effects 2'3
TRANSCRIPT

THE HEMODYNAMICEFFECTS OF HYPOTENSIVEDRUGSINMAN. III. HEXAMETHONIUM1, 2'3
By EDWARDD. FREIS, JOHN C. ROSE, EDWARDA. PARTENOPE,THOMASF.HIGGINS, ROBERTT. KELLEY,4 HAROLDW. SCHNAPER,AND
ROBERTL. JOHNSON
(From the Cardiovascular Research Laboratory, Georgetown University Hospital, the Depart-ment of Medicine, Georgetoun University School of Medicine, and the Veterans
Administration Hospital, Washington, D. C.)
(Submitted for publication July 7, 1952; accepted August 14, 1953)
While searching for derivatives of d-tubocura-rine, Barlow and Ing (1) and Paton and Zaimis(2) independently synthesized a series of poly-methylene bistrimethylammonium salts. The lat-ter investigators demonstrated that the pharma-cological properties of this series were related tothe length of the polymethylene chain; the deca-compound produced neuromuscular block whilethe penta and hexa-compounds prevented thetransmission of impulses across the synapses inall autonomic ganglia. They also carried out pre-liminary trials in man (3) but Arnold and Rosen-heim were the first to use these agents in hy-pertension (4). Finally, Restall and Smirkdemonstrated that it was possible to reduce bloodpressure and obtain clinical improvement in hyper-tensive patients for long periods by the use ofrepeated parenteral doses of hexamethonium (5).
Studies in this laboratory have confirmed theobservations of Restall and Smirk and in additionhave shown the potentiating effect of 1-hydra-zinophthalazine (Apresoline) when alternatedwith doses of hexamethonium in patients with hy-pertension (6, 7). Our studies also suggested thathexamethonium may be useful in the treatment of
1 Supported in part by research grants from the Na-tional Heart Institute, U. S. Public Health Service, theSquibb Institute for Medical Research, New Brunswick,New Jersey, Irwin, Neisler and Company, Decatur, Il-linois and Ciba Pharmaceuticals, Summit, New Jersey.
2 Sponsored (in part) by the VA and published withthe approval of the Chief Medical Director. The state-ments and conclusions published by the authors are a re-sult of their own study and do not necessarily reflect theopinion or policy of the Veterans Administration.
8 Hexamethonium dibromide (Bistrium) was suppliedby H. Sidney Newcomer, M.D., E. R. Squibb and Sons,New York, New York.
4 Research Fellow-Washington, D. C., Heart Associ-ation.
acute peripheral vascular disorders associated withneurogenic vasospasm as well as in the evaluationof the sympathetic vasoconstrictor component incases of peripheral vascular disease (8). Sincefrom these previous studies it appeared that hexa-methonium was a potent agent both for reducingblood pressure and increasing foot and digitalblood flow a more complete analysis of its hemo-dynamic effects seemed indicated.
METHODS
The subjects were 25 hypertensive patients admittedto the wards of Georgetown University Hospital and theVeterans Administration Hospital and four normoten-sive young males (medical students). Hexamethoniumwas administered intravenously at a rate of 1 to 2 mg.per minute for the first 15 mg. and then at a rate of 5mg. per minute, in all instances until a significant hy-potensive effect had been obtained or until 50 to 100 mg.had been administered. All dosages refer to the amountof hexamethonium ion administered.
The methods used in this investigation were essentiallysimilar to those described in a previous communication(9), with the following exceptions: the determination ofarteriovenous oxygen difference were carried out using thespectrophotometric method of Hickam and Frayser (10).The oxygen content of the expired air was determinedusing a Pauling type oxygen analyzer.5 The totalperipheral resistance was calculated according to themethod of Green, Lewis, Nickerson, and Heller (11).In the muscle blood flow experiments it was necessary toestimate the mean arterial pressure from the values forsystolic and diastolic pressure as determined by theauscultatory method. The formula used was as follows:mean arterial pressure = .436 (pulse pressure) + diastolicpressure (12). Calf blood flow was measured as previ-ously described except that a strain gage,6 with a car-
6 Model C, Arnold 0. Beckman, Inc., South Pasadena,California.
6Model P-23-B, Statham Laboratories, Beverly Hills,California.
1285

FREIS, ROSE, PARTENOPE, HIGGINS, KELLEY, SCHNAPER, AND JOHNSON
rier-wave type amplifier and direct writing oscillograph,7replaced the Brodie's bellows apparatus. Glomerular fil-tration rate was determined by the clearance of sodiumthiosulfate (13).
