el largo camino hacia la célula beta artificial...
TRANSCRIPT

I Conget, Consultor Senior
Unidad de Diabetes
Endocrinología y Nutrición
El largo camino hacia la célula beta
Artificial. ¿estamos llegando al final?
Barcelona, 27-28 de Junio de 2014

I Conget
Unidad de Diabetes
Endocrinología y Nutrición
Aclaraciones • No conflicto de intereses con esta charla
• Coordinador del estudio DREAM para España y miembro del Steering
Committee
• Coordinador del estudio TIDE para España y miembro del Steering
Committee
• Coordinador del estudio REWIND para España y miembro del Steering
Committee
• Consultor nacional resultados ADOPT & RECORD
• EDAB Novartis, Vildagliptina
• MEDTRONIC European Advisory Board
• Consultor médico Sitagliptina en España (Merck)
• Miembro del Steering Committee estudio SWITCH
• Miembro del Steering Committee estudio OpT2mise
• Honorarios por charlas patrocinadas por industria farmacéutica (Bayer,
GSK, Lilly, MSD, Novartis, BMS, Pfizer, Gilead, Medtronic-Minimed, Esteve,
NovoNordisk...)


Open- and Closed-Loop
Concepts
5
6
7
8
9
0 2 4 6 8 10 12 14 16 18 20 22 24 0.9
HbA1c < 6.5%
1.4
Continuous
Glucose Monitoring
/ SMBG
Control
Algorithm
Insulin
Delivery
Patient
Rules
Open-Loop Closed-Loop
mmol/l g/l
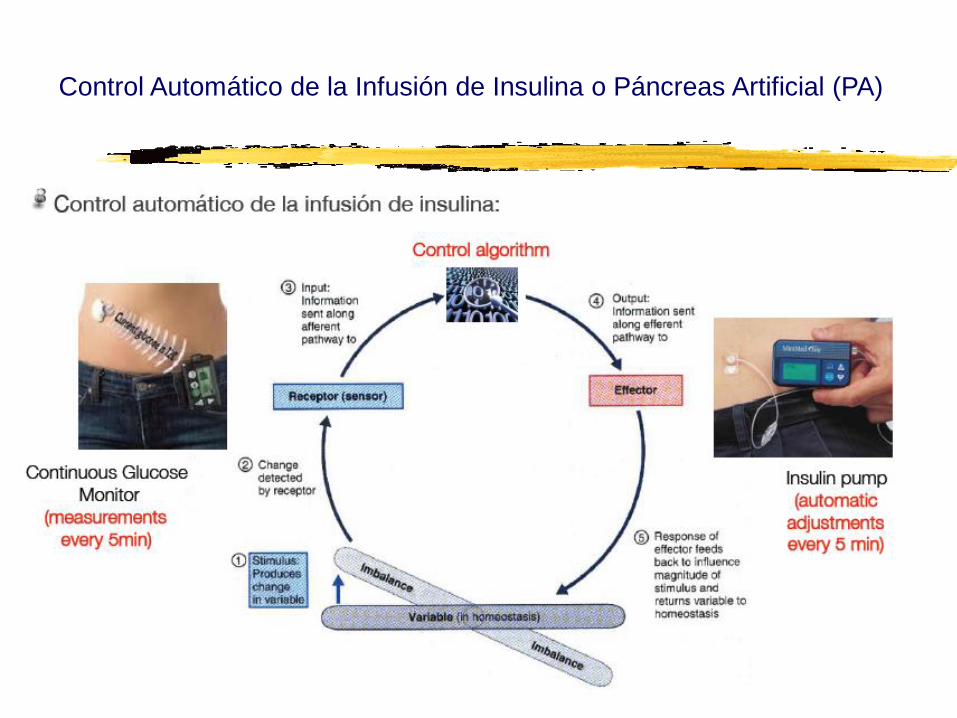
Control Automático de la Infusión de Insulina o Páncreas Artificial (PA)
Introducción




Páncreas Artificial (PA)
= =
Cedido por J Bondía

Limitaciones MCG
Medición de glucosa en el intersticio
Retraso respecto al valor de glucemia real
Diferencias ↑↑ cuando la tasa de cambio es rápida
Necesidad de calibración del sistema (Cuanto mas preciso y exacto el GM, mejor!)
Introducción

Breakthrough Technology – Sensor Innovation
Slide 11
Change sensor accuracy, reliability, consistency and comfort on
the path to the Virtual Pancreas.
Sof-Sensor
Enlite
New Generation
Enlite
Today
Integrated
Sensor & Set
Convenience
Next Generation chemistry
accuracy & consistency
Redundant sensing
Combined electrochemical and Optical sensing
Auto-diagnostic
Improved reliability
Tomorrow - the future’s ! Yesterday

