echocardiography in advanced heart...
TRANSCRIPT
Echocardiography in Advanced
Heart Failure
William F. Armstrong M.D.
University of Michigan
Disclosure: Thoratec
The Role of Echocardiography in
LVADs
• Determine suitability / need of patient
• Assess LV and RV function pre-implant
• LV thrombus
• PHTN
• Pre-implant aortic insufficiency
• Presence of PFO
LVADs General Principles
• Blood removed from LV apex via cannula
• Pump generates flow and pressure• Currently utilized LVADs are continuous flow
devices
• Pump flow is in part preload dependent
• Creates a degree of pulsatility in outflow
• Blood delivered to ascending aorta
• Variable contribution of LV to forward flow
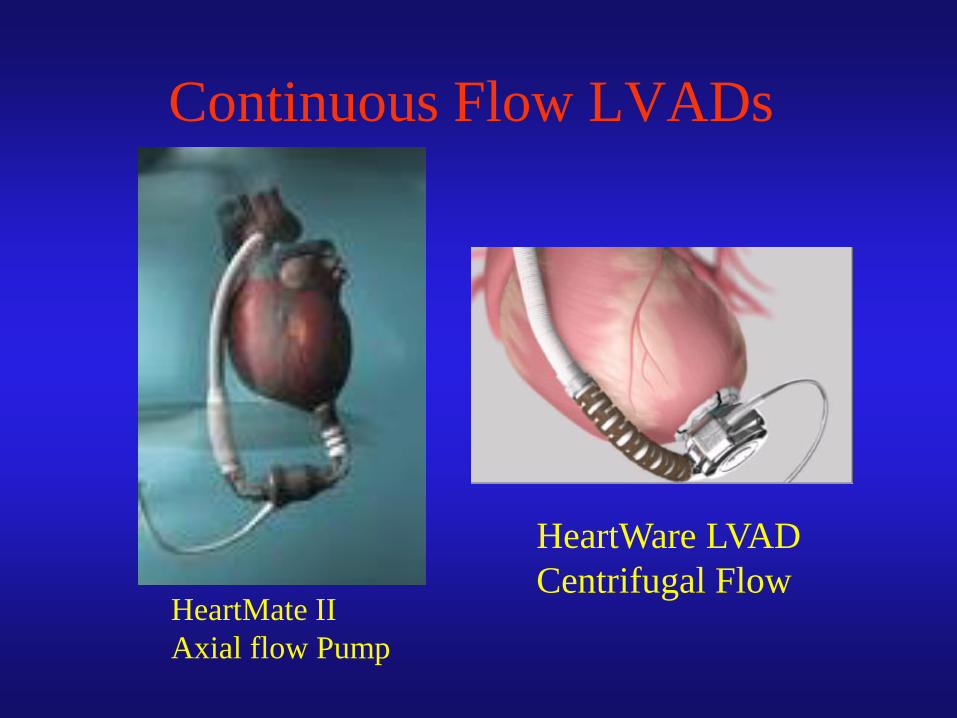
Continuous Flow LVADs
HeartWare LVAD
Centrifugal Flow HeartMate II
Axial flow Pump
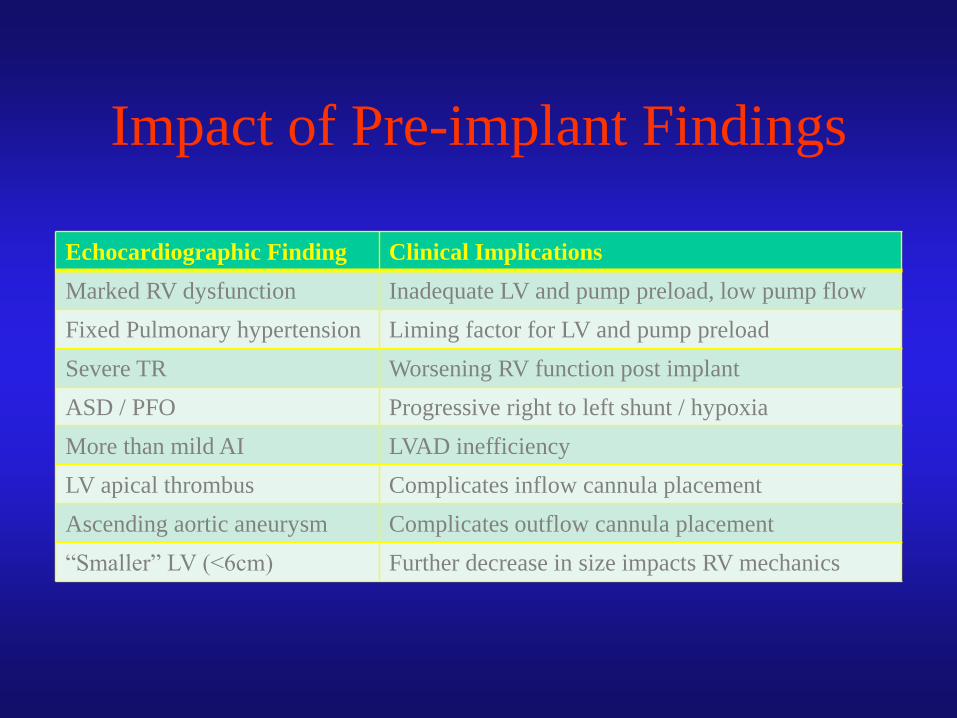
Impact of Pre-implant Findings
Echocardiographic Finding Clinical Implications
Marked RV dysfunction Inadequate LV and pump preload, low pump flow
Fixed Pulmonary hypertension Liming factor for LV and pump preload
Severe TR Worsening RV function post implant
ASD / PFO Progressive right to left shunt / hypoxia
More than mild AI LVAD inefficiency
LV apical thrombus Complicates inflow cannula placement
Ascending aortic aneurysm Complicates outflow cannula placement
“Smaller” LV (<6cm) Further decrease in size impacts RV mechanics
Impact of LVAD on RV Function
Beneficial Impact
• Reduction in LV filling
pressure alleviates
pulmonary congestion and
reduces secondary PHTN
with concurrent
improvement in RV forward
flow and reduction in
secondary TR.
