ecg for interns uci internal medicine mini-lecture
TRANSCRIPT
ECG for InternsUCI Internal Medicine Mini-Lecture
Learning Objectives
• Establish Consistent Approach to Interpreting ECGs
• Review Essential Cases for New Interns
• Provide Additional Resources for Future Learning
ECG Interpretation
What is your approach to reading an ECG?•Rate •Rhythm•Axis•Hypertrophy•Intervals•P wave•QRS complex•ST segment – T wave
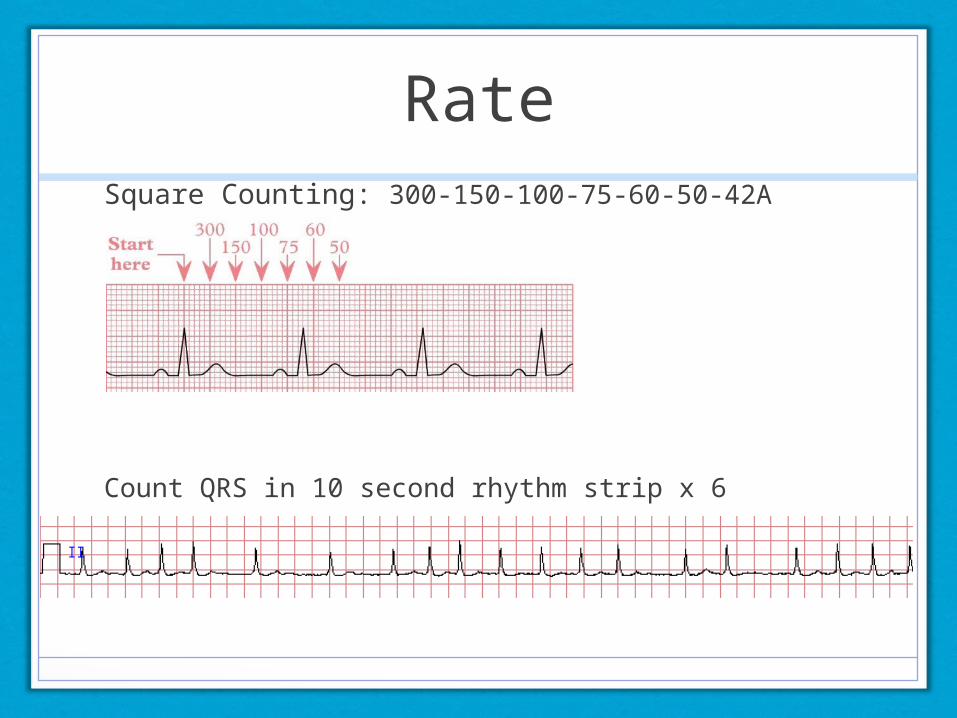
RateSquare Counting: 300-150-100-75-60-50-42A
