early prediction of pre-eclampsia
TRANSCRIPT

PREECLAMPSIAAnswers to Questions
and Questions to Answer
Professor Shaun BrenneckeDepartment of Maternal-Fetal Medicine
University of Melbourne Department of Obstetrics GynaecologyRoyal Women’s Hospital
Parkville, Victoria, Australia

Declaration of conflicts of interest
Name: Shaun Brennecke
Preeclampsia research findings from my department described in this presentation have been supported within the past 5 years by:
Roche Diagnostics (Preeclampsia Biomarker Research)
Australian NHMRC (Other Preeclampsia Research)



BIRTHS IN AUSTRALIA
• Population of Australia = 25 million
• Total annual births in Australia = 300,000 +
• 6.5% of babies born are low birthweight (<2,500 g)
• 8.6% of babies are pre-term (< 37 weeks)
• 1:10 women have gestational diabetes
Australian Bureau of Statistics/Australian Institute of Health and Welfare

Melbourne is the capital city of Victoria, a state of 230,000 square kilometresThe border regions of Victoria are up to 550 kilometres from Melbourne

Royal Women’s Hospital, Melbourne
THE ROYAL WOMEN'S HOSPITAL Melbourne
Opened in 1856
First public hospital for women in Australia
Currently - Annual births = 7,600 +
- Primipara = 4,200 +
- Babies born (>20 weeks) = 7,780 +
- Babies admitted to SCN = 2,000 +
RWH Birth outcomes
• Normal birth rate (NVB) = 51%
• Forceps rate = 13.5%
• Vacuum rate = 6.7%
• Vaginal breech rate = 0.7%
• Caesarean rate = 28.5%
• Induction of Labour rate = 36.1%
• Augmentation with oxytocic rate = 26.1%
• PPH > 1500 mls = 2.1%
• Neonatal death rate = 0.5%
PREECLAMPSIA
is the most common serious medical disease of human pregnancy
with an incidence of 1-5% in most parts of the world

PREECLAMPSIA
SIGNIFICANCE
WORLDWIDE …..
A mother dies every 8 minutes
from
complications of pre-eclampsia
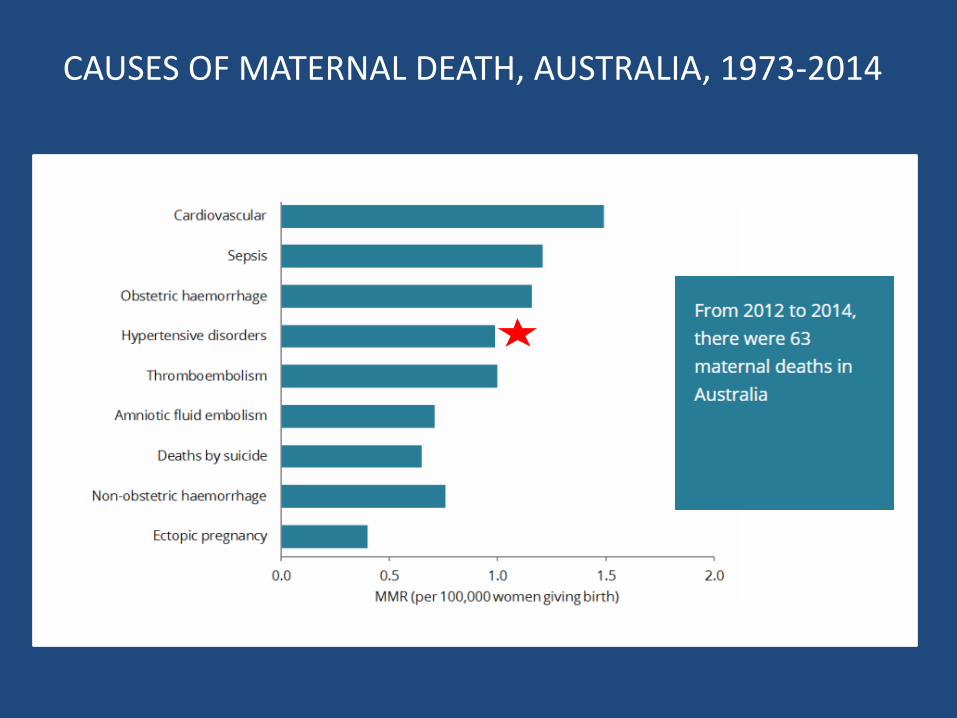
CAUSES OF MATERNAL DEATH, AUSTRALIA, 1973-2014

Diagnosis
Prediction
Prevention
Management
Prognosis
PREECLAMPSIAAnswers to Questions
and Questions to Answer

WHAT IS
PREECLAMPSIA?