Deleterious Effect
• Reduction of LV dimension
/ volume past a threshold
may shift the septum and
alter RV geometry
– Worsening TR
– Worsening RV mechanics
• Prone to adverse outcome if
significant PHTN
• Concept of the “Suction
Event” at high flows
What to Expect on Echo
• High RPMs – closed AV
• Lower RPMs - AV opens intermittently
• Usually phasic flow into apical cannula
– Magnitude of flow and velocity depends on degree of
LV “preload” and forward aortic flow
• Phasic flow into ascending aorta
• MV opens and closes
• For latest generation devices with pump at apex,
expect destructive interference with Doppler
Challenges of Evaluating LVADs
with Echocardiography
• Limited / challenging apical windows
– Parallel interrogation of inlet cannula
– Electronic artifact with devices that have pump
mechanism at apex
• Variable range of normal inlet / outlet flow
velocities
– Best to establish early baseline for comparison
– Velocities depend on pump speed and LV
preload contribution
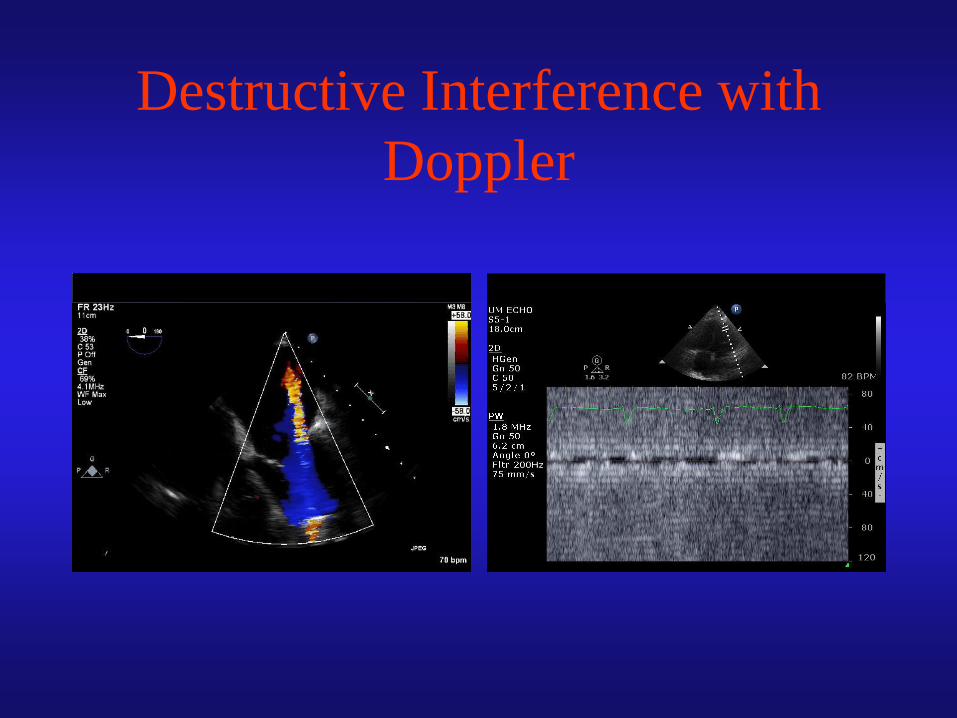
Destructive Interference with
Doppler
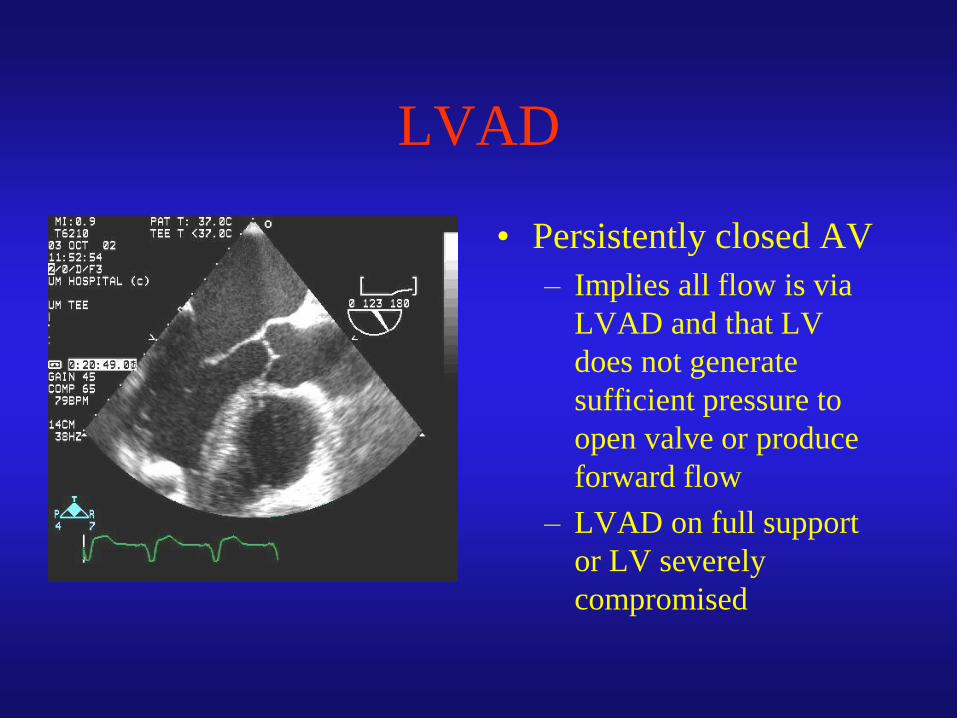
LVAD
• Persistently closed AV
– Implies all flow is via
LVAD and that LV
does not generate
sufficient pressure to
open valve or produce
forward flow
– LVAD on full support
or LV severely
compromised
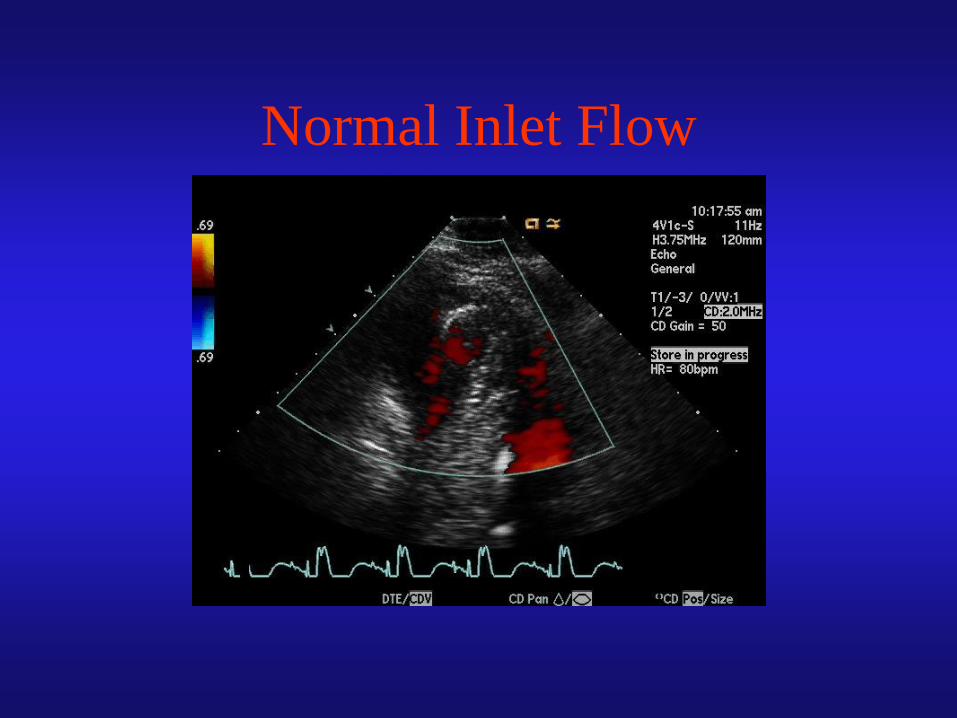
Normal Inlet Flow
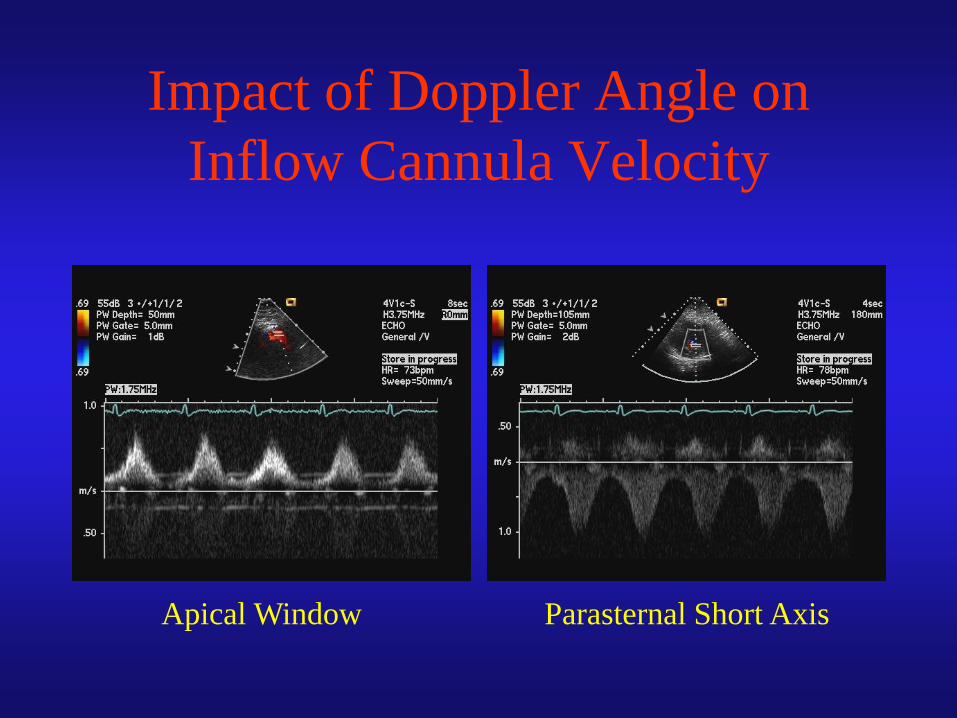
Impact of Doppler Angle on
Inflow Cannula Velocity
Apical Window Parasternal Short Axis
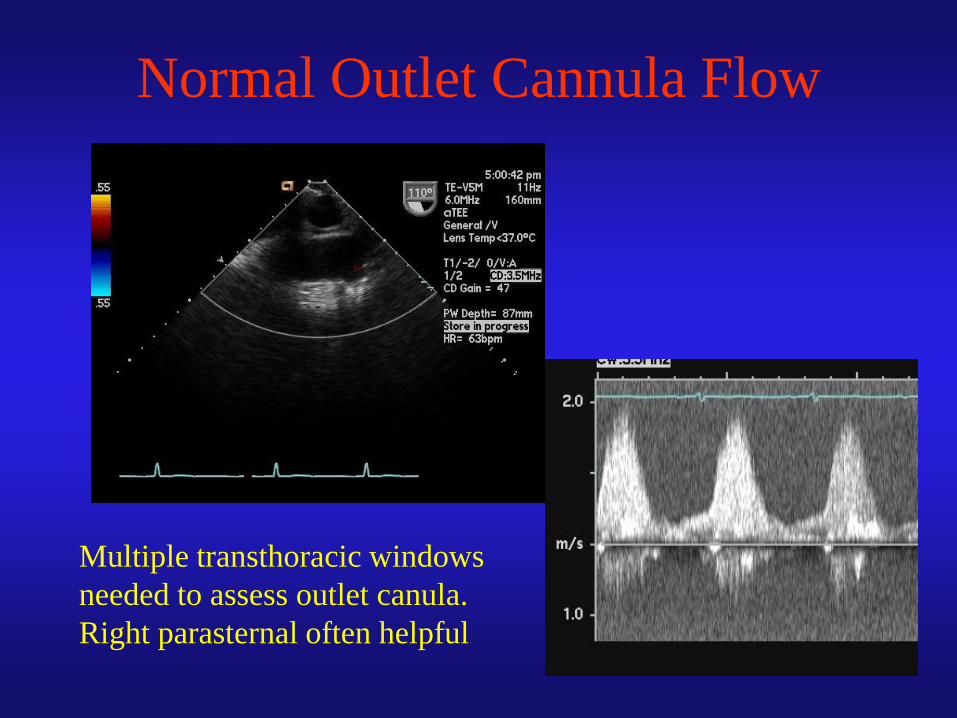
Normal Outlet Cannula Flow
Multiple transthoracic windows
needed to assess outlet canula.
