effective strategies for childhood obesity prevention via
TRANSCRIPT
REVIEW Open Access
Effective strategies for childhood obesityprevention via school based, familyinvolved interventions: a critical review forthe development of the Feel4Diabetes-study school based componentChristina-Paulina Lambrinou1, Odysseas Androutsos2, Eva Karaglani1, Greet Cardon3, Nele Huys3, Katja Wikström4,Jemina Kivelä4, Winne Ko5, Ernest Karuranga5, Kaloyan Tsochev6, Violeta Iotova6, Roumyana Dimova7,Pilar De Miguel-Etayo8,9, Esther M. González-Gil8,9,10, Hajnalka Tamás11, Zoltán JANCSÓ11, Stavros Liatis12,Konstantinos Makrilakis12, Yannis Manios1* and on behalf of the Feel4Diabetes-study group
Abstract
Background: Although there are many interventions targeting childhood obesity prevention, only few havedemonstrated positive results. The current review aimed to gather and evaluate available school-based interventionstudies with family involvement targeting dietary, physical activity and sedentary behaviors among primaryschoolchildren and their families, in order to identify the most effective strategies.
Methods: Studies published between 2000 and January 2015 were retrieved from scientific electronic databasesand grey literature. The databases used included MEDLINE/PubMed, Web-of-Science, CINAHL and Scopus. Includedstudies had to be experimental controlled studies and had duration over 1 school year, had family involvement,combined PA and dietary behaviors and were implemented in school setting. A complementary search wasexecuted to update the review to cover the period from February 2015 to January 2019.
(Continued on next page)
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] of Nutrition and Dietetics, School of Health Science andEducation, Harokopio University, 70 El Venizelou Ave, 176 71 Kallithea,Athens, GreeceFull list of author information is available at the end of the article
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52https://doi.org/10.1186/s12902-020-0526-5

(Continued from previous page)
Results: From the studies examined (n = 425), 27 intervention programs (33 publications) fulfilled the inclusioncriteria. Among these, 15 presented significant effect on weight status and/ or overweight/ obesity or clinicalindices, 3 presented significant effect on most energy balance-related behaviors (EBRBs) while 9 presentedsignificant effect on some/few EBRBs or determinants. Strategies implemented in effective interventions were:teachers acting as role-models and being actively involved in the delivery of the intervention, school policiessupporting the availability of healthy food and beverage choices and limiting unhealthy snacks, changes in theschoolyard, in the recess rules and in the physical education classes to increase physical activity, and involvingparents in the intervention via assignments, meetings, informative material and encouraging them to improve thehome environment. Use of incentives for children, social marketing techniques, collaboration with localstakeholders were found to increase effectiveness. Programs that focused only on educational sessions and materialfor parents, without promoting relevant environmental and policy changes, were found to be less effective. Culturaladaptations have been suggested to increase the intervention’s acceptance in specific or vulnerable populationgroups.
Conclusions: Several effective strategies were identified in the reviewed programs. Outcomes of the current reviewwere taken into account in developing the Feel4Diabetes-intervention and summed up as recommendations in thecurrent work in order to facilitate other researchers designing similar childhood obesity prevention initiatives.
Keywords: Obesity prevention, Type 2 diabetes prevention, Primary school children, Families, School basedintervention
BackgroundChildhood obesity is a growing world-wide health prob-lem. It is estimated that about 170 million children arecurrently with overweight globally [1]. In US children,obesity prevalence has increased from 6% in 1980 to17% in 2008 [2] and to 18.5% in 2016 [3]. In Europe, thetrend of childhood obesity is following the same pattern,with its prevalence increasing across most Europeancountries [4], especially in low-to-middle-income coun-tries (LMICs) and in vulnerable groups [5, 6].
Being overweight or obese has serious health conse-quences, especially for children. Having a high bodymass index (BMI) is a major risk factor for diseases suchas cardiovascular disease, type 2 diabetes and cancerlater in life [7, 8]. These diseases, also known as non-communicable diseases (NCDs), can cause prematuremortality as well as long-term morbidity. Due to the sig-nificant increase in the prevalence of obesity and the ser-ious public health consequences, obesity is consideredone of the most important public health challenges ofthe twenty-first century [9, 10].
Early childhood is considered to provide a unique op-portunity to establish lifestyle behaviors such as healthyeating habits, physical activity and limited sedentary timethat will promote health and minimize the risk of obes-ity. This is further supported by the fact that, as a resultsof these behaviours, childhood obesity tracks into adult-hood with overweight preschool children being morelikely to become overweight adults in comparison totheir normal-weight peers [11–15]. Thus, interventionspromoting such healthy behaviors in childhood providea key strategy in the prevention of obesity, since it has
been shown that treating obesity in adulthood posesmore difficulties than changing lifestyle habits earlier on[16].
To date, many programs have been developed in orderto prevent obesity in children. The vast majority of theseprograms use schools for the implementation of interven-tions [17]. Schools are considered an important setting forintervening in children’s obesity related behavior, for anumber of reasons: (i) primary school education is com-pulsory for all children in most countries and reaches allchildren with different backgrounds (ii) children spend asignificant part of their daily life at school, usually con-suming one or two meals per day; (iii) schools offer phys-ical education classes and provide opportunities forphysical activity during recess; (iv) schools offer a struc-tured environment where interventions can be easily ap-plied/ fit, (v) implementers can reach many children in arelatively short time via schools; (vi) teaching staff can sig-nificantly facilitate and contribute to the delivery of theintervention, thus increasing the intervention’s sustainabil-ity [18]. Despite the aforementioned advantages, the over-all impact of school-based interventions is questionableand generalizable recommendations cannot be easily ex-tracted [2].
For the needs of the European multicenterFeel4Diabetes-study the current study examined inter-ventions that have been implemented in the school set-ting and focused on the promotion of healthy eating andphysical activity and the reduction/interruption of sed-entary behavior aiming to prevent childhood obesity.The Feel4Diabetes-study was implemented in the overallpopulation in low/middle-income countries (Bulgaria,
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 2 of 20

Hungary), in low socio-economic areas in high-incomecountries (Belgium, Finland) and in countries underausterity measures (Greece, Spain). More information onthis project can be found in the literature [19]. The aimof the current review was to identify the most effectivestrategies in improving health behaviors and tacklingobesity in primary school-aged children with special em-phasis given to low socioeconomic status and vulnerablegroups that Feel4Diabete-study specifically targeted, tak-ing into account their increased risk for obesity [9, 20]and type 2 diabetes [21]. The Feel4Diabetes project wasdeveloped using the PRECEDE-PROCEED model as thetheoretical basis. The current review served as a part ofthe PRECEDE phase of this specific theoretical modeland its outcomes were utilized in the development ofthe Feel4Diabetes school- and community-basedintervention.
MethodsSearch strategyThe bibliographic search strategy focused on articlespublished in peer-reviewed, English language journals,published from 2000 to January 2015, when theFeel4Diabetes-intervention was developed. A comple-mentary search was executed to update the results forthe publication to cover the period from February 2015to January 2019 following the same methodology. Thedatabases used included MEDLINE/PubMed, Web-of-Science, CINAHL and Scopus. Citations in reviews werealso used. The PICO key terms used for conducting theliterature search are presented in SupplementaryTable 1.
Selection criteriaTo be included, studies had to be original experimentalcontrolled studies with school-based interventions aim-ing to prevent obesity in primary school-aged childrenfrom any country, published between 2000 and January2019, in English. Additional inclusion criteria were ap-plied based on recent literature [18, 22]. These criteriawere, namely: a) duration of > 1 school year (i.e. at least6 months), b) family involvement, either by contactingparents via their children with the use of newsletters,etc. or by having meetings with them, c) combination ofphysical activity and dietary behaviors, d) implementa-tion of the school-based intervention by schoolpersonnel (i.e. healthcare professionals working atschools or teachers). These criteria were applied in orderto avoid repetition of already proven to be effective strat-egies and take the existing literature a step further.
Exclusion criteriaExclusion criteria included interventions implemented inpreschools, early childcare programs, adolescents or
after-school programs, descriptive or analytic studies, re-views on surgical or pharmaceutical treatments, litera-ture reviews, opinions or editorials, reports published asmeeting abstracts only, reviews of causal relationshipsbetween obesity and related factors, articles reportingstudy design and/or process evaluation only as well aspapers focused on physiological, molecular or geneticresearch and papers focused on morbidities (such askidney disease and diabetes) in which obesity is acomorbidity.
Selection strategy and data extraction proceduresThe flowchart of the publication identification process ispresented in Fig. 1. Data from the included studies wereextracted using a standardized form. Extracted data in-cluded: author, year of publication, project name, coun-try, participant data, intervention duration, theory usedand strategies implemented as described in the method-ology of the relevant publications, outcomes as well asfollow-up period if available. In addition, the setting inwhich the intervention was implemented was also ex-tracted in order to identify strategies that proved to beeffective in low-SES areas or in vulnerable groups. Asummary table of the selected studies was constructedand the clinical significance of the results was evaluatedfor each study, to facilitate interpretation of the effect-iveness of intervention. The scoring is marked in thesummary table as follows:
� (+++) significant effect on weight status and/ oroverweight/ obesity or clinical indices.
� (++) significant improvement in most importanttarget behaviors.
� (+) significant improvement in some/few secondarytarget behaviors.
� (−) no effect.
ResultsThe studies included in the current analysis have beensummarized in Table 1 outlining the target population,intervention strategies and design, measures, outcomes,and findings relevant to obesity prevention. The inter-ventions in table have been arranged alphabeticallybased on first author’s name but with clustering the pub-lications of same projects together.
