ecg monitoring - st segment monitoring - ajcc 1999
DESCRIPTION
cardiologyTRANSCRIPT

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
1 of 20 4/10/2006 9:33 AM
American Journal of Critical Care American Journal of Critical Care Home
NOVEMBER 1999 - VOLUME 8 - NUMBER 6wew
Take The CE TestCONSENSUS STATEMENT FOR PRACTICEMultilead ST-Segment Monitoring in Patients With Acute Coronary Syndromes: A Consensus Statement for Healthcare ProfessionalsBarbara J. Drew and the ST-Segment Monitoring Practice Guideline Working GroupAbout the AuthorsBy Barbara J. Drew, RN, PhD, (Chair) and Mitchell W. Krucoff, MD, (Co-chair) for the ST-Segment Monitoring Practice Guideline International Working Group.* From the School of Nursing, University of California, San Francisco, Calif (BJD). All members of the ST-Segment Monitoring Practice Guideline International Working Group are listed in the Acknowledgments. This article originally appeared in the November 1999 issue of the American Journal of Critical Care, Vol 8, No. 6, pp372-386.
Reprint requests: InnoVision Communications, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 515); fax, (949) 362-2022; e-mail, [email protected].
In patients with acute coronary syndromes (unstable angina, ST elevation and non–STelevation myocardial infarction), the goal of pharmacological and catheter-basedinterventions is to reverse ongoing ischemia and to prevent or interrupt myocardial celldeath. For patients with acute myocardial infarction, early reperfusion and sustainedpatency of the culprit artery are important determinants of survival.1
Thus, continuous monitoring of the status of the culprit artery is mandatory to tailor appropriate therapy for each patient.2 Although coronary angiography reveals vesselanatomy at a brief moment in time, electrocardiographic (ECG) monitoring reflectsmyocardial physiology continuously, both during normal periods and during ischemia. Thus,the ECG provides a more accurate assessment of the myocardium than does angiographyin situations in which vessel patency has been restored but ischemia persists because of“no reflow” or reperfusion injury. Moreover, currently, ECG monitoring is the only practicalway to detect recurrent or transient ischemic events over time.
ECG monitoring is more sensitive than patients’ symptoms for detecting transientmyocardial ischemia because 80% to 90% of ECG-detected episodes are clinicallysilent.3-10 Asymptomatic changes in the ST segment in a patient with known coronary artery disease are a well-established and highly specific indication that the patient is experiencing transient myocardial ischemia. Moreover, compelling data from independent cohorts of patients consistently indicate unfavorable outcomes among patients who have such ST changes during continuous ECG monitoring after episodes of unstable angina4,5,7,11-14 or myocardial infarction.15-21