Count QRS in 10 second rhythm strip x 6
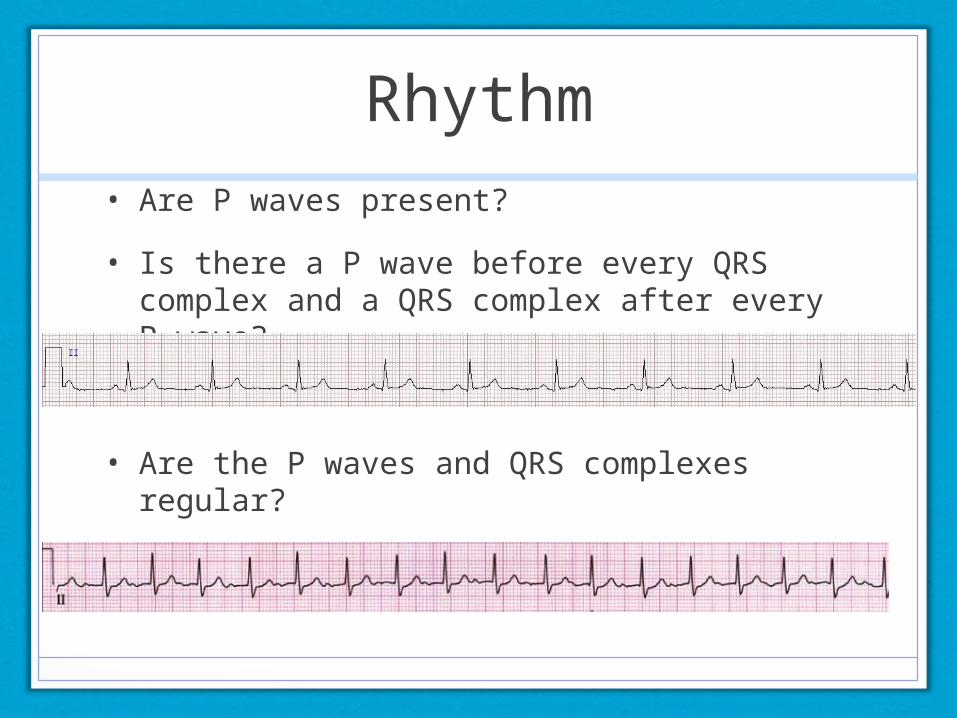
Rhythm• Are P waves present?
• Is there a P wave before every QRS complex and a QRS complex after every P wave?
• Are the P waves and QRS complexes regular?
• Is the PR interval constant?
Axis
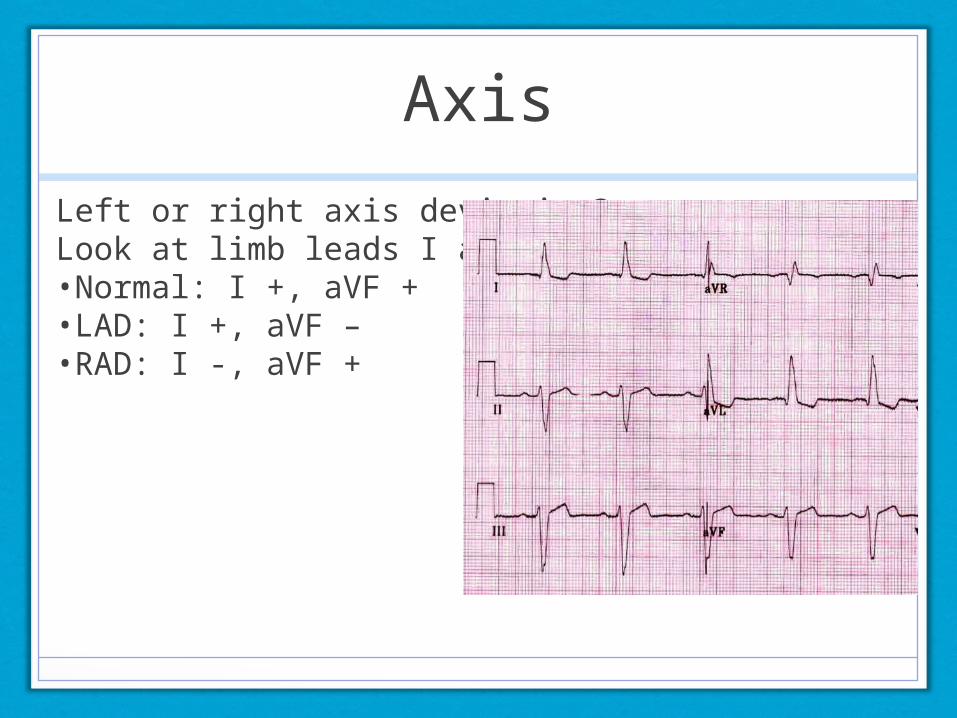
Left or right axis deviation?Look at limb leads I and aVF.•Normal: I +, aVF + •LAD: I +, aVF – •RAD: I -, aVF +
Hypertrophy
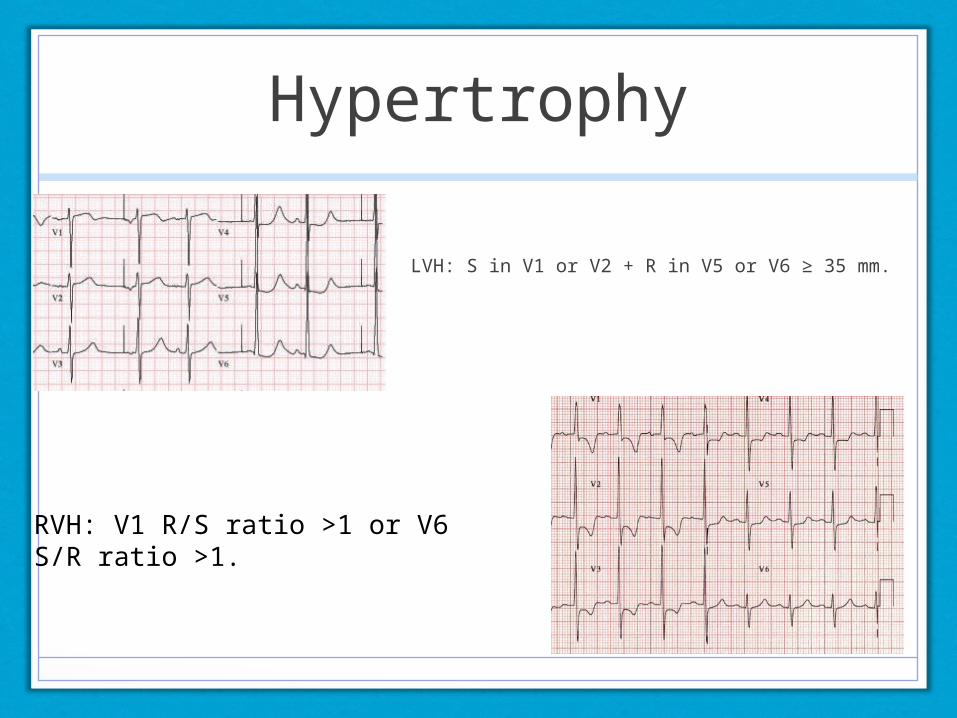
LVH: S in V1 or V2 + R in V5 or V6 ≥ 35 mm.
RVH: V1 R/S ratio >1 or V6 S/R ratio >1.
Intervals
What is the normal PR interval?
•0.12 to 0.20 s (3 - 5 small squares). Short PR – Look for Wolff-Parkinson-White. Long PR – 1st Degree AV block
What is the normal QRS?
•< 0.12 s duration (3 small squares). Long QRS - look for bundle branch block, ventricular pre-excitation, ventricular pacing or ventricular tachycardia
What is the normal QTc (QT/square root of RR)?
•< 0.42 s. Long QTc can lead to torsades to pointes.
