ellen kantor, srna university of pennsylvania n746- summer 2013 pulmonary hypertension
TRANSCRIPT

Ellen Kantor, SRNAUniversity of Pennsylvania
N746- Summer 2013
Pulmonary Hypertension

Let’s Review…From RVpulmonic (semilunar
valve)pulmonary arteryFrom pulmonary veinLALVsystemic
circulationPulmonary vessels
innervated by sympathetic nervous system
Alpha adrenergic- norepinephrine causes vasoconstriction
Beta adrenergic- such as isoproterenol causes vasodilation
Regulation of flow is mostly passive and controlled by OXYGEN.

Pulmonary Hypertension: Statistics
Average age at diagnosis: 36 years Women > Men10-15 million people/million diagnosed each year3 year survival at time of diagnosis: approximately
50%
Pulmonary HypertensionNORMAL PRESSURES:
Systolic: 15-30 mmHgDiastolic: 5-15 mmHgMean: 10-20 mmHg
HYPERTENSION:Defined as a sustained pulmonary artery
pressure of 40/20 mmHg and a mean pulmonary artery pressure of 25 mmHg.

Pulmonary HypertensionWorld Health Organization (WHO) classifies
into 5 groupsI: idiopathic/primary pulmonary arterial hypertension
II: pulmonary venous hypertension
III: lung disease or hypoxemia
IV: chronic thromboembolic disease
V: miscellaneous pulmonary vasculature diseases
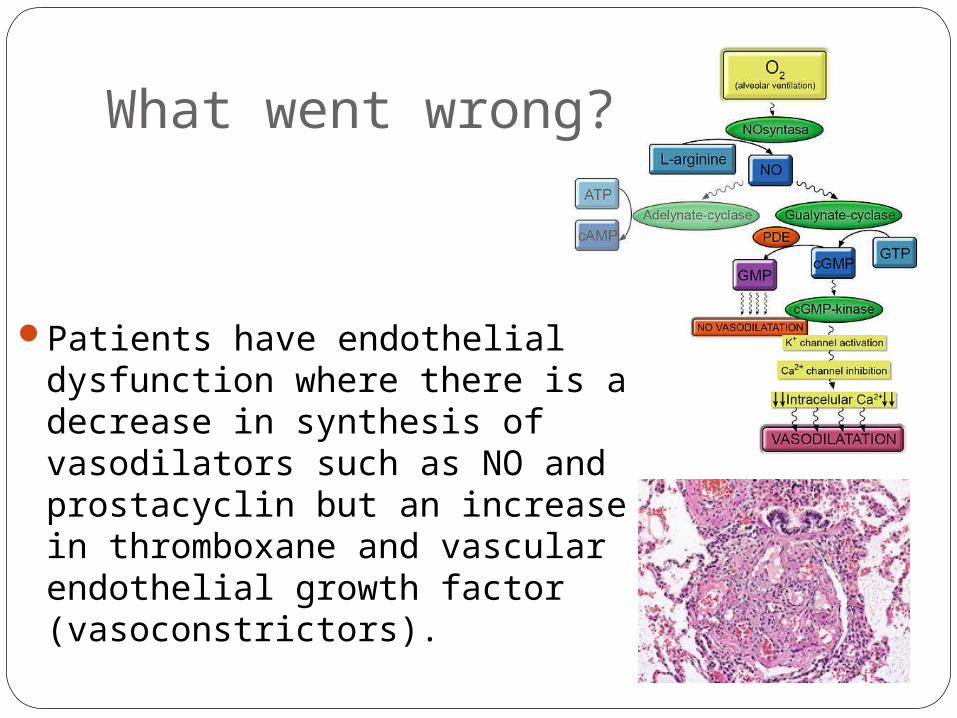
What went wrong?
Patients have endothelial dysfunction where there is a decrease in synthesis of vasodilators such as NO and prostacyclin but an increase in thromboxane and vascular endothelial growth factor (vasoconstrictors).

Side note…Inhaled NO increased systemic O2 in
hypoxemic newborns with pulmonary hypertension.
Decreased need for ECMO
Presenting Signs and SymptomsSymptoms are usually nonspecific
DyspneaAnginaNonproductive coughClubbing
Ring a bell??
Rarely, patients present with syncope and hemoptysis, indicating severe disease.

Signs and Symptoms
While providers are struggling to diagnose a cause of the patient’s nonspecific symptoms, patients can experience acute decompensation from hypoxia, hypercarbia, vasocontrictors, increased sympathetic tone (ANXIETY), and increased pulmonary vascular resistance (PVR) all leading to right heart failure.

Systemic effects• Any abrupt
increase in PVR can lead to right heart failure or desaturation, further leading to decreased blood flow and oxygenation of the left heart, causing decreased cardiac output and ischemia.