General description of findingsUsing the aforementioned search strategy 1148 publica-tions were identified. After removing duplicates and afirst title screening 425 articles remained. These 425 ar-ticles were screened based on their abstract, in order todiscard studies without yet published results, those tar-geting specific populations (e.g. only obese children orpatients), preschoolers or adolescents. Of the 122 articles
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 3 of 20
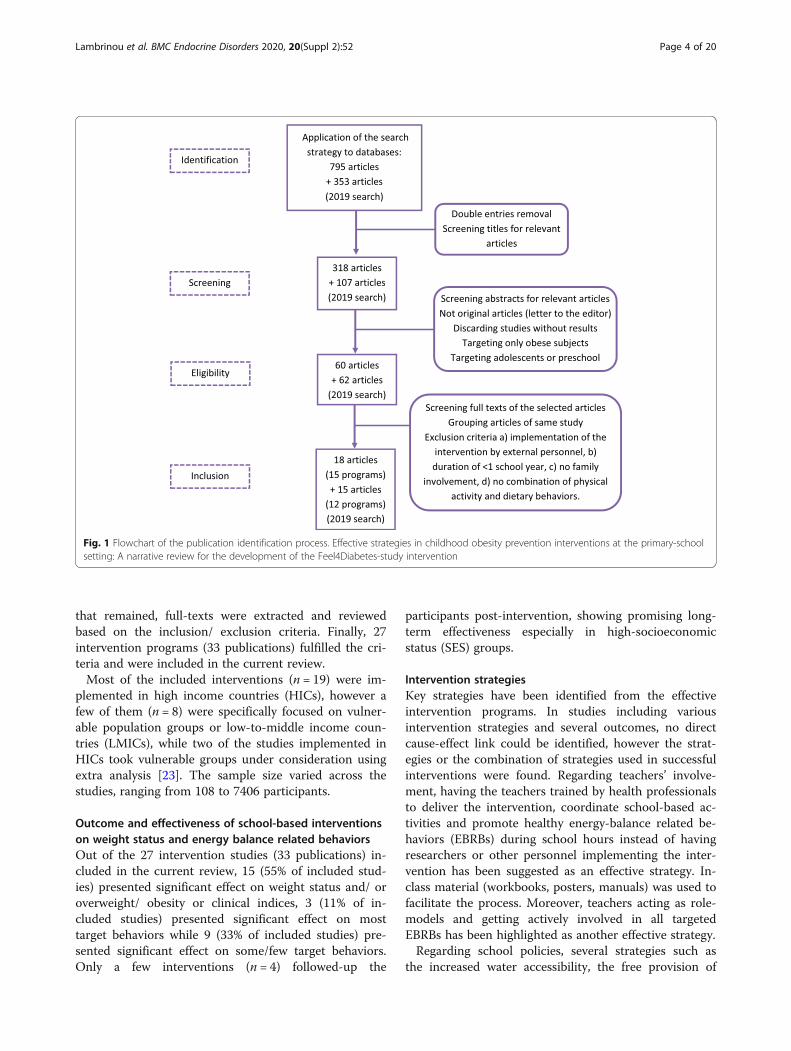
that remained, full-texts were extracted and reviewedbased on the inclusion/ exclusion criteria. Finally, 27intervention programs (33 publications) fulfilled the cri-teria and were included in the current review.Most of the included interventions (n = 19) were im-
plemented in high income countries (HICs), however afew of them (n = 8) were specifically focused on vulner-able population groups or low-to-middle income coun-tries (LMICs), while two of the studies implemented inHICs took vulnerable groups under consideration usingextra analysis [23]. The sample size varied across thestudies, ranging from 108 to 7406 participants.
Outcome and effectiveness of school-based interventionson weight status and energy balance related behaviorsOut of the 27 intervention studies (33 publications) in-cluded in the current review, 15 (55% of included stud-ies) presented significant effect on weight status and/ oroverweight/ obesity or clinical indices, 3 (11% of in-cluded studies) presented significant effect on mosttarget behaviors while 9 (33% of included studies) pre-sented significant effect on some/few target behaviors.Only a few interventions (n = 4) followed-up the
participants post-intervention, showing promising long-term effectiveness especially in high-socioeconomicstatus (SES) groups.
Intervention strategiesKey strategies have been identified from the effectiveintervention programs. In studies including variousintervention strategies and several outcomes, no directcause-effect link could be identified, however the strat-egies or the combination of strategies used in successfulinterventions were found. Regarding teachers’ involve-ment, having the teachers trained by health professionalsto deliver the intervention, coordinate school-based ac-tivities and promote healthy energy-balance related be-haviors (EBRBs) during school hours instead of havingresearchers or other personnel implementing the inter-vention has been suggested as an effective strategy. In-class material (workbooks, posters, manuals) was used tofacilitate the process. Moreover, teachers acting as role-models and getting actively involved in all targetedEBRBs has been highlighted as another effective strategy.Regarding school policies, several strategies such as
the increased water accessibility, the free provision of
Fig. 1 Flowchart of the publication identification process. Effective strategies in childhood obesity prevention interventions at the primary-schoolsetting: A narrative review for the development of the Feel4Diabetes-study intervention
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 4 of 20

Table 1 Overview of the publications included in the review
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Angelopouloset al., 2009[19]
CHILDRENstudy
Greece 13 schools646 pupils5th grade(Mean ± SD:10.3 ± 0.4years)
– 1 schoolyear
School and homeenvironment(availability ofhealthy choices)Policies (Children’sand teachers in-class-material, En-joyable fitness clas-ses, Schoolyardsopen after schoolhours)Parentsengagement(Meetings tosupport children’senergy-balance re-lated behaviors(EBRBs), Increasingparental support,Overcoming thebarriers in acces-sing physical activ-ity (PA) areas))Teachers acting asrole-modelsTheory of PlannedBehavior
– Significantfavorable effect onfruits consumptionand fats/oils andsweets/beveragesconsumption.Significantfavorable effect onBMI (P = 0.047)could be explainedby the changes infruit and fats/oilsintake.(+++)
Benjaminset al., 2010[20]
– Chicago 2 schools581 students1st-8th grade
Jewish schools 2 schoolyears
Formation of awellness councilWriting of awellnesspolicyHealtheducation (viahealth lessons)Physical education(by providingfunding to increasePA, genderseparatedswimming lessons)Schoolenvironment(removing vendingmachines, healthylunches, skim-milkpromotion, fruit ofthe week program)Family involvement(school events,meetings,newsletters)Staff wellness (role-models, privatedietaryconsultations,educationalsessions)The Centers forDisease Control(CDC) ecologicalmodel-based Co-ordinated SchoolHealth Program
– Significantfavorable effect nthe percentage ofolder studentsregularly meetingphysical activityguidelines. Fewchanges inattitudes, otherbehaviors, orenvironmentalfactors were seen.(++)
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 5 of 20
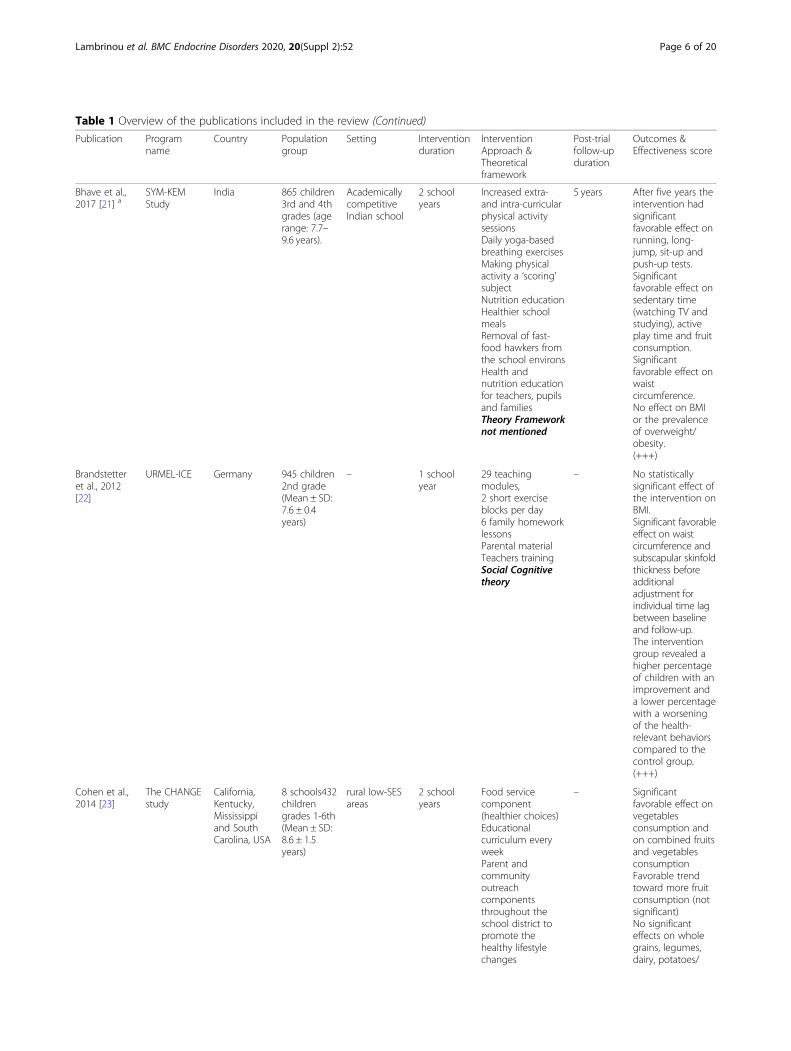
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Bhave et al.,2017 [21] a
SYM-KEMStudy
India 865 children3rd and 4thgrades (agerange: 7.7–9.6 years).
AcademicallycompetitiveIndian school
2 schoolyears
Increased extra-and intra-curricularphysical activitysessionsDaily yoga-basedbreathing exercisesMaking physicalactivity a ‘scoring’subjectNutrition educationHealthier schoolmealsRemoval of fast-food hawkers fromthe school environsHealth andnutrition educationfor teachers, pupilsand familiesTheory Frameworknot mentioned
5 years After five years theintervention hadsignificantfavorable effect onrunning, long-jump, sit-up andpush-up tests.Significantfavorable effect onsedentary time(watching TV andstudying), activeplay time and fruitconsumption.Significantfavorable effect onwaistcircumference.No effect on BMIor the prevalenceof overweight/obesity.(+++)
Brandstetteret al., 2012[22]
URMEL-ICE Germany 945 children2nd grade(Mean ± SD:7.6 ± 0.4years)
– 1 schoolyear
29 teachingmodules,2 short exerciseblocks per day6 family homeworklessonsParental materialTeachers trainingSocial Cognitivetheory
– No statisticallysignificant effect ofthe intervention onBMI.Significant favorableeffect on waistcircumference andsubscapular skinfoldthickness beforeadditionaladjustment forindividual time lagbetween baselineand follow-up.The interventiongroup revealed ahigher percentageof children with animprovement anda lower percentagewith a worseningof the health-relevant behaviorscompared to thecontrol group.(+++)
Cohen et al.,2014 [23]
The CHANGEstudy
California,Kentucky,Mississippiand SouthCarolina, USA
8 schools432childrengrades 1-6th(Mean ± SD:8.6 ± 1.5years)
rural low-SESareas
2 schoolyears
Food servicecomponent(healthier choices)Educationalcurriculum everyweekParent andcommunityoutreachcomponentsthroughout theschool district topromote thehealthy lifestylechanges
– Significantfavorable effect onvegetablesconsumption andon combined fruitsand vegetablesconsumptionFavorable trendtoward more fruitconsumption (notsignificant)No significanteffects on wholegrains, legumes,dairy, potatoes/
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 6 of 20

Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
encouraged duringand after theschool day.Theory Frameworknot mentioned
potato products,saturated fat,added sugars, ordietary fiberconsumption.(+)
De Coenet al., 2012[24]
POP project Belgium 31 schools,1102children3–6 years(Mean ± SD:5.0 ± 1.3years)
– 2 schoolyears
Family involvementvia educationalstrategies,newsletters, tips,recipesDevelopment of anactive playgroundImplementation ofhealth-relatedphysical educationEnvironmental andpolicy changes toincrease availabilityof healthy optionsCommunitystakeholders, localpolicy and media(meetings,brochures)involvementSocio-ecologicalmodel
– Significantfavorable effect onBMI Z-score in thelow-socioeconomicstatus (SES) inter-ventioncommunity.(+++) only in low-socioeconomic sta-tus (SES) groups.
