efficient and effective endodontics - iowa dental handout.pdf · the test cavity is done rarely...
TRANSCRIPT

Our Specialty Dental Education | Your Success | Their Satisfaction
1-800-662-1202 For the latest information consult www.TulsaDentalSpecialties.com
Course Hand Out and Reference Guide
DENTSPLY International is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
The formal continuing education programs of this program provider are accepted by the Academy of General Dentistry (AGD) for Fellowship/Mastership credit. The current term of acceptance extends from 5/2014 through 6/2018. AGD Provider ID# 219143 ©2015 DENTSPLY Tulsa Dental Specialties, Inc. EEEHANDOUT Rev. 1 8/15
Efficient and
Effective
Endodontics
Enhance Your Practice and Skills Through Endodontics

Efficient and Effective Endodontics
PAGE 1
©2015
COURSE OVERVIEW
• Diagnosis
• Access and Glide Path
• Reciprocating Shaping Technique
• Endodontic Microbiology and Irrigation Protocol
• Obturation Concepts and Technique
• Post-treatment Disease
• Review
The presence of microorganism, their byproducts and their supporting biofilms cause disease in the pulp, which can extend to the supporting periodontium (apical/peradicular periodontitis). Root canal procedures are designed to prevent apical/ peradicular periodontitis and to provide an environment within the tooth to allow the human body to heal the inflammatory/infectious responses. Each step within the scope of root canal treatment (diagnosis, access, canal location, canal shaping, canal disinfection, canal obturation as well as temporary and final restorations) will significantly affect the outcome.
NOTES:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Efficient and Effective Endodontics
PAGE 2
©2015
DIAGNOSIS
The standard diagnostic framework in use today is the SOAP format.
Subjective information is the patient’s chief complaint and a history.
Objective Findings are observed conditions in the area and the results of
clinical testing. Assessment is the diagnosis made, and Plan of treatment
is self-explanatory.
• The Medical History Form must be completed by patient. Have the
patient sign and date the form. The clinician must review the form
completely, asking pertinent follow-up questions and considering all
significant conditions which can impact the patient’s oral health and
their suitability for successful endodontic treatment.
• The clinical exam should always include documentation of
everything of relevance (remembering however that seemingly
irrelevant findings may prove to be the most significant in the long
run. This is why insurance carriers insist on documenting
everything.).
• During the visual examination, the clinician is looking for areas of
swelling, asymmetry, discoloration, and anything else that appears
to not be Within Normal Limits (WNL).
• Palpation is performed to detect periapical inflammation that has
spread to the surface mucosa and may indicate an underlying
endodontic problem.
• Percussion is another periapical test looking for inflammation.
• If a sinus tract is present, it must be traced with a gutta percha
point.
• Document all caries, apparent tooth fractures and restorations in
the area looking for a cause for the endodontic disease.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 3
©2015
DIAGNOSIS
• Periodontal probing is mandatory and some states even require it’s
use in the State dental practice Act. It is critically important and
should not be overlooked!
• Note any exposed dentin. Exposed dentin can be quite sensitive
creating a clinical reversible pulpitis.
• Wear facets indicate the presence of strong occlusal forces and
perhaps a para-functional habit such as bruxism. Occlusal trauma is
frequently misdiagnosed as endodontic disease.
• When exposing radiographs, some form of film positioning
device is indicated if it is at all possible to use one. The
radiographic angulations are much more reproducible and
diagnostic for endodontic purposes when compared to the
bisecting angle technique.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 4
©2015
DIAGNOSIS
Every tooth that is considered for endodontics therapy requires an
appropriate cold test. Water ice is convenient to do (fill some used,
cleaned, and disinfected anesthetic cartridges with water and freeze
them to make ice pencils) and delivers cold in a physiologic temperature
range, but cold water from the melting ice can affect other teeth. CO2
snow requires an extensive investment in armamentarium and delivers
cold at a very non-physiologic –70 degrees. If the dry ice pellet sublimes,
shrinks, and falls our of the carrier, it can cause an area of frostbite to
the tissues. Tetraflouroethane spray (Endo Ice) is convenient and easy
to use, but the temperatures are variable so accuracy may be
compromised.
Heat tests should be applied if the chief complaint is of heat sensitivity (indicating a partially necrotic pulp). These can be performed using warm gutta percha, friction from a rubber cup or disk, or application of hot water after rubber dam placement (although the placement of the dam without anesthetic may be painful for the patient).
Bite tests are performed using a Tooth Slooth or similar instrument, wooden stick, or cotton roll. A positive test may indicate a crack in the tooth or perhaps periapical inflammation.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 5
©2015
DIAGNOSIS
Electric pulp test is of limited value when a tooth is heavily restored,
and so will not be used frequently. It is very valuable, however, in
trauma cases.
Transillumination with a fiber optic light source and magnification can reveal fractures in teeth since light transmission through the tooth is disrupted by the crack so the area beyond it is rendered darker.
Selective Anesthesia tests are relatively non-specific. It is impossible, even with intraosseous or intraligamentary injection to anesthetize only one tooth and not the adjacent ones. Thus, this test is only useful to determine if the pain is coming from the upper or lower teeth as a group, and for ruling our non-dental facial pain conditions.
The test cavity is done rarely because of patient apprehension, and on occasion one finds out that the pulp is vital only at the moment of exposure which then condemns the patient to an otherwise unnecessary root canal procedure.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 6
©2015
ACCESS
There are six fundamental aspects for proper access.
• Must permit the removal of the entire chamber contents. The pulp chamber roof must be completely unroofed. This not only allows pulp and other potentially infected material to remain in the chamber during treatment, but the restricted size of the access can cause difficulty in finding all of the canals.