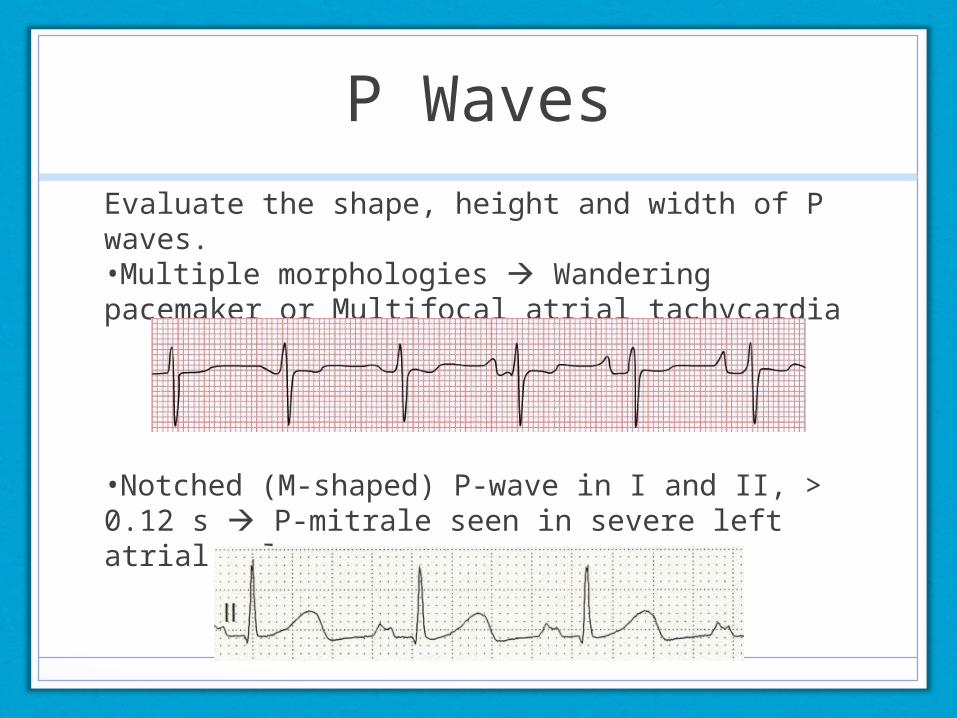
P Waves
Evaluate the shape, height and width of P waves. •Multiple morphologies Wandering pacemaker or Multifocal atrial tachycardia
•Notched (M-shaped) P-wave in I and II, > 0.12 s P-mitrale seen in severe left atrial enlargement

QRS complexPoor R Wave Progression in V1 to V6: suggests prior anterior MI
Pathologic Q wave: previous MI. Q wave amplitude 25% or more of the subsequent R wave, OR > 0.04 s in width + > 2 mm in amplitude in more than one lead
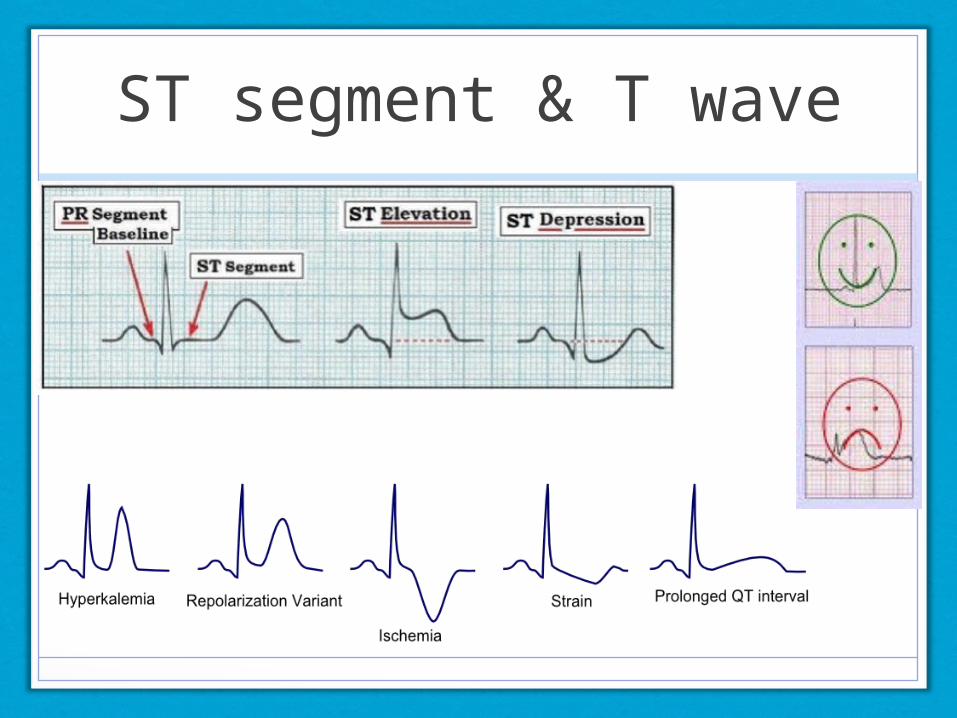
ST segment & T wave
Case #1
70 year old male with history of diabetes mellitus and hypertension occasionally feels lightheaded. He recently fainted while standing.
