empathy, resilience and distress in norwegian and english
TRANSCRIPT

Empathy, resilience and distress in Norwegian and English investigative interviewers.
Thesis submitted in partial fulfilment of the degree of
Doctorate in Clinical Psychology
(DClinPsy)
University of Leicester
By
Stine Iversen
October 2020
Declaration
I confirm that this thesis and the research reported within it compromises my own work. It
was written and submitted for the degree of Doctorate of Clinical Psychology (DClinPsy). It
has not been submitted for any other academic award. The reported thesis has been checked
for errors prior to submission.
Stine Iversen
2

Empathy, resilience and distress in Norwegian and English investigative interviewers.By Stine Iversen
Thesis abstractThere has been increased scrutiny of occupations who less obviously experience adverseimpacts from indirect exposure to trauma. This thesis aimed to understand occupationaldistress in non-traditional professions, who might similarly experience secondary traumathrough exposure to traumatogenic material; legal profession and law enforcement.Literature ReviewA systematic literature review explored the prevalence and predictors of secondary trauma inlegal professions. Repeated exposure to clients who have experienced trauma comprises asignificant part of lawyers’, attorneys’, solicitors’ and judges’ roles. The search elicited tenarticles for review. Quality appraisal showed significant methodological limitations in thestudies. Still, results showed a high prevalence of secondary trauma, compared to populationgroups and other professional groups. Predictors included gender, work experience, personaltrauma and level of exposure. Findings and conclusions are discussed and indicate that thesignificant variability between studies suggest a need for conceptually consistent andscientifically robust studies in the future.Research ReportThe research report examined secondary trauma prevalence and predictors in English andNorwegian investigative interviewers, as well as the potential role of empathy in thedevelopment of secondary trauma. Police officers whose work task involved investigativeinterviewing were invited to complete an online survey, consisting of questionnairesmeasuring psychological distress, secondary trauma, empathy and perceived organisationalsupport. The results indicated moderate levels of distress and secondary trauma, which werefound to be higher than reported national and international norms. Secondary trauma wasfound to correlate with wider psychological morbidity, and predictive models of distress andresilience were suggested. Findings emphasised the need to implement organisational supportstructures and resilience-building schemes to sustain police officers in key roles to ait thevulnerable and secure prosecutions.
3
Acknowledgements
I would like to acknowledge various people who have supported me through this journey in
recent years as I have worked on this thesis. First, I owe an enormous gratitude for the endless
moral support extended with love, by my parents and grandparents, whose financial support
and passionate encouragement made it possible for me to complete this project. I wish to
extend a special thanks to my dad who let me brainstorm ideas and listened to my worries and
thought processes, without fully understanding exactly what I was saying.
A sincere thanks to my supervisor Professor Noelle Robertson, without whose
inspiration, help and support, this project could not have happened. I appreciate your time,
your guidance and your thoughtful sharing of knowledge and reassurance. I also wish to thank
my secondary supervisor in Norway, Professor Eva Oddrun Langvik, who agreed to cooperate
on my research and contribute towards participant collection, despite the long distance and
many challenges along the way.
To my wonderful cohort, who has shared this experience with me over the last three
years. Thank you for the support, the laughs and the encouragements. I truly appreciate the
love and friendships I have gained, and I am so proud of all of us.
Finally, a dear thank you to my friends in Norway, Kjersti, Henriette and Ingjerd who
always have my back. Thank you for spending time with me during this process, planning and
dreaming of our future and travels. I truly appreciate how you always welcome me back as if
no time has passed.
4
Word CountsSection Word count
Thesis Abstract 291
Literature review 7027
Abstract 160
Full text (excluding reference list, figures and tabulated data) 5569
Main research report 8760
Abstract 186
Full text (excluding reference list, figures and tabulated data) 6522
Appendices* (excluding figures and tabulated data) 2540
Total word count (excluding thesis abstract, tabulated data, figures,
references and mandatory appendices) 18327
*Word count for appendices excludes mandatory appendices as specified in the Coursework
Guidelines and Assessment Regulations Handbook.
5

Table of contentsDeclaration..................................................................................................................................2Thesis abstract.............................................................................................................................3Acknowledgements.....................................................................................................................4Word Counts............................................................................................................................... 5Table of contents.........................................................................................................................6List of Tables.............................................................................................................................. 8List of Figures............................................................................................................................. 9List of Appendices.................................................................................................................... 10List of Abbreviations................................................................................................................ 11Section One: Literature Review................................................................................................12
Abstract................................................................................................................................. 13Introduction........................................................................................................................... 14
Occupational distress in the legal profession.................................................................... 14Conceptual clarification.....................................................................................................15Why examine secondary trauma in legal professionals?...................................................16
Method.................................................................................................................................. 16Study design...................................................................................................................... 16Search strategy...................................................................................................................16Selection criteria for studies.............................................................................................. 17Data extraction...................................................................................................................19Quality appraisal................................................................................................................19
Results................................................................................................................................... 19Elicited studies’ characteristics......................................................................................... 19Methodological features.................................................................................................... 20Methodological quality of included studies.......................................................................21Prevalence of secondary trauma........................................................................................ 23Predictive factors............................................................................................................... 23
Discussion............................................................................................................................. 26Prevalence and measurement.............................................................................................26Predictors and associated factors.......................................................................................27Methodological limitations................................................................................................27Implications....................................................................................................................... 28Strengths and limitations................................................................................................... 29Future research.................................................................................................................. 29Conclusions....................................................................................................................... 30
References............................................................................................................................. 31
6

Section Two: Main research report...........................................................................................35Abstract................................................................................................................................. 36Introduction........................................................................................................................... 37
Investigative interviewing................................................................................................. 37Conceptual framing of occupational distress.....................................................................38Resilience...........................................................................................................................39Empathy and distress......................................................................................................... 39Aims...................................................................................................................................40
Method.................................................................................................................................. 41Research design................................................................................................................. 41Ethical approvals............................................................................................................... 41Participants........................................................................................................................ 41Recruitment....................................................................................................................... 41Procedure........................................................................................................................... 42Measures............................................................................................................................42Data analysis......................................................................................................................44Missing data.......................................................................................................................45Prospective Power and sample size analysis..................................................................... 45
Results................................................................................................................................... 46Respondents.......................................................................................................................46Test of reliability............................................................................................................... 46Demographics....................................................................................................................46What levels of distress and resilience (CF/CS) are reported by investigative interviewersin Norway and the UK?..................................................................................................... 48What factors are associated with reported distress and resilience?................................... 52To what extent do noted correlates predict reported distress and resilience?................... 54Does reported empathy moderate/mediate the relationship with CS/CF and proposedpredictor variables in investigative interviewers?............................................................. 54
Discussion............................................................................................................................. 56Summary of findings......................................................................................................... 56Strengths and limitations................................................................................................... 58Implications....................................................................................................................... 58Future research.................................................................................................................. 59Conclusion......................................................................................................................... 60
References............................................................................................................................. 61Appendices:...............................................................................................................................66
7

List of TablesList of Tables Page number
Section One: Literature Review
Table 1. PICOS-statement informing inclusion and exclusioncriteria.
17
Table 2. Quality Appraisal scores using Appraisal Tool forCross-Sectional Studies
22
Section Two: Research Report
Table 3. Reliability analysis with Cronbach’s alpha values for
each of the measures and subtests.
46
Table 4. Sample characteristics of the UK and the Norwegian
populations.
47
Table 5. One-sample t-tests comparing ProQOL sample means
with norm data
48
Table 6. One-sample t-tests for HADS anxiety and depression
scores compared to UK and Norwegian population
norms.
49
Table 7. Means and Standard deviation on measures for each
participant group, with chosen statistical analysis, effect
sizes and p-values.
50
Table 8. Percentages of distribution of level ranking for each of
the measures, between Norwegian and UK participant
group.
51
Table 9 Bivariate non-parametric correlations between ten
variables
53
Table 10 Simple regression model for STS on anxiety. 55
Table 11 Multiple linear regression model of predictors of CS and
burnout.
55
Appendices
Table 12 Study characteristics and results relating to researchquestions.
77
Table 13 Test of Normality and assumptions statistics 110
8
List of FiguresList of Figures Page number
Section One: Literature Review
Figure 1 PRISMA chart of shortlisting process 18
Appendices
Figure 2 SPSS output of Normal Q-Q Plot for ProQOL
Compassion Satisfaction
110
Figure 3 SPSS output of Normal Q-Q Plot for ProQOL burnout 111
Figure 4 SPSS output of Normal Q-Q Plot for ProQOL
Secondary Traumatic Stress
111
Figure 5 SPSS output of Normal Q-Q Plot for HADS Depression 112
Figure 6 SPSS output of Normal Q-Q Plot for HADS Anxiety 112
Figure 7 SPSS output of Normal Q-Q Plot for ProQOL
Cambridge Behaviour Scale – Empathy Quotient
113
Figure 8 SPSS output of Normal Q-Q Plot for Survey of
Perceived Organisational Support.
113
9
List of AppendicesMandatory appendices are marked with an asterisk (*)
Page number
Appendix A* Guidelines to authors for journal targeted for literature
review
67
Appendix B Expanded details on search methodology 73
Appendix C Data extraction form 74
Appendix D* AXIS Quality appraisal tool items 75
Appendix E Table of findings for literature review 77
Appendix F* Guidelines to authors for journal targeted for research
project
87
Appendix G* Ethics letter of approval from UK, UOL 90
Appendix H* Norwegian ethics approval from Regional committee for
medical and health related research ethics (written in
Norwegian)
92
Appendix I* Participant information sheet 94
Appendix J* Online consent form 96
Appendix K* Complete online questionnaires, with public measures 97
Appendix L Exploration of missing data 108
Appendix M Evaluation of assumptions 109
Appendix N Q-Q plots with normality tests 110
Appendix O* Checklist assuring confidentiality and anonymity of
participants.
114
Appendix P* Chronology of research 116
Appendix Q* Statement of epistemological position taken 117
10
List of Abbreviations.AUDIT World Health Organisation’s Alcohol Use Disorders Identification Test
AXIS Appraisal tool for cross-sectional studies
BPNSW Basic Psychological Needs Satisfaction at Work
CBI Copenhagen Burnout Inventory
CES-D Center for Epidemiologic Studies Depression Scale
CF Compassion fatigue
CS Compassion satisfaction
DASS-21 The Depression, Anxiety and Stress Scale
EQ Cambridge Behaviour Scale – Empathy Quotient
HADS Hospital Anxiety and Depression Scale
HSCL-25 The Hopkins Symptoms Checklist-25
IDLS International Depression Literacy Survey
K-10 Kessler Psychological Distress Scale
LEC-5 Life Events Checklist for DSM-5
MBI-GS Maslach’s Burnout Inventory – General survey
MHP Mental Health Practitioners
MRA Multiple regression analysis
PCL-5 PTSD Checklist for DSM-5
POS Perceived organisational support
ProQOL Professional Quality of life Scale
PTSD Post-Traumatic Stress Disorder
SDS Sheehan Disability Scale
SPOS Survey of Perceived Organisational Support
STS Secondary traumatic stress
STSS Secondary Traumatic Stress Scale
TABS Trauma and Attachment Belief Scale
TIPI Ten Item Personality Measure
VT Vicarious Trauma
VTS Vicarious Trauma scale
WHOQOL-
BREF
World Health Organisation’s Quality Of Life –BREF
11

Section One: Literature Review
Prevalence and predictors of secondary trauma in the legal profession: A systematic review
Target journal: Psychiatry, Psychology and Law
See Appendix A for author guidelines
Presented here using BPS Style guidelines.
12

AbstractThere has been increased scrutiny of occupations who less obviously experience adverse
impacts from indirect exposure to trauma. In legal professions, repeated exposure to clients
who have experienced trauma comprises a significant part in the role of lawyers’, attorneys’,
solicitors’ and judges’. The current review aimed to explore the prevalence and risk factors of
secondary trauma reported by such legal professionals. A systematic search using seven
psychological and legal databases elicited ten articles for review. Quality appraisal revealed
several methodological frailties in the reviewed articles, and therefore the findings should be
interpreted with caution. Results indicated a higher prevalence of secondary trauma in legal
professionals, compared to both the general population and other professional groups.
Synthesis also highlighted predictors and correlates of secondary trauma, notably gender,
work experience, personal trauma and level of exposure. The review emphasised significant
variability between the studies making systematic comparisons challenging, as well as the
need for further conceptually consistent and scientifically robust studies.
13
IntroductionRepeated exposure to clients who have encountered trauma is a dimension of working within
legal occupations. Indeed, legal professionals, particularly those employed in criminal law,
will experience work with vulnerable victims of crime. This exposure implies contact with
traumatogenic material, such as graphic, injurious photographic evidence or witness accounts,
and narratives of traumatic events accompanied by heightened levels of emotions and distress
from clients. Work tasks may involve direct and indirect experience of strong emotions
through consultation with clients pursuing custody and liability battles, imprisonment,
managing court proceedings or issuing sentences, which may also imply trauma exposure.
Given the frequency of such work-related exposure, legal professionals may themselves be
vulnerable to adverse psychological impacts (James, 2020).
In 2013, the Diagnostic and Statistical Manual of Mental Disorders (DSM-5;
American Psychiatric Association, 2013) included indirect occupational exposure as a viable
criterion for the Post-Traumatic Stress Disorder (PTSD) diagnosis. Symptoms of PTSD
include intrusions, avoidance, negative alterations in cognition/mood, and alterations in
arousal and reactivity. The reported criterion related to indirect exposure specifies possible at-
risk professions, such as first responders and health professionals (Greinacher et al., 2019).
In recent years there has been greater awareness and research examining the potential
adverse effects of indirect trauma, particularly on health and social care professionals; notably
nurses (Yang & Kim, 2012), mental health professionals (Collins & Long, 2003), therapists
(Canfield, 2005) and social workers (McFadden et al., 2014). Recently research has
broadened its scope to other occupations that may also potentially experience adverse impacts
from indirect exposure to trauma.
Occupational distress in the legal professionFor this review, the term “legal profession” encapsulates several different roles: barristers;
attorneys; solicitors; lawyers; and judges. These professionals, often associated with high
status and high earning, also report significant indices of psychological morbidity, such as
high levels of clinical depression, stress (Parker, 2014) and excessive alcohol use (Krill et al.,
2016).
Furthermore, a growing body of research shows that other groups involved in legal
processes experience distress. Up to 50 per cent of criminal jurors reported trauma-related
symptoms following their involvement in criminal court (Lonergan et al., 2016), known as
14

juror stress (Miller & Bornstein, 2004). It follows that other legal professionals exposed to
similar traumatic processes and materials may be similarly affected.
Additionally, an expanding evidence base suggests that other professions working
within the legal and justice system exhibit adverse effects from indirect exposure to trauma;
notably police officers have been extensively researched compared to other legal professions.
Reviews of adverse impacts for police officers following exposure to traumatised individuals
indicated that gender and personal trauma history were potential risk factors, whilst
peer/social support, use of humour and organisational recognition of distress were potential
resilience factors (Greinacher et al., 2019, MacEachern et al., 2019). Related professions
might show similar predictors from indirect exposure to trauma.
Conceptual clarificationThe adverse impacts of exposure to other’s distress was first identified amongst those working
in human services and constructed as ‘burnout’. Initially conceived by Maslach (Maslach &
Jackson, 1981; Maslach et al., 1996), burnout encompasses exhaustion, depersonalisation,
reduced personal accomplishment and cynicism due to work requiring intense emotional
involvement with clients over time, culminating in occupational exhaustion.
Emerging from psychotherapeutic encounters, vicarious trauma (VT) was described by
Pearlman and Saakvitne (1995). They noted changes in therapists’ inner schemata about their
views of the world and their safety within it, via exposure to traumatised clients. Discriminant
validity proposed that VT is distinct from other concepts of secondary trauma due to the
transformative cognitive processes that occur (Baird & Kracen, 2006).
At much the same time, Figley (1995) noted PTSD-like symptoms in social workers
who had been exposed to traumatised clients, including symptoms such as hyperarousal,
flashbacks and avoidance. This distress with trauma-like features was termed secondary
traumatic stress (STS), arising via four mechanisms: empathetic engagement; personal trauma
history; unresolved trauma; and working with childhood trauma. Figley also coined the term
Compassion Fatigue (CF), using the term interchangeably with STS. In 2010, Stamm
redefined the term CF given the valence of the word fatigue, instead suggesting both STS and
burnout as two constituent elements forming CF. Further refinement of the construct was
conducted by Nolte et al. (2017), whose review offered a model explaining trigger factors,
physical and emotional symptoms. Symptoms included fatigue, physical pain, disturbed sleep,
withdraw and hopelessness.
15
Thus indirect trauma exposure can contribute to forms of occupational distress which
are variably and inconsistently described as burnout, VT, STS, and CF. Attempts have been
made to provide clarification, however overlap in descriptions and domains remains, core
features are contested (Elwood et al., 2011), and diverse operationalisation and measurement
has generated a cadre of research under differing conceptual frameworks. For the purposes of
this review, the collective term of secondary trauma will be used to encapsulate the
phenomena as mentioned earlier (PTSD, burnout, VT, STS and CF), thought to arise from
effects of indirect trauma exposure.
Why examine secondary trauma in legal professionals?Given that legal professionals appear regularly exposed to traumatogenic material, a critical
appraisal and synthesis of the extent of any secondary trauma and potential risk factors seems
warranted. A recent review (James, 2020) examined the history of trauma-informed legal
practise and recent studies of lawyer’s wellbeing, while discussing the recognition of
secondary trauma within the legal profession. This article also puts great emphasis on the
relative paucity of studies so far and the need for organisational recognition and structural
trauma-informed change. To date, there has been no systematic attempt to summarise,
appraise and synthesise published research. While such work-related distress will be captured
variously, examining quantitative research focusing on prevalence and risk factors under the
rubric of secondary trauma should summarise the extent of reported difficulties and factors
related to them. Potentially, this will contribute to identifying gaps in the research base, offer
suggestions to mitigate distress and opportunities for further research. The current review thus
has the following aims:
1) To examine the prevalence of secondary trauma in legal professionals and the
dominant means of measuring the phenomena.
2) To understand what predictors and associated factors within the legal profession
appear to contribute to secondary trauma, including how those suggested factors
explain levels of variance in developed secondary trauma.
MethodStudy designA study protocol, and its reporting, was informed by PRISMA recommendations (Moher et
al., 2009) and the Centre for Reviews and Dissemination (CRD, 2009). The current review
was not registered with PROSPERO (Booth et al., 2012), but interrogation of the database
revealed no registered reviews on this topic.
16
Search strategyThe search strategy was developed with a senior university librarian. Initial scoping searches
identified no current literature reviews on indirect trauma exposure in the legal professions,
but an examination of grey literature via Google scholar revealed a growing evidence base
regarding indirect traumatisation and occupational distress across professional groups.
A systematic search strategy was undertaken in October 2019, informed by PICOS
(Table 1). Seven databases (PsychINFO, PILOTS, PubMed, Web of Science, Westlaw UK,
Business Source Premier and Criminal Justice Abstracts) were utilised, to ensure coverage of
health research, social sciences and legal subjects. The search terms employed included;
“burnout” OR “compassion fatigue” OR “secondary trauma” OR vicarious trauma” OR
“PTSD”, with combinations of; “solicitor” OR “barrister” OR “lawyer” OR “attorney” OR
“judge” OR “legal”, with all variations and synonyms of the terms. Boolean operation and
truncation methods were carried out in individual databases. A complete list of the search
terms and search strategy is provided in Appendix B.
Selection criteria for studiesTable 1PICOS-statement informing inclusion and exclusion criteria.
Inclusion criteria Exclusion criteriaP-population
Legal professions; barristers,attorneys, solicitors, lawyers andjudges.
Other professions, including lawenforcement and policing.
I-intervention
N/A Aim to measure coping strategies
C-comparison
Including both comparative andnon-comparative studies.
N/A
O-outcome
Prevalence or predictors ofsecondary trauma.
Study aimed to measure directtrauma.
S-study type
Quantitative and mixed methodswith independently discerniblequantitative data.
Qualitative studies, editorials andreviews.
The filters applied to the databases limited results to “peer-reviewed publications” and
“English language”. The author determined study eligibility for inclusion. No date restrictions
were made given no literature reviews were found during initial scoping. All results from the
databases were exported to EndNote X9, where all duplicates were removed automatically, as
well as manually.
17
Eligibility criteria for selected studies were guided by the PICOS method. The
inclusion criteria, were employed during the examination of titles and abstracts, with
reference mining employed to ensure all salient articles were included. Thirty-four articles
met the inclusion criteria and were read in full. After reading, 24 articles were excluded.
18