RESULTS
I. Cardiac functionCardiac output, mean arterial pressure and total
peripheral resistanceThe changes in cardiac output and total periph-
eral resistance seemed to vary with the state ofcardiac compensation. In the hypertensive pa-tient with a compensated heart the usual responseto hypotensive doses of hexamethonium was aslight decrease in cardiac output. Thus, in 11 post-treatment analyses carried out in six patients with-out heart failure the cardiac output decreased by 6to 38 per cent (mean 22.0 per cent, S.D. 9.3)(Table I, Cases 1 through 6). The decrease inmean arterial pressure was of similar magnitudevarying from 10 to 37 per cent (mean 23.5 percent, S.D. 7.0). In only one instance did the ar-terial pressure fall to normotensive levels. Thetotal peripheral resistance did not change signifi-cantly varying between + 19 and - 22 per cent(mean - 1.3 per cent).
In contrast, in four additional patients withcongestive heart failure and one with malignanthypertension there was a significant increase incardiac output in three and a slight increase intwo patients following hexamethonium. Therange for nine post-treatment determination was+ 3 to 100 per cent and the mean 38 per cent,S.D. 35.4 (Table I, Cases 7 through 11). Inthese instances the total peripheral resistance fellsignificantly the range being 27 to 70 per centand the mean 47 per cent, S.D. 14.1.
Other aspects of cardiac functionThe heart rate usually increased moderately after
hexamethonium. There were insignificant changesin rate in three patients, slowing in one and rises insix cases; the average increase was 14 beats perminute (Table I).
Pressures on the right side of the circulationwere measured in seven patients and decreased inall instances. In the group with compensated
7 Model 140-C, Sanborn Company, Cambridge, Massa-chusetts.
hearts the pulmonary arterial pressure decreasedin patient W. C. from 26/14 to 14/8 mm. Hg. Inpatient B. J. the right ventricular pressure de-creased from 38/12 to 22/4 mm. Hg (Figure 1).In subject C. A., the mean right auricular pres-sure decreased from - 0.5 to - 2.5 mm. Hg. Inthe decompensated patients the pulmonary ar-terial pressure decreased in patient T. P. from45/22 to 20/12 mm. Hg and in subject R. S. from70/40 to 40/15 mm. Hg. The right ventricularpressures fell in subject J. C. from 115/25 to 85/18mm. Hg and in subject A. C. from 130/20 to 80/8mm. Hg. The decline in right heart pressuresparalleled the fall in systemic arterial pressure.
II. Blood Flow Through Various RegionsBlood flow through the muscles (calf blood flow)
In a previous communication it was pointed outthat a ten-fold increase in foot (primarily skin)blood flow occurred after hexamethonium (14).In the calf segment (primarily muscle) an in-creased blood flow as determined by the plethysmo-graphic method also was observed but to a muchsmaller degree than that observed in the foot(Table II).
Ten hypertensive patients were studied. Twopatients in the malignant phase had previous ther-apy with hexamethonium while the remainingeight were patients with essential hypertensionwho had received no previous treatment withhexamethonium. In the latter eight cases all ex-hibited an increase of muscle blood flow varyingfrom 11 to 61 per cent (mean 39.4 per cent) ofthe control values. The crude peripheral resist-ance decreased by 26 to 56 per cent (mean 40.4per cent). The increase of blood flow began simul-taneously with the decrease of blood pressure andsome increase persisted for at least an hour.
The two patients who had malignant hyperten-sion and who had been under continuous dosagesof hexamethonium immediately prior to testingshowed a decrease of blood flow in one instanceand no change in the other. It could not be deter-mined from this limited data whether these atypi-cal responses were associated with the developmentof tolerance to the vasodilating properties of thedrug or represented a response peculiar to patientsin the malignant phase of hypertension.
1286

1287HEXAMETHONIUMK:HEMODYNAMICEFFECTS
'r-O %o_ t w o
S~~~~~~~~~% 00 U) C4 in mtS te
X~~~~~~~~~~~~~~~~~~~~~ 00Om%o m N +e t
11~~~~~~~00i011 o OQo-0O
et 63 t; e ~~04t m.40o4 lqdoo4o0oV.-oO
o coX ONco
U 08
Xg Pte t~~~~~oooo. U.o o.4 C.4 C4 10 q%
"11 to ~ ~~~~1,4 x-) U) in t oin I
S||' X I i ~~~CO C1 C4CO C4Clq C C4C
@Z*te4mPb b va ux uo uz u) W \03~~~C4 c
4- C'2C;SZ coo oN o co N
3 o U
4*0 ed 6 Y U Y Y Y ee Y.u0
I SsE1z Z & ¢ ti.g S Ko ¢ | Soat~~~~~~~~~~~~~~~~~~~~~~uw4,- o Oi

ROSE, PARTENOPE, HIGGINS,
*100. o
$0o 11.11*1*)
'1)0w
009E
00
KELLEY, SCENAPER,
O0.Ocoow0*0* 0*0
t.. 10inc
( WI) U1) coCh t- 00 00
- -"
%C
- -I
(90iPpv
a oo
tk- co
00-d
co
-00% C%
.Sit Go in
'4414i 9
t0%0
i -(9o!9- 9-
i
o
U)v B2t
C4 C
LI) if)V-4 "'
00
oo(9oo4
C( (4- '4
V-
e00
e cococo) 00
* z
o*
l1)
a co
00o4
0011) 1)
00~o C'0(9
o~~~~~'(
('4
000to No00
0o 0%
000 0
(V) (V)
00
to O
0 0
000ON00V- V-
AND JOHNSON
cooo000('4 ('4
11) (9
coc
CE) (9
-o O
_ _0
01)¢
l1)114
C%4
_ 11
00a
-(
(9(
G0 0- -0 co
co ONb 400 U1) 0% (9e
§,[;Ll >%.° t ~~~~~~~~~~~~~S. t < t: MS>otHS>I~~~~~~~~~~Co 0~~~~~~~~~~~~~.I.
