echocardiographic evaluation of the valves and roots of the pulmonary artery and aorta in the...
TRANSCRIPT

J Clin Ultrasound 20:3-9, January 1992 0 1992 by John Wiley & Sons, Inc. CCC 0091-2751/92/0103-09 $04.00
Echocardiographic Evaluation of the Valves and Roots of the Pulmonary Artery and Aorta
in the Developing Fetus
Jing Deng, M.Med,* Pei-Xuan Cheng, MD,* Shu-Ying Gao,t and LiangZhen Wen$
Abstract: Because of the fluid-filled lungs in the fetus, the ultrasound beam can penetrate to the root of the pulmonary artery perpendicularly. Using M-mode echo- cardiography, the following dimensions were measured: the pulmonary and aortic valve excursion in 19 fetuses, and the pulmonary and aortic root internal diameter in 70 fetuses, between 18 and 42 weeks, menstrual age. The measured dimensions were then correlated with the biparietal diameter. The correlation coefficients for the measurements ranged from 0.873 to 0.892. Regression analysis showed that the best fit of the data was a linear model from which the 5% and 95% confidence limits were derived for individual predictions of the arterial dimensions. The ratios of the pulmonarylaartic valve excursion and the pulmonary/aortic internal diameter were approximately 1 : 1. These results are of potential value in the prenatal detection of great arterial valve or root diseases. Indexing Words: Aorta Pulmonary artery - Semilunar valve
Fetus . Echocardiography -
The growth profiles of many cardiac dimen- sions have been established using M-mode echo- cardiography (M-mode) in the normal human
However, that of pulmonary arterial valve excursion (PAVE) has not been reported previously. Moreover, investigators have found it difficult to diagnose prenatally valvular anoma- lies, such as pulmonary and aortic stenoses, us- ing only real-time two-dimensional echocardiog- r a ~ h y . ~ - " During our study on fetal cardiac di- mensions," we realized that it was possible to evaluate PAVE as well as aortic valve excursion (AOVE), pulmonary arterial root internal diam- eter (PAID), and aortic root internal diameter (AOID) by means of M-mode.
From the Departments of *Pediatrics, tultrasonics, and SOb- stetrics and Gynecology, Tongji Hospital, Tongji Medical University, Wuhan, People's Republic of China. For reprints contact Jing Deng, M.Med, Department of Ultrasonics, Wu- han First Hospital, Wuhan 430022, People's Republic of China.
MATERIALS AND METHODS
Using an RT 2600 linear array scanner with 3.5- MHz transducer (Yokogawa Medical System, Ja- pan), ultrasound examinations were performed in 70 normal human fetuses between 18 and 42 weeks, menstrual age (MA). There was no ma- ternal history of disease that predisposed the fe- tuses to abnormal growth.
Real-time imaging of the fetuses were ob- tained for measurement of the biparietal diame- ter (BPD) and identification of cardiac and non- cardiac anomalies, such as congenital heart dis- ease, arrhythmias, hydrops, intrauterine growth retardation, macrosomia, and poly- and oligohy- dramnios.
All the subjects were followed-up by a pediat- ric cardiologist for more than 3 months after birth to confirm the absence of cardiac abnormal- ities.
M-mode images were obtained by (1) Imaging real-time cardiac planes that contained the structures to be measured, for example, imaging the tricuspid- pulmonary plane or left ventricu- lar short axis plane12 for measuring PAVE and PAID, and imaging the cardiac base short axis
3

4 DENG ET AL.
M
I I
FIGURE 1. (Above and opposite pagel M-mode measurements. In the real-time imaging of the tricuspid-pul- monary plane (1) and 5-chamber plane (3), M-mode cursors (M) were placed perpendicular to the pulmonary and aortic roots, respectively. (2) and (4) These show the M-mode tracings of the pulmonary (PA) and aortic (AO) roots, in which the opening box and closing line of the pulmonary and aortic valve motions were sim- ilar to each other. The fourth box in (2) was standard enough for PAVE measurement because the closing lines of the pre- and postbox were single, not double like the lines before the first box. (5) and (6) Drawings of (1)-(4). The measurements were made in these locations: PAID: 1-4; PAVE: 2-3; AOID: 5-8; AOVE: 6-7. (RA: right atrium; RV: right ventricle; RVOT: right ventricular outflow tract; TV: tricuspid valve; PV: pulmonary valve; LA: left atrium; LV: left ventricle.)
plane or the 5-chamber plane12 for measuring AOVE and AOID. (2) Placing the M-mode cursor perpendicular to the great artery at the level of the valve under real-time guidance. (3) Record-
ing the M-mode tracing when no fetal move- ments were present.