Figure 1. PRISMA chart of shortlisting process
19
Initial search of PsychINFO, PILOTS, PubMed, Web of science, Westlaw UK,Business Source Premier and Criminal Justice Abstracts databases using
specified search terms and applied filters.
Search results n = 3289PsychINFO = 1396, PILOTS = 458, PubMed = 615, Web of science = 461,
Westlaw UK = 8, Business source premier = 140, Criminal justice abstracts =211
Articles exported to EndNote X9n = 3289
Titles and abstracts screened forinclusion criterian = 2303
Articles read in full and examinedfor specific inclusion criterian = 34
Total articles included for reviewn = 10
Duplicates removed n = 986
Articles excluded n = 2269
Articles excluded n = 24Focus on direct trauma (n=14);Review (n=6);Focus on coping strategies (n=1),Focus on conceptual meanings(n=2) Using qualitative method(n=1).
Data extractionA specially constructed form was developed to extract salient information (Appendix C).
Essential information extracted comprised: author and publication date; aims; sample
demographics; sampling method; study design; measures; analysis (reliability and validity);
results; conclusions; implications; and limitations. To clarify how secondary trauma had been
conceived and applied, the definition adopted in each paper was included as well as
psychometric properties of measures, method of statistical analysis and effect sizes.
Quality appraisalAfter paper selection, articles were assessed for quality using Downes et al. (2016) Appraisal
Tool for Cross-sectional Studies (AXIS). AXIS was developed to address a need for
specificity, generalisability and transferability often absent in other tools appraising cross-
sectional studies. Its development included a Delphi panel, adding to its robustness by
applying expertise and evidence from several different disciplines. Its use in this review is to
assess and compare study quality rather than for exclusion of studies.
The AXIS tool comprises twenty questions (Appendix D) across three domains:
“study design” (seven questions); “reporting” (seven questions); and “introduction of bias”
(six questions). The responses to the questions are categorical (“yes”, “no, “do not know”),
rather than numerically linear, to avoid inter-scale incongruity. Each question was
individually appraised as either present (“yes”) or not present in the study (“no” or “do not
know”). The author created a sum out of 20 items, where ≥16 indicated high-quality studies
(Kiss et al., 2018; Wong et al., 2018).
All studies were quality assessed by two individual and independent raters using the
same appraisal criteria to assess 50 per cent of the studies, which were randomly selected.
Inter-rater reliability showed a strong level of agreement, κ=.84, p<.001.
ResultsElicited studies’ characteristicsTen articles satisfied inclusion criteria and were included in the current review. All papers
were published between 2003 and 2019, were cross-sectional in design and employed survey
methodology. Most studies were solely quantitative, but one study reported mixed-methods.
Five of the studies purposively surveyed their target professional group, and the rest used
comparative between-groups designs. One article reported comparison data on mental health
professionals’ (MHP) and lawyers’ occupational distress, without data on sample size or
characteristics (Levin & Greisberg, 2003). The remaining nine articles reported data from
20
1593 participants, 1454 of whom were legal professionals (the remainder from comparator
professions). Legal professionals represented in the papers comprised lawyers (N=907, 62.4
per cent) and judges (N=547, 37.6 per cent), working in different legal domains: immigration
(Lustig et al., 2008); asylum (Piwowaczyk et al., 2009); criminal/non-criminal law (Vrelevski
& Franklin, 2008). In comparative studies, legal professionals’ distress was variously
compared to other professions, such as social workers, MHPs, psychologists (Levin &
Greisberg, 2003; Maguire & Byrne, 2017), or administrative support staff (Levin et al., 2011).
Across the nine studies, 52.6 per cent were female, and 46.3 per cent were male, which
is consistent with distribution in Australia and Canada (FLSE, 2017; LSNSW, 2016). The
gender distribution in this review is different from reported statistics in the USA (Male: 65 per
cent; ABA, 2018). Age was reported both in mean and in percentages per age group, making
direct comparison challenging. All studies were completed in English speaking countries
(Australia, Canada, and the USA). Only two studies offered data on ethnicity, both reporting
that a majority of the participants were reported as either Caucasian or Anglo-Saxon (Leclerc
et al., 2019; Vrelevski & Franklin, 2008). Sample characteristics are presented in detail in
Appendix E.
Methodological featuresAll studies employed survey design and convenience sampling. None of the studies reported
justification for the chosen sample size, which may reflect the sampling method or the
exploratory nature of some of the studies. Two articles (Jaffe et al., 2003; Schrever et al.,
2019) made use of author-designed questionnaire items. In between-group design studies, the
aim of the comparison group was rarely justified or clarified further, mainly methodological
limitations inherent to comparing two different professions.
All studies measured elements of indirect exposure to trauma, either through validated
measures, or through development of their questionnaire items. The studies operationalised
secondary trauma in various ways: VT (Jaffe et al., 2003; Levin & Greisberg, 2003; Maguire
& Byrne, 2017; Vrelevski & Franklin, 2008); PTSD (Leclerc et al., 2019); STS (Lustig et al.,
2008; Piwowarczyk et al., 2009; Schrever et al., 2019); and CF (Levin et al., 2011; Miller et
al., 2018).
Measures focused predominantly on elements of secondary trauma (VTS, IES-r, MBI-
GS, STSS, LEC-5, CBI, PCL-5, ProQOL) and psychological distress (DASS-21, K-10, CES-
D, IDLS, HSCL-25). Furthermore, studies made use of other specific measures related to
alcohol use (AUDIT), personality (TIPI), functional impairment (SDS) and trauma/attachment
21

beliefs (TABS). Only one study explicitly reported instructing participants to focus on work-
related trauma and indirect trauma exposure from clients (Leclerc et al., 2019), making it
questionable whether reported secondary trauma scores were a result of direct or indirect
exposure. Variability in constructs used, and hence measures, precluded direct comparisons
between studies.
Methodological quality of included studiesThe quality scores of the included studies ranged from five to 17 criteria met, with one article
meeting the threshold for high quality (>16). A summary of the studies’ methodological
quality according to specific AXIS items is provided in Table 2, with the complete AXIS
items in Appendix D.
The “quality of reporting” category (seven items) had the highest criteria met (M=5.6;
range=1-7). Aims, target population and methodology were described across most of the
studies, as were basic data and limitations. However, four studies failed to report statistical
significance or precision estimates appropriately.
The “study design” category (seven items) revealed fewer scores in criteria met (M=4;
range=2-5). Most studies showed appropriate design relevant to the proposed aims, measured
relevant outcome variables and linked their results to the discussion. However, none of the
studies presented power calculations to justify their sample size, and only three studies
reported on conflicts of interest. Three studies failed to report on ethical approval or consent
procedures.
The “risk of bias” category (six items) showed fewest criteria met (M=2.9; range=0-5).
Most studies used previously published measures. Sampling methodology was primarily
informed by convenience sampling, which has inherent limitations and difficulties in
addressing non-response bias.
22

23
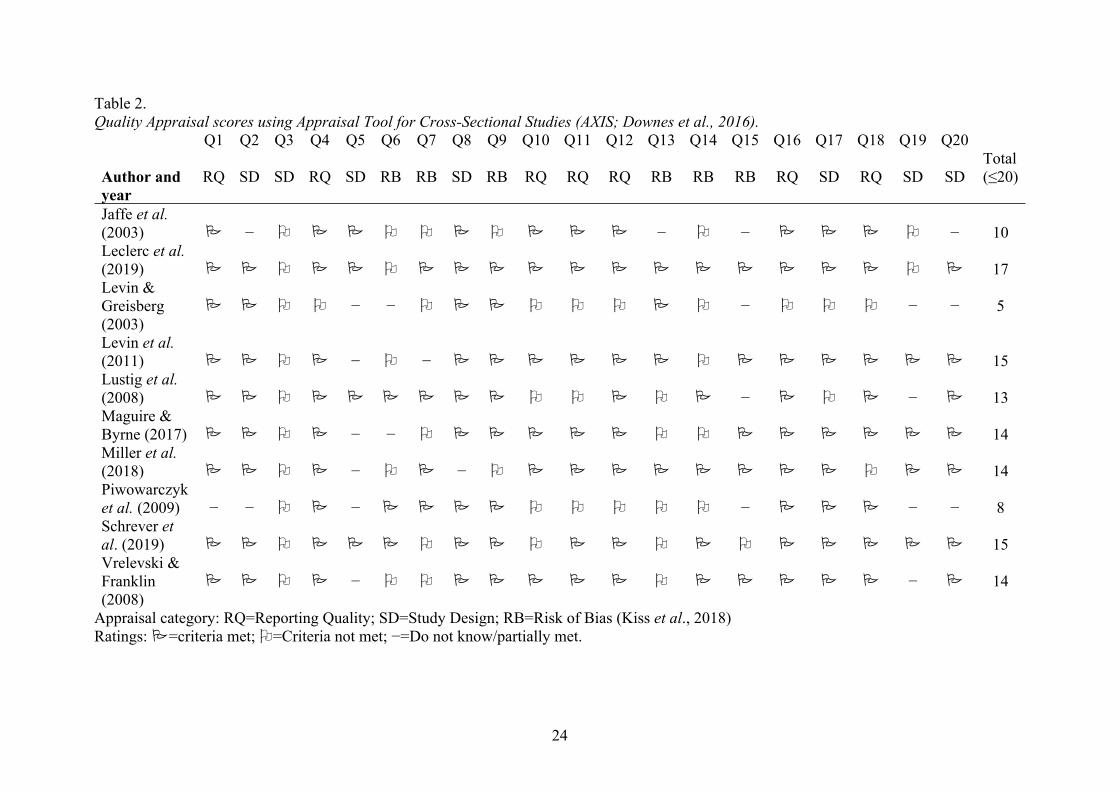
Table 2.Quality Appraisal scores using Appraisal Tool for Cross-Sectional Studies (AXIS; Downes et al., 2016).
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12 Q13 Q14 Q15 Q16 Q17 Q18 Q19 Q20
Author andyear
RQ SD SD RQ SD RB RB SD RB RQ RQ RQ RB RB RB RQ SD RQ SD SDTotal(≤20)
Jaffe et al.(2003) − − − − 10Leclerc et al.(2019) 17Levin &Greisberg(2003)
− − − − − 5
Levin et al.(2011) − − 15Lustig et al.(2008) − − 13Maguire &Byrne (2017) − − 14Miller et al.(2018) − − 14Piwowarczyket al. (2009) − − − − − − 8Schrever etal. (2019) 15Vrelevski &Franklin(2008)
− − 14
Appraisal category: RQ=Reporting Quality; SD=Study Design; RB=Risk of Bias (Kiss et al., 2018)Ratings: =criteria met; =Criteria not met; −=Do not know/partially met.
24
25

Prevalence of secondary traumaAll but one reviewed study (Miller et al., 2018), which reported perceived general stress,
reported the prevalence of secondary trauma. Prevalence was reported in percentages and
through statistical comparison between occupations. Two studies examining judges revealed
that the majority were experiencing one or more symptoms of secondary trauma (63 per cent,
Jaffe et al., 2003; 83.6%, Schrever et al., 2019). When using PTSD screening tools, 9 per cent
(Leclerc et al., 2019) and 11 per cent (Levin et al., 2011) of lawyers met the criteria for
PTSD. By interpreting STSS scores, Schrever et al. (2019) reported that 30.4 per cent of the
judicial officers qualified for a PTSD diagnosis. Piwowarczyk et al. (2009) found that 9 per
cent of their participants scored higher than 30 on the STSS scale, without stating a cut-off
score or providing inferences based on this score.
In studies comparing legal professionals’ secondary trauma to that in other
occupations, PTSD-symptoms and psychological distress were consistently reported as higher
for legal professions: attorneys compared to social workers and psychologists (Levin &
Greisberg, 2003); lawyers and MHPs (Maguire & Byrne, 2017); lawyers and administrative
support staff (Levin et al., 2011); immigration judges and hospital or prison staff (Lustig et
al., 2008). Additionally, criminal lawyers reported significantly higher secondary trauma
scores compared to non-criminal lawyers (Vrelevski & Franklin, 2008), and judges reported
significantly higher secondary trauma scores compared to barristers (Schrever et al., 2019).
Most studies did not report on effect sizes (Appendix E). However, Maguire and Byrne
(2017) comparing lawyers and MHPs reported a large effect size (d=.90) for vicarious trauma
on the VTS and a medium effect size (r=.40) for impact of trauma on IES-r. Levin et al.
(2011) also found large effect sizes from the PROQOL on burnout (d=.98) and STS (d=.78)
when comparing lawyers and administrator staff.
Consequently, nine of the ten papers report elevated levels of secondary trauma in the
legal profession. Furthermore, all comparative studies reported significantly higher scores in
the legal profession, compared to other professions, though not all studies reported on effect
sizes. Prevalence of secondary trauma was primarily reported as the presence of secondary
trauma symptoms or as meeting criteria for a PTSD diagnosis.
Predictive factorsAs demonstrated in Appendix E, all ten studies collected information regarding diverse
predictors. The author will aim to present examined risk factors and highlight similarities or
differences in key findings. The review considered both associated factors emergent from the
26
studies and results from predictive regression analyses. Factors elicited were: gender; age;
work experience; personal trauma; trauma exposure; and personality traits. In total, only three
studies made use of linear regression analysis examining different variables (Levin et al.,
2011; Maguire & Byrne, 2018; Miller et al., 2011), which limits extensive examination of the
level of variance explained by the predictors.
Gender
Six included articles reported on comparative gender data as an influencing factor of
secondary trauma in the legal profession, revealing equivocal results and no reported effect
sizes. Some reported that females were more likely than males to report STS symptoms (Jaffe
et al., 2003), meet a probable PTSD diagnosis (Leclerc et al., 2019) or experience higher
levels of burnout and stress (Lustig et al., 2008). Two studies reported no effect of gender on
STS (Levin et al., 2011; Maguire & Byrne, 2017). Miller et al. (2018) found that gender was a
mediator between social support and outcome variables (burnout, perceived stress and job
performance), such that high levels of social support related to lower levels of burnout, but
only for males. Furthermore, reduced social support in females showed adverse effects on job
performance.
Age
Three studies examining age as a predictor of secondary trauma reported no significant effect
on reported secondary trauma (Levin et al., 2011; Lustig et al., 2008; Maguire & Bryne,
2017).
Personality traits
In the sole paper examining personality, Maguire and Byrne (2018) examined personality
factors in secondary trauma between professions (lawyers and MHPs). Through hierarchical
multiple regression analysis of secondary trauma, profession accounted for 15 per cent of the
variance. Next, the personality trait Emotional Stability (neuroticism) increased explained
variance by 20 per cent. Four further personality traits (Extroversion, Openness,
Agreeableness, and Conscientiousness) explained variance by a further 18 per cent, and
personal trauma history added 6 per cent to the explained variance. The authors framed their
findings where neuroticism/agreeableness were described as potential risk factors, and
conscientiousness/openness potential resilience factors for secondary trauma.
Direct personal trauma
Three of the studies suggested a personal history of trauma correlated with secondary trauma
symptoms. Maguire and Byrne (2017) found that although direct trauma did not correlate
27

significantly with secondary trauma, it contributed to 6 per cent of the variance. Vrelevski and
Franklin (2008) found that direct trauma impacted on secondary trauma, irrespective of the
level of trauma exposure at work. Leclerc et al. (2019) also reported that prior trauma was a
significant distal factor of distress; women, who were reporting prior trauma and elevated
weekly hours at work, had an increased risk of developing depression and anxiety symptoms.
Work experience/ work hours.
Contribution of work experience showed mixed results, either showing no effect of years of
experience psychological distress (Leclerc et al., 2019; Levin et al., 2011) or conversely that
longer work experience predicted higher levels of STS (Jaffe et al., 2003) and burnout (Miller
et al., 2018). Leclerc et al. (2019), whose study suggested a cumulative effect of trauma
exposure, noted increased weekly hours of work heightened the risk of developing PTSD
symptoms by 1.89 times. Levin et al. (2011) also reported that weekly work hours acted as a
significant mediator in developing STS symptoms, when comparing attorneys and
administrative support staff.
Levin et al. (2011) examined the explained variance of work hours and trauma
exposure with secondary trauma between professions (attorneys and administrative staff). A
direct association model showed that attorneys had higher high levels of PTSD symptoms,
and that profession explained 7 per cent of the variance. When work-related exposure was
added, the model explained 14 per cent of the variance. Next, they found that attorneys were
significantly associated with high levels of STS and burnout, which explained 20 per cent of
the variance. When including work hours and trauma-exposure as mediators, the model
explained 32 per cent of the variance.
Level of indirect trauma exposure
Two studies reported within-profession comparisons to control for level of trauma exposure.
Leclerc et al. (2019) collected information on the percentage of respondents’ caseload
containing clients experiencing trauma in the past year, finding the level of trauma exposure
increased the risk of developing PTSD, higher levels of psychological distress and lower
quality of life. Effect sizes between levels of trauma exposure were: no exposure to moderate
exposure (medium; d=.40); no exposure and high exposure (large; d=.70); and moderate and
high exposure (small to medium).
Vrelevski and Franklin’s (2008) comparison of criminal and non-criminal lawyers
reported that criminal lawyers (arguably exposed to more traumatogenic material) were more
likely to develop secondary trauma symptoms and psychological distress, than non-criminal
28

peers; they also disclosed more difficulties relating to self-safety, other-safety and other-
intimacy attachment beliefs.
DiscussionThe current study is the first systematic review to examine the prevalence and measurements
of secondary trauma in legal professionals and associative and predictive factors of secondary
trauma. The review aimed to understand the extent of any difficulties and what factors might
be amenable for mitigation or intervention. After a systematic process of identifying,
interrogating and appraising available research findings, ten articles examining legal
professionals were chosen for review.
Prevalence and measurementAppraisal and synthesis of the ten elicited studies all revealed elevated reported levels of
secondary trauma. The prevalence rate of one or more symptom of secondary trauma ranged
from 63 per cent to 83.6 per cent. A higher percentage of the studies populations met the
DSM criteria for a PTSD diagnosis, ranging from 9 per cent to 30.4 per cent. The prevalence
was significantly higher than reported numbers from The World Health Organisation world
mental health survey (Koenen et al., 2017) reporting cross-national lifetime prevalence of
PTSD at 3.9 per cent. As some studies did not indicate if they instructed participants to only
consider secondary trauma when completing questionnaires, it is unclear whether reported
secondary trauma scores were a result of direct or indirect exposure, or a combination of the
two. This is further complicated by the studies’ chosen prevalence score, as PTSD levels
could potentially include participant’s own past trauma experiences.
Comparative studies also revealed that legal professionals reported significantly higher
levels of secondary trauma compared to MHPs, social workers, psychologists, administrative,
hospital and prison staff. Comparisons were also made within the legal professions, where
criminal lawyers had higher levels of secondary trauma compared to non-criminal lawyers,
and judges were found to have higher levels compared to barristers. The two studies reported
high effect sizes when comparing lawyers with MHPs (Maguire & Byrne, 2017) or with
administrative staff (Levin et al., 2011). Despite these findings, the results should be
interpreted with caution due to the poor scientific methodology in most of the chosen studies.
The disparate studies reflected the conceptual confusion in the area of secondary
trauma, and the lack of reported effect sizes and prevalence rates across key findings made it
more challenging to draw conclusion. As such, prevalence was more distinctly reported in this
review as meeting a diagnosis of PTSD, rather than other typical secondary trauma terms.
29

