effects of threatening information on interpersonal responses to pain
TRANSCRIPT

European Journal of Pain 13 (2009) 431–438
Contents lists available at ScienceDirect
European Journal of Pain
journal homepage: www.EuropeanJournalPain.com
Effects of threatening information on interpersonal responses to pain
Todd Jackson a,b,*, Xiting Huang a, Hong Chen a, Heath Phillips b
a Key Laboratory of Cognition and Personality, School of Psychology, Southwest University, Chongqing, Chinab Department of Psychology, James Cook University, Townsville, Australia
a r t i c l e i n f o
Article history:Received 2 March 2008Received in revised form 4 May 2008Accepted 21 May 2008Available online 3 July 2008
Keywords:Experimental PainThreatAppraisalCopingInterpersonal
1090-3801/$36.00 � 2008 European Federation of Chdoi:10.1016/j.ejpain.2008.05.012
* Corresponding author. Address: Department of PsycTownsville, Australia. Tel.: +61 7 47814968.
E-mail address: [email protected] (T. Jackso
a b s t r a c t
Emerging evidence indicates that meanings attributed to pain contribute to tolerance and coping amongaffected individuals. However, links between pain appraisals and coping responses have received littleattention within a broader interpersonal context. In this experiment, effects of appraisal on pain toler-ance and coping were examined in adult dyads. Eighty-six acquaintance/friend pairs were randomlyassigned to the role of Participant in a cold pressor test (CPT) or observer–helper who assisted in coping.Before the task, pairs in the threat condition read about frostbite symptoms and consequences, whilethose in the reassurance condition read about the safety of the task. In a mixed condition, Participantsand Observers read the reassurance and threat passage, respectively. Between-groups analyses revealedthreat group participants had lower pain tolerance and reported less cognitive coping than did partici-pants in other appraisal conditions. Threat group observers reported less attention diversion, copingself-statements and ignoring in helping their partner than did reassured observers. Pain language wasalso most prominent in transactions of threatened dyads. Finally, use of attention diversion by observerscontributed to pain tolerance, independent of participant factors (reported pain, appraisal condition,reported coping) and pain language in conversations during immersions. The study highlights howappraisal contributes not only to pain tolerance and coping in the affected individual but also to care-giv-ing efforts of others in their social environment.� 2008 European Federation of Chapters of the International Association for the Study of Pain. Published
by Elsevier Ltd. All rights reserved.
1. Introduction
The transactional model (e.g., Lazarus and Folkman, 1984; Laz-arus, 1999) posits that evaluations of stressors as potential sourcesof threat, challenge, loss, or harm contribute directly to stress reac-tions and coping responses. This approach has been a catalyst forstudies with clinical pain samples (e.g., Crombez et al., 1999; Joneset al., 2003; Ramı’rez-Maestre et al., 2008; Truchon et al., 2008;Unruh et al., 1999). For example, challenge appraisals have beenlinked recently to active coping in chronic pain patients; in con-trast, harm, loss, or threat appraisals correspond to passive coping,pain, and impairment (Ramı’rez-Maestre et al., 2008).
Related experimental studies have examined the causal impactof manipulating appraisals of noxious stimuli. Jackson et al.(2005a) found healthy adults exposed to frostbite information be-fore undertaking a cold pressor test (CPT) had reduced pain toler-ance, reported less cognitive coping (i.e., diverting attention,coping self-statements, reinterpretation, ignoring) and catastro-phized more than did reassured participants given safety informa-tion about the CPT or controls given no orienting information. Van
apters of the International Associa
hology, James Cook University,
n).
Damme et al. (2008) used a frostbite passage and false blood pres-sure feedback to increase threat appraisals in healthy respondentsabout to engage in a CPT. Compared to controls, threatened partic-ipants showed marginally reduced pain tolerance and increasedcatastrophic thinking. More notably, the threat manipulation im-paired the capacity to distract, as evidenced by increased interfer-ence with performance on a simultaneously presented diversiontask.
Turk and Kerns (1985) extended the transactional approach tofamilies coping with medical conditions including pain, noting thataffected individuals and family members actively pursue and as-sess information about pain and evaluate their own and others’capacities to cope with its’ challenges. Such appraisals result incoping choices and re-appraisals to evaluate the adequacy of cop-ing responses. Despite reliable evidence that peers and family havea profound impact on adaptation to pain (Kerns and Otis, 2003;Leonard et al., 2006; Roy, 2001), experimental studies on the trans-actional approach have focused exclusively on individuals. Exten-sions that consider people in pain and others in their immediatesocial environment can elucidate interpersonal influences on pain.
In this research, effects of appraisal on pain tolerance and cop-ing were examined in healthy acquaintance/friend dyads servingas participant or observer–helper during a CPT. Following frompast research with individuals, we hypothesized that dyads
tion for the Study of Pain. Published by Elsevier Ltd. All rights reserved.

432 T. Jackson et al. / European Journal of Pain 13 (2009) 431–438
comprised of participants and observers exposed to threateninginformation (pain as nociception signal) before the task wouldshow reduced pain tolerance, endorse lower levels of cognitivecoping, and report more catastrophizing than dyads presentedwith reassuring information (pain independent of tissue damage)or ‘‘mixed” dyads wherein participants and observer–helpers weregiven reassuring and threatening information, respectively. Threa-tened dyads were also expected to use more pain-focused languageduring immersion than dyads in the other conditions. In contrast,differences in tolerance, coping, and language were not expectedbetween reassurance and mixed appraisal conditions or betweenmen and women in participant and observer roles. Finally, we ex-plored whether observers’ encouragement of specific coping strat-egies contributed to participant pain tolerance, independent ofparticipant appraisal condition and coping responses.
2. Method
2.1. Participants
The final sample was comprised of 86 dyads comprised of pairsof research volunteers who were at least acquainted with one an-other (e.g., classmates, friends, relationship partners). In total, 56same sex and 30 mixed-sex dyads engaged in this study. Data fromtwo other dyads were eliminated because one member had takenpart in a previous cold pressor experiment.