Right parasternal often helpful
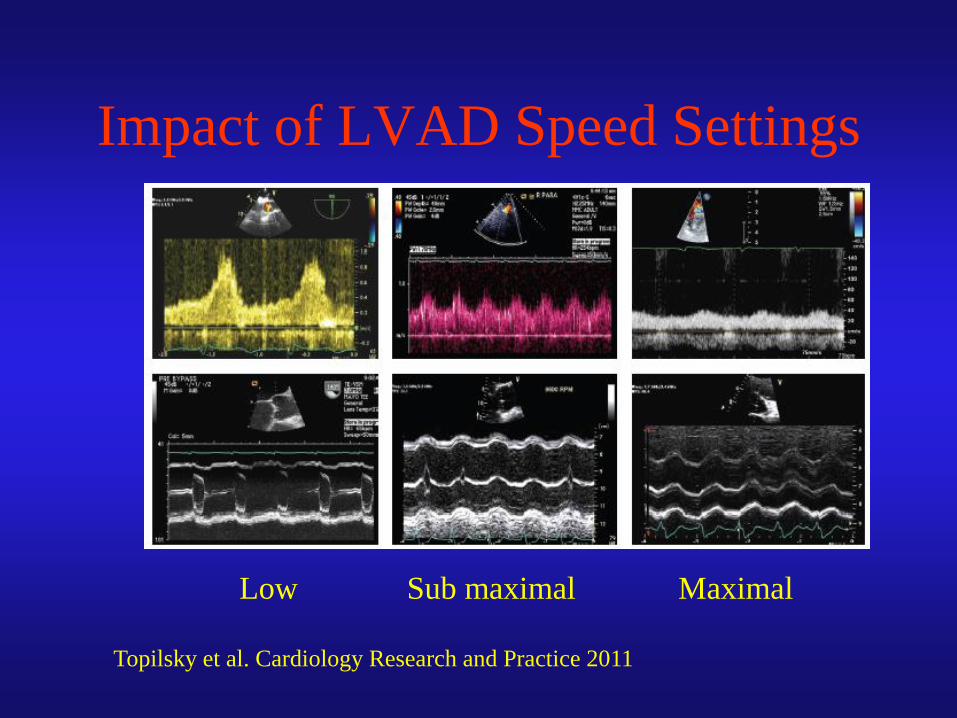
Impact of LVAD Speed Settings
Topilsky et al. Cardiology Research and Practice 2011
Low Sub maximal Maximal
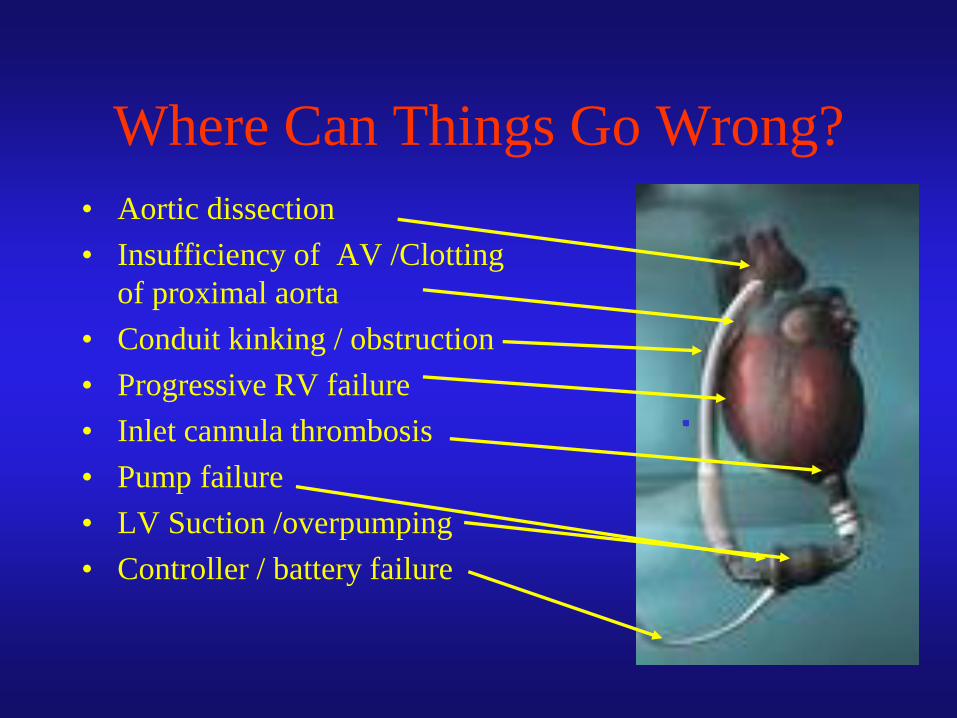
Where Can Things Go Wrong?
