effectiveness of lifestyle interventions in ... -...
TRANSCRIPT

Effectiveness of Lifestyle Interventions in ChildObesity: Systematic Review With Meta-analysis
abstractBACKGROUND AND OBJECTIVES: The effects of lifestyle interventionson cardio-metabolic outcomes in overweight children have not beenreviewed systematically. The objective of the study was to examine theimpact of lifestyle interventions incorporating a dietary component onboth weight change and cardio-metabolic risks in overweight/obesechildren.
METHODS: English-language articles from 1975 to 2010, available from7 databases, were used as data sources. Two independent reviewersassessed articles against the following eligibility criteria: randomizedcontrolled trial, participants overweight/obese and#18 years, comparinglifestyle interventions to no treatment/wait-list control, usual care, orwritten education materials. Study quality was critically appraised by 2reviewers using established criteria; Review Manager 5.1 was used formeta-analyses.
RESULTS: Of 38 eligible studies, 33 had complete data for meta-analysison weight change; 15 reported serum lipids, fasting insulin, or bloodpressure. Lifestyle interventions produced significant weight losscompared with no-treatment control conditions: BMI (21.25kg/m2, 95%confidence interval [CI] 22.18 to 20.32) and BMI z score (20.10, 95% CI20.18 to 20.02). Studies comparing lifestyle interventions to usual carealso resulted in significant immediate (21.30kg/m2, 95% CI 21.58 to21.03) and posttreatment effects (20.92 kg/m2, 95% CI21.31 to20.54)on BMI up to 1 year from baseline. Lifestyle interventions led tosignificant improvements in low-density lipoprotein cholesterol (20.30mmol/L, 95% CI 20.45 to 20.15), triglycerides (20.15 mmol/L, 95% CI20.24 to 20.07), fasting insulin (255.1 pmol/L, 95% CI 271.2 to 239.1)and blood pressure up to 1 year from baseline. No differences werefound for high-density lipoprotein cholesterol.
CONCLUSIONS: Lifestyle interventions can lead to improvements inweight and cardio-metabolic outcomes. Further research is neededto determine the optimal length, intensity, and long-term effectivenessof lifestyle interventions. Pediatrics 2012;130:e1647–e1671
AUTHORS: Mandy Ho, MSc, APD, RN,a,b Sarah P. Garnett,PhD, RNutr, APD,a,b,c Louise Baur, MBBS, PhD, FRACP,a,c
Tracy Burrows, PhD, AdvAPD,d Laura Stewart, PhD, RD,RNutr,e,f Melinda Neve, PhD, APD,d and Clare Collins, PhD,FDAAd
aThe Children’s Hospital at Westmead Clinical School, Universityof Sydney, Sydney, Australia; bInstitute of Endocrinology andDiabetes, and cKids Research Institute, The Children’s Hospital atWestmead, Westmead, Australia; dPriority Research Centre inPhysical Activity and Nutrition, School of Health Sciences, Facultyof Health, University of Newcastle, Newcastle, Australia;ePaediatric Overweight Service Tayside, Perth Royal Infirmary,Perth, United Kingdom; and fThe Children’s Weight Clinic,Edinburgh, United Kingdom
KEY WORDSchild, adolescent, lifestyle interventions, obesity, weight loss,cardio-metabolic risks, systematic review
ABBREVIATIONSCI—confidence intervalHDL—high-density lipoproteinHOMA-IR—homeostasis model assessment of insulin resistanceLDL—low-density lipoproteinWMD—weighted mean difference
All authors were involved in study conception and design,interpretation of data, critical revision, and final approval of thesubmitted manuscript; Ms Ho was involved in qualityassessment, data extraction, data analysis, and manuscriptpreparation; Prof Collins, Dr Baur, and Dr Garnett were involvedin quality assessment, data extraction and study supervision;and Drs Burrow and Steward were involved in qualityassessment and data extraction.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-1176
doi:10.1542/peds.2012-1176
Accepted for publication Aug 7, 2012
Address correspondence to Ms Mandy Ho, Institute ofEndocrinology and Diabetes, The Children’s Hospital at Westmead,Locked Bag 4001, Westmead, NSW 2145, Australia. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: Ms Ho is supported by an Australian National Healthand Medical Research Council Dora Lush Postgraduate ResearchScholarship (APP 1017189). Dr Garnett is supported by a CancerInstitute NSW Early Career Development Fellowship Grant (10/ECF/2-11). Dr Neve is supported by a Priority Research Centre inPhysical Activity and Nutrition Postdoctoral Fellowship. ProfCollins is supported by a National Health and Medical ResearchCouncil Career Development Fellowship.
PEDIATRICS Volume 130, Number 6, December 2012 e1647
REVIEW ARTICLE
by guest on June 4, 2018www.aappublications.org/newsDownloaded from

Obesity in children and adolescents isa global public health concern and isassociated with a range of short- andlong-term health complications.1–4 Al-though prevention of obesity is impor-tant, so too are effective treatments forthose already affected. Lifestyle inter-ventions, involving a combination ofdiet, exercise, and/or behavior modifi-cation, are an essential element ofobesity management.5–7 Several sys-tematic reviews of childhood obesityhave been published and lifestyle inter-ventions targeting treatment of childand adolescent obesity are reported asefficacious in weight loss in the short tomedium term.8–12 The first specific re-view of dietary interventions, publishedin 2006,13,14 included studies publishedup to 2003, and found positive effects ofinterventions that included a dietarycomponent.14,15
The previously mentioned systematicreviews and others have all presenteddata on weight change outcomes;however, obese children and adoles-cents also carry an increased risk forcardio-metabolic complications, includ-ing dyslipidemia, insulin resistance, andhypertension.15–20 To our knowledge,no systematic review has examinedthe effects of lifestyle interventionson cardio-metabolic outcomes in over-weight children and adolescents.Therefore, the aim of this review was topresent the best available evidencefrom randomized controlled studies oflifestyle interventions incorporating adietary component to assess their im-pact on both weight loss and cardio-metabolic risks. This review coversliterature published between 1975 and2010.
METHODS
The protocol and search strategy forthis systematic review was based onthe previous peer-reviewed protocol13
registered with the Joanna Briggs In-stitute. It involved a 2-stage process.
First, a detailed literature search wasconducted in September 2010 to iden-tify studies published between 2003and 2010. Eligible studies from theprevious review13 covering 1975 and2003 were then combined in the datasynthesis with those from the currentsearch.
Eligibility Criteria
Eligible studies were randomized con-trolled trials of treatment of overweightand obesity in children and adolescents#18 years of age comparing the ef-fectiveness of lifestyle interventionprograms incorporating a nutrition ordietary component with no treatmentor wait-list control, usual care, orminimal advice or written diet andphysical activity education materials.Programs that involved the wholefamily or were directed exclusively atparents of overweight or obese chil-dren and adolescents were also in-cluded. Additional inclusion criteriawere a follow-up period from baselineof at least 2 months, and inclusion ofthe outcome measures of body weightor body composition. Participantswerefree living or attending obesity clinicalunits, community programs, camps,schools, or one-off programs. Studieswere excluded if they were targeted atobesity prevention or maintenance ofweight loss, were drug trials or inter-ventions that dealt with eating dis-orders, or if they focused on childrenwith obesity attributable to a second-ary or syndromal cause. Studies thatwere not written in English, or includedchildren who were within the healthyweight range at baseline, were ex-cluded. No restrictions were placed onintervention settings or who deliveredthe interventions.
Data Source and Search Strategy
The search strategy involved a litera-ture search conducted by a medicallibrarian of published literature in the
English language through CINAHL,Cochrane Reviews, Current Concepts,DARE, Embase, Premedline, andMedline.The Medical Subject Headings of theNational Library of Medicine keywordsearch terms used were dietetic,paediatric (pediatric), child, adoles-cent, family, parent, school, over-weight, obesity, intervention, weightcontrol, weight management, weightloss, and healthy weight (SupplementalAppendix 1). In addition, the referencelists of retrieved articles and key sys-tematic reviews of childhood obesitytreatments were scanned for relevantreferences.8,9,11,12
Study Selection
All studies identified in the databasesearch were assessed for relevancefrom the title and abstract by 2 in-dependent reviewers. Articles thatmet,or appeared to meet, the inclusioncriteria were retrieved. All retrievedstudies were assessed for relevance by2 independent reviewers. In case ofdisagreement, a third independent re-viewer made the final decision.
Quality Assessment
Full copies of all included studies wereassessed for methodological quality by2 independent reviewers using theJoanna Briggs Institute critical ap-praisal of study quality tool (Supple-mental Appendix 2). Studies were ratedas positive, negative, or neutral basedon responses to 10 items. Discrep-ancies were resolved by discussion orconsultation with a third reviewer toachieve consensus.
Data Extraction
Data in relation to methodology, in-tervention effect, compliance, and in-tensity were extracted by the firstreviewer by using a standardized formdeveloped specifically for this review.This was verified by a second reviewerfor accuracy and a consensus reached
e1648 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

where disagreement existed. Data de-scribing interventions that were re-ported in more than 1 article wereextracted together.
Data Synthesis
Review Manager (RevMan5.1, TheCochrane Collaboration, Oxford, England)was used for meta-analyses. All theoutcomes in this review were continu-ous outcomes and a weighted meandifference (WMD) was calculated if thesame measurement scale was used.When different outcome measurementscales were reported, we conductedthe meta-analysis by using the stan-dardized mean difference approach.Heterogeneity was assessed by I2 sta-tistics. Heterogeneity is considered tobe low if I2 is #40%, and high if I2 is$75%.21 We used a random effectsmodel for meta-analysis if there wassignificant heterogeneity (I2 .40%),and fixed effects for homogeneous(I2 # 40%). BMI and BMI z score wereused as the primary weight loss out-comes. We also examined the effects ofinterventions on body composition byusing percentage body fat. By usingthe last time point of weight lossmeasurement for each study, we per-formed meta-analyses among sub-groups by age (child defined as meanage at baseline #12 years and ado-lescent as .12 years), and the lengthof the follow-up from baseline. Wherekey details or data were missing, au-thors were contacted, or data im-puted based on methods described inthe Cochrane Handbook.21 The follow-ing cardio-metabolic outcomes wereexamined:
serum lipids, including total choles-terol, low-density lipoprotein (LDL)cholesterol, high-density lipoprotein(HDL) cholesterol, and triglycerides;
fasting glucose, fasting insulin, andinsulin resistance as determined bythe homeostasis model assessmentof insulin resistance (HOMA-IR); and
systolic and diastolic blood pres-sures.
Where outcomes could not be quantita-tively combined in a meta-analysis, theyare described in a narrative summary.For forest plots with sufficient studiesincluded (.10), we generated funnelplots to examine for the publication bias.
RESULTS
Search Result
The literature search identified 4713references (Fig 1), and 434 full articleswere retrieved. Forty-one articles re-lating to 30 different studies met allinclusion criteria.22–62 Eight additionalstudies (12 articles) from the previousreview that met the comparison crite-ria were also included.63–74 The totalnumber of studies included in this re-view is 38.
Description of Included Studies
Study characteristics and weight-related outcomes are summarized inTable 1. Nearly half of the studies wereconducted in the United States (n =18),22,24,29,33,41,46–49,50,56,63,64,66–69,71 5 inAustralia,25,30,35–37 and the others in Israel(n = 3),39,43,44 Germany (n = 2),32,51 theUnited Kingdom (n = 2),34,40 Belgium,65
China,28 Finland,42 Iran,45 Korea,31
Mexico,38 Taiwan,26 and Tunisia.23 Eigh-teen studies targeted obese children ex-clusively,22,23,26,28,29,31,34,38,40–42,44,46,51,64–66,71
whereas the others targeted both over-weight and obese children. Most studies(n = 14) were conducted in a hospitalenvironment,22,25,29,32,36,38,40–41,43–44,46,63,65,68
followedby thecommunity (n=6),23,27,33–35,51
school (n = 6),26,42,48–50,64 and primarycare setting (n = 6).30,37,39,47,67,69 Thir-teen studies were conducted in chil-dren,25,30,33–35,37,40–42,44,47,50,66 7 inadolescents,22–24,28,29,31,36 and othersenrolled both children and adoles-cents.26,27,32,38,39,43,45,46,48,49,51 Only 1 studyincluded children aged,5 years.35 Fouradolescent studies specifically targetedgirls.24,29,31,45 The sample size of included
studies ranged from 16 to 258, witha median of 72 participants per study.Twenty-seven studies had 2 study arms, 9had 3 study arms, and 2 had 4 studyarms (Table 1). Among the no treatmentor wait-list control comparisons (n = 22)(Table 1), the intervention lengthsvaried from 1 month (n = 1) to 2 years.Twelve studies did not follow the par-ticipants after the intervention pro-gram ended.22–24,26,28,29,31,32,36,63,64,68 Forthe comparison of lifestyle interventionwith usual care (n = 11), the inter-vention lengths varied from 3 months to1 year, and 6 studies conducted sub-sequent follow-up,41–43,45,65,69 rangingfrom 2 months to 4 years from the endof the active intervention component.Among the 5 written information studies,1 had a varied intervention length, 2 hadan intervention length of 6 months,48,49
and another 2 were 1-year50,51 interven-tion programs with the outcome evalua-tion at the end of the intervention.
Methodological Quality
No studies fulfilled all requirementslisted in the study quality critical ap-praisal tool, although 8 studies met 8of the 10 requirements25,27,30,32,37,40,49,69
(Table 2). Twenty-four studies didnot specify the method of randomi-zation.22–24,26,28,29,31,33,36,39,42,45,46,48–51,63–68,71
Details of allocation conceal-ment23,24,26,28,29,31,33–36,41,43–46,50,51,63,66–68,71 andstudy blinding24,27–31,33,36,37,39,41–43,45,48,50,51,63–69,71
were not adequately reported for moststudies. Blinding of participants in di-etary and lifestyle interventions isusually not possible. Only 5 studiesreported that outcome assessors wereblinded to participants’ treatment al-location.25,30,37,38,40 Overall, retention ratesfor all included studies ranged from 38%to 100%. Most studies (29/38) had a re-tention rate of $70% at 6 months or.60% at 1 year. Only 9 studies usedintention-to-treat analysis.32,41,44,46,47,62,67–69
Six studies did not report dropout ratesand it was therefore not clear if they usedan intention-to-treat analysis.23,26,35,45,48,63
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1649 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