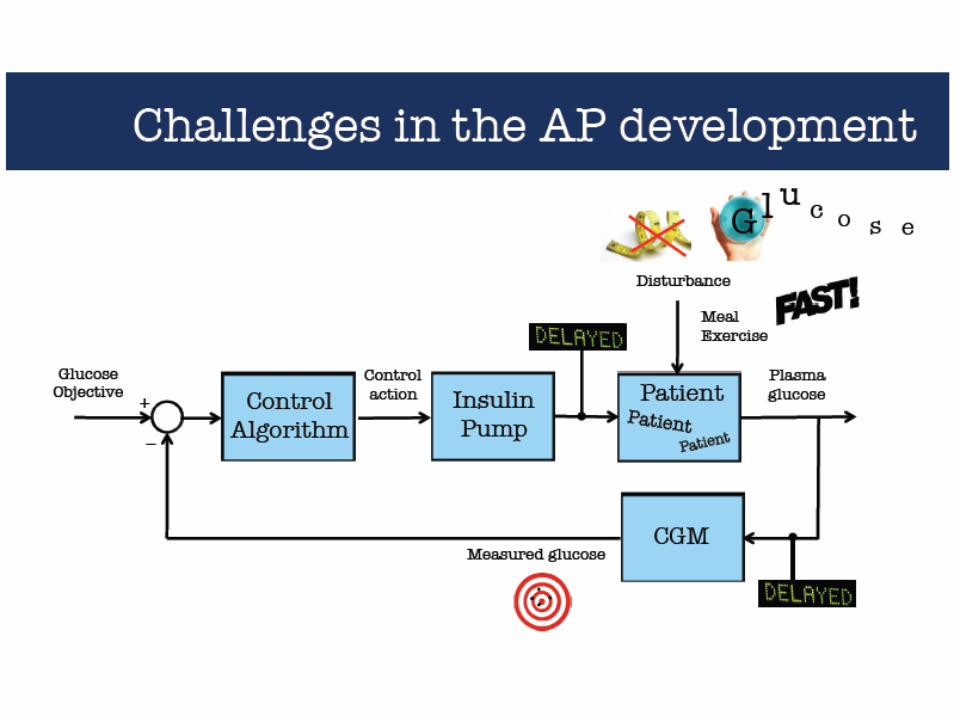
Limitations due to insulin PK and profile !

Artificial pancreas (AP)
Cobelli et al. Diabetes 2011



Eventos clave en el desarrollo del PA
Años 70
• Varios grupos desarrollaron los primeros modelos de PA con control endovenoso
1977 • Primer dispositivo comercializado: Biostator
1979
• Se demuestra que la vía subcutánea es factible para la administración de insulina
Finales 90
• Inicio de la utilización de monitorización continua de glucosa

Steil et al, Diabetes 2006
Eventos clave en el desarrollo del PA
2006
• Primera evidencia de que el PA es factible para la administración de insulina
2006 • JDRF crea el AP Consortium
2008
• Aprobación por la FDA del simulador de Virginia-Padova en sustitución de ensayos con animales
2009
• Diseño de una plataforma que permite la transferencia automática de datos entre CGM, algoritmo de control e ISCI.
Inicio de múltiples estudios multicéntricos en EUA y en Europa

Our own experience……………………….
• LGS set between 50-70 mg/dL
• LGS event everyday or every other
• >50% turn on insulin in <5 minutes
• 2/3 of LGS events during the day
• LGS events lasting 2 hours
• Mainly at night
• 10% of all LGS events
• Decrease in some hypos
• No increase in hyperglycemia