“Preeclampsia is a disease of theories”
Paul ZweifelGerman Obstetrician
1916
Pregnancy Hypertension 2018, 72(1):24-43
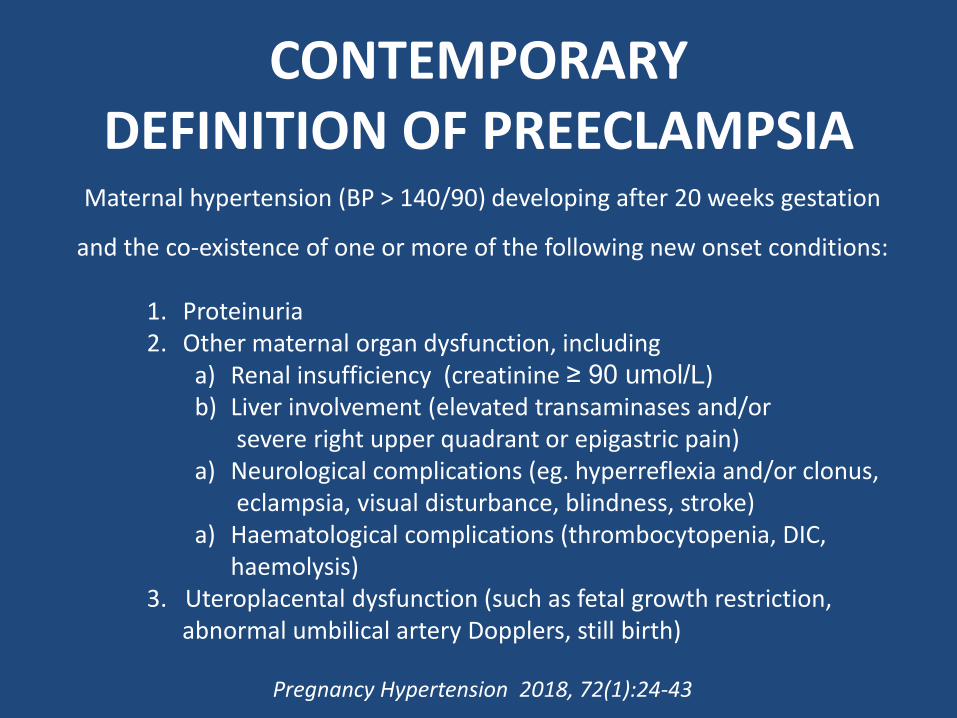
Maternal hypertension (BP > 140/90) developing after 20 weeks gestation
and the co-existence of one or more of the following new onset conditions:
1. Proteinuria2. Other maternal organ dysfunction, including
a) Renal insufficiency (creatinine ≥ 90 umol/L)b) Liver involvement (elevated transaminases and/or
severe right upper quadrant or epigastric pain)a) Neurological complications (eg. hyperreflexia and/or clonus,
eclampsia, visual disturbance, blindness, stroke)a) Haematological complications (thrombocytopenia, DIC,
haemolysis)3. Uteroplacental dysfunction (such as fetal growth restriction,
abnormal umbilical artery Dopplers, still birth)
Pregnancy Hypertension 2018, 72(1):24-43
CONTEMPORARY DEFINITION OF PREECLAMPSIA

PREECLAMPSIA
CONCEPTION
PREECLAMPSIA A CLINICAL SYNDROME
WITH MANY PATHOGENETIC PATHWAYS
SYNDROME
Greek derivation meaning “concurrence”
A set of clinical signs and symptoms that are correlated with each other
A syndrome can be very closely correlated with an aetiology or pathogenesis e.g. Down syndrome,
or it may be not specific to only one disease