1288
I
p1I9414
EREIS,
Fil
()0
0 3U
cn
.44
iS0'1
.4-
Cd
-1-
HEXAMETHONIUM:HEMODYNAMICEFFECTS
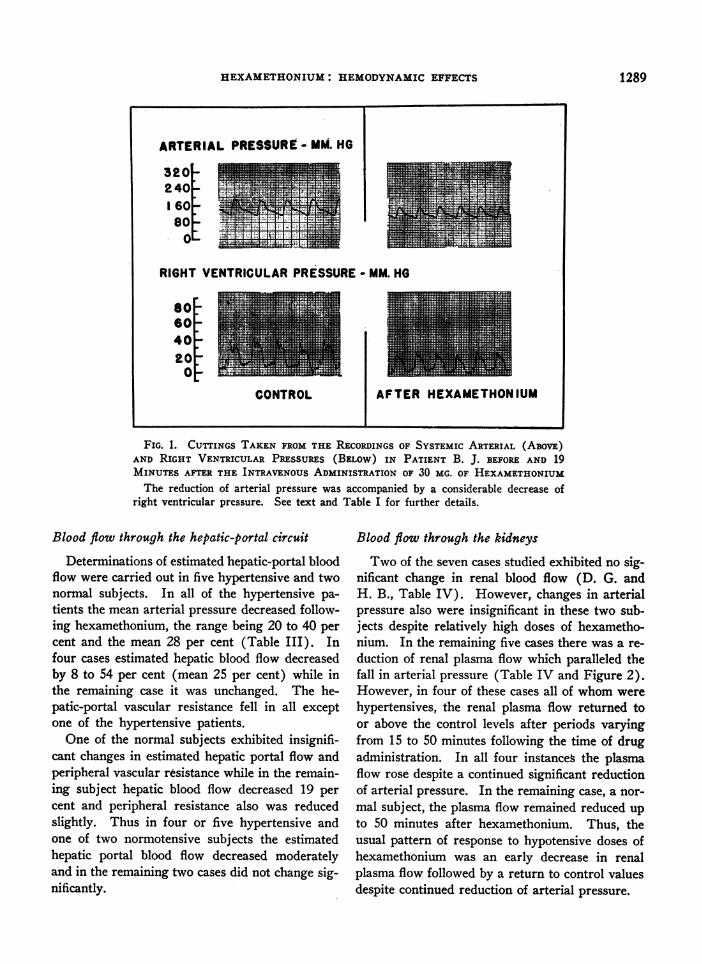
FIG. 1. CUTTINGS TAKEN FROMTHE RECORDINGSOF SYSTEMIC ARTERIAL (ABoVE)AND RIGHT VENTRICULAR PRESSURES (BELOW) IN PATIENT B. J. BEFORE AND 19MINUTES AFTER THE INTRAVENOUSADMINISTRATION OF 30 MG. OF HEXAMETHONIUM
The reduction of arterial pressure was accompanied by a considerable decrease ofright ventricular pressure. See text and Table I for further details.
Blood flow through the hepatic-portal circuit
Determinations of estimated hepatic-portal bloodflow were carried out in five hypertensive and twonormal subjects. In all of the hypertensive pa-
tients the mean arterial pressure decreased follow-ing hexamethonium, the range being 20 to 40 per
cent and the mean 28 per cent (Table III). Infour cases estimated hepatic blood flow decreasedby 8 to 54 per cent (mean 25 per cent) while inthe remaining case it was unchanged. The he-patic-portal vascular resistance fell in all exceptone of the hypertensive patients.
One of the normal subjects exhibited insignifi-cant changes in estimated hepatic portal flow andperipheral vascular resistance while in the remain-ing subject hepatic blood flow decreased 19 per
cent and peripheral resistance also was reducedslightly. Thus in four or five hypertensive andone of two normotensive subjects the estimatedhepatic portal blood flow decreased moderatelyand in the remaining two cases did not change sig-nificantly.