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
2 of 20 4/10/2006 9:33 AM
To date, no large-scale, well-controlled clinical trial has been done to prove that hospital treatment based on the results of ST-segment monitoring improves outcomes in patients with acute coronary syndromes. However, because of the prognostic importance of ischemic events detected with ST-segment monitoring, patients with acute coronary syndromes most likely would benefit from early detection and treatment of ischemia. Accurate detection of ischemic events is especially important in current clinical practice because a variety of recently developed treatment options are available, including new reperfusion strategies, new anticoagulant and antiplatelet agents, and innovative catheter-based techniques.
Although software for ST-segment monitoring is widely available in commercial bedside cardiac monitors, it is not often activated by healthcare professionals for patients with acute coronary syndromes treated in emergency departments, cardiac catheterization laboratories, intensive cardiac care units, or step-down telemetry units. Underuse of ST-segment monitoring appears to stem from 2 general sources: (1) technical problems with noise levels and lack of adequate equipment for accurate ST-segment analysis; and (2) a lack of clarity about how information about changes in the ST segment, especially in asymptomatic patients, should be used to determine clinical therapy.
This report provides consensus guidelines for the optimal application of ST-segment monitoring in patients with acute coronary syndromes. Although ST-segment monitoring has been used in children,22 this discussion focuses on adults, who make up the vast majority of patients with acute ischemic coronary syndromes. The following specific questions are addressed:
1. Who should have ST-segment monitoring?2. What are the goals and recommended time frames for ST-segment monitoring in various diagnostic groups?3. Who should not have ST-segment monitoring?4. What ECG leads should be monitored?5. What equipment requirements are necessary for accurate ST-segment monitoring?6. What strategies improve the accuracy and clinical usefulness of ST-segment monitoring?7. What knowledge and skills should clinicians have for safe and effective ST-segment monitoring of patients in a hospital unit?8. What are priorities for future research and development?
Development of the GuidelinesA literature search was used to determine key nurse and physician scientists who had published articles on ST-segment monitoring of patients in acute care hospital units. These scientists were invited to participate in a working group that met in Dallas, Tex, in November 1998. Additional members were added to the working group as recommended by the initial key scientists. The final group included 10 physicians, 10 nurses, and 1 cardiac monitoring engineering expert.
The 10 nurses included 5 nurse scientists with doctoral degrees and 5 doctoral students involved in research on ischemia. Eleven members of the working group were from various locations throughout the United States; 9 were from other countries, including Denmark, Sweden, the Netherlands, Australia, and Scotland.
At the initial meeting, consensus was reached on each of the 8 substantive areas mentioned earlier. The chair of the working group drafted an initial guideline that was critiqued by all members of the group via telephone calls and e-mail messages. The guideline was revised according to the critiques, and a second draft was circulated. This article includes the final, revised consensus document.
Who Should Have ST-Segment Monitoring?Unstable angina and ST elevation or non–ST elevation myocardial infarction most often
CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
3 of 20 4/10/2006 9:33 AM
occur in patients with significant coronary artery disease who have disruption of anatherosclerotic plaque and a subsequent dynamic coronary occlusive process that involvescycles of plaque rupture, platelet stimulation, coronary vasospasm, and thrombusformation.23-30 For this reason, these patients should be considered the highest priority for ST-segment monitoring, which provides uninterrupted real-time information about the occurrence, frequency, and severity of ischemic episodes over the course of the dynamic occlusive process.
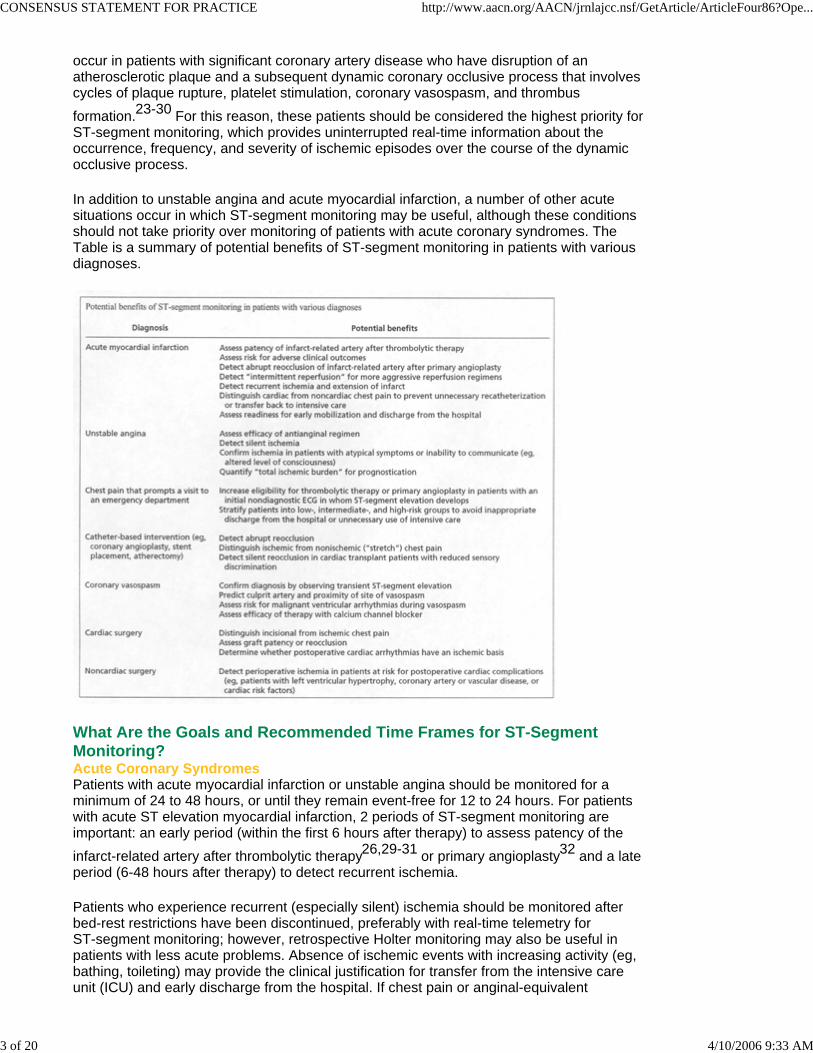
In addition to unstable angina and acute myocardial infarction, a number of other acute situations occur in which ST-segment monitoring may be useful, although these conditions should not take priority over monitoring of patients with acute coronary syndromes. The Table is a summary of potential benefits of ST-segment monitoring in patients with various diagnoses.
xWhat Are the Goals and Recommended Time Frames for ST-Segment Monitoring?Acute Coronary SyndromesPatients with acute myocardial infarction or unstable angina should be monitored for a minimum of 24 to 48 hours, or until they remain event-free for 12 to 24 hours. For patients with acute ST elevation myocardial infarction, 2 periods of ST-segment monitoring are important: an early period (within the first 6 hours after therapy) to assess patency of the infarct-related artery after thrombolytic therapy26,29-31 or primary angioplasty32 and a late period (6-48 hours after therapy) to detect recurrent ischemia.
Patients who experience recurrent (especially silent) ischemia should be monitored after bed-rest restrictions have been discontinued, preferably with real-time telemetry for ST-segment monitoring; however, retrospective Holter monitoring may also be useful in patients with less acute problems. Absence of ischemic events with increasing activity (eg, bathing, toileting) may provide the clinical justification for transfer from the intensive care unit (ICU) and early discharge from the hospital. If chest pain or anginal-equivalent
CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
4 of 20 4/10/2006 9:33 AM
symptoms develop after ST-segment monitoring has been discontinued, monitoring should be reinstituted for 12 to 24 hours.
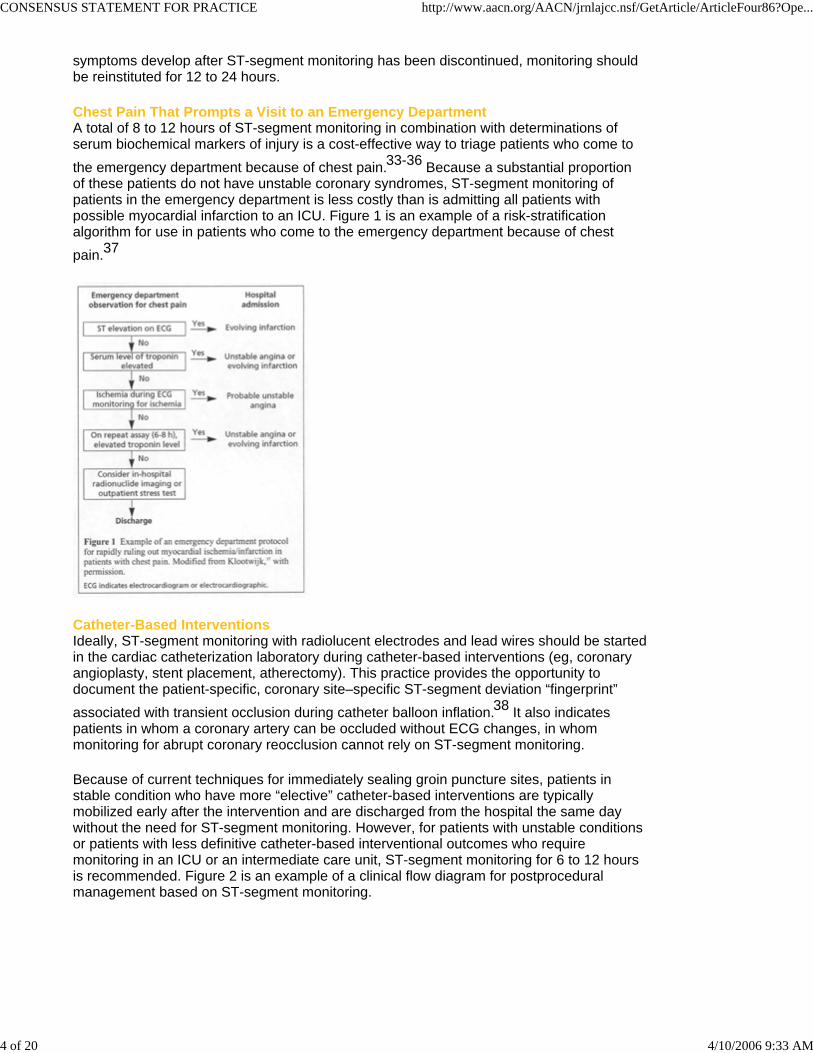
Chest Pain That Prompts a Visit to an Emergency DepartmentA total of 8 to 12 hours of ST-segment monitoring in combination with determinations of serum biochemical markers of injury is a cost-effective way to triage patients who come to the emergency department because of chest pain.33-36 Because a substantial proportion of these patients do not have unstable coronary syndromes, ST-segment monitoring of patients in the emergency department is less costly than is admitting all patients with possible myocardial infarction to an ICU. Figure 1 is an example of a risk-stratification algorithm for use in patients who come to the emergency department because of chest pain.37
xCatheter-Based InterventionsIdeally, ST-segment monitoring with radiolucent electrodes and lead wires should be startedin the cardiac catheterization laboratory during catheter-based interventions (eg, coronaryangioplasty, stent placement, atherectomy). This practice provides the opportunity todocument the patient-specific, coronary site–specific ST-segment deviation “fingerprint”associated with transient occlusion during catheter balloon inflation.38 It also indicates patients in whom a coronary artery can be occluded without ECG changes, in whom monitoring for abrupt coronary reocclusion cannot rely on ST-segment monitoring.
Because of current techniques for immediately sealing groin puncture sites, patients instable condition who have more “elective” catheter-based interventions are typicallymobilized early after the intervention and are discharged from the hospital the same daywithout the need for ST-segment monitoring. However, for patients with unstable conditionsor patients with less definitive catheter-based interventional outcomes who requiremonitoring in an ICU or an intermediate care unit, ST-segment monitoring for 6 to 12 hoursis recommended. Figure 2 is an example of a clinical flow diagram for postproceduralmanagement based on ST-segment monitoring.

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
5 of 20 4/10/2006 9:33 AM
xPostprocedural monitoring in patients undergoing catheter-based interventions has 2 goals: to detect abrupt reocclusion at the intervention site due to vessel dissection or thrombosis38and to distinguish ischemic from nonischemic chest pain. In terms of the first goal, abrupt reocclusion is most likely to occur early after the procedure, either before the patient has left the cardiac catheterization laboratory or within the first several hours after transfer to another hospital unit.39 In terms of the second goal, nearly 50% of patients who have placement of a stent and about 12% of patients who have angioplasty experience chest pain after the interventional procedure.40
This type of chest pain either requires urgent recatheterization/revascularization for treatment of abrupt reocclusion or is benign and requires no intervention. Benign chest pain can be caused by stretching of the coronary vessel during high-pressure balloon inflations or stent deployment.
Benign chest pain, nausea, and other nonspecific symptoms can also be due to gastrointestinal distress brought on by fasting or by esophageal reflux after eating in the supine position. The absence of ST-segment deviation during these situations may provide reassurance that such symptoms are not related to ischemia. A potential cost benefit of ST-segment monitoring is that it may reduce the number of unnecessary repeat cardiac catheterizations by distinguishing between ischemic and benign causes of postprocedural

