economic impact of beta blockade in heart failure
TRANSCRIPT

Economic Impact of Beta Blockade inHeart Failure
Douglas Gregory, PhD, James E. Udelson, MD, Marvin A. Konstam, MD
We reviewed the literature on clinical trials of b-ad-renergic blockade for treatment of heart failure,seeking evidence of reductions in hospital admis-sions. To analyze the economic implications of sixclinical trials, we developed a stochastic cost modelto generate estimates of total medical costs result-ing from heart failure and related causes. The modelincludes inpatient, outpatient, and professional costestimates based on Medicare claims data, and it isdriven by traditional endpoint statistics reported inthe clinical trial literature. It provides a commonframework for comparing cost effectiveness acrossclinical trials in the absence of detailed cost informa-tion collected in the trial.
The incremental expected cost per year of lifesaved is $3,300 for bisoprolol, $2,500 for metoprolol,and $6,700 for carvedilol. The cost per year of lifesaved for each compound is well below acceptedstandards for cost effectiveness.
These results are sensitive to the cost of drugtherapy and the relative mortality rate for the exper-imental group. For example, if the relative mortalityrate of the experimental group were to increase fromthe reported 40% to 82%, and if the annual cost ofthe drug were to decrease from $2,000 to $500, thenwe estimate that carvedilol would break even and thecost per year of life saved would drop to zero.Whether b-blocker therapy, as assumed, sustains itsdifferential effectiveness in terms of relative mortal-ity risk beyond the study duration has not beendemonstrated. Am J Med. 2001;110(7A):74S–80S.© 2001 by Excerpta Medica, Inc.
Heart failure poses a major and growing economicburden, particularly as the population ages.Hospitalization generates the majority of
health-care costs in patients with heart failure. Thus,strategies to reduce the frequency of hospitalization rep-resent a significant opportunity for cost savings.
Beyond its economic impact, hospitalization serves asa marker of heart failure disease activity and/or severity,and contributes to diminished health-related quality oflife. Thus, any intervention that reduces the frequency ofhospital admissions, without adversely affecting survival,may be viewed as improving clinical outcomes and con-tributing to quality of life. Any concomitant reduction inmortality strengthens the assessment of cost effective-ness, which may be graded by an analysis of cost per ad-ditional year of life prolonged.
Recent clinical trials have documented the usefulnessof b blockers in the management of patients with heartfailure and demonstrated the beneficial effect of b block-ade on recurrent hospitalization.1– 6 Moreover, bisopro-lol, carvedilol, and metoprolol have all been shown toprolong survival in patients with heart failure.1,5,6
This analysis compares the results of six recent clinicaltrials of b blockade in terms of their medical and eco-nomic impacts on patients with heart failure. A stochasticcost model is used to derive the medical cost implicationsfrom published data, including inpatient, outpatient, andprofessional cost estimates based on Medicare claimsdata. The model, driven by traditional endpoint statisticsreported in the clinical trial literature, provides a com-mon framework for comparing cost effectiveness acrossclinical trials in the absence of detailed cost information.
METHODS
Literature ReviewThe study objective was to determine the economic effectof b-adrenergic blockade therapy based on publishedclinical trial findings. We reviewed the literature on clin-ical trials of b blockade for evidence of reductions in hos-pital admissions, the key driver of health-care costs. Un-der review were the US and Australian/New ZealandCarvedilol Trials, the Cardiac Insufficiency BisoprololStudies (CIBIS I and II), and the Metoprolol in DilatedCardiomyopathy (MDC) and MERIT-HF Trials.1– 6
Most trials included morbidity, measured by time to hos-pitalization or death, as a primary or secondary endpoint.The total number of patients surviving without a hospi-
From the Department of Medicine, Tufts University and New EnglandMedical Center, Boston, Massachusetts, USA.
Requests for reprints should be addressed to Marvin A. Konstam,MD, Box 108, New England Medical Center, 750 Washington Street,Boston, Massachusetts 02111.