WHAT IS THE “GOLD STANDARD” FOR DIAGNOSING PREECLAMPSIA?
PREECLAMPSIA
ABNORMAL PLACENTATION

SPIRAL ARTERIOLES IN NORMAL AND “PREECLAMPTIC” PREGNANCIES
- EXTENT OF TROPHOBLAST INVASION ( ) -

PREECLAMPSIA IS A MULTISYSTEM DISORDER
PREECLAMPSIA IS A SYNDROME

Maynard SE et al. J Clin Invest (2003)
MATERNAL CIRCULATING sFlt-1 IS ABNORMALLY HIGH IN PREECLAMPSIA
SOLUBLE FMS-LIKE TYROSINE KINASE-1 (sFlt1)
• Tyrosine kinase protein that disables proteins that cause blood vessel growth
• Splice variant of the VEGF receptor 1
• Also known as sVEGFR-1
• Binds and reduces free circulating levels of proangiogenic factors VEGF and PlGF
• Blunts beneficial effects of VEGF and PlGF on maternal vascular endothelium
• Expressed in and released from placental tissue
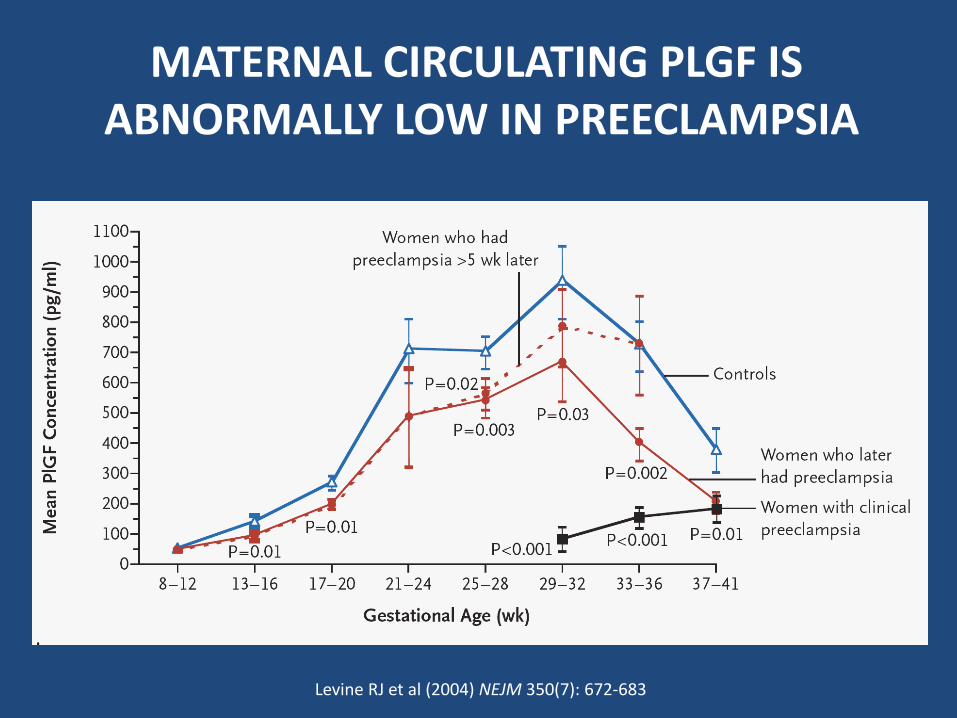
MATERNAL CIRCULATING PLGF IS ABNORMALLY LOW IN PREECLAMPSIA
Levine RJ et al (2004) NEJM 350(7): 672-683

PLACENTAL GROWTH FACTOR (PlGF)
• Key protein in angiogenesis and vasculogenesis
• Member of the vascular endothelial growth factor (VEGF) sub-family
• Main source during pregnancy is the placenta

PREECLAMPSIA IS A PLACENTAL DISORDER

MATERNAL VASCULAR DYSFUNCTION IN PREECLAMPSIA
Benzing T. Nature Reviews Nephrology (2016)