• Aortic dissection
• Insufficiency of AV /Clotting
of proximal aorta
• Conduit kinking / obstruction
• Progressive RV failure
• Inlet cannula thrombosis
• Pump failure
• LV Suction /overpumping
• Controller / battery failure
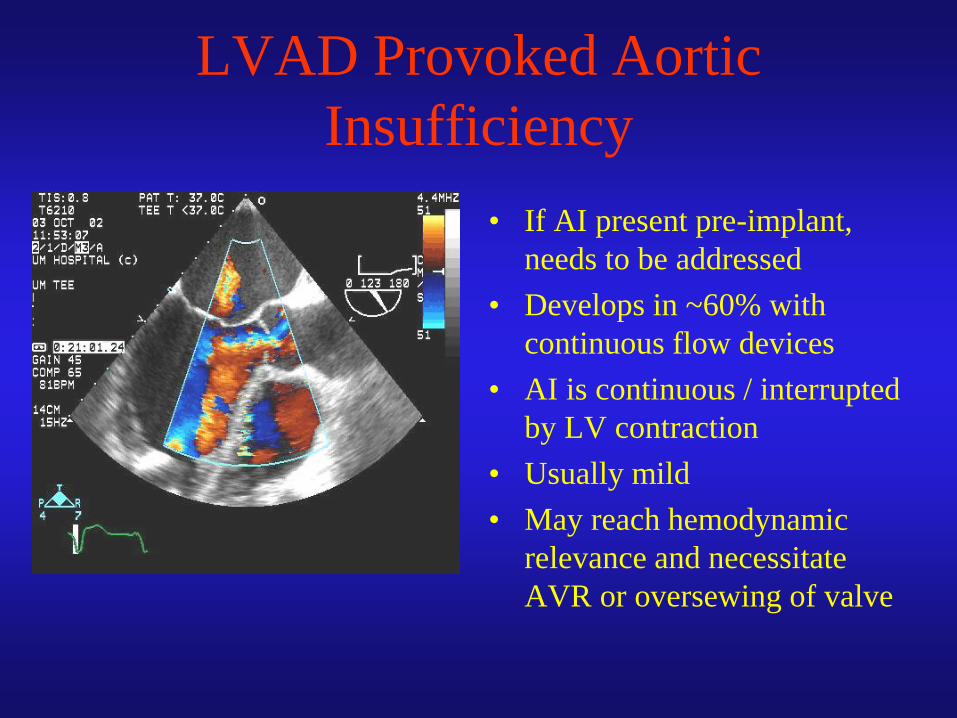
LVAD Provoked Aortic
Insufficiency
• If AI present pre-implant,
needs to be addressed
• Develops in ~60% with
continuous flow devices
• AI is continuous / interrupted
by LV contraction
• Usually mild
• May reach hemodynamic
relevance and necessitate
AVR or oversewing of valve
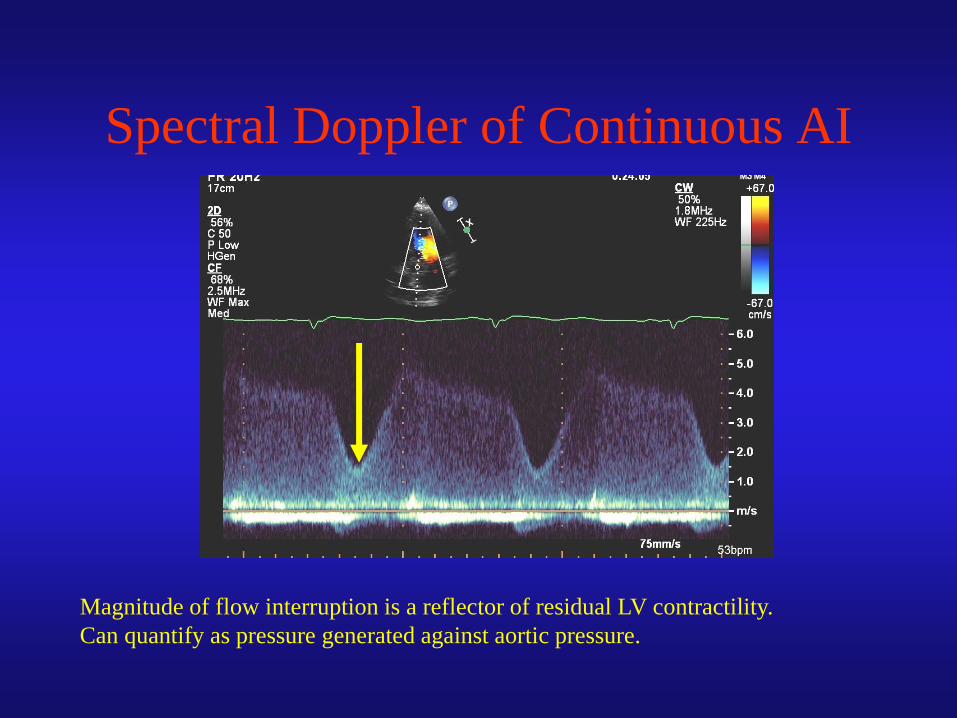
Spectral Doppler of Continuous AI
Magnitude of flow interruption is a reflector of residual LV contractility.
Can quantify as pressure generated against aortic pressure.
Development of AI in LVAD
Supported Patients
• 78 LVAD patients
– HeartMate XVE in 25
– HeartMate-II in 53
• Serial echocardiograms baseline,
1,3,6,12,18 & 24 months after implant
• AI graded none to severe
Cowger et al Circulation –HF, 2010
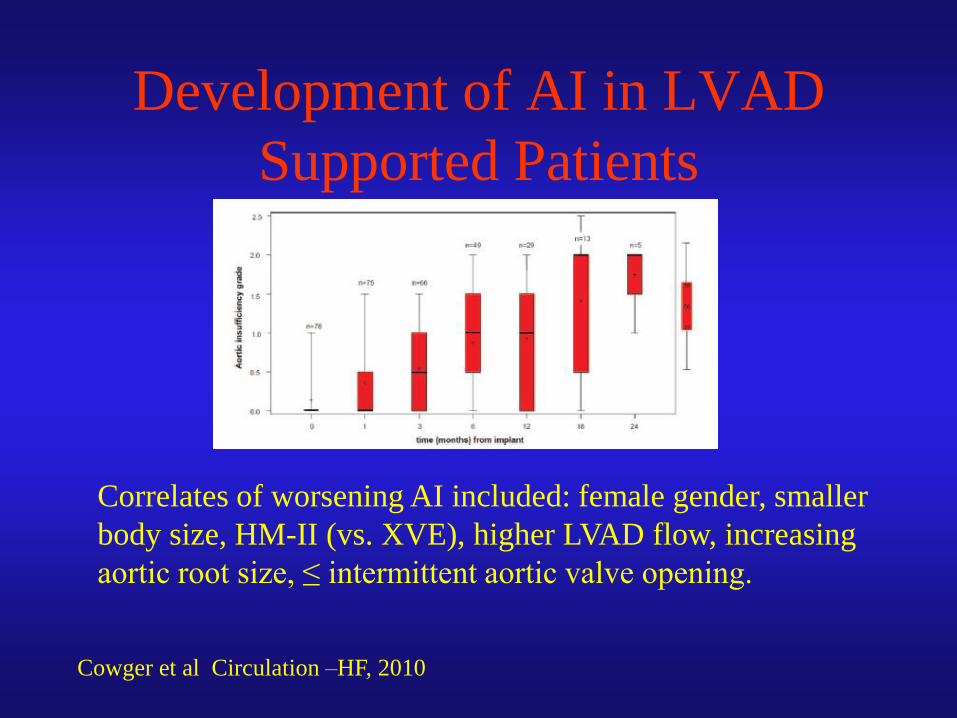
Development of AI in LVAD
Supported Patients
Cowger et al Circulation –HF, 2010
Correlates of worsening AI included: female gender, smaller
body size, HM-II (vs. XVE), higher LVAD flow, increasing
aortic root size, ≤ intermittent aortic valve opening.