74S © 2001 by Excerpta Medica, Inc. 0002-9343/01/$20.00All rights reserved. PII S0002-9343(98)00387-8

talization was reported for control and experimentalgroups for the time observed during the study. The typi-cal statistical formulation entailed fitting a Kaplan-Meiercurve to censored data on time to hospitalization ordeath.7
The endpoint featured below is event-free survival atthe termination of the study, defined as survival withoutthe occurrence of at least one hospitalization. Some au-thors report the probability of hospitalization or deathfor the study duration, which is simply one minus theprobability of event-free survival. Taking Society’s pointof view, we focused on estimating differences in totalmedical costs between the placebo and experimentalgroups based on these reported probabilities.8
Survival ModelLifetime survival distributions were derived from thepublished Kaplan-Meier survival curves for the respec-tive clinical trial analyzed. Hazard rates (ie, actuarialdeath rates) were estimated from gender stratifiedWeibull Distributions fit to Framingham Heart Study(FHS) data on heart failure patients.9 –11 The survival dis-tributions for the placebo group were extrapolated be-yond the clinical trial durations by successively applyingthe FHS Weibull hazard rates to prior year survival prob-abilities to estimate subsequent years of life until therewas approximately zero survival probability. The Weibullhazard rate for the experimental group was derived fromthe hazard rate of the placebo group by using the relativemortality risk parameter estimated in the clinical trial.This assumes that the relative proportional mortality riskfor the experimental group will persist through patients’remaining lifetimes. Life expectancies were calculated bysumming the respective survival curves for experimentaland placebo groups over patients’ remaining lifetimes.
Recurrent Hospitalization ModelIn estimating total health-care costs for heart failure pa-tients, it is critically important to model the recurrenthospitalization process over time. Unfortunately, theb-blocker studies did not publish detailed data on recur-rent hospitalizations and attendant costs. Consequently,we derived a model of recurrent hospitalizations overtime from the literature based on a well-known stochasticrenewal process.
We assume an exponential probability distribution forthe time between subsequent hospitalizations. This dis-tribution has been widely used in modeling mortality andsurvival rates and associated life expectancy.12 The expo-nential distribution is sometimes referred to as the“memoryless” distribution, because the time to hospital-ization or death (given that hospitalization has alreadyoccurred) also follows the exponential distribution and isindependent of the number of prior hospitalizations.13
This property permits us to derive the probability distri-bution for recurrent hospitalizations over time from
published data on the probability of event-free survivalfor the study period. Assumption of an exponential inter-hospitalization time distribution implies a Poisson Pro-cess model for recurrent hospitalizations.13 The PoissonProcess probability model is as follows:
Pr{N(t) 5 n} 5 [lt]n exp[2lt]/n!,Pr{A} 5 the probability of the event, A, in brackets,N(t) 5 the number of hospitalizations
occurring in the interval [0,t],l 5 the hospitalization rate.
Medical CostsTo model medical costs, we analyzed the claims costs ofpatients with a hospitalization for congestive heart failure(CHF) from a 5% sample of Medicare patients in Massa-chusetts in 1995. Claims costs were separated into twocategories: 1) inpatient hospital, and 2) outpatient facilityand professional claims. Hospital inpatient costs werebased on the Health Care Financing Administration’s(HCFA) Prospective Payment System.14 Outpatient andprofessional costs were based on HCFA’s Resource BasedRelative Value Scale.14 Inpatient costs were accumulatedon a per-admission basis, because the clinical trials underreview did not include data on length of stay. Moreover,no published data to date have conclusively demon-strated that lengths of stay differ significantly because ofb-blocker therapy for heart failure patients.
Because the differential costs of b blockers are the fo-cus of this analysis, we estimated the annual costs ofcarvedilol, metoprolol, and bisoprolol based on opti-mum dosage rates cited in the clinical trials and theiraverage wholesale prices for 1998.15 The costs of homecare or long-term care were excluded, and all costs wereinflated to 1998 levels using the medical component ofthe Consumer Price Index.16 Because the reimbursementmethodologies approximate fully allocated costs, our fo-cus is on long-run marginal costs in which all inputs arevariable.17 All costs and survival rates were discounted tothe present using a discount rate of 5%.8,18,19
Cost ModelWe estimated the relationship between the number ofrecurrent hospitalizations and total health-care costs, us-ing the Medicare claims data for Massachusetts. Linearregression analysis was used to estimate the relationshipbetween the number of admissions and hospitalizationcosts (R2 5 .67, P,0.001) and outpatient/professionalcosts (R2 5 .2, P,0.01), respectively.
