effective design and implementation of integrated care...
TRANSCRIPT
HMAHealthManagement.com
Denver, CO
Lori Raney, MD
Principal, Health Management Associates
Effective Design and ImplementationOf Integrated Care Programs
HMA
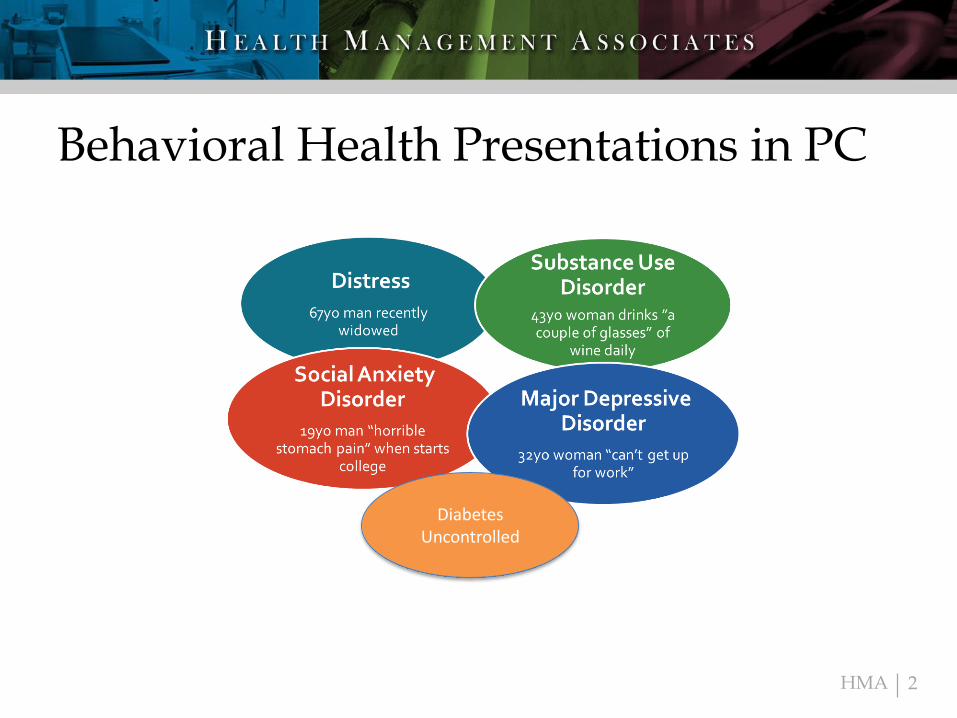
Behavioral Health Presentations in PC
2
Diabetes Uncontrolled
HMA
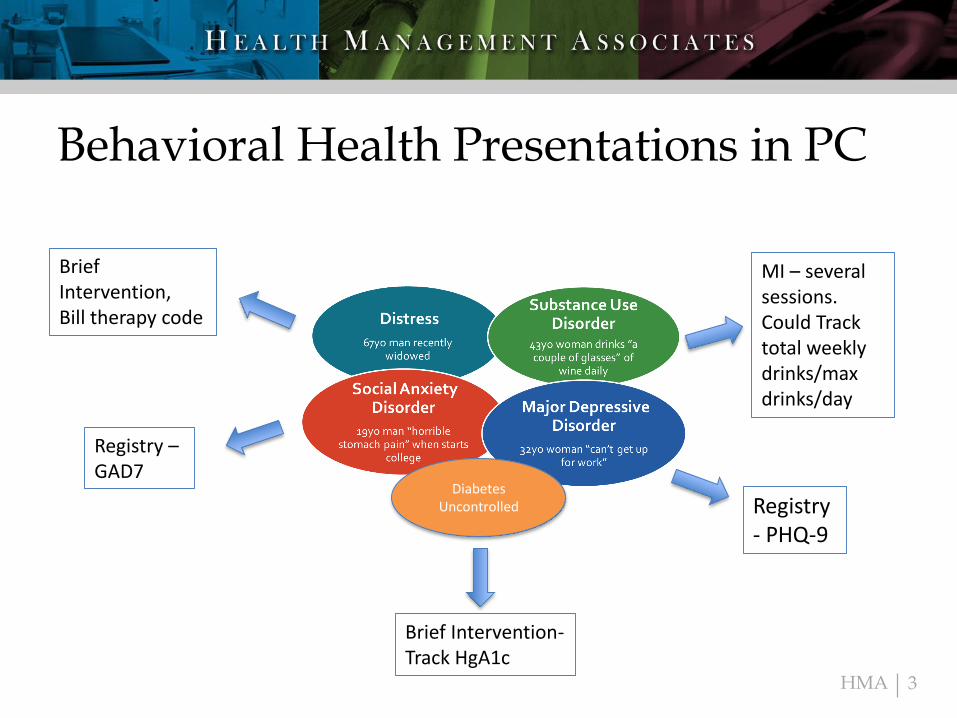
Behavioral Health Presentations in PC
3
Brief Intervention,Bill therapy code
Registry- PHQ-9
Registry –GAD7
MI – several sessions. Could Track total weekly drinks/max drinks/day
Diabetes Uncontrolled
Brief Intervention-Track HgA1c
HMA
Blended Model - Best of Both
4
• Team-driven collaboration that is patient-centered, immediate access in primary care for health behaviors, life stressors, crises, stress-related physical symptoms, ineffective patterns of health care utilization
• Evidence-based, practice-tested
– Mental health and substance use disorders
– Evidence-based behavioral interventions
• Measurement based care (MBC)
– Treat to defined targets
• Population- based
– Track a subgroup with registry as a standard practice
– Caseload review with psychiatric consultant to address patients who are not progressing