The sample included pain-free adults (62 men, 110 women) be-tween 18 and 44 years of age (M = 21.72, SD = 5.29). Respondentswere predominantly Caucasian (94.8%), and current undergraduatestudents (90.1%) or high school graduates (8.1%). A majority weresingle (83.70%), married (8.7%), or cohabiting (5.8%) and 12.8% re-ported having a family member with pain lasting at least 3 months.Exclusion criteria included presence of a pain condition, circulatorydisorder, diabetes, hypertension, Raynaud’s disease, a heart condi-tion, previous cold injury, problems with blood clotting, a skin con-dition, or use of medications for these conditions.
2.2. Measures
2.2.1. DemographicsSex, age, ethnicity, education, marital status, and presence of a
family member with ongoing pain were queried. Participants werealso asked to indicate how long they had known their partner andeach member of the dyad was how well they knew their partner ona six-point scale between ‘‘Very Little” and ‘‘Very Well”.
2.2.2. Coping strategies questionnaire (CSQ; adapted from Rosenstieland Keefe, 1983)
After the CPT, each Participant completed a modified CSQ thatincluded five Ignoring Pain items (e.g., ‘‘During the cold pressortest, I ignored the pain”), seven Reinterpreting Pain items(‘‘. . .imagined the pain was outside my body”), six Diverting Atten-tion items (e.g., ‘‘. . .tried to think of something pleasant”), five Cop-ing Self Statements items (e.g., ‘‘. . .told myself to be brave andcarry on”), and four Catastrophizing items (e.g., ‘‘. . .thought thepain was awful and overwhelming”). Items were rated on a 6-pointLikert scale between 1 (Never Did That) and 6 (Very Often Did That).Participants were asked the degree to which they used each strat-egy to cope with cold pressor pain. Alphas for CSQ subscales ran-ged between a = .73 for Ignoring and a = .84 for Catastrophizingamong participants.
Because the pain literature does not yet include a measure ofothers’ efforts to assist a person in pain with coping, CSQ itemsreflecting cognitive strategies were reformulated to permit Observ-ers to rate the extent to which they encouraged their partner to use
each strategy in coping during the immersion. Specifically, Observ-ers rated the extent to which they encouraged Ignoring (e.g., ‘‘Duringthe cold pressor test, I encouraged my partner to ignore the pain”,‘‘. . .encouraged him/her to go on as if nothing was happening”),Reinterpretation (‘‘. . .encouraged my partner to feel distant fromthe pain, as if it was in someone else’s body”, ‘‘. . .tried to help mypartner think of it as a dull warm feeling rather than pain”), DivertingAttention (e.g., ‘‘. . .encouraged him/her to talk about pleasant expe-riences from the past”, ‘‘. . .encouraged him/her to count numbers orrun a song through his/her mind”), Coping Statements items (e.g.,‘‘. . .told my partner to be brave and carry on”, ‘‘. . .encouraged him/her to see it as a challenge and not bother her/him”).
For Catastrophizing, it made little sense that Observers wouldhelp by encouraging partners to think of the pain as terrible, over-whelming and so forth. Instead, ratings of Catastrophizing itemswere reformulated to tap Observer concerns about participant cat-astrophic reactions (e.g., ‘‘During the cold pressor test, I was con-cerned that the pain was awful and overwhelming”, ‘‘. . .wasconcerned s/he couldn’t stand the pain anymore”). Alphas on themodified Observer CSQ were satisfactory, ranging from a = .74 forCatastrophizing to a = .85 for Coping Statements.
2.2.3. Empathy Quotient (Lawerence et al., 2004)The 28-item EQ was included to assess group differences in ob-
server empathy and control for these if necessary, given evidencethat empathy contributes to others’ reactions and responses to an-other in pain (Goubert et al., 2005). Items reflecting cognitiveempathy, emotional empathy, and social skills were rated on a 5-point scale of agreement. Total scores were calculated from sum-ming responses to all items. Lawerence et al. reported the EQhad satisfactory reliability and validity. In this study, ObserverEQ had an alpha of a = .76.
2.2.4. Self-Efficacy Scale (SES; Jackson et al., 2002)A 4-item SES examined efficacy in coping with the CPT. The
items assessed perceived confidence in coping, certainty in tolerat-ing the task, and control of performing well during the CPT on a 5-point scale between not at all and very much. The alpha coefficientfor this scale was a = .73.
2.2.5. Pain tolerance and reported painPain tolerance was operationalized as total time (to the nearest
100th of a second) a participant’s hand remained immersed in theice water. A rating of reported pain was solicited from each partic-ipant immediately after the task using a 10 point scale between 0(No pain at all) and 10 (Severe pain).
2.3. Apparatus
An insulated ice chest measuring 290 � 512 � 200 mm andfilled with 30 l of water was cooled via heat exchange using PeltierEffect Pumps that removed heat from the apparatus with coolantpumped to a remote cooling station. An aerator was inserted to al-low continuous water circulation. Water temperature was main-tained at 2� Centigrade. The apparatus was fitted with a metalbar having several perforations which participants gripped to re-duce hand movements during immersion.
2.4. Procedure
The study was approved by the Human Research Ethics Com-mittee at James Cook University. Prospective research participants,who were recruited from the Psychology subject research pool, stu-dent residences, and by word of mouth, were informed the studyfocused on pain perception but that dyads were required. Specifi-cally, we requested that interested parties make arrangements to

T. Jackson et al. / European Journal of Pain 13 (2009) 431–438 433
participate with someone they knew such as a classmate, acquain-tance, friend or relationship partner.
To experimentally manipulate appraisal, dyads were randomlyassigned to one of three conditions and each partner read a 200word orienting passage very similar to those used in publishedstudies (Jackson et al., 2005a; Van Damme et al., 2008). Each part-ner was sequestered in another room. All passages began with aninitial statement that the information below was factual. The sec-ond sentence in all passages noted that compared to past cold pres-sor studies at this university, the water temperature was loweredan extra 2 �C. This statement included because it was accurateand we were concerned that awareness of past cold pressor re-search in the setting might reduce its threat value for respondentsexposed to frostbite information.
In the Reassuring appraisal condition, both partners read an ori-enting passage describing the uses and safety of the CPT (indicatingpain can be independent of tissue damage). In the Threat appraisalcondition, both partners read an orienting passage that describedsymptoms of frostbite (tingling, numbness, loss of feeling, reducedmobility) and its effects (e.g., waxy skin, and, in serious cases, skinturning blue, gangrene, amputation). This scenario was selectedbecause numbing, pain, tingling are commonly experienced duringcold water immersions and people reading this information mightwonder if these sensations reflected possible nociception or viewthe safety of the task as uncertain.