Foster et al.,2007 [25]
– Philadelphia,USA
10 schools1349children4th - 6thgrade(Mean ± SD:11.1 ± 1.0years)
– 2 schoolyears
School NutritionPolicy Initiative:School self-assessment (schoolrating and actionplan for change)Staff training (10 h)Nutrition education(50 h)Nutrition policy(cafeteria offeringonly healthyoptions, removal ofvending machines)Social marketing(Slogans, character/hero, raffle tickets)Parent outreach(meetings,workshops)Social marketingand other theories
– The interventionresulted in a 50%reduction in theincidence ofoverweight.Significantly fewerchildren in theinterventionschools than in thecontrol schoolsbecameoverweight after 2years. Theprevalence ofoverweight waslower in theinterventionschools.No differenceswere observed inthe incidence orprevalence ofobesity or in theremission ofoverweight orobesity at 2 years.Significantfavorable effect oninactive hours perweek and on hoursspent on TV onweekdays.(+++)
Jensen et al.,2015 [26]
CopenhagenSchool ChildIntervention
Copenhagen,Denmark
18 schools307 childrenwith full data
– 3 schoolyears
Two additionalphysical education(PE) lessons per
Significantfavorable effect ondietary fibre intake
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 7 of 20
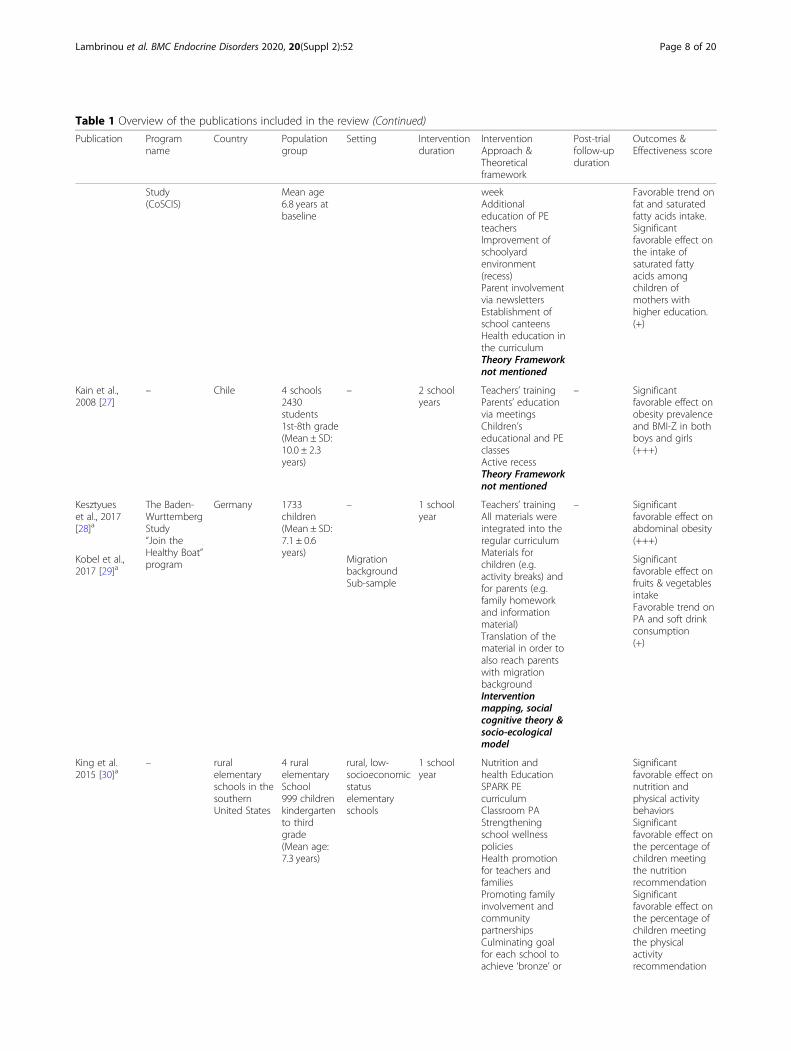
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Study(CoSCIS)
Mean age6.8 years atbaseline
weekAdditionaleducation of PEteachersImprovement ofschoolyardenvironment(recess)Parent involvementvia newslettersEstablishment ofschool canteensHealth education inthe curriculumTheory Frameworknot mentioned
Favorable trend onfat and saturatedfatty acids intake.Significantfavorable effect onthe intake ofsaturated fattyacids amongchildren ofmothers withhigher education.(+)
Kain et al.,2008 [27]
– Chile 4 schools2430students1st-8th grade(Mean ± SD:10.0 ± 2.3years)
– 2 schoolyears
Teachers’ trainingParents’ educationvia meetingsChildren’seducational and PEclassesActive recessTheory Frameworknot mentioned
– Significantfavorable effect onobesity prevalenceand BMI-Z in bothboys and girls(+++)
Kesztyueset al., 2017[28]a
The Baden-WurttembergStudy“Join theHealthy Boat”program
Germany 1733children(Mean ± SD:7.1 ± 0.6years)
– 1 schoolyear
Teachers’ trainingAll materials wereintegrated into theregular curriculumMaterials forchildren (e.g.activity breaks) andfor parents (e.g.family homeworkand informationmaterial)Translation of thematerial in order toalso reach parentswith migrationbackgroundInterventionmapping, socialcognitive theory &socio-ecologicalmodel
– Significantfavorable effect onabdominal obesity(+++)
Kobel et al.,2017 [29]a
MigrationbackgroundSub-sample
Significantfavorable effect onfruits & vegetablesintakeFavorable trend onPA and soft drinkconsumption(+)
King et al.2015 [30]a
– ruralelementaryschools in thesouthernUnited States
4 ruralelementarySchool999 childrenkindergartento thirdgrade(Mean age:7.3 years)
rural, low-socioeconomicstatuselementaryschools
1 schoolyear
Nutrition andhealth EducationSPARK PEcurriculumClassroom PAStrengtheningschool wellnesspoliciesHealth promotionfor teachers andfamiliesPromoting familyinvolvement andcommunitypartnershipsCulminating goalfor each school toachieve ‘bronze’ or
Significantfavorable effect onnutrition andphysical activitybehaviorsSignificantfavorable effect onthe percentage ofchildren meetingthe nutritionrecommendationSignificantfavorable effect onthe percentage ofchildren meetingthe physicalactivityrecommendation
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 8 of 20
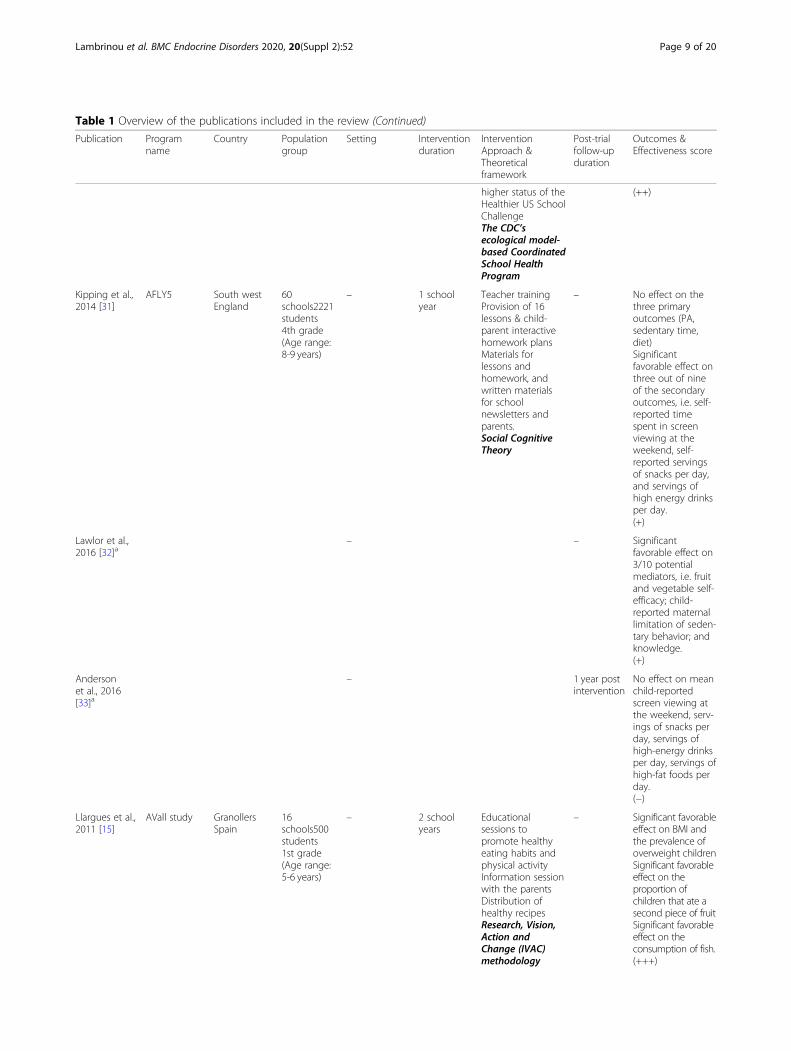
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
higher status of theHealthier US SchoolChallengeThe CDC’secological model-based CoordinatedSchool HealthProgram
(++)
Kipping et al.,2014 [31]
AFLY5 South westEngland
60schools2221students4th grade(Age range:8-9 years)
– 1 schoolyear
Teacher trainingProvision of 16lessons & child-parent interactivehomework plansMaterials forlessons andhomework, andwritten materialsfor schoolnewsletters andparents.Social CognitiveTheory