Moreover, the studies used a mixture of non-validated explorative questions and validated
instruments on trauma (IESr, PCL-r, LEC), burnout (MBI, CBI), secondary trauma (VTS,
STSS, ProQOL) and general psychological distress.
Predictors and associated factorsAcross the ten studies, only two consistent findings were found; age was unrelated to
secondary trauma, and levels of trauma exposure consistently correlated with secondary
trauma levels. The results from the remaining proposed variables were inconsistently found
across studies, notably gender, work-experience, history of personal trauma and personality
traits. These findings were inconsistent with results presented in a review on secondary
trauma in first responders (Greinacher et al., 2019), which found effects of age, gender and
previous trauma. Mediators reported in the studies, which contributed to the variance of
secondary trauma, included work hours, trauma exposure, personality traits and personal
trauma history. Again, these findings should be interpreted with caution.
The current review only reported on factors presented in the ten articles. This does not
exclude the possibility of several other potential factors, which were not presented in the
current review. Interestingly, organisational information was not collected in any of the ten
articles. The lack of consideration around organisational contexts could promote blame on
individuals rather than acknowledging how the organisation could play a part in occupational
distress. One could speculate that an individualistic culture could limit resilience-building
schemes, which are protective of secondary trauma – such as peer support or supervision
(James, 2020).
Methodological limitationsAnalysis of the chosen articles for review revealed multiple methodological flaws and
considerable variation in quality and scientific rigour. All studies made use of self-report
measures and convenience sampling, which elicits several limitations such as social-
desirability bias, confirmation bias and selection bias. Moreover, as several studies were
exploratory, they made use of questionnaire items that had not been validated. It is hard to
assume that the studies were measuring what they intended, especially considering the current
conceptual difficulties. It is unclear if participants were asked to report specifically on work
related indirect trauma, and as such the PTSD measures would likely have included elements
of direct and indirect exposure to traumatic content.
In the studies that made use of control groups, the substantial differences in occupation
could have contributed to numerous confounding variables, and the large reported effect sizes.
30
Furthermore, when comparing the effects of reported trauma exposure with secondary trauma
measures, one could argue that they measure very similar constructs on which the measures
were based. In that regard, it is unclear whether the results in those cases depict significant
effects or if it is merely confirming construct validity in the secondary trauma measures. Most
of the studies did not adequately control for trauma exposure to indicate a valid effect of
secondary trauma.
Consistent results relating to the high prevalence of secondary trauma could indicate a
presence of publication bias, specifically as all presented articles were published in peer-
reviewed journal articles. Among the risk factors, the only observed consistent results were
age and trauma exposure. There seems to be a high need for further examination of the
inconsistent factors: gender; work experience; and personal trauma history.
Given the numerous methodological limitations and variability in quality appraisal
scores, the results should be interpreted with caution. Overall, interpretations of the findings
were challenging due to the methodological and conceptual limitations inherent in the
literature. Nevertheless, the current review of the chosen articles contributed to some
noteworthy findings that might prove useful in informing future research.
ImplicationsDespite the relatively few studies, the disparate measurement and some equivocal findings,
the results from this review signify the importance of understanding secondary trauma in
occupations other than health and social work. Whilst the findings from this review should be
interpreted with caution, they could have implications for diagnostic manuals that currently
focus on first responders and health professions. Interestingly, by opening the diagnostic
criteria to other professions, their occupational distress could be taken seriously in academia
and medical environments. However, implementing professions within the PTSD-diagnosis
might also contribute to a risk of pathologising normal responses to adverse traumatogenic
exposure.
Though the legal profession might not be traditionally viewed as high risk of trauma
exposure, the results suggest that is not the case. Addressing elevated secondary trauma levels
are not only essential to promote professional wellbeing and sustainability of their careers, but
also given their need to argue for delivery of best evidence, judicial reviews and enacting the
law. As health-professionals receive supervision and trauma-training, they might be better
equipped in dealing with indirect trauma-exposure. Findings from the current review could
emphasise the need for training and support available for legal professionals with high trauma
31
exposure through their work. However, the distinct individualistic focus within the studies
prohibits any examination of the development of resilience, or perceived organisational
support. Perhaps the recognised absence of organisational data could have implications for
reviewing legal professionals’ individualistic culture.
Strengths and limitationsThe current study is the first systematic review to examine secondary trauma prevalence,
predictors and associated factors in the legal profession. The inclusion criteria allowed for a
range of legal professions to be included. However, despite this breadth, the search only
elicited a small number of articles fitting the full inclusion criteria. This indicates that the
discipline is still in its infancy. The current review emphasises a great need to improve
research quality and quantity within this area of study. Additionally, this review usefully
highlights that professions other than health and social work might be affected by indirect
trauma exposure.
However, the present review is also subject to several limitations. Given the
considerable variability in conceptual understanding and methodology, this inhibited the
opportunity for adequate comparison of effect sizes. Although the review has contributed to
an understanding of the research aims, they may not have been addressed in a way that
provided a definite answer. Moreover, this study solely focused on quantitative research,
where qualitative sources could have provided a richer comprehension of the experience and
meaning-making with the presented concept and population.
This review focused solely on the psychological construct of secondary trauma. It is
important to note that the legal profession might experience other elements of occupational
and psychological distress. Secondary trauma is merely one possible difficulty within a
greater context.
Future researchAs this is a relatively understudied area, the possibilities for future research are enormous.
Future research would benefit from greater consensus on what constitutes professional
distress, where conceptual clarification would have an impact beyond exploration of legal
professions. As it follows, psychometric instruments would also benefit from comparative
analyses as well as conceptual clarification and target groups.
Clear articles with conventional research structures could contribute to academic
professionals giving greater attention to this vital subject. Research would also benefit from
the development of more scientifically robust methods, especially in consideration of
32

vocational control groups. Addressing the aforementioned methodological weaknesses could
contribute to more scientifically precise findings. Partly, this would include diversifying
sampling methodology and addressing non-responders. Moreover, the sources of participants
are only recruited in Australia and Northern America, in countries subject to an adversarial
jurisdictional system. Potentially examining European inquisitorial systems would elucidate
the topic further.
The ten selected articles comprised several professions with differences that could
benefit from further consideration of the topic of secondary trauma. Lawyers and judges in
criminal, asylum and immigration law might be more exposed to traumatised individuals
compared to other areas of the law. Also, it would be useful to examine how judges’
responsibilities of making rulings and decisions, seemingly without the influence of emotions,
relationships or other factors, are potentially influenced by moral distress and secondary
trauma.
Given an over-emphasis on potential predictive and associated factors located in
individual vulnerability, future developments could focus on factors underpinning resilience
as well as deficits, organisational and training contexts, which feature in understanding
professional distress in other professions (Greinacher et al., 2019; MacEachern et al., 2011).
Within this, there are several possibilities of experimental designs examining the
implementation of organisational changes, peer support or coping strategies.
ConclusionsThis review is the first to provide collated information from a systematic literature search
regarding secondary trauma prevalence, predictors and associated factors in the legal
profession. The results indicated a high prevalence of secondary trauma within this
population. It also emphasised the importance of further exploration regarding predictors of
secondary trauma and suggested improvements for future research. As such, this article
highlights the potential risk of indirect exposure to trauma in legal professions. However,
considering the small number of articles and poor quality of research the findings are subject
to great scrutiny and should be interpreted with caution. Therefore, this review emphasises the
need for more scientifically robust research on this topic.
33

ReferencesReviewed articles are marked with an asterisk (*)
ABA, American Bar Association (2018). A current glance at women in the law, Chicago:
American Bar Association. Available via
https://www.nyipla.org/images/nyipla/Programs/2018December6/
acurrentglanceatwomeninthelawjan2018.pdf Retrieved 23 March 2020
American Psychiatric Association (2013). Diagnostic and statistical manual of mental
disorders (DSM-5®). American Psychiatric Pub.
Baird & Kracen (2006). Vicarious traumatization and secondary traumatic stress: A research
synthesis. Counselling Psychology Quarterly, 19(2), 181-188
Booth, A., Clarke, M., Dooley, G., et al. (2012). The nuts and bolts of PROSPERO: an
international prospective register of systematic reviews. Systematic
Reviews, 1(1), 2.
Canfield, J. (2005). Secondary traumatization, burnout, and vicarious traumatization: A
review of the literature as it relates to therapists who treat trauma. Smith College
Studies in Social Work, 75(2), 81-101.
Collins, S., & Long, A. (2003). Working with the psychological effects of trauma:
consequences for mental health‐care workers–a literature review. Journal of
Psychiatric and Mental Health Nursing, 10(4), 417-424.
Downes, M. J., Brennan, M. L., Williams, H. C. & Dean, R. S. (2016). Development of a
critical appraisal tool to assess the quality of cross-sectional studies (axis). BMJ
Open, 6(12). 10.1136/bmjopen-2016-011458
Elwood, L. S., Mott, J., Lohr, J. M., & Galovski, T. E. (2011). Secondary traumasymptoms in
clinicians: A critical review of the construct, specificity, andbimplications for
trauma focused treatment. Clinical Psychology Review, 31(1), 25-36.
Figley (1995) Compassion Fatigue: Coping With Secondary Traumatic Stress Disorder In
Those Who Treat The Traumatized. Routledge, New York NY
FLSC; Federation of Law Societies of Canada (2017). Membership 2017 Statistical
report of the Federation of Law Societies of Canada. Ottawa: FLSC Available via
https://flsc.ca/wp-content/uploads/2019/04/2017-Stats-Report.pdf Retrieved 23 March
2020
Greinacher, A., Derezza-Greeven, C., Herzog, W., & Nikendei, C. (2019). Secondary
traumatization in first responders: a systematic review. European Journal of
Psychotraumatology, 10(1), 1562840.
34
*Jaffe, P., Crooks, C., Dunford-Jackson, B., & Town, J. (2003). Vicarious trauma in
judges:The personal challenge of dispensing justice. Juvenile & Family Court
Journal, 54(4), 1-9.
James, C. (2020). Towards trauma-informed legal practice: a review. Psychiatry,Psychology
and Law, 1-25.
Kiss, R., Schedler, S. & Muehlbauer, T. (2018). Associations between types of balance
performance in healthy individuals across the lifespan: A systematic review and meta-
analysis. Frontiers in Physiology, 9, (1366-1366). 10.3389/fphys.2018.01366
Koenen, K. C., Ratanatharathorn, A., Ng, L., et al. (2017). Posttraumatic stress disorder in the
world mental health surveys. Psychological Medicine, 47(13), 2260-2274.
Krill, P. R., Johnson, R., & Albert, L. (2016). The prevalence of substance use and other
mental health concerns among American attorneys. Journal of Addiction
Medicine, 10(1), 46.
*Leclerc, M. E., Wemmers, J. A., & Brunet, A. (2019). The unseen cost of justice: post-
traumatic stress symptoms in Canadian lawyers. Psychology, Crime & Law,
21(1).
*Levin, A. & Greisberg, S. (2003) Vicarious trauma in attorneys. Pace Law
Review, 24(11), 245-252.
Lonergan, M., Leclerc, M. È., Descamps, et al. (2016). Prevalence and severity of
trauma and stressor-related symptoms among jurors: A review. Journal of
Criminal Justice, 47, 51-61.
*Lustig, S., Delucchi, K., Tennakoon, L. et al. (2008). Burnout and stress among United
States immigration judges. Benders Immigration Bulletin, 13, 22-30.
MacEachern, A. D., Jindal-Snape, D., & Jackson, S. (2011). Child abuse investigation:
police officers and secondary traumatic stress. International Journal of
Occupational Safety and Ergonomics, 17(4), 329-339.
*Maguire, G., & Byrne, M. K. (2017). The law is not as blind as it seems: Relative rates of
vicarious trauma among lawyers and mental health professionals. Psychiatry,
Psychology and Law, 24(2), 233-243.
Maslach, C., & Jackson, S. E. (1981). The measurement of experienced burnout. Journal of
Organizational Behavior, 2(2), 99-113.
Maslach, C., Jackson, S. E., & Leiter, M. P. (1996). Maslach Burnout Inventory. 3rd ed. Palo
Alto, CA: Consulting Psychologists Press.
35

McFadden, P., Campbell, A., & Taylor, B. (2014). Resilience and burnout in child
protection social work: Individual and organisational themes from a systematic
literature review. The British Journal of Social Work, 45(5), 1546-1563.
Miller, M. K., & Bornstein, B. H. (2004). Juror stress: Causes and interventions. T.
Marshall L. Rev., 30, 237.
*Miller, M. K., Reichert, J., Bornstein, B. H., & Shulman, G. (2018). Judicial stress: the roles
of gender and social support. Psychiatry, Psychology and Law, 25(4), 602- 618.
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for
systematic reviews and meta-analyses: the PRISMA statement. Annals of Internal
Medicine, 151(4), 264-269
Najjar, N., Davis, L W., Beck-Coon, K. & Doebbeling, C.C. (2009). Compassion
fatigue: A Review of the Research to Date and Relevance to Cancer-CareProviders.
Journal of Health Psychology, 14(2), 267-277
Nolte, A. G., Downing, C., Temane, A., & Hastings‐Tolsma, M. (2017). Compassion
fatigue in nurses: A metasynthesis. Journal of Clinical Nursing, 26(23-24), 4364-4378.
LSNSW; the Law Society of New South Wales (2016) NSW Profile of solicitors 2016 Final
report. Sydney: Urbis Pty Ltd Available via: https://www.lawsociety.com.au/sites
/default/files/201804/ NSW%20PROFILE%20OF%20SOLICITORS%202016%
20FINAL%20REPORT.pdf Retrieved 23 March 2020
Parker, C. (2014). The Moral Panic over Psychological Wellbeing in the Legal Profession: A
Personal or Political Ethical Response. UNSW Law Journal, 37, 1103.
Pearlman, L. A., & Saakvitne, K. (1995). Trauma and the Therapist: Countertransference
and vicarious traumatization in psychotherapy with incest survivors. New York: W.W.
Norton
*Piwowarczyk, L., Ignatius, S., Crosby, S. et al. (2009). Secondary trauma in asylum
lawyers. Benders Immigration Bulletin, 14(5), 1-9.
Sabo, B. M. (2006). Compassion fatigue and nursing work: can we accurately capture
The consequences of caring work? International Journal of Nursing Practice.
12(3), 136-142.
Santos, C. M. D. C., Pimenta, C. A. D. M., & Nobre, M. R. C. (2007). The PICOstrategy for
the research question construction and evidence search. Revista Latino-Americana de
Enfermagem, 15(3), 508-511.
36
*Schrever, D., Sourdin, T. & Hulbert, C.A. (2019). The psychological impact of Judicial
Work: Australia’s first empirical research measuring judicial stress and wellbeing.
Journal of Judicial Administration, 28(3)
Stamm, B. H. (2010). The concise ProQOL manual, 2nd ed. Pocatello, ID: ProQOL.org.
*Vrklevski, L. P., & Franklin, J. (2008). Vicarious trauma: The impact on solicitors of
exposure to traumatic material. Traumatology, 14(1), 106-118.
Wong, J. N., McAuley, E. & Trinh, L. (2018). Physical activity programming and counselling
preferences among cancer survivors: A systematic review. International Journal of
Behavioral Nutrition and Physical Activity, 15(1), 48. 10.1186/s12966-018-0680-6
Yang, Y. H. & Kim, J. K. (2012). A literature review of compassion fatigue in
nursing. Korean Journal of Adult Nursing, 24(1), 38-51.
37

Section Two: Main research report
Empathy, resilience and distress in Norwegian and English investigative interviewers.
Target journal: Investigative Interviewing: Research and Practice (II-RP)
See Appendix F for author guidelines
Presented here using BPS Style guidelines.
38

AbstractBackground: Police officers working in investigative interviewing can be exposed to
traumatogenic material through their work. Indirect trauma through occupational exposure is
presented here as compassion fatigue, which proposes adverse effects through empathetic
engagement with traumatised individuals. The current study aims to examine associated
factors, predictors and levels of compassion fatigue and satisfaction. The study also explored
the moderating/mediating relationship of empathy between suggested variables and
compassion fatigue.
Methods: The study used a cross-sectional survey-design of UK and Norwegian police forces.
Results: Levels of distress were reported as low/moderate in the both the UK and Norwegian
participant group, but were also comparatively higher than reported community norms.
Compassion fatigue correlated with measures of psychological distress but did not show a
relationship with empathy.
Discussion: Empathy was not found to be a mediating factor in compassion fatigue, and
further research is required to understand the role of empathy, factors influencing wellbeing,
and strategies to counter distress. Findings suggest that supportive organisational strategies
should be offered to police interviewers, in order to maintain resilience to sustain them in key
roles to aid the vulnerable and secure prosecutions.
39

