effects of le fort i osteotomy on airway
TRANSCRIPT
Q8
Q26
Q27
Q9
Q10
1
2
3
4
5
6
7
89
10
11
12
13
14
15
1617
18
19
20
21
22
23
2425
26
27
28
29
30
31
3233
34
35
36
37
38
39
4041
42
43
44
45
46
47
4849
50
51
52
53
54
55
56
CRANIOMAXILLOFACIAL DEFORMITIES/COSMETIC SURGERY
57
Gla
Co
Gla
Gla
Gla
Gla
58
59
60
61
62
63
6465
Effects of Le Fort I Osteotomy onthe Nasopharyngeal Airway—6-Month
Follow-Up
*Depar
sgow, U
yPostgrllege, G
zMedic
sgow, U
xPostgrsgow, U
kConsusgow, U
{Professgow D
66
67
68
69
70
Mohammed Almuzian, BDS, MScOrtho, MScHCA, DClinDentOrtho,*
Anas Almukhtar, BDS, MScOrtho,y Xiangyang Ju, BEng, PhD,zAli Al-Hiyali, BDS, MScOMFS,x Philip Benington, BDS, MSc,k
and Ashraf Ayoub, BDS, MDS, PhD{
717273
74
75
76
77
78
79
8081
82
83
84
85
86
87
8889
90
91
92
93
94
95
9697
98
Purpose: The literature discussing the impact of a single Le Fort I osteotomy on nasopharyngeal airwaysis limited. This study assessed the volumetric changes in the nasopharyngeal airway after a single Le Fort I
osteotomy and explored the correlation between these changes and 3-dimensional surgical movements of
the upper jaw.
Materials and Methods: This retrospective study was conducted in 40 patients who had undergone a
single Le Fort I (maxillary advancement with or without impaction) to correct Class III malocclusion from
maxillary hypoplasia. Preoperative (T1) and 6-month postoperative (T2) cone-beam computed tomo-
graphic (CBCT) scans of these patients were used for analysis. Maxillary surgical movements and volu-
metric changes in the nasopharyngeal airway were measured. The reproducibility of the measurements
was evaluated using paired t tests and intraclass correlation coefficients. The Wilcoxon test and Pearson
correlation coefficient were applied to evaluate the importance of volumetric changes in the nasopharyn-geal airway space and assess the correlations of these changes to the maxillary surgical movements.
Results: Six patients were excluded from the study owing to major differences (>5�) in their head andneck posture between the T1 and T2 CBCT scans. The errors of the repeated measurements were insig-
nificant (P > .05), with a high level of agreement (r = 0.99; P < .05) between the repeated digitization
of the landmarks. There was a statistically significant impact of a Le Fort I osteotomy on the right maxillary
sinus (decreased by 17.8%) and the lower retropalatal space (expanded by 17.3%; P < .05). The correlation
between the change in airway volume and the magnitude of surgical maxillary movements was moderate
(r = .4). Similarly, there was a moderate correlation between changes in the upper nasopharynx and those
in the hypopharynx.
Conclusion: The single Le Fort I osteotomy was found to increase the retroglossal airway volume. This
could be important for the treatment of obstructive sleep apnea in patients with maxillary deficiency.
A long-term follow-up assessment of a larger sample with a functional assessment of airwaywould be bene-
ficial to confirm these findings.� 2015 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg -:1-12, 2015
tment of Orthodontics, GlasgowDental Hospital & School,
K.
aduate Student, Glasgow University Medical School, MVLS
lasgow Dental Hospital & School, Glasgow, UK.
al Devices Unit, NHS Greater Glasgow and Clyde,
K.
aduate Student, Glasgow Dental Hospital & School,
K.
ltant Orthodontist, Glasgow Dental Hospital & School,
K.
sor, Department of Oral and Maxillofacial Surgery,
ental Hospital & School, Glasgow, UK.
Address correspondence and reprint requests to Dr Almuzian:
Department of Orthodontics, Glasgow Dental Hospital and School,
378 Sauchiehall Street, Glasgow, UK; e-mail: dr_muzian@hotmail.
com
Received February 23 2015
Accepted June 26 2015
� 2015 American Association of Oral and Maxillofacial Surgeons
0278-2391/15/00907-6
http://dx.doi.org/10.1016/j.joms.2015.06.172
1
FLA 5.2.0 DTD � YJOMS56897_proof � 15 July 2015 � 8:55 pm � CE AH
99
100
101
102
103
104105
106
107
108
109
110
111
112

Q11
12
Table 1. POINTS AND LANDMARKS
Point Definition
A Deepest (most posterior) midline point on the curvature between the ANS and the prosthion
ANS Tip of the bony anterior nasal spine at the inferior margin of the piriform aperture in the midsagittal plane
(often used to define the anterior end of the palatal plane)
Ba Basion; most anterior inferior point on the margin of the foramen magnum in the midsagittal plane
C2 Second cervical vertebra
C2sp (or C2od) Superoposterior extremity of the odontoid process of the C2
C3ai Most anteroinferior point of the body of the third cervical vertebra
Cg Most superior point of the crista galli
Cv2ig Tangent point at the superoposterior extremity of the odontoid process of the C2
Cv2ip Most inferoposterior point on the body of the C2
Cv4ip Most inferoposterior point on the body of the fourth cervical vertebra
Cvod Most superior point of the odontoid process of C2
LOr Lowest point on the left inferior orbital margin
Lpo Most superior point of the outline of the left external auditory meatus (anatomic porion)
LtLtPtg Most posterior point of the left lateral pterygoid plate as viewed on the coronal section
Lzyg Most lateral point in the left frontozygomatic suture
N Nasion; junction of the nasal and frontal bones at the most posterior point on the curvature of the bridge
of the nose
PNS Most posterior point on the bony hard palate in the midsagittal plane
Pr Prosthion; most anterior inferior point of the alveolar bone crest of the maxillary incisors
ROr Lowest point on right inferior orbital margin
RtLtPtg Most posterior point of right lateral pterygoid plate as viewed in the coronal section
Rzyg Most lateral point in the right frontozygomatic suture
S Sella; center of the hypophyseal fossa (sella turcica)
So Midpoint of line between the sella and basion
Spip Most posterior point of the middle of the soft palate
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
2 LE FORT I OSTEOTOMYAND NASOPHARYNGEAL AIRWAY Q25
113
114
115
116
117
118
119
120121
122
123
124
125
126
127
128129
130
131
132
133
134
135
136137
138
139
140
141
142
143
144145
146
147
148
149
150
151
152153
154
155
156
157
158
159
160161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176177
178
179
180
181
182
183
184185
186
187
188
189
190
191
192193
194
195
196
197
198
199
200201
202
203
204
205
206
207
208209
210
211
212
213
214
215
216217
218
219
220
221
222
223
224
The impact of corrective jaw surgery on the upper
airway spaces depends on the type of operation, the
amount and direction of the skeletal movements, anda patient’s age, gender, and variations. Mandibular
setback surgery results in a decrease in airway patency;
therefore, bimaxillary osteotomy is indicated for the
correction of large anteroposterior discrepancies.1-5
Rhinomanometric techniques to measure nasal airway
resistance have shown that maxillary impaction
increases alar width, with a subsequent decrease in
nasal airway resistance.6,7 Another study based on2-dimensional cephalometric analysis has proved that
maxillary advancement meaningfully increases dimen-
sions of the airway.8
The lack of information on the impact of a Le Fort I
osteotomy on 3-dimensional measurements of the
nasopharyngeal airway inspired this study.