Bergenstal RM for the Aspire in-Home Study Group. NEJM 2013
Automation to Simulate Pancreatic Insulin Response (ASPIRE) In-Home Study
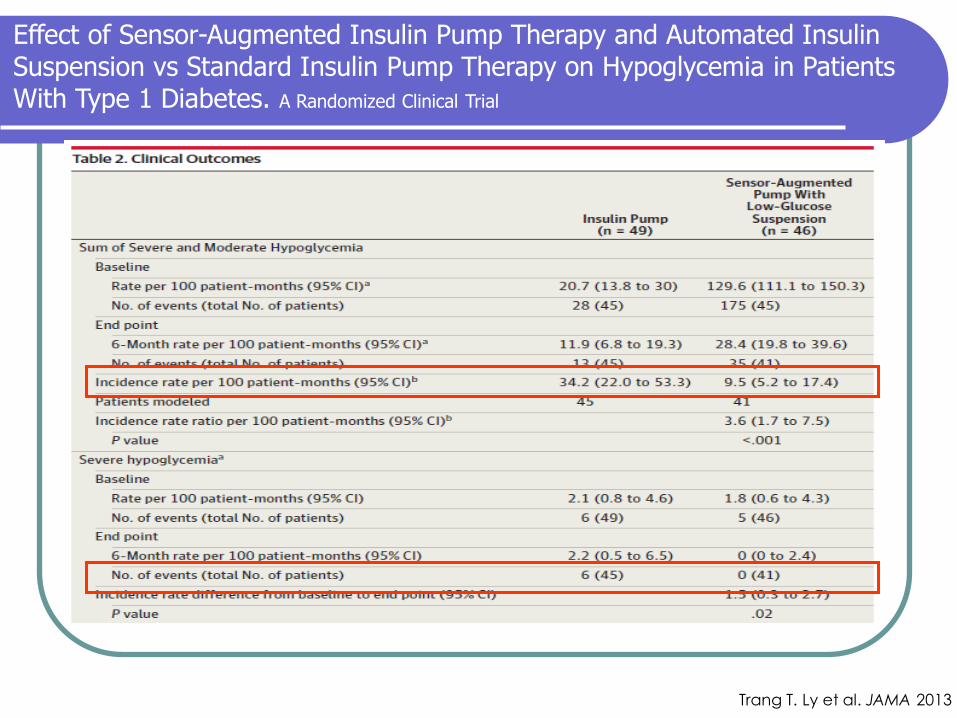
Trang T. Ly et al. JAMA 2013
Effect of Sensor-Augmented Insulin Pump Therapy and Automated Insulin Suspension vs Standard Insulin Pump Therapy on Hypoglycemia in Patients With Type 1 Diabetes. A Randomized Clinical Trial


23
Suspend by Sensor: Suspend before Low
00:00 01:00 02:00
200
180
140
100
60
0
70 above Low Limit
20 above Low Limit
0 30 60 90 120
Low Limit
Suspends basal insulin because SG:
• is at or within 70 mg/dL above the Low Limit
• AND estimated to be at or within 20 mg/dL above the Low Limit within 30 min
Se
ns
or
Glu
co
se
Va
lue
minutes

24
Suspend by Sensor: Auto-resume based on SG
00:00 01:00 02:00
11.0
10.0
7.8
5.6
3.4
0
20 above Low Limit
0 30 60 90 120
Low Limit
Resumes basal delivery because:
• SG is at least 20 mg/dL above Low Limit
• AND estimated to be more than 40 mg/dL above the Low Limit within 30 min
• AND insulin has been suspended for at least 30 min
40 above Low Limit
Se
ns
or
Glu
co
se
Va
lue
minutes


Mayo 2014 “Artificial pancreas systems will be the most revolutionary advance in diabetes care since the discovery of insulin,” said Aaron Kowalski, PhD, a vice president at the Juvenile Diabetes Research Foundation (JDRF),
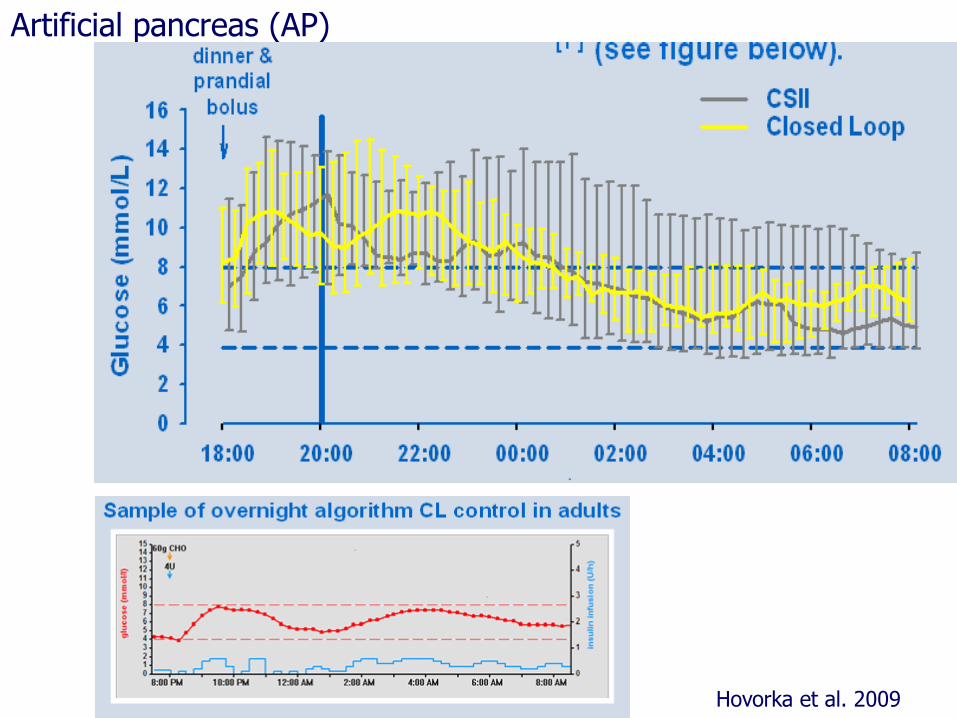
Artificial pancreas (AP)
Hovorka et al. 2009