– No effect on thethree primaryoutcomes (PA,sedentary time,diet)Significantfavorable effect onthree out of nineof the secondaryoutcomes, i.e. self-reported timespent in screenviewing at theweekend, self-reported servingsof snacks per day,and servings ofhigh energy drinksper day.(+)
Lawlor et al.,2016 [32]a
– – Significantfavorable effect on3/10 potentialmediators, i.e. fruitand vegetable self-efficacy; child-reported maternallimitation of seden-tary behavior; andknowledge.(+)
Andersonet al., 2016[33]a
– 1 year postintervention
No effect on meanchild-reportedscreen viewing atthe weekend, serv-ings of snacks perday, servings ofhigh-energy drinksper day, servings ofhigh-fat foods perday.(−)
Llargues et al.,2011 [15]
AVall study GranollersSpain
16schools500students1st grade(Age range:5-6 years)
– 2 schoolyears
Educationalsessions topromote healthyeating habits andphysical activityInformation sessionwith the parentsDistribution ofhealthy recipesResearch, Vision,Action andChange (IVAC)methodology
– Significant favorableeffect on BMI andthe prevalence ofoverweight childrenSignificant favorableeffect on theproportion ofchildren that ate asecond piece of fruitSignificant favorableeffect on theconsumption of fish.(+++)
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 9 of 20
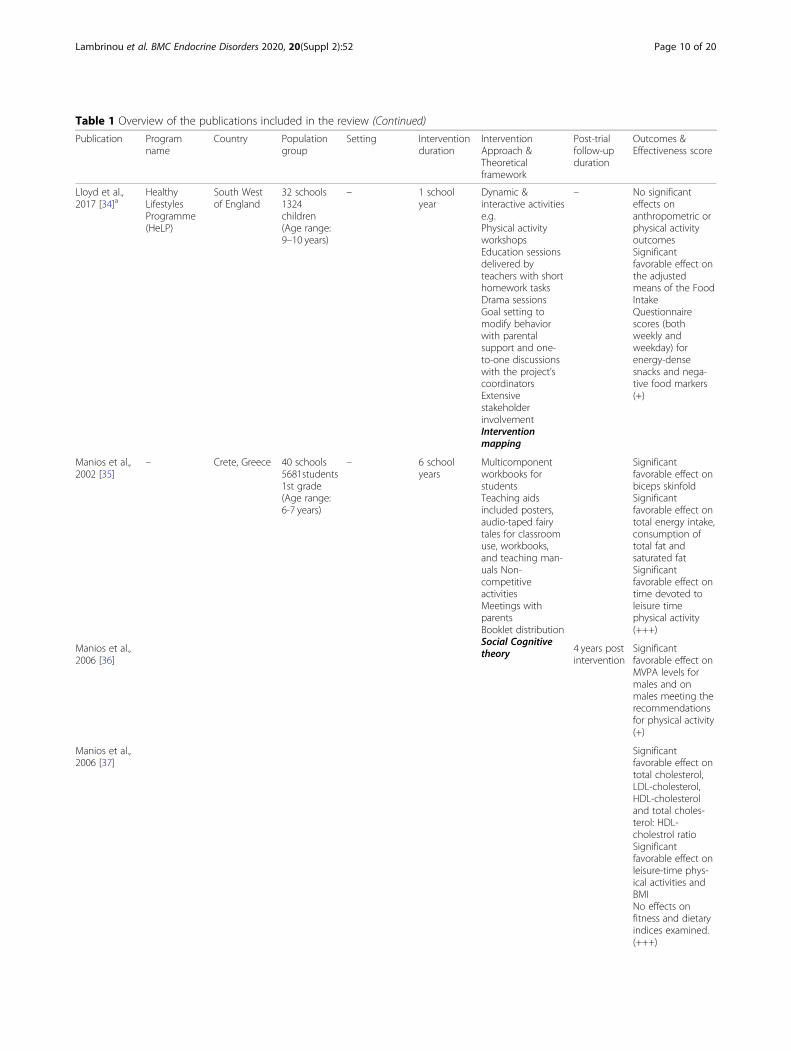
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Lloyd et al.,2017 [34]a
HealthyLifestylesProgramme(HeLP)
South Westof England
32 schools1324children(Age range:9–10 years)
– 1 schoolyear
Dynamic &interactive activitiese.g.Physical activityworkshopsEducation sessionsdelivered byteachers with shorthomework tasksDrama sessionsGoal setting tomodify behaviorwith parentalsupport and one-to-one discussionswith the project’scoordinatorsExtensivestakeholderinvolvementInterventionmapping
– No significanteffects onanthropometric orphysical activityoutcomesSignificantfavorable effect onthe adjustedmeans of the FoodIntakeQuestionnairescores (bothweekly andweekday) forenergy-densesnacks and nega-tive food markers(+)
Manios et al.,2002 [35]
– Crete, Greece 40 schools5681students1st grade(Age range:6-7 years)
– 6 schoolyears
Multicomponentworkbooks forstudentsTeaching aidsincluded posters,audio-taped fairytales for classroomuse, workbooks,and teaching man-uals Non-competitiveactivitiesMeetings withparentsBooklet distributionSocial Cognitivetheory
Significantfavorable effect onbiceps skinfoldSignificantfavorable effect ontotal energy intake,consumption oftotal fat andsaturated fatSignificantfavorable effect ontime devoted toleisure timephysical activity(+++)
Manios et al.,2006 [36]
4 years postintervention
Significantfavorable effect onMVPA levels formales and onmales meeting therecommendationsfor physical activity(+)
Manios et al.,2006 [37]
Significantfavorable effect ontotal cholesterol,LDL-cholesterol,HDL-cholesteroland total choles-terol: HDL-cholestrol ratioSignificantfavorable effect onleisure-time phys-ical activities andBMINo effects onfitness and dietaryindices examined.(+++)
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 10 of 20
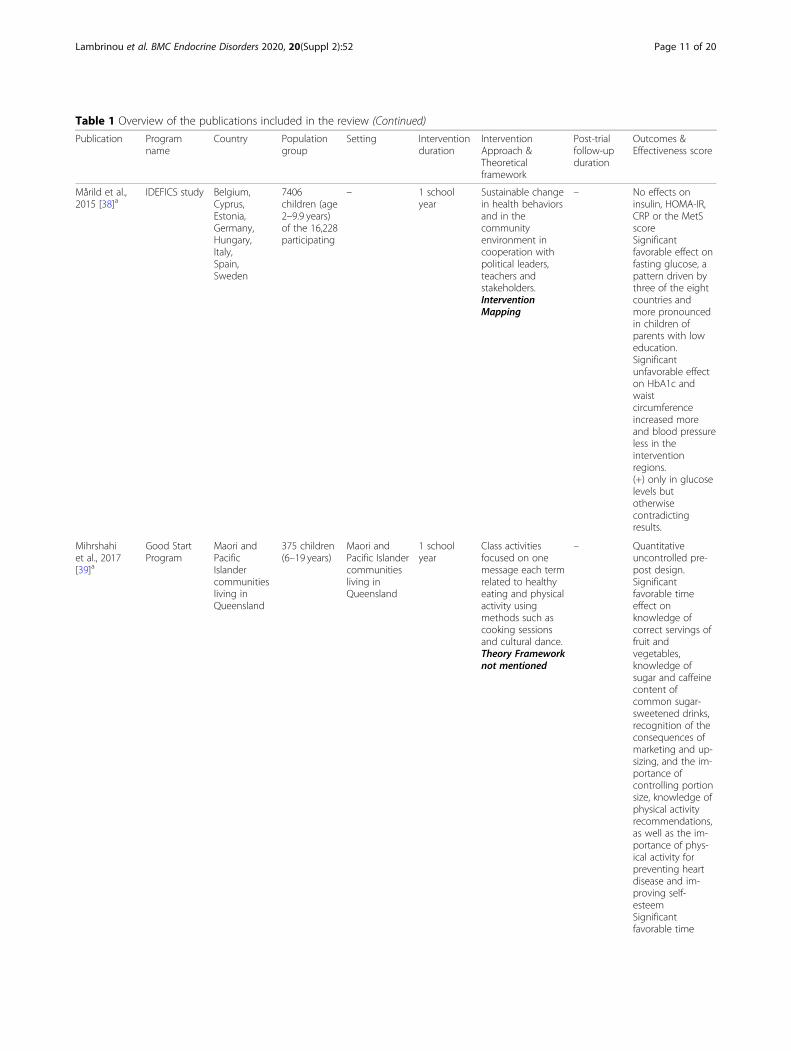
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Mårild et al.,2015 [38]a
IDEFICS study Belgium,Cyprus,Estonia,Germany,Hungary,Italy,Spain,Sweden
7406children (age2–9.9 years)of the 16,228participating
– 1 schoolyear
Sustainable changein health behaviorsand in thecommunityenvironment incooperation withpolitical leaders,teachers andstakeholders.InterventionMapping
– No effects oninsulin, HOMA-IR,CRP or the MetSscoreSignificantfavorable effect onfasting glucose, apattern driven bythree of the eightcountries andmore pronouncedin children ofparents with loweducation.Significantunfavorable effecton HbA1c andwaistcircumferenceincreased moreand blood pressureless in theinterventionregions.(+) only in glucoselevels butotherwisecontradictingresults.