VASCULAR DYSFUNCTION IN PREECLAMPSIA
Ahmed A and Cudmore MJ. Biochemical Society Transactions (2009) 37, 1237-1242

sFLT-1/PlGF RATIO
A Test of Placental Dysfunction

Schoofs K et al. J Perinat Med (2014)
sFlt-1/PlGF RATIO AND PREGNANCY OUTCOME

Can preeclampsia be diagnosed
pathognomonicallyusing the sFlt-1/PlGF ratio test?
QUESTION TO ANSWER
CAN PREECLAMPSIA
BE PREDICTED?
De
tectio
n r
ate
P
E fo
r F
PR
10
%0
10
20
30
40
50
60
70
80
90
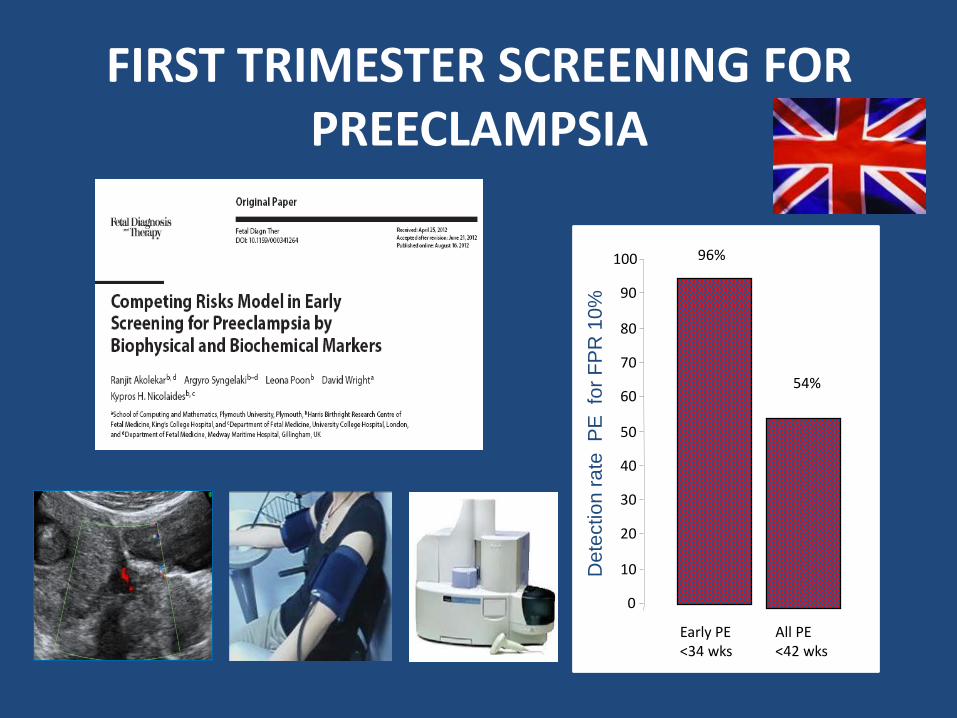
100 96%
54%
Early PE <34 wks
All PE<42 wks
FIRST TRIMESTER SCREENING FOR PREECLAMPSIA
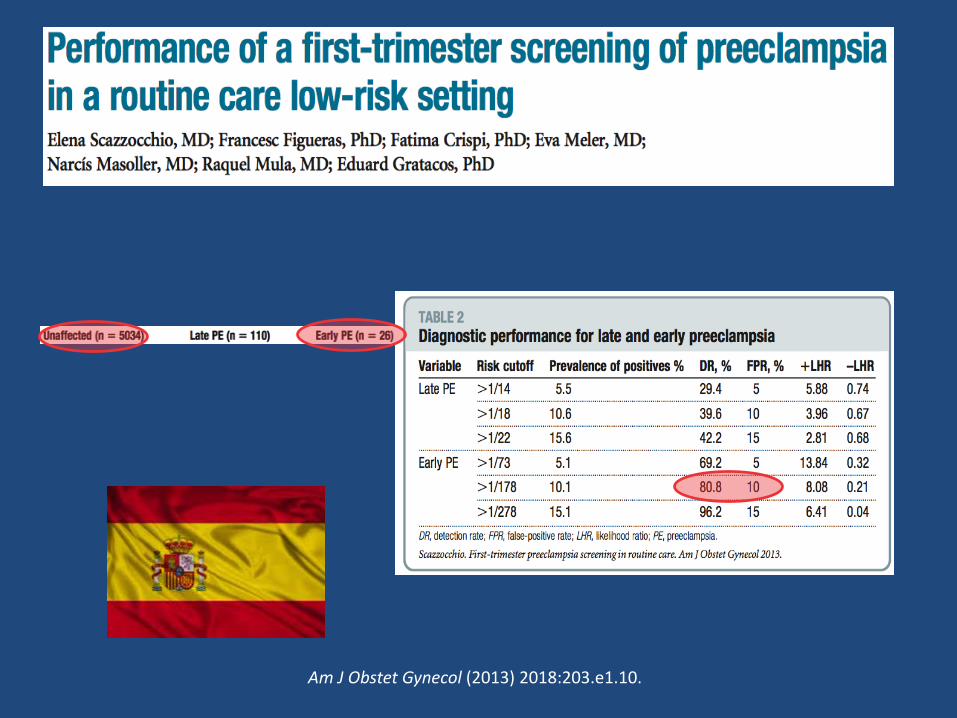
Am J Obstet Gynecol (2013) 2018:203.e1.10.

