Élie azoulay hôpital saint-louis, service de … · Élie azoulay hôpital saint-louis, service...
TRANSCRIPT
Élie AZOULAY
Hôpital Saint-Louis, Service de Réanimation Médicale
Université Paris-Diderot, Sorbonne Paris-Cité Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH)

Thank you for the invitation

Global Data
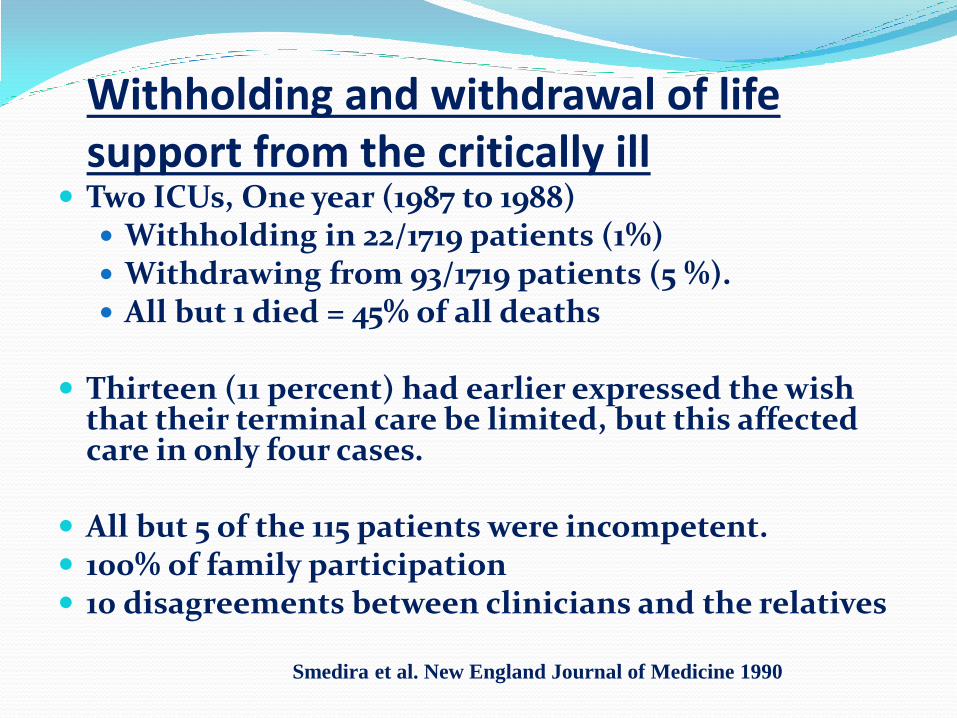
Withholding and withdrawal of life support from the critically ill
Two ICUs, One year (1987 to 1988) Withholding in 22/1719 patients (1%) Withdrawing from 93/1719 patients (5 %). All but 1 died = 45% of all deaths
Thirteen (11 percent) had earlier expressed the wish
that their terminal care be limited, but this affected care in only four cases.
All but 5 of the 115 patients were incompetent. 100% of family participation 10 disagreements between clinicians and the relatives