We combined the derived probability distributions forhospitalizations, the estimated cost functions, and the de-rived survival distributions to produce estimates of theexpected lifetime costs for placebo and experimentalgroups. Finally, we analyzed the cost per year of life savedby dividing the incremental expected cost of the experi-mental versus the placebo group by the incremental life
A Symposium: Economic Impact of Beta Blockade in Heart Failure/Gregory et al
May 7, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (7A) 75S

expectancy. We performed sensitivity analysis on allmodel parameters.
RESULTS
Clinical TrialsThe key findings of the studies analyzed with respect tohospitalization are summarized in Table 1. The averageage of patients enrolled in the clinical trials is relativelyyoung in light of the high prevalence rates of heart failureamong the elderly.11 Thus, the average clinical acuity ofthe study populations may not mirror the general popu-lation of heart failure patients, and direct extrapolation ofthe results may be inappropriate.
Hospital admissions may be caused by cardiovasculardisease, cardiac decompensation, heart failure or ar-rhythmias, or all causes. Variation in reported hospital-ization risk reflects the inclusiveness of the causes for hos-pitalization, differences in study duration, and differ-ences in underlying study populations.
The US Carvedilol Trial1 reported a mean 6.5-monthrisk of hospitalization for cardiovascular disease of 20%for the placebo group and 14% for the experimentalgroup. The relative risk of hospitalization with carvedilolwas .7 and the relative mortality risk was .4. The 19-month Australian/New Zealand Carvedilol Trial3 re-ported the highest risks of hospitalization, 58% and 48%for placebo and experimental groups, respectively. All-cause hospitalization was the defined endpoint, and therelative risk of hospitalization was .72 with carvedilol veryclose to the value reported in the US Carvedilol Trial.
The CIBIS-I2 Bisoprolol Trial reported 23-month hos-pitalization risks of 28% and 19% for placebo and exper-imental groups, and the MDC Metoprolol Trial4 reported28% and 20% hospitalization risks for 12 months. TheCIBIS-II5 and MERIT-HF6 Trials demonstrated thatbisoprolol and metoprolol (CR/XL) are both effectivewith relative mortality risks of .66 and .64, respectively.
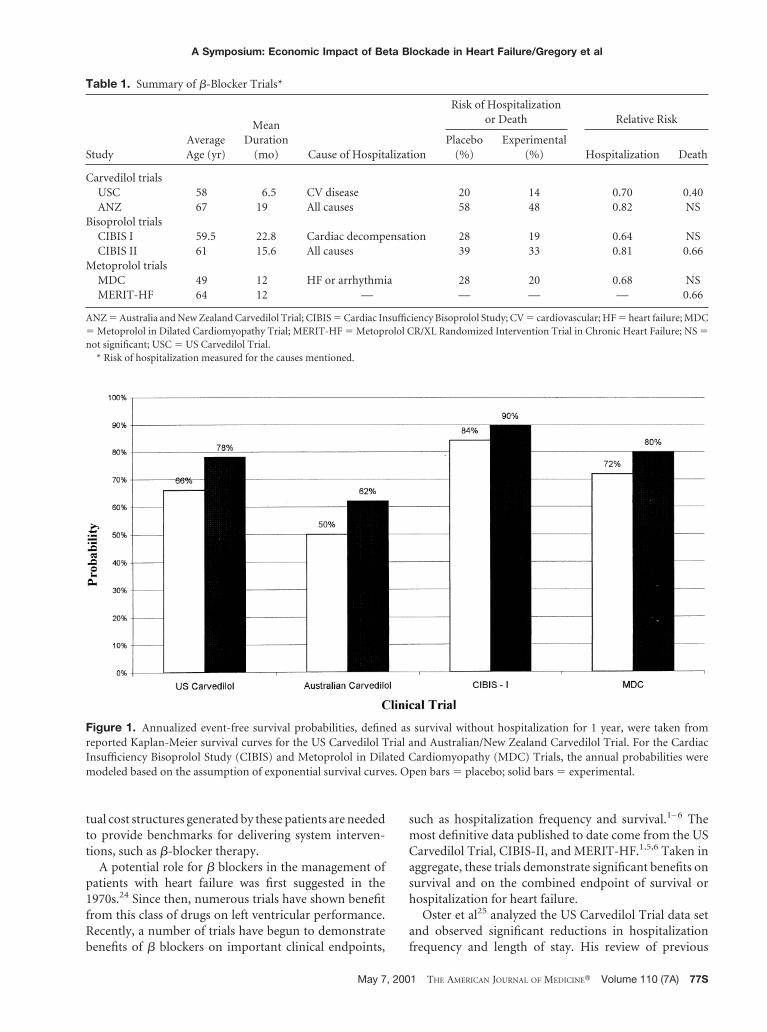
For comparison purposes, we computed 1-year event-free survival probabilities for placebo and experimentalgroups for each trial. Event-free survival is defined as sur-vival without hospitalization. Figure 1 presents the re-sults. The lowest annual event-free survival probabilityfor the baseline placebo population was in the Australian/New Zealand Carvedilol Trial (50%), which is attribut-able to the inclusion of hospitalizations for all causes.