To standardize the procedure, measurements were made only on the M-mode tracings that
JOURNAL OF CLINICAL ULTRASOUND

PULMONARY ARTERY AND AORTA IN FETUS 5
M
I I
FIGURE 1 (continued).
showed both the valve closing line, represent- ed as a single line in the center of the two walls of the artery, and the opened valve box (Figure 1).
All the measurements were done by one oper- ator (JD) with the inner-to-inner edge technique to the nearest 0.5 mm. Statistical analysis was carried out with an IBM PC/XT computer by means of a general statistics program that al- lowed for correlation, regression, derivation of confidence limits in the population and individ- ual prediction limits, and printout of graphs of
the data (Department of Health Statistics, the Medical University of West China).
RESULTS
PAVE and AOVE were measured in 19 fetuses from 20 weeks to 42 weeks, MA, and PAID and AOID in 70 fetuses from 18 weeks to 42 weeks, MA. The normograms for the pulmonary and aortic valve motion in prenatal life were similar to the pattern of the aortic valve motion, and dif-
VOL. 20. NO. 1, JANUARY 1992
6 DENG ET AL.
TABLE 1 Correlation and Regression Analysis Comparing Biparietal
Diameter with Arterial Parameters
Correlation Regression
Y" n r P Value a b S x p FTest
PAVE 19 0.890 <0.001 -0.7235 0.0681 0.4348 65' AOVE 19 0.886 <0.001 -1.2379 0.0713 0.4657 62' PAID 70 0.892 <0.001 -2.8434 0.1329 0.9358 264' AOID 70 0.873 <0.001 -2.1442 0.1154 0.8933 219'
~
" Y = a + bX, i n which Y is the arterial parameter (mm) and X is
bSxy = Standard error of the estimate (rnm). "p < 0.0001.
the biparietal diameter (mm).
ferent from that of the pulmonary valve, in post- natal Iife.13
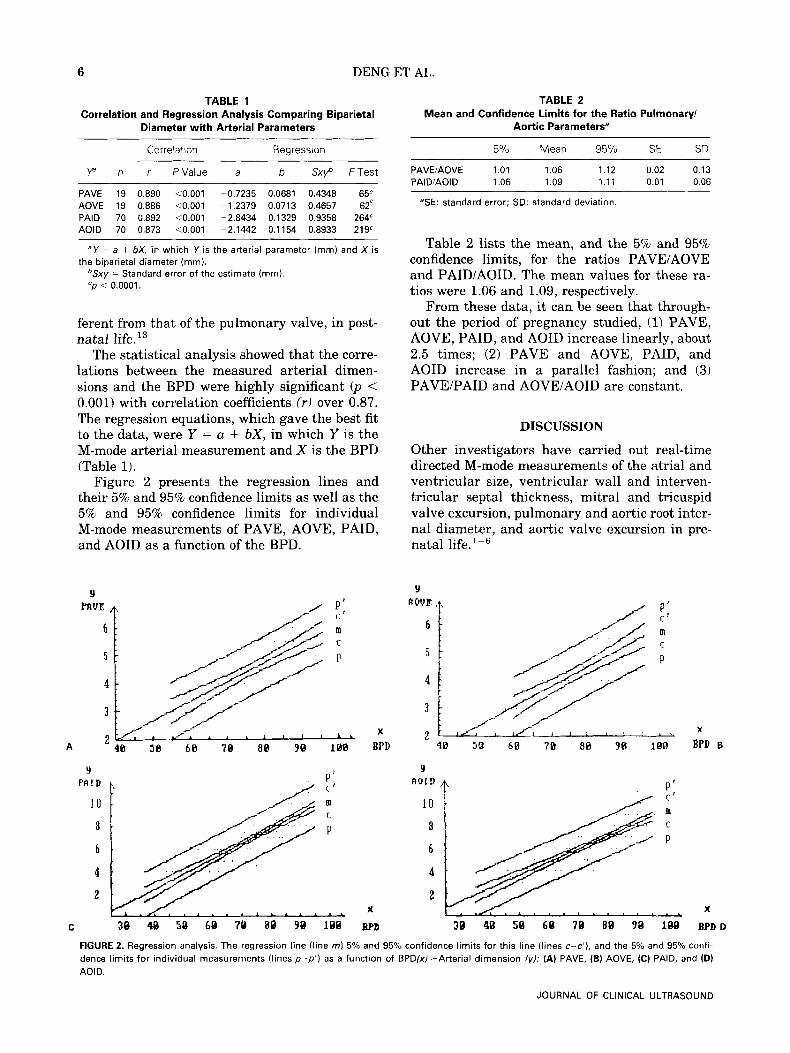
The statistical analysis showed that the corre- lations between the measured arterial dimen- sions and the BPD were highly significant ( p < 0.001) with correlation coefficients (r) over 0.87. The regression equations, which gave the best fit to the data, were Y = a + bX, in which Y is the M-mode arterial measurement and X is the BPD (Table 1).