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
6 of 20 4/10/2006 9:33 AM
symptoms.
However, the absence of ST-segment deviation during chest pain can be considered reassuring only if ST-segment deviation was detected during coronary occlusion in the catheterization laboratory. For example, if a circumflex coronary artery is stented, and no changes in the ST segment are observed on ECGs obtained during balloon inflation, then the absence of ST-segment deviation when chest pain recurs does not rule out ischemia or a problem at the intervention site (eg, an occlusive thrombus).
Cardiac transplant patients who undergo catheter-based interventions are a higher priority than are other patients for postprocedural ST-segment monitoring because the former are vulnerable to silent reocclusion due to altered sensory discrimination.
Cardiac or Noncardiac SurgeryExperience with ST-segment monitoring of patients after cardiac or noncardiac surgery is limited. However, Mangano and coworkers42-45 detected a high-risk period immediately after surgery when patients emerge from anesthesia and experience pain. Such arousal of the sympathetic nervous system is accompanied by an increase in heart rate, and therefore ischemia in the early postoperative period often occurs because myocardial oxygen demand exceeds blood flow capabilities, rather than because of coronary occlusion processes.
Postoperative myocardial ischemia may also develop because of fluid shifts and hypercoagulability, which tend to occur somewhat later in the 24 to 48 hours after surgery. Therefore, ST-segment monitoring of surgical patients with coronary heart disease or cardiac risk factors should begin immediately after surgery when the patient is being monitored in a postanesthesia recovery unit and should continue in the ICU for approximately 24 to 48 hours.
Who Should Not Have ST-Segment Monitoring?Certain subgroups of patients with acute coronary syndromes may not be candidates forcurrently available ST-segment monitoring technologies. In general, these are patients inwhom interpretation of evidence of ischemic changes on the static ECG is confounded byconduction abnormalities, left ventricular hypertrophy, or excessive artifact. If a static ECGis unsuitable for detection of ischemia, use of ST-segment monitoring most likely will lead tofalse alarms, staff fatigue, and disenchantment with the technology, and potentially even tounnecessary therapy, curtailment of patients’ activities, or delay in discharge from thehospital.
Patients who may not be candidates for ST-segment monitoring include those who have (1) left bundle branch block, (2) intermittent right or left bundle branch block, (3) ventricular pacing rhythm, (4) an excessively noisy signal because of restlessness or confusion, or (5) wound dressings over the precordium.
Few current ST-segment monitors automatically change the point at which the ST segment is measured when the heart rate changes, and they do not correct measurements of ST amplitude when changes occur in the QRS amplitude. This situation means that patients with steeply upsloping ST-T waves, such as patients who have left bundle branch block may be plagued with false-positive ST alarms when there is a change in heart rate. In addition, patients who have large changes in QRS amplitude when changing body position also may be plagued with false alarms that confound interpretation of data from ST-segment monitoring.
What ECG Leads Should Be Monitored?Monitoring ST-segment changes in all 12 ECG leads is recommended for accurate detection of myocardial ischemia in patients with acute coronary syndromes because

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
7 of 20 4/10/2006 9:33 AM
ischemia may be due to more than one mechanism and cause changes in different leads at different times.10,46,47 For example, Klootwijk et al47 found that ST changes dispersed and shifted among different leads over time in at least 31% of patients with unstable angina who had more than a single episode of ST-segment deviation during a 48-hour monitoring period.47
Likewise, Drew et al10 found that 42% of recurrent ischemic events detected with full 12-lead ST-segment monitoring were not detected by monitoring the single ECG lead that had maximal ST-segment deviation at the onset of acute myocardial infarction or during catheter balloon inflation. Similarly, Krucoff et al48 reported that of 524 angioplasty patients who had ST-segment monitoring after the coronary intervention, 92 (18%) had episodes of ST deviation; 43% of the episodes were elevations in the ST segment, and 57% were depressions.48
Thus, patients with acute coronary syndromes differ from patients with stable coronary artery disease who have transient myocardial ischemia; the latter typically have only ST depressions, which are reliably visualized on ECG tracings obtained with lead V5 during exercise or ambulatory monitoring. For this reason, single-lead ST-segment monitoring is insufficient for patients with acute coronary syndromes.10,47,49,50
Leads Valuable for Detecting Coronary OcclusionMyocardial ischemia due to coronary occlusion has a variety of causes in patients with acute coronary syndromes: (1) occlusive thrombus with acute myocardial infarction, (2) balloon inflation during catheter-based interventions, (3) rethrombosis of the infarct-related artery after thrombolytic therapy, (4) reocclusion of the treated artery after catheter-based procedures, and (5) coronary vasospasm. The classic ECG pattern produced by coronary occlusion is ST-segment elevation detected by a restricted number of leads that lie directly over the ischemic myocardial zone.
Right Coronary Artery Occlusion. The lead that most often shows maximal ST-segment elevation during occlusion of the right coronary artery and ischemia of the inferior wall of the heart is lead III; next, in order, are lead aVF and lead II.51-53 Interestingly, lead II is the lead most often selected for monitoring in ICUs.54 However, during injury of the inferiorwall, the ECG tracing obtained with lead II typically displays the least ST-segment elevationof the tracings obtained with the 3 available “inferior” leads.
Left Coronary Artery Occlusion. Maximal ST-segment elevation during occlusion of theleft anterior descending coronary artery and injury of the anterior wall of the heart typically isobserved on the “mid” precordial ECG leads V2 and V3, and less often lead V4.49,51-53
Occlusion of the left circumflex artery produces no visible changes in the ST segment on the standard 12-lead ECG in about one third of patients. Patients who have visible changes in the ST segment during occlusion of the circumflex artery may have ischemia of the inferior, lateral, or posterior wall of the heart, and thus a variety of patterns may be observed in patients in whom no ECG lead is indicated as being far superior to other leads.49,51-53
ECGs obtained with additional posterior leads, V7, V8, and V9, may show ST-segmentelevation in these extra leads during injury of the posterior wall. However, because of thedistance of the posterior part of the thorax from the left ventricle, the amplitude of STelevation is low, often less than 1 mm, which is difficult for the human eye to discern.Reciprocal ST-segment depression during injury of the posterior wall is best observed inone of the “rightward” standard precordial leads, V1, V2, and/or V3. Because the heart is situated in the chest more anteriorly than posteriorly, the amplitude of these reciprocal ST