IntroductionOver the last two decades, there has been an increasing awareness of the potentially adverse
impacts of working with vulnerable clients in social and healthcare professions. This has been
variously described under the rubric of “the cost of caring” (Figley, 1995), and is argued to
occur as a result of listening to another person’s traumatic experiences. The effects of such
indirect exposure to trauma appears to be related to emotional engagement with affect-laden
content and client distress.
Certain professions routinely exposed to others’ trauma and suffering have been
identified as particularly vulnerable to occupational distress, notably nurses (Yang & Kim,
2012), mental health professionals (Collins & Long, 2003), therapists (Canfield, 2005) and
social workers (McFadden et al., 2014). Staff in non-therapeutic professions have been
relatively understudied. However, more recently, those undertaking policing roles have been
identified as a similarly vulnerable professional group (Andersen & Papazoglou, 2015).
Whilst police themselves would accept that stress is an inevitable part of the work for which
they are responsible, and that the distress they experience may be manageable and indeed
forge resilience (Kronenberg et al., 2008), it has been increasingly recognised that front line
police officers can be adversely by their work (MacEachern et al., 2010).
Police officers exercising the law through diverse duties are frequently exposed to
traumatogenic events, material and discourse; they may experience and be witness to actual,
or consequences of violent crime, exploitation of the vulnerable, and fatalities (Cross &
Ashley, 2004; Karlsson & Christianson, 2003). They may also experience moral injury if a
lack of resources in the wider judicial system means they are unable to affect legal processes
(Papazoglou et al., 2019).
Akin to therapeutic engagement with traumatised clients, building rapport is an
essential yet often unexamined element of police work, which might engender indirect
trauma. Through the process of investigation, police are regularly and repeatedly tasked with
collecting information from distressed and traumatised victims and witnesses, through
specific methods known as investigative interviewing.
Investigative interviewingInvestigative interviewing is a core duty for police officers in the UK and in other European
countries who investigate alleged crime – in roles such as ‘detective’ and ‘specialist
interviewer’. Investigative interviewing is arguably the most crucial aspect of any criminal
investigation as it seeks to elicit information from witnesses, victims, and suspects that is
40

essential to successful case resolution (Milne & Bull, 1999; Lassiter, 2004). The purpose of
these interviews is to provide an ethical, research-based and non-coercive method of
questioning witnesses and suspects. Through specific methods, such as cognitive
interviewing, the investigators aim to maximise relevant and detailed information, while
minimising bias and contamination of evidence (Bull, 2014; College of Policing, 2019). This
is achieved through adhering to specific protocols including: planning and preparation;
engaging and explaining; account clarification and challenging; closure; and evaluation.
These elements feature in the PEACE model, used by UK investigative interviewers, and
adopted by the other countries’ police forces (McGurk et al., 1993; Milne & Bull, 1999).
Notably, the Norwegian Police University College (NPUC) invited English police staff and
researchers to share their expertise on the PEACE-model, which is presently being utilised
across Norwegian police districts under the acronym KREATIV (Bruusgard et al., 2013).
Critical to extracting detailed evidence through the interview is the need to build
rapport and engage empathically with an interviewee. The purpose of investigative
interviewing is not to mitigate trauma necessarily, but to aim for accuracy and reliability.
Specific guidance is provided for sensitivity training when interviewing witnesses and
suspects. Additional interview training is required for interviewing vulnerable adults or
children, with an emphasis on engagement with the interviewee and eliciting information
(College of Policing, 2019). However, these guidelines do not appear to consider interviewer
needs, with little attention given to the potential effects of engagement with distressed
interviewees and distressing testimony through the interview process.
Conceptual framing of occupational distressUnderstanding how investigative interviewing may potentiate indirect trauma requires
consideration of the constructs which currently describe such phenomena; variously termed as
Post-traumatic Stress Disorder (PTSD), Burnout, Vicarious Trauma, Secondary Traumatic
Stress (STS) and Compassion Fatigue (CF). Najjar et al. (2009) stated that these terminologies
have significant similarities, emerging through empathic emotional engagement with clients,
though there are also noteworthy differences. Due to the difficulties defining and measuring
the different concepts adequately, the literature can be inconsistent in application of the terms
(Elwood et al., 2011). Currently, CF seems to be the most utilised and appropriate concept in
research into the impact of working in law enforcement as a result of exposure to others’
distress.
41
CF, the most recently developed term, describes the potential for experiencing trauma
through learning about the traumatising experiences of others and manifests as a form of
emotional and physical exhaustion (Figley, 1995). The term was used interchangeably with
STS, until it was redefined to include both STS and elements of burnout (Stamm, 2010),
making CF the most inclusive of the different concepts. STS itself encompasses PTSD like
symptoms (Figley, 1995) including avoidance, arousal and intrusion, as well as fatigue,
physical pain, withdrawal and disturbed sleep (Nolte et al., 2017). Burnout, a form of
occupational exhaustion from sustained intense emotional engagement (Maslach & Jackson,
1981; Maslach et al., 1996), presents through exhaustion, depersonalisation, reduced personal
accomplishment and cynicism. Within Stamm’s model, it follows that indirect exposure to
traumatic content might lead to physical and emotional exhaustion and reduced empathetic
capacity (Elwood et al., 2011; Evces, 2015).
ResilienceAlthough police interviewers remain in their post for sustained periods (Crawford et al.,
2017), their responses to their work also appear to be positive. Constructs such as compassion
satisfaction (CS; Stamm, 2002), posttraumatic growth (Arnold et al., 2005) or resilience
(Hernández et al., 2007) may be helpful to understand their experiences. CS (Stamm, 2002)
describes the gaining of pleasure or satisfaction accumulated through working in helping
professions. As a model, CF-CS provides a way of conceptualising occupational distress and
resilience together.
Resilience in policing is relatively underexplored, but both individual and
organisational measures have been proposed to build resistance. Supportive occupational
provision such as supervision, peer support and counselling (Figley, 1995) are argued to
mitigate the combination of high psychological demands, low control in decision-making and
limited social support that are associated with exhaustion (Evans et al., 2006).
Empathy and distressInvestigative interviewing requires professional skills which, along with empathetic
sensitivity, can ease and facilitate an interview. The capacity to understand or feel another’s
experience (Goubert et al., 2005) is needed to navigate a witness’ emotional presentation and
build an effective, trusting relationship (Mathieu, 2007; Risan et al., 2016). This is
challenging for interviewers in a culture where outward resilience is cultivated, emotional
responses are often diminished and caseloads are high (Hanway & Akehurst, 2018); little is
known about the impact of sustained empathic engagement in this role.
42

Empathy appears central in regulating adverse indirect effects of trauma exposure
(Figley, 1995); however, its precise role is unclear. Empathic concern has predicted elevated
CF in oncology nurses (Duarte et al., 2016), which is consistent with Figley’s suggestion that
sensibility to others’ suffering may be a vulnerability in the development of CF. Hunt et al.’s
(2017) review of burnout, STS and empathy in nursing suggested that the relationship
between these constructs are complicated, and an ability to self-regulate emotions during
empathic engagement may reduce the risk of burnout. In only one published study of police
officers, specialist officers working with those alleging rape (Turgoose et al., 2017) revealed
no relationship between empathy and CF or STS, but that trait empathy predicted elevated
burnout. The role of empathy appears to warrant further investigation. There is recognised
need to examine the effects of investigative interviewing on the interviewer as well as
examining the levels of support police officers have available to them (Hanway & Akehurst,
2018).
AimsGiven the nature of the work undertaken by investigative interviewers and likely exposure to
traumatogenic material, this study aimed to describe emotional responses to work (CF-CS) for
police officers undertaking this role. Since investigative interviewing principles are generally
agreed upon internationally, but implementing them has proven to be problematic, it was
decided that officers’ responses would be examined in two nations (the UK and Norway) in
which investigative interviewers adopt similar roles and principles in interviewing. Given
known predictors of CF, and an aim to examine the role of empathic engagement in
investigative interviewing, this study hoped to investigate the relationship between empathy,
distress and resilience within these populations alongside demographic factors associated with
occupational distress in other professional groups. This report aimed to provide a particular
focus on the mediating/moderating role of empathy. Since the developed terminology on
potentially distressing facets of work are variously defined, this study used the CF-CS model,
which includes STS, burnout and CS (Stamm, 2010), to capture the phenomenon in
investigative interviewers, as a term of occupational distress and resilience.
Research questions:
1. What are the levels of distress and resilience (CF/CS) reported by investigative
interviewers in Norway and the UK?
2. What factors are associated with reported distress and resilience?
3. To what extent do associated factors predict reported distress and resilience?
43
4. Does reported empathy moderate/mediate the relationship with CS/CF and proposed
predictor variables in investigative interviewers?
MethodResearch designThe current study utilised a quantitative cross-sectional survey design to examine reported
levels of distress and resilience in investigative interviewers from police forces in the UK and
Norway. Furthermore, the study examined factors and predictors of CS and CF, as well the
level to which empathy was related to the variables. The specific dependent variables
comprised CS, STS and burnout, with the independent variables being gender, age, tenure in
post, empathy, psychological distress (anxiety and depression) and perceived organisational
support (POS).
Ethical approvalsThe University of Leicester Ethics Sub-committee of Psychology granted ethical approval in
May 2019, following both peer and service user reviews (Appendix G). In Norway, ethics
approval was gained from the Regional Committees for Medical and Health Research Ethics
(REC) in September 2019 (Appendix H), and the National Police Directorate (subordinate to
the Ministry of Justice and Public Security).
ParticipantsInclusion criteria for participants were similar for recruitment in the UK and Norway. All
participants were currently employed in the public service as detectives or specialist
interviewers, undertaking the role of investigative interviewing. The roles encompassed
similar tasks in both countries, with specialist interviewers needing additional training for
interviewing vulnerable populations. Having specialist training, or additional interview
training did not exclude participants. Through their respective Colleges of Policing, both UK
and Norwegian participants had received training on completing witness assessment during
investigative interviewing, and cognitive interviewing techniques. Recruitment took place
from police constabularies of varying sizes, and from districts in various geographical areas in
UK and Norway.
RecruitmentThe method of recruitment was convenience sampling, over a period of six months (October
2019 to April 2020). All recruitment information specified that participants should be working
in the role of ‘investigative interviewer’. In the UK, police forces of differing sizes who
44

employed investigative interviewers were approached via gatekeepers in national
investigative resourcing who publicised access to an online questionnaire in the UK. In
Norway, recruitment was coordinated with a researcher from the Norwegian University of
Science and Technology (NTNU) and the STrESOB project, who advertised the project
during a national police conference and distributed printed paper questionnaires to the police
districts who agreed to participate. The STrESOB project involves Norwegian national
research aimed at preventing CF in detectives and specialist interviewers who work with child
sexual abuse.
ProcedureIn the UK, gatekeepers distributed e-mail invitations to complete an online questionnaire. The
e-mail included a participant information sheet (Appendix I), a questionnaire link and
password to access the questionnaire. Whilst the researcher had no direct contact with
participants, all potential participants were provided with the principal investigator’s contact
details should they have additional questions or wanted a summary of findings. Consent was
collected within the online questionnaire, in addition to the assumed consent from
questionnaire completion.
In Norway, questionnaires were sent to districts who had agreed to participate in the
study. Each printed questionnaire also provided stamped and addressed envelopes ready to be
sent to NTNU, participant information sheets and consent forms. The associate Norwegian
researcher had no direct contact with participants.
MeasuresThe questionnaire was prefaced by a privacy/consent declaration (Appendix J). To capture
key variables of interest the questionnaire comprised questions relating to demographic
variables (gender, age, ethnicity, work tenure and level of interview training). Four validated
tools were included (Appendix K) to assess psychological wellbeing, empathy, POS, and CF-
CS. These were selected because of suitability to the research questions, their statistical
properties and availability in both English and Norwegian.
CF-CS
The Professional Quality of Life Compassion and Satisfaction Subscale v5 (ProQOL; Stamm,
2010) is a 30-item questionnaire assessing CS, STS and burnout, and has previously been
used with police officers (Greinacher et al., 2019). It employs a five-point Likert scale
measuring frequency from “never” to “very often”, creating scores of 1-5 for each of ten
questions relating to the assessed variables. Each item which included the identifier as
45
“helper” was changed to consider the investigative interviewing role, fitting more with the
identification of the participant group. Scores are calculated individually for each domain,
with higher scores suggesting higher levels of CS, STS or burnout. Respondents’ scores were
categorised via the self-score methods offered within the ProQOL manual, such that STS,
burnout and CS were categorised as low, average or high.
Stamm (2010) argues the measure shows good construct validity given the number of
published articles utilising the measure. Moreover, within the CF scale, inter-scale
correlations indicated two per cent shared variance (r=-.23) with STS and five per cent shared
variance (r=-.14) with burnout. In 2005, Internal reliability appears high; Cronbach’s α in CS
(α=.87), burnout (α=.72) and STS (α=.80; Stamm, 2010). Watts and Robertson (2015)
suggested supporting the measure with reliable and valid psychometrics, such as the Hospital
Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983).
Psychological wellbeing
The Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) is a 14-item
questionnaire assessing anxiety and depression reported over the preceding seven days. Both
dimensions are assessed through seven questions (14 in total) via a Likert scale scored 0-3.
Higher scores indicate greater levels of distress, with a maximum score of 21 for each
dimension. A dimension score of 11 or above is considered ‘abnormal’ scores according to
the authors, and indicated clinically elevated depression or anxiety, also called clinical
caseness. Bjelland et al. (2002) demonstrated good construct and convergent validity, and
concluded that the HADS performed well when assessing severity and caseness for both
anxiety and depression in the general population. The scores do not automatically infer an
official diagnosis when it is considered without a psychiatric opinion (Silverstone, 1994).
A Norwegian validation review (Leiknes et al., 2016) reported high internal validity
(α>.70). Construct validity was shown in several factor analysis studies, most of them
supporting the two categories. Convergent validity was demonstrated when compared with
the Montgomery-Aasberg Depression Rating Scale, correlating at moderate to high level on
emotional content items. Correlation between GHQ and HADS-D was moderate (Cohen’s
k=0.37, Pearson’s r=0.69, p>.001) and HADS-A was moderate to good (Cohen’s k=0.41,
Pearson’s r=0.69). HADS was chosen as a mental health questionnaire that showed great
statistical properties in both languages and has been recommended by Watts and Robertson
(2010) to support the ProQOL measure.
Empathy
46
The Cambridge Behaviour Scale – Empathy Quotient (EQ; Baron-Cohen & Wheelwright,
2004) short version is a 40-item self-report questionnaire containing items assessing both
cognitive and emotional components of empathy. The questionnaire offers four potential
responses to items (two of which are scored as 0) calculating scores from a range of 0-2, with
higher scores indicating higher levels of empathy. Scores of 0-32 indicate lower than average
empathy, 33-52 average, 53-63 above average, and 64-80 very high empathy.
The EQ has demonstrated face validity (Baron-Cohen & Wheelwright, 2004) and
concurrent validity between the subscales “empathetic concern” and “perspective-taking”
within the Interpersonal Reactivity Index, and they also showed good psychometric properties
of internal and test–re-test reliability (Lawrence et al., 2004).
Perceived Organisational Support
The Survey of Perceived Organisational Support (SPOS; Eisenberger et al., 1986;
Eisenberger, 2019) is a 36-item questionnaire assessing POS. It employs a seven-point Likert
scale capturing agreement with statements (strongly disagree 0 to strongly agree 6). Higher
scores indicate higher POS. Sixteen items, eight-item and three-item scales are also available
for a shorter form versions. The survey is unidimensional, examining elements of POS. The
present survey used the eight-item scale.
Shore and Tetrick (1991) demonstrated the construct validity of the SPOS, showing
that the survey was distinguishable from affective and continuance organisational
commitment. The results also supported the claim of the SPOS as a unidimensional scale. A
reliability analysis indicated good internal consistency (α=0.81) and item-total correlations
ranging from 0.64-0.67 (Worley et al., 2009).
Data analysisIBM/SPSSS Statistics version 26 was used for statistical analyses, analysis of missing data
(Appendix L) and evaluation of assumptions for each of the analyses (Appendix M and N).
To examine levels of distress and resilience between the Norwegian and the UK sample, five
independent t-tests were completed to compare means between groups for the CS, STS,
burnout, empathy, and POS. Following evaluation of assumptions, burnout and CS failed to
meet assumptions, and therefore non-parametric Mann-Whitney U analyses were conducted.
Given the multiple analyses undertaken, p-values were set and interpreted more stringently at
p<.01 (Perneger, 1998).
Bootstrapped single sample t-tests were conducted to compare sample means with
population norm data. Normative studies were used for the ProQOL (De La Rosa et al., 2018)
47
and the HADS for English (Crawford et al., 2001) and Norwegian (Leiknes et al., 2016)
population data. To examine the differences in caseness for anxiety and depression between
the Norwegian and UK participant group, two chi-square analyses were performed. Caseness
was indicated by number of participants who scored over 11 for the anxiety and depression
scores in the HADS.
Spearman’s Rho was applied to the whole sample (N=92) to examine what variables
were significantly associated with occupational distress and resilience. Ten variables were
explores using a correlation analysis, and as such a more stringent p-value was used a p<.01.
Moreover, p-values are also presented with Bonferroni corrections at p<.005.
Regression analyses were performed with the significant correlates as predictors for
the three outcome variables; CS, STS and burnout. Anticipated mediation analyses to explore
the role of empathy were not undertaken, based on the small sample size, the results from the
regression analyses and correlation results.
Missing dataThe sample (N=92) had a low rate of missing data (0.29 per cent) with <5 per cent of data
missing for any individual case, except for gender, missing 6.5 per cent of the items. A total
of 18 data points were missing for outcome variables and seven data points were missing for
demographic items, mainly gender (N=6). The Little’s Missing Completely at Random
(MCAR) test showed that data for each variable were missing randomly χ2(1192, N=92) =
1117.379, p = .939. To address missing categorical gender data, this was treated as a separate
category for analysis (Appendix L).
The remaining outcome data comprised fewer than two percent of items missing
within less than 15 per cent of the data. All missing items in the outcome variables were
imputed using the median score of each questionnaire item. Imputed data was used in all
subsequent analyses. This method was chosen over complete case analysis to preserve
variability of data and statistical power. Given the small proportions of missing data and
random distribution of missing scores it is unlikely that the imputation will significantly affect
variance or statistical power.
Prospective Power and sample size analysisG*Power 3.1 software (Faul et al., 2007) was used to conduct a power analysis for a linear
multiple regression fixed model, with an estimated medium effect size (f2= .15). The results
indicated that a sample of 103 participants were required for a regression analysis with
possible seven predictors (power=0.80, α=.05).
48

ResultsRespondentsThe survey software identified that 49 UK respondents clicked on the hyperlink. From these
respondents, 32 completed the survey (65 per cent), indicating that the hyperlink was pressed
17 times without the participant proceeding to complete the questionnaire. No participants
were excluded as all fit the inclusion criteria, and all participants checked all items on the
privacy and consent form. A final convenience sample of 32 participants were eligible. Sixty
respondents were obtained from the Norwegian police services, from 110 questionnaires
issued, indicating a response rate of 54.5 per cent.
Test of reliabilityThree variables were shown to have acceptable levels and two of the variables had good
levels of internal consistency (Table 3). One measure showed poor internal consistency values
of α=.57 (SPOS), suggesting that the items in the questionnaire may not be measuring the
same construct.
Table 3.
Reliability analysis with Cronbach’s alpha values for each of the measures, and subtests.
Measure Internal consistency Cronbach’s alpha
ProQOL (30 items) Acceptable α=.678.
CS (10 items) Good α=.883
STS (10 items) Good α=.804
Burnout (10 items) Acceptable α=.616
HADS (14 items) Acceptable α=.724
Anxiety (7 items) Acceptable α=.631
Depression (7items) Acceptable α=.671
EQ (40 items) Good α=.853
SPOS (8 items) Poor α=.57
DemographicsStatistical analyses were performed on descriptive data between the UK and Norwegian
participant group (Table 4). Chi-square tests of independence compared UK and Norwegian
samples for gender revealing no significant difference in gender distribution (X2(1, N=85)
=1.312, p=.252, ϕ =.12). The missing gender data did not significantly differ from the data
reported as male or female (Appendix L). Furthermore, the Norwegian participants were
49