Smedira et al. New England Journal of Medicine 1990
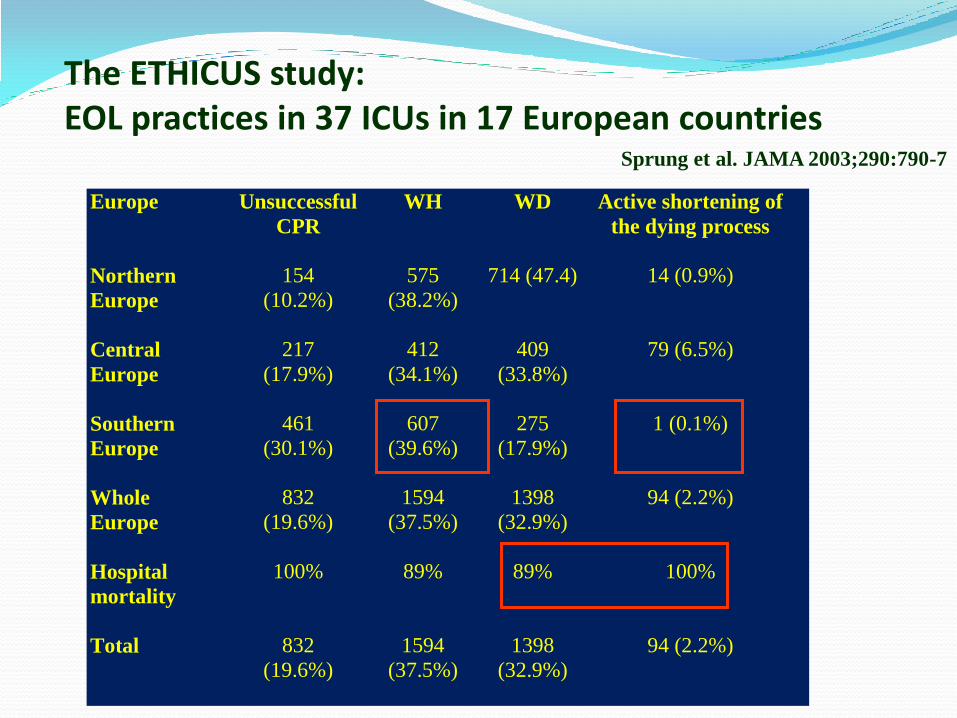
Europe Unsuccessful
CPR
WH WD Active shortening of
the dying process
Northern
Europe
154
(10.2%)
575
(38.2%)
714 (47.4) 14 (0.9%)
Central
Europe
217
(17.9%)
412
(34.1%)
409
(33.8%)
79 (6.5%)
Southern
Europe
461
(30.1%)
607
(39.6%)
275
(17.9%)
1 (0.1%)
Whole
Europe
832
(19.6%)
1594
(37.5%)
1398
(32.9%)
94 (2.2%)
Hospital
mortality
100% 89% 89% 100%
Total
832
(19.6%)
1594
(37.5%)
1398
(32.9%)
94 (2.2%)
The ETHICUS study: EOL practices in 37 ICUs in 17 European countries
Sprung et al. JAMA 2003;290:790-7
Significant differences across countries regarding: Proportion of EOLD in dying patients Time from admission to EOLD Time from EOLD to discharge or death