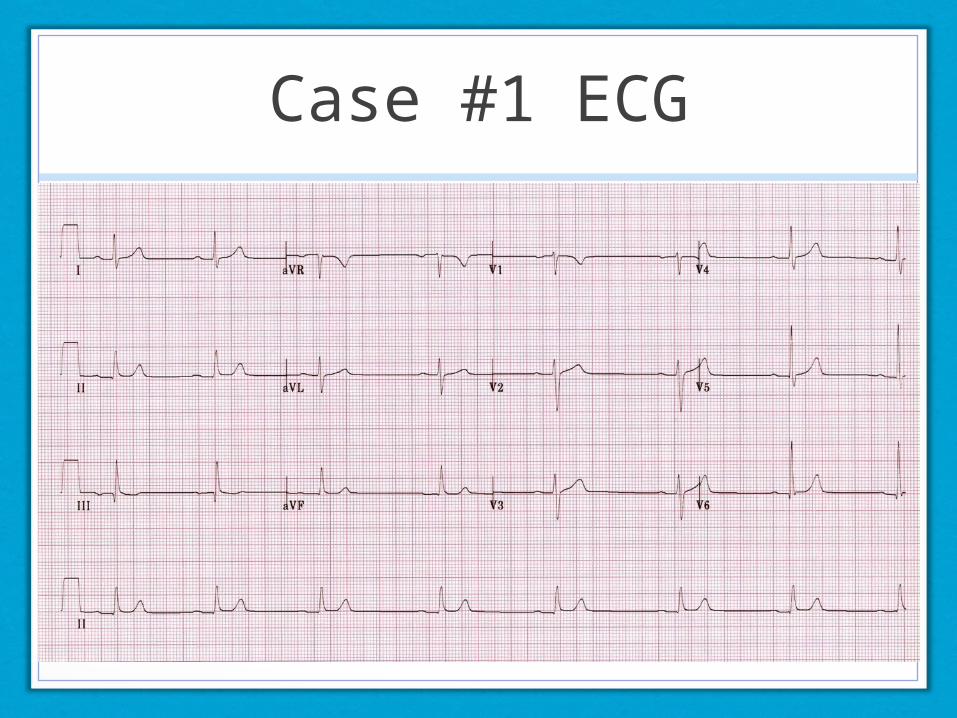
Case #1 ECG
Case #2
58 year old female with no significant past medical history presents with fatigue, lightheadedness and shortness of breath.