The study assessed assess volumetric changes in the
nasal cavity, maxillary sinus, and oropharyngeal airwayafter a Le Fort I osteotomy and investigated the corre-
lation between these changes and surgical maxil-
lary movements.
Materials and Methods
The sample size for this study was calculated using
the Researcher’s Tool Kit Calculator, which indicated
FLA 5.2.0 DTD � YJOMS56897_proof �
that a cohort of 32 patients would produce a confi-
dence level of 95% and a statistical power of 50%.
Therefore, it was decided to recruit 40 patients toovercome the potential exclusion of some cases. The
study was approved by the West of Scotland Qresearch
ethics service (reference, 12/WS/0133). The inclusion
criteria were as follows:
1. Caucasianmale and female patients 16 to 45 years
old who had a Le Fort I osteotomy (maxillary
advancement with or without impaction) to cor-
rect the underlying Class III malocclusion.
2. No previous tonsillar, nasal, adenoid, head or
neck surgery.
3. Nomajor variation in the head and craniocervical
orientation between the preoperative (T1) and
postoperative (T2) cone-beam computed tomo-
graphic (CBCT) scans.
4. No previous orthodontic expansion or mandib-
ular orthognathic surgical procedure.
Surgerywas carried out by the same surgeon and the
orthodontic treatment was carried out by various clini-
cians, ranging from consultants to specialist trainees,
in the Glasgow Dental Hospital and School (GDHS;Glasgow, UK). All patients underwent presurgical
15 July 2015 � 8:55 pm � CE AH

Table 3. CEPHALOMETRIC ANGLES
Angle Definition
Lordosis Measured by the mean of the SN-PAL and CVT-NS angles (Fig 1A)
Pitch angle (P angle) Inner angle of the intersection of the SN and TH planes; represents the change in head
orientation in the sagittal plane (cranial base inclination angle; Fig 1A)
Roll angle (R angle) Inner angle of the intersection of the Z and TH planes; represents change in head orientation in
the frontal plane (Fig 1B)
Yaw angle (Y angle) Represents change in head orientation in the mediolateral plane, measured by right (Cg-Cvod-
RtLtPtg)and left (Cg-Cvod-LtPtg) angles (Fig 1C)
Abbreviations: Cg-Cvod-LtLtPtg, angle formed by the most superior point of the crista galli, the most superior point of the odon-toid process of the second cervical vertebra, and the most posterior point of the left lateral pterygoid plate as viewed in the cor-onal section; Cg-Cvod-RtLtPtg, angle formed by the most superior point of the crista galli, the most superior point of the odontoidprocess of the second cervical vertebra, and the most posterior point of the right lateral pterygoid plate as viewed in the coronalsection; CVT-NS angle, angle formed by the line through and tangent to the superoposterior extremity of the odontoid process ofthe second cervical vertebra and the line connecting the nasion to the sella; SN-PAL angle, angle formed by the line connecting thesella and nasion and the line through the tangent point at the superoposterior extremity of the odontoid process of and the mostinferoposterior point on the body of the second cervical vertebra; TH plane, true horizontal plane; Z plane, zygomatic plane. Q3
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
Table 2. LINES AND PLANES
Line and Plane Definition
ANSV plane Perpendicular plane to true horizontal plane passing through the nasion in the lateral view; if the
midpalatine split extends to involve the anterior nasal spine, then the most posterior anterior nasal
spine is considered
C2sp/V plane Defined by the frontal plane perpendicular to the Frankfort horizontal plane passing through the
superoposterior extremity of the odontoid process of the second cervical vertebra
C3ai/H plane Plane parallel to the Frankfort horizontal plane passing through the most anteroinferior point of the body
of the third cervical vertebra
Cg-Cvod plane Line connecting the crista galli and the superoposterior extremity of the odontoid process of the second
cervical vertebra
CVT plane Line passing through the tangent point at the superoposterior extremity of the odontoid process of the
second cervical vertebra and tangent to the superoposterior extremity of the odontoid process of the
second cervical vertebra
Epi/FH plane Plane parallel to the Frankfort horizontal plane connecting the base of the epiglottis to the entrance of the
esophagus; technically by the plane parallel to the Frankfort horizontal plane connecting the base of the
epiglottis to the most anteroinferior point of the body of the fourth cervical vertebra (C4ai/H plane)