In a Mixed appraisal condition, Participants read the Reassuringpassage and Observers were given the Threat passage. This condi-tion was included to assess the extent whether responses of threa-tened observers might attenuate tolerance and coping ofParticipants who had been ensured the task was safe. Finally, aThreatened Participant–Reassured Observer condition was not in-cluded due to ethical considerations. Specifically, in the contextof immersions that were not monitored by an experimenter, therewas a concern that this condition might create dynamics whereinObservers might unwittingly taunt Participants to continue thetask against their will, contributing to strained dynamics betweendyad members and negative views of experimental research.
Upon arriving at their scheduled appointment, each dyad mem-ber read and signed an informed consent and a self-report medicalscreen that included a checklist assessing pain/specific medicalconditions and open-ended items requesting a list of other condi-tions and current prescription medications. Following a coin toss todetermine who would serve in each role, partners were seques-tered in separate rooms. Participants completed demographicsand self-efficacy measures before reading their orienting passageand Observers completed measures of demographics and empathyprior to reading their passage. Subsequently, each Observer en-gaged in a 20-s immersion, unwitnessed by the Participant, to pro-vide an experiential referent for the task and because associatedsensations might prime appraisals of the task as potentially threat-ening or uncomfortable but safe depending on the orienting infor-mation an Observer read.
Participants were then gathered and asked to first immersetheir left hand in room temperature water to stabilize skin temper-ature. Subsequently, they were instructed to immerse the samehand in the cold water for as long as possible, albeit they couldwithdraw at any point, especially if sensations were too uncom-fortable. Observers stood under an ‘‘X” against a wall several feetbehind Participants. They were instructed to remain in this spotduring the immersion, that their role was to help in coping inany way they chose, and to respect their partner’s right to with-draw at any point. Dyads were told a DVD recorder would recordtheir transaction and the immersion time. Just before leaving theroom, the experimenter asked the pair to let him/her know whenthey finished, turned on the recorder, signaled a start (‘‘On yourmark, get set, go”), stepped out of the room, closed its door and be-
gan timing outside. Immersions were terminated after four min-utes if dyads had not done so beforehand.
After the CPT, partners completed a CSQ in separate rooms.Although effects of exposure to the frostbite information have beenestablished in studies published by different labs, as a manipula-tion check, each was asked to identify details of the orienting pas-sage s/he read to ensure information had been processed. Dyadswere then invited to guess the research hypotheses and share reac-tions about the study. Debriefing followed and email addresseswere solicited from those requesting a summary of findings.
To permit analysis of pain focus during the CPT, verbatim tran-scriptions of recorded dyad interactions were completed by two re-search assistants blind to hypotheses. Each transcribed about 50% ofinteractions and checked the other’s transcriptions against the ac-tual videotape to ensure accuracy in the obtained text records. Dueto a recording malfunction, records of one Threat, three Reassuranceand three Mixed dyad transactions were lost. The 79 remaining con-versations were subjected to word count analysis using Linguistic In-quiry and Word Count (LIWC; Pennebaker et al., 2001), a text analysisprogram that compares text files on a word-by-word basis with de-fault or user-generated dictionaries comprised of words and wordstems. In this study, we created a pain-focus dictionary from pain-re-lated words that occurred at least 20 times in the resulting 156 pagesof transcription. Specifically, the percentage of words in each tran-script that featured pain (i.e., pain, painful), hurt (i.e., hurts, hurting,hurt), cold (i.e., cold, freezing), hand and fingers were summed. Frost-bite and numb also appeared over 20 times but were omitted becauseeach was unique to the threat passage and may have primed those inthe threat condition more strongly.
3. Results
3.1. Preliminary analyses
In a post-CPT manipulation check, participants and observerswere asked to indicate what they recalled from the passage theyread before the immersion. All identified at least some salientinformation, indicating attention towards and retention of salientdetails. When queried, dyads generated gender, another person,and relationship closeness as the focus of hypotheses. In contrast,no one identified effects of pre-task information as a research pur-pose. Hence, any differences observed between appraisal groupswere unlikely to due to demand characteristics.
Table 1 provides descriptive information on demographics andother background measures for each appraisal group. Chi-squareanalyses indicated groups did not differ in sex, ethnicity, education,marital status, or presence of a family member with pain for partic-ipants and observers or for the distribution of pairings based onparticipant and observer sex (all p-values >.25). No main or inter-action effects were observed in 3 (Appraisal Condition) � 2 (Partic-ipant Gender) � 2 (Observer Gender) analyses of variance (ANOVA)for participant age, observer age, length of relationship, familiaritywith partner, or pre-task self efficacy and post-task pain level ofparticipants (all p-values >.092). However, observers in the MixedAppraisal group reported more pre-task empathy than did those inthe Threat and Reassurance groups, F(2,73) = 5.84, p < .004. Empa-thy scores of female observers (M = 67.09 SD = 9.27) were also ele-vated relative to those of male observers (M = 60.66 SD = 8.72), F(1,73) = 9.48, p < .003.