Expected Lifetime Costs of b-Blocker TherapyTable 2 summarizes the economic analysis for the threecompounds. The incremental expected cost associatedwith b-blocker therapy varies from 2$2,603 in the case ofmetoprolol to $15,656 for carvedilol. The higher expectedcost of carvedilol is driven by the cost of the drug and thevery high “survival effect” reported in the 6.5-month USCarvedilol Trial.
Cost Per Year of Life SavedCombining the differential life expectancies with the in-cremental costs produces the estimates of incrementalcost effectiveness presented in Table 2. Differential lifeexpectancies for the compounds were estimated to be1.04, 1.06, and 2.4 years for bisoprolol, metoprolol, andcarvedilol, respectively. The incremented costs per year oflife saved are estimated to be $3,336, $2,472, and $6,740for bisoprolol, metoprolol, and carvedilol, respectively.
Sensitivity AnalysisBecause of the short duration and very low relative mor-tality rate reported in the US Carvedilol Trial, we con-ducted a sensitivity analysis of the cost of carvedilol tochanges in the relative mortality rate and drug cost. Fig-ure 2 presents the graphs of expected cost of the experi-mental and placebo groups based on data from the USCarvedilol Trial. As the relative mortality rate decreases,the contribution of experimental group survivors to fu-ture expected costs increases. This “survival effect” is off-set by the “hospitalization effect” of b blockers, whichreduces future expected costs resulting from hospitaliza-tion. Reductions in drug costs, of course, lower the ex-pected cost for the experimental group. At an annual costof $500 and relative mortality risk of .82, carvedilol breakseven—that is, the incremental expected cost of the ther-apy is zero and the cost per year of life saved is zero. Thecompound is said to dominate standard therapy at thispoint, because it costs no more than standard therapy andincreases life expectancy.
DISCUSSION
More than 4 million US citizens carry a diagnosis of heartfailure. Approximately 400,000 new cases are diagnosedeach year, more than 200,000 deaths are associated withheart failure annually, and approximately 1 million an-nual hospitalizations are related to this diagnosis.10,20 –22
The annual costs of caring for patients with this diseasehave been estimated at $10 billion to $40 billion, withapproximately 75% of these costs related to hospitaliza-tion.20 –22 Both incidence and prevalence of heart failureincrease with age, and heart failure is the most commonand costly diagnosis at hospitalization in the Medicarepopulation.23 Approximately 50% of patients with heartfailure are over age 65.11 By the year 2030, it is projectedthat the elderly (over 65 years of age) will constitutenearly 65% of the total heart failure population. Amongpeople over the age of 80, approximately 10% will haveheart failure. The prevalence of heart failure and its asso-ciated costs will increase dramatically over the next de-cade as the population ages.
These concerns raise the priority of identifying inter-ventions that will reduce overall cost or, at least, offercost-effective approaches to improving outcomes for pa-tients with heart failure. More detailed models of the ac-
A Symposium: Economic Impact of Beta Blockade in Heart Failure/Gregory et al
76S May 7, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (7A)
tual cost structures generated by these patients are neededto provide benchmarks for delivering system interven-tions, such as b-blocker therapy.
A potential role for b blockers in the management ofpatients with heart failure was first suggested in the1970s.24 Since then, numerous trials have shown benefitfrom this class of drugs on left ventricular performance.Recently, a number of trials have begun to demonstratebenefits of b blockers on important clinical endpoints,
such as hospitalization frequency and survival.1– 6 Themost definitive data published to date come from the USCarvedilol Trial, CIBIS-II, and MERIT-HF.1,5,6 Taken inaggregate, these trials demonstrate significant benefits onsurvival and on the combined endpoint of survival orhospitalization for heart failure.