https://aims.uw.edu
HMA 5
Recipe for
Success
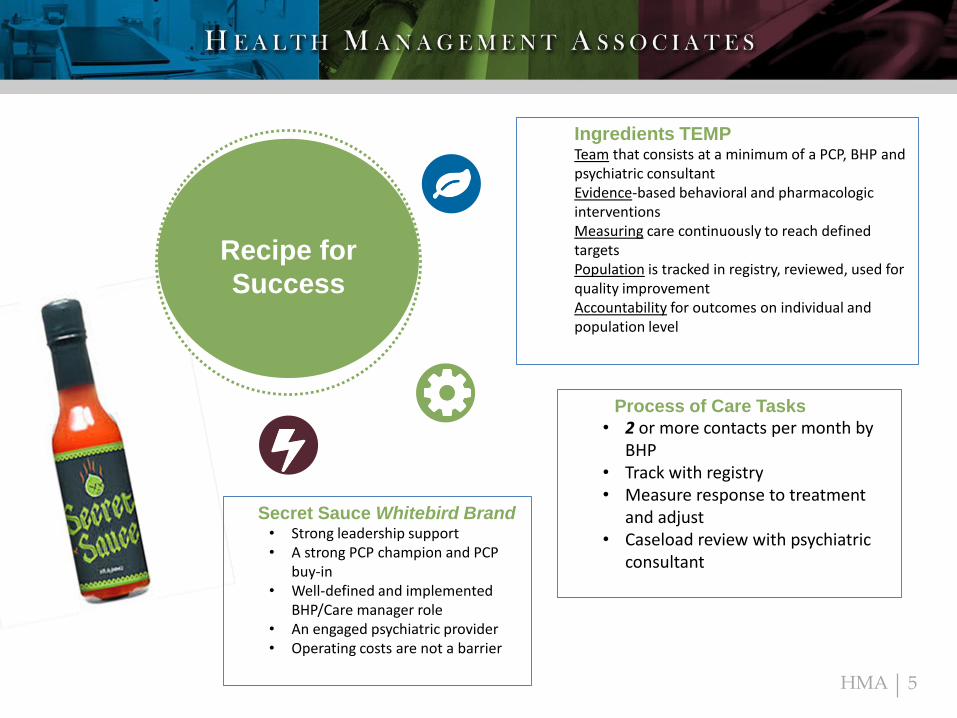
Ingredients TEMPTeam that consists at a minimum of a PCP, BHP and psychiatric consultantEvidence-based behavioral and pharmacologic interventionsMeasuring care continuously to reach defined targetsPopulation is tracked in registry, reviewed, used for quality improvementAccountability for outcomes on individual and population level
Process of Care Tasks
• 2 or more contacts per month by BHP
• Track with registry• Measure response to treatment
and adjust• Caseload review with psychiatric
consultant
Secret Sauce Whitebird Brand• Strong leadership support• A strong PCP champion and PCP
buy-in• Well-defined and implemented
BHP/Care manager role• An engaged psychiatric provider• Operating costs are not a barrier
HMA
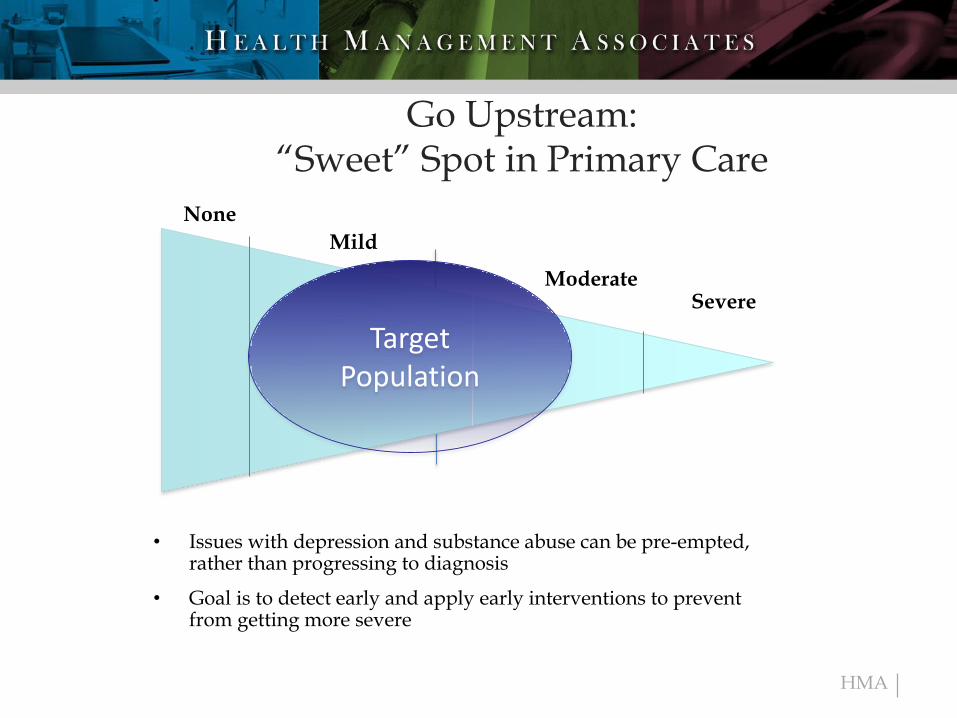
Go Upstream:“Sweet” Spot in Primary Care
• Issues with depression and substance abuse can be pre-empted, rather than progressing to diagnosis
• Goal is to detect early and apply early interventions to prevent from getting more severe
None
Mild
ModerateSevere
Target Population
HMA
Core Principles of Effective Integrated Care