Mihrshahiet al., 2017[39]a
Good StartProgram
Maori andPacificIslandercommunitiesliving inQueensland
375 children(6–19 years)
Maori andPacific Islandercommunitiesliving inQueensland
1 schoolyear
Class activitiesfocused on onemessage each termrelated to healthyeating and physicalactivity usingmethods such ascooking sessionsand cultural dance.Theory Frameworknot mentioned
– Quantitativeuncontrolled pre-post design.Significantfavorable timeeffect onknowledge ofcorrect servings offruit andvegetables,knowledge ofsugar and caffeinecontent ofcommon sugar-sweetened drinks,recognition of theconsequences ofmarketing and up-sizing, and the im-portance ofcontrolling portionsize, knowledge ofphysical activityrecommendations,as well as the im-portance of phys-ical activity forpreventing heartdisease and im-proving self-esteemSignificantfavorable time
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 11 of 20

Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
effect on someattitudes tovegetables andsugar-sweeteneddrinks and the re-ported intake ofvegetables(+)
Pablos et al.,2017 [40]
HealthyHabitsProgram(HHP)
ValencianCommunity,Spain
2 schools158 children(10–12 years)
– 1 schoolyear
Free extracurricularactivity:brief 10-min talkabout healthyhabitsPhysical exercisesession targetingfun, inclusion andcooperation, andsafety (themedgames)All the sessionswere led by thesame specifically-trained teacher.A worksheetdesigned by theresearch team wasgiven to becompleted athome (29 in total)Three 45-min talksfor parents andteachers abouthealthy habits forschool children.Theory Frameworknot mentioned
Significantfavorable effect ontriglycerides, bloodglucose andVO2max, breakfasthabits and qualityof diet, theprevalence ofnormal levels fortotal cholesterol,blood pressure andBMI.(+++)
Plachta-Danielziket al., 2007[41]
KOPS study Kiel, Germany 32schools1764students(Age: 6 years)
– 1 schoolyear
Teachers training ona structured nutritioneducation program.Health messageswere given tochildren, parents,and teachers,conveyed asnutrition fairy tales,interactive games,and by preparing ahealthy breakfast.Six nutrition unitsperformed during 2to 3 weeks withinthe second term ofthe first schoolyear. After eachunit, runninggames wereoffered for 20 minon theschoolyard.Parentswere informedduring a parentalschool meeting.Theory Frameworknot mentioned
4 years postintervention
No effect on meanBMISignificantfavorable effect onthe prevalence ofoverweight andobesity in childrenfrom families withhighsocioeconomicstatus andmarginallysignificant inchildren of normal-weight mothers.(+++) only in high-SES groups.
Plachta-Danielziket al., 2011[42]
8 years postintervention
No effect on meanBMI, lifestyle andblood pressureSignificant favorableeffect on the 8-yearchange in BMI-standard deviationscores (SDS) in highSES groups(+++) only in high-SES groups.
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 12 of 20

Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Rush et al.,2014 [43]a
ProjectEnergize
New Zealand 193 primaryschools4804children(Age range:6-11 years)
42% Māori, theindigenouspeople of NewZealand
Encourage healthybehaviors dailyHealthy choicesavailability anddecrease theavailability of highenergy/ lownutrient foodsIncrease theawareness ofhealthy choicesConsistent nutritionmessages in allaspects of schooland communityinteraction e.g.,healthy fundraisingoptionsEncouragelunchtime physicalactivity at leasttwice a weekRaise awareness ofincidental activityopportunities athome and schoolTheory Frameworknot mentioned
Significantfavorable effect onthe combinedprevalence ofobesity andoverweight andBMI, physicalfitness in bothboys and girls,both indigenousMaori and non-Maori children, andacross SES.(+++)
Sacchettiet al., 2015[44]a
SAMBAproject
Bologna, Italy 11 classes234 schoolchildren(Age range:8-11 years)
– 3 schoolyears
Training modulesfor teachersTraining modulesfor instructors oflocal sport societiesEducationalactivities in classFree and structuredgames inside theschool and in theopen.Cookery workshopsand sensorycourses for parentsand teachers.Moments ofmovement withparents in freetime: homeworkDog walking &Home-schoolroutes on foot/bybikeCreation of didacticmaterials (recipes,leaflets, DVDs, foodpyramids)Precede-ProceedModel
Significantfavorable effect onweight, thepercentage ofchildren whoconsumed anadequate mid-morning snack, thepercentage of chil-dren who con-sumed snacks anddrinks after thedinner and thepercentage ofthose who con-sumed five ormore portions offruits and vegeta-bles daily.(+++)
Sahota et al.,2001 [45]
APPLES Leeds, UK 10 schools634 students(Age range:7-11 years)
– 1 schoolyear
Teacher trainingModification ofschool mealsDevelopment ofschool action plans(Individualized on
– Significantfavorable effect onvegetableconsumptionNo effect onphysical activity or
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 13 of 20
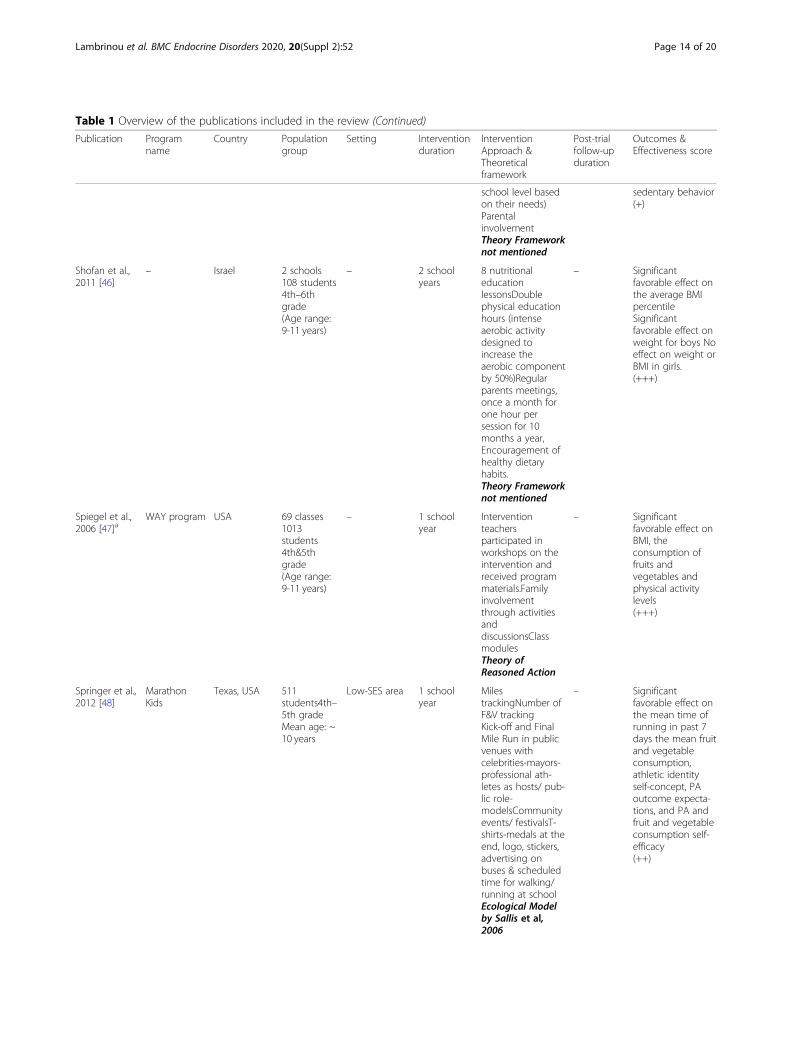
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
school level basedon their needs)ParentalinvolvementTheory Frameworknot mentioned
sedentary behavior(+)
Shofan et al.,2011 [46]
– Israel 2 schools108 students4th–6thgrade(Age range:9-11 years)
– 2 schoolyears
8 nutritionaleducationlessonsDoublephysical educationhours (intenseaerobic activitydesigned toincrease theaerobic componentby 50%)Regularparents meetings,once a month forone hour persession for 10months a year,Encouragement ofhealthy dietaryhabits.Theory Frameworknot mentioned
– Significantfavorable effect onthe average BMIpercentileSignificantfavorable effect onweight for boys Noeffect on weight orBMI in girls.(+++)
Spiegel et al.,2006 [47]a
WAY program USA 69 classes1013students4th&5thgrade(Age range:9-11 years)
– 1 schoolyear
Interventionteachersparticipated inworkshops on theintervention andreceived programmaterials.Familyinvolvementthrough activitiesanddiscussionsClassmodulesTheory ofReasoned Action
– Significantfavorable effect onBMI, theconsumption offruits andvegetables andphysical activitylevels(+++)
Springer et al.,2012 [48]
MarathonKids
Texas, USA 511students4th–5th gradeMean age: ~10 years
Low-SES area 1 schoolyear
MilestrackingNumber ofF&V trackingKick-off and FinalMile Run in publicvenues withcelebrities-mayors-professional ath-letes as hosts/ pub-lic role-modelsCommunityevents/ festivalsT-shirts-medals at theend, logo, stickers,advertising onbuses & scheduledtime for walking/running at schoolEcological Modelby Sallis et al,2006
– Significantfavorable effect onthe mean time ofrunning in past 7days the mean fruitand vegetableconsumption,athletic identityself-concept, PAoutcome expecta-tions, and PA andfruit and vegetableconsumption self-efficacy(++)
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 14 of 20
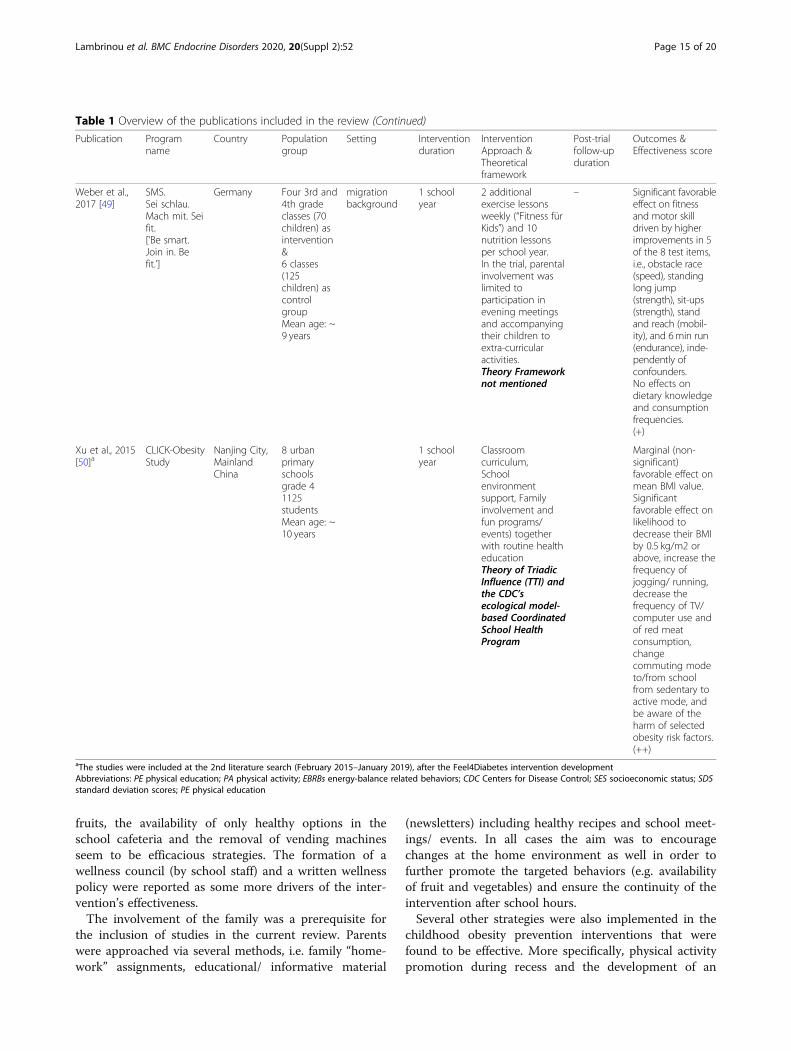
fruits, the availability of only healthy options in theschool cafeteria and the removal of vending machinesseem to be efficacious strategies. The formation of awellness council (by school staff) and a written wellnesspolicy were reported as some more drivers of the inter-vention’s effectiveness.The involvement of the family was a prerequisite for
the inclusion of studies in the current review. Parentswere approached via several methods, i.e. family “home-work” assignments, educational/ informative material
(newsletters) including healthy recipes and school meet-ings/ events. In all cases the aim was to encouragechanges at the home environment as well in order tofurther promote the targeted behaviors (e.g. availabilityof fruit and vegetables) and ensure the continuity of theintervention after school hours.Several other strategies were also implemented in the
childhood obesity prevention interventions that werefound to be effective. More specifically, physical activitypromotion during recess and the development of an
Table 1 Overview of the publications included in the review (Continued)
Publication Programname
Country Populationgroup
Setting Interventionduration
InterventionApproach &Theoreticalframework
Post-trialfollow-upduration
Outcomes &Effectiveness score
Weber et al.,2017 [49]
SMS.Sei schlau.Mach mit. Seifit.[‘Be smart.Join in. Befit.’]