• Must enable complete, direct vision of pulp chamber floor and orifices. Enhanced vision enabled by expanding the access preparation makes it easier to find all of the major canals.
• Must facilitate introduction of endodontic instruments into radicular pulp. An access that is too small makes it difficult to maneuver the instruments into the canals even when they have all been found. This is frustrating for the clinician and can result in procedural mishaps.
• Must provide straight-line access. The overall curvature that the
instruments need to negotiate to get to the terminus is decreased,
making complete shaping, disinfection and obturation more likely.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 7
©2015
INSTRUMENTATION RULES
• Must provide a positive support for temporization. The importance
of providing a tight interappointment seal cannot be over
emphasized. Dislodgement of a restoration will break the seal
allowing ingress of oral fluids and contamination of the canal
system.
• Must always have four walls. Badly broken down teeth provide a
challenge in canal isolation and temporization. Without four walls,
the access preparation cannot retain irrigating solutions during
instrumentation and badly broken down teeth are difficult to seal
with a dental dam.
• All Mechanized Instrumentation Begins with a Hand File!
• Obtain straight line access to the orifice of the canal.
• The canal should be kept unobstructed and the foramen patent.
• Instrumentation should always take place with copious and
abundant irrigation using sodium hypochlorite solution.
• Never exert too much apical pressure (imagine the amount of
pressure used with a mechanical pencil).
• The maximum working time with a NiTi instrument should never
exceed more than 10 seconds within the canal.
• Wipe clean and observe the instrument before and after each use
to observe for metal fatigue or deformation.
• Always maintain a constant speed with traditional rotary
instruments = RPM.
• Observe single use guidelines.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 8
©2015
GLIDE PATH
Endodontic instrumentation is generally broken into three sub-sections.
After the tooth is opened and the pulp chamber is accessed the canal
orifices are identified. With the orifices exposed, a straight line access is
made prior to the exploration and securing of the glide path. Once a
good glide path has been obtained, the shaping of the canal space can
proceed.
ProGlider®
• .16mm tip and progressive taper.
• Speed (300 RPM).
• Torque (2 Ncm is recommended initially, higher torque settings should only be utilized by clinicians experienced with the instrument).
• Irrigate frequently (between each pass) and confirm patency.
• Clean the flutes frequently and check for distortion.
• Passively follow the previously secured canal space until reaching working length.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 9
©2015
MOTOR SETTINGS
e3® operation:
To choose a different file system the file system field (“sys”) in the lower
row must be active. Move the arrow to the ”sys” field by pressing g and
f. By pressing the + and - keys, you can scroll through all systems until
the display selects the desired system. It is not necessary to confirm the
selection.
ProMark® operation:
Press preset 1. This will change the display to PathFile®. The
PROGLIDER® instruments use the same torque and speed settings.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 10
©2015
GLIDE PATH HANDS-ON CHECK LIST
WITH PLASTIC TOOTH
1. Confirm straight line access to canal orifice.
2. Explore the canal up to a .10 K-file.
3. Establish working length.
4. Confirm patency with a .10 K-file
5. Verify a smooth, reproducible glide path.
4. Irrigate.
5. Confirm motor settings.
6. Use PROGLIDER® in one or more passes until the full working length is
reached.
7. Irrigate the expanded glide path.
8. Reconfirm the working length with a .10 K-file.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 11
©2015
SINGLE USE
NiTi is strong and flexible. But it still wears out. There are a number of
factors that contribute to the length of a NiTi instrument’s useful life.
But the question is; do you really know exactly when that file has
reached the end of its natural life?
High magnification Scanning Electron Microscope images show the wear
that can occur after just one use.
A second use contributes more wear.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 12
©2015
SINGLE USE
The wear shown in these SEM images is not visible to the clinician. It is
also important to note that tension on instruments builds up over the
course of its life. Naturally, different diameters of instruments have
different levels of resistance to cyclic fatigue forces. Contact with NaOCl
and EDTA also has an impact.
Researchers have shown through atomic force microscopy, three-
dimensional images and roughness values that short-term contact
between NaOCl and EDTA endodontic irrigants and NiTi instruments
caused alterations in the surface of instruments. Cutting efficiency is
also affected by use. All files rapidly deteriorate when machining dentin
and the decline in efficiency is significant.
Another aspect of single use vs. multiple use to consider is the potential
for cross contamination. In 2013 a dentist in Oklahoma made news
around the world. His dirty dental instruments were directly linked to a
patient contracting Hepatitis C. What about other diseases that might
be spread? The prions for Creutzfeldt-Jakob have not been detected yet
in dental pulp. But new variant CJD patients may harbor more
infectivity.
SINGLE USE
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 13
©2015
SINGLE USE
Instruments that are not pre-sterilized by the manufacturer pose a risk.
Attempts to sterilize previously-used instruments are also problematic.
Research indicates that a number of steps are necessary, and potentially
infectious agent carrying debris cannot always be removed completely.
The multitude of steps with current protocols causes corrosion to the
instruments.
There is strong evidence of the metallurgic property changes in all
aspects of endodontic instruments during root canal preparation.
Combine that information with the known complexities of tooth
anatomy that endodontic instruments work in (3D curvatures, etc.) and
the inability to completely clean a previously used instrument and the
cost/ benefit of single use vs. multiple uses, outweighs all risks in the
decision making of endodontic instrument failure.
Both ProGlider® and WaveOne® Gold come pre-sterilized from the
manufacturer and are recommended as single patient use.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 14
©2015
WORKING LENGTH
Knowledge of the anatomy is critical to the success of any endodontic
procedure. The apical foramen is the large open end of a funnel at the
root end and is not the target for the apical extent of our canal
preparation. The actual target for working length determination is the
apical constriction or cemento-dentinal junction. It is important to
remember that the apical constriction is not visible on radiographs.