• Operationalize the principles of the chronic care model to improve access to evidence based mental health treatments for primary care patients.
• Effective Care is: – Team-based effective collaboration and Patient-centered
– Evidence-based and practice-tested care
– Measurement-based care, treat to target
– Population-based care – registry, systematic screen
– Accountable care
HMA 8
HMA
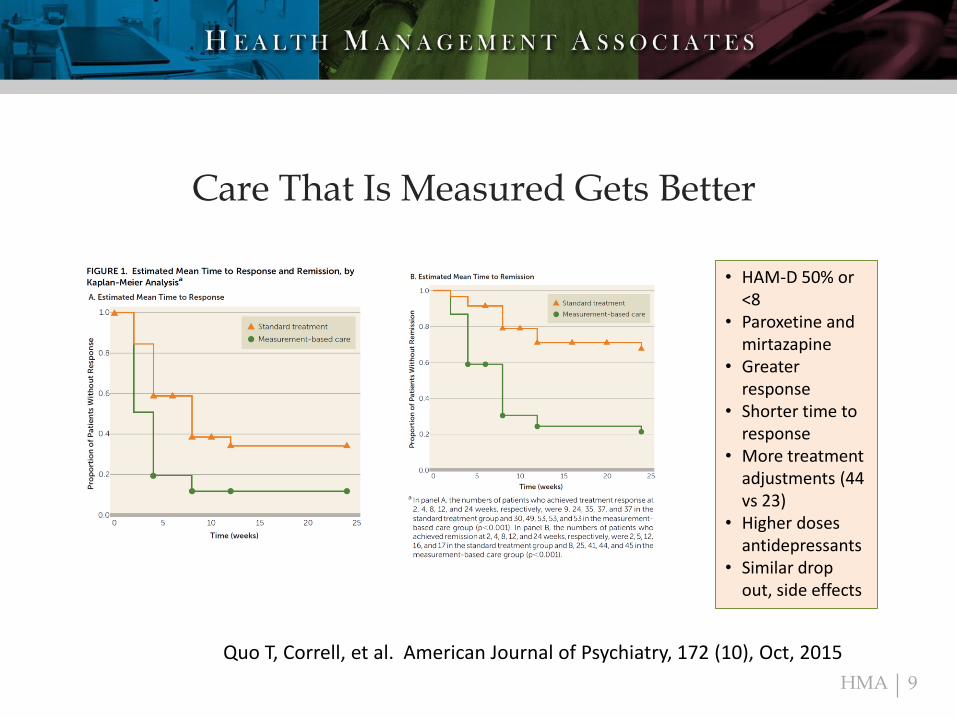
Care That Is Measured Gets Better
9
Quo T, Correll, et al. American Journal of Psychiatry, 172 (10), Oct, 2015
• HAM-D 50% or <8
• Paroxetine and mirtazapine
• Greater response
• Shorter time to response
• More treatment adjustments (44 vs 23)
• Higher doses antidepressants
• Similar drop out, side effects
HMA
MBC Concepts
Process:• Systematic administration of symptom rating scales – use huddle or
registry• NOT a substitute for clinical judgement• Use of the results to drive clinical decision making at the patient
level – overcome clinical inertia• Patient rated scales are equivalent to clinician rated scales• Aggregate data for
– Professional development at the provider level – MACRA– Quality improvement at the clinic level– Inform reimbursement at the payer level