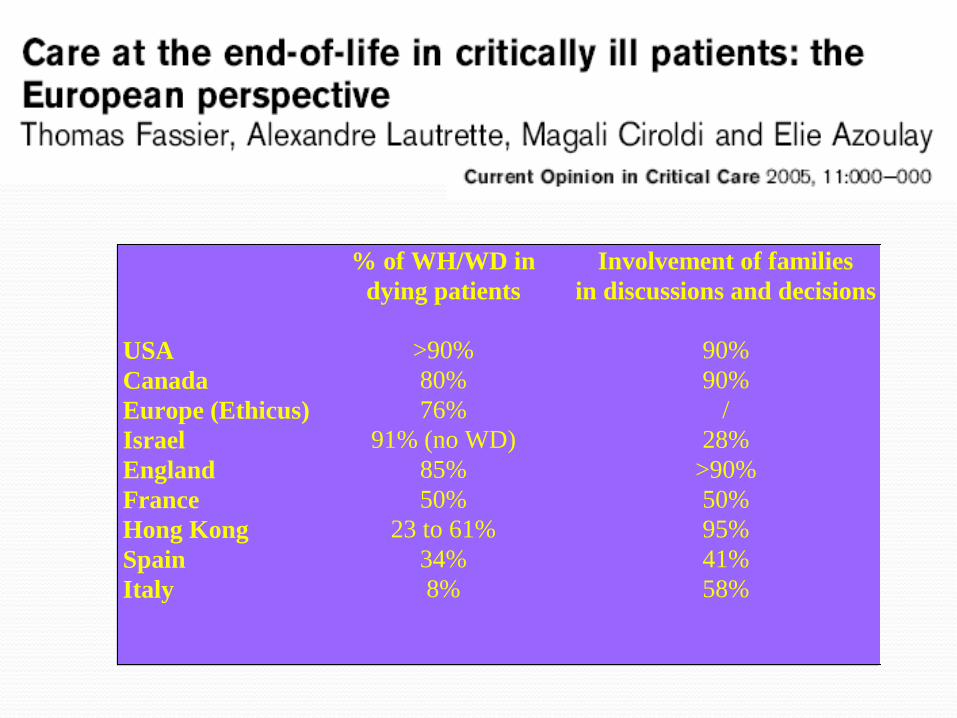
% of WH/WD in
dying patients
Involvement of families
in discussions and decisions
USA >90% 90%
Canada 80% 90%
Europe (Ethicus) 76% /
Israel 91% (no WD) 28%
England 85% >90%
France 50% 50%
Hong Kong 23 to 61% 95%
Spain 34% 41%
Italy 8% 58%
Detailed Data
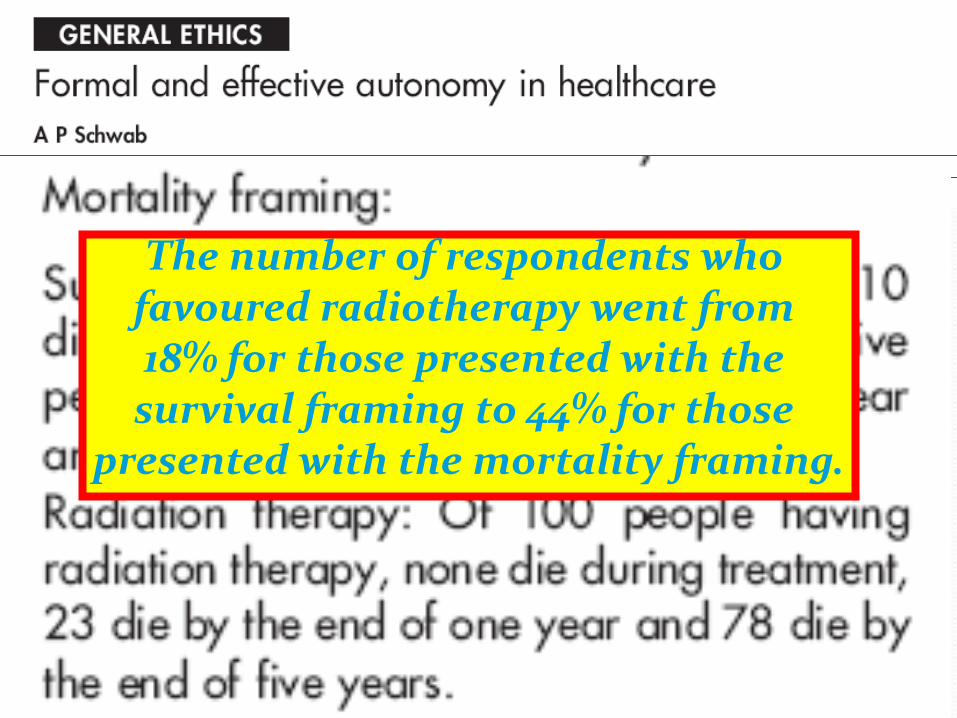
The number of respondents who favoured radiotherapy went from 18% for those presented with the survival framing to 44% for those
presented with the mortality framing.
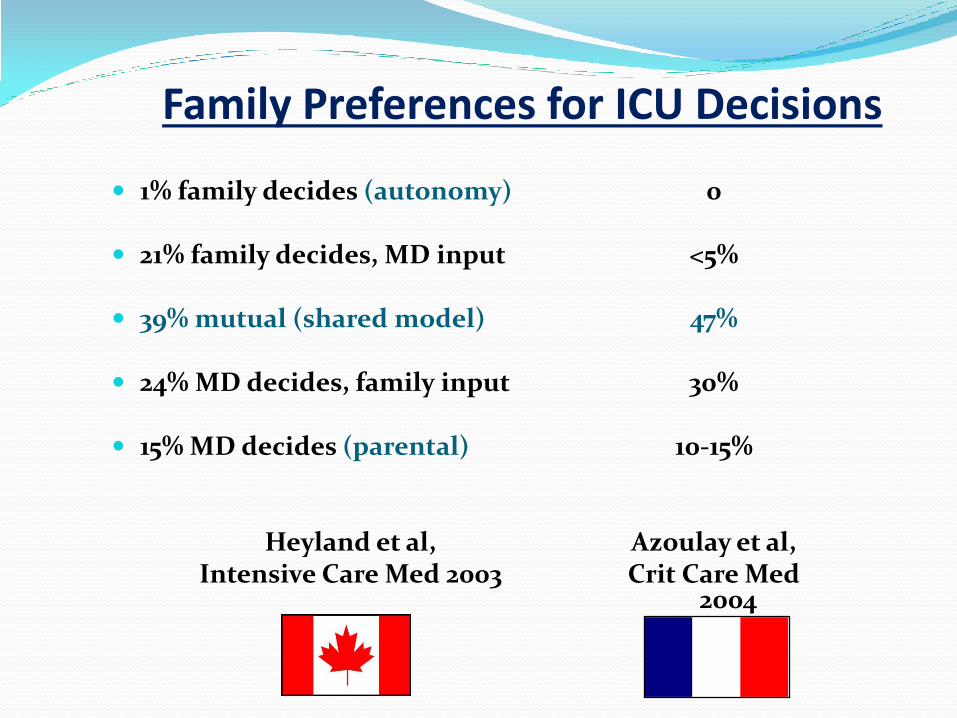
Family Preferences for ICU Decisions
1% family decides (autonomy)
21% family decides, MD input
39% mutual (shared model)
24% MD decides, family input
15% MD decides (parental)
Heyland et al, Intensive Care Med 2003