Determination of the working length begins with the use of a non-
distorted radiograph to make an estimate of the working length. Work a
small hand file to that estimated working length and make a radiograph
(bisecting angle). Adjust the file to .5 to 1 mm short of radiographic
apex. If you are more than 2 mm from the apex you should adjust the
file and make another radiograph.
Application of an electronic apex locator is well accepted. Accuracy of
new units such as the ProMark® is higher than older models such as the
RootZX®
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 15
©2015
WORKING LENGTH
When employing an electronic apex locator note there are several tips
to help obtain an accurate reading.
- Canals can be wet, but chamber must be dry. There
should be no shared fluid between canals and no saliva
from open margins.
- Maintain a reproducible reference point, avoiding
irregularities.
- Advance the file until a reading is obtained.
- Adjust long readings by pulling file back in a
counterclockwise direction.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 16
©2015
CANAL SHAPING WITH WAVEONE® GOLD
There the four WaveOne® Gold files. The “Primary” instrument is shown
in the image below in the center. It is a .25 at the tip and the initial
taper is .07. This will be sufficient to prepare the vast majority of canals.
The taper changes on all of the WaveOne® Gold files as you progress
back from the tip. In most cases, a single instrument is used to
complete the shape of a single canal.
The WaveOne® Gold instruments are utilized in a specially designed
reciprocating motor with a unique motion with fewer clockwise degrees
and more counter-clockwise degrees. The instrument tip is often
referred to as a semi-active tip. These instruments are come in 21, 25,
and 31 mm lengths.
Before introducing any mechanized instrument always negotiate the
canals with hand files and a lubricant, such as ProLube®. Incorporating a
lubricant in the pulp chamber during hand filing helps to minimize the
chance of apical blockage with pulp tissue. Establish apical patency with
small hand files, starting with an .08 k-file in small canals. Begin with a
.10 k-file in medium and large canals. Then utilize the ProGlider® to
establish a glide path for the WaveOne® Gold shaping instrument.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 17
©2015
CANAL SHAPING WITH WAVEONE® GOLD
e3 operation:
To choose a different file system the file system field (“sys”) in the lower
row must be active. Move the arrow to the ”sys” field by pressing g and
f. By pressing the + and - keys, you can scroll through all systems until
the display selects the desired system (WAVEONE ALL). Use the same
setting for any/all WaveOne® Gold file sizes.
ProMark® operation:
Press preset 2 for all sizes of the WaveOne® Gold instruments. The
system will automatically switch to reciprocation mode and lock in the
appropriate back and forth angles as well as the speed and torque
settings for all file sizes.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
Efficient and Effective Endodontics
PAGE 18
©2015
CANAL SHAPING HANDS-ON CHECK LIST
WITH PLASTIC TOOTH
1. Reconfirm the working length and glide path with a .10 K-file.
2. Select the preprogrammed WaveOne® Gold motor settings.
3. Select the WaveOne® Gold Primary file.
4. Initiate shaping procedures with the all WaveOne® Gold files in the presence of your irrigant. Use a gentle inward motion, with short 2 – 3 mm amplitude strokes, to passively advance the WaveOne® Gold file until it does not easily progress anymore.
5. Withdraw the WaveOne® Gold file, remove the debris and inspect its cutting flutes.
6. Irrigate, Reconfirm the working length with a .10 K-file, Irrigate.
7. Reintroduce the file in the presence of your irrigant. Repeat the shaping technique. Only advance 2 – 3 mm with each pass.
8. Irrigate, Reconfirm the working length with a .10 K-file, Irrigate.
9. With irrigant in the canal space, reintroduce the file. Because most canals are between 9 and 11mm, the third pass will often achieve working length. The finished shape is confirmed if the apical flutes of the file are loaded with dentin
10. Confirm patency, verify the glide path and irrigate.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 19
©2015
CANAL SHAPING HANDS-ON CHECK LIST
WITH PLASTIC TOOTH
11. Gauge the size of the foramen with an ISO hand file that has the same diameter as the WaveOne® Gold file carried to working length. If the gauging hand file is snug at length, the preparation is finished. If the gauging file is loose at length, generally use a larger WaveOne® Gold file to finish the preparation.
In very rare cases you need to select the Small WaveOne® Gold file (020/07v) if the Primary WaveOne® Gold file (025/07v) will not readily advance to the desired length. Use this Small WaveOne® Gold file to either initially or fully shape the apical one-third.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 20
©2015
ENDODONTIC MICROBIOLOGY
There is anatomy which no rotary instrument can possibly clean. The
only way to affect webs, fins and anastomoses is through the use of
chemical cleaning agents. Therefore irrigation is the basis of the
cleaning of the canal.
It is well accepted that instrumentation of the canal space creates what
is known as a ‘smear layer’. The smear layer is laden with soft and hard
tissue remnants, along with bacteria, endotoxins, and inflammatory
substances. Removal of the smear layer enhances disinfection and
adaptation of root filling materials to the dentin, thereby creating a
better seal in the root canal system. The first line of defense in
controlling and eliminating endodontic infection is the host’s defenses.
Defense cells try to prevent spread of the infection and invasion of
bacteria into periapical tissue and bone. In many other infections of the
body, the host’s defense system, sometimes helped by antibiotics, is all
that is required for healing. But with endodontic infections more needs
to be done to obtain healing. The anatomy of the root canal system and
a lack of circulation in the necrotic root canal are the main reasons for
this the extra effort.
The other key area of control and elimination of endodontic infection
revolves around a focus of minimizing the potential for re-infection. Use
good practices when filling the canal space and create a good coronal
seal.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 21
©2015
ENDODONTIC MICROBIOLOGY
Choosing the size of the EndoActivator® tip should be done in
conjunction with the size of the canal being treated. There must be
sufficient room in the apical region for the tip to move in the solution.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 22
©2015
IRRIGATION PROTOCOL
• Use paper points to remove extra NaOCl left from shaping procedure.