Blood flow through the kidneys
Two of the seven cases studied exhibited no sig-nificant change in renal blood flow (D. G. andH. B., Table IV). However, changes in arterialpressure also were insignificant in these two sub-jects despite relatively high doses of hexametho-nium. In the remaining five cases there was a re-
duction of renal plasma flow which paralleled thefall in arterial pressure (Table IV and Figure 2).However, in four of these cases all of whomwere
hypertensives, the renal plasma flow returned toor above the control levels after periods varyingfrom 15 to 50 minutes following the time of drugadministration. In all four instances the plasmaflow rose despite a continued significant reductionof arterial pressure. In the remaining case, a nor-
mal subject, the plasma flow remained reduced up
to 50 minutes after hexamethonium. Thus, theusual pattern of response to hypotensive doses ofhexamethonium was an early decrease in renalplasma flow followed by a return to control valuesdespite continued reduction of arterial pressure.
ARTERIAL PRESSURE MM. HG
320
h0 a|Ms
240
1 6
t ~~~~~~~~~~~~~~~...' aS S Z; _ m....~~~~~~~~~.... Eg
RIGHT VtENTRICULAR PRESSURE- MM. HG
40
I _r = I M
AFTER HEXAMETHONIUMCONTROL
1289

FREIS, ROSE, PARTENOPE, HIGGINS, KELLEY, SCHNAPER, AND JOHNSON
e ~ ~ ~~~~++
t ~~I I +
*
Qen++Sen~~i % t.00M 0"ow-o W%0oron o Cow
_-- ('4 ('4 ('4 -I V(4)
0o
e~~~~~~~~c in U- to 00t +M0 ' o( )t n
A N 44Me++ + I
$cE -^ 00 _-
tmmmmmmm~~~~-OOr --S t m ++ e e Z
X ~ ~ ~ ~
_
an oo t-o m o mo m e o c m t t o
0U1)
% 00 o G0 4o
Et C14 C14 Mc4
Ai
ouWI)co co t
C~4 4
00 00 0 01r)t- 'O00 00 t
9-_____W"9-
0'I)
100
U)'
co4.
00W-
- '4 0('14(
0 00 W'4 t"-
"011 '1)0V
noo
% % o co_
-4 -" W4
'oU1)
I
0o 0-4" C4 C4
+
'1m)")"%6 Il if tr
01f)U) 11)
0% 0% 0% 0%0ON)01O1 () 04
1000co MU)i to
00
t' C-00 0(40%
_-_- ('4 C(4 4
0 1) '..
-('4
'1)011)11)N - N
o U" V)4
C? C4 q*
0004C'4
10
z4
'O ('4
e) )In
U1) t)
(64 c4('
000
to U) if)
'0
0
4.14.#E4Sa* X >,N4w.=
1290
d
.C0
.0
0)
I,
ii
qii
b4
10
4)
10
-4
0
10
V0
, &.41gC3
..40
m
1. .
C4
Z10
*
v
xA

HEXAMETHONIUM:HEMODYNAMICEFFECTS
I I
00%0%000 ONrt'r.o RJ40ON0oI-U)in ONts'r.0 0_-+ - V4)+4U)U) _ CN4C
+ '+
c C~4'-400000C- Ui '-40
eq
- - -- - - - -
U 4 0% 00 %0 0%- q U)
00eq
0% 0% t-s0ot- t
o t- 0o
000
* * -4
U) U) U)r' 'o0_" _
t'.2'0 U - t' 0
- ------ -
- -- - - -- -
- eq +4 U)'
0
'0Uin U) '- '
U) 0Ub) U) U)
_) eq In to U)ta" t'. t~- a"- a
* . . . .
%O*RV
I%OC4
1
0o --I0%0 U) C 4e1c4 014 E)U)U)U)MM
U) +q+4
0000 Ul) 0 0 eq4 Il4Id
~'0 Nr 00 eq NO
*q . i . . . .
- eq U) U)
0 U - U) --
0 t'- 00 U)
_ - __4ele6e
0% 0% 0% 0%- --
CN _U
eqU)
0 0
co 4m3wt~~~~~~~~~~~~~~U
so~~~~~~~~~~~~>
u$
1291
*
+
0000
C --4-
eq e
@4U) 04 C4
o C4mU)
NO N O00U)-4 U) '4 U); -
Ol ON 00 o0%
-- -- -
U) 0 in U) 0q U)U) t-
bo
00
ac
tie
N.'
)5U80(4
.0
A¢
'IA
1-
0
0u
0U)
r.
t3
m¢.
*xt 0%
.tIlt -
040
51 C4.e:, eq
2" eq'0
oo- -
000
- - -0002--. 24 2"
- - -
0W)
0%eq
0co*e.d
¢ a*|!>3;i ;-
00
-"'MCd0.(L)ci
4Jt911 Kw>,O.W.=

FREIS, ROSE, PARTENOPE, HIGGINS, KELLEY, SCI
_o M . (1c0%r1 t'.t .'lcoe'Q o.
*: ~ ... . ..+.+.o .r .e .
I,~~~~~iMvrz z c 0 ror -1
'40CN4t- 00 0%0% '- - C~1C M ~Zs~~~~~- co0A 000e t- t-o-Ct
oIn co
o
c
V-4 V- V-- ---4 --4 V-4 -V-
i .~e4001~e~I404C- t- t- )0Ai t0- -e --
0
Z: g nco t m Chco°D
o. W InNONO) - - -qmm(E) 00 -- - q.