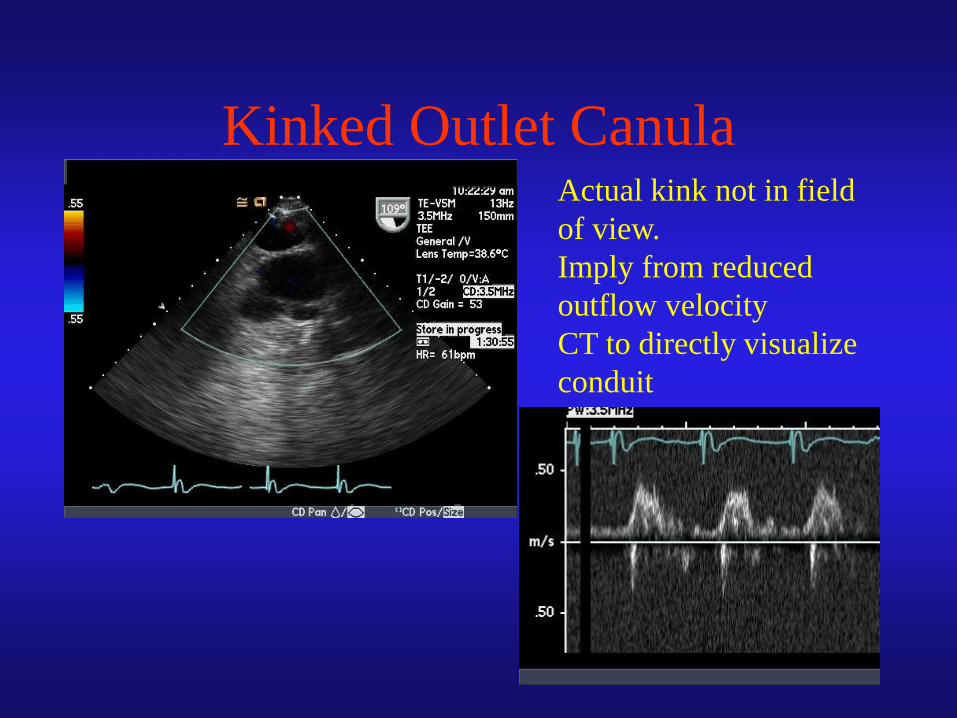
Kinked Outlet Canula Actual kink not in field
of view.
Imply from reduced
outflow velocity
CT to directly visualize
conduit
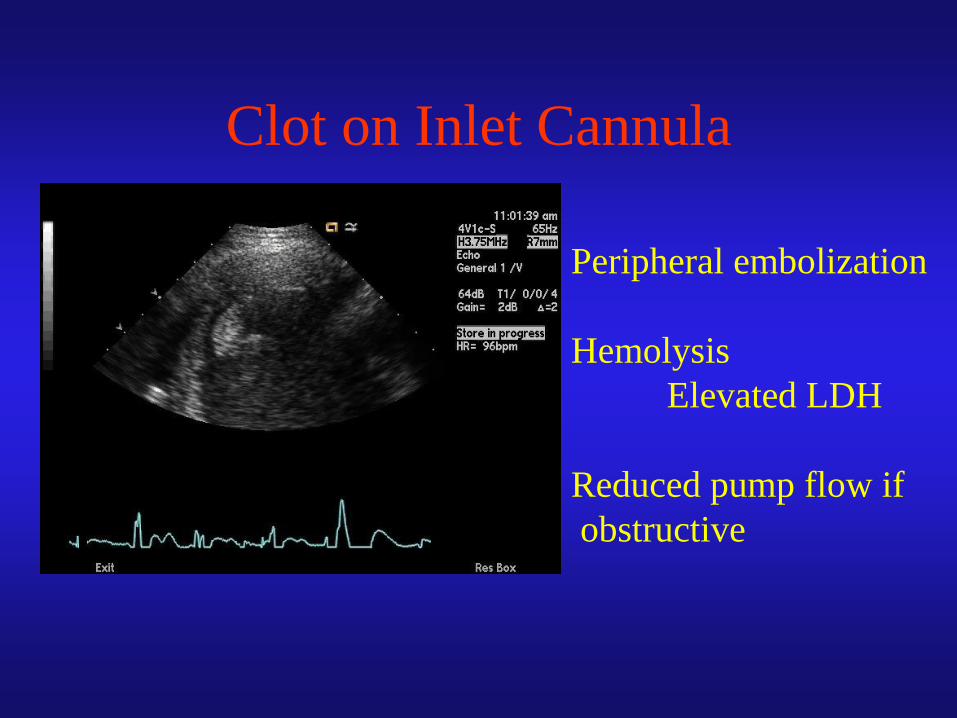
Clot on Inlet Cannula
Peripheral embolization
Hemolysis
Elevated LDH
Reduced pump flow if
obstructive
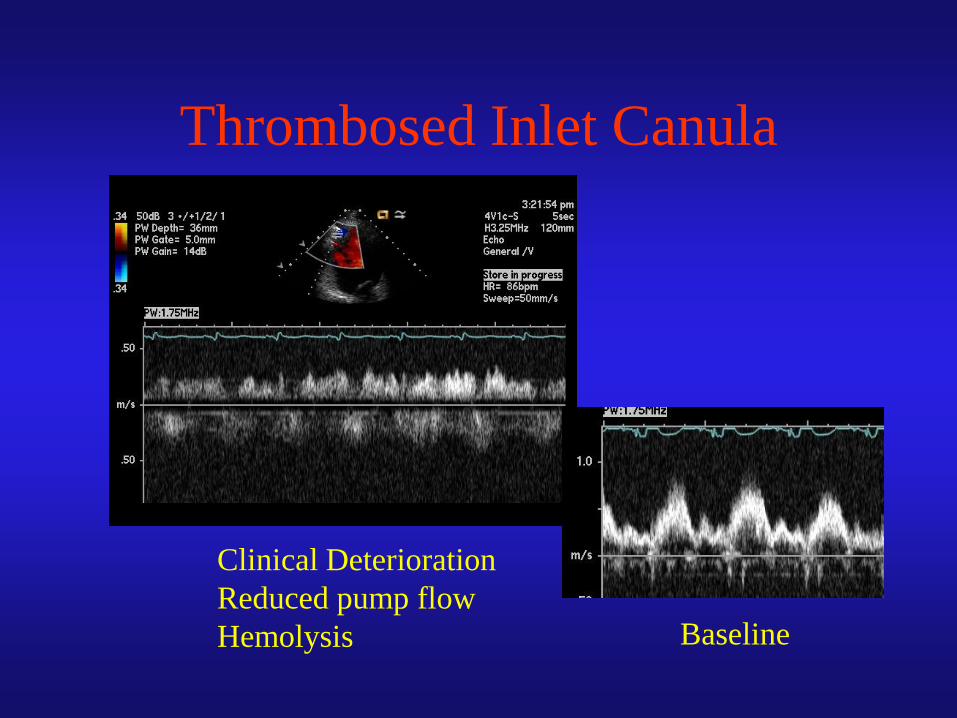
Thrombosed Inlet Canula
Baseline
Clinical Deterioration
Reduced pump flow
Hemolysis
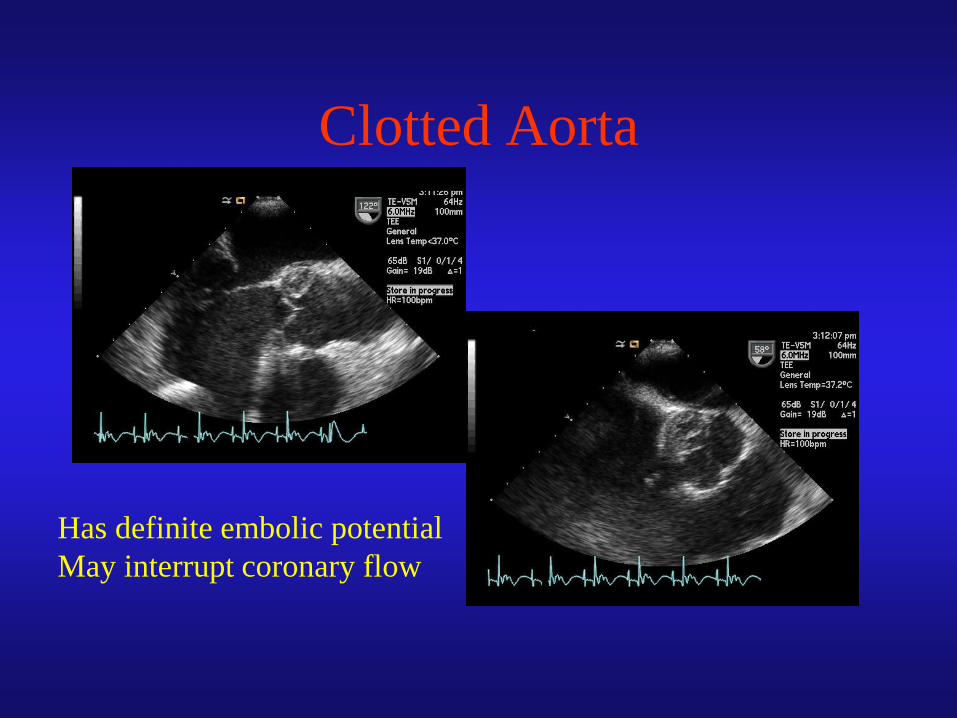
Clotted Aorta
Has definite embolic potential
May interrupt coronary flow

Class IV CHF
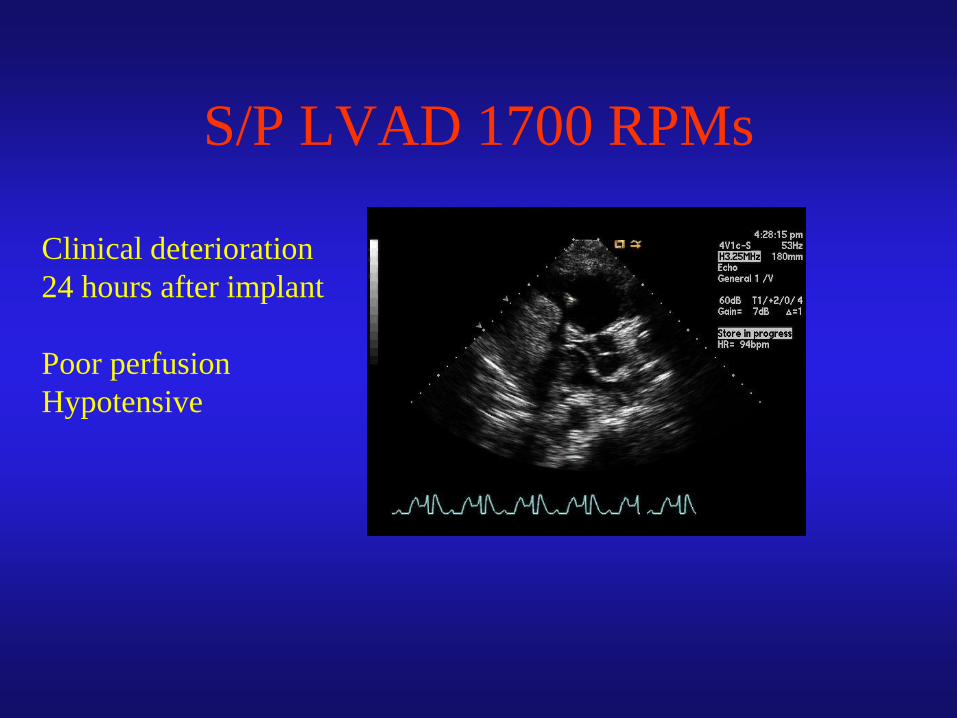
S/P LVAD 1700 RPMs
Clinical deterioration
24 hours after implant