Prof Jon Hyett
Sample 3066


The PROGNOSIS Study
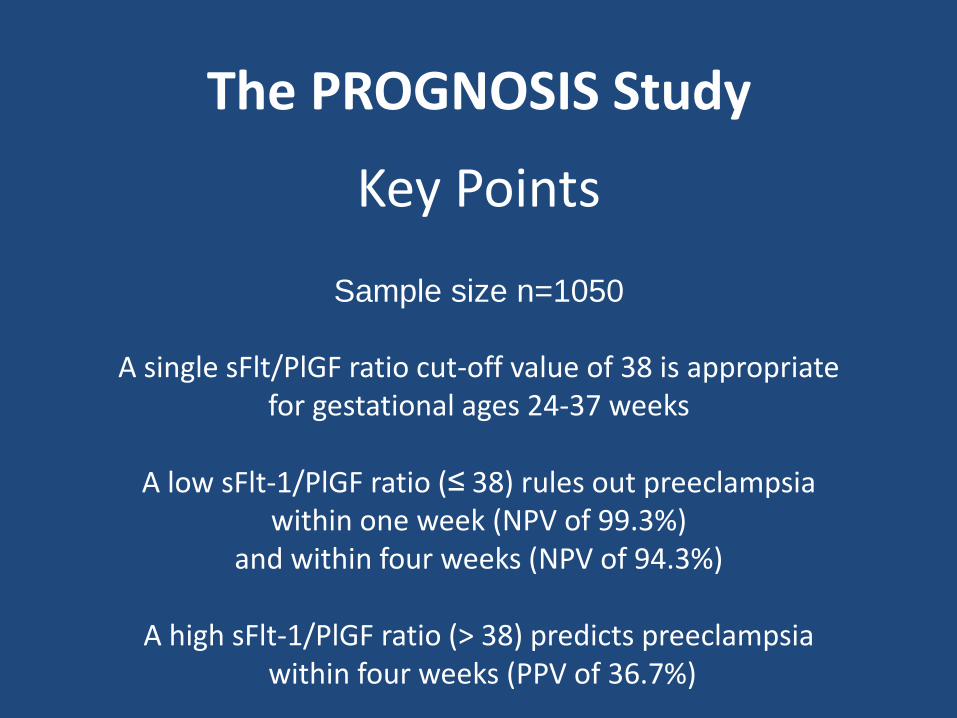
Key Points
Sample size n=1050
A single sFlt/PlGF ratio cut-off value of 38 is appropriate for gestational ages 24-37 weeks
A low sFlt-1/PlGF ratio (≤ 38) rules out preeclampsia within one week (NPV of 99.3%)
and within four weeks (NPV of 94.3%)
A high sFlt-1/PlGF ratio (> 38) predicts preeclampsiawithin four weeks (PPV of 36.7%)
The PROGNOSIS Study
sFLT-1/PlGF
Prediction (Differential) Diagnosis
Progression
sFLT-1/PlGF is a test not a treatment

“ Whether or not patients are better off from undergoing a diagnostic test
will depend on how test information is used to guide subsequent decisions
on starting, stopping or modifying treatment”
Ben Mol et al Semin Reprod Med (2003) 21(1):17-25
Can further studies evaluating the use of biomarkersimprove the ability to predict and manage preeclampsia?
Can the further use of biomarkersminimise observer bias and user error,
and increase clinician confidence in their use?
Can using biomarkers as inclusion criteria for clinical trials assessing preeclampsia interventions
help identify those at highest risk and thereby better target those most likely to benefit?
QUESTIONS TO ANSWER
CAN PREECLAMPSIA
BE PREVENTED?


Combined Multi-Marker Screening and Randomised Patient Treatment with Aspirin for Evidence-Based Preeclampsia Prevention


Am J Obstet Gynecol. (2017) Feb;216(2):110-120.e6.