• Express 2 mL of QMix® 2in1 into the canal.
• Agitate for 60 seconds.
• Use suction and paper points to completely dry the canal.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 23
©2015
OBTURATION CONCEPTS
The purposes of obturating the prepared root canal space are well
founded in the contemporary art and science of endodontology and can
be simply stated as (1) to eliminate all avenues of leakage from the oral
cavity or the periradicular tissues into the root canal system and (2) to
seal within the system any irritants that cannot be fully removed during
canal cleaning and shaping procedures. The rationale for these
objectives recognizes that microbial irritants (microorganisms, toxins,
and metabolites) along with products of pulp tissue degeneration are
the prime causes for pulpal demise and its subsequent extension into
the periradicular tissue. Failure to eliminate these etiologic factors and
to prevent further irritation via continued contamination of the root
canal system are the prime causes for failure with nonsurgical and
surgical root canal treatment.
The importance of three-dimensional obturation of the root canal
system cannot be overstated. However, the ability to achieve this goal is
primarily dependent on the quality of the canal cleaning and shaping
and the skill of the clinician. Even with the most skilled clinician,
however, many other factors enter into the ultimate success or failure
of each case, such as materials used, how they are used, and
radiographic interpretation of process and product. What may loom as
the most important attainment is the ultimate coronal restoration of
the tooth following canal obturation.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 24
©2015
OBTURATION CONCEPTS
There is reasonable evidence to suggest that coronal leakage through
improperly placed restorations after root canal treatment and failure of
the restorative treatment or lack of health of the supporting
periodontium are the final determinants of success or failure in
treatment.
The use of a sealer during root canal obturation is essential for success.
Not only does it enhance the possible attainment of an impervious seal
but also serves as a filler for canal irregularities and minor discrepancies
between the root canal wall and core filling material. Sealers are often
expressed through lateral or accessory canals and can assist in microbial
control should there be microorganisms left on the root canal walls or in
the tubules. Sealers can also serve as lubricants to assist in the thorough
seating of the core filling material during compaction. In canals in which
the smear layer has been removed, many sealers demonstrate
increased adhesive properties to dentin, in addition to flowing into the
patent tubules.
Sealers should be mixed to a creamy consistency, allowing it to adhere
to the master cone and not ball up at the shaft of the cone leaving the
gutta-percha exposed – rather the sealer should adhere to the cone
evenly along its length and at the end of the cone.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 25
©2015
OBTURATION CONCEPTS
Over the years numerous methods have been advocated for obturating
the prepared root canal system, each with their own claims of ease,
efficiency, or superiority. Contemporary obturation techniques are no
different; although they do reflect a certain degree of sophistication and
technologic advancement, most contemporary techniques still rely on
gutta-percha and sealer to achieve their goal--a three-dimensional filling
of the cleaned and shaped root canal space. Therefore this discussion
focuses on the basics of root canal obturation, with an emphasis on
techniques and variations thereof that have proven successful and easy
to master.
Four basic techniques exist for the obturation of the root canal system
with gutta-percha and sealer: (1) the cold compaction of gutta-percha;
(2) the compaction of gutta-percha that has been heat softened in the
canal and compacted until it has cooled with cold instruments; (3) the
compaction of gutta-percha that has been thermoplasticized, injected
into the system, and compacted with cold instruments; and (4) the
compaction of gutta-percha that has been placed in the canal and
softened through mechanical means. A multitude of variations on these
four basic themes exists.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 26
©2015
GUTTACORE® CROSSLINKED GUTTA PERCHA
CARRIER TECHNIQUE
The most important concept of the GuttaCore® techniqe is what is
known as crosslinking. This is a proven scientific process with numerous
applications the world over. With GuttaCore®, the process allows for
the creation of a firm, non-melting, gutta-percha core.
At the molecular level, gutta-percha is polymer chain. The flowable
gutta-percha of the GuttaCore® obturator is depicted with the blue
molecules.
This image above shows an artist’s idea of the molecular view of a
gutta-percha polymer chain. In the bubble on the right, the crosslinkers
are added to the gutta-percha and activated with an initiator (energy).
These crosslinkers bond the gutta-percha to provide the subtle strength
and flexibility of the GuttaCore® core.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 27
©2015
GUTTACORE® CROSSLINKED GUTTA PERCHA
CARRIER TECHNIQUE
A minimum 25/.04 shape is necessary for the GuttaCore® technique.
Check passivity by taking the size verifier to working length and confirm
by rotating in the canal 180°. If the fit is passive, remove a
corresponding GuttaCore® Obturator from the package and proceed to
final irrigation.
If the fit is not passive, use the size verifier as a finishing file to gently
enlarge the canal terminus or select a smaller size verifier. If the smaller
size verifier fits passively, remove a GuttaCore® Obturator of the same
size as the verifier and proceed to final irrigation.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 28
©2015
GUTTACORE® CROSSLINKED GUTTA PERCHA
CARRIER TECHNIQUE
Use a sterile paper point of the same tip and taper as the last file taken
to working length. Brush a very light coating of ThermaSeal® Plus
Ribbon® sealer circumferentially to the canal wall with the paper point.
To help ensure the obturator reaches working length, use an additional
absorbent point to remove any excess sealer that may have
accumulated on the canal walls or pooled in the apex.
If obturating more than one canal in a single tooth, place sealer in all
the canals at the same time. This facilitates removal of excess gutta-
percha by preventing the gutta-percha from sticking to other orifices or
dentin.