Dietary Interventions
Ten studies used the Traffic Light ormodified Traffic Light diet as their di-etary intervention.27,28,32,38,40,41,48,49,66,69
The Traffic Light diet is a calorie-controlled approach in which foods ineach category are color-coded ac-cording to their calorie density peraverage serving: green for low-caloriefoods that can be eaten freely; yellowfor moderate-calorie foods that can beeaten occasionally; and red for high-calorie foods that should be eatenrarely. Four studies used a hypocaloricdiet or a calorie restriction approach.Two aimed for a 30% of reported en-ergy intake deficit or 15% less thanestimated daily requirements.43,44 Onestudy targeted 500 kcal less than the
reported baseline energy intake,23 andanother imposed caloric restrictionson snacks and beverages.22 One-fifthof the included studies inadequatelydescribed the details of dietary inter-ventions.31,33,36,39,48,50,71 Other studiesprovided general healthy eating ad-vice (Table 1). A dietitian was reportedto be involved in the delivery of thedietary interventions in 13 stud-ies.25,35,38,40,42–47,51,63,67
Exercise Interventions
Nineteen studies conducted super-vised physical activity sessions orexercise training as part of the inter-vention,22–26,31,32,34,42–46,48,49,51,63,64,68 althoughthe intensity and variety varied. The totalduration of physical activity sessions
ranged from 20 minutes per month25
to 6 hours per week,23 most providing∼1.5 to 2.0 hours of training each week(Table 1). Three studies used pedome-ters to promote physical activity.27,33,36
Effects of Lifestyle InterventionCompared With No Treatment orWait-Listed Control
Eighteen of the 22 studies that com-pared lifestyle intervention with notreatment or a wait-listed controlgroup reported a positive effect onweight loss22,23,25–28,31,32,34–36,63,64,66–69,71
(Table 1). In the meta-analysis, whichincluded 19 studies (24 comparisons)and 1234 participants, there wasa significantly larger effect on weightand body composition (standardized
FIGURE 1Flowchart for identification of trials for inclusion in a systematic review of lifestyle interventions incorporating a dietary component in overweight and obesechildren and adolescents. aCollins CE, Warren JM, Neve M, McCoy P, Stokes B. Systematic review of interventions in the management of overweight and obesechildren which include a dietary component. International Journal of Evidence-Based Healthcare. 2007;5(1):2–53.
e1650 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
StudyCharacteristicsandWeight-Related
Outcom
es(Structuredby
Year
ofPublication)
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Lifestyleinterventioncomparedwith
no-treatm
entorwait-listcontrol
Botvin1979,64
,e,
School,USA
119
F+M
12to
17Obese(120%
oftheir
idealBW)
10wk,
10wk
(1)Control
(2)DA
+PA
+BM
(2)Weeklysession(1
classperiod
each)
conductedby
alliedhealthprofessionalsand
byschoolfaculty
mem
bers.
DA:Healthyfood
selection,prudentd
iet,pre-
planning
andchanging
eatingpatterns.
PA:10-minsupervised
sessioneach
week
(jogging,jum
ping
rope,bicycling)
(1)74%
(2)100%
%ofparticipants
$130%
and
,130%
ofideal
weight
Yes:Significant
decrease
in%overweight
ofthe
intervention
(P,
.05)
Nosignificant
change
in%
overweightof
thecontrol
group
Epstein
1984,66
,70,73,e,
Setting:
unclear,USA
53families
F+M
8to12
Obese($
20%
overweightand
tricep
skinfolds
.85th
percentile)
6mo, 1,5,
and10
y
(1)Wait-list
control
(2)DA
(3)DA
+PA
(2)15
treatm
entsessions,parent
andchild
inseparategroups
(session
1–8:weekly;
session9–11:biweekly;session12–15:
monthly).Parentsencouraged
tolose
weight
too.TrafficLightDiet(1200–1500
kcal/d,limit
to4redfoods/wk).
Overall:
94%at1y
Change
in%
overweight
%overweight:Yes
(3.1at6mo)
(3)DA:asgroup2
PA:lifestylechange
exercise
program-increase
energy
expenditure
200–400kcal/d
Kirshenbaum
1984,71,
Setting:
unclear,USA
40families
F+M
9to13
Obese($
20%
overweight)
9wk, 3and
12mo
(1)Wait-list
control
(2)DA
+PA
+CBT
(Childonly)
(3)DA
+PA
+CBT
(Parent&
child)
(2)9weekly90-mintreatm
entsessions.Focus
oncognitive-behavioraltreatment.
DAandPA:nodetails
given.Onlychildren
attended
thegroup(6–9childrenpergroup)
(3)as
group2,both
parentsandchildren
attended
allsessionstogether
(4–5dyads
pergroup)
(1)89%
(2)67%
(3)87.5%
%overweight,
adjusted
weight
%overweight:Yes
at3mo(2.1)
Mellin
1987,67
“Shapedown
Program,”
Primarycare,
USA
66 F+M
12to
18Overweight
andobese
(113%to213%
relativeweight)
3mo, 6and
15mo
(1)Control
(2)DA
+PA
+CBT
(2)14
weeklysessions
(90mineach)for
adolescentsp
lus2
parentsessions.Usesself-
directed
change
form
atandencourages
participantstomakesuccessive,
sustainable,sm
allm
odifications
indiet,
exercise,lifestyles,and
attitudes.Avoidvery
lowcalorieor
restrictivediets.
Overall:84%
Change
inrelative
weight
Relativeweight:
Yes(2.1)
Becque
1988,63
Hospital
environm
ent,
USA
36 F+M
12to
13Overweight
andobese
(BWandtriceps
skinfold.75th
percentile)
20wk,
20wk
(1)Control
(2)DA
+BM
e
(3)DA
+BM
+PA
(2)D
A:Am
erican
DieteticAssociationExchange
Programwith
kcalprescriptiontogive
weightloss
of1–2lb/wk.Weeklynutrition
educationmaterialsandadjustmentof
eatingpatternandkcalintake.
(3)DA:asgroup2
PA:50minflexibility,m
usclestrengtheningand
aerobicexercise
for(3
times/wk)
NR%body
fat
(hydrostatic
weighing)
%body
fat:Yes
(3.1)
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1651 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(W
hen
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Rocchini1988,68
,74
Hospital
environm
ent,
USA
72 F+M
10to17
Overweightand
obese(Weight
forheight
.75th
percentile;
tricepsand
subscapular
skinfolds
.80th
percentile)
20wk,
20wk
(1)Control
(2)DA
+BM
e
(3)DA
+PA
+BM
(2)Weekly1-hclass
DA:m
odified
kcalexchange
programto
produceaweightlossofapproximately
1lb/wk
(3)DA:asgroup2
PA:supervisedexercise3tim
es/wk(1heach,10
minstretching
andmusclestrengthening
exercise
plus
40minaerobicexercise)
(1)82%
(2)85%
(3)92%
%body
fat
(hydrostatic
weighting)
%body
fat:Yes
(3.1)
Balagopal
2003,22
,52,53
“Shapedown
Program,”
Hospital
environm
ent,
USA
16 F+M
14to18
Obese(BMI$
30)
3mo,
3mo
(1)No-treatm
ent
control
(2)DA+PA+SB+B
M
(2)DA:caloricrestriction(snacksand
beverage);metwith
anutritionistonce/wk
PA:45min3tim
es/wk;1monitoredPA
session/
wkinthepresence
ofparent
SB:limiting
TVview
ing
Overall:95%
BMI,%body
fat
(DXA)
BMIand
%body
fat:Yes(2.1)
Jiang2005,28
Family,China
75families
F+M
7thto9th
grade
Obese(Chinese
references
weightfor
height
$120%
)
2y,
2y
(1)No-treatm
ent
control
(2)DA+PA+SB+B
M
(2)Homevisitb
ypediatrician
once
permonth
DA:m
odified
trafficlight
diet
PA:20–30
min/d,4
d/wk
SB:generaladvice
(1)90%
(2)92%
BMI
BMI:Yes(2.1)
Rooney
2005,33
,e,
“Growing
HealthyFamily
study”,
Community,USA
98families,
353people
F+M
5to12
Overweightand
obese(CDC
Grow
thChart
BMI.
84th
percentile)
12wk,
1y
(1)No-treatm
ent
control
(2)PA
(3)DA+PA
(2)family
mem
bers
received
apedometer
and
instructed
towalk10
000stepsdaily
and
received
abiweeklynewsletter
(3)as
group2plus
attended
6,1-hbiweekly
sessions
concerning
nutrition,physical
activity,and
otherparentingissues.
Overall:89%
BMIpercentile
No
Golley2007,25
,54
Hospital
environm
ent,
Australia
111
F+M
6to9
Overweightand
obese(IO
TFcut-
offand
BMIz
score#
3.5)
6mo,
12mo
(1)Wait-list
control
(2)PS
(parents
only)e
(2)Parentattended4weekly2-hgroupsessions
onparentingskillstraining
(fam
ilylifestyle
change)followed
by4weekly,then
3monthly
15-to20-minindividualtelephonesessions.
(1)86%
(2)78%
(3)82%
BMIz
score,WCz
score
BMIz
score:No
WCzscore:Yes
(2.1;3.
1)
(3)PS
+DA
+PA
(3)Parentscompleted
thesameparentingskills
training
asgroup2plus
anadditional7
intensivelifestylesupportgroup
sessions.
Childrenattended
7supervised
activity
sessions
(focused
onaerobicactivity
and
motor
skillsdevelopm
ent).
DA:generaleatingguidelines
andcore
food
serverecommendations
e1652 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Huang2007,26
School,Taiwan
120
F+M
10to
13Obese(Taiwanese
referenceBM
I$95th
percentile)
12wk,
12wk
(1)No-treatm
ent
control
(2)DA
+PA
nutrition
(2)DA:childrenreceived
30-minnutrition
instructiontwice/wkatschool
PA:40-minclassroom-based
noncom
petitive
aerobicactivities
3tim
es/wk
NRBM
I,%body
fat
(BIA)
BMIand
%body
fat:Yes(2.1)
McCallum
2007,30
,58
“LEAPtrial,”
Primarycare,
Australia
163
F+M
5.0to
9.9
Overweightand
obese(IO
TFcut-
offand
BMIz
score,3.0)
12wk,
9mo,
15mo
(1)No-treatm
ent
control
(2)DA+PA+SB
(2)4standard
consultations
bygeneral
practitioners
assisted
bya20-page“fam
ilyfolder”written
ata12-y-oldreadinglevel,
targetingchange
innutrition,physical
activity,and
sedentarybehavior.
(1)85%
(2)94%
BMI,BM
Izscore
No
Park
2007,31
Setting:unclear,
Korea
44 F13
to15
Obese(Korean
referenceBM
I$95th
percentile)
12wk,
12wk
(1)No-treatm
ent
control
(2)DA+PA+BM
(2)Lifestyleeducationofferedby
atrained
counseloronce/wk.
DA:generaladvice
PA:w
alking
6d/wk(10minfor3dand30
to40
minfor3d)
(1)95%
(2)91%
BMI,%
fat(BIA),WC
andwaist/hip
ratio
BMI,%
bodyfatand
waist/hipratio:
Yes(2.1)
Shelton2007,35
Community,
Australia
43 F+M
3to10
Overweightand
obese(CDC
grow
thchart
BMI$
85th
percentile)
4wk,
3mo
(1)Wait-listcontrol
(2)DA+PA+BM
(parentonly)
(2)Parentsattended
4,2-hweeklygroup
sessions
andreceived
parent
treatm
ent
manual.
NRBM
IBM
I:Yes(2.1)
Janicke2008,27
,55,56
“ProjectSTORY”,
Community
(rural
setting),USA
93 F+M
8to14
Overweightand
obese(CDC
grow
thchart
BMI.
85th
percentile)
4mo,
10mo
(1)Wait-list
control
(2)DA+PA
(3)DA+PA
(parents
only)
(2)Weeklygroupsessions
(90mineach)for8
wk,followed
bybiweeklyfor8wk.Parentand
child
participated
inseparategroups,then
broughttogetheratthe
endofeach
sessionto
developgoalsforthewkandspecificplans.
(1)81%
(2)73%
(3)77%
BMIz
score
BMIz
score:Yes
(2.1;3.
1)
DA:m
odified
versionoftheStoplight
Diet
PA:pedom
eter-based
step
program
(3)asgroup2,butonlyparentsattended
group
meetings.
Tsiros
2008,36
“ChooseHealth
program,”
Hospital
environm
ent,
Australia
47 F+M
12to
18Overweightand
obese(IO
TFcut-off)
20wk,
20wk
(1)No-treatm
ent
control
(2)D
A+PA+BM+CBT
(2)Coreprogram(first10wk):8clinicsessions
(1heach)plus
1phone-callsessionand
provided
with
abook
onhealthyeating
andtheAustralianGuidetoHealthyEating.
Maintenance
phase(10wk):4
fortnightly
phonecalls.
DA:AustralianGuidetoHealthyEating
PA:providedwith
apedometer
Overall:38%
BMI,WC,body
fat
(DXA)
BMI,body
fatand
abdominalfat:
Yes(2.1)
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1653 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Davis2009,24
Setting:unclear,
USA
50 F14
to18
Overweightand
obese(CDC
grow
thchart
BMI.
84th
percentile)
16wk,
16wk
(1)No-treatm
ent
control
(2)DA
e
(3)DA
+PA
(strength
training)
(4)DA
+PA
(strengthand
cardiotraining)
(2)Weekly90-mindietarysessionplus
4motivationalinterview
sessions.
DA:#
10%ofenergy
from
addedsugarplus
atleast14g·1000
kcal21ofdietaryfiberaday
(3)dietaryinterventionas
group2plus
twice/
wk60
minstrength
training.
(4)as
group3but30mincardioand30
min
strength
training.
Overall:82%
BMI,BM
Izscores,
BMIpercentile
andfatm
ass
(DXA)
BMI:Yes(1.3;
1=4)
BMIzscoreandfat
mass:No
Kitzman-Ulrich
2009,29
Hospital
environm
ent,
USA
4212
to15
Obese(CDC
4mo,
(1)Wait-list
control
(2)DA:FoodGuidePyramid
Overall:83%
BMIz
score
NoF
grow
thchart
BMI.
95th
percentile)
4mo
(2)DA+PA+BM
PA:generaladvice
(3)DA+PA+BM
+Multifam
ilytherapy
(3)as
group2plus
attended
a45-min
multifam
ilytherapygroup.
Wake2009,37
“LEAP2trial,”,
Primarycare,
Australia
258
F+M
5to9.99
Overweightand
obese(IO
TFcut-offand
BMIz
score
,3.0)
12wk,
6mo,
12mo
(1)No-treatm
ent
control
(2)DA+PA+SB
(2)4standard
consultations
bygeneral
practitioners
assisted
bya16-page“fam
ilyfolder”written
ata12-y-oldreadinglevel,
targetingchange
innutrition,physical
activity,and
sedentarybehavior.
(1)98%
(2)96%
BMI
No
BenOunis2010,23
Community,
Tunisia
28 F+M
Meanage
13.160.8
Obese(BMI.
97th
percentile,
referencenot
specified)
8wk,
8wk
(1)No-treatm
ent
control
(2)PA
+DA
(2)Nutrition
educationprogram4h/wk
DA:calorierestriction(500
kcalless
than
the
reported
energy
intake
atbaseline,15%
energy
from
protein,55%carbohydrate,30%
fat)
PA:supervisedexercise
training
4tim
es/wk(90
mineach)
NRBM
I,%body
fat
(skinfold)
BMIand
%body
fat:Yes(2.1)
Reinehr2010,32
“Obeldicks
Light”
Program,Hospital
environm
ent,
Germ
any
71 F+M
8to16
Overweightand
obese
(Germany
reference
BMI90thto97th
percentile)
6mo,
6mo
(1)Wait-list
control
(2)DA+PA+SB+B
M
(2)Intensivephase(3
mo):6
nutrition
groups
(1.5heach)educationsessionforchildren
(stratified
bygender
andage)plus
6parent
eveningsessions
(1.5h)
plus
30min
individualdietarycounseling;Establishing
phase(3
mo):1
individualnutrition
counselingsessionplus
3counseling
sessions.
(1)84%
(2)97%
BMI,BM
Izscore,
WC,%body
fat
(BIA)
BMIz
score,WC
and%body
fat:
Yes(2.1)
DA:Optimized
mixed
diet(food-baseddietary
guideline)
andTrafficLightsystem
PA:w
eeklyphysicalactivity
training
(1.5heach,
mainlyaerobicexercise)for6mo
SB:generaladvice
e1654 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Sacher
2010,34
MENDprogram,
Community,
UnitedKingdom
116
F+M
8to12
Obese(UK1990
reference
dataBM
I.98th
percentile)
6mo,
12mo
(1)Wait-list
control
(2)DA+PA+B
M+12-
wkfree
family
swim
pass
(2)18,2-hbiweeklysessions
forchildrenand
theirparentsandsiblings.
DA:8
sessions,generalnutrition
educationand
nondietingapproaching
PA:16sessions
(1heach),noncom
petitivegroup
play
(1)68%
(2)70%
BMIand
BMIz
score
BMIand
BMIz
score:Yes
(2.1)
Lifestyleinterventionprogramcomparedwith
usualcareor
minimaladvice
Braet1997,65,72,e,
Hospital
environm
ent,
Belgium
259children
(1yfollow-
upstudy)
136children
(4.6y
follow-
upstudy)
F+M
7to17
Obese($
20%
overweight)
Varied,
1.0and4.6y
(1)Minimal
therapeutic
contact:DA,PA
(2)Individual
treatm
ent:CBT,
DA,PA
(3)Group
treatm
ent:CBT,
DA,PA)
(4)Summer
camp
training:CBT,
DA,PA
(1)Advicein1session(3h)andgiventreatm
ent
manualfor
parentsandworkbookfor
children
(2)R
eceivedthesameinform
ationpackages
asgroup1plus
childrenreceived
7sessions
of90
min(twice/mo)
and7monthlyfamily
follow-upsessions
onan
individualbasis.
DA:Healthyeating+3mid-mealsnacks.
Unhealthymealslim
itedto1/moor
small
amount
weekly.No
kcalcounting.
PA:m
oderateexercise
30min/d
(3)sameas
group2butonagroupapproach
(4)10-dsummer
camp:Balanced
healthyfood
1500
kcal/dplus
daily
lifestyleexercises5h/
dandfamilies
encouraged
toattend
monthly
follow-upsessions
for1y
Overall:81%
at1y
80%at4.6y
1yfollow-uppaper,
Mean%weight
loss
4.6yfollow-up
paper,%
overweightand
mean%weight
loss
No:Significant
decrease
in%
overweightin
allgroupsat3,6
mo,1.0and4.6y
Saelens2002,69
,
Primarycare,USA
44 F+M
12to
16Overweight
andobese
(20%
to100%
abovethe
medianforBM
I)
4mo,
7mo
(1)Typicalcare:
DA,PA
(2)Intensive
follow-up:DA,
BM,PA,SB
(1)Singleappointm
entwith
apediatrician
atbaseline(nontailoredcounselingsession)
DA:FoodGuidePyramid
PA:60min/d
(2)Computer-basedprogram:assessm
entof
eating,PA
andSB.Atbaseline,apediatrician
provided
tailoredcounselingsessionbased
onthecomputer-generatedindividualized
actionplan.W
eeklytelephonecounselingfor
8wkthen
biweeklyuntil14
to16
wk.Also
received
behavior
modificationmanual.
DA:1200–1500
kcal/d
andweeklygoalof40
green(#
1gfat,,150kcalandnutrient
dense)
and,15
redfoods(5
gor
morefat
ordietversions
ofhigh-fatfoods)
PA:$
60minmoderateintensity
exercise
5d/wk
SB:generaladvice
(1)90%
(2)78%
BMI,%overweight
BMI:Yes(2.1)
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1655 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Nemet2005,43
,60
Hospital
environm
ent,
Israel
54 F+M
6to16
NR3mo,
1y
(1)M
inimaladvice:
DA,PA
(1)Atleast1
ambulatory
nutritional
consultationplus
generalexerciseadvice.
(1)67%
(2)83%
BMI,%body
fat
(skinfold),BM
Ipercentile
BMIand
%body
fat
Yes(2.1)
(2)Lifestyle
program:DA,PA
(2)D
A:hypocaloricdiet(30%
deficientbased
onreported
intake
or15%less
than
estim
ated
daily
requirem
ent).M
etdietitian
6tim
esin3
mo(2.5hintotal).
PA:twice-weeklytraining
(mostly
endurance
training,1
h/session)
Gillis2007,39
Primarycare,
Israel
27 F+M
7to16
Overweightand
obese(BMI
$90th
percentile,
referencenot
specified)
6mo,
6mo
(1)M
inimaladvice:
DA,PA
(2)Lifestyle
program:DA,PA
(1)A0.5-htalkon
exercise
anddietatbaseline
(2)Talksof0.5hatbaselineand3mo,plus
weekly
followup
phonecalls.Also,instructed
torecord
dietandexercise
on1dayofeach
wk
(1)54%
(2)79%
BMIz
score
No
Kalavainen
2007,42
,59
School,Finland
70 F+M
7to
9Obese(Finnish
reference
weightfor
height
120%
to200%
)
6mo,
12mo
(1)Routine
Program:DA
(2)Lifestyle
program:DA,
PA,SB,BM
,CBT
(1)2individualcounselingsessions
byschool
nurse(30mineach)plus
inform
ation
bookletsforfamily.
(2)Family-based
grouptreatm
ent,15
sessions
(90mineach)with
separatesessions
for
parentsand
childrenand1jointsession.First
10sessions
wereheldweeklyandthen
fortnightly.
DA:generalhealthyeating
PA:noncompetitiveactivities
(1)100%
(2)97%
BMIand
BMIz
score
BMIand
BMIz
score:Yes
(2.1)
Savoye
2007,46
,61
“YaleBright
Bodies
Weight
Managem
ent
Program”,
Hospital
environm
ent,USA
209
F+M
8to16
Obese(CDC
grow
thchart
BMI.
95th
percentile)
1y,
1y
(1)Standard
care:
DA(1)Metdietitian
every6mo,generalhealthy
eatingandphysicalactivity
advice.
(1)64%
(2)71%
BMIand
%body
fat(BIA)
BMIand
body
fat:
Yes(2.1)
(2)Lifestyle
program:DA,
PA,BM
(2)Intensivefamily-based
nutrition
and
behavior
modification(weekly40
minforthe
first6mothen
everyotherwk).
DA:a
nondietingapproach,focused
onbetter
food
choices
PA:twice50-minsessions
ofhigh-intensity
aerobicexerciseforthe
first6mofollowed
by100mintwice/month.Plusencouraged
toexercise
3additionaldaysathomeperwk
e1656 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
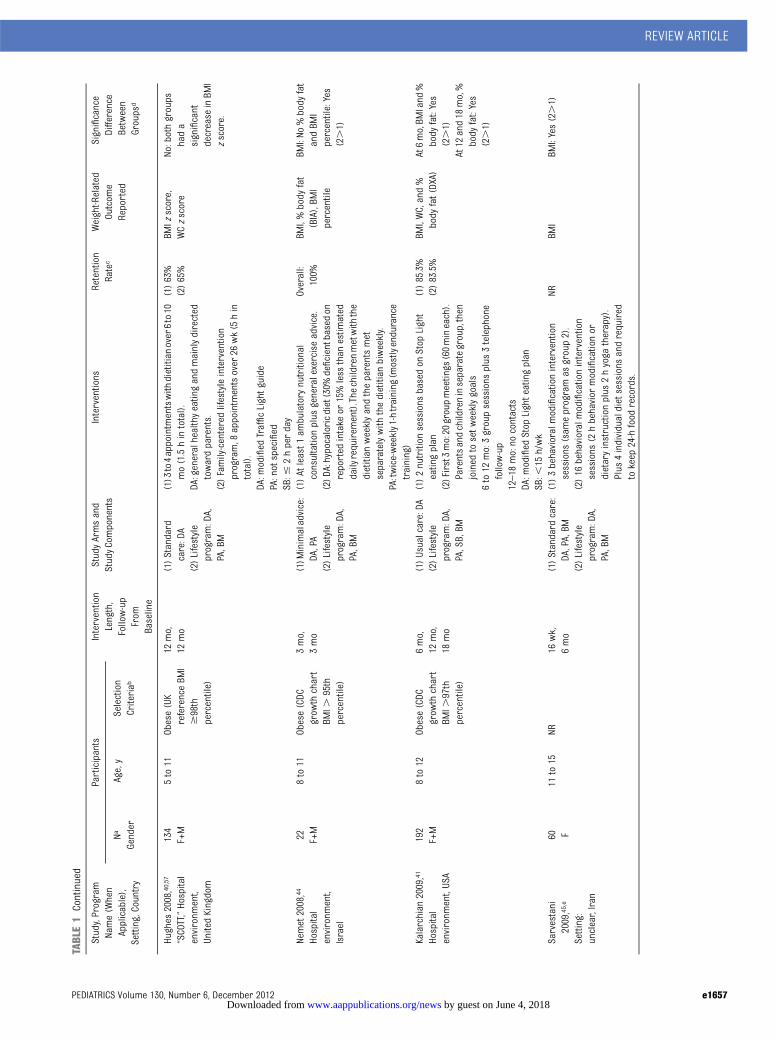
TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Hughes
2008,40
,57
“SCOTT,”Hospital
environm
ent,
UnitedKingdom
134
F+M
5to11
Obese(UK
referenceBM
I$98th
percentile)
12mo,
12mo
(1)Standard
care:DA
(2)Lifestyle
program:DA,
PA,BM
(1)3
to4appointm
entswith
dietitian
over6to10
mo(1.5hintotal).
DA:generalhealthyeatingandmainlydirected
towardparents.
(2)Family-centeredlifestyleintervention
program,8
appointm
entsover
26wk(5hin
total).
DA:m
odified
TrafficLightguide
PA:notspecified
SB:#
2hperday
(1)63%
(2)65%
BMIz
score,
WCzscore
No:bothgroups
hada
significant
decrease
inBM
Izscore.
Nemet2008,44
Hospital
environm
ent,
Israel
22 F+M
8to11
Obese(CDC
grow
thchart
BMI.
95th
percentile)
3mo,
3mo
(1)M
inimaladvice:
DA,PA
(2)Lifestyle
program:DA,
PA,BM
(1)Atleast1
ambulatory
nutritional
consultationplus
generalexerciseadvice.
(2)D
A:hypocaloricdiet(30%
deficientbased
onreported
intake
or15%less
than
estim
ated
dailyrequirem
ent).The
childrenmetwith
the
dietitian
weeklyandtheparentsmet
separatelywith
thedietitian
biweekly.
PA:twice-weekly1-htraining
(mostly
endurance
training)
Overall:
100%
BMI,%body
fat
(BIA),BM
Ipercentile
BMI:No
%body
fat
andBM
Ipercentile:Yes
(2.1)
Kalarchian
2009,41
Hospital
environm
ent,USA
192
F+M
8to12
Obese(CDC
grow
thchart
BMI.
97th
percentile)
6mo,
12mo,
18mo
(1)Usualcare:DA
(2)Lifestyle
program:DA,
PA,SB,BM
(1)2nutrition
sessions
basedon
Stop
Light
eatingplan
(2)First3mo:20
groupmeetings
(60mineach).
Parentsandchildreninseparategroup,then
joined
tosetw
eeklygoals
6to
12mo:3groupsessions
plus
3telephone
follow-up
12–18
mo:no
contacts
DA:m
odified
Stop
Lighteatingplan
SB:,
15h/wk
(1)85.3%
(2)83.5%
BMI,WC,and%
body
fat(DXA)
At6mo,BM
Iand
%body
fat:Yes
(2.1)
At12
and18
mo,%
body
fat:Yes
(2.1)
Sarvestani
2009,45
,e
Setting:
unclear,Iran
60 F11
to15
NR16
wk,
6mo
(1)Standard
care:
DA,PA,BM
(1)3behavioralmodificationintervention
sessions
(sam
eprogramas
group2).
NRBM
IBM
I:Yes(2.1)
(2)Lifestyle
program:DA,
PA,BM
(2)16
behavioralmodificationintervention
sessions
(2hbehavior
modificationor
dietaryinstructionplus
2hyoga
therapy).
Plus
4individualdietsessions
andrequired
tokeep
24-hfood
records.
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1657 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Diaz
2010,38
Shapedow
nProgram,Hospital
environm
ent,
Mexico
76 F+M
9to17
Obese(CDC
grow
thchart
BMI.
95th
percentileor
BMI.
90th
percentilewith
WC.90th
percentile)
12mo,
12mo
(1)Usualcare:DA
(2)Lifestyle
program:DA,
PA,SB,BM
(1)Monthly10-to15-minconsultations
with
primarycare
physician
(1)58%
(2)55%
BW,BMI,BM
Izscore,WC,
body
fat(DXA)
BMI,BM
Izscore,
WC,andbody
fat:Yes(2.1)
DA:FoodGuidePyramid
PA:30minmostd
aysofthewk
SB:#
2h/d
(2)12
weekly2-hbehavior
groupprogramand
weeklydietitian
counselingsessions
forthe
first3
mo,then
monthlyuntil12
mo.Plus
12monthlyphysicianconsultations.Parents
received
6educationsessions
andwere
encouraged
tolose
weightifthey
were
overweight.
DA:TrafficLightdietapproachplus
educationon
glycem
icindexandprovided
with
anindividualized
dietplan
of1200
to1800
kcal/d
PA:notspecified
SB:notspecified
Face-to-face
educationcomparedwith
written
educationmaterials
Fullerton
2007,48
School,USA
80 F+M
6thand7th
graders
Overweightand
obese(CDC
grow
thchart
BMI$
85th
percentile)
6mo,
6mo
(1)Written
materials
(1)To
followa12-wkparent-guidedmanualof
Trim
Kids.
NRBM
Izscore
BMIz
score:Yes
(2.1)
(2)Intensive
instructor-led
intervention
group:DA,PA,
BM
(2)Childrenreceived
aninstructor-leddaily
interventionduring
schooldays
(1nutrition
classand4physicalactivity
classesweekly)
for12
wk,then
monthlyboostersessions.
Parentsofferedmonthlyeveningtraining
sessions.
Johnston
2007,49
,62
School,USA
71 F+M
10to
14Overweightand
obese(CDC
grow
thchart
BMI$
85th
percentile)
6mo,
6mo
(1)Written
materials
(1)To
followa12-wkparent-guidedmanualof
Trim
Kids.
(1)88%
(2)95%
BMIand
%body
fat(BIA)
BMI:Yes(2.1)
%body
fat:No
(2)Intensive
instructor-led
intervention
group:DA,
PA,BM
(2)Childrenreceived
aninstructor-leddaily
intervention(1nutrition
classand4physical
activity
classesweekly,35
to40
mineach)
for12
wk,then
biweeklyduring
thelast
period
ofschool.Plusreceived
snackbars
foradaily
afternoonschoolsnackand
acerealforbreakfast.Parent
attended
monthlymeetings.
e1658 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(When
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
DA:foodgroups
werelabeled“safety”
(most
fruitsandnonstarchy
vegetables),“caution”
(low
-fatm
eat,low-fatd
airy
andcomplex
carbohydrate)and“danger”
($5gram
sof
fator$
15gram
sofsugarperserving)zone
food
PA:2-stage
approach,wk1to6aimed
todevelop
abasiclevelofphysicalfitness;wk7to12
tofocuson
sportskilldevelopm
ent
Weigel2008,51
Community,
Germ
any
73 F+M
7to15
Obese(WHO
grow
thstandard)
1y,
1y
(1)Written
dietary
advice:DA
(2)Group
sessions:DA,PA,
BM
(1)Written
advice
(FoodGuidePyramid)from
apediatrician
during
anoutpatient
visitat
baselineand6mo.
(1)83%
(2)97%
BMI,BM
Izscore
BMIz
scoreand
BMI:Yes(2.1)
(2)Childrenreceived
weeklygroupnutrition
education(adapted
from
theFood
Guide
Pyramidfruitand
vegetabletemplate,45–60
min/session)andcoping
strategy
training.
Parentsreceived
monthly2hsupport
sessions.
PA:w
eeklysession,alternatingsw
immingand
indoor
sports
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1659 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE1
Continued
Study,Program
Name(W
hen
Applicable),
Setting,Country
Participants
Intervention
Length,
Follow-up
From
Baseline
StudyArmsand
StudyComponents
Interventions
Retention
Rate
c
Weight-Related
Outcom
eReported
Significance
Difference
Between
Groups
d
Na
Gender
Age,y
Selection
Criteriab
Estabrooks
2009,47
Primary
care,USA
220
F+M
8to12
Overweightand
obese(CDC
grow
thchart
BMI$
85th
percentile)
Intervention
length
varied,
followup
at6
and12
mo
(1)Written
materials:DA,
PA,SB
(2)Written
materials+
Groupsession
with
dietitian:
DA,PA,SB,BM
(3)Written
materials+
Groupsession
with
dietitian
+interactive
voiceresponse
technology:DA,
PA,SB,BM
(1)Received
a61-pageworkbookdesigned
toprom
otephysicalactivity,increase
consum
ptionoffruitsandvegetables
and
decreasedsugareddrinks,TVview
ing,and
sedentarybehavior.
(2)As
group1
plus
2weeklysm
allgroup
educationsessions
(2heach).
(3)As
group2plus
10weeklyfollow-upphone
calls
delivered
byinteractivevoiceresponse
system
andbasedon
goalssetb
ythe
participants.
(1)72%
(2)66%
(3)74%
BMIz
score
BMIz
score:Yes
(3.1;1.
2)
Resnick2009,50
,e,
CHEERProgram,
School,USA
46families
F+M
Kindergarten
and5th
graders
Overweight
andobese
(CDC
grow
thchartB
MI
$85th
percentile)
1y,
1y
(1)Written
materials
(2)Written
materials+
homevisitor
phonecall
(1)6
mailingsofeducationalm
aterialsat∼5-wk
intervals.
(2)As
group1plus
atleast1
homevisitor
phonecallby
thecommunity
health
workers.
(1)100%
(2)86%
BMIpercentile
No:bothgroups
lostweight
F,female;M,m
ale;BW
,bodyweight;DA,dietaryadvice;PA,physicalactivity;BM,behavioralm
odification;kcal,kilocalorie;CBT,cognitive
behavior
therapy;NR
,notreported;SB,sedentarybehavior;DXA,dual-energyx-rayabsorptiometry;CDC
,Centers
for
DiseaseControland
Prevention;IOTF,InternationalObesityTaskforce;WC,waistcircum
ference;PS,parentingskill;BIA,bio-im
pedanceanalyzer;ProjectSTORY,Projectsensibletreatm
entofobesityinruralyouth;SCOTT,ScottishChildhood
Overweight
Treatm
entTrial;WHO
,WorldHealth
Organization;CHEERProgram,Com
municatingaboutHealth,Exercising,andEatingRightProgram.
aNumberofparticipantsatrandom
ization.
bClassificationofoverweightandobesity
standardized
usingthefollowingdefinitions:Overw
eight=BM
I85thto95th
percentileforageandsex;obese=BM
I$95th
percentileforageandgender
orweight$
120%
ofaverageweightforheight.
cRetentionratesreported
postinterventionifno
follow-up,or
atlatestpointoffollow-up.
d2.
1means
group2hadagreaterreductionthan
group1(P
,.05).
eNotincluded
inthemeta-analyses.
e1660 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