younger, when comparing those over 40, with those under 40 (X2(1, N=92) =5.6135, p=.018,
ϕ =.25). A further chi-square indicated that the UK population reported a significantly greater
attainment of further training to work with vulnerable clients (X2(1, N=91) =10.743, p=.001, ϕ
=.34). A Mann-Whitney U test indicated that the UK population (Mdn=16.00) had
significantly lengthier tenure at work, compared to the Norwegian population (Mdn=9.00),
U=467.000, p<.001.
Table 4.
Sample characteristics of the UK and the Norwegian populations.
UK (N=32) Norway (N=60)
Gender
N % N %
Female 13 40.6 17 28.3
Male 17 53.1 38 63.3
Prefer not to say 1 3.1 - -
Missing data 1 3.1 5 8.3
Age
N % N %
18-29 2 6.3 23 38.3
30-39 10 31.3 15 25
40-49 13 40.6 16 26.7
50-59 7 21.9 6 10
60+ - - - -
Interview training for vulnerable populations
N % N %
Yes 26 81.3 27 45
No 6 18.8 32 53.3
Missing - - 1 1.7
Tenure in post (years)
M SD M SD
18 7.18 10.87 8.90
What levels of distress and resilience (CF/CS) are reported by investigative interviewersin Norway and the UK?
50
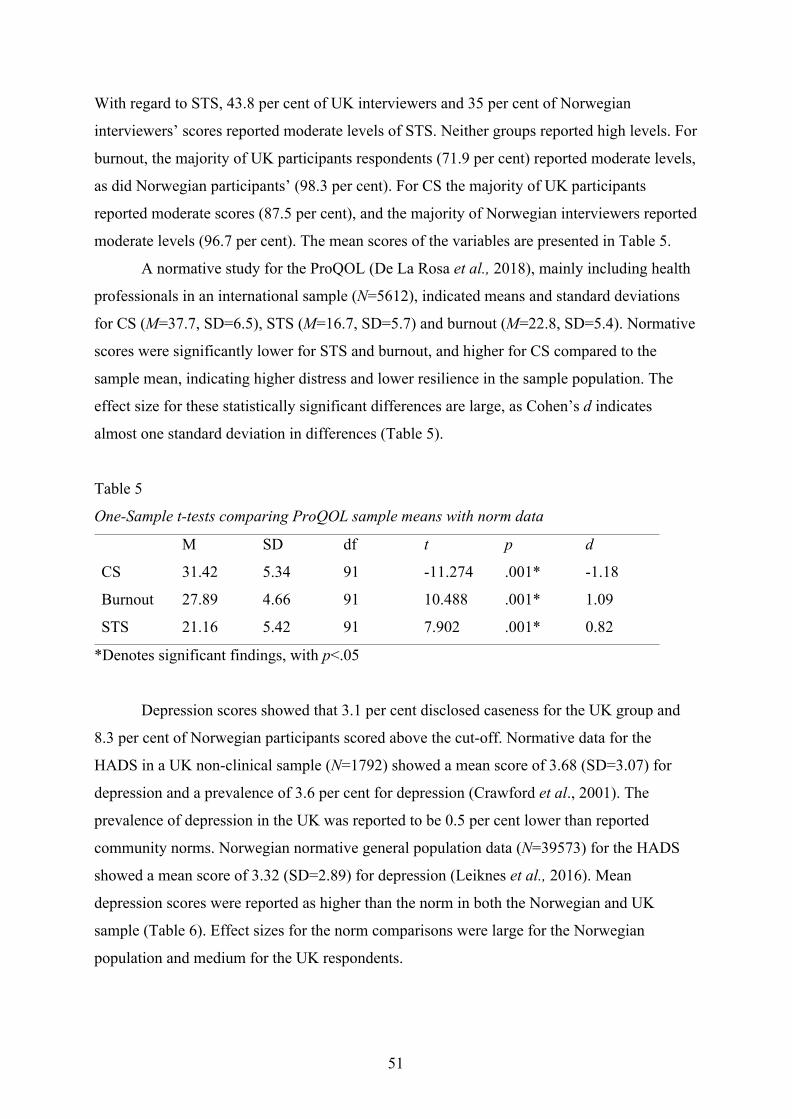
With regard to STS, 43.8 per cent of UK interviewers and 35 per cent of Norwegian
interviewers’ scores reported moderate levels of STS. Neither groups reported high levels. For
burnout, the majority of UK participants respondents (71.9 per cent) reported moderate levels,
as did Norwegian participants’ (98.3 per cent). For CS the majority of UK participants
reported moderate scores (87.5 per cent), and the majority of Norwegian interviewers reported
moderate levels (96.7 per cent). The mean scores of the variables are presented in Table 5.
A normative study for the ProQOL (De La Rosa et al., 2018), mainly including health
professionals in an international sample (N=5612), indicated means and standard deviations
for CS (M=37.7, SD=6.5), STS (M=16.7, SD=5.7) and burnout (M=22.8, SD=5.4). Normative
scores were significantly lower for STS and burnout, and higher for CS compared to the
sample mean, indicating higher distress and lower resilience in the sample population. The
effect size for these statistically significant differences are large, as Cohen’s d indicates
almost one standard deviation in differences (Table 5).
Table 5
One-Sample t-tests comparing ProQOL sample means with norm data
M SD df t p d
CS 31.42 5.34 91 -11.274 .001* -1.18
Burnout 27.89 4.66 91 10.488 .001* 1.09
STS 21.16 5.42 91 7.902 .001* 0.82
*Denotes significant findings, with p<.05
Depression scores showed that 3.1 per cent disclosed caseness for the UK group and
8.3 per cent of Norwegian participants scored above the cut-off. Normative data for the
HADS in a UK non-clinical sample (N=1792) showed a mean score of 3.68 (SD=3.07) for
depression and a prevalence of 3.6 per cent for depression (Crawford et al., 2001). The
prevalence of depression in the UK was reported to be 0.5 per cent lower than reported
community norms. Norwegian normative general population data (N=39573) for the HADS
showed a mean score of 3.32 (SD=2.89) for depression (Leiknes et al., 2016). Mean
depression scores were reported as higher than the norm in both the Norwegian and UK
sample (Table 6). Effect sizes for the norm comparisons were large for the Norwegian
population and medium for the UK respondents.
51

Among the UK participants, there was a 21.9 per cent caseness for anxiety prevalence
and the Norwegian participants scored 16.7 per cent for anxiety caseness. Anxiety normative
data (Crawford et al., 2001) for the UK (N=1792) showed a mean score of 6.14 (SD= 3.76),
and a caseness prevalence of 12.6 per cent for anxiety. Norwegian normative general
population data (N=39277) for the HADS showed a mean score of 4.02 (SD=3.29) for
anxiety, and a prevalence rate of 12.6 per cent was noted in the community norms (Leiknes et
al., 2016). The Norwegian sample anxiety mean were significantly higher than the population
norms. This difference demonstrated a large effect size (Table 6). UK anxiety scores showed
no significant difference between the sample and population means.
Table 6.
One sample t-test for HADS anxiety and depression sample scores compared to UK and
Norwegian population norms
M SD df t p d
Norwegian sample
Anxiety 8.45 2.11 59 16.257 .001* 2.10
Depression 5.09 3.47 59 28.105 .001* 3.63
UK sample
Anxiety 7.16 4.54 31 1.265 .205 0.22
Depression 9.42 1.68 31 2.306 .035* 0.41
*Denotes significant findings, with p<.05
Five between group analyses were performed to examine statistical difference of the
means, with a more stringent alpha-value set at p=.01 (Table 7). Independent samples t-test
were performed for STS, EQ and SPOS as they met assumptions for parametric tests. Neither
STS (t(90=.920, p=.360) nor EQ variables (t(90)=-2.364, p=.020) showed a statistical
significant difference between means the Norwegian and English participant groups (Table 5),
when using the adjusted alpha value. However, Norwegian participants (N=60) reported
significantly higher levels of POS (M=28.77, SD=10.58, t(90)= -2.855, p=.005) than the UK
participant group (N=32, M=22.13, SD=10.72).
Mann-Whitney U test were performed for burnout and CS, as the variables did not
meet assumptions for parametric tests. Comparison between Norwegian (Mdn=47.92) and UK
participants (Mdn=43.84) indicated no statistical difference in CS (U=875.000, p=.485).
52
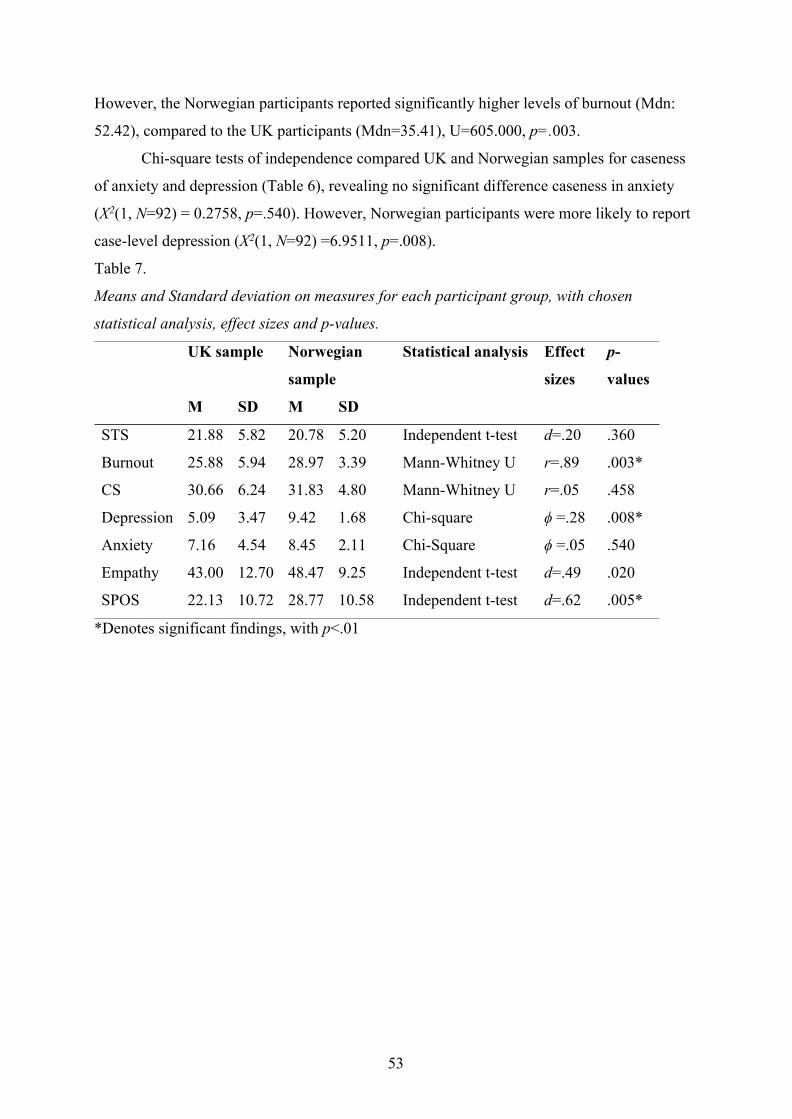
However, the Norwegian participants reported significantly higher levels of burnout (Mdn:
52.42), compared to the UK participants (Mdn=35.41), U=605.000, p=.003.
Chi-square tests of independence compared UK and Norwegian samples for caseness
of anxiety and depression (Table 6), revealing no significant difference caseness in anxiety
(X2(1, N=92) = 0.2758, p=.540). However, Norwegian participants were more likely to report
case-level depression (X2(1, N=92) =6.9511, p=.008).
Table 7.
Means and Standard deviation on measures for each participant group, with chosen
statistical analysis, effect sizes and p-values.
UK sample Norwegian
sample
Statistical analysis Effect
sizes
p-
values
M SD M SD
STS 21.88 5.82 20.78 5.20 Independent t-test d=.20 .360
Burnout 25.88 5.94 28.97 3.39 Mann-Whitney U r=.89 .003*
CS 30.66 6.24 31.83 4.80 Mann-Whitney U r=.05 .458
Depression 5.09 3.47 9.42 1.68 Chi-square ϕ =.28 .008*
Anxiety 7.16 4.54 8.45 2.11 Chi-Square ϕ =.05 .540
Empathy 43.00 12.70 48.47 9.25 Independent t-test d=.49 .020
SPOS 22.13 10.72 28.77 10.58 Independent t-test d=.62 .005*
*Denotes significant findings, with p<.01
53
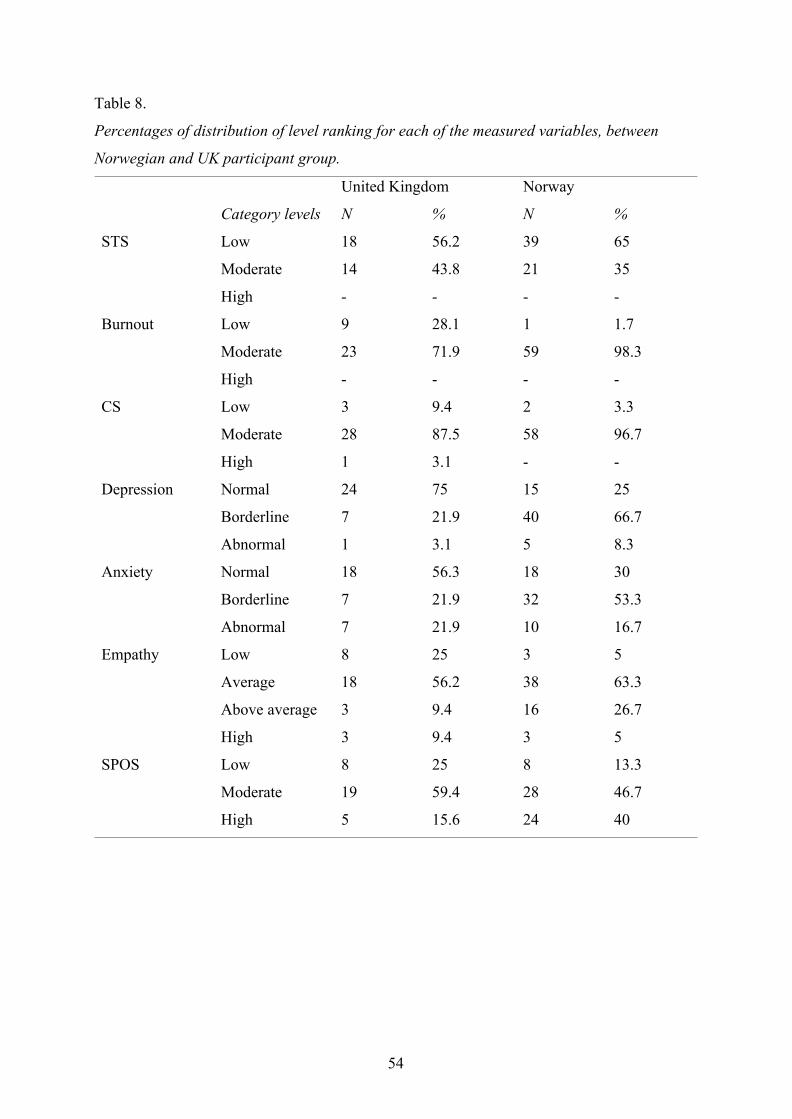
Table 8.
Percentages of distribution of level ranking for each of the measured variables, between
Norwegian and UK participant group.
United Kingdom Norway
Category levels N % N %
STS Low 18 56.2 39 65
Moderate 14 43.8 21 35
High - - - -
Burnout Low 9 28.1 1 1.7
Moderate 23 71.9 59 98.3
High - - - -
CS Low 3 9.4 2 3.3
Moderate 28 87.5 58 96.7
High 1 3.1 - -
Depression Normal 24 75 15 25
Borderline 7 21.9 40 66.7
Abnormal 1 3.1 5 8.3
Anxiety Normal 18 56.3 18 30
Borderline 7 21.9 32 53.3
Abnormal 7 21.9 10 16.7
Empathy Low 8 25 3 5
Average 18 56.2 38 63.3
Above average 3 9.4 16 26.7
High 3 9.4 3 5
SPOS Low 8 25 8 13.3
Moderate 19 59.4 28 46.7
High 5 15.6 24 40
54
What factors are associated with reported distress and resilience?Relationships between ten variables were examined for the entire sample (N=92).
Correlational results for scores on CS, STS, burnout, anxiety, depression, empathy, POS and
participant demographics are presented in Table 9. Gender was found to have no significant
relationship with any of the proposed variables. Age was unsurprisingly significantly related
tenure (r=.90, p<.005) as they are similar constructs.
The three main constructs (CS, STS and burnout) showed some significant
correlations with each other. CS correlated negatively with burnout (r=-.40), but not with
STS. Burnout and STS revealed a strong positive correlation with each other (r=.51, p<.005),
supporting the construct of CF.
When examining how the three main constructs related to other variables, the results
showed that CS also correlated with anxiety (r=-.29, p<.01), empathy (r=.28, p<.01) and POS
(r=.49, p<.005). Burnout significantly correlated with depression (r=.42, p<.005) and anxiety
(r=.47, p<.005), in addition to STS. STS correlated strongly with anxiety (r=.47, p<.005).
Empathy showed no relationship with the CF-constructs, but appeared significantly correlated
with CS (r=.28, p<.01) with a low effect size. Empathy was signiEmpaEmpathy also
correlated significantly with Empathy was also significantly correlatied with POS (r
55

Table 9.
Bivariate non-parametric correlations between ten variables
Gender Age Tenure CS Burnout STS Depression Anxiety Empathy POS
Gender 1
Age .061 1
Tenure .011 .895** 1
CS -.084 .227 .098 1
Burnout .125 -.218 -.246 -.404** 1
STS .017 .002 .020 -.201 .512** 1
Depression -.083 -.203 -.260 -.139 .419** .208 1
Anxiety -.085 -.157 -.123 -.290* .467** .597** -.439** 1
Empathy .132 .010 -.065 .281* .520 -.133 .240 -.047 1
POS .126 -.165 -.278 .491** -.208 -.260 .095 -.241 .244* 1
**Denotes significant correlations at the .005 level (2-tailed).
*Denotes significant correlations at the .01 level (2-tailed).
56
To what extent do noted correlates predict reported distress and resilience?To address this, simultaneous forced entry multiple regression analyses (MRA) and a single
regression analysis were conducted, for each of the dependent variables; STS burnout and CS
with variables previously shown to have a relationship added simultaneously to the MRA.
Results are presented in Table 10 and 11. For STS, a simple linear regression was conducted
to examine the degree to which anxiety predicts STS, revealing a significant equation (F(1,90)
= 52.731, p<.001), with an R2 of .369.
For burnout, a forced entry MRA with anxiety and depression as predictors, revealed a
significant effect of the model (F(2, 89) = 29.769, p<.001) with an R2 of .401. The coefficient
analyses indicated that anxiety (t=4.158, p<.001) and depression (t=3.073, p=.003) were both
significant predictors in the model. Anxiety had the largest unique contribution of the
predictor variables in this model.
For CS a forced entry MRA of anxiety, EQ and POS revealed a significant model
(F(3, 88) =13.318, p<.001), with an R2 of .312. POS (t=4.699, p<.001) was the only
significant predictor in the model.
Does reported empathy moderate/mediate the relationship with CS/CF and proposedpredictor variables in investigative interviewers?Comparative examination of reported empathy (at 75 per cent of the UK sample and 95 per
cent of Norwegian sample reporting average or higher categories on the EQ-scale) revealed
no significant difference. Whilst empathy showed significant positive correlations with CS
(r=.28), no significant relationship was evidenced with either STS or burnout. Moreover,
MRA showed that empathy was not a significant contributor in the CS regression model.
Given this, and a small, underpowered study, model construction via mediation analysis was
not pursued.
57