If the canal has been properly shaped and the gutta-percha properly
heated, the obturator should seat to place without twisting or forcing.
To avoid overextension, don’t force the GuttaCore® Obturator beyond
the working length. You will note a backflow of sealer and gutta-percha
resulting in an accumulation at the orifice.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 29
©2015
GUTTACORE® CROSSLINKED GUTTA PERCHA
CARRIER TECHNIQUE
This is to be expected, especially in multi-rooted teeth, because the
obturator is designed with excess gutta-percha to accommodate even
the most widely flared or anatomically irregular canals.
Place paper point in any unfilled canals until time for obturation.
One technique for removing the handle from the shaft is by bending to
either side of the canal wall until the handle breaks loose from the
stable portion in the canal space.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 30
©2015
CANAL OBTURATION HANDS-ON CHECK LIST
WITH PLASTIC TOOTH
1. Confirm the canal shape and a passive fit with the GuttaCore® Size Verifier.
2. Completely dry the canal space with paper points.
3. Place a small amount of sealer in the canal space with a paper point.
4. Blot out the excess sealer with a clean paper point.
5. Set the rubber stop on the GuttaCore® carrier using the length determination rings.
6. Place the obturator in the oven with the stopper below the oven arm.
7. Gently press the arm down so that the obturator slides into the well without touching the sides of the heating well.
8. Heat the obturator in the GuttaCore®oven. Use setting #1 for all GuttaCore® obturator sizes.
9. After the oven beeps, gently press the oven arm release allowing the arm to lift the obturator out of the well.
10. Grasping the obturator by the handle, place it in the designated canal in one smooth stroke until the rubber stopper touches the reference point on the crown of the tooth indicating it has reached working length.
11. After a few moments of cooling the handle may be removed by simply bending it back and forth.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
Efficient and Effective Endodontics
PAGE 31
©2015
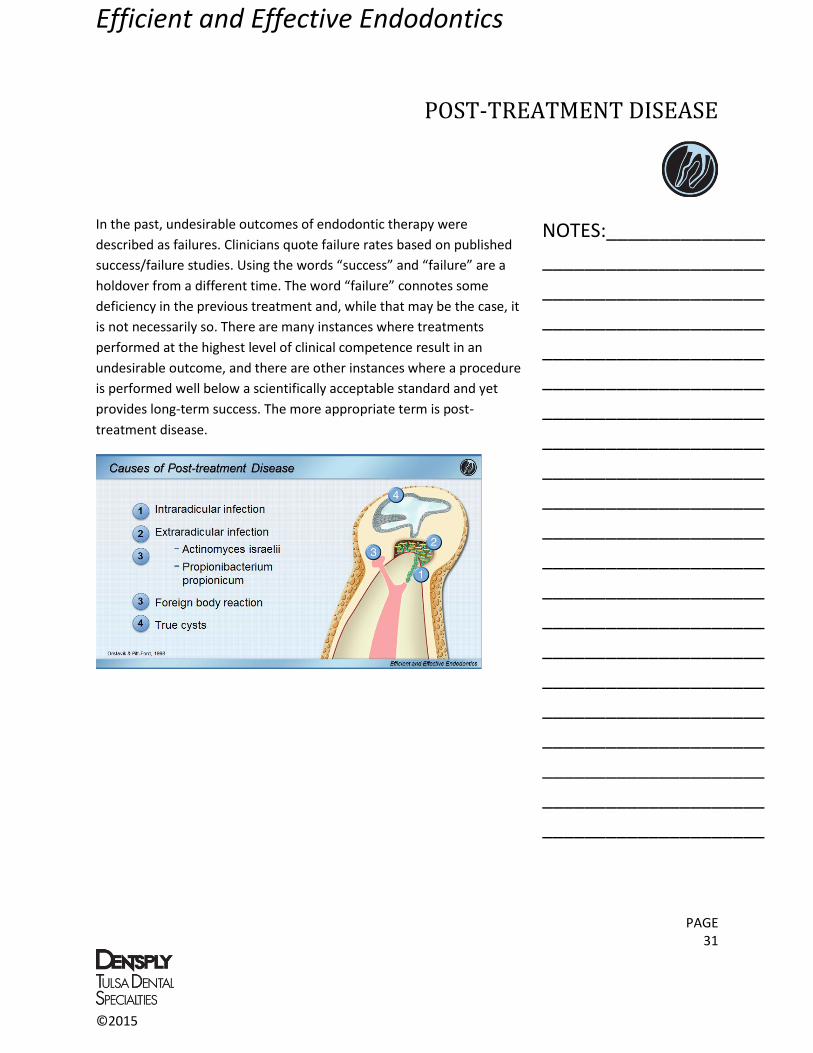
POST-TREATMENT DISEASE
In the past, undesirable outcomes of endodontic therapy were
described as failures. Clinicians quote failure rates based on published
success/failure studies. Using the words “success” and “failure” are a
holdover from a different time. The word “failure” connotes some
deficiency in the previous treatment and, while that may be the case, it
is not necessarily so. There are many instances where treatments
performed at the highest level of clinical competence result in an
undesirable outcome, and there are other instances where a procedure
is performed well below a scientifically acceptable standard and yet
provides long-term success. The more appropriate term is post-
treatment disease.
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 32
©2015
REVIEW
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 33
©2015
REVIEW
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 34
©2015
REVIEW
NOTES:_______________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________
_____________________

Efficient and Effective Endodontics
PAGE 35
©2015
ADDITIONAL MATERIALS:
AAE Case Assessment Form
References

Efficient and Effective Endodontics
PAGE 36
©2015

Efficient and Effective Endodontics
PAGE 37
©2015

Efficient and Effective Endodontics
PAGE 38
©2015
REFERENCES
Gutmann JL, Lovdahl PE. Problem Solving in Endodontics, 5th edition, Elsevier, St. Louis, 2011, Part 1,
Chapters 1-6.