Germany Four 3rd and4th gradeclasses (70children) asintervention&6 classes(125children) ascontrolgroupMean age: ~9 years
migrationbackground
1 schoolyear
2 additionalexercise lessonsweekly (“Fitness fürKids”) and 10nutrition lessonsper school year.In the trial, parentalinvolvement waslimited toparticipation inevening meetingsand accompanyingtheir children toextra-curricularactivities.Theory Frameworknot mentioned
– Significant favorableeffect on fitnessand motor skilldriven by higherimprovements in 5of the 8 test items,i.e., obstacle race(speed), standinglong jump(strength), sit-ups(strength), standand reach (mobil-ity), and 6min run(endurance), inde-pendently ofconfounders.No effects ondietary knowledgeand consumptionfrequencies.(+)
Xu et al., 2015[50]a
CLICK-ObesityStudy
Nanjing City,MainlandChina
8 urbanprimaryschoolsgrade 41125studentsMean age: ~10 years
1 schoolyear
Classroomcurriculum,Schoolenvironmentsupport, Familyinvolvement andfun programs/events) togetherwith routine healtheducationTheory of TriadicInfluence (TTI) andthe CDC’secological model-based CoordinatedSchool HealthProgram
Marginal (non-significant)favorable effect onmean BMI value.Significantfavorable effect onlikelihood todecrease their BMIby 0.5 kg/m2 orabove, increase thefrequency ofjogging/ running,decrease thefrequency of TV/computer use andof red meatconsumption,changecommuting modeto/from schoolfrom sedentary toactive mode, andbe aware of theharm of selectedobesity risk factors.(++)
aThe studies were included at the 2nd literature search (February 2015–January 2019), after the Feel4Diabetes intervention developmentAbbreviations: PE physical education; PA physical activity; EBRBs energy-balance related behaviors; CDC Centers for Disease Control; SES socioeconomic status; SDSstandard deviation scores; PE physical education
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 15 of 20

active playground as well as non-competitive, enjoyableactivities, promoting whole class participation duringphysical education (PE) classes and the provision ofadditional hours to physical activity were shown to beeffective strategies. Motivational incentives (e.g. stickers,t-shirts) as well as social marketing techniques targetingchildren, e.g. slogans, characters, raffle tickets have alsobeen shown to contribute to effectiveness of the inter-ventions. The collaboration with community stake-holders, local community and school policy and mediain every aspect of a health promotion project targetingphysical activity, healthier diet or both has been alsohighlighted as an important contributor to the imple-mentation fidelity, and thus effectiveness, of the inter-vention, also providing the basis for a sustainableapproach.Regarding intervention programs delivered in vulner-
able groups and/ or low-SES areas, effective strategiesfocused on school policy and environmental changes,parental engagement, incentives and interactive activitiessuch as cooking lessons and cultural dance classes, withless emphasis given on the educational part of the inter-vention. Furthermore, an intervention program particu-larly targeting Jewish population offered genderseparated physical activity classes for pupils, adaptingthe intervention to the needs of the specific populationgroup thus increasing adherence and effectiveness of theintervention.
Theoretical frameworksVarious behavioral theories, models and frameworkshave been utilized for the development of the studiedschool-based interventions. More specifically: the SocialCognitive Theory, the Theory of Planned Behavior, theTheory of Reasoned Action, the Ecological model, theSocial-Ecological model, the Coordinated School HealthProgram model developed by the Centers for DiseaseControl and Prevention (CDC), Social Marketing, Inter-vention Mapping, the Precede-Proceed Model, as well asthe Research, Vision, Action and Change methodologyor a combination of the above were used as the theoret-ical basis for interventions’ development. On the otherhand, about half of the projects (11 out of 27) did notmention whether their intervention was based on a the-oretical model. Based on the current review, the most ef-fective theories used in the development of healthpromotion programs in the school setting are the SocialCognitive Theory and the CDC’s ecological model-basedCoordinated School Health Program which is commonlyused in the US.
DiscussionThe current review aimed to gather and evaluate avail-able school-based, family-involved obesity prevention
interventions targeting dietary, physical activity and sed-entary behaviors among primary schoolchildren andtheir families. Moreover, it aimed to identify the most ef-fective strategies in improving those EBRBs and tacklingobesity in primary school-aged children with special em-phasis given on low-SES and vulnerable groups.Previous reviews on the same field were used as a basis
for the current review and the inclusion criteria applied[18, 22, 24]. In order to avoid repetition of alreadyproven to be effective strategies and in order to extractnew meaningful results from the existing literature, thecurrent review goes one step further in the identificationof effective strategies by incorporating those alreadyknown to be effective as inclusion criteria. From thetotal number of studies selected 27 intervention studies(33 publications) fulfilled the inclusion criteria and wereincluded in the current analysis.As previously described, primary schools seem to be
the ideal setting for childhood obesity prevention inter-ventions since it offers many opportunities for physicalactivity promotion and nutrition education and reduc-tion of sedentary behavior through practice, policy, anda supportive environment [18]. This approach requiresthe active involvement and participation of teachers.Since schools mainly focus on academic achievement,many teachers find it difficult to include extracurricularmodules into the already tight schedule. Furthermore,not all teachers are willing to act as champions for ahealth promotion intervention, especially if their ownlifestyle habits do not follow/ agree with the healthy life-style messages delivered via the intervention [25]. Strongengagement by the school headmaster/ leadership is cru-cial in order to achieve engagement of families andteachers [26] and ensure the delivery of the interventionwith the highest possible fidelity and thus, effectivenessas well as teachers’ behavior as role-models.Parental influence on children‘s nutrition and physical
activity habits is a well-known determinant of childhoodobesity [27]. Based on research indicating that the in-volvement of parents in addressing nutrition, physicalactivity and sedentary behavior in children is essential,the current review only included interventions that in-volved parents [18, 22]. Several effective strategies suchas including parents via family “homework” assignments,educational/ informative material (newsletters) andschool meetings/ events have been used to involve par-ents in the intervention. Meetings with parents at schoolseemed to lead to increased effectiveness in more casesin comparison to written material, i.e. newsletters.Given that vulnerable groups and/ or people living in
low-SES areas are more likely to be overweight or obese,have poorer health outcomes, and tend to benefit lessfrom interventions in comparison with their counter-parts from more affluent backgrounds, both developed
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 16 of 20

and developing countries should also target low-income,high-risk groups [28]. Tailoring interventions to fit theneeds of a specific population group, as done in the studyby Benjamins et al. where gender separated physical activ-ity classes were offered for Jewish pupils, has been shownto be imperative for the intervention’s acceptability and ef-fectiveness [28]. A thorough situational analysis and for-mative research should be included in the time planningfor the development of interventions, especially when tar-geting schools in low-SES areas and vulnerable groups[28]. The results of the current review are in agreementwith previous work highlighting that intervention pro-grams delivered in vulnerable groups and/ or low-SESareas should focus on school policy and environmentalchanges and interactive activities with less emphasis onthe educational part of the intervention [28, 29].Using a solid theoretical framework as a basis in an in-
tervention’s design is vital to its chances of success, as evi-dence suggests that such interventions are more effectivecompared to those that are not based on a theory [30].Various theoretical frameworks have been utilized by theincluded interventions, while almost half of the projectsdid not mention the use of a theoretical model, a fact thatmight have limited their effectiveness. CDC’s ecologicalmodel-based Coordinated School Health Program whichis commonly used in the US was one of the two morepopular theories used in the development of health pro-motion programs in the current review. Its significant ef-fect might derive from the fact that among several targetsand in contrast to most frameworks it also aims at im-proving employee wellness. This characteristic might havemade a difference for its popularity and effectiveness. Onethe other hand, the Social Cognitive Theory is a com-monly used basis for interventions design. In the currentreview, even though it was popular in the current review,its effectiveness varied. Last but not least, integrating pol-icies and/ or environmental changes, such as increasedavailability and accessibility of healthy choices and re-moval of unhealthy choices but also the collaboration withcommunity stakeholders, have been shown to be a highimpact intervention strategies [31, 32], especially whentargeting lower SES groups.Several outcomes have been considered to assess the in-
terventions’ effectiveness in various studies. Both behav-iors and clinical outcomes where considered in theincluded studies, however the interventions did not alwayssucceed in having an effect on clinical outcomes. Themost commonly used and assessed behavioral outcomewas the consumption of fruits and vegetables and manyinterventions succeeded in increasing their consumptionfollowed by physical activity, which proved to be more dif-ficult for the interventions to significantly improve. Onthe other hand, BMI was the most commonly used clinicaloutcome assessed. Several interventions succeeded in
improving BMI, while some that did not showed an effecton other important adiposity measures, i.e. waist circum-ference of skinfold thickness. Still, having a significant ef-fect on clinical outcomes is not always feasible even inwell-designed interventions, especially in this age group.
