emergency treatment module 2 - session 6 postabortion complications and management
TRANSCRIPT

Emergency Treatment
Module 2 - Session 6Postabortion Complications
and Management
Module 2 - Session 6Objectives
At the end of this session, participants will be able to:
1. Describe possible complications and their signs/symptoms
2. Describe initial treatment and other measures for:
a. Shock
b. Severe vaginal bleeding
c. Infection and sepsis
d. Intra-abdominal injury
e. Uterine perforation
3. Explain elements of emergency resuscitation/preparation for referral and transport to tertiary care hospital
2
Common Postabortion Complications
• Regardless of the type of abortion, complications can develop at any time, even before the woman seeks care.
• If prompt actions are not taken, they can become life-threatening within minutes.
• When a woman presents for care, the provider must be able to both recognize and manage complications.
• Initiating treatment for life-threatening conditions immediately is essential to keep the woman’s condition from worsening.
3

Initial Treatment
• Initial steps are similar, regardless of complication.• Definitive treatment may vary:
– Follow local protocols/guidelines.• The goal is to recognize the problem and prevent it from
worsening while saving the woman’s life.
4

Presenting Complications of PAC Clients
Complications may include:• Shock• Severe vaginal bleeding• Infection and sepsis• Intra-abdominal injury • Uterine perforation
5

Shock
• A life-threatening condition that requires immediate and intensive treatment to save the client’s life.
• It is characterized by failure of the circulatory system to maintain adequate blood flow to vital organs, depriving them of oxygen.
• With incomplete abortion, shock is usually caused by blood loss (hemorrhage), dilation of the blood vessels (vasodilation) from infection/sepsis or trauma.
6

Shock (2)
• Clients suffering from shock must be treated immediately and closely monitored because their condition can worsen quickly.
• The primary goal in treating shock is to stabilize the client; that is, to restore the volume and efficiency of the circulatory system as measured by an increase in blood pressure and decrease in the pulse and respiratory rates.
7

Shock (3)
• While the immediate and intensive treatment of shock is essential to save to the woman’s life, it is only the first step: the underlying cause must also be treated immediately in order to prevent the woman’s condition from worsening.
8

Signs and Symptoms of Shock
• Fast, weak pulse (rate ≥110 per minute)• Low blood pressure (systolic <90)• Pallor (especially inner eyelid, palms or around the mouth)• Sweatiness or cold, clammy skin• Rapid breathing (respirations ≥30 per minute)• Anxiousness, confusion or unconsciousness• Scanty urine output (<30 ml per hour)
9

Initial Treatment for Shock
• Call for help.• Monitor vital signs. • Turn the client onto her side to minimize the risk of aspiration if
she vomits.• Make sure her airway is open.• Give oxygen at 6–8 liters per minute (mask or cannula).• Keep the client warm (do not overheat).• Elevate her legs to increase return of blood to her heart.
10
Initial Treatment for Shock (2)
• Give IV fluids (normal saline or Ringer’s lactate), 1 liter in 15–20 minutes with large bore needle (16–18 gauge).
• Note: A more rapid replacement is required in the management of shock resulting from bleeding. Replace 2–3 times the estimated fluid loss: – REFER if IV fluids are not available.
• Do not give fluids or medications orally.
11
Initial Treatment for Shock (3)
• Monitor vital signs, IV fluids and urine output. • Collect blood for hemoglobin or hematocrit—a hemoglobin of 5
g/100 ml or less or hematocrit of 15% or less is life-threatening and will require blood transfusion.
• Cross-match blood; perform a bedside clotting test.• Give broad-spectrum IV or IM antibiotics. • Refer if IV/IM antibiotics are not available.
12
Initial Treatment for Shock (4)
• Remove any visible POC, which may help the uterus to contract and control bleeding. Do not do a complete pelvic exam at this time.
• If the woman’s condition improves, adjust the rate of the IV infusion to 1 liter in 6 hours and continue managing the underlying cause of shock.
13
Severe Vaginal Bleeding
• Prolonged or excessive vaginal bleeding and symptoms of incomplete abortion are usually caused by retained products of conception (POC) or by injury to the vagina, cervix or uterus, including perforation of the uterus.
• Taking prompt action to stop the bleeding and replace fluid or blood volume can be lifesaving.
• The blood pressure and heart rate should also be closely monitored, as shock may develop at any time.
• Blood pressure, pulse rate, hematocrit or hemoglobin, and urine output are the primary measures of the amount of blood loss.
14
Severe Vaginal Bleeding (2)
• Treatment includes control of bleeding, intravenous fluids (when available) to replace fluid volume, antibiotics to fight infection and stabilization before uterine evacuation can occur.
• Surgery may sometimes be required to identify and repair the source of bleeding:– Refer the client to a higher level of care as soon as she is
stable.
15