0
<5%
47%
30%
10-15%
Azoulay et al, Crit Care Med
2004
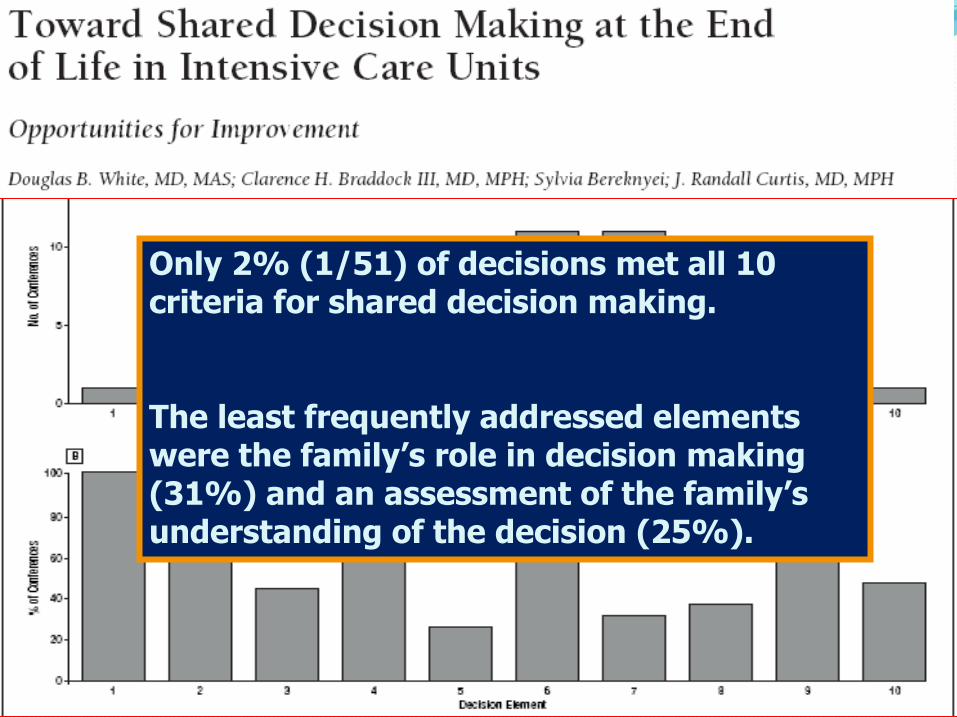
Only 2% (1/51) of decisions met all 10 criteria for shared decision making. The least frequently addressed elements were the family’s role in decision making (31%) and an assessment of the family’s understanding of the decision (25%).
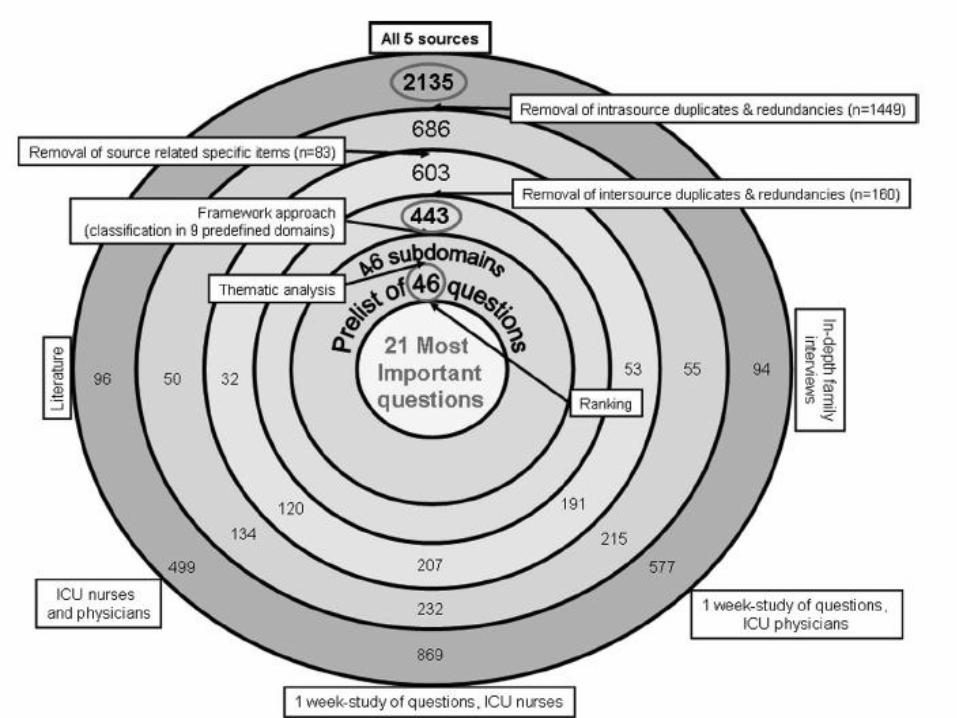
Countries/Regions
ICUs
¨Patients/ Relatives
Clinicians
Context
I am convinced that the variability in the decision-making process is somewhere else
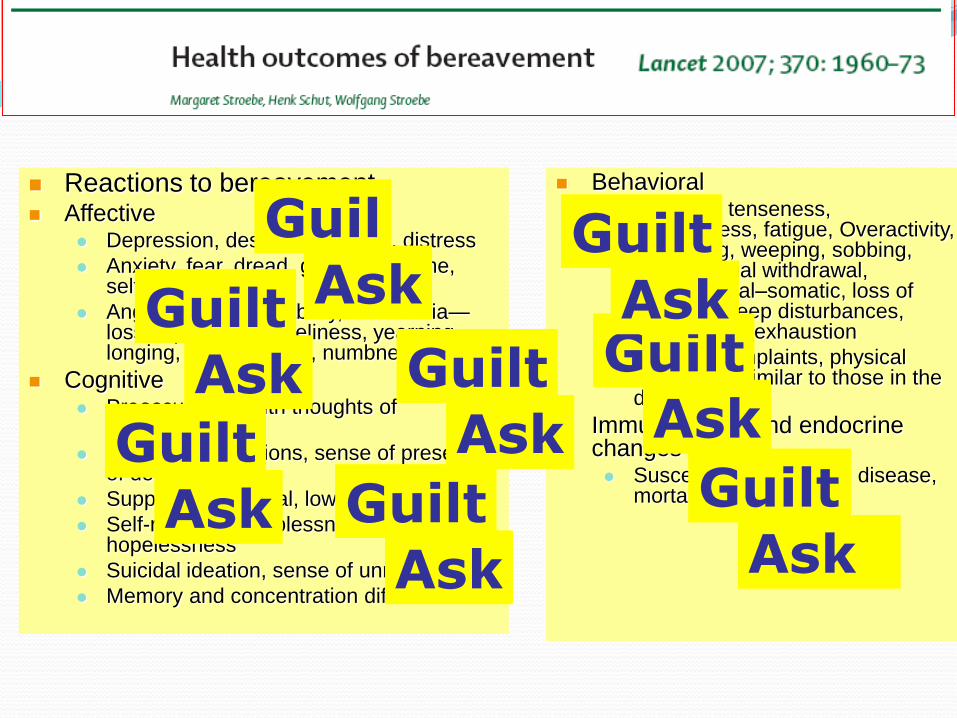
Reactions to bereavement Affective
Depression, despair, dejection, distress
Anxiety, fear, dread, guilt, self-blame, self-accusation
Anger, hostility, irritability, anhedonia—loss of pleasure, loneliness, yearning, longing, pining, shock, numbness