3.2. Main analyses
3.2.1. Differences between appraisal conditionsTo test hypotheses that (1) pain tolerance would be lower, (2)
cognitive coping would be reduced and (3) catastrophizing would
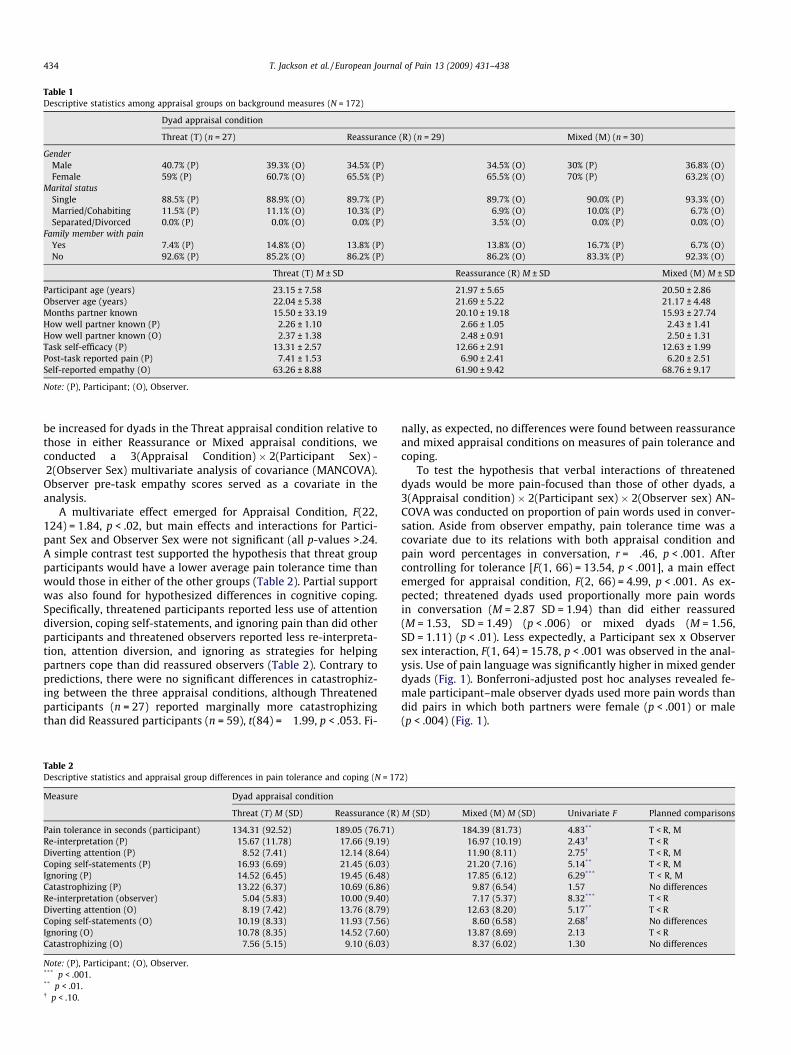
Table 1Descriptive statistics among appraisal groups on background measures (N = 172)
Dyad appraisal condition
Threat (T) (n = 27) Reassurance (R) (n = 29) Mixed (M) (n = 30)
GenderMale 40.7% (P) 39.3% (O) 34.5% (P) 34.5% (O) 30% (P) 36.8% (O)Female 59% (P) 60.7% (O) 65.5% (P) 65.5% (O) 70% (P) 63.2% (O)
Marital statusSingle 88.5% (P) 88.9% (O) 89.7% (P) 89.7% (O) 90.0% (P) 93.3% (O)Married/Cohabiting 11.5% (P) 11.1% (O) 10.3% (P) 6.9% (O) 10.0% (P) 6.7% (O)Separated/Divorced 0.0% (P) 0.0% (O) 0.0% (P) 3.5% (O) 0.0% (P) 0.0% (O)
Family member with painYes 7.4% (P) 14.8% (O) 13.8% (P) 13.8% (O) 16.7% (P) 6.7% (O)No 92.6% (P) 85.2% (O) 86.2% (P) 86.2% (O) 83.3% (P) 92.3% (O)
Threat (T) M ± SD Reassurance (R) M ± SD Mixed (M) M ± SD
Participant age (years) 23.15 ± 7.58 21.97 ± 5.65 20.50 ± 2.86Observer age (years) 22.04 ± 5.38 21.69 ± 5.22 21.17 ± 4.48Months partner known 15.50 ± 33.19 20.10 ± 19.18 15.93 ± 27.74How well partner known (P) 2.26 ± 1.10 2.66 ± 1.05 2.43 ± 1.41How well partner known (O) 2.37 ± 1.38 2.48 ± 0.91 2.50 ± 1.31Task self-efficacy (P) 13.31 ± 2.57 12.66 ± 2.91 12.63 ± 1.99Post-task reported pain (P) 7.41 ± 1.53 6.90 ± 2.41 6.20 ± 2.51Self-reported empathy (O) 63.26 ± 8.88 61.90 ± 9.42 68.76 ± 9.17
Note: (P), Participant; (O), Observer.
434 T. Jackson et al. / European Journal of Pain 13 (2009) 431–438
be increased for dyads in the Threat appraisal condition relative tothose in either Reassurance or Mixed appraisal conditions, weconducted a 3(Appraisal Condition) � 2(Participant Sex) -2(Observer Sex) multivariate analysis of covariance (MANCOVA).Observer pre-task empathy scores served as a covariate in theanalysis.
A multivariate effect emerged for Appraisal Condition, F(22,124) = 1.84, p < .02, but main effects and interactions for Partici-pant Sex and Observer Sex were not significant (all p-values >.24.A simple contrast test supported the hypothesis that threat groupparticipants would have a lower average pain tolerance time thanwould those in either of the other groups (Table 2). Partial supportwas also found for hypothesized differences in cognitive coping.Specifically, threatened participants reported less use of attentiondiversion, coping self-statements, and ignoring pain than did otherparticipants and threatened observers reported less re-interpreta-tion, attention diversion, and ignoring as strategies for helpingpartners cope than did reassured observers (Table 2). Contrary topredictions, there were no significant differences in catastrophiz-ing between the three appraisal conditions, although Threatenedparticipants (n = 27) reported marginally more catastrophizingthan did Reassured participants (n = 59), t(84) = �1.99, p < .053. Fi-
Table 2Descriptive statistics and appraisal group differences in pain tolerance and coping (N = 17
Measure Dyad appraisal condition
Threat (T) M (SD) Reassurance (R)
Pain tolerance in seconds (participant) 134.31 (92.52) 189.05 (76.71)Re-interpretation (P) 15.67 (11.78) 17.66 (9.19)Diverting attention (P) 8.52 (7.41) 12.14 (8.64)Coping self-statements (P) 16.93 (6.69) 21.45 (6.03)Ignoring (P) 14.52 (6.45) 19.45 (6.48)Catastrophizing (P) 13.22 (6.37) 10.69 (6.86)Re-interpretation (observer) 5.04 (5.83) 10.00 (9.40)Diverting attention (O) 8.19 (7.42) 13.76 (8.79)Coping self-statements (O) 10.19 (8.33) 11.93 (7.56)Ignoring (O) 10.78 (8.35) 14.52 (7.60)Catastrophizing (O) 7.56 (5.15) 9.10 (6.03)
Note: (P), Participant; (O), Observer.*** p < .001.** p < .01.� p < .10.
nally, as expected, no differences were found between reassuranceand mixed appraisal conditions on measures of pain tolerance andcoping.