Ineffective Approaches:• One-time screening• Assessing symptoms infrequently• Feeding back outcomes outside the context of the clinical encounter
10Fortney et al Psych Serv Sept 2016
HMA
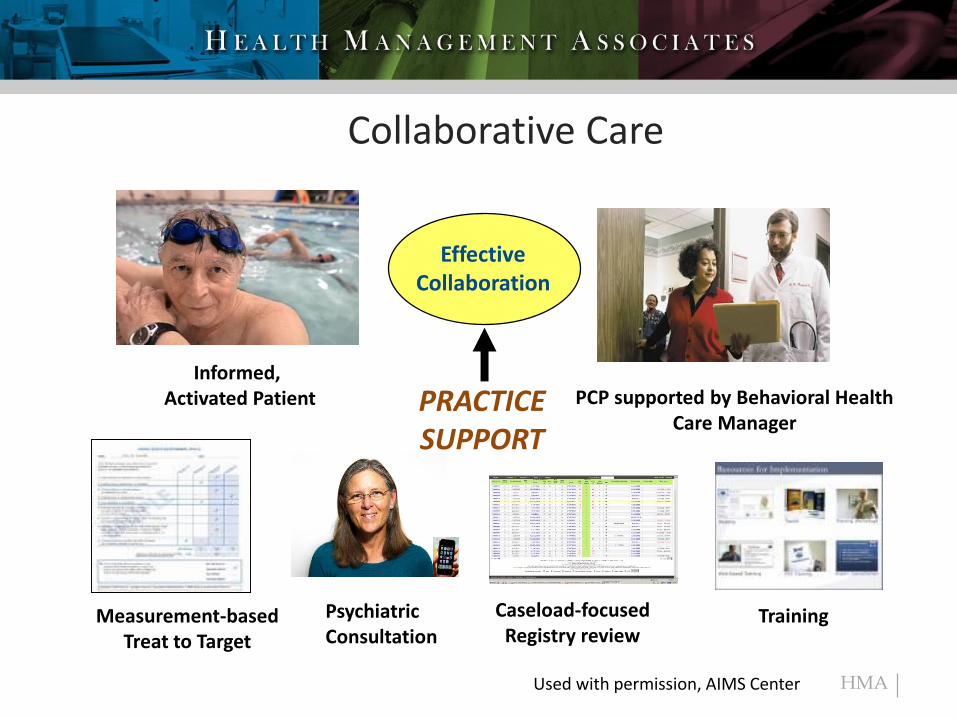
Collaborative Care
EffectiveCollaboration
PCP supported by Behavioral Health Care Manager
Informed, Activated Patient PRACTICE
SUPPORT
Measurement-basedTreat to Target
Caseload-focusedRegistry review
TrainingPsychiatricConsultation
Used with permission, AIMS Center
HMA
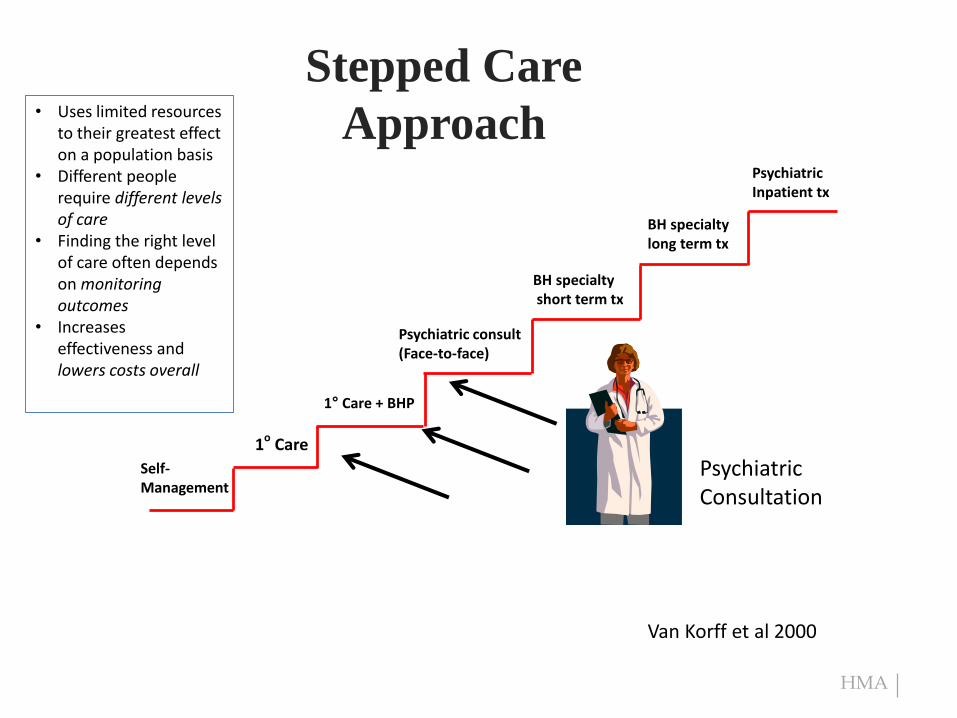
Stepped Care
Approach
1o Care
Psychiatric consult(Face-to-face)
PsychiatricInpatient tx
Self-Management
1° Care + BHP
BH specialtyshort term tx
BH specialty long term tx
PsychiatricConsultation
• Uses limited resources to their greatest effect on a population basis
• Different people require different levels of care
• Finding the right level of care often depends on monitoring outcomes
• Increases effectiveness and lowers costs overall
Van Korff et al 2000
HMA
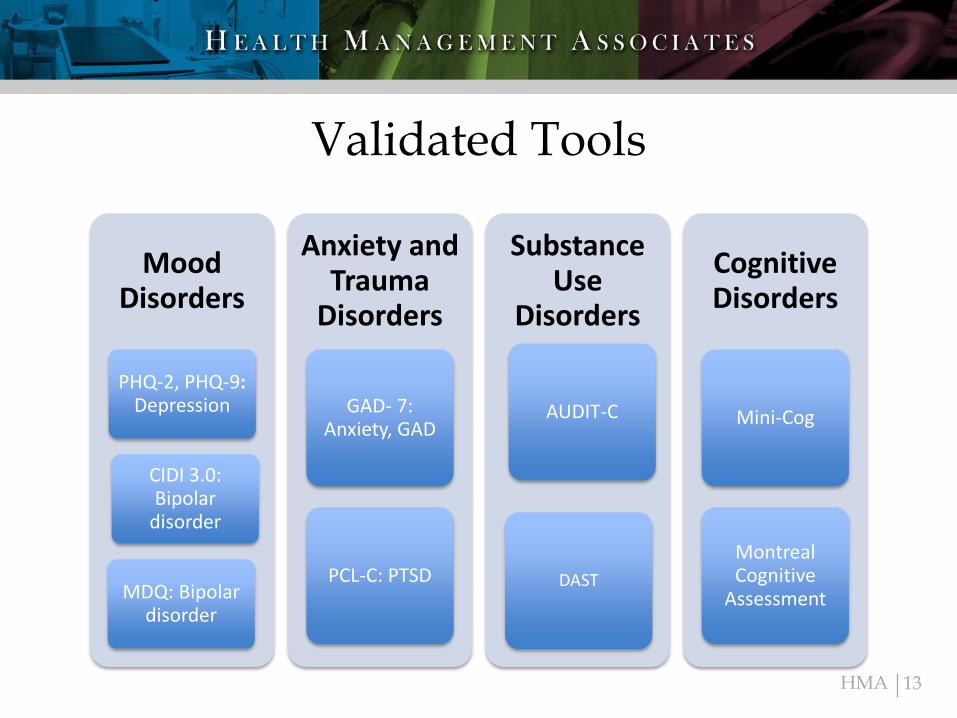
Validated Tools
13
MoodDisorders
PHQ-2, PHQ-9: Depression
MDQ: Bipolar disorder