LF plane Left Frankfort; line connecting left orbit and left porionQ2 points
LOrH plane True horizontal plane tangent to the lowest point on the left inferior orbital margin
Orbital plane Line connecting right orbit and left orbit
PAL Line through the tangent point at the superoposterior extremity of the odontoid process of the second
cervical vertebra and the most inferoposterior point on the body of the second cervical vertebra
PNSH plane Plane parallel to the Frankfort horizontal plane passing through the posterior nasal spine and extending to
the posterior wall of the pharynx
PNSV plane Perpendicular to true horizontal plane passing through the posterior nasal spine; if the midpalatine split
extends to involve the posterior nasal spine, then the most posterior end of the palate is considered
PNSV plane True vertical plane passing through the posterior nasal spine
Ptg plane Line connecting the most posterior points of the left and right lateral pterygoid plate as viewed in the
coronal section
SN plane Plane representing a line connecting the sella to the nasion
Spip/FH plane Plane parallel to the Frankfort horizontal plane passing through the most posterior point of the middle of
the soft palate
SPPFH plane Sagittal plane perpendicular to the Frankfort horizontal plane passing through the lateral walls of the
maxillary sinus
TH plane True horizontal; a reference line constructed by drawing a line perpendicular to the true vertical line
TV plane True vertical; a reference line constructed perpendicular to the floor
Z plane Zygomatic; line connecting the most lateral points on the right and left frontozygomatic suture
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
FLA 5.2.0 DTD � YJOMS56897_proof � 15 July 2015 � 8:55 pm � CE AH
ALMUZIAN ET AL 3
225
226
227
228
229
230
231
232233
234
235
236
237
238
239
240241
242
243
244
245
246
247
248249
250
251
252
253
254
255
256257
258
259
260
261
262
263
264265
266
267
268
269
270
271
272273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288289
290
291
292
293
294
295
296297
298
299
300
301
302
303
304305
306
307
308
309
310
311
312313
314
315
316
317
318
319
320321
322
323
324
325
326
327
328329
330
331
332
333
334
335
336

print&
web4C=FPO
FIGURE1. Head and craniocervical orientation angles.A, Pitch and lordosis angle. B, Roll angle.C, Yaw angle. CVT-NS angle, angle formedby the line through and tangent to the superoposterior extremity of the odontoid process of the second cervical vertebra and the line connectingthe nasion to the sella; P angle, pitch angle; R angle, roll angle; SN-PAL angle, angle formed by the line connecting the sella and nasion and theline through the tangent point at the superoposterior extremity of the odontoid process of and the most inferoposterior point on the body of thesecond cervical vertebra; Y angle, yaw angle. Q1
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
FLA 5.2.0 DTD � YJOMS56897_proof � 15 July 2015 � 8:55 pm � CE AH
4 LE FORT I OSTEOTOMYAND NASOPHARYNGEAL AIRWAY
337
338
339
340
341
342
343
344345
346
347
348
349
350
351
352353
354
355
356
357
358
359
360361
362
363
364
365
366
367
368369
370
371
372
373
374
375
376377
378
379
380
381
382
383
384385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400401
402
403
404
405
406
407
408409
410
411
412
413
414
415
416417
418
419
420
421
422
423
424425
426
427
428
429
430
431
432433
434
435
436
437
438
439
440441
442
443
444
445
446
447
448

print&
web4C=FPO
FIGURE 2. Standardized orientation technique.
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
print&web4C=FPO
ALMUZIAN ET AL 5
449
450
451
452
453
454
455
456457
458
459
460
461
462
463
464465
466
467
468
469
470
471
472473
474
475
476
477
478
479
480481
482
483
484
485
486
487
488489
490
491
492
493
494
495
496497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512513
514
515
516
517
518
519
520521
522
523
524
525
526
527
528529
530
531
orthodontic treatment using upper and lower fixed
appliances, with or without dental extractions.
Two CBCT scans were acquired for each patient:
immediately before the Le Fort I osteotomy (T1) and6 months after surgery (during or after orthodontic
FIGURE 3. Superimposition o
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Ora
FLA 5.2.0 DTD � YJOMS56897_proof �
treatment; T2). All CBCT scans were taken at the
GDHS using an iCAT scanner (Imaging Sciences Inter-
national, Hatfield, PA) by a trained radiographer.
Patients were required to take off any spectacles orjewelry, keep their eyes gently closed, and keep their
n cranial-base technique.
l Maxillofac Surg 2015.