Castellucci A. Access cavity and endodontic anatomy. Endodontics Vol 1, Florence, Il Tridente Edizioni
Odontiatriche, 2004.
Vertucci FJ, Haddix JE. Tooth morphology and access cavity preparation. In Hargreaves KM, Cohen S
(eds) Cohen’s Pathways of the Pulp, 10th edition, St. Louis, Mosby Elsevier 2011
Berutti et al 2013
Moscoso S, Pineda K, Basilio J, et al. Evaluation of Dentaport ZX and Raypex 6 electronic apex locators:
An in vivo study Med Oral Patol Cir Bucal. 2013 Ahead of Print. (SPAIN: Independent & Clinical)
Lucena C, Lopez JM, Martin JA, et al. Accuracy of working length measurement: electronic apex locator
versus cone-beam computed tomography. International Endodontic Journal. 2013 Epub Ahead of
Print.
Hernandez HM, Nissan R. Comparing Accuracy of Two Electronic Apex Locators: the Root ZX mini vs.
the ProMark. An In Vitro Study. Pending Publication. 2013 (Temple University)
Rapisarda, Ernesto et al. Wear of Nickel-Titanium Endodontic Instruments Evaluated by Scanning Electron Microscopy: Effect of Ion Implantation. JOE , Volume 27 , Issue 9 , 588 - 592
Cheryl J. Ullmann, Ove A. Peters. Effect of Cyclic Fatigue on Static Fracture Loads in ProTaper Nickel-Titanium Rotary Instruments. JOE, Vol. 31, No. 3, pag. 183-186, Mar. 2005
Ametrano G1, D'Antò V, Di Caprio MP, Simeone M, Rengo S, Spagnuolo G.. Effects of sodium
hypochlorite and ethylenediaminetetraacetic acid on rotary nickel-titanium instruments evaluated
using atomic force microscopy. Int Endod J. 2011 Mar;44(3):203-9
Ove A. Peters, Jan O. Roehlike, Michael A. Baumann. Effect of Immersion in Sodium Hypochlorite on
Torque and Fatigue Resistance of Nickel-Titanium Instruments. Journal of Endodontics, Vol. 33, Issue
5, p589–593
e a a e i, ve t ten an, a p ng e g The endodontic file is a disposable instrument.
Journal of Endodontics, Vol. 21, Issue 9, p451–455. September, 1995

Efficient and Effective Endodontics
PAGE 39
©2015
REFERENCES
Ingrosso, Pisani and Pocchiari; Transmission of the 263K Scrapie Straing by the Dental Route. J Gen
Vir, 80:3043-3047, Nov. 1999
Sonntag, D., Peters, O.; Effect of Prion Decontamination Protocols on Nickel-Titanium Rotary Surfaces.
JOE, Vol. 33, No. 5, pag. 442-446, Apr. 2007
Kuttler, Y. et al. Microscopic Investigation of Root Apexes JADA, vol. 50, No. 5, page. 544-552, May
1955
Betancourt Elisa; Bonilla Carmen; Kuttler Sergio; Ruddle Cliff; Webber Julian & Hardigan Patrick;.
Incidence of Third Medial Canal in Mesial Roots of Lower Molars: A Micro CT Study. June 2010
Love, R.; Regional variation in root dentinal tubule infection by Streptococcus gordonii . J Endod
1996;22:290-3
Bystrom A, Claesson R, Sundqvist G. The antibacterial effect of camphorated paramonochlorophenol,
camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endod Dent
Traumatol. 1985 Oct;1(5):170-5.
Sjögren U, Figdor D, Spångberg L, Sundqvist G. The antimicrobial effect of calcium hydroxide as a
short-term intracanal dressing. Int Endod J. 1991 May;24(3):119-25.
Ørstavik D, Kerekes K, Molven O. Effects of extensive apical reaming and calcium hydroxide dressing on
bacterial infection during treatment of apical periodontitis: a pilot study. Int Endod J 1991: 24: 1–7.
Shuping GB, Orstavik D, Sigurdsson A, Trope M. Reduction of intra-canal bacteria using nickel-
titanium rotary instrumentation and various medications. J Endod 2000: 26: 751–755.
Peters LB, Van Winkelhoff AJ, Buijs JF, Wesselink PR. Effects of instrumentation, irrigation and dressing
with calcium hydroxide on infection in pulpless teeth with periapical bone lesions. Int Endod J 2002:
35: 13–21.
Haapasalo, M., Can I use chlorhexidine as the only irrigating solution in my endodontic treatments?; J
Can Dent Assoc 2011;77:b16;
Tatsuta CT, Morgan LA, Baumgartner JC, Adey JD. Effect of calcium hydroxide and four irrigation
regimens on instrumented and uninstrumented canal wall topography. J Endod. 1999;25(2):93-8.

Efficient and Effective Endodontics
PAGE 40
©2015
REFERENCES
Marending M, Paqué F, Fischer J, Zehnder M. Impact of irrigant sequence on mechanical properties of
human root dentin. J Endod. 2007;33(11):1325-8.
Dai L, Khechen K, Khan S, Gillen B, Loushine B, Wimmer C, Gutmann J, Pashley D, Tay F. The Effect of
QMix, an Experimental Antibacterial Root Canal Irrigant, on Removal of Canal Wall Smear Layer and
Debris. J Endod 2011;37:80-4
Cheung GS, Stock CJ. In vitro cleaning ability of root canal irrigants with and without endosonics. Int
Endod J. 1993;26:334-43.
Becker TD, Woollard GW. Endodontic irrigation. Gen Dent. 2001;49:272-6.