CIDI 3.0: Bipolar
disorder
Anxiety and Trauma
Disorders
GAD- 7: Anxiety, GAD
PCL-C: PTSD
Substance Use
Disorders
DAST
AUDIT-C
CognitiveDisorders
Mini-Cog
Montreal Cognitive
Assessment
HMA
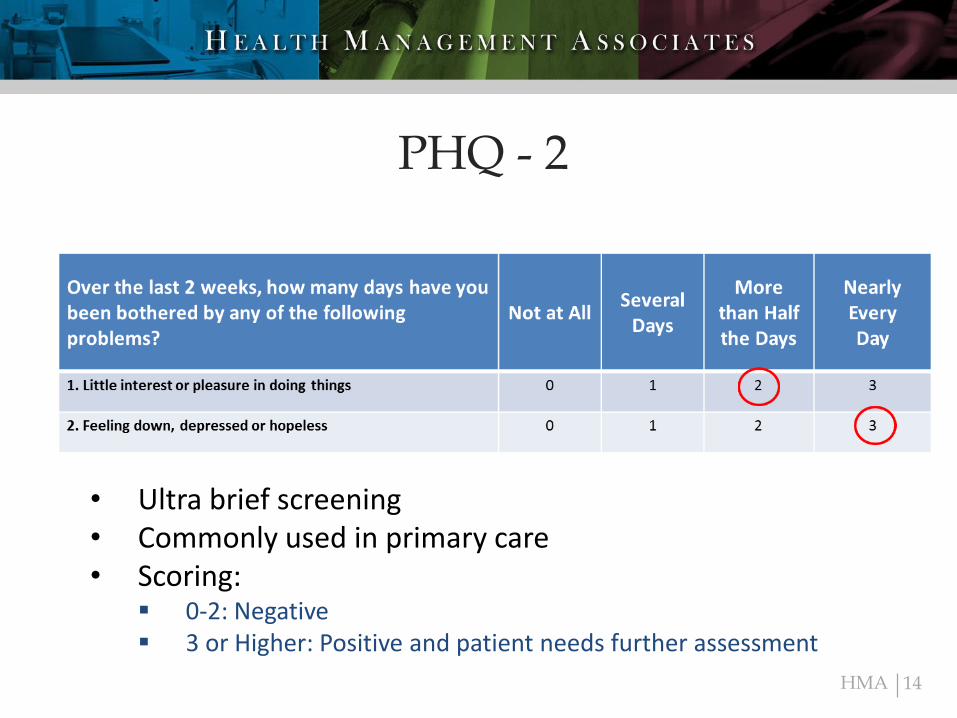
PHQ - 2
14
• Ultra brief screening • Commonly used in primary care• Scoring:
0-2: Negative 3 or Higher: Positive and patient needs further assessment
HMA
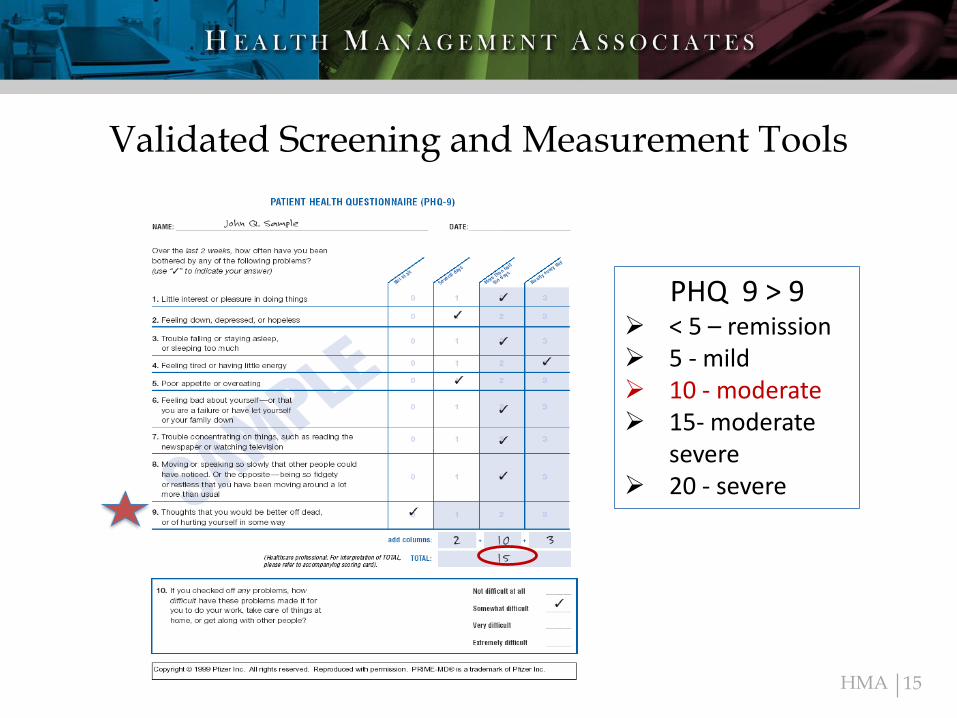
Validated Screening and Measurement Tools
15
PHQ 9 > 9 < 5 – remission 5 - mild 10 - moderate 15- moderate
severe 20 - severe
HMA 16
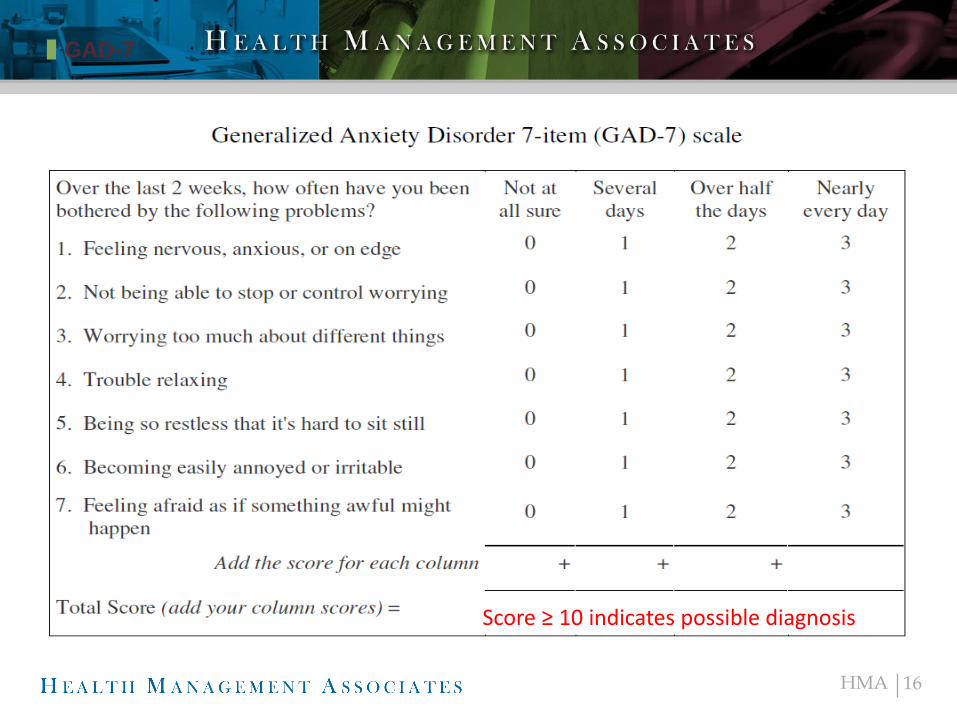
GAD-7
✚ Bulleted List #1
✚ Bulleted List #2
✚ Bulleted List #3
✚ Bulleted List #4
✚ Bulleted List #5
Score ≥ 10 indicates possible diagnosis
HMA 17
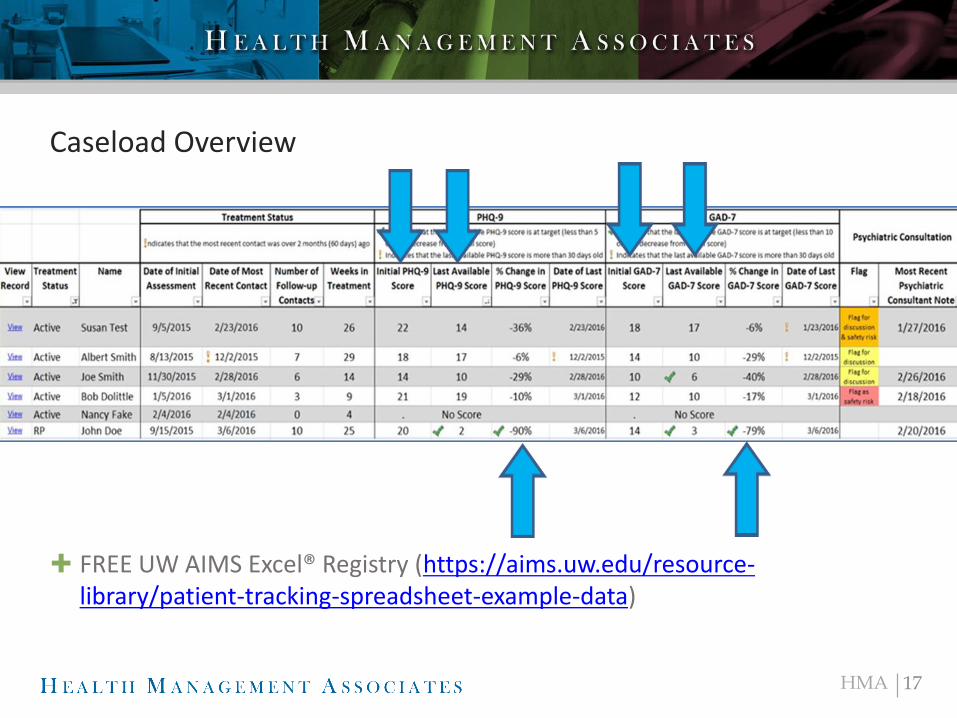
Caseload Overview
✚ FREE UW AIMS Excel® Registry (https://aims.uw.edu/resource-library/patient-tracking-spreadsheet-example-data)
HMA
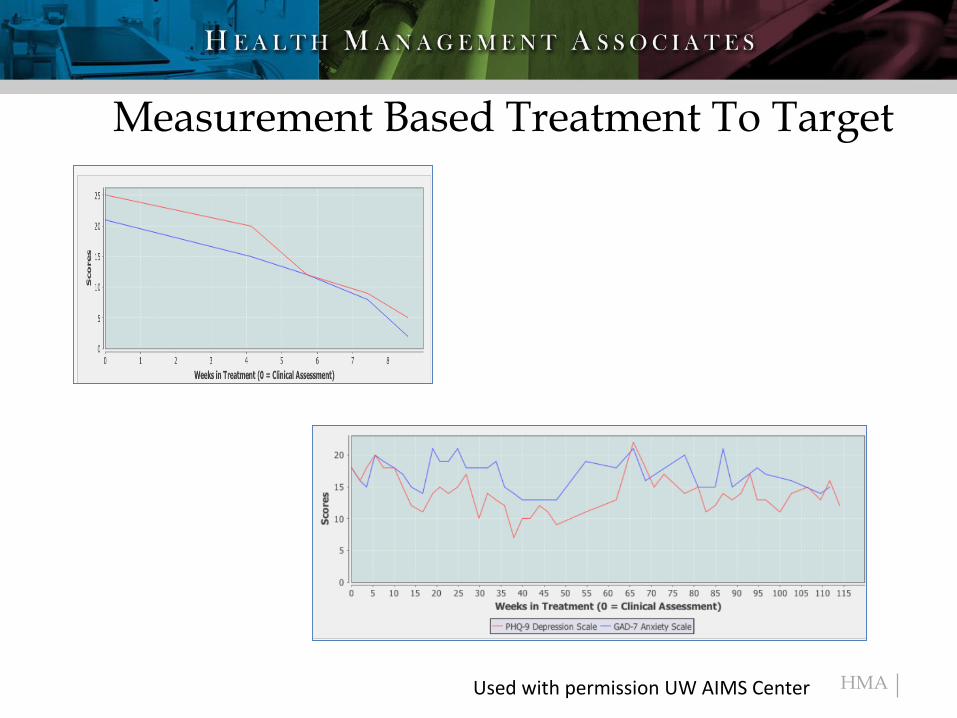
Measurement Based Treatment To Target
Used with permission UW AIMS Center
HMA
BHPs/Care Managers
• Typically MSW, LCSW, MA, RN, PhD, PsyD, paraprofessionals
• Brief intervention skills, generalists
Who are the BHPs/CMs?
