ecg: multifocal atrial tachycardia
TRANSCRIPT
Physician’s MeetM3 unit Dr. S Sundar’s Unit ECG of the weekDr. Deepu Sebin
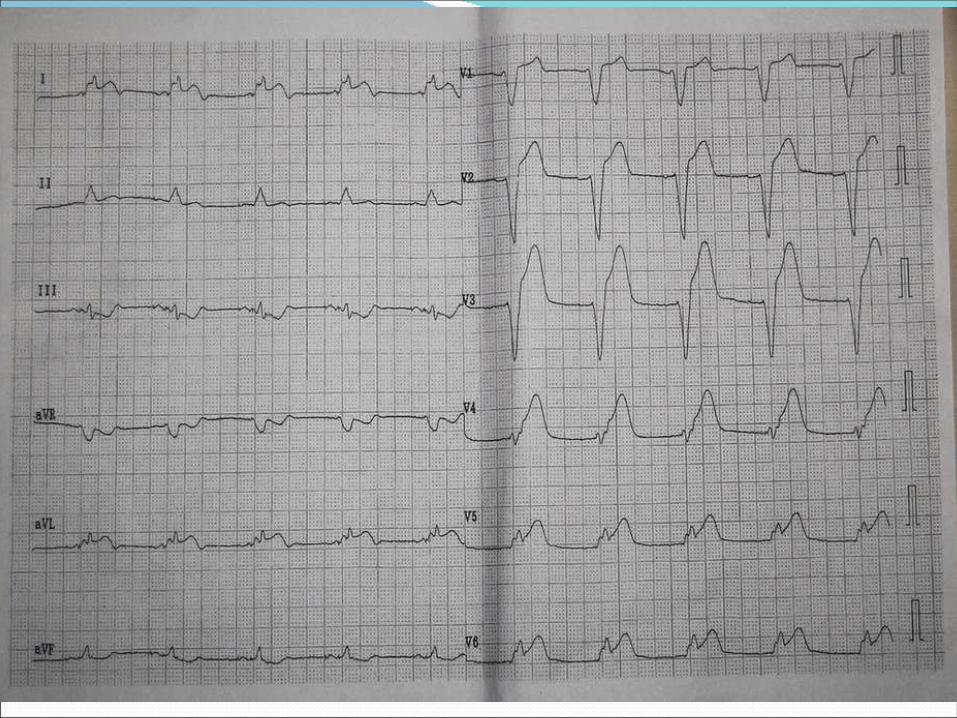
12 lead ECG Sinus Rhythm Rate = 62/m Axis = +30 Pace maker spikes + PR Interval = 0.12 QRS duration = 0.16sec LBBB pattern Concordent ST evelevation in V4,V5,V6,1,aVL ST segment depression in 111,aVF