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
8 of 20 4/10/2006 9:33 AM
depressions may be greater than the amplitude of ST elevations recorded with posterior leads.
Summary. In summary, the most valuable leads for detecting occlusion of the 3 major epicardial coronary arteries encompass 9 of the 12 standard ECG leads. The arteries and the leads are as follows: right coronary artery, leads III, aVF, and II; left anterior descending artery, leads V2, V3, and V4. For the left circumflex artery, a variety of leads may be involved, depending on the myocardial zone affected (lateral, inferior, and/or posterior), as follows: leads V5 and V6 (lateral), leads III, aVF, and II (inferior), and leads V1, V2, and V3(posterior).
Leads Valuable for Detecting “Demand-Related” IschemiaIn addition to coronary occlusion, patients with acute coronary syndromes may have global,subendocardial ischemia due to an increase in myocardial oxygen demand beyond the flowlimits of stenotic coronary vessels. Although patients with these “demand-related” ischemicevents may not require urgent interventions such as thrombolytic therapy or immediateangioplasty, their prognosis is worse than that of patients without such events.3-9
Thus, detection of demand-related ischemia with ST-segment monitoring is important. Ischemic events related to an increase in myocardial oxygen demand may occur during a tachyarrhythmia or, in patients with severe coronary artery disease, may be elicited by only a slight increase in heart rate. The classic ECG pattern of demand-related ischemia is 1 to 2 mm of horizontal or down-sloping ST-segment depression on the tracings from several leads, with maximal ST depression typically recorded by leads lying over the left ventricular apex (eg, lead V5).55
Monitoring a Patient’s ST “Fingerprint”Krucoff et al38 introduced the concept of the ST “fingerprint,” which is defined as the12-lead ECG pattern of ST-segment elevations and depressions that is unique to aparticular patient and is based on the anatomic site of coronary occlusion.38 During acutemyocardial infarction, a patient’s ST-fingerprint ECG is ideally recorded at peak ST-segmentdeviation, before thrombolytic or primary angioplasty therapy is started. Subsequentduplication of this patient-specific ECG pattern can be used to diagnose reocclusion of theinfarct-related artery.2,24,26,56-58
When 12-lead ST-segment monitoring is not available, evidence of rapid ST-segment recovery (normalization) in the single lead with peak ST-segment elevation is useful for predicting patency of the infarct-related artery.29,59,60 However, single-lead monitoring is not sensitive for diagnosing ischemia related to other mechanisms (eg, ischemia of myocardial zones that do not get their blood supply from the infarct-related artery).10Therefore, 12-lead ECG monitoring, rather than single-lead monitoring, is recommendedbecause the former “covers more of the bases” for detecting both coronary artery occlusionand demand-related ischemia in anterior, inferior, lateral, and often, posterior myocardialzones.
In patients undergoing catheter-based interventions, the ST-fingerprint ECG is ideally recorded during inflation of the catheter balloon. Subsequent duplication of this patient-specific ECG pattern can be used to diagnose abrupt reocclusion of the treated artery, which requires urgent recatheterization/revascularization.38 A partial reocclusion ofthe treated artery may not reproduce the patient’s ST-fingerprint ECG pattern and thus maybe impossible to distinguish from other ischemic mechanisms. Partial reocclusion, however,is less of an emergency than is abrupt, total reocclusion, and the latter should never goundetected in clinical practice.
CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
9 of 20 4/10/2006 9:33 AM
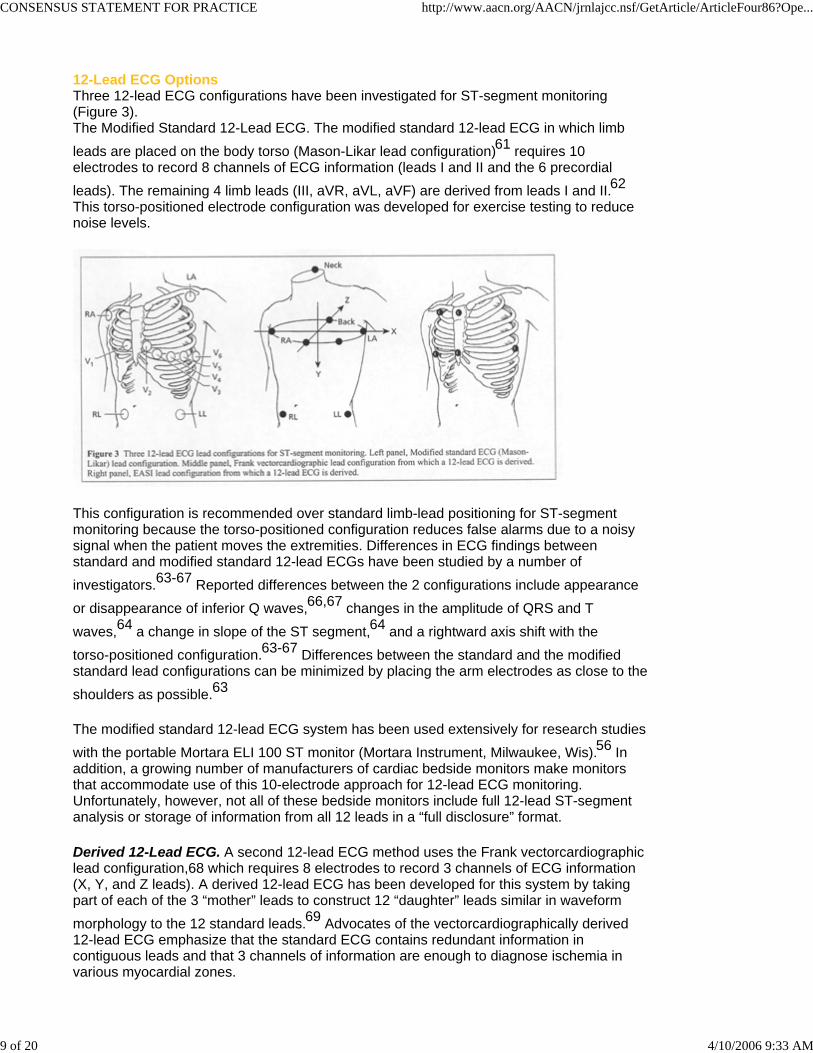
12-Lead ECG OptionsThree 12-lead ECG configurations have been investigated for ST-segment monitoring (Figure 3).The Modified Standard 12-Lead ECG. The modified standard 12-lead ECG in which limb leads are placed on the body torso (Mason-Likar lead configuration)61 requires 10 electrodes to record 8 channels of ECG information (leads I and II and the 6 precordial leads). The remaining 4 limb leads (III, aVR, aVL, aVF) are derived from leads I and II.62This torso-positioned electrode configuration was developed for exercise testing to reduce noise levels.
xThis configuration is recommended over standard limb-lead positioning for ST-segment monitoring because the torso-positioned configuration reduces false alarms due to a noisy signal when the patient moves the extremities. Differences in ECG findings between standard and modified standard 12-lead ECGs have been studied by a number of investigators.63-67 Reported differences between the 2 configurations include appearance or disappearance of inferior Q waves,66,67 changes in the amplitude of QRS and T waves,64 a change in slope of the ST segment,64 and a rightward axis shift with the torso-positioned configuration.63-67 Differences between the standard and the modified standard lead configurations can be minimized by placing the arm electrodes as close to the shoulders as possible.63
The modified standard 12-lead ECG system has been used extensively for research studies with the portable Mortara ELI 100 ST monitor (Mortara Instrument, Milwaukee, Wis).56 Inaddition, a growing number of manufacturers of cardiac bedside monitors make monitorsthat accommodate use of this 10-electrode approach for 12-lead ECG monitoring.Unfortunately, however, not all of these bedside monitors include full 12-lead ST-segmentanalysis or storage of information from all 12 leads in a “full disclosure” format.
Derived 12-Lead ECG. A second 12-lead ECG method uses the Frank vectorcardiographiclead configuration,68 which requires 8 electrodes to record 3 channels of ECG information(X, Y, and Z leads). A derived 12-lead ECG has been developed for this system by takingpart of each of the 3 “mother” leads to construct 12 “daughter” leads similar in waveformmorphology to the 12 standard leads.69 Advocates of the vectorcardiographically derived 12-lead ECG emphasize that the standard ECG contains redundant information in contiguous leads and that 3 channels of information are enough to diagnose ischemia in various myocardial zones.

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
10 of 20 4/10/2006 9:33 AM
They assert that all important clinical information is contained within the 3 orthogonal X, Y, and Z leads and that ischemia can be readily recognized by clinicians when the 3-lead format is translated into the more familiar 12-lead ECG format.70 Importantly, the Franklead configuration includes electrodes on the patient’s back and an electrode under the rightaxilla, so this system may be more sensitive than the standard ECG for detecting injury ofthe posterior wall of the heart and of the right ventricle. The Frank lead system has beenused extensively in research studies with the MIDA system (Ortivus Medical, Täby,Sweden) to analyze both ST-segment and QRS changes during ischemia.14,27,31,71-77
The EASI 12-Lead ECG. A third 12-lead ECG method uses a modified Frank lead configuration and requires 5 electrodes to record 3 channels of ECG information. A 12-lead ECG has also been derived for this lead configuration by Dower et al78 and is referred to as the EASI 12-lead ECG (Zymed Inc, Camarillo, Calif). Investigations with the EASI 12-lead ECG indicate that it is comparable to the standard 12-lead ECG for detection of arrhythmia79,80 and ischemia.81-83 Future research and development are required to make available use of the EASI 12-lead ECG in commercial bedside monitors having 12-lead ST-segment analysis and full-disclosure capabilities.
Summary. Sound scientific evidence indicates that all three 12-lead ECG configurations are valuable for ST-segment monitoring. However, all 3 lead configurations, Mason-Likar,63-67Frank vectorcardiographic, and EASI, differ from the standard extremity lead configuration,and thus clinicians should be cautious when making serial ECG comparisons recorded with2 different lead configurations in a given patient. In addition, clinicians should be cautiouswhen comparing “snapshot” 12-lead ECGs, which are obtained with patients supine, withECGs printed from an ST monitor, because the latter may involve a different body positionand associated alterations in ST-T wave morphology.
Most Valuable Leads When 12-Lead ECG Monitoring Is UnavailableIf only 2 leads are available for ST-segment monitoring, use of leads III and V3 isrecommended for patients with acute coronary syndromes, unless available informationfrom a patient’s prior 12-lead ECG recorded during an ischemic event indicates that anotherlead is more sensitive.10,51-53 The best 3-lead combination is leads III, V3, and V5; however, many bedside cardiac monitors are capable of monitoring only a single precordial (V) lead because the monitors provide only a single chest electrode. In addition, these 2- and 3-lead combinations for ischemia exclude lead V1, which is considered the best lead to monitor for detection of cardiac arrhythmias.
What Equipment Requirements Are Necessary for Accurate ST-Segment Monitoring?Bedside cardiac monitors used to detect cardiac arrhythmias in real time in hospital units are often not suitable for ST-segment monitoring, although the displayed ECG lead may show ST abnormalities when ST-segment deviation is striking. Often distortions of the low-frequency content of the signal due to inadequate filtering techniques and baseline wander correction may result in distortions of the ST segment.84,85
In addition, typically, information from only 1 to 2 ECG leads is displayed at the patient’sbedside and from only 1 lead at the central monitoring station, although many systemsrecord information from 2 to 3 leads simultaneously. Therefore, the sensitivity for detectingepisodes of ST deviation in areas not covered by the lead(s) being monitored is decreased.Moreover, in current ICUs selection of ECG leads typically focuses on detection ofarrhythmias, and the usual selection is lead V1 and/or lead II, neither of which is highlysensitive for detection of ischemia.53,54