0 X9
0CE 0 t- " t- ON00o 0 00 000ON coNo W o (
co :4 ' -t 00 00 In)11) 000 0 '( V4)J 00 V- '011l) 11)04%o" -W
¢ oo -d to
00 00 eqi 0'
Ola
.84-}
EINAPEX, AND
e4 c 0%m)'0 e4OSi0C1 en a Io0- oooo
- C- O-F--
O< m l) in
0%s '0 I0C 0' 0
U)O0%Ow O%"(4"
0 0U) 0
~0 t(14 %O 4
o t001)4
0%
4
WI
C-0C:r
JOHNSON
0 t- 0% mE I-~~0%000-0'-
0 C:Fk00 Q'0in1)11 V'0IR
o o co No
NOLO o) X
C14oo In
1292
.le,4
m
*wb1~
U) U) U)cooo
C1 C%lC1U) U) U)
C~4 0% ONco t- t'.
0.
I
0
I...
*L
4)4J
*1a
Ei*_Ca
laIm0
C4rl. -iV-0 (4

HEXAMETHONIUM:HEMODYNAMICEFFECTS
eqinoo- ino U-) NOtr.. 0 ooZ-U et4 O_Sa~~~~~~~~~~~~~~~~~~~~, e6 e6 cl r. senSbr.: ui o
n e.-o~~~CNoOm0 eIn > Ne4 o +0+04_0%
sCui&O in NO t- NONO ld k-1o%O_-o00%k 00
o
.04 clq t-*00N Wm I* 1-q* m 0-00 r- 00 NO 0 00 C
a~~~ ~~~0t A. oN ZZ4 (4 eNOm400mO"14mmdC4NGC4 enwin ONn emtC1 4 4v-
.;0% wt-_ _ toab 'IO -_4_ ___ r o 0
to0iE $ XoXo U) i+o SNo X o inoooo
Aot XW an_X V-_MIn _Xe4
X~~~~~~~~~~~~~~~~~~~~~C O
>~~~~~~~~~~~~~~~~~~1Oi*id4" tz N O
<: e me.0 e~~~~t co0- v- .00+oto0o n o
G-oeW0et.X>> mb oret~~~~~Q~v.- 000 0 r_
& mg t . ZZ etOItin C%4 -4
C- C'14ooo mm 14 Ne IF4 to m o %
C40m Ge0 o00"!00
"lot_- _, v.. _- coo
ooooc"I NO cooo00 t 0" 1w e NOco 000N0mC1
C4 04 V-. V- .V- .W- W-.04
"cd0 I33 0nt 03t co
1293

FREIS, ROSE, PARTENOPE, HIGGINS, KELLEY, SCHNAPER, AND JOHNSON
FIG. 2. CHARTOF EFFECTIVE RENALPLASMAFLOW, GLOMERULARFILTRATION RATE,FILTRATION FRACTION, URINE VOLUMEANDARTERIAL PRESSUREBEFOREANDAFTER THEINTRAVENOUSADMINISTRATION OF 40 MG. OF HEXAMETHONIUMION IN PATIENT A. Z.
In the early period there was a decrease in renal plasma flow, glomerular filtrationrate and urine volume. However, 45 minutes after hexamethonium renal plasma flowhad returned to and glomerular filtration rate approached control values despite con-tinued significant reduction in filtration fraction, urine volume and arterial pressure.
III. Other Aspects of Renal Function
Glomerular filtration rate was determined insix of the subjects listed in Table IV. In threehypertensive patients there was a reduction ofglomerular filtration rate followed by a rise to-ward but not to the control values (A. Z., A. S.,and M. Y., Table IV and Figure 2). In one hy-pertensive and one normal subject there was acontinued fall in glomerular filtration rate through-out the experimental period. The final normalsubject who had exhibited no significant changein arterial pressure or renal blood flow alsoshowed no change in glomerular filtration rate.It was apparent, therefore, that the rate of glo-merular filtration decreased paralleling the bloodpressure fall and complete compensation usuallydid not occur during the experimental period. Thefiltration fraction decreased in all of the hyperten-
sive patients. In the two normal subjects therewas no significant change in the patient whoshowed no reduction of arterial pressure and aslight rise in filtration fraction in the other.
The volume of urine flow did not change in thetwo cases who exhibited insignificant reductionof arterial pressure (D. G. and H. B., Table IV).Four of the five remaining cases exhibited a reduc-tion of urine volume which persisted throughoutthe experimental period. The final patient (C. S.)exhibited a slight rise in urine volume.