Cognitive Preoccupation with thoughts of
deceased,
Intrusive ruminations, sense of presence of deceased
Suppression, denial, lowered self-esteem
Self-reproach, helplessness, hopelessness
Suicidal ideation, sense of unreality
Memory and concentration difficulties
Behavioral Agitation, tenseness,
restlessness, fatigue, Overactivity, Searching, weeping, sobbing, crying, social withdrawal, physiological–somatic, loss of appetite, sleep disturbances, energy loss, exhaustion
Somatic complaints, physical complaints similar to those in the deceased
Immunological and endocrine changes Susceptibility to illness, disease,
mortality
Guil
GuiltGuilt
Guilt
GuiltGuiltGuilt
Guilt
Guil
GuiltGuilt
Guilt
GuiltGuiltGuilt
Guilt
Ask
AskAsk
Ask
AskAskAsk
Ask
Ask
AskAsk
Ask
AskAskAsk
Ask

Interventions
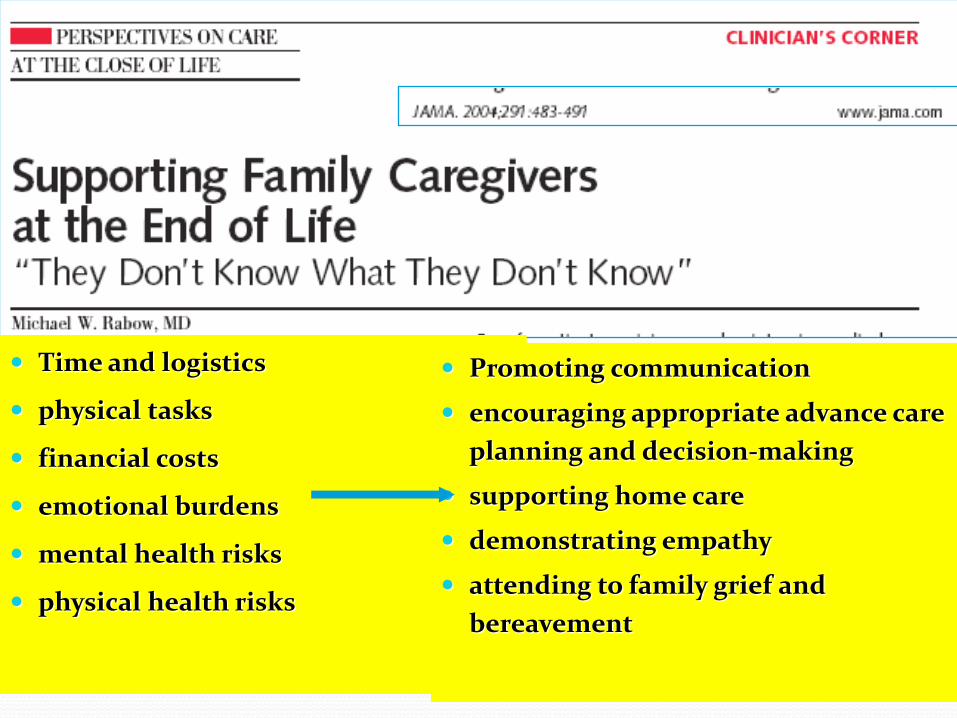
Time and logistics
physical tasks
financial costs
emotional burdens
mental health risks
physical health risks
Promoting communication
encouraging appropriate advance care
planning and decision-making
supporting home care
demonstrating empathy
attending to family grief and
bereavement
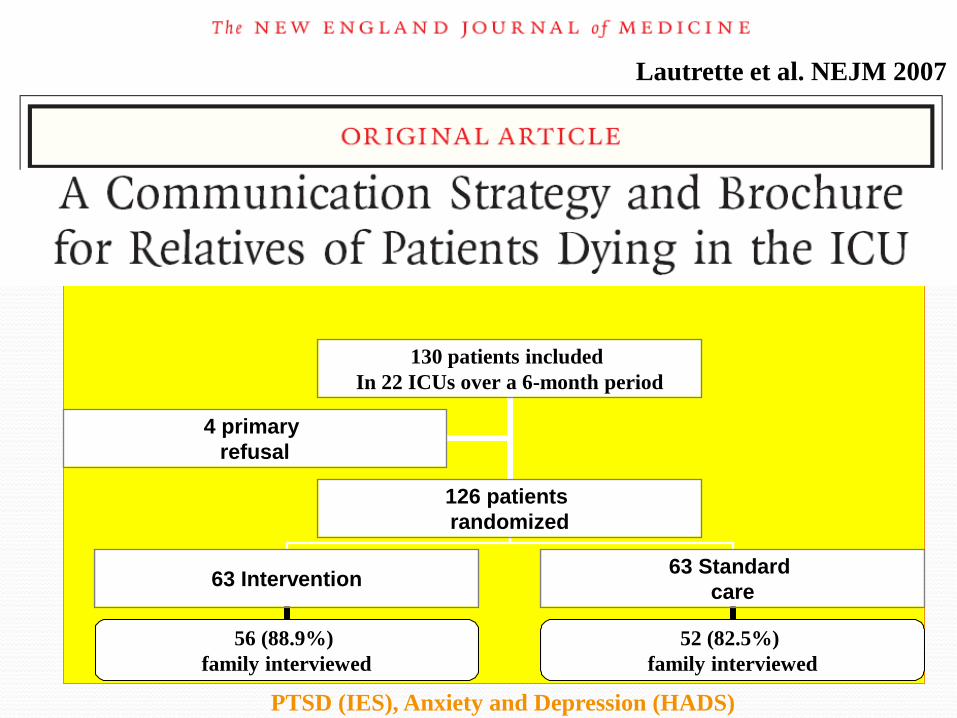
PTSD (IES), Anxiety and Depression (HADS)
130 patients included
In 22 ICUs over a 6-month period
4 primary
refusal
126 patients
randomized
63 Intervention 63 Standard
care
56 (88.9%)
family interviewed
52 (82.5%)
family interviewed
Lautrette et al. NEJM 2007
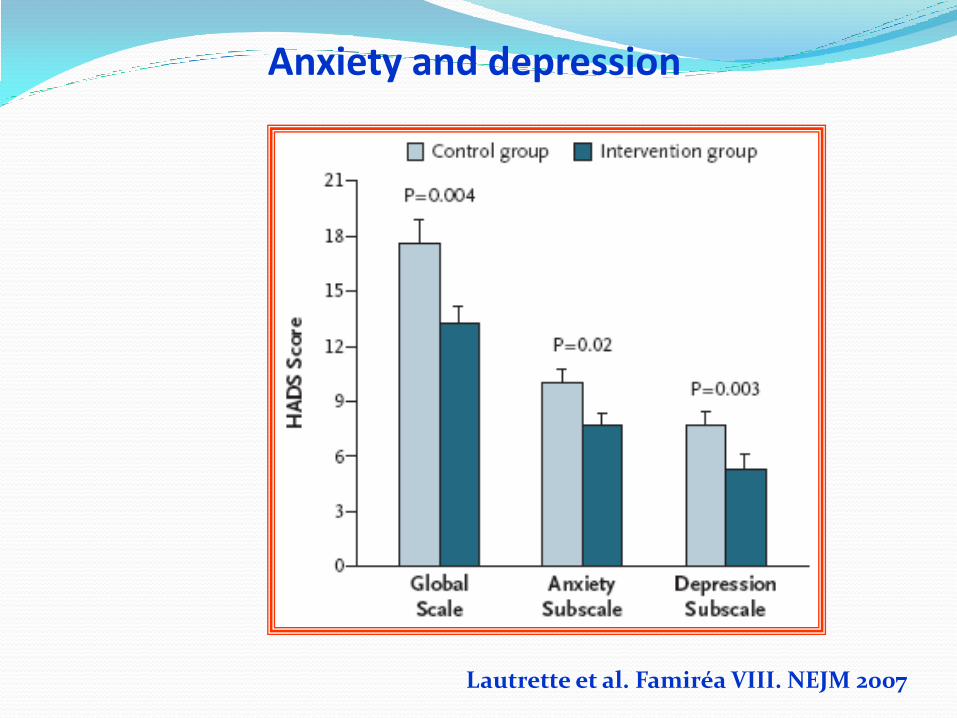
Anxiety and depression
Lautrette et al. Famiréa VIII. NEJM 2007