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
11 of 20 4/10/2006 9:33 AM
Finally, fatigue of the person watching the monitor, partly due to the display of tracings for multiple patients, results in underdetection of changes in the ST segment, especially when no ST analysis software and alarm notification are available to augment human observation.86 In summary, ST-segment monitoring devices can only be used reliably for detection of ischemia in the following situations: (1) filtering techniques result in an adequate low-frequency response; (2) full 12-lead or vectorcardiographic lead capability is available; (3) proper algorithms for detection of ischemia are integrated, including storage of complexes and measurements for comparison in full-disclosure format and trending of the ST deviations over time.84
What Strategies Improve the Accuracy and Clinical Usefulness of ST-Segment Monitoring?Proper Application of ElectrodesBecause the amplitude of clinically significant ST-segment deviations is typically as small as 1 mm, a noisy signal is a problem for accurate diagnosis. Careful preparation of the skin that includes shaving areas where the electrodes will be placed and removing skin oils and cutaneous debris with alcohol and abrasion is imperative and will substantially reduce false alarms.
Consistent Placement of LeadsMarking the locations of the electrodes with indelible ink is advantageous so that electrodes that are removed for any reason (eg, leads V2 and V3 are typically removed during recording of echocardiograms) can be replaced in their original locations. ECG information obtained from electrodes located close to the heart (ie, the precordial leads) is especially prone to waveform changes when the electrodes are relocated as little as 1 cm away from the original locations. Figure 4 shows ECG tracings that resulted in misdiagnosis and a subsequent unnecessary cardiac catheterization in a patient with inconsistent lead placement.

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
12 of 20 4/10/2006 9:33 AM
xSelection of the ST-Segment Measurement PointMany monitors offer a choice of points, such as J + 60 ms or J + 80 ms, for measuring the ST segment. Most experts program monitors to measure the ST segment at the earlier J + 60 ms point because this point is less likely to coincide with the upslope of the T wave in patients in whom sinus tachycardia develops.
Measurement of “Delta” ST in the Diagnosis of Transient IschemiaA widely accepted definition of transient myocardial ischemia, developed for use with ambulatory Holter monitoring, is ST-segment deviation of 0.1 mV or greater (1 mm with normal standardization of 1 mV = 10 mm) that lasts at least 1 minute.87 Although the same definition has been applied to 12-lead ST-segment monitoring, clinicians must recognize that the 12-lead configuration has more redundancy than does the 1- to 3-lead Holter system because electrodes are placed closer to each other (especially the 6 precordial leads) in the 12-lead configuration.
Therefore, changes in the ST segment during an ischemic event are typically visible on tracings from more than 1 of the 12 ECG leads, and if just 1 mm of ST change is observed with just 1 lead, the ST episode should be considered questionable, especially in asymptomatic patients. Although patients may have ST-segment deviation for less than 1 minute during a brief inflation of an angioplasty balloon, spontaneous ischemia typically lasts 1 to 30 minutes. When ST-segment deviation lasts for more than 30 minutes without a return to the baseline ST value, the probability of cell death and myocardial infarction increases.
For diagnosis of transient myocardial ischemia, the baseline ST level must first be

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
13 of 20 4/10/2006 9:33 AM
established at a time when the patient is not experiencing ischemia.47,88 In patients without acute infarction, the baseline ST level is usually established upon initiation of ST-segment monitoring. The baseline measurement is often not isoelectric (ie, identical to the TP or PR segments) because patients may have chronic repolarization abnormalities due to conditions such as left ventricular hypertrophy, digitalis therapy, or normal early repolarization.88
When an acute change occurs in the ST level on a tracing obtained with a particular ECGlead, the baseline ST value for this lead should be subtracted from the new ST value toobtain a change score or “delta” ST measurement. Delta ST values that are at least 1 mmindicate an ischemic event. Thus, an ischemic event may produce a normal-lookingisoelectric ST segment in a patient whose baseline ST level is depressed due to leftventricular hypertrophy or digitalis therapy. This situation is called “pseudonormalization” ofthe ST segment, and if pseudonormalization is not recognized, an ischemic event may notbe detected.
Setting ST Alarm Parameters AppropriatelyFor research studies, the alarms for 12-lead ST-segment monitoring are often programmedto trigger an audible alarm if 1 mm of ST-segment deviation occurs on tracings from 2 ECGleads or 2 mm of deviation occurs on a tracing from a single lead and either deviation lastsmore than 1 minute. For bedside cardiac monitoring, the alarm thresholds should be set 1 to2 mm above and below the patient’s baseline ST level (rather than the isoelectric level),because the patient’s baseline level is rarely isoelectric.88
Recognition of “Good” and “Bad” ST AlarmsCurrent technology for ST-segment monitoring is generally configured to detect a change in the ST segment but does not include any interpretative function that characterizes the change as clinically good or bad for the patient. The interpretative function is fulfilled by the bedside healthcare professional who assesses whether the new deviation from a previous ST value represents improvement or worsening. The ST-segment monitor simply records the degree, extent, and timing of the ST change.
In the early stages of myocardial infarction, rapid ST-segment recovery is predictive of patency of the infarct-related artery.29,59,60 For example, a reduction of 50% or more in the peak ST elevation within 1 hour of thrombolytic therapy is predictive of a patent vessel.59 Such rapid changes in the ST segment will trigger alarms that should beconsidered “good” alarms. Conversely, a silent ST monitor during thrombolytic therapysuggests no change in the ST segment, and a more aggressive approach (eg, rescueangioplasty) may be warranted.89 In the later stages of acute myocardial infarction, whenST recovery is complete (ie, the ST segments have returned to baseline levels), a ST alarmshould be considered a “bad” alarm, signifying recurrent ischemia.
Recognition of False Alarms Due to Changes in Body PositionUntil the advent of continuous 12-lead ST-segment monitoring, ECG changes related tochanges in body position were not a concern because “snapshot” 12-lead ECGs werealways recorded with the patient supine. However, when patients are monitored over time,they assume multiple body positions, such as lying on their right or left side, sitting upright,or even standing.
Echocardiographic data indicate that the heart moves closer to the chest wall when a patient moves from the supine to the left-lying position.90 Such a positional change often produces greater amplitude QRS waveforms and exaggerated amplitudes in ST-segment deviations, which can be mistaken for evidence of an ischemic event.88,91

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
14 of 20 4/10/2006 9:33 AM
One way to ascertain whether a patient will have false alarms due to positional changes is to compare changes in the ST-T wave that occur when the patient moves from supine, to right-lying, to left-lying positions at the initiation of ST-segment monitoring. These positional templates can be used subsequently to distinguish ST changes due to ischemia from those due to changes in body position.
A second approach is to consider that all changes in the ST segment that occurinstantaneously over 1 to 2 cardiac cycles and that are accompanied by a change in theQRS waveform are due to changes in body position rather than to true ischemia. When thepatient’s body position during an alarm condition is not clearly known (eg, the monitorwatcher at the central nursing station cannot see the patient), a 12-lead ECG should berecorded with the patient supine to verify that observed ST changes are also present whenthe patient is supine.
Confirmation of ST-Segment Monitoring Trends With 12-Lead ECG PrintoutsMost computer-assisted ST monitors have graphic representations of the ST-segment trend detected with a single lead or summated leads. Although trend information is convenient for quickly detecting potential ischemic events, the ECG findings in question should be printed out to confirm that the changes in the ST segment are due to ischemia rather than to a transient arrhythmia such as an accelerated ventricular rhythm. In addition, if the ST monitor indicates an ischemic event but ST deviation is not visually detected on the printed out ECG, the accuracy of the ST monitor should be questioned, because the human eye is capable of observing 1 mm of ST-segment deviation.92
What Knowledge and Skills Should Clinicians Have for Safe and Effective ST-Segment Monitoring of Patients in a Hospital Unit?Ideally, each hospital unit should develop a protocol for ST-segment monitoring that is relevant to the types of patients cared for in that unit. For example, the goals and lengths of monitoring differ among various hospital units, such as emergency department areas for observation of chest pain, cardiac care units, cardiac surgical ICUs, and step-down telemetry units.
The best education for learning about ST-segment monitoring is hands-on clinicalexperience, because expertise is developed over time by experiencing numerous clinicalscenarios. Accurate ST-segment monitoring requires expertise in interpreting 12-leadECGs, an understanding of the patient’s clinical situation, and knowledge of the functionsand limitations of the ST-segment monitoring system.
At a minimum, clinicians should be able to do the following:1. accurately place and consistently maintain ECG leads;2. identify the lead that shows peak ST elevation and recognize rapid ST recovery versus sustained ST elevation in acute myocardial infarction;3. recognize abrupt reocclusion during monitoring of patients after angioplasty;4. recognize false alarms that are due to a noisy signal or to transient arrhythmia; and5. assess a patient’s cardiac symptoms and hemodynamic status to determine the clinicalimportance of changes in the ST segment.
What Are Priorities for Future Research and Development?Research and Development by ManufacturersFuture cardiac monitors should incorporate analysis of the ST segment in all 12 leads plusarrhythmia analysis. Monitors should provide full disclosure of data from all 12 leads for atleast 24 hours to ensure accurate diagnosis and documentation of transient ischemic andarrhythmic events. “Seamless” ST-segment monitoring should be available from theemergency department to the cardiac catheterization laboratory to the cardiac care unit tothe step-down telemetry unit, and the system should be portable, for use duringintrahospital transport between units. In addition, better noise-reduction strategies should be