Figure 2 presents the regression lines and their 5% and 95% confidence limits as well as the 5% and 95% confidence limits for individual M-mode measurements of PAVE, AOVE, PAID, and AOID as a function of the BPD.
TABLE 2 Mean and Confidence Limits for the Ratio Pulmonary/
Aortic Parameters"
5% Mean 95% SE SD
PAVEIAOVE 1.01 1.06 1.12 0.02 0.13 PAIDIAOID 1.06 1.09 1.11 0.01 0.06
5 E : standard error; SD: standard deviation.
Table 2 lists the mean, and the 5% and 95% confidence limits, for the ratios PAVE/AOVE and PAID/AOID. The mean values for these ra- tios were 1.06 and 1.09, respectively.
From these data, it can be seen that through- out the period of pregnancy studied, (1) PAVE, AOVE, PAID, and AOID increase linearly, about 2.5 times; (2) PAVE and AOVE, PAID, and AOID increase in a parallel fashion; and (3) PAVE/PAID and AOVE/AOID are constant.
DISCUSSION
Other investigators have carried out real-time directed M-mode measurements of the atrial and ventricular size, ventricular wall and interven- tricular septa1 thickness, mitral and tricuspid valve excursion, pulmonary and aortic root inter- nal diameter, and aortic valve excursion in pre- natal
P PAID
1 0 10 '
8
6
4
2 X X
C 38 48 50 69 78 88 98 188 BPI) 38 48 58 68 78 88 98 188 BPDD
FIGURE 2. Regression analysis. The regression line (line rn) 5% and 95% confidence limits for this line (lines c-c') , and the 5% and 95% confi- dence limits for individual measurements (lines p - p ' ) as a function of BPDlxl-Arterial dimension (yl; (A) PAVE, (B) AOVE, (C) PAID, and ID) AOID.
JOURNAL OF CLINICAL ULTRASOUND

PULMONARY ARTERY AND AORTA IN FETUS 7
In postnatal life, it remains a problem to di- rect the ultrasound beam perpendicular to the pulmonary root because of lung interference. M-mode tracing of the pulmonary valve, a single curve with “A Dip,” is actually the echogram of its posterior cusp,13 different from the box- shaped tracing revealed from studies of the fetal pulmonary valve. Thanks to the presence of fluid in the lungs, which does not obstruct ultrasound, and the relatively low impedance of the fetal ribs to ultrasound except in the late pregnancy, a wider imaging window is available for fetal echo- cardiography. Therefore, the real-time image of the pulmonary artery can be obtained much eas- ier in utero; only in utero can the M-mode trac- ing of the box-shaped PAVE be obtained, permit- ting positioning the ultrasound beam perpendic- ular to the arterial root.
No significant difference was found between PAVE measurements sampled in the tricuspid- pulmonary plane, and in the left ventricular short axis plane, although PAVE tracings from the former plane was the echo of the anatomi- cally anteroleft and anteroright cusps, while that from the latter was the echo of anteroright and posterior cusps.