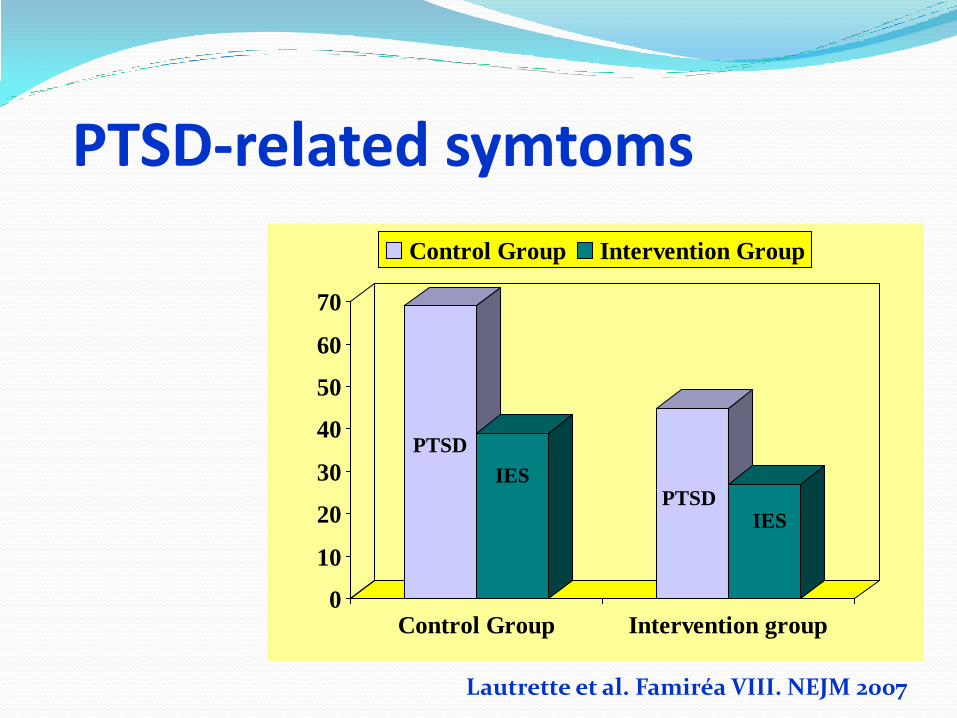
PTSD-related symtoms
0
10
20
30
40
50
60
70
Control Group Intervention group
Control Group Intervention Group
IES
IES
PTSD
PTSD
Lautrette et al. Famiréa VIII. NEJM 2007
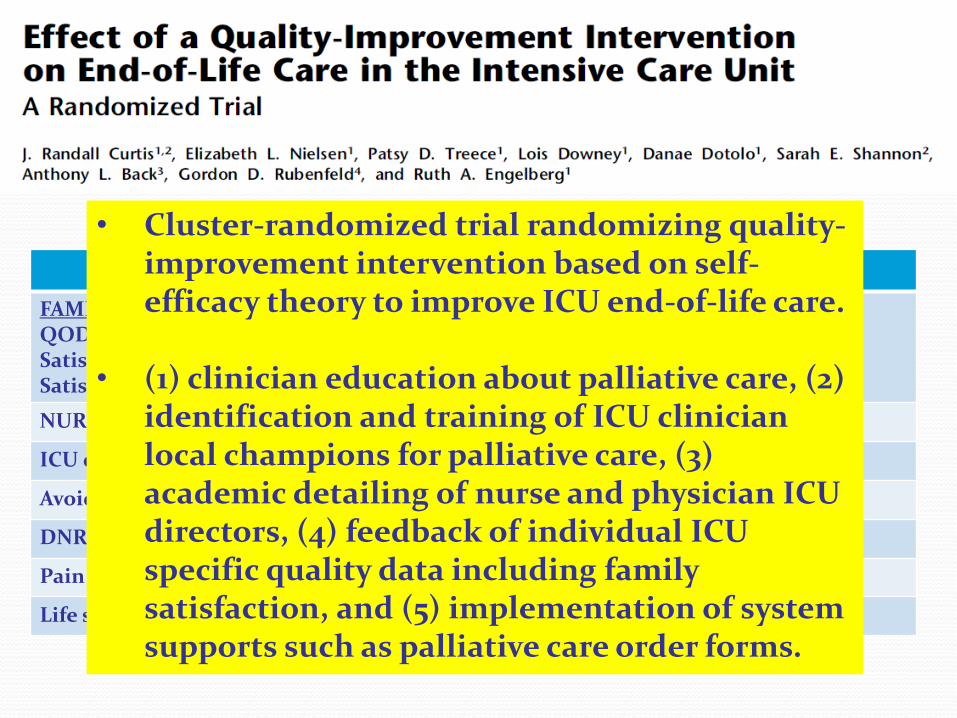
Intervention Control P Value
FAMILY QODD Satisfaction with care Satisfaction with DM
61.8 (23.9) 75% 72.4%
59.9 (21.9) 76.3% 75.7%
0.33 0.63 0.54
NURSE QODD 69 69 0.81
ICU days to ventilator withdrawal 5 7.5 0.81
Avoided CPR in last hour of life 87.1% 89.4%
DNR orders at death 82.7% 82.1% 0.68
Pain assesment 79.2% 77.2% 0.81
Life support withheld or withdrawn 72.3% 68.7% 0.10
• Cluster-randomized trial randomizing quality-improvement intervention based on self-efficacy theory to improve ICU end-of-life care.