Table 10.
Simple regression model for STS on anxiety.
Variable Predictor B SEb P R2 change F P R square Adjusted
R2
STS .369 52.731 .000 .369 .362
Anxiety 1.026 .141 .000
Table 11.
Multiple linear regression model of predictors of CS and burnout.
Model Independent
variables
B SEb b’ t P R2 change F P R
square
Adjusted
R2
CS .312 13.318 .000 .312 .289
Anxiety -.293 .153 -.176 -1.914 .059
EQ .066 .045 .133 1.475 .144
SPOS .214 .046 .442 4.699 .000
Burnout .401 29.769 .000 .401 .387
Anxiety .596 .144 .304 3.073 .003
Depression .458 .153 .313 3.001 .004
58
DiscussionThis exploratory study sought to assess the extent of work-related distress and resilience
(measured via STS, burnout and CS) reported by police investigative interviewers
operating in similar systems in Europe (the UK and Norway). The study also examined
significant correlates and predictors of distress and considered empathy as a possible
mediating variable between independent and dependent variables.
Summary of findingsReported levels of CF (STS and burnout) fell within moderate and low categories for
both UK and Norwegian interviewers, with CS also largely reported as moderate. The
findings reveal CF at levels (low to moderate) similar to those reported by police
officers working with rape victims (Turgoose et al., 2017) and first responders
(Greinacher et al., 2019). Nevertheless, comparisons with community norms suggest
that both the UK and Norwegian respondents are disclosing elevated distress, with
higher mean scores in anxiety, depression, STS and burnout. Moreover, levels of
reported CS appeared lower than community norms. Differences showed large effect
sizes when compared to the norms, for the three main constructs and for the Norwegian
participant group’s anxiety and depression scores, compared to the norm population.
Examination between UK and Norwegian interviewers found significant
differences in burnout, caseness for depression and POS. Surprisingly, Norwegian
participants reported higher scores for burnout, despite being a younger group. Burnout
is often understood to arise from cumulative effect, although the group reported mean
time in post exceeding 10 years. However, they also appeared to be younger and have
fewer years in post than their UK counterparts, so this distress may be a manifestation
of less experience or emotional resource to manage the challenge of interviewing.
Although appearing inconsistent with the fact that Norwegian interviewers also reported
higher POS, it may be that whilst Norwegian police officers have supportive measures
and additional training during early years of employment, this is does not necessarily
mitigate distress or impact on individual resilience.
Regarding relationships with distress measures, burnout was significantly related
to wider psychological morbidity, such that higher anxiety and depression correlated
positively. STS was also correlated with anxiety, which is unsurprising given the role of
anxiety in conceptualisation of STS as a trauma reaction. Correlations between burnout
and STS, which show similar correlations with other studies on police (Turgoose et al.,
59
2017), could indicate construct confirmation of CF. Burnout was negatively associated
with CS, indicating that higher burnout levels was associated with lower reported levels
of CS. Empathy and POS were both positive correlates of CS, which was observed in
studies with social work staff (Thomas & Otis, 2010). Contradicting Greinacher et al.
(2019), the current study found no effects of gender. Moreover, this study found no
correlations between CF and CS, which have been suggested to be opposite but related
processes (Stamm, 2010). Perhaps their separateness may help understand why empathy
correlates with CS and not with CF. Linley and Joseph (2007) suggested that for
therapists, CS is not the obverse of CF and they are related to different processes.
Multiple regression analysis significantly explained 31.2 per cent of variance in
CS with three predictors: anxiety; empathy; and POS. POS was the only significant
contributors to variance in the model. In a simple regression model, anxiety was found
to predict 36.9 per cent of STS scores significantly. Finally, a multiple regression
analysis was conducted for burnout, where depression and anxiety were predictors. This
model indicated that 40.1 per cent explained variance in the model. Though the
regression models account for a significant part of variability, the prediction levels also
indicate presence of other explanatory variables. Potentially this could include social
support or alcohol use (Greinacher et al., 2019), different elements of empathy or
mindfulness coping strategies (Thomas & Otis, 2010).
Empathy only showed significant correlation with CS, which within this
underpowered study, deterred pursuing mediation analysis. However, it is notable that
as with the study examining empathy in police interviewers of rape victims (Turgoose et
al. (2017), no relationship was evident with CF. This differs from studies of caring
professions, in which empathy has shown significant association with CF (Duarte et al.,
2016; Wagaman et al., 2015). No significant relationship was found between empathy
and work-related distress, which may reflect the non-therapeutic role of investigative
interviews or that the pragmatically selected measure of empathy (for language reasons)
was insufficient to capture the specific elements of empathy needed to build rapport or
relate to interviewees. As empathy levels seem high within this group, the results may
reflect engagement in emotional suppression against distress, or the measure lacks a
focus on empathy related to the specific skills in investigative interviewing. Potentially,
the methodology of cognitive interviewing techniques and the PEACE model inhibits
the emotional engagement with the work. As Turgoose et al. (2017) has noted, the
60
conceptual model Figley (1995) advances is not clear about what facets of empathy
potentiate CF (Sabo, 2011), so further consideration of how empathy is measured
towards vulnerable witnesses is needed.
Strengths and limitationsThe current study is the first to examine the extent and predictors of work-related
distress and resilience in investigative interviewers, using robust measures amenable to
exploration in two comparable national police services. Indeed selected questionnaires
were given availability and validity for both UK and Norwegian populations.
Despite endorsement and the use of national gatekeepers such as the UK College
of Policing, recruitment in the timeframe was insufficient to power the study fully, and
caution should therefore be exercised in data interpretation. In both UK and Norway
legislatures budgetary cuts have increased pressure on forces such that this study may
have been viewed as of low priority whilst significant job stressors, increased workloads
and limited resources are evident (HMIC, 2012). Low response rate may also be
associated with interviewers’ concerns about social desirability, fear of job loss
(Kronenberg et al., 2008) and reluctance to disclose distress given known covert
cultural pressures to use emotional suppression to cope. Response bias may have been
created by officers’ reluctance to endorse symptoms of a psychological burden, and
electing not to participate. Bias may also have been created through those officers who
felt most distressed by their work having additional motivation to respond to a study
with this focus.
This study did not control for impacts of direct trauma, and as such the levels of
distress might have been impacted by variables unbeknownst to the principle researcher.
However, recruitment methods made sure to target those police officers who are in the
main role of interviewers, and the CF-CS measure was specified to consider the
investigative interviewing role in particular.
ImplicationsPsychological morbidity, in both UK and Norwegian samples, exceeded community
norms for both anxiety and depression, with particularly large effect sizes for the
comparisons with the Norwegian sample. On dimensions of work-related distress, a
considerable proportion of investigative interviewers reported moderate levels of both
STS and burnout, in the UK and Norway; again above community norms and with large
61
effect sizes. There appeared a need to acknowledge that there are significant
psychological challenges inherent in undertaking interviewing of this type, as well as
greater organisational awareness and communication to normalise emotional challenges
and risks of distress from work in this area. There has been awareness that multiple
interviews of this type can be traumatising to witnesses and victims, and addressed via
initiatives such as Barnahus (Haldorsson, 2017). It seems timely to consider parallel
innovations to support staff and to ensure that service to victims through interview
quality is maintained.
Whilst there were some differences between UK and Norwegian samples there
were also consistent findings. The study suggested benefits in examining impacts of
work in similar legislatures offering similar support to witnesses and victims.
Collaborative examination of distress and resilience in policing between nationalities
can facilitate mutual understanding of strengths and weaknesses in procedures, in a
world where international police cooperation is growing.
In addition, this research raises questions regarding organisational resilience
measures and their efficacy, as well as specific coping mechanisms and possible
inherent resilience in those who have chosen a policing career. The results might be
supportive of successful measures aimed to promote good mental health and wellbeing,
though the comparison to community norms still show a higher level of distress in the
sample. The potential links between CF and empathy remain unclear and raises
questions relating to the theoretical background of CF as a construct.
Awareness of the moderate levels of distress, which are greater than community
norms, should encourage further studies and support, particularly with literature
revealing comparable levels of distress (Greinacher et al., 2019; Turgoose et al., 2017).
Addressing police wellbeing in the UK has recently been enhanced through Oscar Kilo
and the Bluelight frameworks (Coleman et al., 2018). To date, the impact of trauma has
prioritised the needs of those officers more obviously exposed to trauma (e.g. through
direct violence to themselves, road traffic fatalities or breaking bad news to families of
victims). The data, revealing elevated distress and its correlates, suggests the emotional
needs of those occupying less obviously distressing roles in interviewing should be
further assessed and supportive interventions developed.
Future research
62

Although it is reasonable to assume that being indirectly exposed to trauma might have
negative impacts or contribute to psychological distress, the cross-sectional nature of
this explorative study cannot provide a definite answer regarding causality. Studies
utilising larger samples and longitudinal designs can contribute to more robust
understanding of how psychological and occupational distress and resilience develops
in investigative interviewers. Whilst both UK and Norwegian interviewers had been in
post for some time, it would also be useful to examine those who have been in post for
significant periods to examine the potential cumulative impact of their work
The CF-CS model could potentially benefit from some restructuring and a
clearer examination of how occupational distress or resilience forms. Although empathy
has been suggested to be the lead process through which CF and CS is developed, these
findings do not support that. It would be beneficial to understand better how these
processes occur, to provide a more robust theoretical standing to the model.
ConclusionThis is the first exploratory study to examine levels and predictors of work-related
distress and resilience in investigative interviewers. It revealed elevated psychological
morbidity and work-related distress, as well as lower CS in national police services in
the UK and Norway. The suggested role of empathy as a mediating factor was not
evidenced and more research is required both to further understand factors influencing
wellbeing, and strategies to counter distress. Nevertheless, findings suggest that further
organisational strategies should be offered to support police interviewers, which might
help to maintain resilience and sustain them in key roles to aid the vulnerable and secure
prosecutions.
63
ReferencesAndersen, J. P., & Papazoglou, K. (2015). Compassion fatigue and compassion
satisfaction among police officers: An understudied topic. International Journal
of Emergency Mental Health and Human Resilience, 17(3), 661-663
Arnold, D., Calhoun, L.G., Tedeschi, R & Cann, A. (2005). Vicarious posttraumatic
growth in psychotherapy. Journal of Humanistic Psychology. 45(2), 239-263
Baron-Cohen, S., & Wheelwright, S. (2004). The empathy quotient: An investigation of
adults with Asperger syndrome or high functioning autism, and normal sex
differences. Journal of Autism and Developmental Disorders, 34(2), 163–175
Bjelland, I., Dahl, A. A., Haug, T. T., & Neckelmann, D. (2002). The validity of the
Hospital Anxiety and Depression Scale: an updated literature review. Journal of
Psychosomatic Research, 52(2), 69-77.
Bruusgard, R., Bjerknes, O.T., Buseth, S. et al. (2013). Riksadvokatens arbeidsgruppe:
Avhørsmetodikk i Politiet. Available via https://www.riksadvokaten.no/wp-
content/uploads/2017/10/Avh%C3%B8rsmetodikk-i-Politiet-med-vedlegg.pdf
retrieved 24 April 2020
Bull, R. (2014). Investigative interviewing. New York: Springer Science & Business
Media
Canfield, J. (2005). Secondary traumatization, burnout, and vicarious traumatization: A
review of the literature as it relates to therapists who treat trauma. Smith College
Studies in Social Work, 75(2), 81-101.
Coleman, R., Kirby, S., Birdsall, N., Cox, C., & Boulton, L. (2018). Wellbeing in
Policing: Blue Light Wellbeing Framework. University of Central Lancashire
and Lancashire Constabulary
College of Policing (2019). Investigation: Investigative interviewing. Available via
https://www.app.college.police.uk/app-content/investigations/investigative-
interviewing/ Retrieved 23 April 2020
Collins, S., & Long, A. (2003). Working with the psychological effects of trauma:
consequences for mental health‐care workers–a literature review. Journal of
Psychiatric and Mental Health Nursing, 10(4), 417-424.
Crawford, R., Disney, R., & Simpson, P. (2017). Police officer retention in England and
Wales. Institute For Fiscal Studies for Economic and Social Research Council.
Available via https://www.ifs.org.uk/publications/8824 Retrieved 25 Mai 2020
64
Crawford, J. R., Henry, J. D., Crombie, C., & Taylor, E. P. (2001). Normative data for
the HADS from a large non‐clinical sample. British Journal of Clinical
Psychology, 40(4), 429-434.
Cross, L.C. & Ashley, L. (2004). Police trauma and addiction: Coping with the dangers
of the job. FBI Law Enforcement Bulletin, 73(10), 24-32.
De La Rosa, G. M., Webb-Murphy, J. A., Fesperman, S. F., & Johnston, S. L. (2018).
Professional quality of life normative benchmarks. Psychological Trauma:
Theory, Research, Practice, and Policy, 10(2), 225.
Duarte, J., Pinto-Gouveia, J., & Cruz, B. (2016). Relationships between nurses’
empathy, self- compassion and dimensions of professional quality of life: A
cross-sectional study. International Journal of Nursing Studies, 60, 1-11.
Eisenberger, R., Huntington, R., Hutchison, S., & Sowa, D. (1986). Perceived
organizational support. Journal of Applied Psychology, 71(3), 500-507.
Eisenberger, R. (2019). Perceived Organizational Support.
http://classweb.uh.edu/eisenberger/perceived-organizational-support/ Retrieved
on 12th February 2019
Elwood, L. S., Mott, J., Lohr, J. M., & Galovski, T. E. (2011). Secondary trauma
symptoms in clinicians: A critical review of the construct, specificity, and
implications for trauma focused treatment. Clinical Psychology Review, 31(1),
25-36.
Evans, S., Huxley, P., Gately, C. et al. (2006). Mental health, burnout and job
satisfaction among mental health social workers in England and Wales. The
British Journal of Psychiatry, 188(1), 75-80
Evces, M. R. (2015). What is vicarious trauma? In G. Quintangon & M. R. Evces (eds),
Vicarious trauma and disaster mental health (pp. 9-23). Routledge.
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G* Power 3: A flexible
statistical power analysis program for the social, behavioral, and biomedical
sciences. Behavior Research Methods, 39(2), 175-191.
Figley (1995). Compassion Fatigue: Coping With Secondary Traumatic Stress Disorder
In Those Who Treat The Traumatised. Routledge, New York NY.
Goubert, L., Craig, K. D., Vervoort, T., et al. (2005). Facing others in pain: the effects
of empathy. Pain, 118(3), 285-288.
65

Haldorsson, O. L. (2017). Barnahus Quality Standards Summary: Guidance for
Multidisciplinary and Interagency Response to Child Victims and Witnesses of
Violence. Council of the Baltic Sea States Secretaries and Child Circle.
Available via http://www.childrenatrisk.eu/promise/
wp-content/uploads/sites/4/2015/11/Guidance_short_reformatted.pdf
Hanway, P. & Akehurst, L. (2018). The voice from the front line: Police officers’
perceptions of real-world interviewing with vulnerable witnesses. Investigative
Interviewing: Research and Practise. 9(1) 14-33
Her Majesty’s Inspectorate of Constabulary (HMIC) (2012). Policing in Austerity: One
Year On. Available via https://www.justiceinspectorates.gov.uk/
hmicfrs/media/policing-in-austerity-one-year-on.pdf Retrieved on 31 May 2020.
Hunt, P.A., Denieffe, S. & Gooney, M. (2017). Burnout and its relationship to empathy
in nursing: A review of the literature. Journal of Research in Nursing. 22(1)
Karlsson, I. & Christianson, S-A. (2003). The phenomenology of traumatic experiences
in police work. Policing: An International Journal of Police Strategies &
Management, 26(3), 419-438.
Kronenberg, M., Osofsky, H. J., Osofsky, J. D. et al. (2008). First responder culture:
Implications for mental health professionals providing services following a
natural disaster. Psychiatric Annals, 38(2), 114–118.
Lawrence, E. J., Shaw, P., Baker, D., et al. (2004). Measuring empathy: reliability and
validity of the Empathy Quotient. Psychological Medicine, 34(5), 911-920.
Lassiter, G. D. (Ed.) (2004). Interrogations, Confessions, and Entrapment. New York:
Springer.
Leiknes, K. A., Dalsbø, T. K. & Siqveland, J. (2016). Psychometric assessment of the
Norwegian version of the Hospital Anxiety and Depression Scale (HADS). Oslo:
Norwegian Institute of Public Health.
MacEachern, A. D., Jindal-Snape, D., & Jackson, S. (2011). Child abuse investigation:
police officers and secondary traumatic stress. International Journal of
Occupational Safety and Ergonomics, 17(4), 329-339.
Maslach, C., & Jackson, S. E. (1981). The measurement of experienced
burnout. Journal of Organizational Behavior, 2(2), 99-113.
Maslach, C., Jackson, S. E., & Leiter, M. P. (1996). Maslach Burnout Inventory. 3rd ed.
Palo Alto, CA: Consulting Psychologists Press.
66
Mathieu, F. (2007). Running on empty: Compassion fatigue in health professionals.
Retrieved from http://www.compassionfatigue.org/pages/RunningOnEmpty.pdf
Retrieved 4 May 2020
McFadden, P., Campbell, A., & Taylor, B. (2014). Resilience and burnout in child
protection social work: Individual and organisational themes from a
systematic literature review. British Journal of Social Work, 45(5), 1546-1563.
Milne, R. & Bull, R. (1999). Investigative Interviewing: Psychology and Practice.
Chichester: Wiley.
Najjar, N., Davis, L W., Beck-Coon, K. & Doebbeling, C.C. (2009). Compassion
fatigue: A Review of the Research to Date and Relevance to Cancer-Care
Providers. Journal of Health Psychology. 14(2) 267-277
Papazoglou, K., Bonanno, G., Blumberg, D., & Keesee, T. (2019). Moral injury in
police work. FBI Law Enforcement Bulletin.
Papazoglou, K., Koskelainen, M. & Steuwe, N. (2017). Exploring the Role of
Compassion Satisfaction and Compassion Fatigue in Predicting Burnout among
Police Officers. Open Journal of Psychiatry & Allied Sciences. 9(2), 107-112
Perneger, T. V. (1998). What's wrong with Bonferroni adjustments. Bmj, 316(7139),
1236-1238.
Risan, P., Milne, R., & Binder P. (2016). Regulating and coping with distress during
police interviews of traumatised victims. Psychological Trauma: Theory,
Research, Practise and Policy. 8(6), 736-744
Shore, L.M. & Tetrick, L.E. (1991). A Construct Validity Study of the Survey of
Perceived Organizational Support. Journal of Applied Psychology, 76(5), 637
643
Silverstone, P. H. (1994). Poor efficacy of the Hospital Anxiety and Depression Scale in
the diagnosis of major depressive disorder in both medical and psychiatric
patients. Journal of Psychosomatic Research, 38(5), 441-450.
Stamm, B. H. (2002). Measuring compassion satisfaction as well as fatigue:
Developmental history of the Compassion Satisfaction and Fatigue Test. In C. R.
Figley Ed.), Psychosocial stress series, no. 24. Treating compassion fatigue (p.
107–119). Brunner-Routledge.
Stamm, B. H. (2010). The concise ProQOL manual, 2nd ed. Pocatello, ID: ProQOL.org.
67
Thomas, J. T., & Otis, M. D. (2010). Intrapsychic correlates of professional quality of
life: Mindfulness, empathy, and emotional separation. Journal of the Society for
Social Work and Research, 1(2), 83-98.
Turgoose, D., Glover, N., Barker, C., & Maddox, L. (2017). Empathy, compassion
fatigue, and burnout in police officers working with rape
victims. Traumatology, 23(2), 205.
Zigmond, A.S. & Snaith, R.P. (1983). The hospital anxiety and depression scale. Acta
Psychiatrica Scandinavica, 67(6)
Watts, J., & Robertson, N. (2015). Selecting a measure for assessing secondary trauma
in nurses. Nurse Researcher, 23(2).
Worley, J. A., Fuqua, D. R., & Hellman, C. M. (2009). The survey of perceived
organizational support: Which measure should we use? SA Journal of Industrial
Psychology, 35(1), 112-116.
Yang, Y. H. & Kim, J. K. (2012). A literature review of compassion fatigue in
nursing. Korean Journal of Adult Nursing, 24(1), 38-51.
68
Appendices:Mandatory appendices are marked with an asterisk *
69
Appendix A*: Guidelines to authors for journal targeted for literature review
About the Journal: Psychiatry, Psychology and Law is an international, peer-reviewed
journal publishing high-quality, original research. Please see the journal's Aims &
Scope for information about its focus and peer-review policy. Please note that this
journal only publishes manuscripts in English.
Psychiatry, Psychology and Law accepts the following types of article: original articles
and empirical studies, analyses of professional issues, controversies and developments
in these areas, case studies and case commentaries, book reviews.
Peer Review and Ethics: Taylor & Francis is committed to peer-review integrity and
upholding the highest standards of review. Once your paper has been assessed for
suitability by the editor, it will then be double blind peer reviewed by independent,
anonymous expert referees. Find out more about what to expect during peer review and
read our guidance on publishing ethics.
Preparing Your Paper: All authors submitting to medicine, biomedicine, health
sciences, allied and public health journals should conform to the Uniform Requirements
for Manuscripts Submitted to Biomedical Journals, prepared by the International
Committee of Medical Journal Editors (ICMJE).
Structure: Your paper should be compiled in the following order: title page; abstract;
keywords; main text introduction, materials and methods, results, discussion;
acknowledgments; declaration of interest statement; references; appendices (as
appropriate); table(s) with caption(s) (on individual pages); figures; figure captions (as a
list).
Word Limits: Please include a word count for your paper. A typical paper for this
journal should be no more than 12000 words, inclusive of tables, references, figure
captions.
Style Guidelines: Please refer to these quick style guidelines when preparing your
paper, rather than any published articles or a sample copy. Please use British (-ise)
spelling style consistently throughout your manuscript. Any form of consistent
quotation style is acceptable. Please note that long quotations should be indented
without quotation marks.
Psychological manuscripts should be prepared in accordance with the format and style
specified in the ‘Publication Manual of the American Psychological Association’, fifth
edition. Pages should be numbered consecutively. References should be cited in the text
70