mean difference20.97, 95% confidenceinterval (CI)21.39 to20.55) for lifestyleinterventions compared with controlover 2 years (Supplemental Fig 8).However, the studies were significantlyheterogeneous (I2 = 90%) and the effectsize varied by age and length of study.There was no evidence of publicationbias or small-study effects with visualinspection of the funnel plot.
We also conducted meta-analyses of12 studies (899 participants) that re-ported BMI (Fig 2A) and 7 studies (493participants) that reported BMI z score(Fig 2B). There was a pooled BMI re-duction of 1.25 kg/m2 (95% CI: 0.32–2.18, I2 = 98%) and a 0.10 BMI z scorereduction (95% CI: 0.02–0.18, I2 = 0%–50%) greater for the lifestyle in-tervention compared with the controlcondition.
The short-term study of children withthegreatestpostinterventioneffectwasa 6-month community-based program(mean BMI difference = 2.10 kg/m2) inwhich parents and children attendedeighteen 2-hour group education andexercise sessions held twice weekly insports centers and schools, followedby a 12-week free family swimmingpass (Table 1).34 However, the greatestBMI reduction in the studies of ado-lescents (mean BMI difference 4.30kg/m2) was in a 2-month community-based intensive exercise training pro-gram (4 times per week, 90 minuteseach) combined with dietary restric-tion (500 kcal/d less than the reportedbaseline energy intake).23
Effects of Lifestyle InterventionProgram Compared With UsualCare or Minimal Intervention
Eight of the 11 studies reported a posi-tive effect of the lifestyle intervention ascompared with usual care or minimalinterventions.38,41–46,69 The overall effectsize in the meta-analysis, which included7 studies (586 participants),38,41–44,46,69
was a decrease in BMI of 1.30 kg/m2 atthe end of active intervention (95% CI:1.03–1.58, I2 = 0% to 48%) (Fig 3A). Stud-ies with longer intervention periods (.6months)41,42 showed greater weight lossthan shorter term interventions.41–44,69
Four studies followedupparticipants at 7months to 1 year from baseline and thepooled results indicate that weight losswas sustained after program completion(Fig 3B). Similar observations were ob-tained for percentage body fat change,with the lifestyle intervention group los-ing 3.2% more body fat (95% CI: 1.39–5.01) than the usual care groupat the endof active intervention (Supplemental Fig9A).The fat loss effect was sustained at1 year follow-up (Supplemental Fig 9B).Four studies38–40,42 reported BMI z scorechange after the active intervention, withthe pooled weight loss being 0.09 BMIz score greater (0.02 to 0.15, I2 , 40%)in the lifestyle intervention comparedwith usual care (Supplemental Fig 9C).
Effects of Lifestyle InterventionProgram Compared With WrittenEducational Materials
Two of the 5 studies reported BMI and3 reported BMI z score. There was
a 2.52 kg/m2 greater reduction inpooled BMI (95% CI: 0.91–5.95, I2 =97%) and 0.06 greater reduction inpooled BMI z score (95% CI: 0.02–0.10,I2 = 99%) for the lifestyle interventionprograms compared with written ed-ucational materials only over 1 year(Fig 4A and B).
Effects of Lifestyle Interventions onCardio-metabolic Outcomes
Table 3 summarizes the metabolicoutcomes reported by each study.Fifteen of the 38 studies reportedat least 1 cardio-metabolic outcome.22,24,26,28,31,32,34,39,41,43,46,49,51,63,68 All except 2small studies (with 7 to 15 participants ineach study arm)24,39 reported a positiveweight loss effect of lifestyle inter-ventions compared with control groups.Eight studies reported blood lipidsresults26,28,31,39,43,46,49,63; 6 studies re-ported results of fasting glucose, fast-ing insulin, or HOMA-IR,22,24,26,31,46,49;and 12 studies reported blood pres-sure findings.26,28,31,32,34,41,43,46,49,51,63,68
Total Cholesterol and Triglycerides
Meta-analysis of 5 studies including 440participants between 8 and 16 yearsold (Supplemental Fig 10) showed thatlifestyle intervention had a significantlygreater impact on total cholesterol im-provement compared with no treatment/wait-list control, usual care, or writteneducational materials, both in the short-term (WMD20.40mmol/L, 95% CI:20.51to 20.30; I2 = 0%; study length: 4 to 6
TABLE 2 Selected Methodological Quality of Included Studies: Results Are Presented as Number of Studies (%)
TrueRandomization
AllocationConcealment
Blinding of OutcomeMeasurement
BaselineComparability
Retention Rate $70% at6 mo or $60% at 1 y
Intention-to-Treat Analysis
Lifestyle interventions comparedwith no-treatment/wait-listcontrol, n = 22 studies
Yes 7 (32) 5 (23) 3 (14) 18 (82) 16 (73) 3 (14)No 0 (0) 0 (0) 2 (9) 1 (4) 1 (4) 13 (59)Unclear 15 (68) 17 (77) 17 (77) 3 (14) 5 (23) 6 (27)
Lifestyle interventions comparedwith standard care/minimaladvice, n = 11 studies
Yes 5 (45) 3 (27) 2 (18) 10 (91) 8 (73) 4 (36)No 0 (0) 1 (0) 1 (9) 1 (9) 2 (18) 5 (46)Unclear 6 (55) 7 (73) 8 (73) 0 (0) 1 (9) 2 (18)
Lifestyle interventions comparedwith written education materials,n = 5 studies
Yes 2 (40) 1 (20) 0 (0) 4 (80) 4 (80) 2 (40)No 0 (0) 0 (0) 0 (0) 1 (20) 0 (0) 2 (40)Unclear 3 (60) 4 (80) 5 (100) 0 (0) 1 (20) 1 (20)
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1661 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