To test the hypothesis that verbal interactions of threateneddyads would be more pain-focused than those of other dyads, a3(Appraisal condition) � 2(Participant sex) � 2(Observer sex) AN-COVA was conducted on proportion of pain words used in conver-sation. Aside from observer empathy, pain tolerance time was acovariate due to its relations with both appraisal condition andpain word percentages in conversation, r = �.46, p < .001. Aftercontrolling for tolerance [F(1, 66) = 13.54, p < .001], a main effectemerged for appraisal condition, F(2, 66) = 4.99, p < .001. As ex-pected; threatened dyads used proportionally more pain wordsin conversation (M = 2.87 SD = 1.94) than did either reassured(M = 1.53, SD = 1.49) (p < .006) or mixed dyads (M = 1.56,SD = 1.11) (p < .01). Less expectedly, a Participant sex x Observersex interaction, F(1, 64) = 15.78, p < .001 was observed in the anal-ysis. Use of pain language was significantly higher in mixed genderdyads (Fig. 1). Bonferroni-adjusted post hoc analyses revealed fe-male participant–male observer dyads used more pain words thandid pairs in which both partners were female (p < .001) or male(p < .004) (Fig. 1).
2)
M (SD) Mixed (M) M (SD) Univariate F Planned comparisons
184.39 (81.73) 4.83** T < R, M16.97 (10.19) 2.43� T < R11.90 (8.11) 2.75� T < R, M21.20 (7.16) 5.14** T < R, M17.85 (6.12) 6.29*** T < R, M
9.87 (6.54) 1.57 No differences7.17 (5.37) 8.32*** T < R
12.63 (8.20) 5.17** T < R8.60 (6.58) 2.68� No differences
13.87 (8.69) 2.13 T < R8.37 (6.02) 1.30 No differences

1
1.5
2
2.5
3
3.5
Male Observer Female Observer
MaleParticipant
FemaleParticipant
Fig. 1. Percentage of pain words in immersion conversations based on participantand observer gender.
Tabl
e3
Inte
rcor
rela
tion
sam
ong
pain
tole
ranc
ean
dit
spr
edic
tors
indy
adsa
mpl
e
Mea
sure
12
34
56
78
910
1112
13
1.Pa
into
lera
nce
(P)
–2.
Pain
inte
nsi
ty(P
)�
.43*
**
–3.
Thre
atap
prai
sal
(P)
�.2
8**
.18
–4.
Re-
inte
rpre
tati
on(P
).1
4�
.02
�.1
9–
5.D
iver
tin
gat
ten
tion
(P)
.09
.15
�.2
0.3
4**
–6.
Cop
ing
self
-sta
tem
ents
(P)
.35*
*�
.05
�.3
0**
.46*
**
.46*
**
–7.
Ign
orin
g(P
).5
5***
�.3
1**
�.3
4**
.44*
**
.37*
*.5
3***
–8.
Cat
astr
oph
izin
g(P
)�
.56*
**
�.6
3***
.21*
�.1
8.1
3�
.13
�.5
1***
–9.
Re-
inte
rpre
tati
on(O
).0
6.1
4�
.23*
.17
.16
.23*
.11
�.0
1–
10.D
iver
tin
gat
ten
tion
(O)
.41*
**
�.1
5�
.28*
*.0
6.3
1.3
8***
.33*
*�
.18
.43*
**
–11
.Cop
ing
stat
emen
ts(O
).0
5.1
6�
.00
�.0
0.1
5.1
7�
.01
.10
.47*
**
.27*
–12
.Ign
orin
g(O
).1
2.0
8�
19�
.05
.28*
*.1
3.1
1.0
9.3
7***
.52*
**
.64*
**
–13
.Cat
astr
oph
izin
g(O
)�
.14
.34*
*�
.10
.25*
.09
.11
.02
.13
.24*
.22*
.09
.12
–14
.Pai
nla
ngu
age
(dya
d)�
.46*
**
.34*
*.3
8***
�12
�.1
5�
.29*
*�
40***
�30
**
.02
�.4
3***
�.0
2�
.27*
.11
(P),
Part
icip
ant;
(O),
Obs
erve
r.*
p<
.05.
**
p<
.01.
***
p<
.001
.
T. Jackson et al. / European Journal of Pain 13 (2009) 431–438 435
3.2.2. The prediction of pain toleranceCorrelation and regression analyses were conducted to explore
whether observer efforts to assist in coping contributed to partici-pants’ pain tolerance, independent of participant demographic fac-tors, reported pain, appraisal condition, and coping. Initial bivariatecorrelations were calculated between pain tolerance and partici-pant, observer and dyad factors. As shown in Table 3, seven mea-sures had significant correlations (p < .01) with tolerance.Reported pain level, the only background/pain measure related totolerance time, was entered in Step 1 of the subsequent hierarchi-cal multiple regression model. Exposure to threat information (Par-ticipant) had a negative association with tolerance and wasentered in Step 2 of the equation. Three Participant coping mea-sures, catastrophizing, coping self-statements, and ignoring, corre-lated with tolerance and were entered next in the model. In Step 4,proportion of pain words used in dyad immersion conversationswas entered. Attention diversion, the only significant Observercoping strategy related to pain tolerance, was entered in Step 5.
Overall, the predictors explained Adj. R2 = .51 of the variance inpain tolerance, F(7, 71) = 12.42, p < .001, and measures within eachstep made marginal to significant contributions (Table 4). Notably,even though participant coping measures accounted for more thanhalf of the explained variance, attention diversion reported byobservers had a unique impact, beyonall participant factors inthe model.