Strengths and limitationsThe results of the current work should be interpreted inconsideration of the study’s strengths and limitations. Inthe current review studies in languages other than Englishwere omitted, which could limit the generalization of theresults in other countries, especially low-to-middle incomecountries (LMICs). Studies without published outcomeswere excluded as it was not possible to evaluate their effi-cacy. Although the benefits of single health behaviorchange interventions vs. multiple health behavior changeinterventions remain unclear [33], the present review onlyincluded interventions targeting dietary, physical activityand sedentary behaviors simultaneously. On the otherhand, the current review goes beyond the existing litera-ture by applying specific inclusion criteria that have beenlinked to increased effectiveness and thus, focusing on themost effective programs to extract the best interventionstrategies, contributing to the updating of the literature.
ConclusionsSchool-based interventions are vital in the prevention ofthe globally rising childhood obesity. Many interventionshave shown promising results, which were supported bya number of effective and high-impact strategies. Mul-tiple strategies are used in effective interventions,highlighting the fact that a one-size-fits-all approach isnot applicable in childhood obesity prevention interven-tion programs development and that many differentstrategies can be effective. However, future school-basedobesity prevention interventions should build on alreadysuccessful intervention strategies while also addressingand integrating culture specific strategies. Includinglong-term follow-up measurements to assess the efficacyof school-based interventions will facilitate the identifi-cation of the most effective strategies in the long-term.Further studies are needed to elucidate the effectiveness
of specific strategies aiming at long duration interventions.Both the development and the implementation method-ology of the research, as well as the barriers, challengesand possible facilitators should be encouraged to be thor-oughly recorded and published in order to inform the sci-entific community on the feasibility and sustainability ofimplementing interventions in real life situations.
Recommendations for future school-based obesityprevention interventionsApart from the already mentioned recommendationsthat have been used as inclusion criteria in the present
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 17 of 20
review, several strategies have been proven efficacious,i.e.:
� The use of a suitable theoretical framework shouldbe considered in the intervention design
� Interventions should be adapted to the needs of thetargeted population group(s)
� Collaboration with community stakeholders, localpolicy and media should be targeted in order toincrease intervention’s acceptability andsustainability
� School teachers should act as role-models and getactively involved in all targeted behaviors
� The teaching staff and school personnel shouldpromote the availability and accessibility of healthysnacks and water and monitor the provision only ofhealthy food options by the school cafeteria/canteenand attend to the removal of unhealthy choices andvending machines, if any
� Schools should be encouraged to form a wellnesscouncil (school staff and/or parents’ association) andwrite a wellness policy
� Families should be targeted via educational/informative material (newsletters), family“homework” assignments or school meetings/ eventsfor the children and their families in order to changethe home environment to promote the targetedbehaviors (e.g. availability of fruit and vegetable, aswell as other healthy food items/snacks)
� School yards should be accessible after school hoursand physical activity during recess should bepromoted
� PE-instructor/school teachers should develop andpromote non-competitive, enjoyable activities, pro-moting whole class participation
� Social marketing techniques, interactive activitiesand motivational incentives can be utilized forchildren.
� In low-SES areas or in migrant population groups,interventions should focus on school policy and en-vironmental changes, parental engagement andinteractive team activities, rather than the educa-tional part of the intervention.
Supplementary informationSupplementary information accompanies this paper at https://doi.org/10.1186/s12902-020-0526-5.
Additional file 1: Table 1 PICO keywords.
AbbreviationsBMI: Body mass index; CDC: Centers for Disease Control and Prevention;EBRBs: Energy balance related behaviors; HICs: High Income Countries;LMICs: Low-to-Middle Income Countries; SES: Socio-economic status;PE: Physical education
AcknowledgementsThe authors would like to thank the members of the Feel4Diabetes-studygroup: Coordinator: Yannis Manios Steering Committee: Yannis Manios,Greet Cardon, Jaana Lindström, Peter Schwarz, Konstantinos Makrilakis, LievenAnnemans, Ignacio Garamendi Harokopio University (Greece) Yannis Man-ios, Kalliopi Karatzi, Odysseas Androutsos, George Moschonis, Spyridon Kanel-lakis, Christina Mavrogianni, Konstantina Tsoutsoulopoulou, ChristinaKatsarou, Eva Karaglani, Irini Qira, Efstathios Skoufas, Konstantina Maragko-poulou, Antigone Tsiafitsa, Irini Sotiropoulou, Michalis Tsolakos, Effie Argyri,Mary Nikolaou, Eleni-Anna Vampouli, Christina Filippou, Kyriaki Apergi, AmaliaFilippou, Gatsiou Katerina, Efstratios Dimitriadis National Institute for Healthand Welfare (Finland) Jaana Lindström, Tiina Laatikainen, Katja Wikström,Petteri Hovi, Jemina Kivelä, Päivi Valve, Esko Levälahti, Eeva Virtanen GhentUniversity (Belgium) Department of Movement and Sports Sciences: Greet Car-don, Vicky Van Stappen, Nele Huys Department of Public Health: Lieven Anne-mans, Ruben Willems Department of Endocrinology and Metabolic Diseases:Samyah Shadid Technische Universität Dresden (Germany) Peter Schwarz,Patrick Timpel University of Athens (Greece) Konstantinos Makrilakis, StavrosLiatis, George Dafoulas, Christina-Paulina Lambrinou, Angeliki GiannopoulouInternational Diabetes Federation European Region (Belgium) Lala Rabe-mananjara, Maria Stella de Sabata, Winne Ko, Ignacio Garamendi UniversidadDe Zaragoza (Spain) Luis Moreno, Fernando Civeira, Gloria Bueno, Pilar DeMiguel-Etayo, Esther Mª Gonzalez-Gil, María L. Miguel-Berges, Natalia Gimé-nez-Legarre; Paloma Flores-Barrantes, Aleli M. Ayala-Marín, Miguel Seral-Cortés, Lucia Baila-Rueda, Ana Cenarro, Estíbaliz Jarauta, Rocío Mateo-GallegoMedical University of Varna (Bulgaria) Violeta Iotova, Tsvetalina Tankova,Natalia Usheva, Kaloyan Tsochev, Nevena Chakarova, Sonya Galcheva,Rumyana Dimova, Yana Bocheva, Zhaneta Radkova, Vanya Marinova, YuliyaBazdarska, Tanya Stefanova University of Debrecen (Hungary) Imre Rurik,Timea Ungvari, Zoltán Jancsó, Anna Nánási, László Kolozsvári, Csilla Semá-nova, Éva Bíró, Emese Antal, Sándorné Radó Extensive Life Oy (Finland)Remberto Martinez, Marcos Tong.
About this supplementThis article has been published as part of BMC Endocrine Disorders, Volume20 Supplement 2, 2020: Designing, implementing and evaluating acommunity-based intervention to prevent diabetes in vulnerable familiesacross Europe. The Feel4Diabetes-study. The full contents of the supplementare available at https://bmcendocrdisord.biomedcentral.com/articles/supplements/volume-20-supplement-2.
Authors’ contributionsCPL and OA constructed the search strategy for review and they also readand selected articles. CPL, OA, EK (HUA) and YM wrote the first draft of themanuscript. GC, NH, KW, JK, WK, EK (IDFE), KT, VI, RD, DMEP, GGEM, HT, ZJ, SLand KM critically revised the manuscript and read and approved the finalmanuscript.
FundingThe Feel4Diabetes-study has received funding from the European Union’sHorizon 2020 research and innovation programme [Grant Agreement: n°643708]. The content of this article reflects only the authors’ views and theEuropean Community is not liable for any use that may be made of the in-formation contained therein.
Availability of data and materialsNot applicable.
Ethics approval and consent to participateThis study was conducted according to the guidelines laid down in theDeclaration of Helsinki and all procedures involving human subjects wereapproved by the ethics committees in all countries (in Belgium, by theMedical Ethics Committee of the Ghent University Hospital; in Bulgaria, bythe Ethics Committee of the Medical University of Varna; in Finland, by thehospital district of Southwest Finland ethical committee; in Greece, by theBioethics Committee of Harokopio University; in Hungary, by the NationalCommittee for Scientific Research in Medicine; in Spain, by the ClinicalResearch Ethics Committee).
Consent for publicationNot applicable.
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 18 of 20
Competing interestsTwo co-authors are members of the editorial board (Associate Editor - Odys-seas Androutsos, Section Editor- Stavros Liatis) of this journal. The authors de-clare that they have no further competing interests.
Author details1Department of Nutrition and Dietetics, School of Health Science andEducation, Harokopio University, 70 El Venizelou Ave, 176 71 Kallithea,Athens, Greece. 2Department of Nutrition and Dietetics, School of PhysicalEducation, Sport Science and Dietetics, University of Thessaly, Trikala, Greece.3Department of Movement and Sports Sciences, Faculty of Medicine andHealth Sciences, Ghent University, Ghent, Belgium. 4Department of PublicHealth Solutions, National Institute for Health and Welfare, Helsinki, Finland.5International Diabetes Federation European Region, Brussels, Belgium.6Department of Pediatrics, Medical University Varna, Varna, Bulgaria.7Department of Diabetology, Clinical Center of Endocrinology, MedicalUniversity Sofia, Sofia, Bulgaria. 8Growth, Exercise, NUtrition andDevelopment (GENUD) Research Group. Instituto Agroalimentario de Aragón(IA2), Instituto de Investigación Sanitaria Aragón (IIS Aragón), University ofZaragoza, Zaragoza, Spain. 9Centro de Investigación Biomédica en Red deFisiopatología de la Obesidad y Nutrición (CIBERObn), University of Zaragoza,Zaragoza, Spain. 10Institute of Nutrition and Food Technology. Departmentof Biochemistry and Molecular Biology II, Center of Biomedical Research,University of Granada, Granada, Spain. 11University of Debrecen, Departmentof Family and Occupational Medicine, Debrecen, Hungary. 12National andKapodistrian University of Athens, Athens, Greece.
Received: 14 March 2020 Accepted: 23 March 2020Published: 6 May 2020
References1. Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in
public health. Obes Rev. 2004;5:4–85.2. Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high
body mass index in US children and adolescents, 2007-2008. Jama. 2010;303(3):242–9.
3. Hales CM, Fryar CD, Carroll MD, Freedman DS, Ogden CL. Trends in obesityand severe obesity prevalence in us youth and adults by sex and age, 2007-2008 to 2015-2016. JAMA. 2018;319(16):1723–5.
4. Jackson-Leach R, Lobstein T. Estimated burden of paediatric obesity and co-morbidities in Europe. Part 1. The increase in the prevalence of child obesityin Europe is itself increasing. Int J Pediatr Obes. 2006;1(1):26–32.