Treatment OptionsSupplemental O2 at homeMedication management: diuretics,
anticoagulants, calcium channel blockers, phosphodiesterase inhibitors, prostanoids, endothelin receptor antagonists
Surgical managementLung transplantHeart/lung transplantPulmonary Thromboendarterectomy

Preoperative Management2D ECHO: gold standardEKGX RAYLabs: CBC, CMP (include LFTs)Spirometry (PFTs)Conduct an extensive ROS to identify
moderate-severe disease.Consider pre-operative Iloprost inhalation
***CONTINUE ALL MEDICATIONS ON DAY OF SURGERY
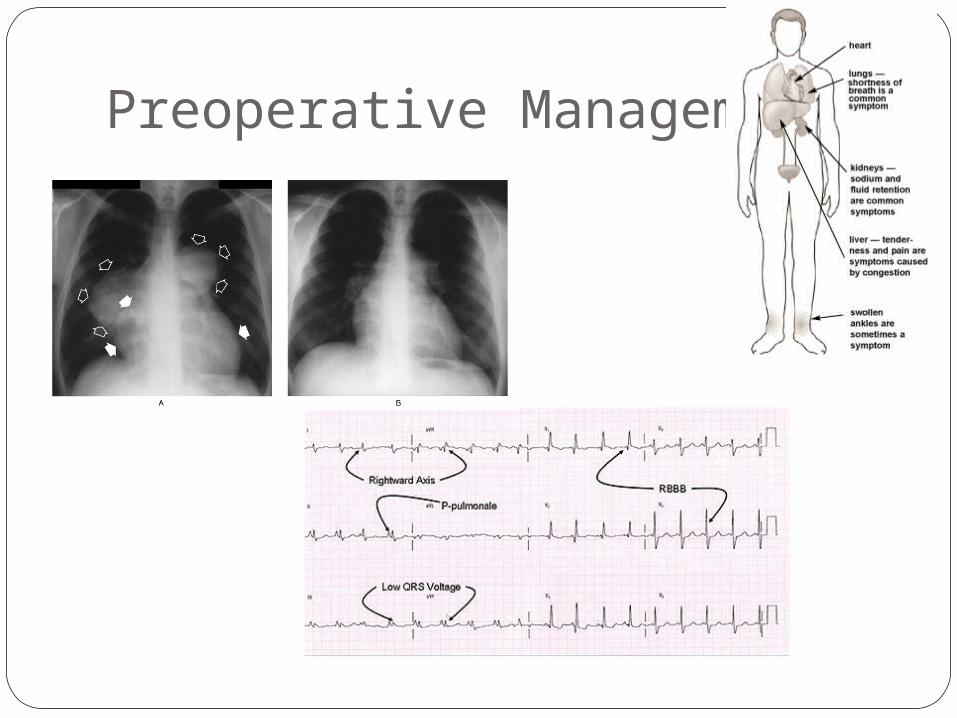
Preoperative Management
Intraoperative Management***CONTINUE ALL MEDICATIONS ON DAY OF SURGERYConsider regional anesthesia, MACConsider fiberoptic intubationStandard ASA monitors +/- ABG, a-line, central line,
foley***Any airway manipulation can cause activation of
sympathetic nervous system and cause a pulmonary hypertensive crisis.
MOST IMPORTANTLY: avoid pulmonary hypertensive crisis (hypoxemia, hypercarbia, metabolic acidosis, hypothermia, airway manipulation)
Postoperative ManagementInterdisciplinary challenge
Intermittent iloprost inhalationLong half life
Continuous monitoring- O2 sats, pain, vital signsConsider continous regional analgesia to
avoid high opioid doses
Case Report #1

Case Report #2

Case Report #3

References Elkassabany NM. Should we delay surgery in the aptient with recent cocaine use? In: Fleisher
LA, ed. Evidence-Based Practice of Anesthesiology. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2013.
Gandhimathi K, Atkinson S, Gibson FM. Pulmonary hypertension complicating twin pregnancy: continuous spinal anaesthesia for caesarean section. International Journal of Obstetric Anesthesia: 2002: 11: 301-305.
Gille J, Seyfarth H, Gerlach S, et al. (2012). Perioperative anesthesiological management of patients with pulmonary hypertension. Anesthesiology Research and Practice: 2012: 1-16.
Kaw R, Pasupuleti V, Deshpande A, et al. Pulmonary hypertension: an important predictor of outcomes in patients undergoing non-cardiac surgery. Respiratory Medicine: 2011: 105: 619-624.
Maxwell B, Pearl R, Kudelko K, et al. Airway management and perioperative decision making in the patient with severe pulmonary hypertension who requires emergency noncardiac surgery. Journal of Cardiothoracic and Vascular Anesthesia: 2012: 26(5): 940-944.
Roizen MF, Fleisher, LA. Anesthetic Implications of Concurrent Diseases. In: Miller RD, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Young WL, eds. Miller’s Anesthesia. 7 th ed. Philadelphia, PA: Churchill Livingstone; 2010: 1020-1021.
Shinohara H, Hirota K, Sato M, et al. (2010). Monitored anesthesia care with dexmedetomidine of a patient with severe pulmonary arterial hypertension for inguinal hernioplasty. J Anesth: 24: 611-613.
Stoelting RL. The Lungs. In: Stoelting RK, Hiller SC, eds. Pharmacology and Physiology in Anesthetic Practice. 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2006.
Strumpher J, Jacobsohn E. Pulmonary hypertension and right ventricular dysfunction: physiology and perioperative management. Journal of Cardiothoracic and Vascular Anesthesia: 2011: 25(4): 687-704.