Stojicic S, Zivkovic S, Qian W, Zhang H, Haapasalo M. Tissue dissolution by sodium hypochlorite: effect
of concentration, temperature, agitation, and surfactant. J Endod. 2010;36:1558-62.
Caron G: Cleaning efficiency of the apical millimeters of curved canals using three different modalities
of irrigant activation: a SEM study, Master Thesis, Paris 7 University, 2006.
Naidorf IJ: Clinical microbiology in endodontics, Dent Clin North Am 18:329, 1974.
Buckley M, Spångberg L: The prevalence and technical quality of endodontic treatment in an American
subpopulation, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 79:92, 1995.
Gutmann JL: Clinical, radiographic, and histologic perspectives on success and failure in endodontics,
Dent Clin North Am 36:379, 1992.
Rud J, Andreasen JO: A study of failures after endodontic surgery by radiographic, histologic and
stereomicroscopic methods, Int J Oral Surg 1:311, 1972.
Sjögren U, Hägglund B, Sundqvist G, Wing K: Factors affecting the long-term results of endodontic
treatment, J Endod 16:498, 1990.
Saunders WP, Saunders EM: Coronal leakage as a cause of failure in root canal therapy: a review,
Endod Dent Traumatol 10:105, 1994.
Vire DE: Failure of endodontically treated teeth, J Endod 17:338, 1991.
Ray HA, Trope M: Periapical status of endodontically treated teeth in relation to the technical quality
of the root filling and the coronal restoration, Int Endod J 28:12-18, 1995.

Efficient and Effective Endodontics
PAGE 41
©2015
REFERENCES
American Association of Endodontists Guide to Clinical Endodontics, Chicago 2004.
Friedman CE, Sandrik JL, Heuer MA, Rapp GW. Composition and physical properties of gutta-percha
endodontic filling materials. J Endod 3:304, 1977.
Friedman CE, Sandrik JL, Heuer MA, Rapp GW. Composition and mechanical properties of gutta-
percha endodontic points. J Dent Res 54:921, 1975.
Goodman A, Schilder H, Aldrich W. The thermomechanical properties of gutta-percha. II. The history
and molecular structure of gutta-percha. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 37:954,
1974.
Moorer WR, Genet JM. Antibacterial activity of gutta-percha cones attributed to the zinc oxide
component. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 53:508, 1982.
Moorer WR, Genet JM. Evidence for antibacterial activity of endodontic gutta-percha cones, Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 53:503, 1982.
Sjögren U, Sundqvist G, Nair PNR. Tissue reaction to gutta-percha particles of various sizes when
implanted subcutaneously in guinea pigs. Eur J Oral Sci 103:313, 1995.
Ørstavik D. Materials used for root canal obturation: technical, biological and clinical testing. Endod
Topics 12:25, 2005.
Al-Khatib ZZ et al. The antimicrobial affect of various endodontic sealers. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 70:784, 1990.
Heling I, Chandler NP. The antimicrobial effect within dentinal tubules of four root canal sealers. J
Endod 22:257, 1996.
Peters LB, Wesselink PR, Moorer WR. The fate and role of bacteria left in root dentinal tubules. Int
Endod J 28:95, 1995.
Gutmann JL. Adaptation of injected thermoplasticized gutta-percha in the absence of the dentinal
smear layer. Int Endod J 26:87, 1993.
Oksan T, Aktener BO, Sen BH, Tezel H. The penetration of root canal sealers into dentinal tubules: a
scanning electron microscopic study. Int Endod J 26:301, 1993.

Efficient and Effective Endodontics
PAGE 42
©2015
REFERENCES
Sen BH, Piskin B, Baran N. The effect of tubular penetration of root canal sealers on dye microleakage.
Int Endod J 29:23, 1996.
Wennberg A, Ørstavik D. Adhesion of root canal sealers to bovine dentine and gutta-percha. Int Endod
J 23:13, 1990.
Lee K-W, et al. Adhesion of endodontic sealers to dentin and gutta-percha. J Endod 28:684, 2002.
ANSI/ADA specification no. 57 for endodontic filling materials. J Am Dent Assoc 108:88, 1984.
Kokkas AB, et al. The influence of the smear layer on dentinal tubule penetration depth by three
different root canal sealers: an in vitro study. J Endod 30:100, 2004.
Eldeniz AU, Erdemir A, Belli S. Shear bond strength of three resin based sealers to dentin with and
without smear layer. J Endod 31:293, 2005.
Cobankara FK, et al. The quantitative evaluation of apical sealing of four endodontic sealers. J Endod
32:66, 2006.
Tagger M et al. Interaction between sealers and gutta-percha cones. J Endod 29:835, 2003.
Facer SR, Walton RE. Intracanal distribution patterns of sealers after lateral condensation. J Endod
29:832, 2003.
Baumgartner G, et al. Enterococcus faecalis type strain leakage through root canals filled with gutta-
percha/AH Plus or Resilon/Epiphany. J Endod 33:45, 2006.
Granche D et al. Endodontic cements induce alterations in the cell cycle of in vitro cultured osteoblasts.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 79:359, 1995.
Langeland K. Root canal sealants and pastes. Dent Clin North Am 18:309, 1974.
Briseno BM, Willerhausen B. Root canal sealer cytotoxicity on human gingival fibroblasts. I. Zinc oxide-
eugenol based sealers, J Endod 16:383, 1990.
Briseno BM, Willerhausen B: Root canal sealer cytotoxicity on human gingival fibroblasts. II. Silicone-
and resin-based sealers, J Endod 17:537, 1991.

Efficient and Effective Endodontics
PAGE 43
©2015
REFERENCES
Briseno BM, Willerhausen B. Root canal sealer cytotoxicity on human gingival fibroblasts. III. Calcium
hydroxide-n-based sealers. J Endod 18:110, 1992.