Admittedly, only 19 cases of PAVE and AOVE were measured, but this does not mean that the M-mode recordings of the valve excursion are difficult to obtain. In fact, we could obtain such recordings in about 70% of the cases after realiz- ing that the excursion could also be imaged and measured during the original M-mode study of PAID, AOID, and other cardiac dimensions.” And we think that the measurement of PAVE is not more difficult than that of AOVE in the fe- tus.
Standardizing the recordings by using the maximal opening box and the single closing line of the semilunar valve motion minimized mea- suring error. The standard errors of the esti- mates for PAVE and AOVE were, in fact, small enough (Sxy <0.5) for practical purposes.
That we used BPD as the independent vari- able is based on the fact that the BPD is one of the best predicted and most commonly used pa- rameters for relating other cardiac dimensions to fetal age during second- and third-trimester p r e g n a n ~ y . ~ . ~ But if the fetal head is thought to be abnormal (e.g., anencephaly and hydroceph- aly), one should use the mean BPD of a normal fetus at the same menstrual age instead.
Our study has shown that PAVE, AOVE, PAID, and AOID grow linearly with the fetal age. PAVE and PAID are nearly equal to, or slightly larger than, AOVE and AOID, respec- VOL. 20. NO. 1, JANUARY 1992
tively. The results are similar to that reported
The establishment of intrauterine growth pro- files for arterial dimensions measured by M-mode is of potential value in detecting fetal cardiac disease affecting the outflow tract of the right or left ventricle. For instance, if the ratio of the pulmonary/aortic dimension is significantly different from 1 : 1, a malformation and/or mal- function of one or both of the arteries should be suspected. By measuring the individual PAVE, AOVE, PAID, and AOID, and comparing the measured dimensions with the normal limits specified by the BPD, investigators may be sure which one or whether both of the arteries are ab- normal.
Semilunar valve atresia can be excluded when the M-mode displays actual cusp separation of valve leaflets, where real time may only show a moving valve which could be a t re tk2
With only real-time scanning, the moderate and mild stenoses were frequently over l~oked ,~- l~ although most of the critical cases may be diag- nosed14 in utero. The few successful diagnoses of noncritical cases were only based on indirect signs in real-time imaging, such as hypertrophy or hy- poplasia of the right ventricle in pulmonary steno- sis, or on the turbulent high-velocity blood flow in pulsed Doppler recordings,” which might have exposed the fetus to high sound energy. With the M-mode technique described here, it appears pos- sible to prenatally recognize semilunar valve stenoses, at least the moderate and critical ones, when valve excursions are shown to be narrower than expected.
It was noted that the stenotic semilunar valve opening in systole is like a dome.15 Thus, by po- sitioning the M-mode cursor at different levels above the valve attachment to the orifice, differ- ent appearances of the valve M-mode tracing will be obtained, leading to different diagnoses for the same case (Figure 3). At level a or d, no measurement should be made because of the presence of two closing lines (a) or no closing line (d) in diastole. At level b, the stenosis might be overlooked or its degree underestimated. Only at level (c) could the correct diagnosis of the de- fect be made. In practice, however, the exact po- sition of the sampling cursor is uncertain due to the resolution limit of updated real-time imag- ing. Therefore, it is necessary to sweep the cur- sor from the root to the top (from levels a t o d) of the semilunar valves. Because the stenosis may develop in late pregnancy,’~~~ exclusion of the disease should not be dependent on normal valve excursion measured in early pregnancy.

8 DENG ET AL.
a b c d
OVPFLOU TRACT ‘m ERIAL ROOT
* I b I C I d
FIGURE 3. Different sampling positions and corresponding appear- ances of M-mode tracings of stenotic semilunar valve motion which may affect the diagnosis (see text). The solid line indicates the valve location in systole while the dotted line its location in diastole.
Before concluding that a malformation is present, functional factors should be ruled out that may lead to abnormal arterial dimension. In another study,17 diminished AOVE and AOID were found in an M-mode recording in a fetus. Because a primary lesion, coarctation of the aorta, was identified with real-time imaging, the finding of diminished aortic dimensions, instead of the increased dimensions scan in postnatal life, was considered secondary to less blood flow through the ascending aorta rather than a struc- tural defect of the aortic root or valve. In this sit- uation Doppler echocardiography would be use- ful in differentiating organic stenosis from func- tional hypohemodynamics.lO,ls
In conclusion, fetal M-mode echocardiography appears to be a practical method for evaluating the dimensions of the great arteries and semilu- nar valve motions. It is likely to play a role in detecting fetuses with arterial root and valve ab- normalities.