3.2.3. Supplementary mediation analysisFinally, as reflected in Table 3, Observers whose partner had
been exposed to reassuring information used significantly moreattention diversion than Observers who partner read threateninginformation, despite being unaware of the orienting passage thattheir partner had received. To evaluate the extent to which therelation between Participant appraisal condition and Observeruse of attention diversion was mediated by factors related to eachof these variables (i.e., coping self-statements and ignoring by par-ticipants, proportion of pain-focused language in immersion con-versations), two partial correlations were calculated. First, afterstatistically controlling for the two participant coping measures,the relation of Participant appraisal to Observer attention diver-sion decreased from r = �.28, p < .01, to r = �.16, p < .16. The asso-ciation was attenuated even further when pain language wasadded as a third control; variable, r = �.05, p < .67. In sum, thecomparatively reduced use of attention diversion reported byObservers whose partners had received threatening informationwas explained by Participant coping and dyad pain focus duringthe immersion.
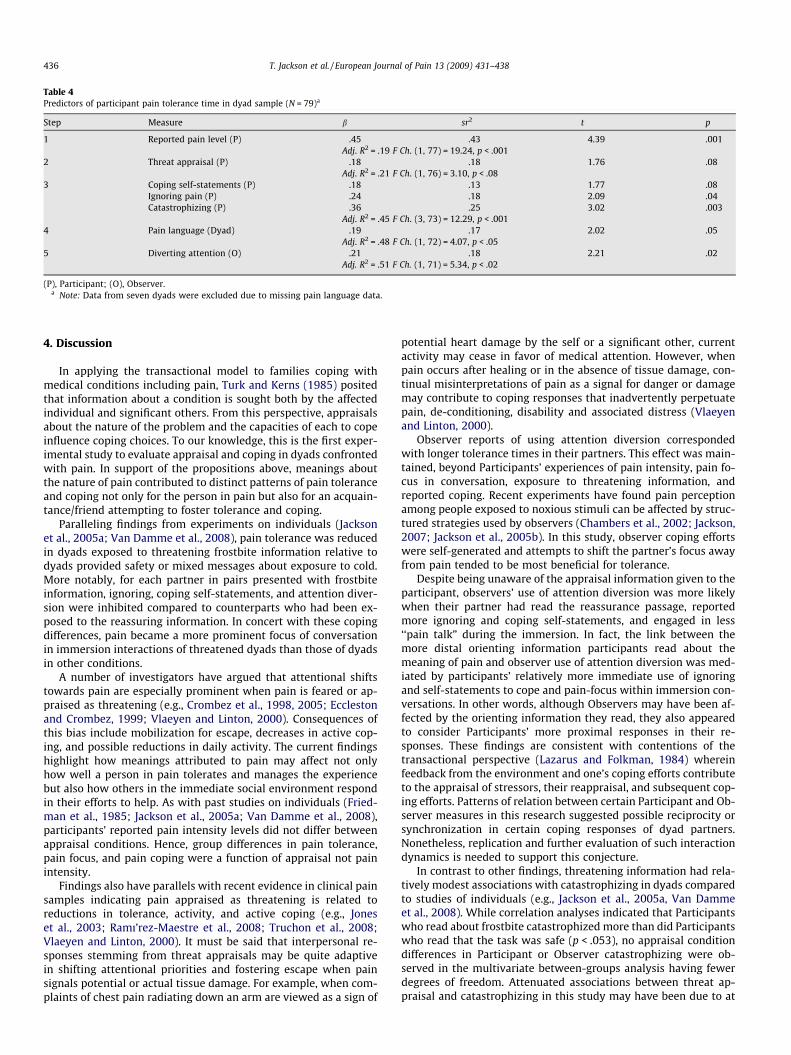
Table 4Predictors of participant pain tolerance time in dyad sample (N = 79)a
Step Measure b sr2 t p
1 Reported pain level (P) �.45 �.43 �4.39 .001Adj. R2 = .19 F Ch. (1, 77) = 19.24, p < .001
2 Threat appraisal (P) �.18 �.18 �1.76 .08Adj. R2 = .21 F Ch. (1, 76) = 3.10, p < .08
3 Coping self-statements (P) .18 .13 1.77 .08Ignoring pain (P) .24 .18 2.09 .04Catastrophizing (P) �.36 �.25 �3.02 .003
Adj. R2 = .45 F Ch. (3, 73) = 12.29, p < .0014 Pain language (Dyad) �.19 �.17 2.02 .05
Adj. R2 = .48 F Ch. (1, 72) = 4.07, p < .055 Diverting attention (O) .21 .18 2.21 .02
Adj. R2 = .51 F Ch. (1, 71) = 5.34, p < .02
(P), Participant; (O), Observer.a Note: Data from seven dyads were excluded due to missing pain language data.
436 T. Jackson et al. / European Journal of Pain 13 (2009) 431–438
4. Discussion
In applying the transactional model to families coping withmedical conditions including pain, Turk and Kerns (1985) positedthat information about a condition is sought both by the affectedindividual and significant others. From this perspective, appraisalsabout the nature of the problem and the capacities of each to copeinfluence coping choices. To our knowledge, this is the first exper-imental study to evaluate appraisal and coping in dyads confrontedwith pain. In support of the propositions above, meanings aboutthe nature of pain contributed to distinct patterns of pain toleranceand coping not only for the person in pain but also for an acquain-tance/friend attempting to foster tolerance and coping.
Paralleling findings from experiments on individuals (Jacksonet al., 2005a; Van Damme et al., 2008), pain tolerance was reducedin dyads exposed to threatening frostbite information relative todyads provided safety or mixed messages about exposure to cold.More notably, for each partner in pairs presented with frostbiteinformation, ignoring, coping self-statements, and attention diver-sion were inhibited compared to counterparts who had been ex-posed to the reassuring information. In concert with these copingdifferences, pain became a more prominent focus of conversationin immersion interactions of threatened dyads than those of dyadsin other conditions.
A number of investigators have argued that attentional shiftstowards pain are especially prominent when pain is feared or ap-praised as threatening (e.g., Crombez et al., 1998, 2005; Ecclestonand Crombez, 1999; Vlaeyen and Linton, 2000). Consequences ofthis bias include mobilization for escape, decreases in active cop-ing, and possible reductions in daily activity. The current findingshighlight how meanings attributed to pain may affect not onlyhow well a person in pain tolerates and manages the experiencebut also how others in the immediate social environment respondin their efforts to help. As with past studies on individuals (Fried-man et al., 1985; Jackson et al., 2005a; Van Damme et al., 2008),participants’ reported pain intensity levels did not differ betweenappraisal conditions. Hence, group differences in pain tolerance,pain focus, and pain coping were a function of appraisal not painintensity.