Am J Obstet Gynecol. (2017) Feb;216(2):121-128.e.2.


LDA DECREASES sFLT1/PlGF RATIO IN PE SERA TREATED BeWo CELLS



QUESTIONS TO ANSWER
Low dose Aspirin…
How much?When?
Mechanism(s)?What time?

DOESANTENATAL
CAREIMPROVE
MORBIDITY AND MORTALITY FROM
PREECLAMPSIA?


DECREASING PREECLAMPSIA MORTALITY
Historical Perspective
Dr John Ballantyne1861-1923
Edinburgh PerinatologistApostle of Antenatal Care

PREECLAMPSIA
Historically, the primary medical justification
for antenatal care


DECREASING PREECLAMPSIA MORTALITY
Historical Perspective

Cause 1935 1950 1950 as a percentage of 1935
Toxaemia 7.8 2.6 33.3
Maternal mortality rates per 10,000 births.
Source: A. Macfarlane and M. Mugford, Birth Counts: Statistics of Pregnancy and Childbirth (London, 1984), ii. 276-7.
DECLINE IN PREECLAMPSIA MATERNAL MORTALITY ENGLAND AND WALES
1935-1950
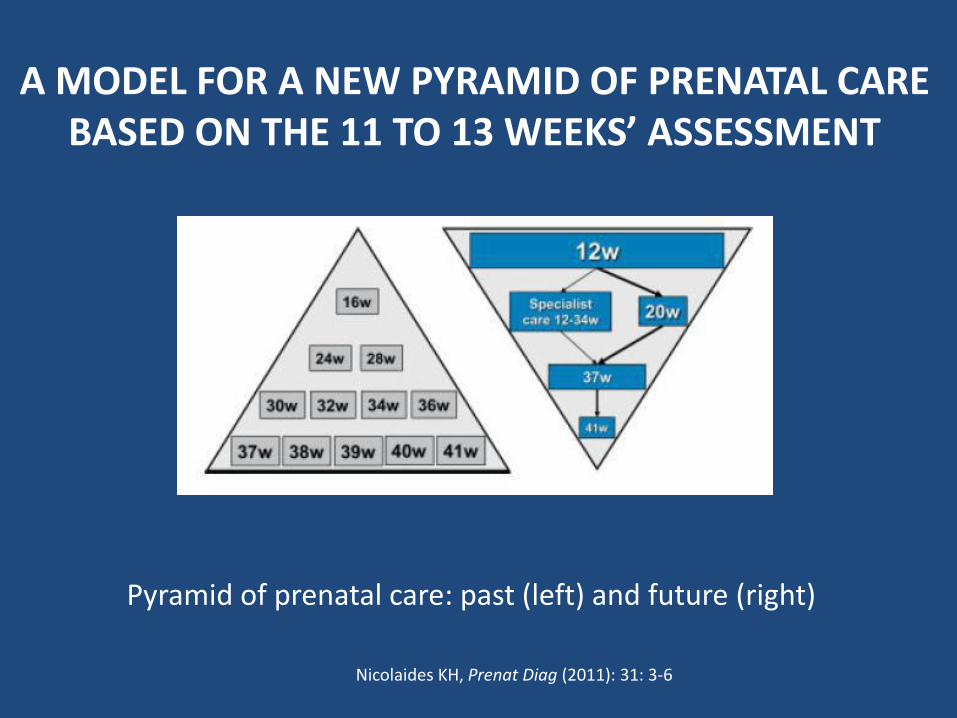
Nicolaides KH, Prenat Diag (2011): 31: 3-6
Pyramid of prenatal care: past (left) and future (right)
A MODEL FOR A NEW PYRAMID OF PRENATAL CAREBASED ON THE 11 TO 13 WEEKS’ ASSESSMENT

Is there a better pregnancy care model?
Can we reverse the over-medicalisation of pregnancy that has evolved since the start of antenatal care?
QUESTIONS TO ANSWER
Do we now have the potential to provide the right care to the right woman at the right time
by improving risk assignment so as to minimise false positives and false negatives,
by reducing direct and indirect costs to the health system and society
via the more efficient use of expensive resources by optimising patient access to management
that is targeted and ultimately improves outcomes by preventing disease early in its development?
QUESTIONS TO ANSWER

DOES PREECLAMPSIA
IMPACT ON
LATER LIFE MATERNAL
HEALTH?