Brodin P, Røed A, Aars H, Ørstavik D. Neurotoxic effects of root filling materials on rat phrenic nerve in
vitro. J Dent Res 61:1020, 1982.
Holland R, de Souza V. Ability of a new calcium hydroxide root canal filling material to induce hard
tissue formation. J Endod 11:535, 1985.
Sonat B, Dalat D, Günhan O. Periapical tissue reaction to root fillings with Sealapex. Int Endod J 23:46,
1990.
Kontakiotis E, Panopoulos P. pH of root canal sealers containing calcium hydroxide. Int Endod J
29:202, 1996.
Layhausen G, et al. Genotoxicity and cytotoxicity of the epoxy resin-based root canal sealer AH plus. J
Endod 25:109, 1999.
Lai CC, et al. Antimicrobial activity of four root canal sealers against endodontic pathogens. Clin Oral
Investig 5:236, 2001.
Schwarze T, et al. The cellular compatibility of five endodontic sealers during the setting period. J
Endod 28:784, 2002.
Gomes BP et al. In vitro evalution of the antimicrobial activity of five root canal sealers. Braz Dent J
15:30, 2004.
Huang TH, et al. Root canal sealers induce cytotoxicity and necrosis. J Mater Sci Mater Med 15:767,
2004.
Ørstavik D. Materials used for root canal obturation: technical, biological and clinical testing. Endod
Topics 12:25, 2005.
Dahl JE. Toxicity of endodontic filling materials. Endod Topics 12:39, 2005.
Hensten A, Jacobsen N. Allergic reactions in endodontic practice. Endod Topics 12:44, 2005.
Gluskin A. Mishaps and serious complications in endodontic obturation. Endod Topics 12:52, 2005.
Efficient and Effective Endodontics
PAGE 44
©2015
REFERENCES
Budd CS, Weller RN, Kulild JC. A comparison of thermoplasticized injectable gutta-percha obturation
techniques. J Endod 17:260, 1991.
Evans JT, Simon JHS. Evaluation of the apical seal produced by injected thermoplasticized gutta-
percha in the absence of smear layer and root canal sealer. J Endod 12:101, 1986.
Gutmann JL. Adaptation of injected thermoplasticized gutta-percha in the absence of the dentinal
smear layer. Int Endod J 26:87, 1993.
Sjögren U, Sundqvist G, Nair PNR. Tissue reaction to gutta-percha particles of various sizes when
implanted subcutaneously in guinea pigs. Eur J Oral Sci 103:313, 1995.
Barbosa SV, Burkard DH, Spångberg LSW. Cytotoxic effects of gutta-percha solvents. J Endod 20:6,
1994.
Gutmann JL, Heaton JF. Management of the open (immature) apex. II. Non-vital teeth. Int Endod J
14:173, 1981.
Gutmann JL, Dumsha TC, Lovdahl. Problems in root canal obturation. Problem solving in endodontics,
ed 4, St Louis, 2006, Elsevier-Mosby.
Haas SB et al. A comparison of four root canal filling techniques. J Endod 15:596, 1989.
Kaplowitz GJ. Evaluation of gutta-percha solvents. J Endod 16:539, 1990.
Keane K, Harrington GW. The use of a chloroform-softened gutta-percha master cone and its effect on
the apical seal. J Endod 10:57, 1984.
McDonald NM, Vire DE. Chloroform in the endodontic operatory. J Endod 18:301, 1992.
Metzger Z et al. Apical seal by customized versus standardized master cones: a comparative study in
flat and round canals. J Endod 14:381, 1988.
Metzger Z et al. Residual chloroform and plasticity in customized gutta-percha master cones. J Endod
14:546, 1988.
Wong M, Peters DB, Lorton L. Comparison of gutta-percha filling techniques: three chloroform gutta-
percha filling techniques: part 2. J Endod 8:4, 1982.

Efficient and Effective Endodontics
PAGE 45
©2015
REFERENCES
Grove CJ: Why root canals should be filled to the dentinocemental junction, J Am Dent Assoc 17:293,
1930.
Orban B: Why root canals should be filled to the dentinocemental junction, J Am Dent Assoc 17:1086,
1930.
Grahnén H, Hansson L: The prognosis of pulp and root canal therapy: a clinical and radiographic
follow-up examination, Odontol Revy 12:146, 1961.
Seltzer S. Endodontology: biologic considerations in endodontic procedures. ed 2, Philadelphia, 1988,
Lea & Febiger.
Seltzer S, Bender IB, Turkenkopf S. Factors affecting successful repair after root canal therapy. J Am
Dent Assoc 67:651, 1963.
Swartz DB, Skidmore AE, Griffin JA. Twenty years of endodontic success and failure. J Endod 9:198,
1983.
Seltzer S, Naidorf I. Flare-ups in endodontics. II. Therapeutic measures. J Endod 11:559, 1985.
Sjögren U, Hägglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic
treatment. J Endod 16:498, 1990.
Hasselgren G: Where shall the root filling end? NY State Dent J 60(6):34, 1994.
Gutmann JL, Leonard JE: Problem solving in endodontic working length determination, Comp Contin
Educ Dent 16:288, 1995.
Wu M-K, Wesselink PR, Walton RE. Apical terminus location of root canal treatment procedures. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 89:99, 2000.
Whitworth J. Methods of filling root canals: principles and practices. Endod Topics 12:2, 2005.
ProGlider®, PathFile®, ProTaper®, ProMark®, e3®, WaveOne®, GuttaCore®, Thermafil® are trademarks
and/or registered marks of DENTSPLY.
RootZX® is a registered mark of J.Morita.