Findings also have parallels with recent evidence in clinical painsamples indicating pain appraised as threatening is related toreductions in tolerance, activity, and active coping (e.g., Joneset al., 2003; Ramı’rez-Maestre et al., 2008; Truchon et al., 2008;Vlaeyen and Linton, 2000). It must be said that interpersonal re-sponses stemming from threat appraisals may be quite adaptivein shifting attentional priorities and fostering escape when painsignals potential or actual tissue damage. For example, when com-plaints of chest pain radiating down an arm are viewed as a sign of
potential heart damage by the self or a significant other, currentactivity may cease in favor of medical attention. However, whenpain occurs after healing or in the absence of tissue damage, con-tinual misinterpretations of pain as a signal for danger or damagemay contribute to coping responses that inadvertently perpetuatepain, de-conditioning, disability and associated distress (Vlaeyenand Linton, 2000).
Observer reports of using attention diversion correspondedwith longer tolerance times in their partners. This effect was main-tained, beyond Participants’ experiences of pain intensity, pain fo-cus in conversation, exposure to threatening information, andreported coping. Recent experiments have found pain perceptionamong people exposed to noxious stimuli can be affected by struc-tured strategies used by observers (Chambers et al., 2002; Jackson,2007; Jackson et al., 2005b). In this study, observer coping effortswere self-generated and attempts to shift the partner’s focus awayfrom pain tended to be most beneficial for tolerance.
Despite being unaware of the appraisal information given to theparticipant, observers’ use of attention diversion was more likelywhen their partner had read the reassurance passage, reportedmore ignoring and coping self-statements, and engaged in less‘‘pain talk” during the immersion. In fact, the link between themore distal orienting information participants read about themeaning of pain and observer use of attention diversion was med-iated by participants’ relatively more immediate use of ignoringand self-statements to cope and pain-focus within immersion con-versations. In other words, although Observers may have been af-fected by the orienting information they read, they also appearedto consider Participants’ more proximal responses in their re-sponses. These findings are consistent with contentions of thetransactional perspective (Lazarus and Folkman, 1984) whereinfeedback from the environment and one’s coping efforts contributeto the appraisal of stressors, their reappraisal, and subsequent cop-ing efforts. Patterns of relation between certain Participant and Ob-server measures in this research suggested possible reciprocity orsynchronization in certain coping responses of dyad partners.Nonetheless, replication and further evaluation of such interactiondynamics is needed to support this conjecture.
In contrast to other findings, threatening information had rela-tively modest associations with catastrophizing in dyads comparedto studies of individuals (e.g., Jackson et al., 2005a, Van Dammeet al., 2008). While correlation analyses indicated that Participantswho read about frostbite catastrophized more than did Participantswho read that the task was safe (p < .053), no appraisal conditiondifferences in Participant or Observer catastrophizing were ob-served in the multivariate between-groups analysis having fewerdegrees of freedom. Attenuated associations between threat ap-praisal and catastrophizing in this study may have been due to at

T. Jackson et al. / European Journal of Pain 13 (2009) 431–438 437
least two factors. First, Sullivan et al. (2001) have argued thatcatastrophizing can help to mobilize social support in the face ofpotential dangers. Perhaps compared to studies of individuals cop-ing alone with pain, there was less need to catastrophize amongthreatened participants and observers due to the presence of an-other person with whom to interact during the immersion. Alter-nately, consistent with themes in the preceding paragraph andevidence that observer inferences of pain in another person are afunction of both information about pain-eliciting stimuli andbehaviour of the affected party (Sullivan et al., 2006), the impactof pre-task appraisal information on catastrophizing may havebeen dampened as a result of more immediate expressions of painor concern among participants and observers, respectively.
Neither participant nor observer sex contributed to overall paintolerance or self-reported coping. However, participant sex inter-acted with observer sex regarding pain as a focus of conversation:pain words were more prominent in cross-sex conversations thanin same sex conversations. Adding to select studies regarding ef-fects of experimenter sex on pain perception (Baker and Kirsh,1991; Fillingim, 2000), proportionately more pain-focused lan-guage was found in female participant–male observer dyads thanin same sex pairs. Mechanisms are unknown, but it is possible thatmale observers were more solicitous and/or female participantswere more expressive when interacting with a partner of the othersex. Replications and extensions to marital versus non-maritalrelationships and patient–physician transactions may further clar-ify the impact of such interactions on pain perception and coping.
In sum, this research suggests that pain appraised as a threatcontributes to lowered tolerance, reduced use of cognitive coping,and increases in pain-related language among people undergoingnoxious experimental stimulation. More notably, findings under-score how meanings that nearby others ascribe to pain may influ-ence the care-giving efforts they provide to help another in pain.Finally, this research suggests that how we respond to others inpain has implications for their capacities to bear pain, beyond theirown perceptions and experience of pain.
Strengths of this study included its consideration of interper-sonal as well as individual responses to pain, use of an experimen-tal research design, and assessment of multiple outcomes (i.e.,behavior, language, and self-report). Nonetheless, its main limita-tions must also be highlighted along with directions for future re-search. First, because a healthy, young adult sample was assessed,findings do not necessarily generalize to clinical samples, otherkinds of close relationship (e.g., spouses, parent–child) and otherage groups; these populations must be considered in future work.
Furthermore, as noted above, threatened participant–reassuredobserver dyads were omitted from the research design due to eth-ical concerns. In completing and reflecting upon the experiment,this subgroup might be considered in future designs with theinclusion of several safeguards. Specifically, briefly exposingobservers to the noxious experimental stimulus can provide themwith an experiential referent for the pain a partner may undergo.Requiring face-to-face interactions in designs can provide eachpartner important non-verbal cues absent when observers standbehind participants as in some experimenter-directed coping stud-ies. Real-time monitoring by the researcher from another roommight be considered in concert with recordings of transactions,although reduced spontaneity in transactions may be a potentialresult. Third, although it can be argued that appraisal manipula-tions had effects on pain tolerance, language and coping, directionsof causality between coping and tolerance were more ambiguousbecause coping was assessed after the immersions. Developingreliable methods for assessing pain coping in ‘‘real time” may ad-dress this issue.