15 July 2015 � 8:55 pm � CE AH
532
533
534
535
536537
538
539
540
541
542
543
544545
546
547
548
549
550
551
552553
554
555
556
557
558
559
560
Q13
Q14
Q1516
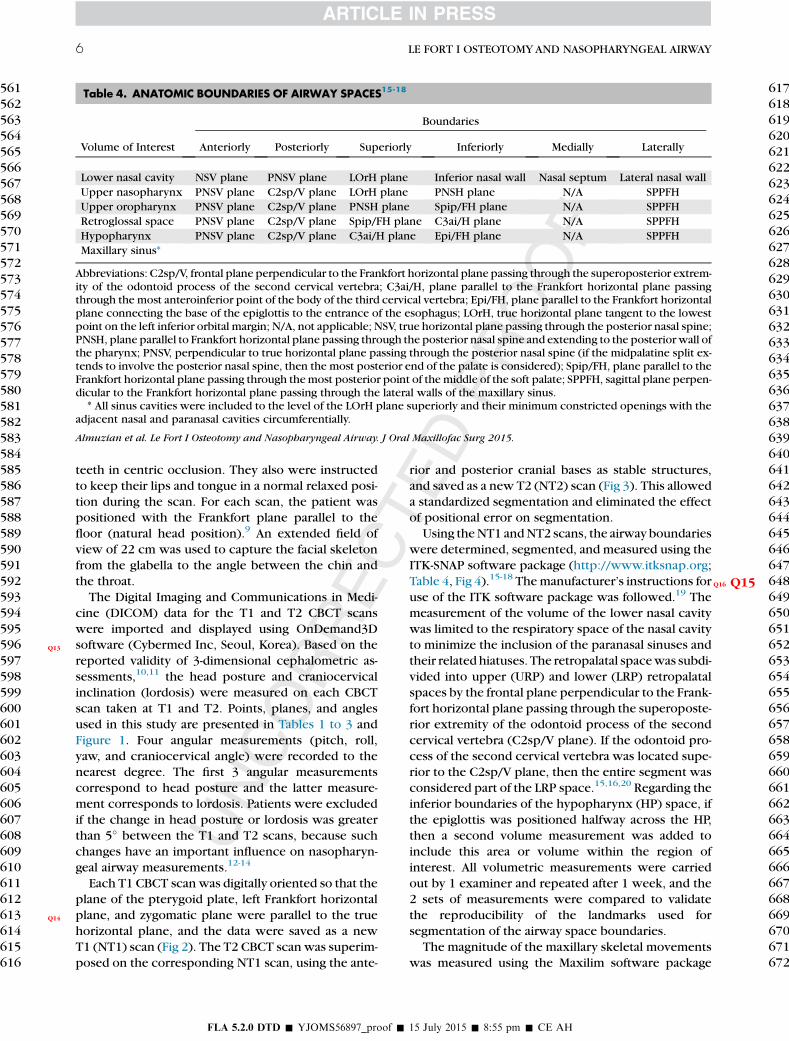
Table 4. ANATOMIC BOUNDARIES OF AIRWAY SPACES15-18
Volume of Interest
Boundaries
Anteriorly Posteriorly Superiorly Inferiorly Medially Laterally
Lower nasal cavity NSV plane PNSV plane LOrH plane Inferior nasal wall Nasal septum Lateral nasal wall
Upper nasopharynx PNSV plane C2sp/V plane LOrH plane PNSH plane N/A SPPFH
Upper oropharynx PNSV plane C2sp/V plane PNSH plane Spip/FH plane N/A SPPFH
Retroglossal space PNSV plane C2sp/V plane Spip/FH plane C3ai/H plane N/A SPPFH
Hypopharynx PNSV plane C2sp/V plane C3ai/H plane Epi/FH plane N/A SPPFH
Maxillary sinus*
Abbreviations: C2sp/V, frontal plane perpendicular to the Frankfort horizontal plane passing through the superoposterior extrem-ity of the odontoid process of the second cervical vertebra; C3ai/H, plane parallel to the Frankfort horizontal plane passingthrough the most anteroinferior point of the body of the third cervical vertebra; Epi/FH, plane parallel to the Frankfort horizontalplane connecting the base of the epiglottis to the entrance of the esophagus; LOrH, true horizontal plane tangent to the lowestpoint on the left inferior orbital margin; N/A, not applicable; NSV, true horizontal plane passing through the posterior nasal spine;PNSH, plane parallel to Frankfort horizontal plane passing through the posterior nasal spine and extending to the posteriorwall ofthe pharynx; PNSV, perpendicular to true horizontal plane passing through the posterior nasal spine (if the midpalatine split ex-tends to involve the posterior nasal spine, then the most posterior end of the palate is considered); Spip/FH, plane parallel to theFrankfort horizontal plane passing through themost posterior point of the middle of the soft palate; SPPFH, sagittal plane perpen-dicular to the Frankfort horizontal plane passing through the lateral walls of the maxillary sinus.* All sinus cavities were included to the level of the LOrH plane superiorly and their minimum constricted openings with the
adjacent nasal and paranasal cavities circumferentially.
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
6 LE FORT I OSTEOTOMYAND NASOPHARYNGEAL AIRWAY
561
562
563
564
565
566
567
568569
570
571
572
573
574
575
576577
578
579
580
581
582
583
584585
586
587
588
589
590
591
592593
594
595
596
597
598
599
600601
602
603
604
605
606
607
608609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624625
626
627
628
629
630
631
632633
634
635
636
637
638
639
640641
642
643
644
645
646
647
648649
650
651
652
653
654
655
656657
658
659
660
661
662
663
664665
666
667
668
669
670
671
672
teeth in centric occlusion. They also were instructed
to keep their lips and tongue in a normal relaxed posi-
tion during the scan. For each scan, the patient waspositioned with the Frankfort plane parallel to the
floor (natural head position).9 An extended field of
view of 22 cm was used to capture the facial skeleton
from the glabella to the angle between the chin and
the throat.
The Digital Imaging and Communications in Medi-
cine (DICOM) data for the T1 and T2 CBCT scans
were imported and displayed using OnDemand3Dsoftware (Cybermed Inc, Seoul, Korea). Based on the
reported validity of 3-dimensional cephalometric as-
sessments,10,11 the head posture and craniocervical
inclination (lordosis) were measured on each CBCT
scan taken at T1 and T2. Points, planes, and angles
used in this study are presented in Tables 1 to 3 and
Figure 1. Four angular measurements (pitch, roll,
yaw, and craniocervical angle) were recorded to thenearest degree. The first 3 angular measurements
correspond to head posture and the latter measure-
ment corresponds to lordosis. Patients were excluded
if the change in head posture or lordosis was greater
than 5� between the T1 and T2 scans, because such
changes have an important influence on nasopharyn-
geal airway measurements.12-14
Each T1 CBCT scan was digitally oriented so that theplane of the pterygoid plate, left Frankfort horizontal
plane, and zygomatic plane were parallel to the true
horizontal plane, and the data were saved as a new
T1 (NT1) scan (Fig 2). The T2 CBCT scan was superim-
posed on the corresponding NT1 scan, using the ante-
FLA 5.2.0 DTD � YJOMS56897_proof �
rior and posterior cranial bases as stable structures,
and saved as a new T2 (NT2) scan (Fig 3). This allowed
a standardized segmentation and eliminated the effectof positional error on segmentation.