DISCUSSION
Previous hemodynamic studies in this labora-tory demonstrated that hexamethonium producesa marked to complete abolition of such vasocon-strictor reflexes as the vasopressor "overshoot"following the Valsalva maneuver, the cold pres-
1294

HEXAMETHONIUM:HEMODYNAMICEFFECTS
sor response and the reflex vasoconstrictions to"noxious" stimuli as determined by digital plethys-mography (15). As would be expected followingsuch inhibition of moderator reflexes by a gangli-onic blocking agent the pressor responses to epi-nephrine and norepinephrine were augmented con-siderably, after as compared to before, hexametho-nium (16). In a constant temperature cold roomthe increase in foot blood flow was as great fol-lowing hexamethonium as after extradural orintrathecal anesthesia in normal subjects, suggest-ing nearly complete ganglionic blockade in man(14). In addition, probably by reason of theinhibition of vasoconstrictor reflexes, hexametho-nium was found to induce marked hypotension innormal or hypertensive subjects following minordegrees of blood loss such as that occasioned bythe brief application of venous tourniquets to theextremities or by small venesections of 250 to 500cc. of blood (17). Thus, the previous studies dem-onstrated that hexamethonium in man interfereswith transmission of sympathetic vasoconstrictorimpulses more completely than any previouslyknown agent. The present investigation has de-termined the effects of such widespread inhibitionof sympathetic impulses on cardiovascular dy-namics.
In the patients who did not exhibit congestiveheart failure and whose cardiac outputs were inthe normal range, the hypotensive response tohexamethonium was accompanied by a decreasedcardiac output and little or no change in totalperipheral resistance. These observations arein approximate agreement with those of Werko,Frisk, Wade, and Eliasch (18), but are opposedto those of Gilmore, Kopelman, McMichael, andMilne (19) who found essentially no change incardiac output after hexamethonium. Thus, the,reduction of arterial pressure in the present seriesseemed to be secondary to a diminished cardiacoutput rather than to arteriolar vasodilation. Thedecreased cardiac output in turn appeared to bedue to a failure of venous return since the pres-sures on the right side of the circulation were re-duced uniformly.
The failure of venous return probably was pro-duced by pooling of blood in the peripheral circu-lation. Such pooling could be due to (1) an in-crease in the total vascular capacity, and (2) theblockade of reflex vasoconstrictor responses (17).
By contrast in the patients with congestive heartfailure or malignant hypertension the decreasesin systemic and right heart pressures were ac-companied by an increased cardiac output and de-creased total peripheral resistance. These di-vergent observations in the patients with heartfailure as compared to compensated subjects maybe explained, however, in the light of the followingconsiderations: first, in the case of the heart fail-ure subjects the peripheral pooling of blood in-duced by hexamethonium would act like a vene-section reducing the loading pressure of the con-gested right side of the heart thereby facilitatingits recovery. Second, it is evident that pa-tients with this type of heart failure are in astate of elevated vasoconstrictor tone since nor-mal or elevated levels of systemic arterial pressureare maintained despite a cardiac output whichusually is reduced. Hexamethonium by its block-ing action on vasoconstrictor reflexes abolishesthis increased tone thus permitting a decrease intotal peripheral resistance and thereby also in thedemand for cardiac work. These considerationsand their implications in regard to the nature ofcongestive heart failure have been discussed morefully in another communication (20).
Muscle blood flows increased only moderately,while renal and hepatic-portal blood flows fellduring the maximum action of the drug. Footblood flow increased approximately ten fold (14)but since this vascular area is small in relation tothe total vasculature the decrease in vascular re-sistance in the foot had little influence on the totalperipheral resistance. These results suggest thatthere is an uneven distribution of sympatheticvasocontrictor nerves in different vascular areas.Only in a single region, the distal parts of the ex-tremities, was a marked increase in flow observed.In the other and larger vascular areas (muscles,hepatic-portal and renal vascular beds) moderateincreases or actual decreases in flow occurredwhile the total peripheral resistance usually wasonly slightly reduced. These data do not sup-port the view that the sympathetic vasoconstric-tor system is of great importance in regulatingarteriolar tone in the resting, supine subject ex-cept for its role in temperature regulation of theskin particularly of the distal parts of the extremi-ties. The results also emphasize the fallacies in-herent in drawing conclusions as to the overall
1295

FREIS, ROSE, PARTENOPE, HIGGINS, KELLEY, SCHNAPER, AND JOHNSON
vasodilating effects of agents which increase skintemperature, color or blood flow.
The hemodynamic effects of hexamethonium,however, are due to more than simple inhibitionof sympathetic vasoconstrictor nerves since thedrug interferes with transmission through allautonomic ganglia. Vasodilator nerves whichsynapse in the ganglia as well as vasoconstrictorimpulses will be inhibited. For example, blockadeof vasodilator impulses is seen in the cessation ofsalivary flow following the drug (21). Thus, theresults observed after hexamethonium may be inreality the net effect of combined inhibition ofautonomic vasoconstrictor and vasodilator im-pulses.