Oster et al25 analyzed the US Carvedilol Trial data setand observed significant reductions in hospitalizationfrequency and length of stay. His review of previous
Figure 1. Annualized event-free survival probabilities, defined as survival without hospitalization for 1 year, were taken fromreported Kaplan-Meier survival curves for the US Carvedilol Trial and Australian/New Zealand Carvedilol Trial. For the CardiacInsufficiency Bisoprolol Study (CIBIS) and Metoprolol in Dilated Cardiomyopathy (MDC) Trials, the annual probabilities weremodeled based on the assumption of exponential survival curves. Open bars 5 placebo; solid bars 5 experimental.
Table 1. Summary of b-Blocker Trials*
StudyAverageAge (yr)
MeanDuration
(mo) Cause of Hospitalization
Risk of Hospitalizationor Death Relative Risk
Placebo(%)
Experimental(%) Hospitalization Death
Carvedilol trialsUSC 58 6.5 CV disease 20 14 0.70 0.40ANZ 67 19 All causes 58 48 0.82 NS
Bisoprolol trialsCIBIS I 59.5 22.8 Cardiac decompensation 28 19 0.64 NSCIBIS II 61 15.6 All causes 39 33 0.81 0.66
Metoprolol trialsMDC 49 12 HF or arrhythmia 28 20 0.68 NSMERIT-HF 64 12 — — — — 0.66
ANZ 5 Australia and New Zealand Carvedilol Trial; CIBIS 5 Cardiac Insufficiency Bisoprolol Study; CV 5 cardiovascular; HF 5 heart failure; MDC5 Metoprolol in Dilated Cardiomyopathy Trial; MERIT-HF 5 Metoprolol CR/XL Randomized Intervention Trial in Chronic Heart Failure; NS 5not significant; USC 5 US Carvedilol Trial.
* Risk of hospitalization measured for the causes mentioned.
A Symposium: Economic Impact of Beta Blockade in Heart Failure/Gregory et al
May 7, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (7A) 77S

b-blocker trials consistently concluded that b blockersreduce hospitalization frequency in patients with heartfailure. Meta-analyses of published trials of b blockers inpatients with heart failure have demonstrated an overallbenefit on survival,26 although these findings have beenprimarily driven by the carvedilol data. Recently com-pleted clinical trials of bisoprolol and metoprolol (CR/XL) have demonstrated the beneficial survival effect ofthese compounds.5,6
We analyzed the effect of three b blockers on survivalfrom the perspective of cost effectiveness, expressed ascost per year of life prolonged for patients with heart fail-
ure and New York Heart Association (NYHA) class II orIII symptoms. The analysis presented in this article isbased on six trials that compared b blockers to placebo;thus, both costs and effectiveness (in extending life ex-pectancy) of b blockade are compared with not using bblockers in similar patients. We cannot assess the relativecost effectiveness of b-blocker therapy compared withangiotensin-converting enzyme (ACE) inhibition ordigoxin, because the vast majority of patients in thesetrials (in both the b-blockade and the placebo groups)were treated with ACE inhibitors and digoxin, reflectingcontemporary clinical trial practice. Therefore, cost effec-
Figure 2. Sensitivity analysis of the expected cost per patient in experimental and placebo groups for various levels of the relativemortality risk and annual drug therapy cost.
Table 2. b-Blocker Cost-effectiveness Measures*
Parameter
Measure†
Carvedilol Metoprolol Bisoprolol
Annual drug cost $ 2,000 $ 612 $ 379Total expected cost
Placebo $14,901 $13,312 $15,048Experimental $30,557 $15,926 $18,503Incremental cost $15,656 $ 2,613 $ 3,455
Incremental life expectancy (yr) 2.4 1.06 1.04Incremental cost per YOLS $ 6,740 $ 2,472 $ 3,336
YOLS 5 years of life saved.* Annual expected costs discounted at a rate of 5%. All costs expressed in 1998 dollars.† Cost model parameters for carvedilol and bisoprolol based, respectively, on data published in the US Carvedilol Trial1 and the CIBIS-II Trial.5
Cost model parameters for metoprolol based on mortality data from the MERIT-HF Trial and hospitalization data from the MDC Trial.4,6
A Symposium: Economic Impact of Beta Blockade in Heart Failure/Gregory et al
78S May 7, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (7A)

tiveness of b blockade presented here is relative to stan-dard heart failure therapy, as reflected by the backgroundtherapy in the placebo groups of these trials.