Artificial Pancreas Using a Personalized Rule-Based Controller Achieves Overnight Normoglycemia in Patients with Type 1 Diabetes Capel et al. DT&T 2014
Randomized crossover 10 T1DM patients treated CSII spent two nonconsecutive nights in the research facility: one with their usual CSII pattern (open-loop [OL]) and one controlled by the pRBA (CL). The CL period lasted from 10 p.m. to 10 a.m., including overnight control, and control of breakfast.
instant value of glucose predicted rate of change nominal basal insulin

Correcto control nocturno
pero…
dificultades en el control postprandial
Búsqueda de alternativas

· 20 pacientes adultos · Bolus preprandial, 30 min de ejercicio
· 2 sistemas modulares basados en algoritmos MPC: sCTR y eCTR.
sCTR mejor que OL en: % de tiempo 70-180% Variabilidad intra-sujeto Num de hipoglicemias
eCTR mejor que OL en:
% de tiempo 70-180% % de tiempo: 80-140% nocturno Variabilidad intra-sujeto Glucosa media
Breton et al, Diabetes 2012
Introducción

El-Kathib et al, Sci Transl Med, 2010
· 11 pacientes adultos
· Algoritmo MPC, sin bolus preprandial
· Sistema bihormonal
Glucagón capaz de evitar hipos sólo si la
sobreinsulinización no es excesiva

Hovorka et al.2011
Elleri et al. DT&T 2011
Close-loop nowadays and future
Although SAP seems to be able to lower A1c, it
requires non-stop active commitment of the patient
and caregivers.
CL therapy differs essentially from the available
treatment strategies because it aims at less rather
than more patient self-management.
CL Studies are limited to controlled or supervised
conditions and performed with systems that consist of
a combination of separate devices
First studies performed outside the clinical research
center are being reported

O’Grady et al..Diabetes Care 2012
The Use of an Automated, Portable, Glucose Control System for Overnight
Glucose Control in Adolescents and Young AdultsWith Type 1 Diabetes

O’Grady et al..Diabetes Care 2012
The Use of an Automated, Portable, Glucose Control System for Overnight
Glucose Control in Adolescents and Young AdultsWith Type 1 Diabetes

O’Grady et al..Diabetes Care 2012
The Use of an Automated, Portable, Glucose Control System for Overnight
Glucose Control in Adolescents and Young AdultsWith Type 1 Diabetes

Sistema de comunicación funcionante durante el 97,7% del tiempo
Kovatchev et al, Diabetes Care 2013

· 56 adolescentes en campamentos
· Diseño cruzado
· CL vs SAP
· Control nocturno sin comidas
· Controlador MD-Logic
Menor número de hipos, glicemia media más baja. Phillip et al, NEJM 2013