FIGURE 2Meta-analysis of studies comparing lifestyle intervention with no-treatment or wait-list controls.
e1662 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
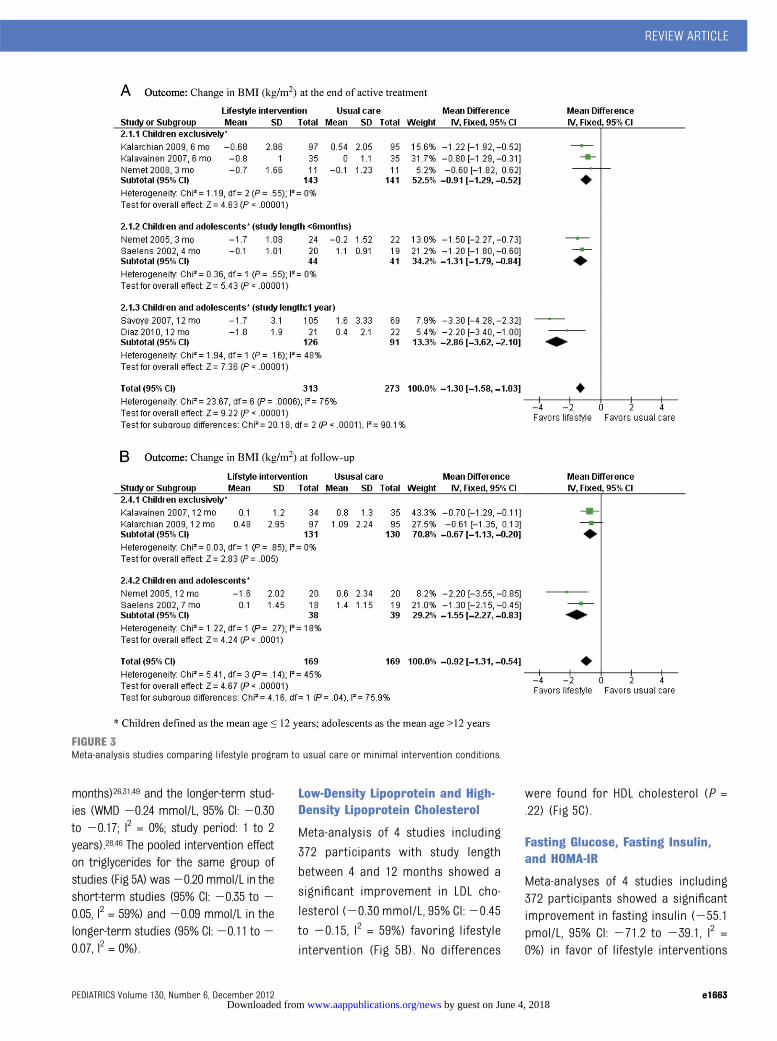
months)26,31,49 and the longer-term stud-ies (WMD 20.24 mmol/L, 95% CI: 20.30to 20.17; I2 = 0%; study period: 1 to 2years).28,46 The pooled intervention effecton triglycerides for the same group ofstudies (Fig 5A) was20.20 mmol/L in theshort-term studies (95% CI: 20.35 to 20.05, I2 = 59%) and20.09 mmol/L in thelonger-term studies (95% CI:20.11 to20.07, I2 = 0%).
Low-Density Lipoprotein and High-Density Lipoprotein Cholesterol
Meta-analysis of 4 studies including
372 participants with study length
between 4 and 12 months showed a
significant improvement in LDL cho-
lesterol (20.30 mmol/L, 95% CI:20.45
to 20.15, I2 = 59%) favoring lifestyle
intervention (Fig 5B). No differences
were found for HDL cholesterol (P =.22) (Fig 5C).
Fasting Glucose, Fasting Insulin,and HOMA-IR
Meta-analyses of 4 studies including372 participants showed a significantimprovement in fasting insulin (255.1pmol/L, 95% CI: 271.2 to 239.1, I2 =0%) in favor of lifestyle interventions
FIGURE 3Meta-analysis studies comparing lifestyle program to usual care or minimal intervention conditions.
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1663 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