Our estimate of the economic costs of heart failurewith and without b-blocker therapy deals with directmedical costs only. Inclusion of indirect economic costsin the analysis (eg, costs attributable to caregivers, sup-port groups, transportation, lost income) would likelyhave driven our findings toward even more favorableconclusions regarding the economic impact of b block-ers.
Our analysis estimates added costs per year of life savedof approximately $2,000 to $7,000 for the study popula-tions analyzed. Because the cost per year of life saved isquite low, the drugs would be judged to be cost effectiveby most analysts.
These findings have important implications with re-spect to managed care. A number of clinical practiceguidelines have been developed in an attempt to definestandard practice in the management of heart failure.15,27
Although such guidelines have proven useful, there areinherent difficulties in their application by payers andcapitated providers who seek mechanisms for translatingnewly reported therapeutic advances into cost-effectiveclinical practice. Such guidelines have seldom incorpo-rated issues of cost into their conclusions. This analysisrepresents a prototype for translating demonstrated ef-fects of a treatment on hospitalization frequency and onsurvival into the impact on overall health-care costs.
The disease management implications of this analysisassume particular interest, because health maintenanceorganizations emphasize contracting for disease manage-ment services on the basis of risk. Providers and diseasemanagement vendors are increasingly expected to as-sume partial or complete risk for a panel of patients withthe disease in question, such as heart failure. Moreover,heart failure is a primary focus of disease managementprograms because of its documented high rate of hospi-talization. There is very little literature profiling health-care costs resulting from heart failure. Consequently,models useful in predicting the actuarial health-care costsof patients with heart failure are of increasing importanceto health plans, providers, disease management vendors,and payers.
In conclusion, based on results of recently publishedlarge-scale clinical trials, b-blocker treatment may be ex-pected to achieve increases in life expectancy at minimalcost, when prescribed for patients with reduced left ven-tricular ejection fraction and NYHA class II or III heartfailure symptoms. Based on the trials reviewed here, allthree compounds appear to be cost effective because ofthe low cost of prolonging life in this patient population.
Limitations in this analysis include reliance on theMedicare database for Massachusetts’ claims, the relativeyouth of the clinical trial populations, and the fact that
cost effectiveness results were modeled. We did not at-tempt to model the impact of b blockade on hospitalresource consumption, because there was no evidencepresented in the trials of this effect. In addition, becauseof lack of data we did not attempt to explicitly model thedisease process after administration of b-blockade ther-apy, which could result in increased cost resulting fromtemporary increases in hospitalization after administra-tion of the b blocker. Despite our estimates of improve-ment in annual medical costs attributable to reduction inhospitalization, it may be that the clinical situation andconcomitant medical costs initially deteriorate after ini-tiation of the drug and during titration to optimum doselevels. Finally, we did not include data from the b-BlockerEvaluation of Survival Trial (BEST), because the finaldata have not yet been published in peer-reviewed publi-cations. Thus, we cannot extract the “official data” for usefor the analysis presented here.
Analysis of results of ongoing clinical trials will deter-mine whether these findings and projections are sus-tained by direct measurement of costs and benefits inother study populations. The benefits of b blockers havebeen most clearly demonstrated in patients with NYHAclasses II and III heart failure, in whom the potential forprovoking an exacerbation is less likely than for patientswith class IV symptoms. Once a large data set of patientswith NYHA class IV heart failure is accumulated, thisanalysis should be revisited.
REFERENCES1. Packer M, Bristow MR, Cohn JN, et al. The US Carvedilol
Heart Failure Study Group. The effect of carvedilol on mor-bidity and mortality in patients with chronic heart failure.N Engl J Med . 1996;334:1349–1355.
2. CIBIS Investigators and Committees. A randomized trial ofb-blockade in heart failure: the cardiac insufficiency biso-prolol Study (CIBIS). Circulation. 1994;90:1765–1773.
3. Australia/New Zealand Heart Failure Research Collabora-tive Group. Randomized, placebo-controlled trial of carve-dilol in patients with congestive heart failure due to isch-aemic heart disease. Lancet. 1997;349:375–380.