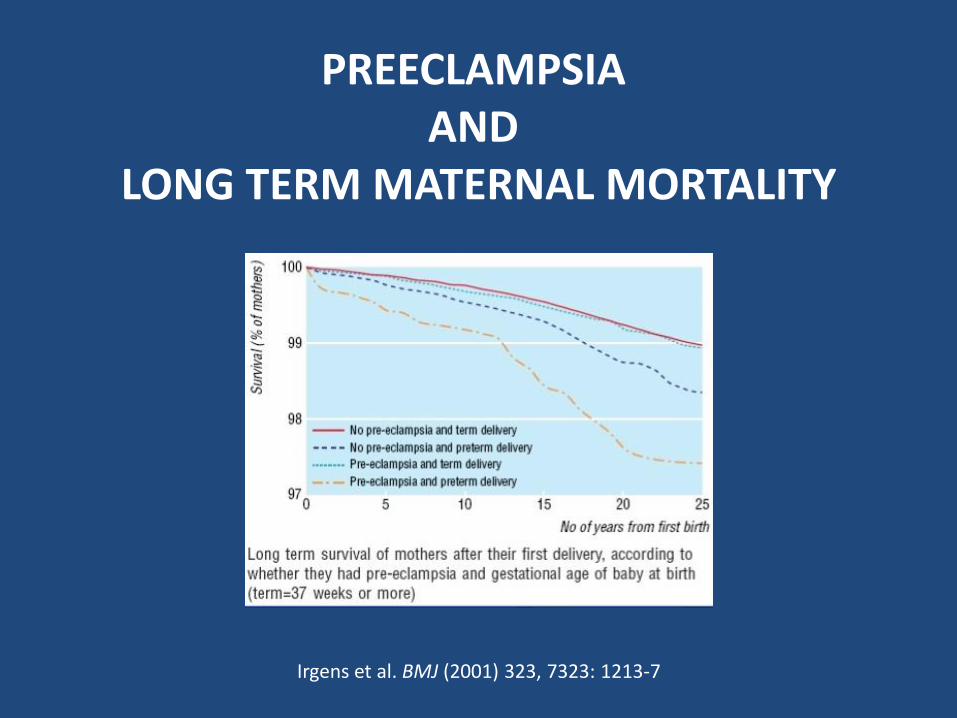
PREECLAMPSIA AND
LONG TERM MATERNAL MORTALITY
Irgens et al. BMJ (2001) 323, 7323: 1213-7
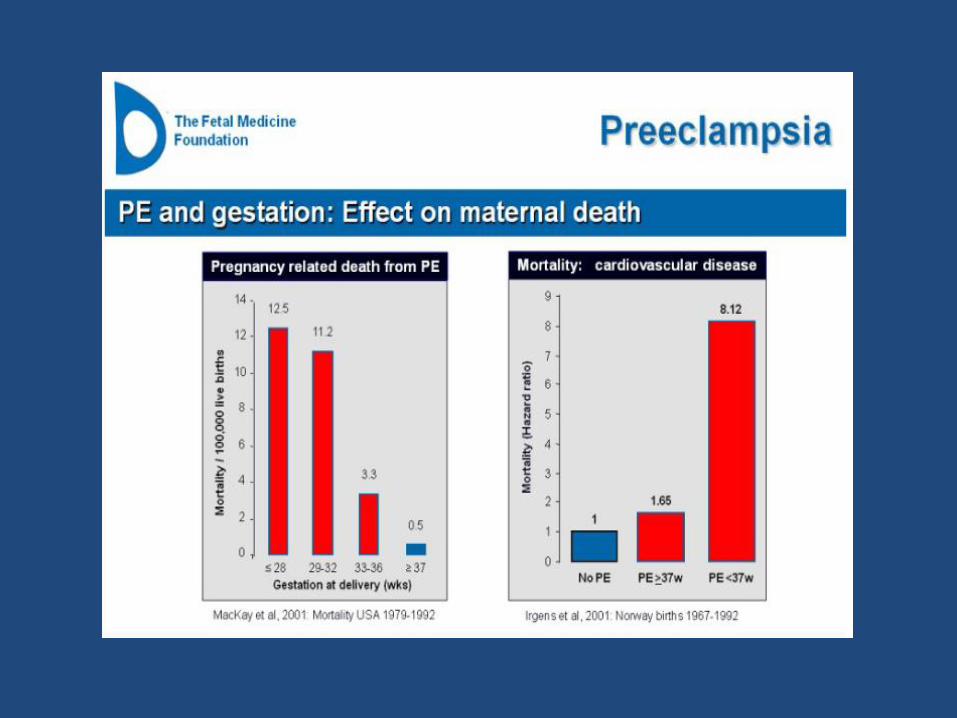
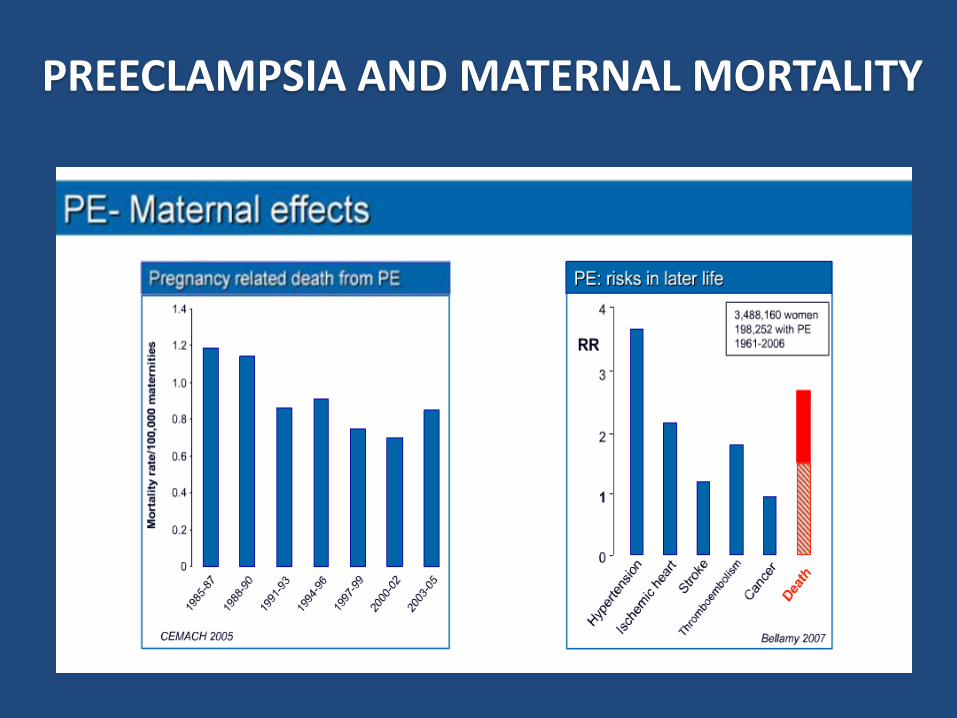
PREECLAMPSIA AND MATERNAL MORTALITY