The pattern of change in renal function wasqualitatively similar to that observed after certainother hypotensive agents including veratrum viride(9), the dihydrogenated alkaloids of ergot (22)and sodium nitrite given as a single, oral dose (23).The renal vasculature did not share in the decreasein vascular resistance associated with the fall inarterial pressure. This is indicated by the factthat the renal plasma flow decreased sharply atthe onset of the hypotensive response regardlessof the drug used. However, as the arterial pres-sure stabilized at a lower level or began to risethe resistance of the renal vessels decreased to per-mit a return to normal rates of plasma flow. Thiseffect, which was first observed by Smith and hisco-workers folowing spinal anaesthesia, has beeninterpreted by him as indicating an autonomy ofthe renal arterioles (24).
A recent study by Machinnon indicated that theclosely related compound, pentamethonium pro-duced a decrease in renal blood flow in both nor-motensive and hypertensive subjects (25). How-ever, the design of his experiments was such thatonly the early hypotensive response to the drugwas studied. Thus, insufficient time was allowedto permit observation of the later return of renalplasma flow to control levels. Mills, Moyer, andHandley found no change in renal clearances fol-lowing hexamethonium in normal subjects butobserved some diminution in hypertensive patients(26).
As a result of the percentally greater fall inglomerular filtration rate than in plasma flow therewas a decrease in filtration fraction which in hy-pertensive subjects approached normal values.
The urine during this period became quite con-centrated suggesting that tubular function wasnot significantly impaired. This pattern of changehas been observed with hypotensive agents of alltypes tested in this laboratory (23) and thereforeprobably is secondary to the sudden alteration ofarterial pressure rather than to any specific actionof individual drugs on the kidney.
From the point of view of effects on hemody-namics the response to hexamethonium does notappear to be entirely desirable. Thus, cardiacoutput may decrease, renal clearances especiallyglomerular filtration rate fall at least temporarilyand homeostatic, vasomotor reflexes are seriouslycompromised. However, despite these apparentlyundesirable. and abnormal acute actions, the clini-cal response to hexamethonium frequently hasappeared to be beneficial (5, 7, 8). These corre-lative clinical and experimental studies empha-size the fact that the results of hemodynamic analy-sis need not always indicate the desirability of agiven agent in clinical practice where other fac-tors may determine the usefulness of the drug.
SUMMARYAND CONCLUSIONS
Hexamethonium administered to hypertensiveand normal subjects produces the following hemo-dynamic effects.:
1. In hypertensive patients who do not havecardiac decompensation the reduction of systemicarterial pressure is accompanied by a decrease inright heart pressures and cardiac output. The totalperipheral resistance does riot change significantly.It is suggested that these alterations are the re-sult of a combination of "venous pooling" and fail-ure of reflex vasoconstriction.
2. In patients with heart failure the fall in sys-temic arterial pressure appears to be accompaniedby a reduction of right heart pressures, an in-crease in cardiac output and a significant decreasein total peripheral resistance. These alterationsmay be due to unloading of the congested rightside of the heart as well as to inhibition of vasocon-strictor reflexes activated by the low output heartfailure.
3. In contrast to the marked increase in bloodflow in the foot observed previously, blood flowthrough the muscles increases only moderately.Since the arterial pressure falls after hexametho-
1296

HEXAMETHONIUM:HEMODYNAMICEFFECTS
nium a significant decrease in peripheral resistanceis assumed to occur in this area.
4. Despite a moderate reduction of hepatic vas-cular resistance estimated hepatic-portal blood flowusually decreases after hexamethonium.
5. Renal plasma flow decreases paralleling theinitial fall in arterial pressure and then rises to ap-proximate control levels despite a continued hypo-tensive response. This is consistent with previousobservations indicating an autonomy of tone of therenal arterioles.
6. In most cases the changes in glomerular fil-tration rate follow a pattern similar to the altera-tions in renal plasma flow, but occasionally filtra-tion may remain below control values. Oliguriawith increased concentration of urine usually oc-curs. All of these renal effects begin to diminishafter 30 to 60 minutes despite continued signifi-cant hypotension.
7. The studies to date suggest that sympatheticvasoconstrictor nerves blocked by hexamethoniumexert the controlling influence on homeostatic ad-justments to postural change as well as in main-taining the tone of the vessels of the distal partof the extremities. However, in resting supinesubjects such nerves appear to exert a much lessimportant influence on arteriolar tone in the he-patic-portal, renal and muscle areas.
ACKNOWLEDGMENT
The authors wish to thank Miss Jean Pietras for valu-able technical assistance.
REFERENCES
1. Barlow, R. B., and Ing, H. R., Curare-like action ofpolymethylene bisquaternary ammonium salts.Nature, 1948, 161, 718.
2. Paton, W. D. M., and Zaimis, E. J., Clinical poten-tialities of certain bisquaternary salts causingneuromuscular and ganglionic block. Nature, 1948,162, 810.
3. Organe, G., Paton, W. D. M., and Zaimis, E. J.,Preliminary trials of bistrimethylammonium de-cane and pentane diiodide (ClO and C5) in man.Lancet, 1949, 1, 21.