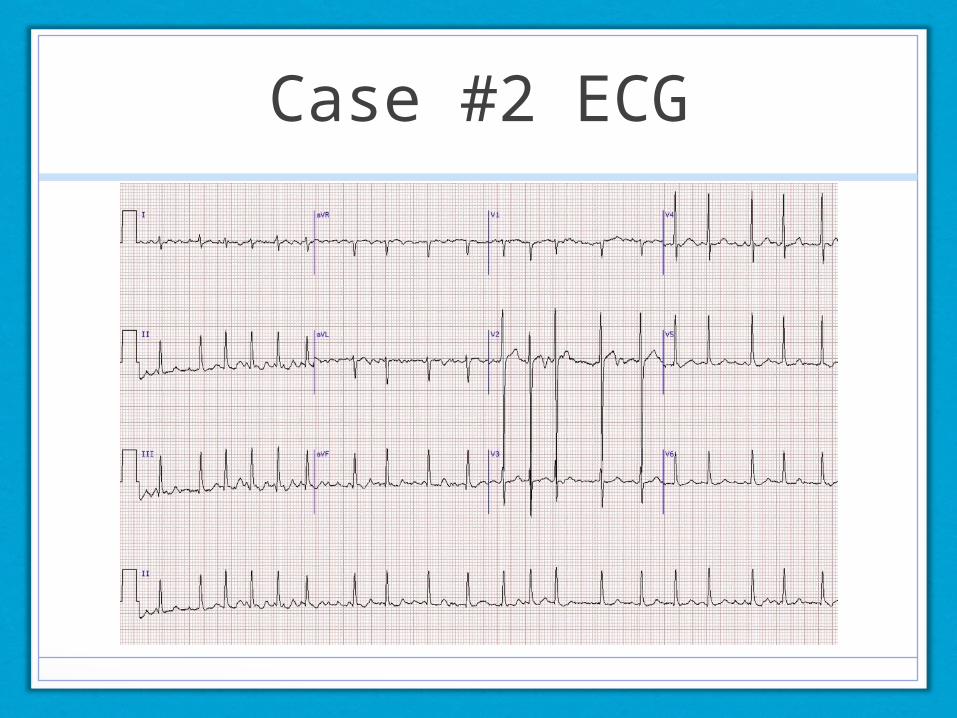
Case #2 ECG
Case #3
78 year old female with history of HTN, DM, HL, CAD admitted for syncope complains of palpitations and lightheadedness.
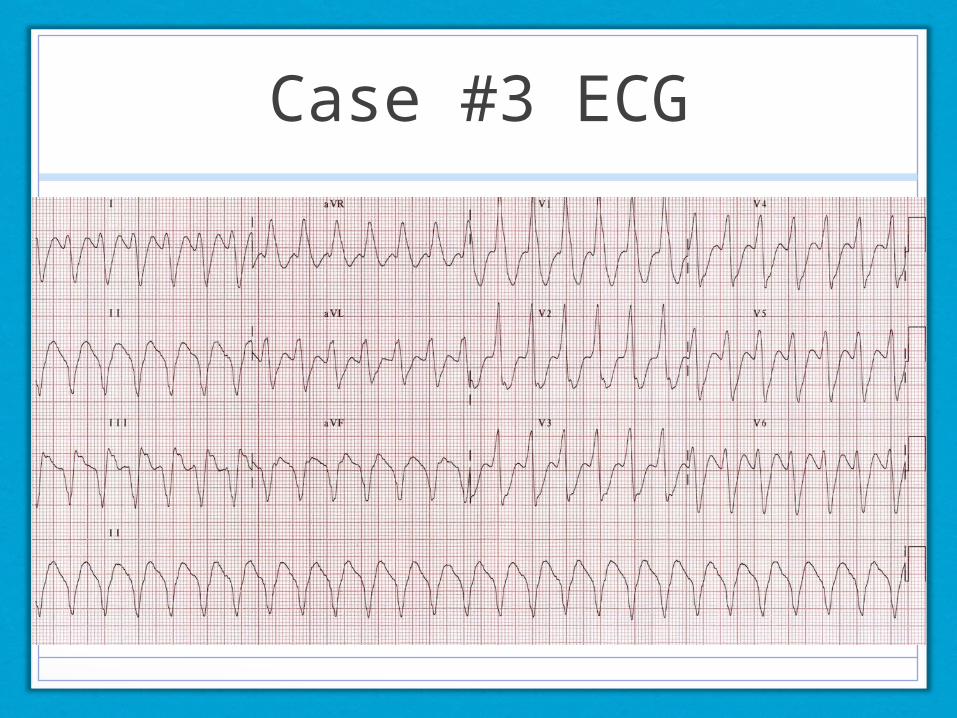
Case #3 ECG
Case #4
67 year old male with history of diabetes, hypertension, COPD presents with chest pain.