AnteroLateral MI with LBBB

LBBB and MI Left bundle branch block (LBBB) is present in
approximately 7 percent of acute infarctions
Patients with LBBB have more comorbid conditions, are less likely to receive therapy, and have an increased risk for in-hospital death compared with patients with no BBB.
- - - . TI Bundle branch block and in hospital mortality in acute myocardial infarction National Registry of 2 .Myocardial Infarction Investigators
- ; ; ; ; AU Go AS Barron HV Rundle AC Ornato JP Avins AL - 1998 1;129(9):690-7.SO Ann Intern Med Nov
The sequence of repolarization is altered in LBBB, with the ST segment and T wave vectors being directed opposite to the QRS complex. These changes may mask the ST segment depression and T wave inversion induced by ischemia.
The diagnosis of an acute MI or ischemia can occasionally be made in a patient with underlying LBBB if certain ST-T changes are seen, particularly if the ST-T vectors are in the same direction as the QRS complex.
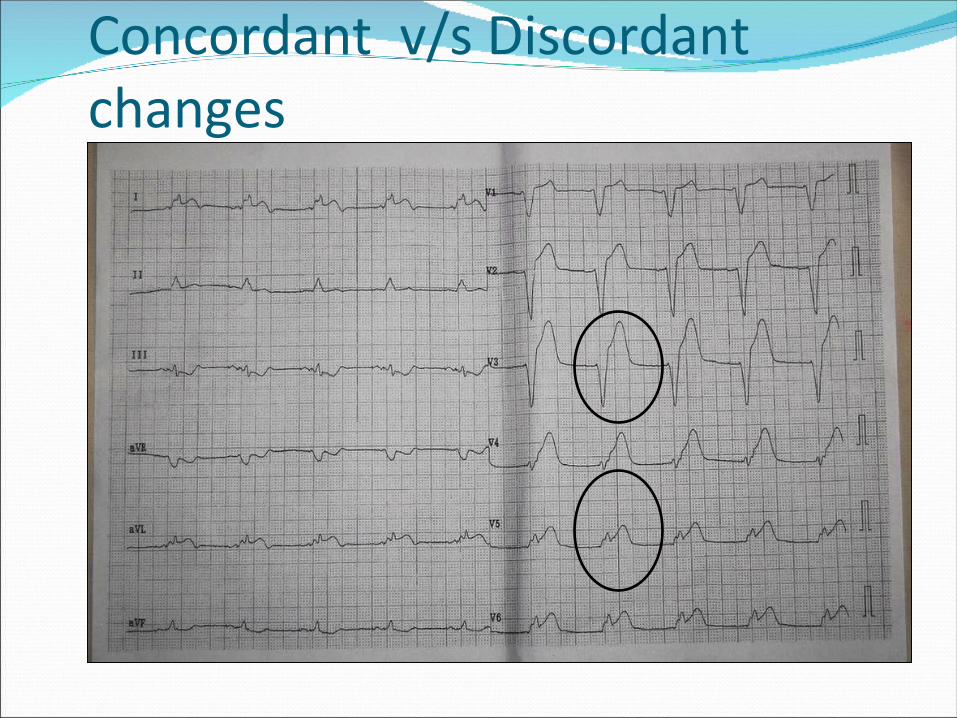
Concordant v/s Discordant changes
Sgarbossa Criteria The three ECG criteria with an independent value in the
diagnosis of acute infarction and the score for each were: ST segment elevation of 1 mm or more that was in the same
direction (concordant) as the QRS complex in any lead — score 5.
ST segment depression of 1 mm or more in any lead from V1 to V3 — score 3.
ST segment elevation of 5 mm or more that was discordant with the QRS complex (ie, associated with a QS or rS complex) — score 2
Electrocardiographic - . -1 diagnosis of evolving acute myocardial infarction in the presence of left bundle branch block GUSTO
( ) Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries.Investigators
- ; ; ; ; ; ; ; AU Sgarbossa EB Pinski SL Barbagelata A Underwood DA Gates KB Topol EJ Califf RM Wagner GS
- 1996 22;334(8):481-7SO N Engl J Med Feb

At a score-sum of 3, these criteria have a specificity of 90% for detecting a myocardial infarction.

A Sgarbossa score of ≥ 3 was highly specific (ie, few false positives) but much less sensitive (36 percent) in the validation sample in the original report. Similar findings were noted in a subsequent meta-analysis of 10 studies of 1614 patients in which a Sgarbossa score of ≥ 3.

Additional Findings The presence of deep T wave inversions in leads with a
predominantly negative QRS complex (eg, V1-V3) is highly suggestive of evolving ischemia or MI.
The presence of QR complexes in leads I, V5, or V6, or in II, III, and aVF with LBBB strongly suggests underlying infarction.
Pseudonormalization of previously inverted T waves is suggestive but not diagnostic of ischemia.

Additional Findings An anterolateral MI should be suspected if new S waves
appear in leftward leads (I, aVL, and V6) in a patient with preexisting common LBBB.
Underlying MI is also suggested by notching of the ascending part of a wide S waves in the mid-precordial leads ( ' Cabrera s sign) is present.

Additional Findings Cabrera's sign
refers to prominent (0.05 sec) notching in the ascending limb of the 3 4 . S wave in leads V and V
Chapman's sign : a similar finding is prominent notching (>/= 0.05 sec ) of
the ascending limb of the 5 6 . R wave in lead V or V
These signs have a specificity that approaches 90 percent. However, there may be a high degree of interobserver variability in accurate identification and their sensitivity is quite low.

Serial ECG changes — 67 percent sensitivity ST segment elevation — 54 percent sensitivity Abnormal Q waves — 31 percent sensitivity Initial positivity in V1 with a Q wave in V6 — 20 percent
sensitivity but 100 percent specificity for anteroseptal MI. Cabrera's sign — 27 percent sensitivity overall, 47 percent
for anteroseptal MI
In addition to difficulties in ECG interpretation, approximately one-half of patients with LBBB and an acute MI do not have chest pain. These patients are much less likely to receive appropriate medical therapy (eg, aspirin, beta blockers) or reperfusion therapy than LBBB patients with chest pain.

Serial ECGs, Enzymes help in diagnosis American College of Cardiology/American Heart
Association guidelines recommend reperfusion therapy for all patients with LBBB whose history suggests acute myocardial infarction.

Thank you