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
15 of 20 4/10/2006 9:33 AM
developed to reduce the number of false alarms.
Advancing the Science for Patients With Acute Coronary SyndromesThe notion that early detection and suppression of myocardial ischemia (especially silentischemia) benefit patients with acute coronary syndromes by improving the poor prognosisassociated with ST-deviation episodes should be investigated in a large-scale,well-controlled clinical trial. Such a trial should include only “hard” clinical end points suchas death or (re)infarction because “soft” end points such as urgent recatheterization orrevascularization may be affected by events observed with ST-segment monitoring.
Future research is also needed to sort out the value of leads other than the standard 12-lead set that are recorded directly or are derived from other leads. In addition, the value of ST-segment monitoring in the prehospital phase is unknown. Finally, the clinical importance and independent contribution of QRS and T-wave abnormalities and changes are unclear and require further investigation.
AcknowledgmentsThe members of the ST-Segment Monitoring Practice Guideline International Working Group were as follows: Mary G. Adams, RN, MS, University of California, San Francisco, Calif; Kathy J. Booker, RN, MS, Millikin University, Decatur, Ill; Mary Caldwell, RN, PhD, University of California, San Francisco, Calif; Peter Clemmensen, MD, DSc, the Rigshospital Copenhagen and University Hospital, Copenhagen, Denmark; Mikael Dellborg, MD, PhD, Sahlgrenska University Hospital/Östra, Göteborg, Sweden; Barbara J. Drew, RN,PhD, chair of writing group and panel of experts, School of Nursing, University of California, San Francisco, Calif; Denis W. Drew, MD, Alameda Hospital, Alameda, Calif; Sven V. Eriksson, MD, PhD, Danderyd Hospital, Karolinska Institutet, Daneryd, Sweden; Marjorie Funk, RN, PhD, Yale University School of Nursing, New Haven, Conn; W. Brian Gibler, MD, University of Cincinnati Hospital, Cincinnati, Ohio; Brigid Ide, RN, MS, University of California, San Francisco Stanford Health Care, San Francisco, Calif; Peter Klootwijk, MD, PhD, University Hospital Rotterdam Dijkzigt, Rotterdam, the Netherlands; Mitchell W. Krucoff, MD, cochair, Veterans Affairs Medical Center, Durham, NC; Angela Kucia, RN, MA, The Queen Elizabeth Hospital, Woodville, South Australia; Arthur C. Maas, MD, Duke Clinical Research Center, Durham, NC; Anders Melcher, MD, PhD, Danderyd Hospital, Karolinska Institutet, Danderyd, Sweden; Simon Meij, MSc, University Hospital Rotterdam Dijkzigt, Rotterdam, the Netherlands; Michele M. Pelter, RN, MS, University of California, San Francisco, Calif; Simon Stewart, RN, PhD, Department of Public Health, Glasgow, Scotland; Rolf F. Veldkamp, MD, PhD, University Hospital Rotterdam Dijkzigt, Rotterdam, the Netherlands; and Shu-Fen Wung, RN, PhD, University of Illinois at Chicago, Chicago, Ill.
References1. Simoons ML, Vos J, Tijssen JGP, et al. Long-term benefit of early thrombolytic therapy inpatients with acute myocardial infarction: 5 year follow-up of a trial conducted by the Interuniversity Cardiology Institute of the Netherlands. J Am Coll Cardiol.1989;14:1609-1615.2. Klootwijk P, Cobbaert C, Fioretti P, Kint PP, Simoons ML. Noninvasive assessment ofreperfusion and reocclusion after thrombolysis in acute myocardial infarction. Am J Cardiol. 1993;72:75G-84G.3. Gottlieb SO, Weisfeldt ML, Ouyang P, Mellits DE, Gerstenblith G. Silent ischemia as amarker for early unfavorable outcomes in patients with unstable angina. N Engl J Med. 1986;314:1214-1219.4. Gottlieb SO, Weisfeldt ML, Ouyang P, Mellits DE, Gerstenblith G. Silent ischemiapredicts infarction and death during 2 year follow-up of unstable angina. J Am Coll Cardiol.1987;10:756-760.5. Nademanee K, Intarachot V, Josephson MA, Rieders D, Mody FV, Singh BN. Prognosticsignificance of silent myocardial ischemia in patients with unstable angina. J Am Coll Cardiol. 1987;10:1-9.6. Krucoff M. Identification of high-risk patients with silent myocardial ischemia afterpercutaneous transluminal coronary angioplasty by multilead monitoring. Am J Cardiol. 1988;61:29F-34F.7. Langer A, Freeman MR, Armstrong PW. ST segment shift in unstable angina:pathophysiology and association with coronary anatomy and hospital outcome. J Am Coll Cardiol. 1989;13:1495-1502.8. Larsson H, Jonasson T, Ringqvist I, Fellenius C, Wallentin L. Diagnostic and prognostic

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
16 of 20 4/10/2006 9:33 AM
importance of ST recording after an episode of unstable angina or non-Q-wave myocardial infarction. Eur Heart J. 1992;13:207-212.9. Amanullah AM, Lindvall K. Prevalence and significance of transient—predominantlyasymptomatic—myocardial ischemia on Holter monitoring in unstable angina pectoris, andcorrelation with exercise test and thallium-201 myocardial perfusion imaging. Am J Cardiol. 1993;72:144-148.10. Drew BJ, Pelter MM, Adams MG, Wung SF, Chou TM, Wolfe CL. 12-Lead ST-segmentmonitoring vs single-lead maximum ST-segment monitoring for detecting ongoing ischemia in patients with unstable coronary syndromes. Am J Crit Care. 1998;7:355-363.11. von Arnim T, Gerbig HW, Krawietz W, Hofling B. Prognostic implications oftransient—predominantly silent—ischaemia in patients with unstable angina pectoris. Eur Heart J. 1988;9:435-440.12. Johnson SM, Mauritson DR, Winniford MD, et al. Continuous electrocardiographicmonitoring in patients with unstable angina pectoris: identification of high-risk subgroup with severe coronary disease, variant angina, and/or impaired early prognosis. Am Heart J.1982;103:4-12.13. Langer A, Singh N, Freeman MR, Tibshirani R, Armstrong PW. Detection of silentischemia adds to the prognostic value of coronary anatomy and left ventricular function in predicting outcome in unstable angina patients. Can J Cardiol. 1995;11:117-122.14. Holmvang L, Andersen K, Dellborg M, et al. Relative contributions of a single-admission12-lead electrocardiogram and early 24-hour continuous electrocardiographic monitoring for early risk stratification in patients with unstable coronary artery disease. Am J Cardiol.1999;83:667-674.15. Ouyang P, Chandra NC, Gottlieb SO. Frequency and importance of silent myocardialischemia identified with ambulatory electrocardiographic monitoring in the early in-hospital period after acute myocardial infarction. Am J Cardiol. 1990;65:267-270.16. Gottlieb SO, Gottlieb SH, Achuff SE, et al. Silent ischemia on Holter monitoring predictsmortality in high-risk postinfarction patients. JAMA. 1988;259:1030-1035.17. Tzivoni D, Gavish A, Zin D, et al. Prognostic significance of ischemic episodes inpatients with previous myocardial infarction. Am J Cardiol. 1988;62:661-664.18. Langer A, Minkowitz J, Dorian P, et al for the Tissue Plasminogen Activator: Toronto(T-PAT) Study Group. Pathophysiology and prognostic significance of Holter-detected ST segment depression after myocardial infarction. J Am Coll Cardiol. 1992;20:1313-1317.19. Solimene MC, Ramires JA, Gruppi CJ, et al. Prognostic significance of silent myocardialischemia after a first uncomplicated myocardial infarction. Int J Cardiol. 1993;38:41-47.20. Silva P, Galli M, Campolo L. Prognostic significance of early ischemia after acutemyocardial infarction in low-risk patients. IRES (Ischemia Residua) Study Group. Am J Cardiol. 1993;71:1142-1147.21. Gill JB, Cairns JA, Roberts RS, et al. Prognostic importance of myocardial ischemiadetected by ambulatory monitoring early after acute myocardial infarction. N Engl J Med.1996;334:65-70.22. McCulley ME, Bennett RL. ST segment monitoring in the pediatric ICU: detectingmyocardial ischemia in children. Crit Care Nurse. April 1997;17:81-92.23. DeWood MA, Spores J, Notske R, et al. Prevalence of total coronary occlusion duringthe early hours of transmural myocardial infarction. N Engl J Med. 1980;303:897-902.24. Kwon K, Freedman SB, Wilcox I, et al. The unstable ST segment early afterthrombolysis for acute infarction and its usefulness as a marker of recurrent coronary occlusion. Am J Cardiol. 1991;67:109-115.25. Hackett D, Davies G, Chierchia S, Maseri A. Intermittent coronary occlusion in acutemyocardial infarction: value of combined thrombolytic and vasodilator therapy. N Engl J Med. 1987;317:1055-1059.26. Krucoff MW, Croll MA, Pope JE, et al. Continuously updated 12-lead ST-segmentrecovery analysis for myocardial infarct artery patency assessment and its correlation with multiple simultaneous early angiographic observations. Am J Cardiol. 1993;71:145-151.27. Dellborg M, Riha M, Swedberg K. Dynamic QRS complex and ST-segment monitoringin acute myocardial infarction during recombinant tissue-type plasminogen activator therapy. Am J Cardiol. 1991;67:343-349.28. Davies GJ, Chierchia S, Maseri A. Prevention of myocardial infarction by very early