over 1 year (Fig 6A) and no differenceswas found for fasting glucose (P = .08)(Supplemental Fig 11). The pooled dif-ference for HOMA-IR was 22.32 (95%CI:23.25 to21.39) in favor of lifestyleintervention over 1 year; however, theheterogeneitywashigh (I2 = 79%) (Fig 6C).
Blood Pressure
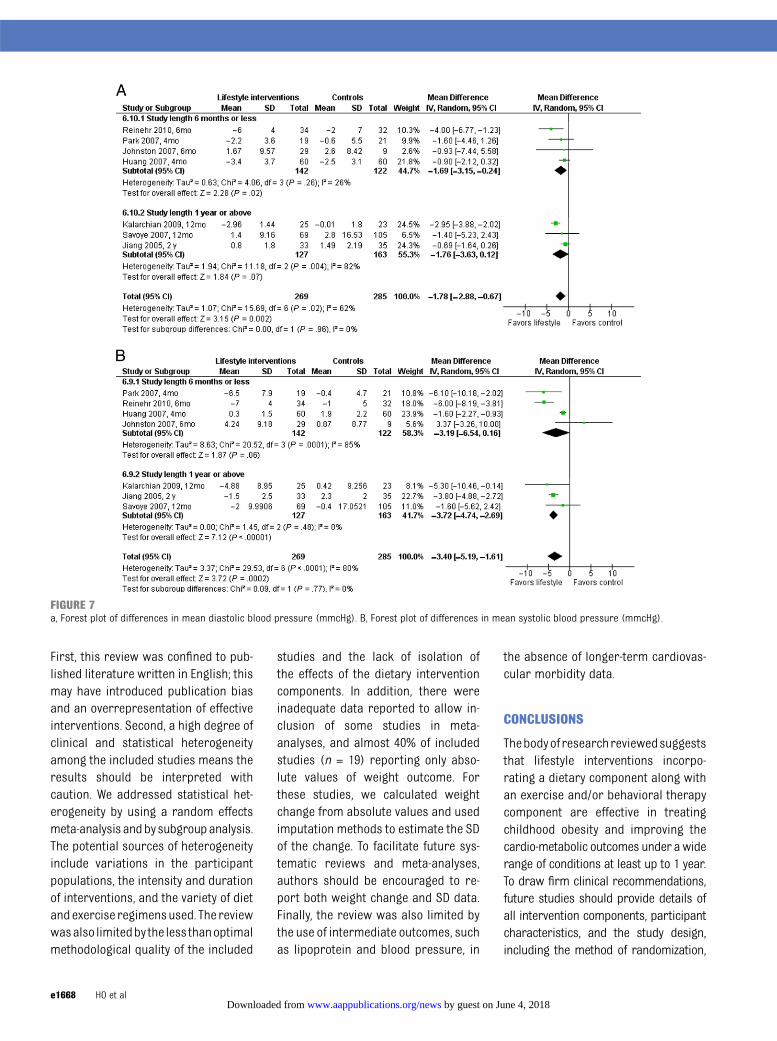
Meta-analyses of 7 studies (554 par-ticipants) showed that lifestyle inter-ventions led to a significantly greaterimprovement in diastolic bloodpressurein the short-term studies (WMD 21.69mm Hg, 95%CI:23.15 to20.24, I2 = 26%,study length: 6months or less) but therewas no difference in the longer-termstudies (Fig 7A). On the contrary, a sig-nificantly greater improvement in sys-tolic blood pressure was shown onlyin the studies with a study length of1 year or more (WMD 23.72 mm Hg,95% CI:24.74 to22.69, I2 = 0%) (Fig 7B).Five studies were not included in themeta-analyses, as they reported theabsolute values only at baseline andfollow-up.34,43,51,63,68 These studies re-ported a similar trend as those includedin the meta-analyses.
The study that achieved the greatest im-provement across all cardio-metabolic
outcome measures, including blood lip-ids, fasting glucose and insulin, HOMA-IR,and blood pressure, was a 12-weekintensive school-based lifestyle inter-ventionprogram targeting10- to 13-year-old obese students.26 The participantsreceived 30-minutes of nutrition in-struction twice per week at school plus40-minutes of classroom-based non-competitive aerobic activity 3 timesper week. The mean BMI and bodyfat percentage difference betweenthe intervention group and the no-treatment control at the end of activeintervention was 21.5 kg/m2 and21.2% respectively.
DISCUSSION
This systematic review reports on life-style intervention trials incorporatinga dietary component aimed at treatingoverweight and obesity in children andadolescents published between 1975and September 2010 (n = 38). It is thefirst review to summarize the effectsof lifestyle interventions on cardio-metabolic outcomes in this age groupand provides an improved understand-ing of the effects of lifestyle interventionson weight loss and cardio-metabolicoutcomes. The results support the
importance of lifestyle interventionsincorporating a dietary component as acritical part of treatment of childhoodobesity.
The meta-analyses indicate that life-style interventions incorporating a di-etary component led to significantweight loss when compared with notreatment. These results support pre-vious reviews,8,9,11–14 and extend theevidence base on the use of lifestyleinterventions in the treatment of child-hood obesity, as this review includesmore trials, uses clearly defined no-treatment, or wait-list controls, andextends ascertainment to September2010. Studies comparing lifestyle inter-ventionswith usual care also resulted insignificant immediate and posttreat-ment effects on BMI up to 1 year frombaseline. The meta-analysis shows thatweight loss was greater when the du-ration of treatment was longer than6 months. Lifestyle interventions alsoproduced significant treatment effectson BMI and BMI z score, compared withwritten information only, over a 6- to12-month intervention period.
Meta-analyses showed that lifestyleinterventions resulted in significant
FIGURE 4Meta-analysis of studies comparing lifestyle intervention program with written education materials.
e1664 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