• Organization
• Persistence- tenacity
• Creativity and flexibility
• Enthusiasm for learning
• Strong patient advocate
• Willingness to be interrupted
• Ability to work in a team
What makes a good BHP/CM?
19
CAUTION:Traditional Approach to therapyNot willing to be interruptedTimid, insecure about skills

HMA
Evidence-based Brief Interventions
Motivational Interviewing
Distress Tolerance Skills
Behavioral Activation
Problem Solving Therapy
20
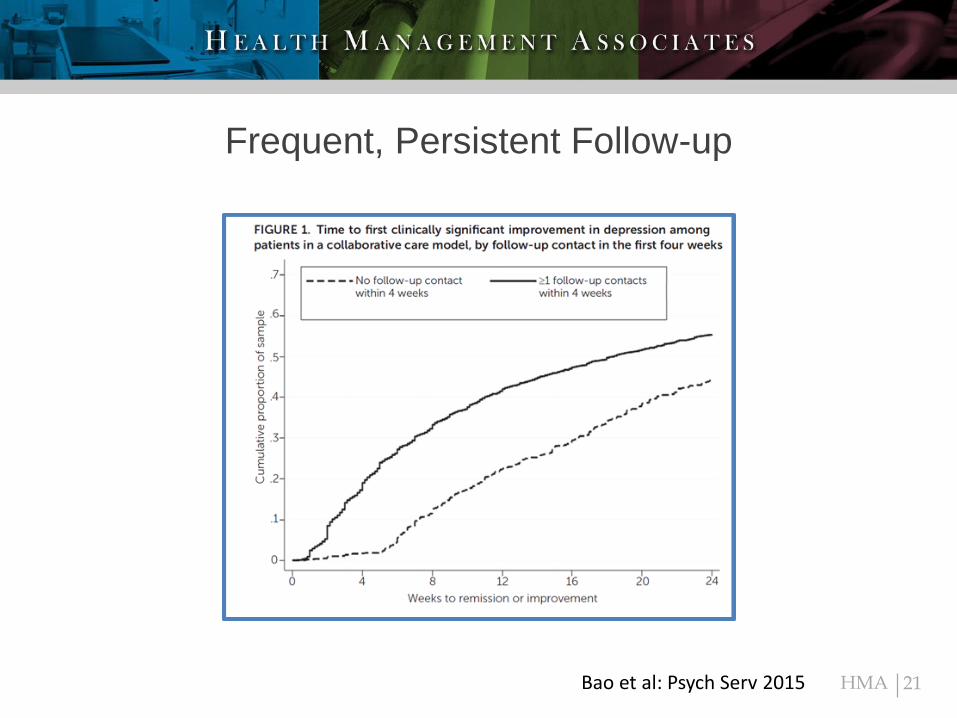
HMA 21
Frequent, Persistent Follow-up
Bao et al: Psych Serv 2015
HMA
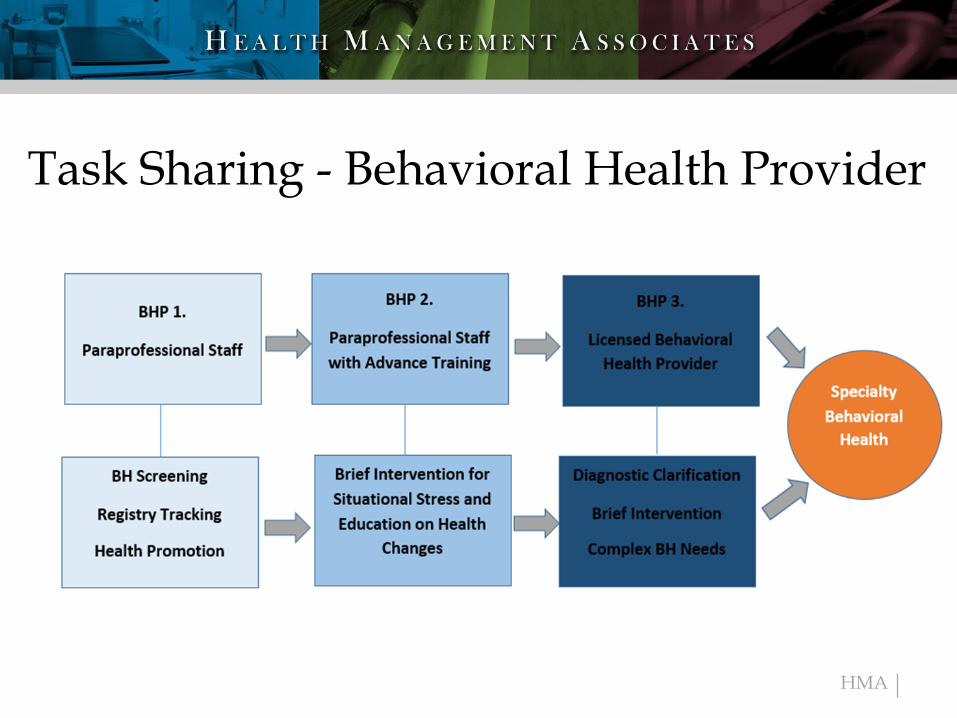
Task Sharing - Behavioral Health Provider
HMA
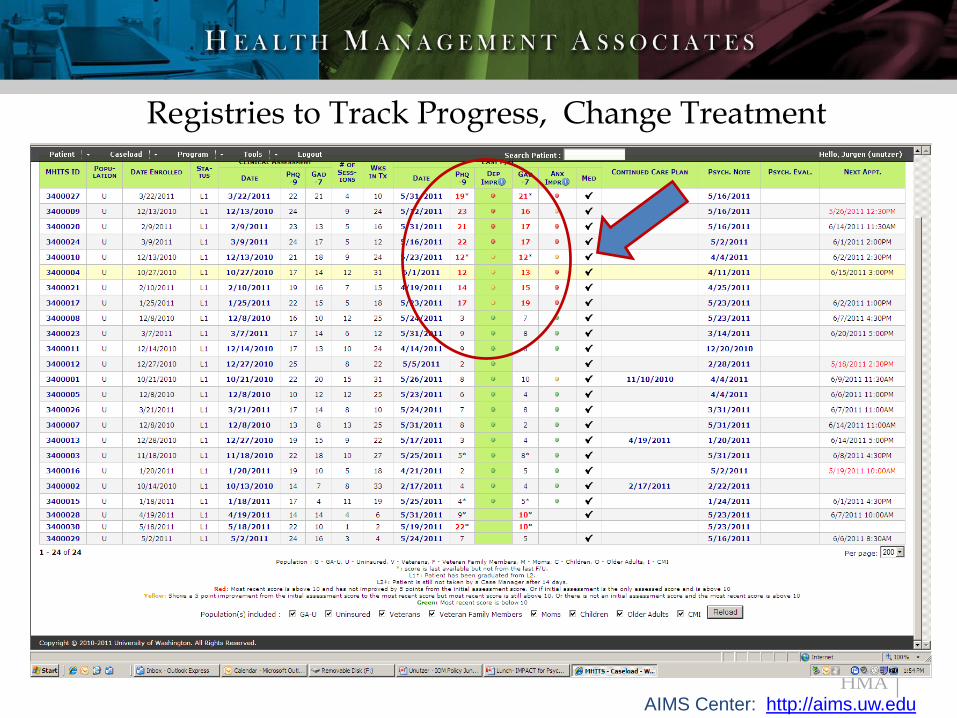
Registries to Track Progress, Change Treatment
AIMS Center: http://aims.uw.edu

HMA
Psychiatric Consultant
Caseload Reviews
• Scheduled (ideally weekly)
• Prioritize patients that are not improving – extends psychiatric expertise to more people in need
• Make recommendations –PCP may or may not implement
• NO RX
Availability to Consult Promptly
• Diagnostic dilemmas
• Education about diagnosis or medications