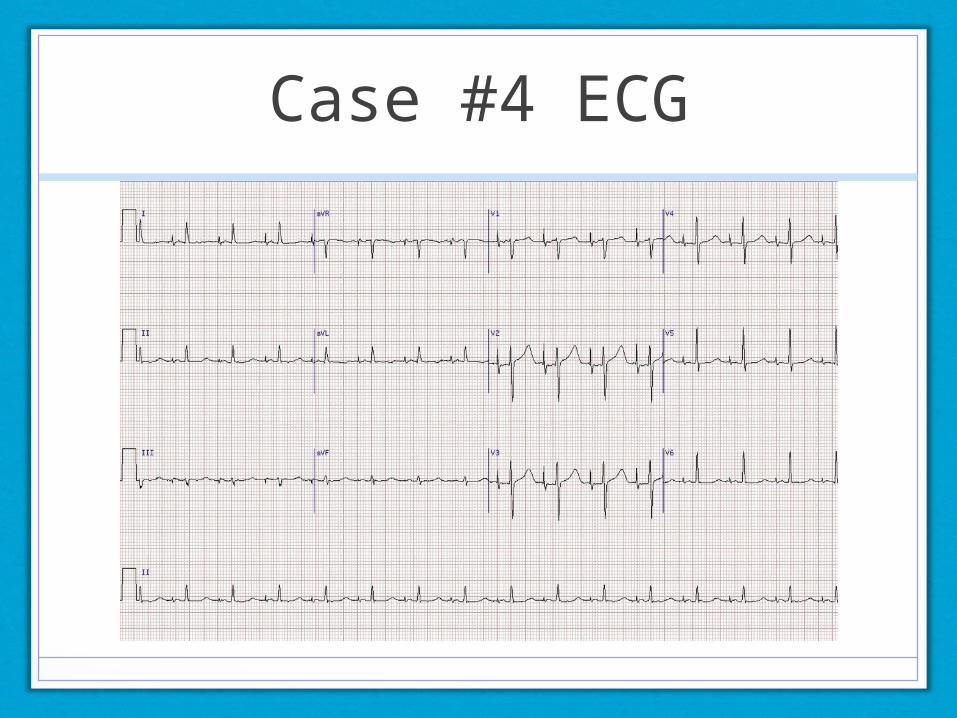
Case #4 ECG
Case #5
38 year old female with history of DM, HTN, CKD presents with 2 days of nausea and abdominal pain.
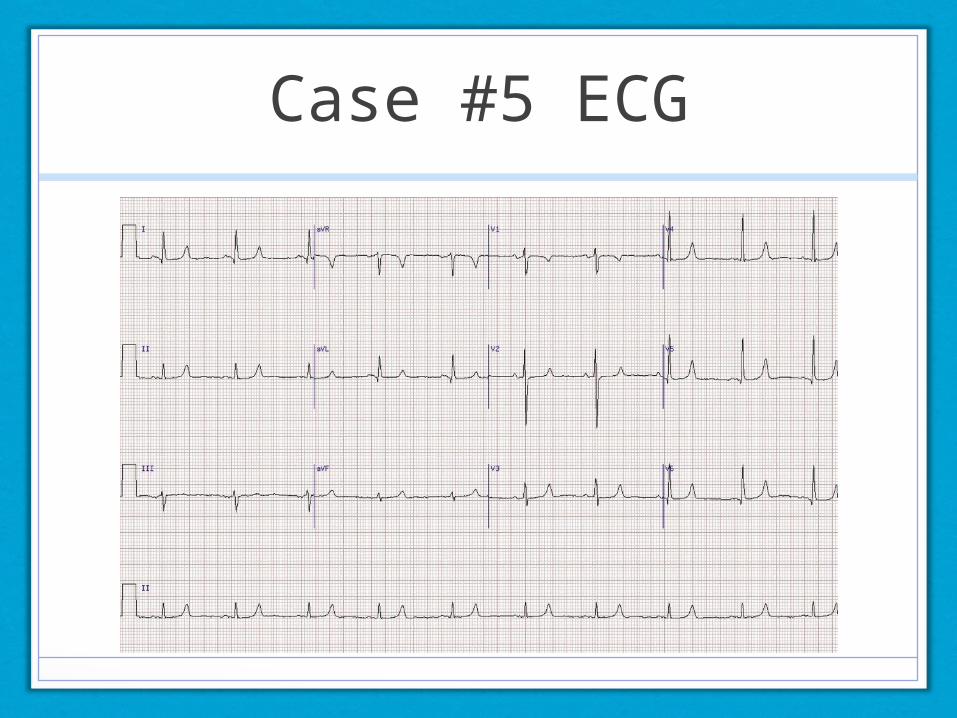
Case #5 ECG
Case #6
60 year-old man with history of HTN, HL, CAD presents with nausea, shortness of breath and chest pain.
