number of goals set using the GAS has an impact on its effectiveness.
a. What was the mean number of goals completed with clients for this study?
4 (SD±2 i.e. range from 2 to 6) (p. 214 column 1)
b. How does this number compare with the recommended number of goals to be set with clients.
During this module there was guidance on how many goals is considered the optimum by the authors of the GAS and those who have written guidelines on using the GAS.(p. 14)
3. The authors timed the length of time it took clients to identify their goals with practitioners.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])

Draft Workbook Page 44 of 1
Responses (Learning Activity 5: Part i) Question Response
a. What was the mean length of time it took to identify goals?
45 minutes (SD±15) (p. 314, column 1)
b. When it took longer than 30 minutes to set goals what the reasons for this?
Lack of insight, emotional communication problems, problems with specifying goals and having more than three goals (p. 314, column 1)
c. Consider the implications of Question 3b for your work role of these findings and your implementation of the use of the GAS.
4. The authors report on the mean goal attainment levels for the clients who participated in this study.
a. At six months what was the percentage level of attainment for the client goals?
Overall attainment:
• Not attained: 28%
• Attained: 72%
More specifically:
• Much lower than expected: 8%
• Lower than expected: 20%
• Attained: 30%
• Higher than expected: 31%
• Much higher than expected 11%
(p. 316 column 1)
Thus, just under one third of clients attained their goals to a higher level than they had expected to.
b.
5. The practitioners used telephone calls to set goals with clients.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])
Draft Workbook Page 45 of 1
Responses (Learning Activity 5: Part i) Question Response
a. What were consequences of using telephone calls to set goals with clients.
Advantages
• Time efficient;
• Can be used as a follow-up to face-to-face meeting where goals initially discussed;
• It worked when goals set were simple and straight forward; and
• It worked when goals did not require the practitioner to observe outcome.
Disadvantages
• Client reluctant to share intimate feelings over the phone; and
• Cannot work for goal setting where an activity requires direct face-to-face observation.
(p. 317 column 1)
b. Consider what impact these findings will have on whether you use telephone calls with clients and informal carers/ family members to set goals.
6. The authors reported a concern that clients might report socially desirable answers when goal attainment is reviewed (p. 317 column 1).
Consider the consequences of this when setting goals with your clients.
This is a consequence of all goal setting and not unique to the GAS.
7. In some cases the informal carer/ family member contributed to helping the client setting goals (p. 316 column 1 and p. 317 column 2).
Explain how the findings from this research could provide you with insights into what it will be like to use the GAS with your clients and informal carers/ family members.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])
Draft Workbook Page 46 of 1
Responses (Learning Activity 5: Part i) Question Response
8. In the abstract the authors state that having a depressive illness has an impact on whether the use of the GAS is effective.
a. How many clients in this study did the authors find with depressive illness?
N =1 (p. 316 column 2)
b. What is the significance of this finding for your work? This finding should be considered with caution because it only involved n=1. It was surprising to this finding included as a highlight from this study in the abstract because the authors reported this finding for only one participant. Abstracts of studies only include the key findings from a study.
Also, many clients undergoing rehabilitation experience depressive illness and so if the GAS is to be effective an strategy practitioners need to be able to use the GAS effectively with individuals who are experiencing a depressive illness. Individuals living with a depressive illness need to be enabled to set goals as part of their recovery plan.
c. Use the library databases to locate one other research paper in which the GAS is implemented with or at least includes clients with a depressive illness.
9. The authors state that the GAS should not be used on its own but in conjunction with other measures of therapeutic effect (p. 317 column 2) and that specific objective measures are also required to measure the gaol attainment alongside the GAS scores, for example, the distance a client can walk following an intervention (p. 317 column 1).
a. Where in this Module is this approach discussed. On p. 16 the example of using a pain assessment scale is used as an additional way to measure goal attainment alongside the GAS score.
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])

Draft Workbook Page 47 of 1
Responses (Learning Activity 5: Part i) Question Response
b. What examples from your practice can you think of which will require you to use another assessment tool/ additional criteria to evaluate the outcome of
GAS: YOD: Learning Activity 5(i) Responses: August 2013 ([email protected])

Draft Workbook Page 48 of 1
5. Developing, implementing and evaluating an action plan/ care plan using the GAS: Responses
Learning Activity 5: Part ii: Applying the GAS in practice: What is the research evidence it works?: Responses Table 6: List of potential goals generated from a workshop when Hugh’s story was shown to dementia care practitioners
Goals (potential list generated as responses to Learning Activity 5(ii) Hugh’s goals Wife’s goals Children’s goals
• Continue living in the care home where I moved to from my home
• Continue staying connected to Hugh • Be a source of music making for dad
• Keep physically active with incidental physical activity
• Maintaining my physical health • Be a memory maker for dad to record his life so far and his life into the future
• Start a gym programme for my exercise
• Better manage the stress associated with caring for Hugh
• Be a support for mum in her caring role
• Listening to music to suit my mood • Find time to fit in enjoyable everyday activities
• Help mum manage everyday tasks that dad used to do or mum no longer has time for
• Enjoying day trips • Maintain my social networks • Manage the grief associated with having a dad living with younger onset dementia
• Maintaining independence at meal times
• Learn more about dementia • Manage the juggling act of doing studies, maintaining own social network and supporting mum and dad
• Spending time with and being a part of my family
• Start planning for future needs and organising the legal documents I will need
• Be a support for my siblings and how they manage with having dad who has a younger onset dementia
• Being a part of my community • Find out from Hugh, before it is too late, what he wants to happen to him if/ when he becomes less able to tell us what he wants
• Create joyful moments for dad
GAS: YOD: Learning Activity 5(ii) Responses: August 2013 ([email protected])

Draft Workbook Page 49 of 1
Goals (potential list generated as responses to Learning Activity 5(ii) Hugh’s goals Wife’s goals Children’s goals
• Finding new ways to express my views and opinions about what I want to do
• Make sure the care home where Hugh lives know what he needs and what he likes
• Create joyful moments for different family members to join in with dad
• Choosing the music I listen to • Adjust to my changing relationship with Hugh as a wife who has a husband living with a dementia
•
• Playing a musical instrument • •
• Singing • •
• Joining my family on outings • •
• Ensuring my family can visit me when it suits them
• •
• Have intimate moments with my wife • •
• Stay connected to my children • •
GAS: YOD: Learning Activity 5(ii) Responses: August 2013 ([email protected])