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
17 of 20 4/10/2006 9:33 AM
treatment with intracoronary streptokinase: some clinical observations. N Engl J Med.1984;311:1488-1492.29. Veldkamp RF, Green CL, Wilkins ML, et al. Comparison of continuous ST-segmentrecovery analysis with methods using static electrocardiograms for noninvasive patency assessment during acute myocardial infarction. Thrombolysis and Angioplasty in Myocardial Infarction (TAMI) 7 Study Group. Am J Cardiol. 1994;73:1069-1074.30. Langer A, Krucoff MW, Klootwijk P, et al. Noninvasive assessment of speed and stabilityof infarct-related artery reperfusion: results of the GUSTO ST-segment monitoring study. J Am Coll Cardiol. 1995;25:1522-1557.31. Dellborg M, Topol EJ, Swedberg K. Dynamic QRS complex and ST-segmentvectorcardiographic monitoring can identify vessel patency in patients with acute myocardial infarction treated with reperfusion therapy. Am Heart J. 1991;122:943-948.32. Santoro GM, Valenti R, Buonamici P, et al. Relation between ST-segment changes andmyocardial perfusion evaluated by myocardial contrast echocardiography in patients with acute myocardial infarction treated with direct angioplasty. Am J Cardiol. 1998;82:932-937.33. Gomez M, Anderson JL, Karagounis LA, Mulhestein JB, Mooers FB. An emergencydepartment-based protocol for rapidly ruling out myocardial ischemia reduces hospital time and expense: results of a randomized study (ROMIO). J Am Coll Cardiol. 1996;28:25-33.34. DeLeon AC, Farmer CA, King G, Manternach J, Ritter D. Chest pain evaluation unit: acost-effective approach for ruling out acute myocardial infarction. South Med J.1989;82:1083-1089.35. Gaspov JM, Lee TH, Cook EF, Weisberg MC, Goldman L. Outcome of rule-outmyocardial infarction patients admitted to a new short stay unit. Am J Cardiol. 1991;68:145-149.36. Gibler WB, Walsh RA, Levy RC, Runyon JP. Rapid diagnostic and treatment center forpatients with chest pain in the emergency department. Ann Emerg Med. 1995;25:1-8.37. Klootwijk P, Hamm C. Acute Coronary Syndromes: Diagnosis. Lancet. 1999;353, Suppl II:10-1538. Krucoff MW, Parente AR, Bottner RK, et al. Stability of multilead ST-segment“fingerprints” over time after percutaneous transluminal coronary angioplasty and itsusefulness in detecting reocclusion. Am J Cardiol. 1988;61:1232-1237.39. Detre K, Holubkov R, Kelsey S, et al. One-year follow-up results of the 1985-1986National Heart, Lung, and Blood Institute’s Percutaneous Transluminal CoronaryAngioplasty Registry. Circulation. 1989;80:421-428.40. Jeremias A, Kutscher S, Haude M, et al. Nonischemic chest pain induced by coronaryinterventions: a prospective study comparing coronary angioplasty and stent implantation. Circulation. 1998;98:2656-2658.41. Tomai J, Crea F, Gaspardone A, et al. Mechanisms of cardiac pain during coronaryangioplasty. J Am Coll Cardiol. 1993;22:1892-1896.42. Mangano DT, Browner WS, Hollenberg M, London MJ, Tubau JF, Tateo IM. Associationof perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. The Study of Perioperative Ischemia Research Group. N Engl J Med. 1990;323:1781-1788.43. Mangano DT, Hollenberg M, Fegert G, et al. Perioperative myocardial ischemia inpatients undergoing noncardiac surgery, I: incidence and severity during the four-day perioperative period. The Study of Perioperative Ischemia (SPI) Research Group. J Am Coll Cardiol. 1991;17:843-850.44. Mangano DT, Wong MG, London MJ, Tubau JF, Rapp JA. Perioperative myocardialischemia in patients undergoing noncardiac surgery, II: incidence and severity during the first week following surgery. The Study of Perioperative Ischemia (SPI) Research Group. J Am Coll Cardiol. 1991;17:851-857.45. Hollenberg M, Mangano DT, Browner WS, London MJ, Tubau JF, Tateo IM. Predictorsof postoperative myocardial ischemia in patients undergoing noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA. 1992;268:205-209.46. Krucoff MW, Sawchak ST, Pope JE, Veldkamp RF. Rethinking classical ECG patternsof ischemia and infarction: insights from investigations with continuous ECG monitoring. Newspaper Cardiol. December 1992:8-17.47. Klootwijk P, Meij S, von Es GA, et al. Comparison of usefulness of computer assisted