TABLE3
Effectsof
LifestyleInterventions
onAnthropometricandMetabolicOutcom
es(Structuredby
Year
ofPublication)
Study
Timeof
Measurementa
Anthropometric/Body
Composition
Metabolic
BMI
BMIz
Score
Body
Fat%
Waist
Circum
ference
Total
Cholesterol
LDL
HDL
Triglyceride
Fasting
Glucose
Fasting
Insulin
Insulin
Resistance
iSBP
DBP
Lifestyleinterventioncomparedwith
no-treatm
entorwait-listcontrol
Becque
1988
6320
wk
✓b,d
✓✓
✓b
✓✓
✓b
Rocchini1988
6820
wk
✓b,d
✓b
✓b
Balagopal20032
23mo
✓b
✓b,e
✓b,c
✓b,c
Jiang2005
2824
mo
✓b
✓b
✓b
✓b
✓b
Huang2007
2612
wk
✓b
✓b,f
✓b
✓b
✓b
✓b
✓b
✓b
✓b
✓✓
Park
2007
3112
wk
✓b
✓b,f
✓b
✓b
✓b
✓✓
b✓
b✓
b✓
b✓
b✓
Davis2009
2416
wk
✓b
✓✓
✓
Reinehr2010
326mo
✓b
✓b
✓b,f
✓b
✓b
✓b
Sacher
2010
346mo
✓b
✓b
✓g
✓b
✓✓
b
Lifestyleinterventioncomparedwith
usualcare
Nemet2005
433mo
✓b
✓b,h
✓b
✓b
✓✓
✓✓
b
Nemet2005
4312
mo
✓b
✓b,h
Gillis2007
396mo
✓✓
✓✓
Savoye
2007
466mo
✓b
✓b,f
✓b
✓✓
✓✓
✓b
✓b
✓✓
Savoye
2007
4612
mo
✓b
✓b,f
✓b
✓✓
✓✓
✓b
✓b
✓✓
Kalarchian
2009
416mo
✓b
✓b,e
✓b
✓b
✓
Kalarchian
2009
4112
mo
✓✓
b,e
✓b
✓b
✓
Lifestyleinterventioncomparedwith
written
educationmaterialsonly
Johnston
2007
496mo
✓b
✓f
✓b
✓b
✓✓
✓✓
✓✓
Weigel20085
112
mo
✓b
✓b
✓b
✓
DBP,diastolic
bloodpressure;SBP,systolic
bloodpressure;✓
,the
outcom
eswerereported.
aCountedfrom
baseline.
bIndicatesastatisticallysignificant
improvem
entinthat
outcom
ewhencomparedwith
no-treatm
entcontrol/usualcare/written
educationmaterials.
cFindings
reported
ingraph.
dBody
fat%measuredby
hydrostatic
weighting.
eBody
fat%measuredby
dual-energyx-rayabsorptiometry.
fBody
fat%measuredby
bio-impedanceanalyzer.
gBody
fat%determ
ined
bydeuteriumdilution.
hBody
fat%determ
ined
byskinfolds.
iInsulin
resistance
determ
ined
bythehomeostasismodelassessmentofinsulin
resistance
(HOM
A-IR).
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1665 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

improvements in total cholesterol andtriglycerides up to 2 years from base-line, as well as improvements in fastinginsulin and HOMA-IR up to 1 year frombaseline; however, the improvementswere not uniformly associated with theextent of weight loss or body fat re-duction. It is uncertain whether thepositive effects were attributable toweight loss per se or attributable toaspects of the lifestyle intervention thatwere independent of weight loss, suchas reduction in saturated fat intakeor increased physical activity. Somestudies have reported that lifestyle in-
tervention resulted in improvement inplasma lipid concentrations, insulinsensitivity, and blood pressure in obesechildren, even in the absence of weightloss or body composition change.75,76
The absence of individual participants’data on weight and cardio-metabolicoutcome changes makes it impossibleto characterize the relationship be-tween the extent of weight loss andchanges in various cardio-metabolicoutcomes. Although most studiesshowed a significant improvement intotal cholesterol (6/7)26,28,31,43,46,49 orLDL cholesterol,26,31,43,49 fewer than half
demonstrated significant improvementsin triglycerides26,28,31 or HDL choles-terol.26,63 High triglycerides and lowHDL cholesterol levels are the impor-tant risk factors of cardiovasculardisease. Future studies should ex-plore effective strategies to improvetriglycerides and HDL cholesterolconcentrations.
The impact of lifestyle interventions onblood pressure is less certain from theincluded studies. Most overweight orobese children are likely to be normo-tensive. In addition, blood pressure is
FIGURE 5a, Forestplot ofmeandifferences in triglycerides concentrations (mmol/L). B, Forestplot ofmeandifferences in LDLcholesterol concentrations (LDL,mmol/L). C,Forest plot of mean differences in HDL concentrations (HDL, mmol/L).
e1666 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