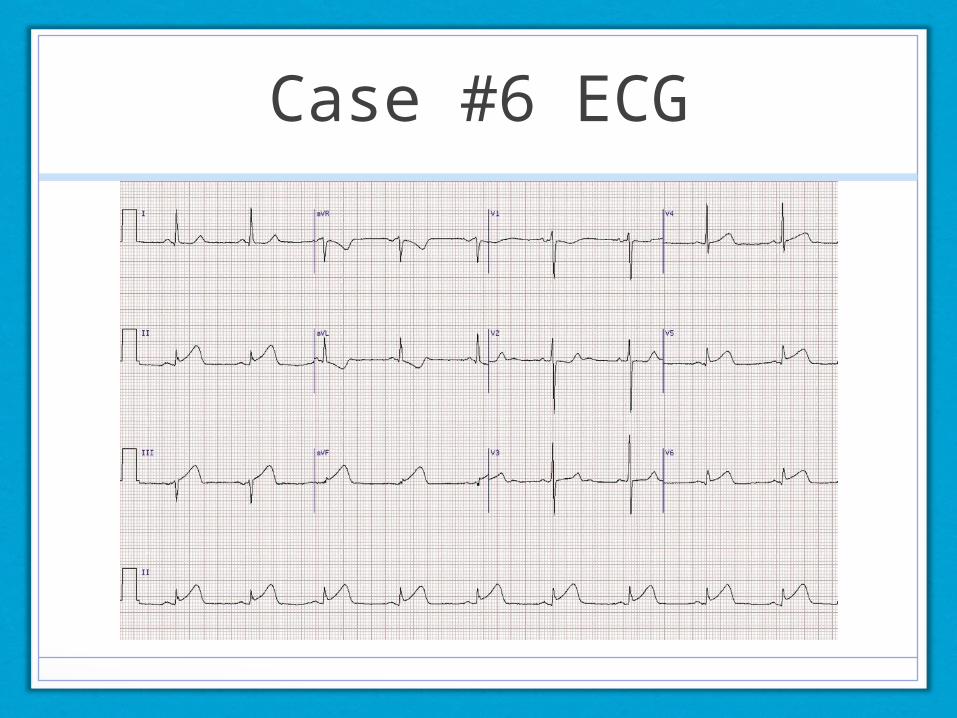
Case #6 ECG
Additional Resources
Websites:•http://en.ecgpedia.org/•http://ecg.utah.edu•http://ecg.bidmc.harvard.edu/maven/
Apps:•ECG Guide by QxMD (iPad and iPhone)•ECG Interpret (iPhone)
Books: •12-Lead ECG: The Art of Interpretation, Tomas Garcia (perhaps the best book on ECGs with detailed explanations and physiology.)•Arrhythmia Recognition, Tomas Garcia
Summary
• Always keep a consistent approach.
• Do not rely upon machine reads.
• Practice makes perfect.