Using theNT1 andNT2 scans, the airway boundaries
were determined, segmented, and measured using the
ITK-SNAP software package (http://www.itksnap.org;
Table 4, Fig 4).15-18 QThemanufacturer’s instructions for
use of the ITK software package was followed.19 The
measurement of the volume of the lower nasal cavity
was limited to the respiratory space of the nasal cavityto minimize the inclusion of the paranasal sinuses and
their related hiatuses. The retropalatal spacewas subdi-
vided into upper (URP) and lower (LRP) retropalatal
spaces by the frontal plane perpendicular to the Frank-
fort horizontal plane passing through the superoposte-
rior extremity of the odontoid process of the second
cervical vertebra (C2sp/V plane). If the odontoid pro-
cess of the second cervical vertebra was located supe-rior to the C2sp/V plane, then the entire segment was
considered part of the LRP space.15,16,20 Regarding the
inferior boundaries of the hypopharynx (HP) space, if
the epiglottis was positioned halfway across the HP,
then a second volume measurement was added to
include this area or volume within the region of
interest. All volumetric measurements were carried
out by 1 examiner and repeated after 1 week, and the2 sets of measurements were compared to validate
the reproducibility of the landmarks used for
segmentation of the airway space boundaries.
The magnitude of the maxillary skeletal movements
was measured using the Maxilim software package
15 July 2015 � 8:55 pm � CE AH

Q17
print&web4C=FPO
FIGURE 4. Airway space volumetric measurement and segmentation using ITK-SNAP. A, Saggital view. B, Coronal view. (Fig 4 continuedon next page.)
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
ALMUZIAN ET AL 7
673
674
675
676
677
678
679
680681
682
683
684
685
686
687
688689
690
691
692
693
694
695
696697
698
699
700
701
702
703
704705
706
707
708
709
710
711
712713
714
715
716
717
718
719
720721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736737
738
739
740
741
742
743
744745
746
747
748
749
750
751
752753
754
755
756
757
758
759
760761
762
763
764
765
766
767
768769
770
771
772
773
774
775
776777
778
779
780
781
782
783
784
(Medicim NV, Mechelen, Belgium). Several markers
were identified and digitized directly on the DICOM
slices of the NT1 and NT2 scans. For maxillary surgical
movements, orthogonal distances were recorded to
the 3 common reference planes. The net movements
were calculated as the differences between the NT1
and NT2 landmark positions in the X, Y, and Z planes
(Fig 5).
STATISTICAL ANALYSIS
The distribution of the sample data was assessed
using the Kolmogorov-Smirnov test, which showed
non-Gaussian distribution for most parameters. The
Friedman test and Wilcoxon rank sum test (P < .05)were applied to determine a statistical difference
owing to age or gender and to evaluate the importance
of volumetric changes in the nasopharyngeal spaces
secondary to a Le Fort I osteotomy.
FLA 5.2.0 DTD � YJOMS56897_proof �
The Pearson correlation coefficient was applied to
assess the correlation between volumetric changes
and the magnitude of surgical maxillary movement
in 3 planes of space as a result of a Le Fort I osteotomy.
Results
Six patients were excluded from the study because
of a major difference ($5�) in head and neck posture
between the T1 and T2 CBCT scans. There was no sta-
tistically significant difference between the repeated
volumetric measurements (P > .05), with a high level
of agreement (r = 0.99; P < .05; Table 5).
The main surgical movement of the maxilla was ananterior shift of 6.42 � 1.51 mm (range, 3.43 to
8.5 mm). This also was associated with a mild vertical
impaction of 0.65� 0.28 mm (range, 0.07 to 2.27 mm)
more on the right side (mean, 0.82 � 0.32 mm; range,
15 July 2015 � 8:55 pm � CE AH

18
print&
web4C=FPO
FIGURE 4 (cont’d). C, Axial view. D, Virtual model representation of nasopharyngeal airway spaces.
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
8 LE FORT I OSTEOTOMYAND NASOPHARYNGEAL AIRWAY
785
786
787
788
789
790
791
792793
794
795
796
797
798
799
800801
802
803
804
805
806
807
808809
810
811
812
813
814
815
816817
818
819
820
821
822
823
824825
826
827
828
829
830
831
832833
834
835
836
837
838
839
840
841
842
843
844
845
846
847
848849
850
851
852
853
854
855
856857
858
859
860
861
862
863
864865
866
867
868
869
870
871
872873
874
875
876
877
878
879
880881
882
883
884
885
886
887
888889
890
891
892
893
894
895
896
0.1 to 2.9 mm) than on the left side (mean, 0.47 �0.24 mm; range, 0.03 to 1.63 mm), with a mild medio-
lateral rotation of 0.86 � 0.44 mm (range, 0.2 to1.73 mm; Table 6).
Table 7 presents the volumetric changes of the naso-
pharyngeal airway spaces secondary to a Le Fort I
Osteotomy. The right maxillary sinus (RMS) was signif-
icantly decreased by 17.8%, whereas the LRP was
significantly expanded by 17.3% (P < .05). Gender-
related changes were not detected in this study (Fried-
man test, P = .4452).The correlation between the change in the volume
of airway space and the magnitude of surgical maxil-
lary movements was mild (r = 0.4; Table 8). Similarly,
there was a weak correlation between the volumetric
changes at different levels of the nasopharyngeal
FLA 5.2.0 DTD � YJOMS56897_proof �
airway space, except between the upper nasopharynx
(UNP) and the URP (correlation coefficient,
Q0.53; Table 9).