4. Waagstein F, Bristow MR, Swedberg K, Camerini F, et al.The Metoprolol in Dilated Cardiomyopathy (MDC) TrialStudy Group. Beneficial effects of metoprolol in idiopathicdilated cardiomyopathy. Lancet. 1993;342:1441–1446.
5. CIBIS-II Investigators and Committees. The cardiac insuf-ficiency bisoprolol study II (CIBIS-II): a randomized trial.Lancet. 1999;353:9–13.
6. MERIT-HF Study Group. Effect of metoprolol CR/XL inchronic heart failure: metoprolol CR/XL randomized inter-vention trial in chronic heart failure (MERIT-HF). Lancet.1999;353:2001–2007.
7. Lee ET. Statistical Methods for Survival Data Analysis. NewYork: John Wiley & Sons, 1992.
8. Drummond MF, O’Brien B, Stoddart GL, Torrance DW.Methods for the Economic Evaluation of Health Care Pro-grammes. New York: Oxford University Press, 1996.
9. Massie BM, Conway M. Survival of patients with congestiveheart failure: past, present, and future prospects. Circula-tion. 1987;75 (suppl IV):11–19.
A Symposium: Economic Impact of Beta Blockade in Heart Failure/Gregory et al
May 7, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (7A) 79S
10. Massie BM, Shah NB. Evolving trends in the epidemiolog-ical factors of heart failure: rationale for preventive strate-gies and comprehensive disease management. Am Heart J.1997;133:703–712.
11. Kannell WB, Belanger AJ. Epidemiology of heart failure. AmHeart J. 1991;121:951–957.
12. Beck JR, Kassirer JP, Pauker SG. A convenient approxi-mation of life expectancy (the “DEALE”). Am J Med. 1982;73:883–897.
13. Sheldon SM. Introduction to Probability Models. New York:Academic Press, 1997.
14. Medicare Payment Advisory Commission. Report to theCongress: Medicare Payment Policy. Volume II: AnalyticalPapers, 1998.
15. Drug Topics Red Book Prices. Montvale, NJ: Medical Eco-nomics, 1998.
16. Consumer Price Index. US Department of Labor, Bureau ofLabor Statistics, 1998.
17. Phelps CE. Health Economics. New York: Harper-Collins,1992.
18. Gold MR, Siegel JE, Russell LB, Weinstein MC. Cost Effec-tiveness in Health and Medicine. New York: Oxford Univer-sity Press, 1996.
19. Sloan FA. Value in Health Services. New York: Oxford Uni-versity Press, 1996.
20. Konstam MA, Dracup K, Baker D, et al. Heart Failure:
Evaluation and Care of Patients With Left Ventricular Sys-tolic Dysfunction. US Department of Health and HumanServices, Agency for Health Care Policy and Research,1994.
21. American Heart Association. 1998 Heart and Stroke Statis-tical Update, 1997.
22. US Department of Health and Human Services. Morbidityand Mortality Chartbook on Cardiovascular, Lung andBlood Diseases. National Institutes of Health, NationalHeart, Lung, and Blood Institute, 1990 and 1994.
23. O’Connell JB, Bristow MR. Economic impact of heart fail-ure in the United States: time for a different approach.J Heart Lung Transplant. 1993;13:S107–S112.
24. Waagstein F, Hjalmarson A, Varnauskas E, Wallentin I. Ef-fect of chronic beta-adrenergic receptor blockade in con-gestive cardiomyopathy. Br Heart J. 1975;37:1022–1036.
25. Oster G, Menzin J, Richner RE, et al. Impact of carvediloltherapy for heart failure on costs of cardiovascular-relatedhospitalization. J Am Coll Cardiol. 1997;29:326A.
26. Doughty RN, Rodgers A, Sharpe N, MacMahon S. Effectsof beta blocker therapy on mortality in patients with heartfailure. A systematic overview of randomized controlledtrials. Eur Heart J. 1997;18:560–565.
27. ACC/AHA Task Force Report. Guidelines for the evaluationand management of heart failure. Circulation. 1995;952:2764–2784.
A Symposium: Economic Impact of Beta Blockade in Heart Failure/Gregory et al
80S May 7, 2001 THE AMERICAN JOURNAL OF MEDICINEt Volume 110 (7A)