June 2013

June 2013

June 2013

Close-loop nowadays and future (ii)
Next step will be the transition to free-living conditions.
With or without announcements: meals, exercise…
CL prototypes developed for research have to evolve into “friendly” devices suitable for day-to-day clinical (realiable, portable…Fully-automated portable)
The final goal of “perfect” control-to-target may be preceded by nocturnal CL or control-to-range systems where the risk of adverse events is less.
Only well-established diabetes device companies are likely to afford this relatively long road and can guarantee market access. Collaboration is crucial!
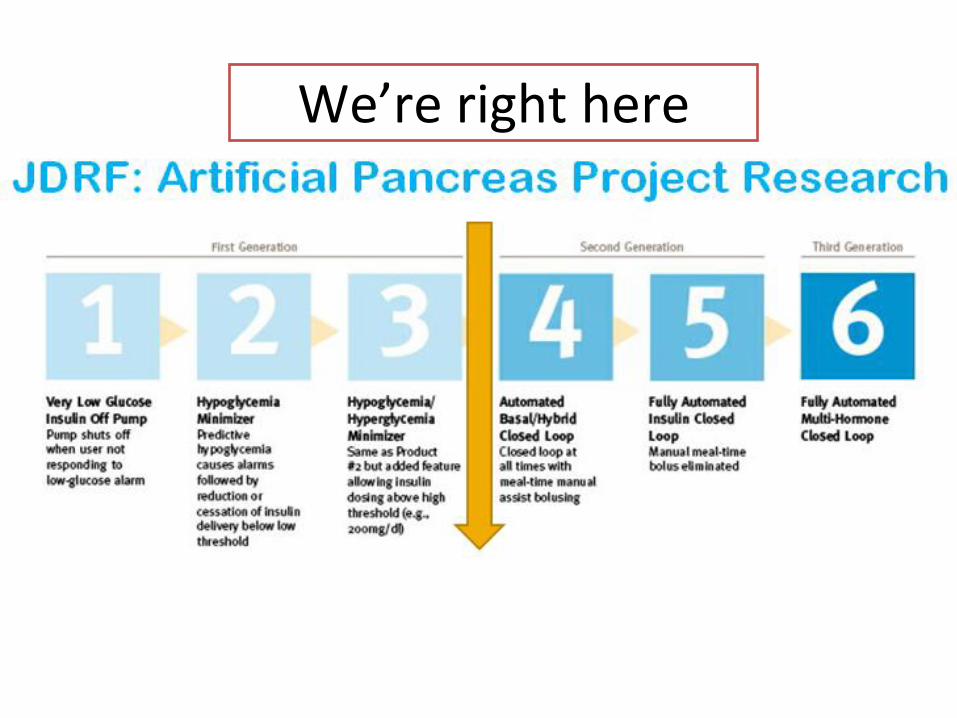
We’re right here

closedloop4meal.org


Mayo 2014. CL4M presntación a pacientes

Close-loop nowadays and future
The End
Until CL arrival, let’s do as much as we can (right now) for our patients avoiding therapeutic inertia !
Gracias


MPC
Introducción

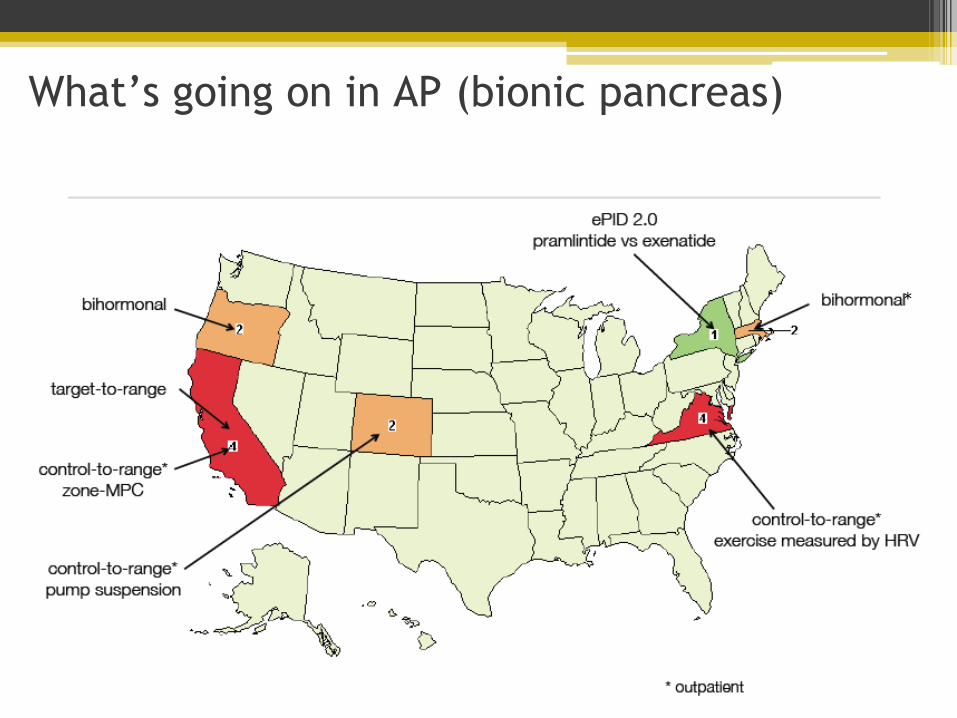
What’s going on in AP (bionic pancreas)
*

What’s going on in AP (bionic pancreas)