Signs of Severe Vaginal Bleeding
• Heavy, bright red vaginal bleeding with or without clots • Blood-soaked pads, towels or clothing • Pallor (conjunctiva and around the mouth, or palms) • Dizziness, fainting
16
Initial Treatment for Severe Bleeding
• Same as for shock:– Check vital signs.– Elevate the legs or, if possible, raise the foot of the bed.– Make sure that the airway is open; if available, start oxygen
at 6–8 liters per minute by mask or nasal cannula.– Restore fluid volume:
• Start IV with a large-bore needle or catheter (16 gauge or higher).
17
Initial Treatment for Severe Bleeding (2)
• Monitor amount of blood loss:– Heart rate– Blood pressure– Hematocrit (if lab available) – Number of pads soaked or amount of blood on sheets,
mattress, clothing, etc.• Monitor vital signs, IV fluids and urine output. • Collect blood for hemoglobin or hematocrit; cross-match blood
and perform a bedside clotting test.• If there are signs of intra-abdominal injury or ectopic pregnancy,
do further assessment and appropriate treatment immediately.
18

Disseminated Intravascular Coagulation (DIC)
• If the woman is bleeding from several places and the bleeding is not easily stopped, quickly assess her for DIC, a bleeding disorder that is sometimes seen with severe sepsis.
19
Signs of DIC
• Bleeding from inside the mouth, bladder, injection site or venipuncture site
• Blood in the urine• Failure of the woman’s blood to clot:
– If no lab is available, look at places where blood has pooled such as on the bed or floor to assess clotting
• Decreased platelet count
20

Management of DIC
• Treating the underlying cause of bleeding is the mainstay of DIC management.
• Giving blood products, such as fresh whole blood or fresh frozen plasma, can help control bleeding while the infection is being treated.
• REFERRAL to a higher level (tertiary) facility is usually required.
21