4. Arnold, P., and Rosenheim, M. L., Effect of penta-methonium iodide on normal and hypertensive per-sons. Lancet, 1949, 2, 321.
S. Restall, P. A., and Smirk, F. H., The treatment ofhigh blood pressure with hexamethonium iodide.New Zealand M. J., 1950, 49, 206.
6. Freis, E. D., Methonium compounds in hypertension.Letter to the editor. Lancet, 1951, 1, 909.
7. Freis, E. D., Finnerty, F. A., Jr., Schnaper, H. W.,and Johnson, R. L., The treatment of hypertensionwith hexamethonium. Circulation, 1952, 5, 20.
8. Finnerty, F. A., Jr., and Freis, E. D., Clinical ap-praisal of hexamethonium (C6) in peripheral vas-cular diseases. New England J. Med., 1951, 245,325.
9. Freis, E. D., Stanton, J. R., Culbertson, J. W., Litter,J., Halperin, M. H., Burnett, C. H., and Wilkins,R. W., The hemodynamic effects of hypotensivedrugs in man. I. Veratrum viride. J. Clin. Invest.,1949, 28, 353.
10. Hickam, J. B., and Frayser, R., Spectrophotometricdetermination of blood oxygen. J. Biol. Chem.,1949, 180, 457.
11. Green, H. D., Lewis, R. N., Nickerson, N. D., andHeller, A. L., Blood flow, peripheral resistance andvascular tonus, with observations on the relation-ship between blood flow and cutaneous temperature.Am. J. Physiol., 1944, 141, 518.
12. B6ger, A., and Wezler, K., Die Bestimmung des ar-teriellen Gasamtwiderstandes am Menschen. Arch.f. exper. Path. u. Pharmakol., 1937, 186, 43.
13. Pitts, R. F., Lotspeich, E. D., Schiess, W. A., andAyer, J. L., Renal regulation of acid-base balancein man. I. Nature of the mechanism for acidify-ing urine. J. Clin. Invest., 1948, 27, 48.
14. Schnaper, H. W., Johnson, R. L., Tuohy, E. B., andFreis, E. D., The effect of hexamethonium as com-pared to procaine or metycaine lumbar block onthe blood flow to the foot of normal subjects.J. Clin. Invest., 1951, 30, 786.
15. Finnerty, F. A., and Freis, E. D., Experimental andclinical evaluation in man of hexamethonium (C6),a new ganglionic blocking agent. Circulation,1950, 2, 828.
16. Freis, E. D., MacKay, J. C., and Oliver, W. F., Theeffect of "sympatholytic" drugs on the cardiovas-cular responses to epinephrine and norepinephrinein man. Circulation, 1951, 3, 254.
17. Freis, E. D., Stanton, J. R., Finnerty, F. A., Jr.,Schnaper, H. W., Johnson, R. L., Rath, C. E., andWilkins, R. W., The collapse produced by venouscongestion of the extremities or by venesection fol-lowing certain hypotensive agents. J. Clin. In-vest., 1951, 30, 435.
18. Werko6, L., Frisk, A. R., Wade, G., and Eliasch, H.,Effect of hexamethonium bromide in arterial hy-pertension. Lancet, 1951, 2, 470.
19. Gilmore, H. R., Kopelman, H., McMichael, J., andMilne, I. G., The effect of hexamethonium bromideon the cardiac output and pulmonary circulation.Lancet, 1952, 2, 898.
20. Kelley, R. T., Freis, E. D., and Higgins, T. F., Theeffects of hexamethonium on certain manifestationsof congestive heart failure. Circulation, 1953, 1, 169.
1297

FREIS, ROSE, PARTENOPE, HIGGINS, KELLEY, SCHNAPER, AND JOHNSON
21. Freis, E. D., Unpublished observations.22. Freis, E. D., Stanton, J. R., Litter, J., Culbertson,
J. W., Halperin, M. H., Moister, F. C., and Wilkins,R. W., The hemodynamic effects of hypotensivedrugs in man. II. Dihydroergocornine. J. Clin.Invest., 1949, 28, 1387.
23. Freis, E. D., Stanton, J. R., Litter, J., Culbertson,J. W., Halperin, M. H., Moister, F. C., and Wilkins,R W., Hemodynamic effects of hypotensive agentsin man. Am. J. Med., 1949, 7, 414.
24. Smith, H. W., Rovenstine, E. A., Goldring, W.,
Chasis, H., and Ranges, H. A., The effects ofspinal anesthesia on the circulation in normal, un-
operated man with reference to the autonomy ofthe arterioles, and especially those of renal circu-lation. J. Clin. Invest., 1939, 18, 319.
25. Machinnon, J., Effect of hypotension-producing drugson the renal circulation. Lancet, 1952, 2, 12.
26. Mills, L. C., Moyer, J. H., and Handley, G. A., Ef-fect of hexamethonium (C6) on renal hemody-namics. Laboratory and clinical evaluation. Am.J. Med., 1952, 13, 103.
1298