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
18 of 20 4/10/2006 9:33 AM
continuous 48-h 3-lead with 12-lead ECG ischaemia monitoring for detection and quantitation of ischaemia in patients with unstable angina. Eur Heart J. 1997;18:931-940.48. Krucoff MW, Jackson YR, Stark KS, Kent KM. Electrocardiographic patterns ofimpending coronary closure independent of unstable anginal symptoms. In: von Arnim Th, Maseri A, eds. Predisposing Condition for Acute Ischemic Syndromes. Darmstadt, Germany: Steinkopff Verlag; 1989:96-106.49. Veldkamp RF, Pope JE, Wilderman NM, Trollinger KM, et al. ST segment deviation onthe 12-lead electrocardiogram during acute myocardial infarction: Optimal leads for continuous ST segment monitoring. In: Veldkamp RF. Continuous Digital 12-Lead ST Segment Monitoring in Acute Myocardial Infarction [doctoral thesis]. Delft, The Netherlands: Eburon; 1995: 54-66.50. Krucoff MW. Poor performance of lead V5 in single- and dual-channel ST-segmentmonitoring during coronary occlusion. J Electrocardiol. 1988;21(suppl):S30-S34.51. Aldrich HR, Hindman NB, Hinohara T, et al. Identification of the optimalelectrocardiographic leads for detecting acute epicardial injury in acute myocardial infarction. Am J Cardiol. 1987;59:20-23.52. Bush HS, Ferguson JJ, Angelini P, Willerson JT. Twelve-lead electrocardiographicevaluation of ischemia during percutaneous transluminal coronary angioplasty and its correlation with acute reocclusion. Am Heart J. 1991;121:1591-1599.53. Drew BJ, Tisdale LA. ST-segment monitoring for coronary artery reocclusion followingthrombolytic therapy and coronary angioplasty: identification of optimal bedside monitoring leads. Am J Crit Care. 1993;2:280-292.54. Drew BJ, Ide B, Sparacino PSA. Accuracy of bedside electrocardiographic monitoring: areport on current practices of critical care nurses. Heart Lung. 1991;20:597-609.55. Quyyumi AA, Crake T, Mockus LJ, Wright CA, Frickards A, Fox KM. Value of the bipolarlead CM5 in electrocardiography. Br Heart J. 1986;56:372-376.56. Krucoff MW, Wagner NB, Pope JE, et al. The portable programmablemicroprocessor-driven real-time 12-lead electrocardiographic monitor: a preliminary report of a new device for the noninvasive detection of successful reperfusion or silent coronary reocclusion. Am J Cardiol. 1990;65:143-148.57. Krucoff MW, Green CE, Satler LF, et al. Noninvasive detection of coronary arterypatency using continuous ST-segment monitoring. Am J Cardiol. 1986;57:916-922.58. Krucoff MW, Pope JE, Bottner RK, Renzi RH, Wagner GS, Kent KM. Computer-assistedST-segment monitoring: experience during and after brief coronary occlusion. J Electrocardiol. 1987;20(suppl):15-21.59. Fernandez AR, Sequeira RF, Chakko S, et al. ST-segment tracking for rapiddetermination of patency of the infarct-related artery in acute myocardial infarction. J Am Coll Cardiol. 1995;26:675-683.60. Klootwijk P, Langer A, Meij S, et al. Non-invasive prediction of reperfusion and coronaryartery patency by continuous ST segment monitoring in the GUSTO-I trial. Eur Heart J. 1996;17:689-698.61. Mason RE, Likar I. A new system of multiple-lead exercise electrocardiography. Am Heart J. 1966;71:196-204.62. Macfarlane PW. Lead systems. In: Macfarlane PW, Lawrie TDV, eds. Comprehensive Electrocardiology. New York, NY: Pergamon Press Inc; 1989:315-352.63. Gamble P, McManu H, Jensen D, Froelicher V. A comparison of the standard 12-leadelectrocardiogram to exercise electrode placements. Chest. 1984;85:616-622.64. Rautaharju PM, Prineas RJ, Crow RS, Seale D, Furberg C. The effect of modified limbelectrode positions on electrocardiographic wave amplitudes. J Electrocardiol.1980;13:109-113.65. Papouchado M, Walker PR, James MA, Clarke LM. Fundamental differences betweenthe standard 12-lead electrocardiograph and the modified (Mason-Likar) exercise lead system. Eur Heart J. 1987;8:725-733.66. Sevilla DC, Dohrmann ML, Somelofski CA, Wawrzynski RP, Wagner NB, Wagner GS.Invalidation of the resting electrocardiogram obtained via exercise electrode sites as a standard 12-lead recording. Am J Cardiol. 1989;63:35-39.67. Pahlm O, Haisty WK, Edenbrandt L, et al. Evaluation of changes in standardelectrocardiographic QRS waveforms recorded from activity-compatible proximal limb lead

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
19 of 20 4/10/2006 9:33 AM
positions. Am J Cardiol. 1992;69:253-257.68. Frank E. An accurate, clinically practical system for spatial vectorcardiography.Circulation. 1956;13:737-749.69. Dower GE, Machado HB, Osborne JA. On deriving the electrocardiogram fromvectorcardiographic leads. Clin Cardiol. 1980;3:87-95.70. Pipberger HV, Bialek SM, Perloff JK, Schnaper HW. Correlation of clinical information inthe standard 12-lead ECG and in a corrected orthogonal 3-lead ECG. Am Heart J.1961;61:34-43.71. Dellborg M, Riha M, Swedberg K. Dynamic QRS and ST segment changes inmyocardial infarction monitored by continuous on-line vectorcardiography. J Electrocardiol.1991;23(suppl):1-9.72. Lundin P, Eriksson SV, Erhardt L, Strandberg LE, Rehnqvist N. Continuousvectorcardiography in patients with chest pain indicative of acute ischemic heart disease. Cardiology. 1992;81:145-156.73. Jensen SM, Johansson G, Osterman G, Reiz S, Näslund U. On-line computerizedvectorcardiography monitoring of myocardial ischemia during coronary angioplasty: comparison with 12-lead electrocardiography. Coron Artery Dis. 1994;5:507-514.74. Lundin P, Eriksson SV, Strandberg LE, Rehnqvist N. Prognostic informa tion fromon-line vectorcardiography in acute myocardial infarction. Am J Cardiol.1994;74:1103-1108.75. Lundin P, Eriksson SV, Fredrikson M, Rehnqvist N. Prognostic information from on-linevectorcardiography in unstable angina pectoris. Cardiology. 1995;86:60-66.76. Dellborg M, Steg PG, Simoons M, et al. Vectorcardiographic monitoring to assess earlyvessel patency after reperfusion therapy for acute myocardial infarction. Eur Heart J.1995;16:21-29.77. Klootwijk P, Meij S, Melkert R, Lenderink T, Simoons ML. Reduction of recurrentischemia with abciximab during continuous ECG-ischemia monitoring in patients with unstable angina refractory to standard treatment (CAPTURE). Circulation. 1998;98:1358-1364.78. Dower GE, Yakush A, Nazzal SB, Jutzy RV, Ruiz CE. Deriving the 12-leadelectrocardiogram from four (EASI) electrodes. J Electrocardiol. 1988;21(suppl):S182-S187.79. Drew BJ, Scheinman MM, Evans GT. Comparison of a vectorcardiographically derived12-lead electrocardiogram with the conventional electrocardiogram during wide QRS complex tachycardia and its potential application for continuous bedside monitoring. Am J Cardiol. 1992;69:612-618.80. Denes P. The importance of derived 12-lead electrocardiography in the interpretation ofarrhythmias detected by Holter recording. Am Heart J. 1992;124:905-911.81. Drew BJ, Adams MG, Pelter MM, Wung SF. ST-segment monitoring with a derived12-lead electrocardiogram is superior to routine CCU monitoring. Am J Crit Care. 1996;5:198-206.82. Drew BJ, Adams MG, Pelter MM, Wung SF, Caldwell MA. Comparison of standard andderived 12-lead electrocardiograms for diagnosis of coronary angioplasty-induced myocardial ischemia. Am J Cardiol. 1997;79:639-644.83. Drew BJ, Pelter MM, Wung SF, et al. Accuracy of the EASI 12-lead electrocardiogramcompared to the standard 12-lead electrocardiogram for diagnosing multiple cardiac abnormalities. J Electrocardiol. In press.84. Veldkamp RF. Chapter 10, Discussion. In: Continuous Digital 12-Lead ST Segment Monitoring in Acute Myocardial Infarction [doctoral thesis]. Delft, The Netherlands: Eburon; 1995: 92-128. 85. Mirvis DM, Berson AS, Goldberger AL, et al. Instrumentation and practice standards forelectrocardiographic monitoring in special care units: a report for health professionals by a task force of the Council on Clinical Cardiology, American Heart Association. Circulation. 1989;79:464-471.86. Biagini A, L’Abbate A, Testa R, et al. Unreliability of conventional visualelectrocardiographic monitoring for detection of transient ST segment changes in acoronary care unit. Eur Heart J. 1984;5:784-791.87. Pepine C, Singh B, Gibson R, Kent K. Report of Group IV: management options. In:Cohn PF, Kannel WB, eds. Recognition, Pathogenesis, and Management Options in Silent

CONSENSUS STATEMENT FOR PRACTICE http://www.aacn.org/AACN/jrnlajcc.nsf/GetArticle/ArticleFour86?Ope...
20 of 20 4/10/2006 9:33 AM
Coronary Artery Disease. Circulation Monograph No. 2. 1987;75(3):II52-II53. 88. Drew BJ, Wung SF, Adams MG, Pelter MM. Bedside diagnosis of myocardial ischemiawith ST-segment monitoring technology: measurement issues for real-time clinical decision making and trial designs. J Electrocardiol. 1998;30(suppl):174-182.89. Schröder R, Dissmann R, Brüggemann T, et al. Extent of early ST-segment elevationresolution: a simple but strong predictor of outcome in patients with acute myocardial infarction. J Am Coll Cardiol. 1994;24:384-391.90. Feldman T, Borow K, Neumann A, Lang RM, Childers RW. Relation ofelectrocardiographic R wave amplitude to changes in left ventricular chamber size and position in normal subjects. Am J Cardiol. 1985;55:1168-1174.91. Adams MG, Drew BJ. Body position effects on the ECG. J Electrocardiol. 1997;30:285-291.92. Pelter MM, Adams MG, Drew BJ. Computer versus manual measurement ofST-segment deviation. J Electrocardiol. 1997;30:151-156.
Take The CE Test
American Association of Critical-Care Nurses101 Columbia, Aliso Viejo, CA 92656-4109
1-800-899-2226 or 949-362-2000 (Phone)  949-362-2020 (Fax) email: [email protected] ©2006 All Rights Reserved
AACN Website Disclaimer