ACKNOWLEDGMENTS
We thank Qing-Ping Zhang, MD, Xin-Fang Wang, MD, Ke Shi, and Mou-Yi He for techno- logical advising, and Yue-Wu Liang of Tongji Medical University for computer operating.
1
REFERENCES
Wladimiroff JW, McGie JS: M-mode ultrasonic as- sessment of fetal cardiovascular dynamics. B r J Obstet Gynecol 88:1241, 1981.
2. Allan LD, Joseph MC, Boyd EC, et al: M-mode echocardiography in the developing human fetus. B r Heart J 47:573-583, 1982.
3. De Vore GR, Siassi B, Platt LD: Fetal echocardi- ography IV. M-mode assessment of ventricular size and contractility during the second and third trimesters of pregnancy in the normal fetus. A m J Obstet Gynecol 150:981-98, 1984.
4. De Vore GR, Siassi B, Platt LD: Fetal echocardi- ography V. M-mode measurements of the aortic root and aortic valve in second- and third-trimes- ter normal human fetus. Am J Obstet Gynecol
5. Cartier MS, Davidoff A, Warneke LA, et al: The normal diameter of the fetal aorta and pulmonary artery: Echocardiographic evaluation in utero.
6. De Vore GR, Siassi B, Platt LD: Fetal echocardi- ography VIII. Aortic root dilation-A marker for tetralogy of Fallot. Am J Obstet Gynecol 159:129- 136,1988.
7. Cope1 JA, Pilu G, Green J, et al: Fetal echocardio- graphic screening for congenital heart disease: The importance of 4-chamber view. Am J Obstet Gynecol 157:648-652, 1987.
8. Benacerraf BR, Pober BR, Sanders SP: Accuracy of fetal echocardiography. Radio1 165:847- 849, 1987.
9. Allan LD, Crawford DC, Chita SK: Confidence limits of fetal echocardiography. Pediatr Cardiol 9:188, 1988.
10. Hata T, Takamori H, Hata K, et al: Antenatal di- agnosis of congenital heart disease and fetal ar- rhythmias by ultrasound: Prospective study. Gy- necol Obstet Invest 26:118-125, 1988.
11. Deng J, Cheng PX, Gao SY, et al: M-mode echocardiographic measurements of the cardiac and great arterial dimensions in the developing fetus. Presented at The First National Congress of Echocardiography, Beijing, Dec. 10, 1989, p 133.
12. Allan LD, Tynan MJ, Campbell S, et al: Echocar- diographic and anatomical correlates in the fetus. Br Heart J 44:444-451, 1980.
13. Hagen-Ansert SL: Echocardiographic techniques and evaluation, in Textbook of Diagnostic Ultra- sonography (ed 21, Hagen-Ansert SL (ed). CV Mosby Co, St. Louis, MO, 1983, p 378-420.
14. Allan LD, Crawford DC, Tynan MJ. Pulmon- ary atresia in prenatal life. B r Heart J 54:640, 1985.
15. Sahn DJ, Anderson F: Pulmonary valve stenosis, Two-Dimensional Anatomy of the Heart, in Sahn DJ, Anderson F (eds). John Wiley & Sons, New York, 1982, p 84.
16. Todros T, Presbitero P, Gaglioti P, et al: Pulmo- nary stenosis with intact ventricular septum: Doc- umentation of development of the lesion echocar- diographically during fetal life. Int J Cardiol
17. Deng J , Cheng PX, Gao SY, et al: Echocardio-
152:543-550, 1985.
A J R 149(5):1003-1007, 1987.
19~355-362, 1988.
JOURNAL OF CLINICAL ULTRASOUND

PULMONARY ARTERY AND AORTA IN FETUS 9
graphic differentiation of the types of coarctation of the aorta in utero. Chin J Phys Med 12278, 1990.
18. Yagel S, Hochner-Celnikier D, Hurwitz A, et al:
The significance and importance of prenatal diag- nosis of fetal cardiac malformations by Doppler echocardiography. Am J Obstet Gynecol 158:272- 277, 1988.
VOL. 20, NO. 1, JANUARY 1992