strongly related to age and height77–79 inchildren and adolescents, and thereforedirect comparison of blood pressurereading possibly underestimates theintervention effects and limits our abil-ity to draw definitive conclusions on theeffects of lifestyle interventions on bloodpressure.
Features of Effective Interventions
The heterogeneity of the includedstudies makes it difficult to give de-finitive recommendations for practice.However, the studies provide evidenceto support a variety of dietary andlifestyle components in treating child-hood obesity across a wide range oftreatment settings, age groups, andseverity of obesity.
Family Involvement
Family involvement in treatment ofchildhood obesity is widely advocatedand discussed.9,80,81 Our review demon-strated that almost all effective inter-ventions (particularly in studies thatenrolled children ,12 years of age)reported including a family component,including separate education sessionsfor parent and child,25,27,32,41,42,44,48,49,51,66
targeted parents as the sole agent ofchange,35 encouraged parents to loseweight if they were overweight,38,66 orprovided a free family swim pass toparticipants.34
Dietary Intervention
We found that dietary interventionswere rarely evaluated as a sole com-ponent of treatment in comparisonwitha waited-list or no-treatment controlgroup. Dietary interventions wereusually part of a broader lifestyle in-tervention program. Not all studiesadequately described the dietary in-tervention. The most commonly re-ported dietary interventions were themodified Stop/Traffic Light approachand a hypocaloric diet/calorie re-striction approach. Both dietary ap-proacheswere demonstrated to achieveeffective relative weight loss acrossdifferent age groups, settings, andcountries.22,23,27,32,38,41–44,66 The influen-ces on weight were sustained up to 1year from baseline.27,41–43
Exercise Intervention
Another frequent feature of effective stud-ies is involvement of a structured exer-
cise training component.22,31,43,46,48,49,64,68
Again, the varied strategies, intensity,and duration of intervention make itdifficult to conduct direct comparisonsand to identify the most effective exer-cise intervention for weight loss in thisage group.
Strengths and Limitations
This review comprehensively includedlifestyle intervention trials publishedbetween 1975 and 2010 during whichtime childhood obesity became preva-lent. Strengths of the study include thereporting of mean differences in BMIandpercentagebody fat,weight changeindicators commonly used by clini-cians, as well as cardio-metabolic out-comes, Also, separate meta-analyseswere conducted to compare lifestyleinterventions with clearly defined no-treatment or wait-list controls, usualcare, orminimal advice andwrittendietand physical activity education mate-rials respectively. This provides clini-cally meaningful information for futurepediatric obesity treatment serviceplanning.
A number of limitations of the presentanalyses should be acknowledged.
FIGURE 6a, Forest plot of differences in mean fasting insulin (pmol/L). B, Forest plot of mean differences in homeostasis model assessment of insulin resistance(HOMA-IR).
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1667 by guest on June 4, 2018www.aappublications.org/newsDownloaded from
First, this review was confined to pub-lished literature written in English; thismay have introduced publication biasand an overrepresentation of effectiveinterventions. Second, a high degree ofclinical and statistical heterogeneityamong the included studies means theresults should be interpreted withcaution. We addressed statistical het-erogeneity by using a random effectsmeta-analysis andbysubgroupanalysis.The potential sources of heterogeneityinclude variations in the participantpopulations, the intensity and durationof interventions, and the variety of dietandexercise regimensused. The reviewwasalso limitedby the less thanoptimalmethodological quality of the included
studies and the lack of isolation ofthe effects of the dietary interventioncomponents. In addition, there wereinadequate data reported to allow in-clusion of some studies in meta-analyses, and almost 40% of includedstudies (n = 19) reporting only abso-lute values of weight outcome. Forthese studies, we calculated weightchange from absolute values and usedimputation methods to estimate the SDof the change. To facilitate future sys-tematic reviews and meta-analyses,authors should be encouraged to re-port both weight change and SD data.Finally, the review was also limited bythe use of intermediate outcomes, suchas lipoprotein and blood pressure, in
the absence of longer-term cardiovas-cular morbidity data.
CONCLUSIONS
Thebodyof researchreviewedsuggeststhat lifestyle interventions incorpo-rating a dietary component along withan exercise and/or behavioral therapycomponent are effective in treatingchildhood obesity and improving thecardio-metabolic outcomes under awiderange of conditions at least up to 1 year.To draw firm clinical recommendations,future studies should provide details ofall intervention components, participantcharacteristics, and the study design,including the method of randomization,
FIGURE 7a, Forest plot of differences in mean diastolic blood pressure (mmcHg). B, Forest plot of differences in mean systolic blood pressure (mmcHg).
e1668 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

blinding, allocation concealment, andattrition rates. Further work is requirednot only to determine the optimal length,intensity, and long-term effectivenessof lifestyle interventions, but also to
determine what magnitude of weightreduction in the pediatric population iscompatible with clinically significant ben-efits. Further, cost-effectiveness analysesneed to be conducted.
ACKNOWLEDGMENTWe thank Ms Debbie Booth, librarian,Faculty of Health, The University of New-castle, for assistance with the search-and-retrieve strategies.
REFERENCES
1. Lobstein T, Baur L, Uauy R; IASO In-ternational Obesity TaskForce. Obesity inchildren and young people: a crisis inpublic health. Obes Rev. 2004;5(suppl 1):4–104
2. Daniels SR, Arnett DK, Eckel RH, et al.Overweight in children and adolescents:pathophysiology, consequences, prevention,and treatment. Circulation. 2005;111(15):1999–2012
3. Weiss R. Cardiovascular Risk Clustering inObese Children. In: Debasis B, ed. GlobalPerspectives on Childhood Obesity. SanDiego: Academic Press; 2011:139–146
4. Steinberger J, Daniels SR, Eckel RH, et al;Progress and challenges in metabolicsyndrome in children and adolescents:a scientific statement from the AmericanHeart Association Atherosclerosis, Hyper-tension, and Obesity in the Young Commit-tee of the Council on CardiovascularDisease in the Young; Council on Cardio-vascular Nursing; and Council on Nutrition,Physical Activity, and Metabolism. Circula-tion. 2009;119(4):628–647
5. National Institute for Health and ClinicalExcellence. NICE clinical guideline 43 Obe-sity: guidance on the prevention, identifi-cation, assessment and management ofoverweight and obesity in adults andchildren. London, UK:NICE; December 2006(last updated in 2010). Available at www.nice.org.uk/CG043. Accessed February 6,2012
6. National Health and Medical ResearchCouncil. Clinical Practice Guidelines for theManagement of Overweight and Obesity inChildren and Adolescents. Canberra, Aus-tralia: NHMRC; 2003
7. Logue J, Thompson L, Romanes F, WilsonDC, Thompson J, Sattar N; Guideline De-velopment Group. Management of obesity:summary of SIGN guideline. BMJ. 2010;340:c154
8. Whitlock EP, O’Connor EA, Williams SB, BeilTL, Lutz KW. Effectiveness of weight man-agement interventions in children: a tar-geted systematic review for the USPSTF.Pediatrics. 2010;125(2). Available at: www.pediatrics.org/cgi/content/full/125/2/e396
9. McGovern L, Johnson JN, Paulo R, et al.Clinical review: treatment of pediatricobesity: a systematic review and meta-analysis of randomized trials. J Clin Endo-crinol Metab. 2008;93(12):4600–4605
10. Kelly KP, Kirschenbaum DS. Immersiontreatment of childhood and adolescentobesity: the first review of a promising in-tervention. Obes Rev. 2011;12(1):37–49
11. Oude Luttikhuis H, Baur L, Jansen H, et al.Interventions for treating obesity in chil-dren. Cochrane Database Syst Rev. 2009;(1):CD001872
12. Wilfley DE, Tibbs TL, Van Buren DJ, Reach KP,Walker MS, Epstein LH. Lifestyle inter-ventions in the treatment of childhoodoverweight: a meta-analytic review of ran-domized controlled trials. Health Psychol.2007;26(5):521–532
13. Collins CE, Warren J, Neve M, McCoy P,Stokes BJ. Measuring effectiveness of di-etetic interventions in child obesity: a sys-tematic review of randomized trials. ArchPediatr Adolesc Med. 2006;160(9):906–922
14. Collins CE, Warren JM, Neve M, McCoy P,Stokes B. Systematic review of inter-ventions in the management of overweightand obese children which include a dietarycomponent. Int J Evid-Based Healthc. 2007;5(1):2–53
15. Weiss R, Dziura J, Burgert TS, et al. Obesityand the metabolic syndrome in childrenand adolescents. N Engl J Med. 2004;350(23):2362–2374
16. Freedman DS, Dietz WH, Srinivasan SR,Berenson GS. The relation of overweight tocardiovascular risk factors among childrenand adolescents: the Bogalusa Heart Study.Pediatrics. 1999;103(6 pt 1):1175–1182
17. Reilly JJ, Methven E, McDowell ZC, et al.Health consequences of obesity. Arch DisChild. 2003;88(9):748–752
18. Garnett SP, Baur LA, Srinivasan S, Lee JW,Cowell CT. Body mass index and waist cir-cumference in midchildhood and adversecardiovascular disease risk clustering inadolescence. Am J Clin Nutr. 2007;86(3):549–555
19. Juonala M, Magnussen CG, Berenson GS,et al. Childhood adiposity, adult adiposity,
and cardiovascular risk factors. N Engl JMed. 2011;365(20):1876–1885
20. Bindler RC, Daratha KB. Relationship ofweight status and cardiometabolic out-comes for adolescents in the TEAMS study.Biol Res Nurs. 2012;14(1):65–70
21. Higgins JPT, Green S, eds. Cochrane Hand-book for Systematic Reviews of Inter-ventions. Version 5.1.0 (updated March2011). The Cochrane Collaboration, 2011.Available at: www.cochrane-handbook.org.Accessed September 2011
22. Balagopal P, Bayne E, Sager B, Russell L,Patton N, George D. Effect of lifestylechanges on whole-body protein turnover inobese adolescents. Int J Obes Relat MetabDisord. 2003;27(10):1250–1257
23. Ben Ounis O, Elloumi M, Zouhal H, et al.Effect of individualized exercise trainingcombined with diet restriction on in-flammatory markers and IGF-1/IGFBP-3 inobese children. Ann Nutr Metab. 2010;56(4):260–266
24. Davis JN, Tung A, Chak SS, et al. Aerobic andstrength training reduces adiposity inoverweight Latina adolescents. Med SciSports Exerc. 2009;41(7):1494–1503
25. Golley RK, Magarey AM, Baur LA, SteinbeckKS, Daniels LA. Twelve-month effectivenessof a parent-led, family-focused weight-management program for prepubertalchildren: a randomized, controlled trial.Pediatrics. 2007;119(3):517–525
26. Huang SH, Weng KP, Hsieh KS, et al. Effectsof a classroom-based weight-control in-tervention on cardiovascular disease inelementary-school obese children. ActaPaediatr Taiwan. 2007;48(4):201–206
27. Janicke DM, Sallinen BJ, Perri MG, et al.Comparison of parent-only vs family-basedinterventions for overweight children inunderserved rural settings: outcomes fromproject STORY. Arch Pediatr Adolesc Med.2008;162(12):1119–1125
28. Jiang JX, Xia XL, Greiner T, Lian GL,Rosenqvist U. A two year family basedbehaviour treatment for obese children.Arch Dis Child. 2005;90(12):1235–1238
29. Kitzman-Ulrich H, Hampson R, Wilson DK,Presnell K, Brown A, O’Boyle M. An adolescent
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1669 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