Infection and Sepsis
• Infection is a common complication of incomplete abortion. • The presence of retained POC makes it easy for infection to
grow, especially when they result from an unsafe abortion that used unsafe methods or contaminated instruments.
• Localized infections from induced or spontaneous abortion can rapidly lead to more generalized sepsis and septic shock, which can be fatal.
22
Signs/Symptoms of Infection or Sepsis
• Chills, fever, sweats, general discomfort • Foul-smelling vaginal discharge• Lower abdominal pain/tenderness • Mucopus from the cervix• Excessive pain or cervical motion tenderness on bimanual
examination• Distended abdomen• History of attempting to end the pregnancy or history of recent
miscarriage• Prolonged bleeding (>8 days)
23
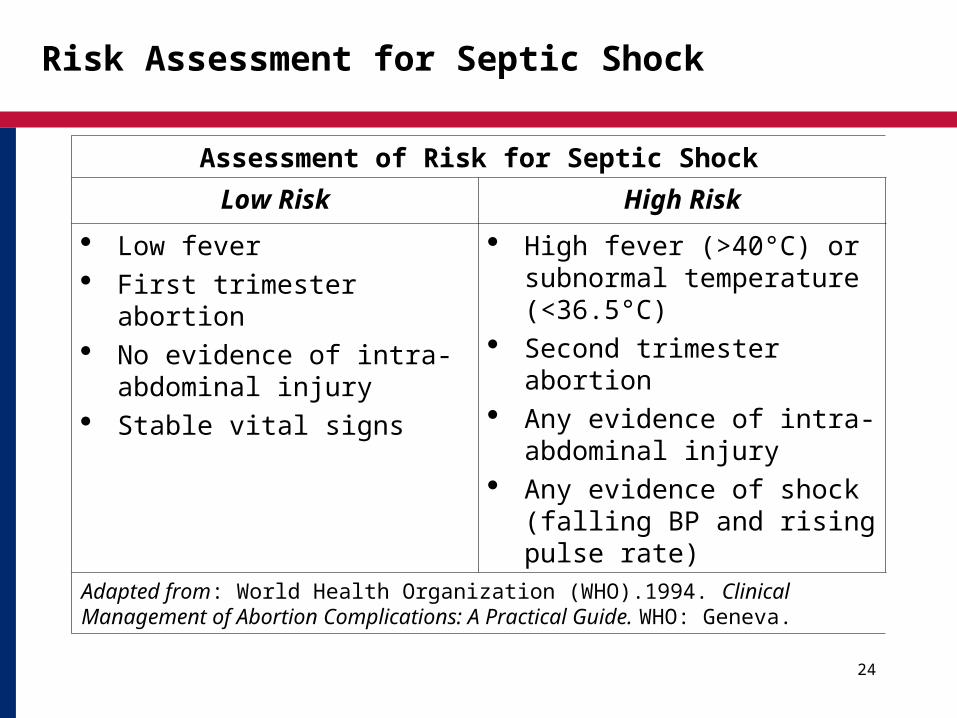
Risk Assessment for Septic Shock
Assessment of Risk for Septic Shock
Low Risk High Risk
Low fever First trimester abortion No evidence of intra-
abdominal injury Stable vital signs
High fever (>40°C) or subnormal temperature (<36.5°C)
Second trimester abortion Any evidence of intra-
abdominal injury Any evidence of shock
(falling BP and rising pulse rate)
Adapted from: World Health Organization (WHO).1994. Clinical Management of Abortion Complications: A Practical Guide. WHO: Geneva.
24
Infection/Sepsis Initial Treatment
• Check vital signs. • Do not give anything by mouth; surgery may be needed.• Make sure the airway is open. If needed, give oxygen 6–8
liters/minute by cannula or mask. • Start IV broad spectrum antibiotics immediately (first obtain
blood cultures—if available).• If the woman has been exposed to tetanus and her vaccination
history is uncertain, give her tetanus toxoid.
25
Infection/Sepsis Initial Treatment (2)
• If the woman becomes unstable, give IV fluids (normal saline or Ringer’s lactate), 1 liter in 15–20 minutes or faster.
• If the woman has lost a lot of blood or appears anemic, check her hemoglobin or hematocrit; cross-match and do clotting test, if available.
• All sources of infection must be identified and treated.• Monitor vital signs, IV fluids and urine output.
26

Intra-Abdominal Injury
• Includes uterine perforation and possible damage to surrounding organs, including the cervix, vagina or bowel.
• Risk of infection, sepsis, peritonitis and tetanus is very high.• May be discovered during the initial physical exam or later during
uterine evacuation (rare with MVA).• May initially present without symptoms, and then progress rapidly
to serious and even life-threatening complications.• A ruptured ectopic pregnancy or ovarian cyst can present with
symptoms of intra-abdominal hemorrhage similar to intra-abdominal injury:– History of ectopic pregnancy, pelvic infection or use of certain
contraceptive methods has greater possibility of ectopic pregnancy.
– Delay in treatment is extremely dangerous and may lead to death unless there surgical intervention.
27