Discussion
This study relied on an internal reference structure
during segmentation that would not be affected by
occlusal settling or orthodontic movement between
the T1 and T2 CBCT scans. This is one of the explana-
tions for the differences between the results of this
study and other published data that have relied ondental reference points.17 Park et al17 used cervical
vertebral levels to subdivide the airway space, but
this was prone to errors because it relied on the pa-
tient’s head and neck posture during CBCT scanning.
15 July 2015 � 8:55 pm � CE AH

19
20
print&web4C=FPO
FIGURE 5. Skeletal movement measurement using Maxilim software.
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
ALMUZIAN ET AL 9
897
898
899
900
901
902
903
904905
906
907
908
909
910
911
912913
914
915
916
917
918
919
920921
922
923
924
925
926
927
928929
930
931
932
933
934
935
936937
938
939
940
941
942
943
944945
946
947
948
949
950
951
952
953
954
955
956
957
958
959
960961
962
963
964
965
966
967
968969
970
971
972
973
974
975
976977
978
979
980
981
982
983
984985
986
987
988
989
990
991
992993
994
995
996
Changes in the head and neck posture owing to the ef-fect of surgery or projectional scanning errors would
affect the pharyngeal airway volume and cross-
sectional measurements.12,21-23 This source of error
was detected in this study by measuring the angles
of head orientation and neck lordosis at T1 and T2;
approximately 10% of patients showed major
changes in head and neck posture and were excluded.
This study used 2 distinguishing methodologies.First, it assessed the effects of a single Le Fort I osteot-
omy on the nasopharyngeal airway space. Second, seg-
mentation of the nasopharyngeal space allowed
Table 5. REPRODUCIBILITY OF VOLUMETRIC MEASUREMENTS
LMS RMS LNC
Wilcoxon signed rank test,
P < .05
0.742 0.945 0.43
ICC 0.999 1.000 0.99
Abbreviations: HP, hypopharynx; ICC, intraclass correlation coefretropalatal space; RG, ---; RMS, right maxillary sinus; UNP, u
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Ora
FLA 5.2.0 DTD � YJOMS56897_proof �
changes at different levels to be quantified becauseeach anatomic segment is related to a specific prob-
lem. Hern�andez-Alfaro et al16 Qfound a statistical expan-
sion in total pharyngeal airway space (37.7%). This is
dissimilar from the findings of the present study,
which could be due to the fact that the entire airway
space was considered and measured as a single unit,
rather than in segments. With regard to volumetric
changes in levels of the nasal cavity, the LNC Qwasdecreased by one tenth of its preoperative volume.
This could be due to the combined maxillary vertical
impaction, which decreases the effective volume of
UNP URP LRP RG HP
8 0.156 0.375 0.250 0.383 0.844
9 1.000 1.000 1.000 1.000 1.000
ficient; LMS, left maxillary sinus; LNC, ---; LRP, lowerpper nasopharynx; URP, upper retropalatal space. Q4
l Maxillofac Surg 2015.
15 July 2015 � 8:55 pm � CE AH
997
998
999
10001001
1002
1003
1004
1005
1006
1007
1008

Q21
Table 6. DEGREE OF MAXILLARY SURGICALMOVEMENTS
Mean SD Minimum Maximum
Net anteroposterior
movement
6.42 1.51 3.43 8.5
Net vertical movement 0.65 0.28 0.07 2.27
Right-side vertical
movement
0.82 0.32 0.1 2.9
Left-side vertical
movement
0.47 0.24 0.03 1.63
Net mediolateral
movement
0.86 0.44 0.2 1.73
Abbreviation: SD, standard deviation.
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway.J Oral Maxillofac Surg 2015.
Table 8. CORRELATION BETWEEN CHANGE INVOLUME OF AIRWAY SPACE AND MAGNITUDE OFSURGICAL SKELETAL MOVEMENT
Anteroposterior
Movement
Vertical
Movement
Mediolateral
Movement
LMS 0.020 0.014 0.040
RMS 0.039 0.030 0.030
LNC �0.128 �0.100 �0.041
UNP 0.018 �0.082 �0.069
URP 0.053 0.047 0.022
LRP �0.044 �0.104 �0.088
RG �0.12 �0.184 �0.226
HP 0.032 0.007 0.025
Abbreviations: HP, hypopharynx; LMS, left maxillary sinus;LNC, ---; LRP, lower retropalatal space; RG, ---;RMS, right maxillary sinus; UNP, upper nasopharynx; URP,upper retropalatal space. Q6
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway.J Oral Maxillofac Surg 2015.
10 LE FORT I OSTEOTOMYAND NASOPHARYNGEAL AIRWAY
1009
1010
1011
1012
1013
1014
1015
10161017
1018
1019
1020
1021
1022
1023
10241025
1026
1027
1028
1029
1030
1031
10321033
1034
1035
1036
1037
1038
1039
10401041
1042
1043
1044
1045
1046
1047
10481049
1050
1051
1052
1053
1054
1055
10561057
1058
1059
1060
1061
1062
1063
1064
1065
1066
1067
1068
1069
1070
1071
10721073
1074
1075
1076
1077
1078
1079
10801081
1082
1083
1084
1085
1086
1087
10881089
1090
1091
1092
1093
1094
1095
10961097
1098
1099
1100
1101
1102
the LNC and disguises the effect of maxillary advance-
ment. Although the changes were not statistically
meaningful, they were similar to the findings of Pour-
danesh et al.23
The ratio of the RG space at T1 to T2 was approxi-
mately 4:6, with approximately 15% of volumetric
expansion after the Le Fort I osteotomy. An anatomi-
cally based explanation is that the superior attach-ments of the palatoglossus muscle were displaced
anteriorly secondary to maxillary advancement with
subsequent anterior displacement of the tongue and
expansion of the RG airway volume.24 Because the
main pathophysiology of obstructive sleep apnea and
hypopnea (OSAH) is that the tongue falls backward
and blocks the RG airway space during sleep, the Le
Fort I osteotomy might be an alternative option fortreatment of OSAH in patients with maxillary
hypoplasia.