Finally, because there appear to be no validated measures thatassess others’ perceptions and responses to a loved one in pain, ori-
ginal CSQ subscales were modified to assess Observer efforts toencourage specific coping strategies in the partner. If the modifiedsubscales had satisfactory internal consistencies and Observer re-ports of various cognitive strategies correlated with one anotherin expected directions, the reliability and validity of the CSQ as ameasure of others’ attempts to assist in coping requires furtherevaluation. More broadly, the current findings and clinically ori-ented studies (Kerns and Otis, 2003; Leonard and Cano, 2006;Leonard et al., 2006; Roy, 2001) highlight interpersonal influenceson personal experiences of pain and related impairment. On thisbasis, the development of interpersonal measures that considersignificant others’ pain beliefs and appraisals, their perceived con-fidence in helping loved ones in pain, and their efforts to encouragecoping in the other is essential for more fully elucidating the socialcontext of pain.
Acknowledgements
This project was supported by a China National Key SubjectFoundation of Fundamental Psychology grant (NSKD06014) toTodd Jackson. We thank Alyssa Machin for the assistance with datacollection. Thank you to Karina O’Malley and Reuben Wurm fortheir work in transcribing conversations of dyads. We thank Mr.Wayne Morris for his work in building and maintaining the coldpressor apparatus. Finally, we are grateful to two anonymousreviewers for the insightful feedback they provided in relation tothis research.
References
Baker S, Kirsh I. Cognitive mediators of pain perception and tolerance. J Pers SocPsychol 1991;61:504–11.
Chambers CT, Craig KD, Bennett SM. The impact of maternal behaviour on children’spain experiences: an experimental analysis. J Pediatric Psychol2002;27:293–301.
Crombez G, Eccleston C, Baeyens F, Eelen P. Attentional disruption is enhanced bythe threat of pain. Behav Res Ther 1998;36:195–204.
Crombez G, Van Damme S, Eccleston C. Hypervigilance to pain: an experimental andclinical analysis. Pain 2005;116:4–7.
Crombez G, Vlaeyen JWS, Heuts P, Lysens R. Pain-related fear is more disabling thanpain itself: evidence on the role of pain-related fear in chronic back paindisability. Pain 1999;80:329–39.
Eccleston C, Crombez G. Pain demands attention: a cognitive-affective model on theinterruptive function of pain. Psychol Bull 1999;125:356–66.
Fillingim RB. Sex, gender, and pain: progress in pain research andmanagement. Seattle (WA): IASP Press; 2000.
Friedman H, Thompson RB, Rosen EF. Perceived threat as a major factor in tolerancefor experimentally induced cold-water pain. J Abnormal Psychol1985;94:624–9.
Goubert L, Craig KD, Vervoot T, Morley S, Sullivan MJL, Williams AC, et al. Facingothers in pain: the effects of empathy. Pain 2005;118:285–8.
Jackson T. Interpersonal transactions and responses to cold pressor pain amongAustralian women and men. Sex Roles 2007;56:55–62.
Jackson T, Iezzi T, Chen H, Ebnet S, Eglitis K. Gender, interpersonal transactions, andthe perception of pain: an experimental analysis. J Pain 2005b;6:228–36.
Jackson T, Iezzi T, Gunderson J, Nagasaka T, Fritch A. Gender differences in painperception: The mediating role of self-efficacy beliefs. Sex Roles2002;47:561–9.
Jackson T, Pope L, Nagasaka T, Fritch A, Iezzi T, Chen H. The impact of threateninginformation about pain on coping and pain tolerance. Br J Health Psychol2005a;10:441–51.
Jones DA, Rollman GB, White KP, Hill ML, Brooke RE. The relationship betweencognitive appraisal, affect, and catastrophizing in patients with chronic pain. JPain 2003;4:267–77.
Kerns RD, Otis J. Family therapy for persons experiencing pain. Evidence for itseffectiveness. Semin Pain Med 2003;1:79–89.
Lazarus RS. Stress and emotion: a new synthesis. New York: Springer; 1999.Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984.Lawerence EJ, Shaw P, Baker D, Baron-Cohen S, Wild AS. Measuring empathy:
reliability and validity of the Empathy Quotient. Psychol Med 2004;34:911–24.Leonard MT, Cano AM. Pain affects spouses too: personal experience with pain and
catastrophizing as correlates of spouse distress. Pain 2006;126:139–46.Leonard MT, Cano AM, Johansen AB. Chronic pain in a couples context: a review and
integration of theoretical models and empirical evidence. J Pain 2006;7:377–90.Pennebaker JW, Francis ME, Booth RJ. Linguistic Inquiry and Word Count (LIWC):
LIWC2001. Mahwah (NJ): Erlbaum; 2001.

438 T. Jackson et al. / European Journal of Pain 13 (2009) 431–438
Ramı’rez-Maestre C, Esteve R, Lo’pez AE. Cognitive appraisal and coping in chronicpain patients. European J Pain 2008;12:749–56.
Roy R. Social relations and chronic pain. New York: Kluwer AcademicPublishers; 2001.
Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back painpatients: relationship to patient characteristics and current adjustment. Pain1983;17:33–44.
Sullivan MJL, Martel MO, Tripp DA, Savard A, Crombez G. Catastrophicthinking and heightened perception of pain in others. Pain2006;123:37–44.
Sullivan MJL, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al.Theoretical perspectives on the relation between catastrophizing and pain. ClinJ Pain 2001;17:52–64.
Truchon M, Cote D, Fillion L, Arsenault B, Dionne C. Low-back-pain relateddisability: an integration of psychological risk factors into the stress processmodel. Pain 2008.
Turk DC, Kerns RD. The family in health and illness. In: Turk DC, Kerns RD, editors.Health, illness and families: a life span perspective. New York: Wiley; 1985. p.1–22.
Unruh AM, Ritchie J, Merskey H. Does gender affect appraisal of pain and paincoping strategies? Clin J Pain 1999;15:31–40.
Van Damme S, Crombez G, Van Nieuwenborgh-De Wever K, Goubert L. Is distractionless effective when pain is threatening? An experimental investigation with thecold pressor task. Euro J Pain 2008;12:60–7.
Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronicmusculoskeletal pain: a state of the art. Pain 2000;85:317–32.