"There are very few identified risk factors
for later life heart disease in women;
preeclampsia is one of the few warning signs we'll get and we should take advantage of it"
Eleni Tsigas,
Executive Director,
Pre-eclampsia Foundation

Female Sex and Cardiovascular Disease Risk Factors
LIFE LONG SURVEILLANCE OF CARDIOVASCULAR HEALTH
Weight
Exercise
Diet
Blood Lipids
Blood Pressure
Smoking
Diabetes Screening
Alcohol
Depression and Stress
LINKING PREECLAMPSIA AND SUBSEQUENT INCREASED RISK OF
LATER LIFE CARDIOVASCULAR DISEASE…
PREECLAMPSIA
Genetic Predisposition
Percentage of preeclamptic women among relatives of index women
Daughters 23.8%Daughters-in-law 6.5%
Mothers 15.9%Mothers-in-law 4.4%
Cooper, Brennecke and Wilton (1993) J Hyperten Preg 12(1), 1-23


Can we use the known linkbetween preeclampsia and
long term morbidity and mortality risk to improve health outcomes
for women and their offspring?
QUESTION TO ANSWER
Are we close to a revolutionary opportunity
for a new paradigm of pregnancy care
which will lead to a life time benefit for mothers and their babies
and an improvement in the health of the population as a whole?
IN CONCLUSION….
THANK YOU FOR YOUR ATTENTION!
ANY QUESTIONS?