Moreover, there was a decrease in the volume of the
2 maxillary sinuses, specifically the volume of the
Table 7. VOLUMETRIC CHANGES IN NASOPHARYNGEAL AIR
Airway Space
T1 T2
Mean SD Mean SD
LMS 9,705.6 2,482.1 9,511.7 2,468.2
RMS 10,471.6 3,488.6 8,606.2 3,427.4
LNC 7,917.2 1,452.5 7,189.2 2,306.7
UNC 6,640.2 2,661.6 7,311.7 2,434.1
RG 2,000.7 3,227.0 1,704.6 2,091.0
URP 8,534.1 7,738.0 9,053.8 4,039.1
LRP 8,605.2 4,684.9 10,089.6 5,590.3
HP 3,863.6 2,180.9 3,243.5 1,939.1
Abbreviations: HP, hypopharynx; LMS, left maxillary sinus; LNC,-maxillary sinus; SD, standard deviation; T1, preoperative; T2, 6 moURP, upper retropalatal space.
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Ora
FLA 5.2.0 DTD � YJOMS56897_proof �
RMS, which was decreased to one fifth of its preoper-
ative value. This can be explained by the differential
impaction of the right and left sides of the maxilla to
correct occlusal canting as a result of the dominance
of the right facial half.25-28 This assumption requiresa larger sample in which a Le Fort I osteotomy is
performed to correct the underlying asymmetry.
Although the main objective of the study was to
assess the impact of Le Fort I maxillary advancement
on the nasopharyngeal airway, minor simultaneous
surgical movements in the vertical or medial and
vertical directions were unavoidable.
The study showed a weak correlation between thevolumetric changes at different levels of the upper
airway tract and the magnitude of maxillary surgical
movement. However, there was a moderate positive
correlation between changes in the volume of the
WAY SPACES SECONDARY TO LE FORT I OSTEOTOMY
Percentage of Volumetric
Changes, (T2 � T1)/T1 � 100
Wilcoxon Signed Rank
Test, P < .05
�2.0 .408
�17.8 .015
�9.2 .109
10.1 .162
14.8 .5186
6.1 .1627
17.3 .013
�16.1 .501
--; LRP, lower retropalatal space; RG,---; RMS, rightnths postoperative; UNC,---; UNP, upper nasopharynx;
Q5
l Maxillofac Surg 2015.
15 July 2015 � 8:55 pm � CE AH
1103
11041105
1106
1107
1108
1109
1110
1111
11121113
1114
1115
1116
1117
1118
1119
1120

Q22
23
Table 9. CORRELATION BETWEEN VOLUMETRIC CHANGES AT DIFFERENT LEVELS OF THE UPPER AIRWAY TRACT
LMS RMS LNC UNP URP LRP RG HP
LMS 1.000
RMS 0.073 1.000
LNC 0.145 0.040 1.000
UNP 0.084 0.384 0.063 1.000
URP �0.333 0.336 0.218 0.532 1.000
LRP 0.350 0.073 0.009 0.326 �0.114 1.000
RG �0.398 �0.137 �0.036 0.205 0.362 �0.038 1.000
HP 0.013 0.167 0.145 0.419 0.151 0.301 0.008 1.000
Abbreviations: HP, hypopharynx; LMS, left maxillary sinus; LNC,---; LRP, lower retropalatal space; RG,---; RMS, rightmaxillary sinus; UNP, upper nasopharynx; URP, upper retropalatal space. Q7
Almuzian et al. Le Fort I Osteotomy and Nasopharyngeal Airway. J Oral Maxillofac Surg 2015.
ALMUZIAN ET AL 11
1121
1122
1123
1124
1125
1126
1127
11281129
1130
1131
1132
1133
1134
1135
11361137
1138
1139
1140
1141
1142
1143
11441145
1146
1147
1148
1149
1150
1151
11521153
1154
1155
1156
1157
1158
1159
11601161
1162
1163
1164
1165
1166
1167
11681169
1170
1171
1172
1173
1174
1175
1176
1177
1178
1179
1180
1181
1182
1183
11841185
1186
1187
1188
1189
1190
1191
11921193
1194
1195
1196
1197
1198
1199
12001201
1202
1203
1204
1205
1206
1207
12081209
1210
1211
1212
1213
1214
1215
12161217
1218
1219
1220
1221
1222
1223
12241225
1226
1227
1228
1229
1230
1231
1232
UNP and URP spaces, which is due to the close
anatomic relation of these airway spaces. These find-
ings differ from those of Sears et al,18 probably becausethe design of the present study was limited to cases
that had a Le Fort I osteotomy only.
Although the outcomes of this study showed that
the applied technique in quantifying the airway vol-
ume was sensitive and reliable, its specificity in
measuring airway functionality needs to be assessed
clinically. The authors acknowledge that one of the
limitations of this study is the short-term follow-up,which was limited to 6 months after surgery. A future
comparative clinical study with long-term follow-up
would be beneficial to support changes in the naso-
pharyngeal airway spaces after a Le Fort I osteotomy.
Further applications of the ITK-SNAP software pack-
age could be used to gauge the size of the bony cleft
defect and the success of alveolar bone grafting in pa-
tients with cleft lip and roof of the mouth.The Le Fort I osteotomy was found to increase the
retroglossal airway volume and the right maxillary
antrum. This could be important for the treatment of
OSAH in patients with maxillary deficiency. A long-
term follow-up study in a larger samplewith functional
assessment of the airway would be beneficial to
confirm these findings.