as specified in the Publication Manual of the American Psychological Association, fifth
edition. A concise description of APA referencing style can be found her.
Personal communications should be cited as such in the text and should not be included
in the reference list. For an overview of APA style (including referencing)
visit http://www.lib.monash.edu.au/tutorials/citing/apa.html
Formatting and Templates: Papers may be submitted in Word format. Figures should
be saved separately from the text. To assist you in preparing your paper, we provide
formatting template(s). Word templates are available for this journal. Please save the
template to your hard drive, ready for use. If you are not able to use the template via the
links (or if you have any other template queries) please contact us here.
References: Please use this reference guide when preparing your paper.
Checklist: What to Include
1. Author details. Please ensure everyone meeting the International Committee of
Medical Journal Editors (ICMJE) requirements for authorship is included as an
author of your paper. All authors of a manuscript should include their full name
and affiliation on the cover page of the manuscript. Where available, please also
include ORCiDs and social media handles (Facebook, Twitter or LinkedIn). One
author will need to be identified as the corresponding author, with their email
address normally displayed in the article PDF (depending on the journal) and the
online article. Authors’ affiliations are the affiliations where the research was
conducted. If any of the named co-authors moves affiliation during the peer-
review process, the new affiliation can be given as a footnote. Please note that
no changes to affiliation can be made after your paper is accepted. Read more on
authorship.
2. Should contain an unstructured abstract of 150 words.
3. Graphical abstract (optional). This is an image to give readers a clear idea of
the content of your article. It should be a maximum width of 525 pixels. If your
image is narrower than 525 pixels, please place it on a white background 525
pixels wide to ensure the dimensions are maintained. Save the graphical abstract
as a .jpg, .png, or .tiff. Please do not embed it in the manuscript file but save it as
a separate file, labelled GraphicalAbstract1.
71
4. You can opt to include a video abstract with your article. Find out how these
can help your work reach a wider audience, and what to think about when
filming.
5. At least 10 keywords. Read making your article more discoverable, including
information on choosing a title and search engine optimization.
6. Funding details. Please supply all details required by your funding and grant-
awarding bodies as follows: For single agency grants. This work was supported
by the [Funding Agency] under Grant [number xxxx]. For multiple agency
grants: This work was supported by the [Funding Agency #1] under Grant
[number xxxx]; [Funding Agency #2] under Grant [number xxxx]; and [Funding
Agency #3] under Grant [number xxxx].
7. Disclosure statement. This is to acknowledge any financial interest or benefit
that has arisen from the direct applications of your research. Further guidance on
what is a conflict of interest and how to disclose it.
8. Supplemental online material. Supplemental material can be a video, dataset,
fileset, sound file or anything which supports (and is pertinent to) your paper.
We publish supplemental material online via Figshare. Find out more
about supplemental material and how to submit it with your article.
9. Figures. Figures should be high quality (1200 dpi for line art, 600 dpi for
grayscale and 300 dpi for colour, at the correct size). Figures should be supplied
in one of our preferred file formats: EPS, PS, JPEG, TIFF, or Microsoft Word
(DOC or DOCX) files are acceptable for figures that have been drawn in Word.
For information relating to other file types, please consult our Submission of
electronic artwork document.
10. Tables. Tables should present new information rather than duplicating what is in
the text. Readers should be able to interpret the table without reference to the
text. Please supply editable files.
11. Equations. If you are submitting your manuscript as a Word document, please
ensure that equations are editable. More information about mathematical
symbols and equations.
12. Units. Please use SI units (non-italicized).
Using Third-Party Material in your Paper: You must obtain the necessary
permission to reuse third-party material in your article. The use of short extracts of text
72

and some other types of material is usually permitted, on a limited basis, for the
purposes of criticism and review without securing formal permission. If you wish to
include any material in your paper for which you do not hold copyright, and which is
not covered by this informal agreement, you will need to obtain written permission from
the copyright owner prior to submission. More information on requesting permission to
reproduce work(s) under copyright.
Disclosure Statement: Please include a disclosure statement, using the subheading
“Disclosure of interest.” If you have no interests to declare, please state this (suggested
wording: The authors report no conflict of interest). For all NIH/Wellcome-funded
papers, the grant number(s) must be included in the declaration of interest
statement. Read more on declaring conflicts of interest.
Clinical Trials Registry: In order to be published in a Taylor & Francis journal, all
clinical trials must have been registered in a public repository at the beginning of the
research process (prior to patient enrolment). Trial registration numbers should be
included in the abstract, with full details in the methods section. The registry should be
publicly accessible (at no charge), open to all prospective registrants, and managed by a
not-for-profit organization. For a list of registries that meet these requirements, please
visit the WHO International Clinical Trials Registry Platform (ICTRP). The registration
of all clinical trials facilitates the sharing of information among clinicians, researchers,
and patients, enhances public confidence in research, and is in accordance with
the ICMJE guidelines.
Complying With Ethics of Experimentation: Please ensure that all research reported
in submitted papers has been conducted in an ethical and responsible manner, and is in
full compliance with all relevant codes of experimentation and legislation. All papers
which report in vivo experiments or clinical trials on humans or animals must include a
written statement in the Methods section. This should explain that all work was
conducted with the formal approval of the local human subject or animal care
committees (institutional and national), and that clinical trials have been registered as
legislation requires. Authors who do not have formal ethics review committees should
include a statement that their study follows the principles of the Declaration of Helsinki.
Consent: All authors are required to follow the ICMJE requirements on privacy and
informed consent from patients and study participants. Please confirm that any patient,
service user, or participant (or that person’s parent or legal guardian) in any research,
73
experiment, or clinical trial described in your paper has given written consent to the
inclusion of material pertaining to themselves, that they acknowledge that they cannot
be identified via the paper; and that you have fully anonymized them. Where someone
is deceased, please ensure you have written consent from the family or estate. Authors
may use this Patient Consent Form, which should be completed, saved, and sent to the
journal if requested.
Health and Safety: Please confirm that all mandatory laboratory health and safety
procedures have been complied with in the course of conducting any experimental work
reported in your paper. Please ensure your paper contains all appropriate warnings on
any hazards that may be involved in carrying out the experiments or procedures you
have described, or that may be involved in instructions, materials, or formulae.
Please include all relevant safety precautions; and cite any accepted standard or code of
practice. Authors working in animal science may find it useful to consult
the International Association of Veterinary Editors’ Consensus Author Guidelines on
Animal Ethics and Welfare and Guidelines for the Treatment of Animals in Behavioural
Research and Teaching. When a product has not yet been approved by an appropriate
regulatory body for the use described in your paper, please specify this, or that the
product is still investigational.
Submitting Your Paper: This journal uses ScholarOne Manuscripts to manage the
peer-review process. If you haven't submitted a paper to this journal before, you will
need to create an account in ScholarOne. Please read the guidelines above and then
submit your paper in the relevant Author Centre, where you will find user guides and a
helpdesk.
Please note that Psychiatry, Psychology and Law uses Crossref™ to screen papers for
unoriginal material. By submitting your paper to Psychiatry, Psychology and Law you
are agreeing to originality checks during the peer-review and production processes. On
acceptance, we recommend that you keep a copy of your Accepted Manuscript. Find out
more about sharing your work.
Publication Charges: There are no submission fees, publication fees or page charges
for this journal. Colour figures will be reproduced in colour in your online article free of
charge. If it is necessary for the figures to be reproduced in colour in the print version, a
charge will apply. Charges for colour figures in print are £300 per figure ($400 US
Dollars; $500 Australian Dollars; €350). For more than 4 colour figures, figures 5 and
74
above will be charged at £50 per figure ($75 US Dollars; $100 Australian Dollars; €65).
Depending on your location, these charges may be subject to local taxes.
Copyright Options: Copyright allows you to protect your original material, and stop
others from using your work without your permission. Taylor & Francis offers a
number of different license and reuse options, including Creative Commons licenses
when publishing open access. Read more on publishing agreements.
Complying with Funding Agencies: We will deposit all National Institutes of Health
or Wellcome Trust-funded papers into PubMedCentral on behalf of authors, meeting the
requirements of their respective open access policies. If this applies to you, please tell
our production team when you receive your article proofs, so we can do this for you.
Check funders’ open access policy mandates here. Find out more about sharing your
work.
My Authored Works: On publication, you will be able to view, download and check
your article’s metrics (downloads, citations and Altmetric data) via My Authored
Works on Taylor & Francis Online. This is where you can access every article you have
published with us, as well as your free eprints link, so you can quickly and easily share
your work with friends and colleagues. We are committed to promoting and increasing
the visibility of your article. Here are some tips and ideas on how you can work with us
to promote your research.
Article Reprints: You will be sent a link to order article reprints via your account in
our production system. For enquiries about reprints, please contact the Taylor & Francis
Author Services team at [email protected]. You can also order print copies of the
journal issue in which your article appears.
Queries: Should you have any queries, please visit our Author Services website or
contact us here.
Updated 6-05-2020
75

Appendix B: Expanded details on search methodology
Database Applied filters Secondary trauma
key terms
Legal profession
key terms
PsychINFO English
Peer reviewed
Peer-reviewed
journal
Exclude
dissertations
burnout OR
“compassion
fatigue” OR
“secondary
trauma*” OR
vicarious trauma*
OR PTSD OR
“Post-traumatic
stress*” OR “Post
traumatic stress*”
solicitor* OR
barrister* OR
lawyer* OR
attorney* OR
judge* OR legal
PILOTS Peer reviewed
Journal article
English
PubMed English
Journal articles
Web of science Article
English
Westlaw UK Journal
Business source
premier
Academic journal
Article
Criminal justice
abstracts
Scholarly peer-
reviewed journals
English
Article
Academic journal
76
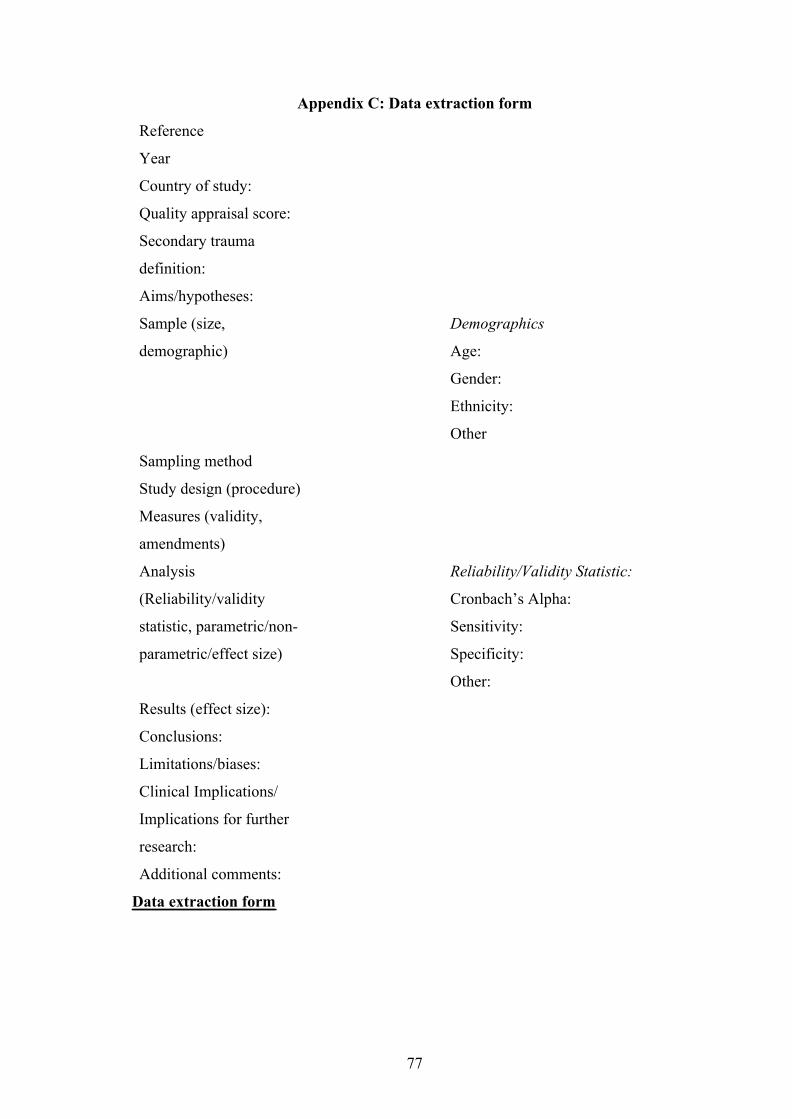
Appendix C: Data extraction form
Reference
Year
Country of study:
Quality appraisal score:
Secondary trauma
definition:
Aims/hypotheses:
Sample (size,
demographic)
Demographics
Age:
Gender:
Ethnicity:
Other
Sampling method
Study design (procedure)
Measures (validity,
amendments)
Analysis
(Reliability/validity
statistic, parametric/non-
parametric/effect size)
Reliability/Validity Statistic:
Cronbach’s Alpha:
Sensitivity:
Specificity:
Other:
Results (effect size):
Conclusions:
Limitations/biases:
Clinical Implications/
Implications for further
research:
Additional comments:
Data extraction form
77

Appendix D: AXIS Quality appraisal tool items
Introduction
1. Were the aims/objectives of the study clear?
Methods
2. Was the study design appropriate for the stated aim(s)?
3. Was the sample size justified?
4. Was the target/reference population clearly defined? (Is it clear who the research
was about?)
5. Was the sample frame taken from an appropriate population base so that it
closely represented the target/reference population under investigation?
6. Was the selection process likely to select subjects/participants that were
representative
7. Were measures undertaken to address and categorise non-responders?
8. Were the risk factors and outcome variables measured appropriate to the aims of
the study?
9. Were the risk factors and outcome variables measured correctly using
instruments/measurements that had been trialled, piloted or published
previously?
10. Is it clear what was used to determined statistical significance and/or precision
estimates? (eg. P values, Cis)
11. Were the methods (including statistical methods) sufficiently described to enable
them to be repeated?
Results
12. Were the basic data adequately described?
13. Does the response rate raise concerns about non-response bias?
14. If appropriate, was information about non-responders described?
15. Were the results internally consistent?
16. Were the results for the analysis described in the methods, presented?
78
Discussion
17. Were the authors’ discussion and conclusions justified by the results?
18. Were the limitations of the study discussed?
Other
19. Were there any funding sources or conflicts of interests that may affect the
authors’ interpretation of the results?
20. Was ethical approval or consent of participants attained?
Downes, M. J., Brennan, M. L., Williams, H. C. & Dean, R. S. (2016). Development of
a critical appraisal tool to assess the quality of cross-sectional studies (axis).
BMJ Open, 6(12). 10.1136/bmjopen-2016-011458
79
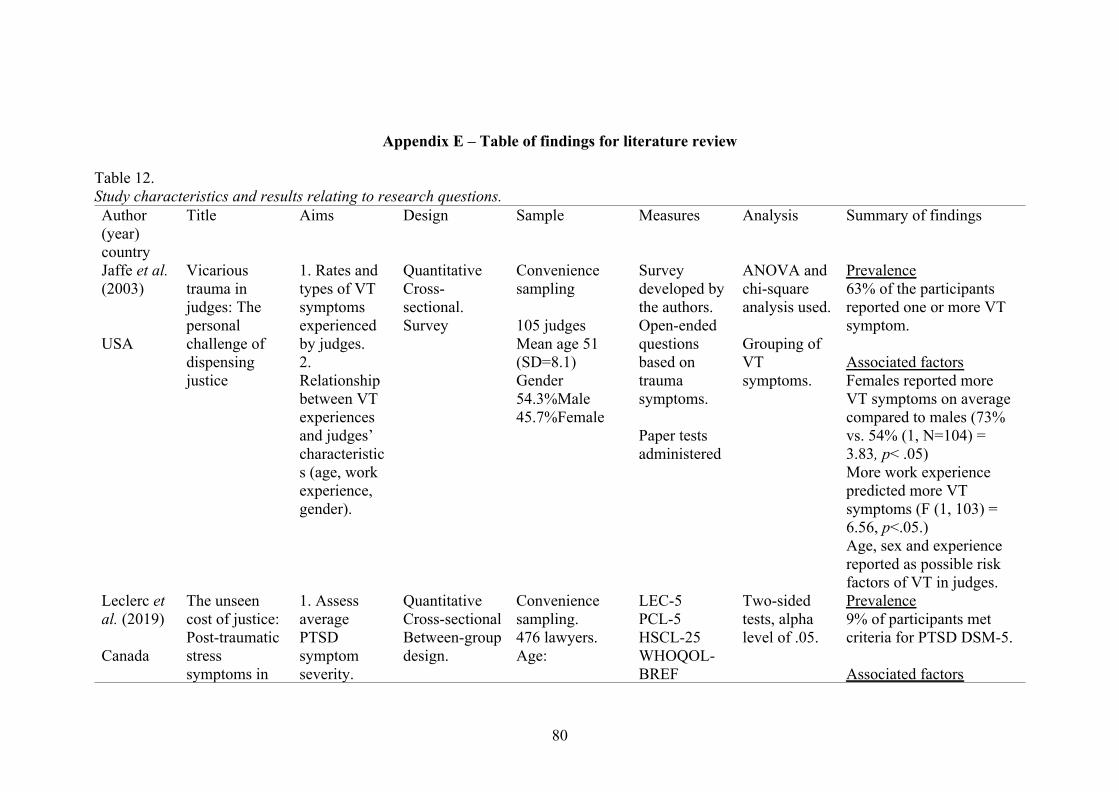
Appendix E – Table of findings for literature review
Table 12.Study characteristics and results relating to research questions.Author(year)country
Title Aims Design Sample Measures Analysis Summary of findings
Jaffe et al.(2003)
USA
Vicarioustrauma injudges: Thepersonalchallenge ofdispensingjustice
1. Rates andtypes of VTsymptomsexperiencedby judges.2.Relationshipbetween VTexperiencesand judges’characteristics (age, workexperience,gender).
QuantitativeCross-sectional.Survey
Conveniencesampling
105 judgesMean age 51(SD=8.1)Gender54.3%Male45.7%Female
Surveydeveloped bythe authors.Open-endedquestionsbased ontraumasymptoms.
Paper testsadministered
ANOVA andchi-squareanalysis used.
Grouping ofVTsymptoms.
Prevalence63% of the participantsreported one or more VTsymptom.
Associated factorsFemales reported moreVT symptoms on averagecompared to males (73%vs. 54% (1, N=104) =3.83, p< .05)More work experiencepredicted more VTsymptoms (F (1, 103) =6.56, p<.05.)Age, sex and experiencereported as possible riskfactors of VT in judges.
Leclerc etal. (2019)
Canada
The unseencost of justice:Post-traumaticstresssymptoms in
1. AssessaveragePTSDsymptomseverity.
QuantitativeCross-sectionalBetween-groupdesign.
Conveniencesampling.476 lawyers.Age:
LEC-5PCL-5HSCL-25WHOQOL-BREF
Two-sidedtests, alphalevel of .05.
Prevalence9% of participants metcriteria for PTSD DSM-5.
Associated factors
80