• (1) clinician education about palliative care, (2) identification and training of ICU clinician local champions for palliative care, (3) academic detailing of nurse and physician ICU directors, (4) feedback of individual ICU specific quality data including family satisfaction, and (5) implementation of system supports such as palliative care order forms.
Thinking differently

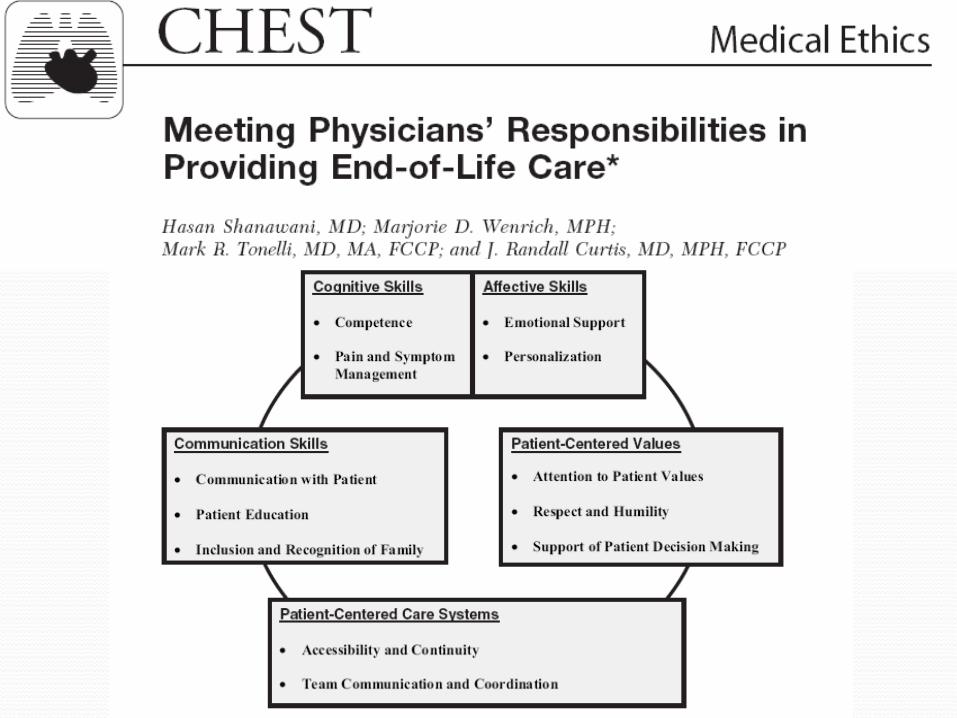
Definition of high-quality ICU palliative care Communication by clinicians
Patient-focused medical decision-making:
Clinical care : dignity, treating the patient as a person
Protecting privacy
Care of the family: Providing access, proximity, and support
Answering to “What do you think the patient would choose?” is emotionally, cognitively, and morally complex.
We should stop distributing patient’s values expertise to surrogates and technical/medical expertise to physicians.
Many surrogates need assistance in identifying and working through the sometimes conflicting values relevant to medical decisions near the end of life.
Framework for clinicians to help surrogates overcome the
emotional, cognitive, and moral barriers to high-quality
surrogate decision making for incapacitated patients.
Open the
ICU Doors
You have Nothing To Hide
You can be Proud of how you Care

Happy hours for ICU relatives (Famirea)
We’ve
changed
happy hours to
an « Interlude
for reflection »

Thank you for your Attention