Poor perfusion
Hypotensive

S/P LVAD 1700 RPMs
“Suction” Event
• Overly aggressive LVAD pumping
– Concurrent RV failure / PHTN
• LVAD empties the LV
– Septum shifts to the left, further worsening TR
and RV geometry / function
• Treatment: reduce LVAD flow rate
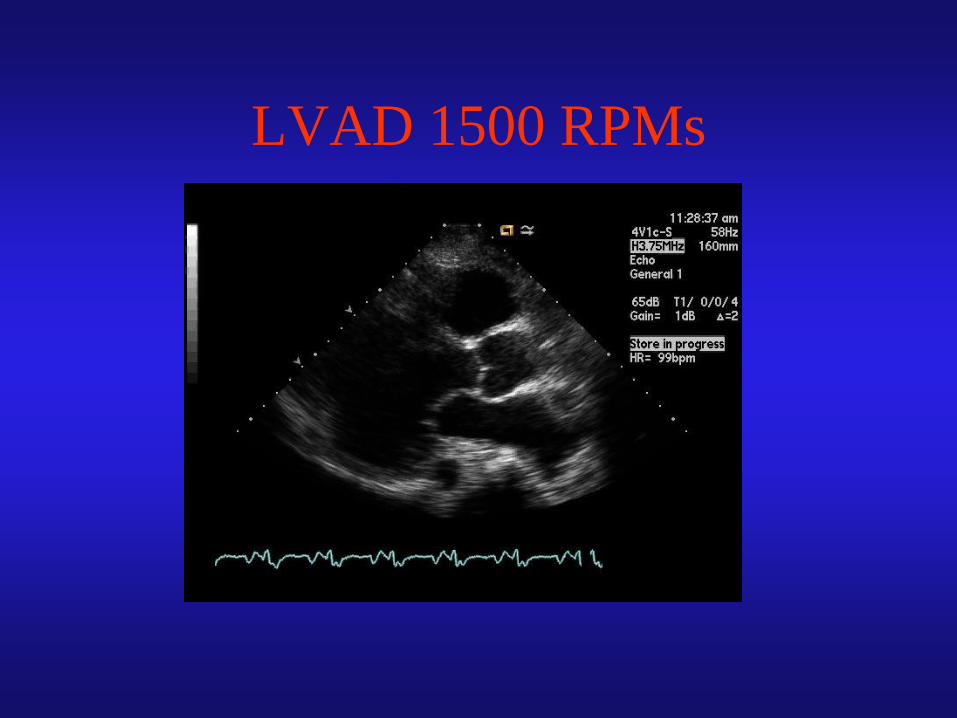
LVAD 1500 RPMs
Progressive RV Failure after
LVAD Placement
• Progressive RV failure in up to 35% post implant
– Doubles post-implant mortality
• Predicted by:
– Clinical evidence of RVF pre-implant
– “Smaller” pre-implant LV size (<63mm)
• Probably a set up for “suction event”
– Short duration TR
– RV strain
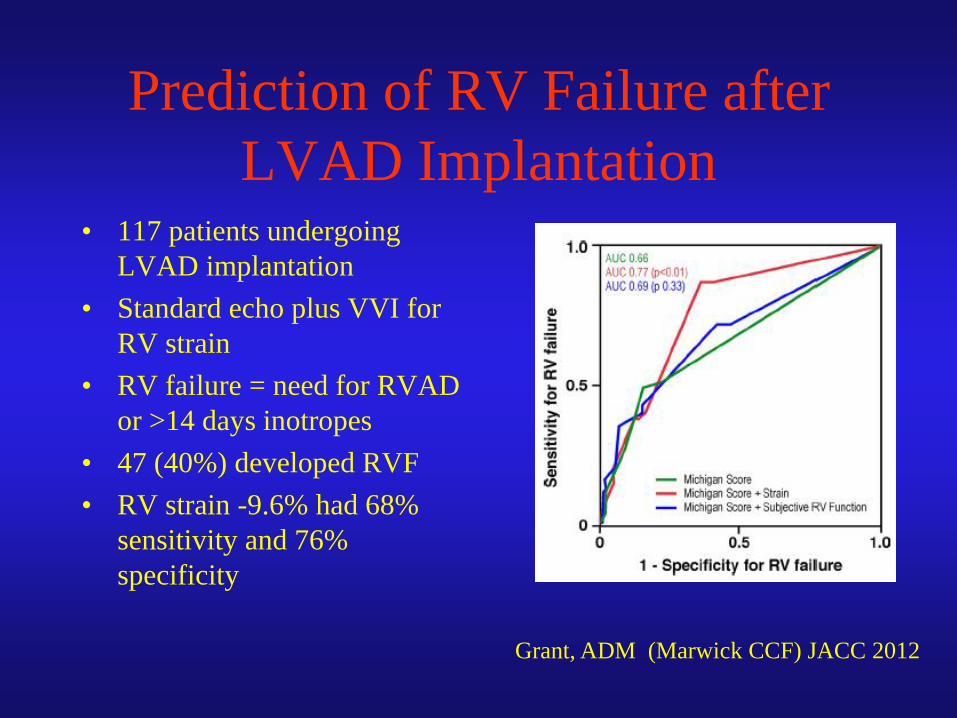
Prediction of RV Failure after
LVAD Implantation • 117 patients undergoing
LVAD implantation
• Standard echo plus VVI for
RV strain
• RV failure = need for RVAD
or >14 days inotropes
• 47 (40%) developed RVF
• RV strain -9.6% had 68%
sensitivity and 76%
specificity
Grant, ADM (Marwick CCF) JACC 2012
Conclusions: The Role of
Echocardiography in LVADs
• Determine suitability / need of patient for support
• Identify complicating factors for implant– RV function / TR / PHTN
– LV thrombus
– PFO
– Aortic Insufficiency
• Monitor function of LVAD– Impact on RV
– Development of AI
– Must integrate pump / flow settings with echo / Doppler findings
• Evaluate for possible LVAD withdrawl