Signs/Symptoms of Intra-Abdominal Injury
• Severe abdominal pain/cramping• Distended abdomen• Nausea/vomiting• Fever• Shoulder pain• Decreased bowel sounds• Tense, hard abdomen• Rebound tenderness• Any of above symptoms combined with signs of shock may
indicate major intra-abdominal hemorrhage
28

Initial Treatment of Intra-Abdominal Injury
• Check vital signs. • Do not give anything by mouth as surgery may be needed.• Make sure the airway is open. If the woman is unstable, give
oxygen 6–8 liters/minute by cannulae or mask. • If there is any indications of infection (fever, chills, pus) give
broad-spectrum antibiotics (IV or IM). • If possible exposure to tetanus and her vaccination history is
uncertain, give tetanus toxoid.
29

Intra-Abdominal Injury Initial Treatment (2)
• To restore fluid volume, give IV fluids (normal saline or Ringer’s lactate), 1 liter in 15–20 minutes or faster, using a large-gauge needle.
• It may take 1–3 liters of IV fluids to stabilize a woman who has lost a lot of blood or is in shock.
• Check her hemoglobin or hematocrit. • Cross-match and perform a clotting test, if available.• Give IV or IM analgesia for pain management.• Monitor urine output. • If possible, take abdominal x-rays.
30

Signs of Perforation before Vacuum Aspiration
• Fast pulse (≥110 per minute)• Falling blood pressure (diastolic <60)• Excess bleeding• Signs and symptoms of intra-abdominal injury
31

Signs of Perforation during Vacuum Aspiration
• Cannula, dilator or other instrument penetrates beyond expected size of the uterus.
• Syringe vacuum decreases with the cannula well inside the uterus.
• Excessive bleeding after the uterus is empty.• Fat or bowel in aspirated tissue found during or after the
procedure.
32

Initial Treatment for Uterine Perforation
• If uterine evacuation not started:– Check for signs of intra-abdominal injury:
• If present, treat accordingly before performing evacuation.• If not present, proceed cautiously with evacuation.
• Treatment during uterine evacuation (evacuation is not complete):– Begin IV fluids and antibiotics.– Check hematocrit; arrange for blood transfusion if indicated
(hematocrit <15% or hemoglobin <5 mg/100 ml).
33
Treatment during Uterine Evacuation (2)
• Complete the evacuation under direct visual control (laparoscopy or laparotomy) to assess damage to pelvic organs and to prevent further damage. If laparoscope not available, REFER.
• Repair damage as necessary.• After surgery, give uterotonic (if the uterus has not been
removed) and observe vital signs every 15 minutes for 2 hours.• If the client becomes stable and bleeding slows, give
ergometrine (0.2–0.5 mg IM if not contraindicated) and observe overnight.
• If condition worsens, transfer to a higher level of care.
34
Treatment of Perforation If the Evacuation Is Complete
• Begin IV and broad-spectrum antibiotics.• Give ergometrine 0.2–0.5 mg IM; repeat up to 3 doses as needed.• Observe for 2 hours, checking vital signs frequently.• If client becomes stable and bleeding slows, give additional
ergometrine (same dose) and continue observation overnight.• If client condition worsens, give additional doses of oxytocin or
ergometrine.• If bleeding continues, a laparoscopy or minilaparotomy may be
needed.• Transfer the woman as soon as possible to a higher level of care.
35

Referral Guidelines
• When a client needs to be referred or transferred, arrangements should be timely and efficient.
• The referral site must have everything possible to stabilize the woman and provide continued treatment.
• Standing arrangements for referral and transport should exist at all health facilities.
36

Referral Guidelines (2)
• Stabilize the client.• Prepare referral information.• If possible, trained staff should accompany the client.• If possible, continue treatments including oxygen and IV
therapy.• Keep client warm.• If in shock or hemorrhage, keep feet elevated.
37