5. Manios Y, Androutsos O, Katsarou C, Vampouli EA, Kulaga Z, Gurzkowska B,et al. Prevalence and sociodemographic correlates of overweight andobesity in a large Pan-European cohort of preschool children and theirfamilies: the ToyBox study. Nutrition. 2018;55–56:192–8.
6. Blundell JE, Baker JL, Boyland E, Blaak E, Charzewska J, de Henauw S, et al.Variations in the prevalence of obesity among European countries, and aconsideration of possible causes. Obesity Facts. 2017;10(1):25–37.
7. Ezzati M, Lopez AD, Rodgers A, Murray CJ. Comparative quantification ofhealth risks: global and regional burden of disease attributable to selectedmajor risk factors: OMS; 2004.
8. Fund WCR, Research AIfC. Food, nutrition, physical activity, and theprevention of cancer: a global perspective: Amer Inst for Cancer research;2007.
9. Organization WH. Global status report on noncommunicable diseases 2010.Geneva: World Health Organization; 2011.
10. Organization WH, Canada PHAo, Canada CPHAo. Preventing chronicdiseases: a vital investment: World Health Organization; 2005.
11. Olstad DL, McCargar L. Prevention of overweight and obesity in childrenunder the age of 6 years. Appl Physiol Nutr Metab. 2009;34(4):551–70.
12. Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH. Predicting obesity inyoung adulthood from childhood and parental obesity. N Engl J Med. 1997;337(13):869–73.
13. Parsons TJ, Power C, Logan S, Summerbell CD. Childhood predictors ofadult obesity: a systematic review. Int J Obes Relat Metab Disord. 1999;23(Suppl 8):S1–107.
14. Singh AS, Mulder C, Twisk JW, van Mechelen W, Chinapaw MJ. Tracking ofchildhood overweight into adulthood: a systematic review of the literature.Obes Rev. 2008;9(5):474–88.
15. Evensen E, Wilsgaard T, Furberg A-S, Skeie G. Tracking of overweight andobesity from early childhood to adolescence in a population-based cohort -the Tromsø Study, Fit Futures. BMC Pediatr. 2016;16:64.
16. Pandita A, Sharma D, Pandita D, Pawar S, Tariq M, Kaul A. Childhood obesity:prevention is better than cure. Diabetes Metab Syndr Obes. 2016;9:83–9.
17. Pyle SA, Sharkey J, Yetter G, Felix E, Furlong MJ, Poston WSC. Fighting anepidemic: the role of schools in reducing childhood obesity. Psychol Sch.2006;43(3):361–76.
18. Khambalia AZ, Dickinson S, Hardy LL, Gill T, Baur LA. A synthesis of existingsystematic reviews and meta-analyses of school-based behaviouralinterventions for controlling and preventing obesity. Obes Rev. 2012;13(3):214–33.
19. Manios Y, Androutsos O, Lambrinou CP, Cardon G, Lindstrom J, AnnemansL, et al. A school- and community-based intervention to promote healthylifestyle and prevent type 2 diabetes in vulnerable families across Europe:design and implementation of the Feel4Diabetes-study. Public Health Nutr.2018;21(17):3281–90.
20. Wang Y, Lobstein T. Worldwide trends in childhood overweight andobesity. Int J Pediatr Obes. 2006;1(1):11–25.
21. Agardh E, Allebeck P, Hallqvist J, Moradi T, Sidorchuk A. Type 2 diabetesincidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol. 2011;40(3):804–18.
22. Sharma M. Dietary education in school-based childhood obesity preventionprograms. Adv Nutr. 2011;2(2):207S–16S.
23. Neil Fantom HF, William C. Prince. 2014. Available from: https://blogs.worldbank.org/opendata/lics-lmics-umics-and-hics-classifying-economies-analytical-purposes.
24. Nixon CA, Moore HJ, Douthwaite W, Gibson EL, Vogele C, Kreichauf S, et al.Identifying effective behavioural models and behaviour change strategiesunderpinning preschool- and school-based obesity prevention interventionsaimed at 4-6-year-olds: a systematic review. Obes Rev. 2012;13(Suppl 1):106–17.
25. Jago R, Rawlins E, Kipping RR, Wells S, Chittleborough C, Peters TJ, et al.Lessons learned from the AFLY5 RCT process evaluation: implications forthe design of physical activity and nutrition interventions in schools. BMCPublic Health. 2015;15:946.
26. Blaine RE, Franckle RL, Ganter C, Falbe J, Giles C, Criss S, et al. Using school staffmembers to implement a childhood obesity prevention intervention in low-income school districts: the Massachusetts childhood obesity researchdemonstration (MA-CORD project), 2012-2014. Prev Chronic Dis. 2017;14:E03.
27. Budd GM, Hayman LL. Childhood obesity: determinants, prevention, andtreatment. J Cardiovasc Nurs. 2006;21(6):437–41.
28. Coupe N, Cotterill S, Peters S. Tailoring lifestyle interventions to low socio-economic populations: a qualitative study. BMC Public Health. 2018;18(1):967.
29. Ickes MJ, McMullen J, Haider T, Sharma M. Global school-based childhoodobesity interventions: a review. Int J Environ Res Public Health. 2014;11(9):8940–61.
30. Sharma M. International school-based interventions for preventing obesityin children. Obes Rev. 2007;8(2):155–67.
31. Lloyd J, Creanor S, Logan S, Green C, Dean SG, Hillsdon M, et al.Effectiveness of the healthy lifestyles Programme (HeLP) to prevent obesityin UK primary-school children: a cluster randomised controlled trial. LancetChild Adolesc Health. 2018;2(1):35–45.
32. Marild S, Russo P, Veidebaum T, Tornaritis M, De Henauw S, DeBourdeaudhuij I, et al. Impact of a community based health-promotionprogramme in 2- to 9-year-old children in Europe on markers of themetabolic syndrome, the IDEFICS study. Obes Rev. 2015;16(Suppl 2):41–56.
33. James E, Freund M, Booth A, Duncan MJ, Johnson N, Short CE, et al.Comparative efficacy of simultaneous versus sequential multiple healthbehavior change interventions among adults: a systematic review ofrandomised trials. Prev Med. 2016;89:211–23.
34. Lloyd J, Creanor S, Logan S, Green C, Dean SG, Hillsdon M, et al.Effectiveness of the Healthy Lifestyles Programme (HeLP) to prevent obesityin UK primary-school children: a cluster randomised controlled trial. LancetChild Adolesc Health. 2018;2(1):35-45.
35. Manios Y, Moschandreas J, Hatzis C, Kafatos A. Health and nutritioneducation in primary schools of Crete: changes in chronic disease riskfactors following a 6-year intervention programme. Br J Nutr. 2002;88(3):315-24.
36. Manios Y, Kafatos I, Kafatos A. Ten-year follow-up of the Cretan Health andNutrition Education Program on children's physical activity levels. Prev Med.2006;43(6):442-6.
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 19 of 20

37. Manios Y, Kafatos A. Health and nutrition education in primary schools inCrete: 10 years follow-up of serum lipids, physical activity andmacronutrient intake. Br J Nutr. 2006;95(3):568-75.
38. Marild S, Russo P, Veidebaum T, Tornaritis M, De Henauw S, DeBourdeaudhuij I, et al. Impact of a community based health-promotionprogramme in 2- to 9-year-old children in Europe on markers of themetabolic syndrome, the IDEFICS study. Obes Rev. 2015;16(Suppl 2):41-56.
39. Mihrshahi S, Vaughan L, Fa'avale N, De Silva Weliange S, Manu-Sione I,Schubert L. Evaluation of the Good Start Program: a healthy eating andphysical activity intervention for Maori and Pacific Islander children living inQueensland, Australia. BMC Publ Health. 2017;17(1):77.
40. Pablos A, Nebot V, Vano-Vicent V, Ceca D, Elvira L. Effectiveness of a school-based program focusing on diet and health habits taught through physicalexercise. Appl Physiol Nutr Metab. 2018;43(4):331-7.
41. Plachta-Danielzik S, Pust S, Asbeck I, Czerwinski-Mast M, Langnase K, FischerC, et al. Four-year follow-up of school-based intervention on overweightchildren: the KOPS study. Obesity (Silver Spring, Md). 2007;15(12):3159-69.
42. Plachta-Danielzik S, Landsberg B, Lange D, Seiberl J, Muller MJ. Eight-yearfollow-up of school-based intervention on childhood overweight--the KielObesity Prevention Study. Obes Facts. 2011;4(1):35-43.
43. Rush E, McLennan S, Obolonkin V, Vandal AC, Hamlin M, Simmons D, et al.Project Energize: whole-region primary school nutrition and physical activityprogramme; evaluation of body size and fitness 5 years after therandomised controlled trial. Br J Nutr. 2014;111(2):363-71.
44. Sacchetti R, Dallolio L, Musti MA, Guberti E, Garulli A, Beltrami P, et al. Effectsof a school based intervention to promote healthy habits in children 8-11years old, living in the lowland area of Bologna Local Health Unit. Ann Ig.2015;27(2):432-46.
45. Sahota P, Rudolf MC, Dixey R, Hill AJ, Barth JH, Cade J. Randomisedcontrolled trial of primary school based intervention to reduce risk factorsfor obesity. BMJ (Clinical research ed). 2001;323(7320):1029-32.
46. Shofan Y, Kedar O, Branski D, Berry E, Wilschanski M. A school-basedprogram of physical activity may prevent obesity. Eur J Clin Nutr. 2011;65(6):768-70.
47. Spiegel SA, Foulk D. Reducing overweight through a multidisciplinaryschool-based intervention. Obesity (Silver Spring, Md). 2006;14(1):88-96.
48. Springer AE, Kelder SH, Ranjit N, Hochberg-Garrett H, Crow S, Delk J.Promoting physical activity and fruit and vegetable consumption through acommunity-school partnership: the effects of Marathon Kids(R) on low-income elementary school children in Texas. J Phys Act Health. 2012;9(5):739-53.
49. Weber KS, Sporkel O, Mertens M, Freese A, Strassburger K, Kemper B, et al.Positive Effects of Promoting Physical Activity and Balanced Diets in aPrimary School Setting with a High Proportion of Migrant School Children.Exp Clin Endocrinol Diabetes. 2017;125(8):554-62.
50. Xu F, Ware RS, Leslie E, Tse LA, Wang Z, Li J, et al. Effectiveness of aRandomized Controlled Lifestyle Intervention to Prevent Obesity amongChinese Primary School Students: CLICK-Obesity Study. PloS One. 2015;10(10):e0141421.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Lambrinou et al. BMC Endocrine Disorders 2020, 20(Suppl 2):52 Page 20 of 20