References
1. Kawamata A, Fujishita M, Ariji Y, et al: Three-dimensionalcomputed tomographic evaluation of morphologic airwaychanges after mandibular setback osteotomy for prognathism.Oral Surg Oral Med Oral Path Oral Radiol, Endodont 89:278,2000
2. LiukkonenM, V€ah€atalo K, Peltom€aki T, et al: Effect of mandibularsetback surgery on the posterior airway size. Int J Adult Ortho-don Orthognath Surg 17:41, 2001
3. Chen F, Terada K, Hua Y, et al: Effects of bimaxillary surgery andmandibular setback surgery on pharyngeal airway measure-ments in patientswith Class III skeletal deformities. Am J OrthodDentofacial Orthop 131:372, 2007
4. Greco JM, Frohberg U, Van Sickels JE: Long-term airway spacechanges after mandibular setback using bilateral sagittal splitosteotomy. Int J Oral Maxillofac Surg 19:103, 1990
FLA 5.2.0 DTD � YJOMS56897_proof �
5. Muto T, Yamazaki A, Takeda S, et al: Effect of bilateral sagittalsplit ramus osteotomy setback on the soft palate and pharyngealairway space. Int J Oral Maxillofac Surg 37:419, 2008
6. GuenthnerTA, SatherAH,KernEB:Theeffect of LeFort Imaxillaryimpaction on nasal airway resistance. Am J Orthod 85:308, 1984
7. Turvey TA, Hall DJ, Warren DW: Alterations in nasal airway resis-tance following superior repositioning of the maxilla. Am JOrthod 85:109, 1984
8. Jakobsone G, Stenvik A, Espeland L: The effect of maxillaryadvancement and impaction on the upper airway after bimaxil-lary surgery to correct Class III malocclusion. Am J Orthod Den-tofacial Orthop 139:e369, 2011
9. Solow B, Tallgren A: Natural head position in standing subjects.Acta Odontol 29:591, 1971
10. Gribel BF, Gribel MN, Fraz~ao DC, et al: Accuracy and reliability ofcraniometric measurements on lateral cephalometry and 3Dmeasurements on CBCT scans. Angle Orthod 81:26, 2010
11. de Oliveira AE, Cevidanes LH, Phillips C, et al: Observer reli-ability of three-dimensional cephalometric landmark identifica-tion on cone-beam computerized tomography. Oral Surg OralMed Oral Pathol Oral Radiol Endod 107:256, 2009
12. Shelton RL, Bosma JF: Maintenance of the pharyngeal airway.J Appl Physiol 17:209, 1962
13. Muto T, Takeda S, Kanazawa M, et al: The effect of head postureon the pharyngeal airway space (PAS). Int J Oral Maxillofac Surg31:579, 2002
14. Stepovich ML: A cephalometric positional study of the hyoidbone. Am J Orthod 51:882, 1965
15. Chang Y, Koenig LJ, Pruszynski JE, et al: Dimensional changes ofupper airway after rapid maxillary expansion: A prospectivecone-beam computed tomography study. Am J Orthod Dentofa-cial Orthop 143:462, 2013
16. Hern�andez-Alfaro F, Guijarro-Mart�ınez R, Mareque-Bueno J:Effect of mono- and bimaxillary advancement on pharyngealairway volume: Cone-beam computed tomography evaluation.J Oral Maxillofac Surg 69:e395, 2011
17. Park SB, Kim YI, Son WS, et al: Cone-beam computed tomogra-phy evaluation of short-and long-term airway change and stabil-ity after orthognathic surgery in patients with Class III skeletaldeformities: Bimaxillary surgery and mandibular setback sur-gery. Int J Oral Maxillofac Surg 41:87, 2012
18. Sears CR, Miller AJ, Chang MK, et al: Comparison of pharyngealairway changes on plain radiography and cone-beam computedtomography after orthognathic surgery. J Oral Maxillofac Surg69:e385, 2011
19. Ibanez L, SchroederW, Ng L, et al: The ITK Software Guide; 2003 Q
20. Lenza MG, Lenza MD, Dalstra M, et al: An analysis of differentapproaches to the assessment of upper airway morphology:A CBCT study. Orthod Craniofac Res 13:96, 2010
21. Huggare J: Natural head position recording on frontal skull radio-graphs. Acta Odontol 47:105, 1989
22. Cevidanes L, Oliveira AE, Motta A, et al: Head orientation inCBCT-generated cephalograms. Angle Orthod 79:971, 2009
15 July 2015 � 8:55 pm � CE AH

24
12 LE FORT I OSTEOTOMYAND NASOPHARYNGEAL AIRWAY
1233
1234
1235
1236
1237
1238
1239
1240
1241
1242
1243
1244
1245
23. Pourdanesh F, Sharifi R, Mohebbi A, et al: Effects of maxillaryadvancement and impaction on nasal airway function. Int JOral Maxillofac Surg 41:1350, 2012
24. Goodday R, Bourque S: Subjective outcomes of maxillomandib-ular advancement surgery for treatment of obstructive sleepapnea syndrome. J Oral Maxillofac Surg 70:417, 2012
25. Bj€ork A, Bj€ork L: Artificial deformation and cranio-facial asymme-try in ancient Peruvians. J Dent Res 43:353, 1964
FLA 5.2.0 DTD � YJOMS56897_proof �
26. Woo T: On the asymmetry of the human skull. Biometrika 324,1931 Q
27. Arvystas MG, Antonellis P, Justin AF: Progressive facial asymme-try as a result of early closure of the left coronal suture. Am JOrthod 87:240, 1985
28. Almuzian M, Adai K: Computerised frontal symmetry analysis ofIraqi adultswith Class I normal occlusion. Al-RafedeenDent J 12:27, 2002
15 July 2015 � 8:55 pm � CE AH
1246