• Complex patients, such as pregnant or medical complicated
• Pattern recognition**
• Education**
• Build confidence and competence**
HMA
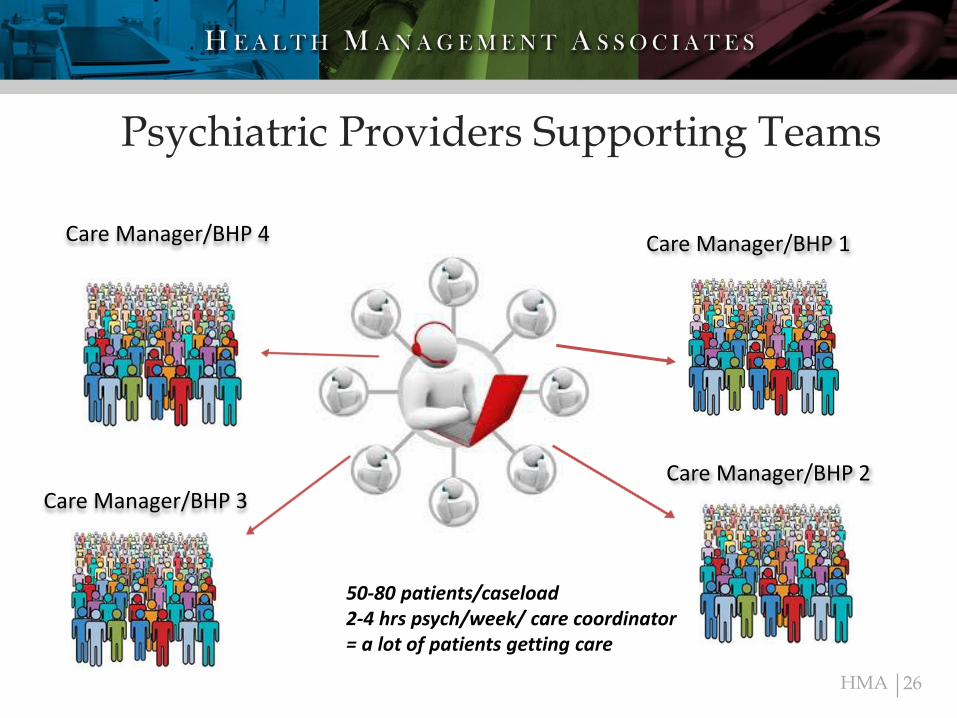
Psychiatric Providers Supporting Teams
26
Care Manager/BHP 1
Care Manager/BHP 2Care Manager/BHP 3
Care Manager/BHP 4
50-80 patients/caseload2-4 hrs psych/week/ care coordinator= a lot of patients getting care
HMA
Roles of Primary CareProvider
• IDENTIFY individuals who need BH support and
• ENGAGE them in the treatment model
• Utilize screening tools to track progress (e.g., PHQ-9)
• Sufficient knowledge of psychopharmacology
27
HMA
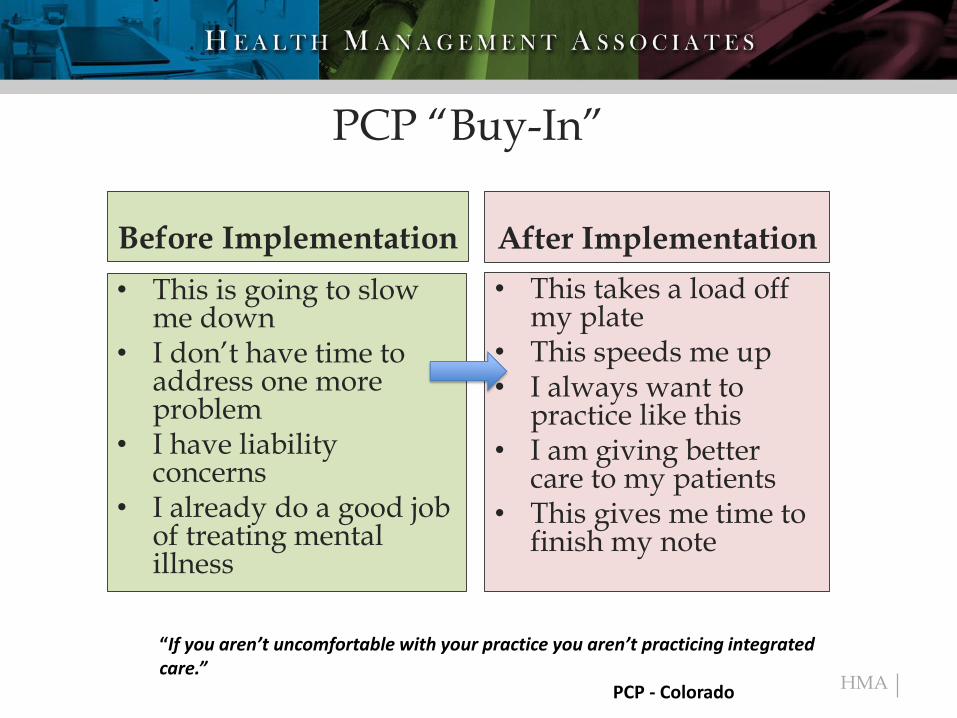
PCP “Buy-In”
Before Implementation After Implementation
• This is going to slow me down
• I don’t have time to address one more problem
• I have liability concerns
• I already do a good job of treating mental illness
• This takes a load off my plate
• This speeds me up• I always want to
practice like this• I am giving better
care to my patients• This gives me time to
finish my note
“If you aren’t uncomfortable with your practice you aren’t practicing integrated care.”