weight-loss program integrating family vari-ables reduces energy intake. J Am DietAssoc. 2009;109(3):491–496
30. McCallum Z, Wake M, Gerner B, et al. Out-come data from the LEAP (Live, Eat andPlay) trial: a randomized controlled trial ofa primary care intervention for childhoodoverweight/mild obesity. Int J Obes (Lond).2007;31(4):630–636
31. Park TG, Hong HR, Lee J, Kang HS. Lifestyleplus exercise intervention improves meta-bolic syndrome markers without change inadiponectin in obese girls. Ann Nutr Metab.2007;51(3):197–203
32. Reinehr T, Schaefer A, Winkel K, Finne E,Toschke AM, Kolip P. An effective lifestyleintervention in overweight children: find-ings from a randomized controlled trial on“Obeldicks light.” Clin Nutr. 2010;29(3):331–336
33. Rooney BL, Gritt LR, Havens SJ, MathiasonMA, Clough EA. Growing healthy families:family use of pedometers to increasephysical activity and slow the rate of obe-sity. WMJ. 2005;104(5):54–60
34. Sacher PM, Kolotourou M, Chadwick PM,et al. Randomized controlled trial of theMEND program: a family-based communityintervention for childhood obesity. Obesity(Silver Spring). 2010;18(suppl 1):S62–S68
35. Shelton D, Le Gros K, Norton L, Stanton-CookS, Morgan J, Masterman P. Randomisedcontrolled trial: a parent-based group edu-cation programme for overweight children.J Paediatr Child Health. 2007;43(12):799–805
36. Tsiros MD, Sinn N, Brennan L, et al. Cogni-tive behavioral therapy improves diet andbody composition in overweight and obeseadolescents. Am J Clin Nutr. 2008;87(5):1134–1140
37. Wake M, Baur LA, Gerner B, et al. Outcomesand costs of primary care surveillance andintervention for overweight or obese chil-dren: the LEAP 2 randomised controlledtrial. BMJ. 2009;339(7730):b3308
38. Díaz RG, Esparza-Romero J, Moya-CamarenaSY, Robles-Sardín AE, Valencia ME. Lifestyleintervention in primary care settingsimproves obesity parameters among Mex-ican youth. J Am Diet Assoc. 2010;110(2):285–290
39. Gillis D, Brauner M, Granot E. A community-based behavior modification interventionfor childhood obesity. J Pediatr EndocrinolMetab. 2007;20(2):197–203
40. Hughes AR, Stewart L, Chapple J, et al.Randomized, controlled trial of a best-practice individualized behavioral programfor treatment of childhood overweight:Scottish Childhood Overweight TreatmentTrial (SCOTT). Pediatrics. 2008;121(3). Avail-
able at: www.pediatrics.org/cgi/content/full/121/2/e539
41. Kalarchian MA, Levine MD, Arslanian SA,et al. Family-based treatment of severepediatric obesity: randomized, controlledtrial. Pediatrics. 2009;124(4):1060–1068
42. Kalavainen MP, Korppi MO, Nuutinen OM.Clinical efficacy of group-based treatmentfor childhood obesity compared with rou-tinely given individual counseling. [seecomment] Int J Obes (Lond). 2007;31(10):1500–1508
43. Nemet D, Barkan S, Epstein Y, Friedland O,Kowen G, Eliakim A. Short- and long-termbeneficial effects of a combined dietary-behavioral-physical activity interventionfor the treatment of childhood obesity. Pe-diatrics. 2005;115(4). Available at: www.pediatrics.org/cgi/content/full/115/4/e443
44. Nemet D, Barzilay-Teeni N, Eliakim A. Treat-ment of childhood obesity in obese fami-lies. J Pediatr Endocrinol Metab. 2008;21(5):461–467
45. Sabet Sarvestani R, Jamalfard MH, KargarM, Kaveh MH, Tabatabaee HR. Effect of di-etary behaviour modification on anthropo-metric indices and eating behaviour inobese adolescent girls. J Adv Nurs. 2009;65(8):1670–1675
46. Savoye M, Shaw M, Dziura J, et al. Effects ofa weight management program on bodycomposition and metabolic parameters inoverweight children: a randomized con-trolled trial. [see comment] JAMA. 2007;297(24):2697–2704
47. Estabrooks PA, Shoup JA, Gattshall M,Dandamudi P, Shetterly S, Xu S. Automatedtelephone counseling for parents of over-weight children: a randomized controlledtrial. Am J Prev Med. 2009;36(1):35–42
48. Fullerton G, Tyler C, Johnston CA, Vincent JP,Harris GE, Foreyt JP. Quality of life inMexican-American children followinga weight management program. Obesity(Silver Spring). 2007;15(11):2553–2556
49. Johnston CA, Tyler C, Fullerton G, et al.Results of an intensive school-based weightloss program with overweight MexicanAmerican children. Int J Pediatr Obes. 2007;2(3):144–152
50. Resnick EA, Bishop M, O’Connell A, et al. TheCHEER study to reduce BMI in elementaryschool students: a school-based, parent-directed study in Framingham, Massachu-setts. J Sch Nurs. 2009;25(5):361–372
51. Weigel C, Kokocinski K, Lederer P, Dötsch J,Rascher W, Knerr I. Childhood obesity:concept, feasibility, and interim results ofa local group-based, long-term treatmentprogram. J Nutr Educ Behav. 2008;40(6):369–373
52. Balagopal P, George D, Patton N, et al.Lifestyle-only intervention attenuates theinflammatory state associated with obesity:a randomized controlled study in adoles-cents. J Pediatr. 2005;146(3):342–348
53. Balagopal P, George D, Yarandi H, FunanageV, Bayne E. Reversal of obesity-related hypo-adiponectinemia by lifestyle intervention:a controlled, randomized study in obeseadolescents. J Clin Endocrinol Metab. 2005;90(11):6192–6197
54. Golley RK, Perry RA, Magarey A, Daniels L.Family-focused weight management programfor five- to nine-year-olds incorporating par-enting skills training with healthy lifestyleinformation to support behaviour modifica-tion. Nutr Diet 2007;64(3):144–150
55. Janicke DM, Sallinen BJ, Perri MG, Lutes LD,Silverstein JH, Brumback B. Comparison ofprogram costs for parent-only and family-based interventions for pediatric obesity inmedically underserved rural settings. JRural Health. 2009;25(3):326–330
56. Janicke DM, Sallinen BJ, Perri MG, et al.Sensible treatment of obesity in rural youth(STORY): design and methods. Contemp ClinTrials. 2008;29(2):270–280
57. Stewart L, Houghton J, Hughes AR, PearsonD, Reilly JJ. Dietetic management of pedi-atric overweight: development and de-scription of a practical and evidence-basedbehavioral approach. J Am Diet Assoc.2005;105(11):1810–1815
58. Wake M, Gold L, McCallum Z, Gerner B,Waters E. Economic evaluation of a primarycare trial to reduce weight gain inoverweight/obese children: the LEAP trial.Ambul Pediatr. 2008;8(5):336–341
59. Kalavainen M, Karjalainen S, Martikainen J,Korppi M, Linnosmaa I, Nuutinen O. Cost-effectiveness of routine and group pro-grams for treatment of obese children.Pediatr Int. 2009;51(5):606–611
60. Nemet D, Berger-Shemesh E, Wolach B,Eliakim A. A combined dietary-physical ac-tivity intervention affects bone strength inobese children and adolescents. Int JSports Med. 2006;27(8):666–671
61. Shaw M, Savoye M, Cali A, Dziura J,Tamborlane WV, Caprio S. Effect of a suc-cessful intensive lifestyle program on insulinsensitivity and glucose tolerance in obeseyouth. Diabetes Care. 2009;32(1):45–47
62. Johnston CA, Tyler C, McFarlin BK, et al.Weight loss in overweight Mexican Ameri-can children: a randomized, controlledtrial. Pediatrics. 2007;120(6). Available at:www.pediatrics.org/cgi/content/full/120/6/e1450
63. Becque MD, Katch VL, Rocchini AP, MarksCR, Moorehead C. Coronary risk incidence
e1670 HO et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from

of obese adolescents: reduction by exerciseplus diet intervention. Pediatrics. 1988;81(5):605–612
64. Botvin GJ, Cantlon A, Carter BJ, Williams CL.Reducing adolescent obesity througha school health program. J Pediatr. 1979;95(6):1060–1063
65. Braet C, Van Winckel M. Long-term follow-up ofa cognitive behavioral treatment program forobese children. Behav Ther. 2000;31(1):55–74
66. Epstein LHL, Wing RRR, Koeske RR, ValoskiAA. Effects of diet plus exercise on weightchange in parents and children. J ConsultClin Psychol. 1984;52(3):429–437
67. Mellin LM, Slinkard LA, Irwin CE Jr. Ado-lescent obesity intervention: validation ofthe SHAPEDOWN program. J Am Diet Assoc.1987;87(3):333–338
68. Rocchini AP, Katch V, Anderson J, et al.Blood pressure in obese adolescents: effectof weight loss. Pediatrics. 1988;82(1):16–23
69. Saelens BE, Sallis JF, Wilfley DE, Patrick K,Cella JA, Buchta R. Behavioral weight con-trol for overweight adolescents initiated inprimary care. Obes Res. 2002;10(1):22–32
70. Epstein LH, Valoski A, Wing RR, McCurley J.Ten-year outcomes of behavioral family-
based treatment for childhood obesity.Health Psychol. 1994;13(5):373–383
71. Kirschenbaum DS, Harris ES, Tomarken AJ.Effects of parental involvement in behavioralweight loss therapy for preadolescents.Behav Ther. 1984;15(5):485–500
72. Braet C, Van Winckel M, Van Leeuwen K.Follow-up results of different treatmentprograms for obese children. Acta Pae-diatr. 1997;86(4):397–402
73. Epstein LH, McCurley J, Wing RR, Valoski A.Five-year follow-up of family-based behav-ioral treatments for childhood obesity. JConsult Clin Psychol. 1990;58(5):661–664
74. Rocchini A, Katch V, Schork A, Kelch R. In-sulin and blood pressure during weightloss in obese adolescents. Hypertension.1987;10(3):267–273
75. Bell LM, Watts K, Siafarikas A, et al. Exercisealone reduces insulin resistance in obesechildren independently of changes in bodycomposition. J Clin Endocrinol Metab. 2007;92(11):4230–4235
76. Watts K, Jones TW, Davis EA, Green D. Ex-ercise training in obese children and ado-lescents: current concepts. Sports Med.2005;35(5):375–392
77. Falkner B, Gidding SS, Portman R, Rosner B.Blood pressure variability and classifica-tion of prehypertension and hypertensionin adolescence. Pediatrics. 2008;122(2):238–242
78. National High Blood Pressure EducationProgram Working Group on High BloodPressure in Children and Adolescents. Thefourth report on the diagnosis, evaluation,and treatment of high blood pressure inchildren and adolescents. Pediatrics. 2004;114(2 suppl 4th report):555–576
79. Rosner B, Prineas R, Daniels SR, Loggie J.Blood pressure differences between blacksand whites in relation to body size amongUS children and adolescents. Am J Epi-demiol. 2000;151(10):1007–1019
80. Golan M, Kaufman V, Shahar DR. Childhoodobesity treatment: targeting parents ex-clusively v. parents and children. Br J Nutr.2006;95(5):1008–1015
81. Shrewsbury VA, Steinbeck KS, Torvaldsen S,Baur LA. The role of parents in pre-adolescent and adolescent overweightand obesity treatment: a systematic reviewof clinical recommendations. Obes Rev.2011;12(10):759–769
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1671 by guest on June 4, 2018www.aappublications.org/newsDownloaded from

originally published online November 19, 2012; Pediatrics Neve and Clare Collins
Mandy Ho, Sarah P. Garnett, Louise Baur, Tracy Burrows, Laura Stewart, MelindaWith Meta-analysis
Effectiveness of Lifestyle Interventions in Child Obesity: Systematic Review
ServicesUpdated Information &
012-1176http://pediatrics.aappublications.org/content/early/2012/11/14/peds.2including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 4, 2018www.aappublications.org/newsDownloaded from

originally published online November 19, 2012; Pediatrics Neve and Clare Collins
Mandy Ho, Sarah P. Garnett, Louise Baur, Tracy Burrows, Laura Stewart, MelindaWith Meta-analysis
Effectiveness of Lifestyle Interventions in Child Obesity: Systematic Review
http://pediatrics.aappublications.org/content/early/2012/11/14/peds.2012-1176located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2012/11/14/peds.2012-1176.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2012 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 4, 2018www.aappublications.org/newsDownloaded from