PCP - Colorado
HMA
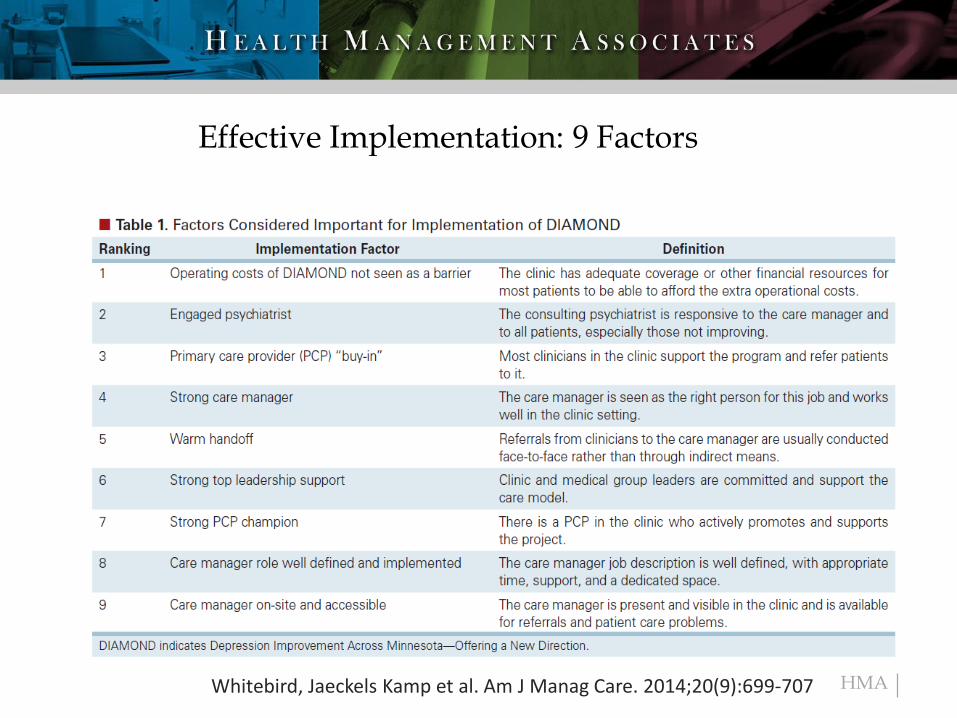
Effective Implementation: 9 Factors
Whitebird, Jaeckels Kamp et al. Am J Manag Care. 2014;20(9):699-707
HMA
Performance Measures: Accountability
• Process Metrics:
– Percent of patients screened for depression
– Percent with follow-up with behavioral care manager within 2 weeks
– Percent not improving that received case review and psychiatric recommendations
– Percent treatment plan changed based on advice
– Percent not improving referred to specialty BH
• Outcome Metrics
– Percent with 50% reduction PHQ-9 – Clinical Response
– Percent reaching remission (PHQ-9 < 5 ) NQF 710 and 711
• Satisfaction – patient and provider
• Functional –work, school, homelessness
• Utilization/Cost
– ED visits, 30 day readmits, med/surg/ICU, overall cost
HMA
July 1st – 6 Visits in Primary Care
HMA
Documentation Requirements
• The requirements for this type of note have four parts/requirements that we use to make documentation simple and compliant
• First visit
Diagnosis -patient referred by primary care provider for depression follow-up
Assessment of symptoms-patient scored a 14 on the PHQ9, reports difficulty sleeping and concentrating as most prominent symptoms
Clinical Intervention- utilized behavioral activation to establish short term goal of XX to begin care and engage patient into treatment
Plan-patient provided with follow up phone appointment ( 1-2 days) on XX and follow up visit on XXX (within the week) to begin care for depression and PHQ9 reduction ……..
• This documentation can be short and often done concurrently with the patient and during a warm hand off and can be done to help keep up with the volume
HMA
CPT Codes for CoCM
99492 - $162
99493 - $130 Billed once a month by the PCP99494 - $6699484 - $48G0512 -$134 (FQHCs only)
• Outreach and engagement by BHP• Initial assessment of the patient, including administration of
validated rating scales• Entering patient data in a registry and tracking patient follow-up
and progress • Participation in weekly caseload review with the psychiatric
consultant• Provision of brief interventions using evidence-based techniques
such as behavioral activation, motivational interviewing, and other focused treatment strategies.
34
HMA
HMA 36
Recipe for
Success
Ingredients TEMPTeam that consists at a minimum of a PCP, BHP and psychiatric consultantEvidence-based behavioral and pharmacologic interventionsMeasuring care continuously to reach defined targetsPopulation is tracked in registry, reviewed, used for quality improvementAccountability for outcomes on individual and population level
Process of Care Tasks
• 2 or more contacts per month by BHP
• Track with registry• Measure response to treatment
and adjust• Caseload review with psychiatric
consultant
Secret Sauce Whitebird Brand• Strong leadership support• A strong PCP champion and PCP
buy-in• Well-defined and implemented
BHP/Care manager role• An engaged psychiatric provider• Operating costs are not a barrier
HMA
Resources
University of WA AIMS Center http://aims.uw.edu
Center for Integrated Health Solutions https://www.integration.samhsa.gov
www.seattlechildrens.org/pdf/PAL/WA/WA-care-guide.pdf
37