Canadianlawyers
2. Identifytheproportion oflawyersmeeting thediagnosticcriteria ofPTSD.3. Levels ofpsychologicaldistress andquality oflife,understanding lawyers’wellbeing.
Comparinglawyers withno, moderateand highwork-relatedtraumaexposure.
20-29 (13.7%)30-39 (34.9%)40-49 (24.8%)50-59 (18.3%)60+ (8.4%)Gender :42.4%Male57.6%FemaleEthnicity:Canadian(84.5%)Caucasian(88.9%) livingin Quebec(59%)
Onlinesurvey.
Descriptives(chi-squares,t-tests andANOVA).Post-hocBonferronicontrastanalysis wasconductedbetweengroups.ANCOVAused to testmoderatinghypotheses.
Higher trauma exposurepredicted higher levels ofPTSD symptoms (F (1,471) = 4.79, p=.029,partial η2=.01).Prior trauma historypredicted higher levels ofPTSD symptoms.Females more likely todevelop PTSD symptoms,and had more severesymptoms relative to men.Higher number of weeklywork hours increased therisk of PTSD by 1.89times
Levin &Greisberg(2003)
USA
Vicarioustrauma inattorneys
Exploringlevels of VTin attorneyscompared tomental healthprofessionals.
Quantitative.Cross-sectionalBetween-groupdesign.
Social workers,mental healthprofessionalsand Attorneys
STQ,Itemsassessingburnout.Caseload,personal
Method ofanalysis notreported.
PrevalenceAttorneys showed higherlevels of STS and burnout,compared to socialworkers and mental healthprofessionals.
81
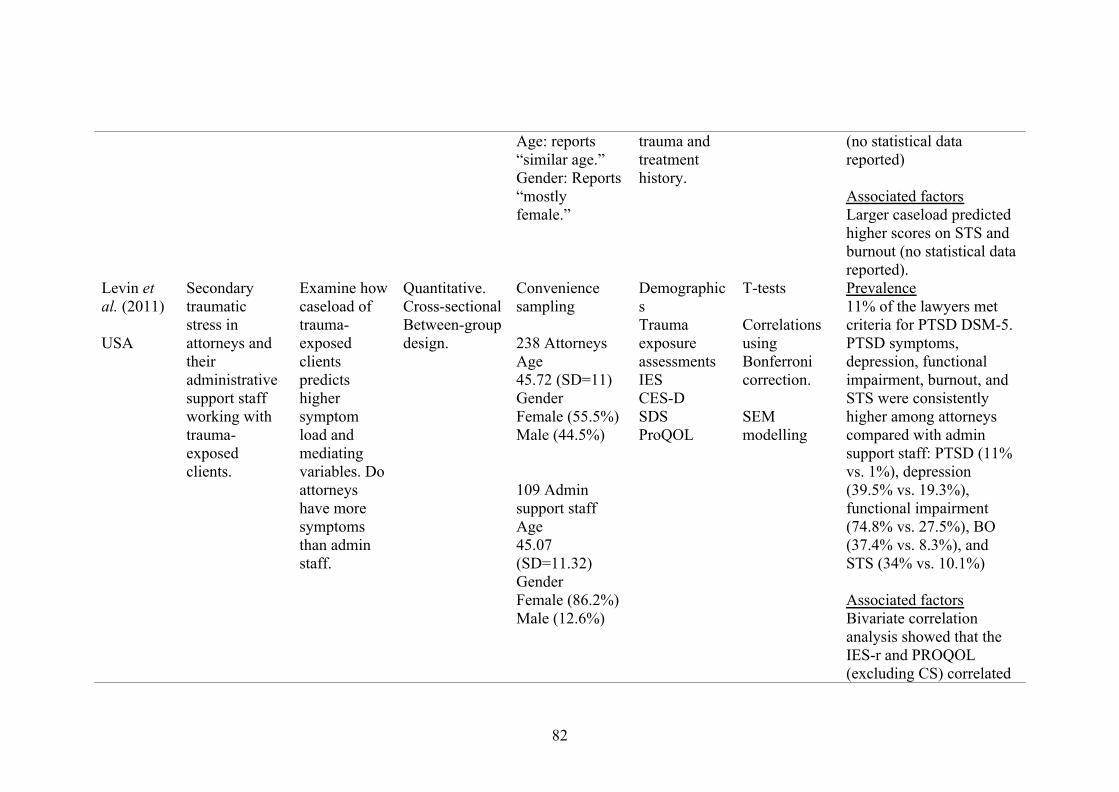
Age: reports“similar age.”Gender: Reports“mostlyfemale.”
trauma andtreatmenthistory.
(no statistical datareported)
Associated factorsLarger caseload predictedhigher scores on STS andburnout (no statistical datareported).
Levin etal. (2011)
USA
Secondarytraumaticstress inattorneys andtheiradministrativesupport staffworking withtrauma-exposedclients.
Examine howcaseload oftrauma-exposedclientspredictshighersymptomload andmediatingvariables. Doattorneyshave moresymptomsthan adminstaff.
Quantitative.Cross-sectionalBetween-groupdesign.
Conveniencesampling
238 AttorneysAge45.72 (SD=11)GenderFemale (55.5%)Male (44.5%)
109 Adminsupport staffAge45.07(SD=11.32)GenderFemale (86.2%)Male (12.6%)
DemographicsTraumaexposureassessmentsIESCES-DSDSProQOL
T-tests
CorrelationsusingBonferronicorrection.
SEMmodelling
Prevalence11% of the lawyers metcriteria for PTSD DSM-5.PTSD symptoms,depression, functionalimpairment, burnout, andSTS were consistentlyhigher among attorneyscompared with adminsupport staff: PTSD (11%vs. 1%), depression(39.5% vs. 19.3%),functional impairment(74.8% vs. 27.5%), BO(37.4% vs. 8.3%), andSTS (34% vs. 10.1%)
Associated factorsBivariate correlationanalysis showed that theIES-r and PROQOL(excluding CS) correlated
82

significantly (p<.001) withhours worked per week(IESr: r=.25-.29,ProQOL5: r=.26-.40) andthe number of trauma-exposed clients (IESr:r=.24-.28, ProQOL5:r=.30-.37).
Participant groupsignificantly explained 7%of the variance in PTSDsymptoms. Work-relatedexposure significantlyexplained 14% of thevariance in PTSDsymptoms. Work-relatedexposure variablesmediated (albeit notexclusively) the attorneys’vulnerability to PTSDsymptoms.
Participant groupsignificantly explained 20% of the variance in STSand burnout scores. Work-related exposure variablesmediated albeit notexclusively attorneys’
83
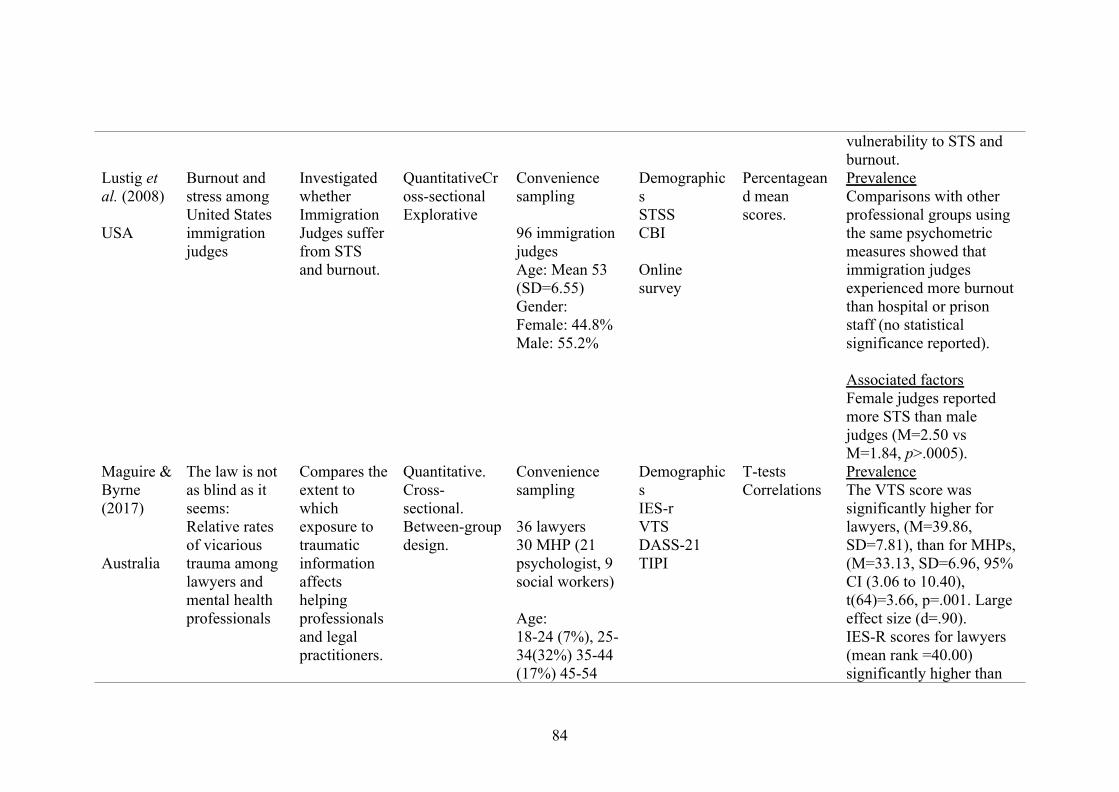
vulnerability to STS andburnout.
Lustig etal. (2008)
USA
Burnout andstress amongUnited Statesimmigrationjudges
InvestigatedwhetherImmigrationJudges sufferfrom STSand burnout.
QuantitativeCross-sectionalExplorative
Conveniencesampling
96 immigrationjudgesAge: Mean 53(SD=6.55)Gender:Female: 44.8%Male: 55.2%
DemographicsSTSSCBI
Onlinesurvey
Percentageand meanscores.
PrevalenceComparisons with otherprofessional groups usingthe same psychometricmeasures showed thatimmigration judgesexperienced more burnoutthan hospital or prisonstaff (no statisticalsignificance reported).
Associated factorsFemale judges reportedmore STS than malejudges (M=2.50 vsM=1.84, p>.0005).
Maguire &Byrne(2017)
Australia
The law is notas blind as itseems:Relative ratesof vicarioustrauma amonglawyers andmental healthprofessionals
Compares theextent towhichexposure totraumaticinformationaffectshelpingprofessionalsand legalpractitioners.
Quantitative.Cross-sectional.Between-groupdesign.
Conveniencesampling
36 lawyers30 MHP (21psychologist, 9social workers)
Age:18-24 (7%), 25-34(32%) 35-44(17%) 45-54
DemographicsIES-rVTSDASS-21TIPI
T-testsCorrelations
PrevalenceThe VTS score wassignificantly higher forlawyers, (M=39.86,SD=7.81), than for MHPs,(M=33.13, SD=6.96, 95%CI (3.06 to 10.40),t(64)=3.66, p=.001. Largeeffect size (d=.90).IES-R scores for lawyers(mean rank =40.00)significantly higher than
84
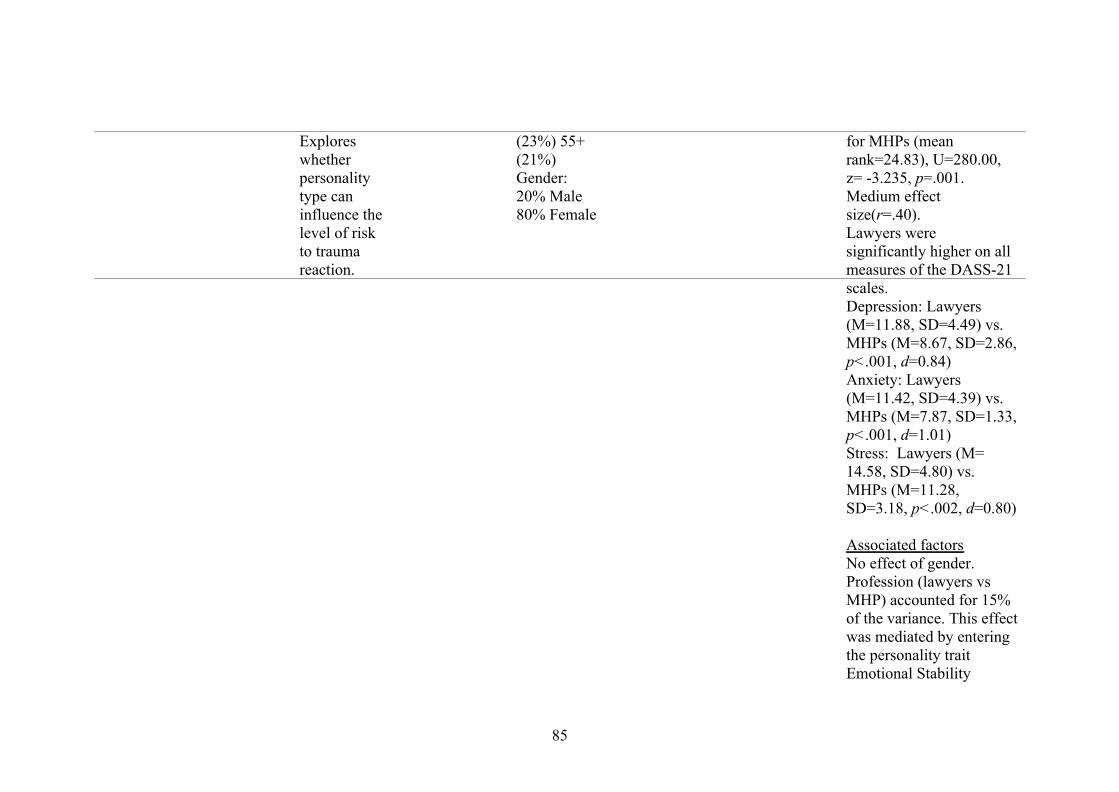
Exploreswhetherpersonalitytype caninfluence thelevel of riskto traumareaction.
(23%) 55+(21%)Gender:20% Male80% Female
for MHPs (meanrank=24.83), U=280.00,z= -3.235, p=.001.Medium effectsize(r=.40).Lawyers weresignificantly higher on allmeasures of the DASS-21scales.Depression: Lawyers(M=11.88, SD=4.49) vs.MHPs (M=8.67, SD=2.86,p<.001, d=0.84)Anxiety: Lawyers(M=11.42, SD=4.39) vs.MHPs (M=7.87, SD=1.33,p<.001, d=1.01)Stress: Lawyers (M=14.58, SD=4.80) vs.MHPs (M=11.28,SD=3.18, p<.002, d=0.80)
Associated factorsNo effect of gender.Profession (lawyers vsMHP) accounted for 15%of the variance. This effectwas mediated by enteringthe personality traitEmotional Stability
85
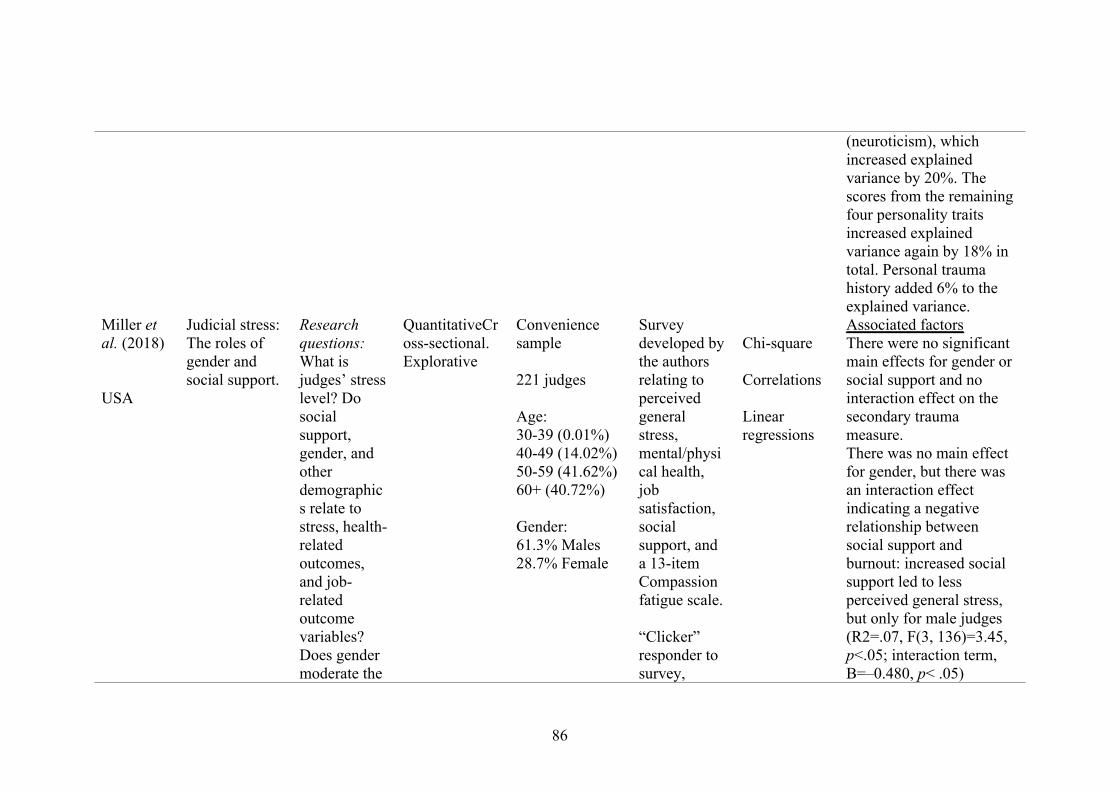
(neuroticism), whichincreased explainedvariance by 20%. Thescores from the remainingfour personality traitsincreased explainedvariance again by 18% intotal. Personal traumahistory added 6% to theexplained variance.
Miller etal. (2018)
USA
Judicial stress:The roles ofgender andsocial support.
Researchquestions:What isjudges’ stresslevel? Dosocialsupport,gender, andotherdemographics relate tostress, health-relatedoutcomes,and job-relatedoutcomevariables?Does gendermoderate the
QuantitativeCross-sectional.Explorative
Conveniencesample
221 judges
Age:30-39 (0.01%)40-49 (14.02%)50-59 (41.62%)60+ (40.72%)
Gender:61.3% Males28.7% Female
Surveydeveloped bythe authorsrelating toperceivedgeneralstress,mental/physical health,jobsatisfaction,socialsupport, anda 13-itemCompassionfatigue scale.
“Clicker”responder tosurvey,
Chi-square
Correlations
Linearregressions
Associated factorsThere were no significantmain effects for gender orsocial support and nointeraction effect on thesecondary traumameasure.There was no main effectfor gender, but there wasan interaction effectindicating a negativerelationship betweensocial support andburnout: increased socialsupport led to lessperceived general stress,but only for male judges(R2=.07, F(3, 136)=3.45,p<.05; interaction term,B=–0.480, p< .05)
86
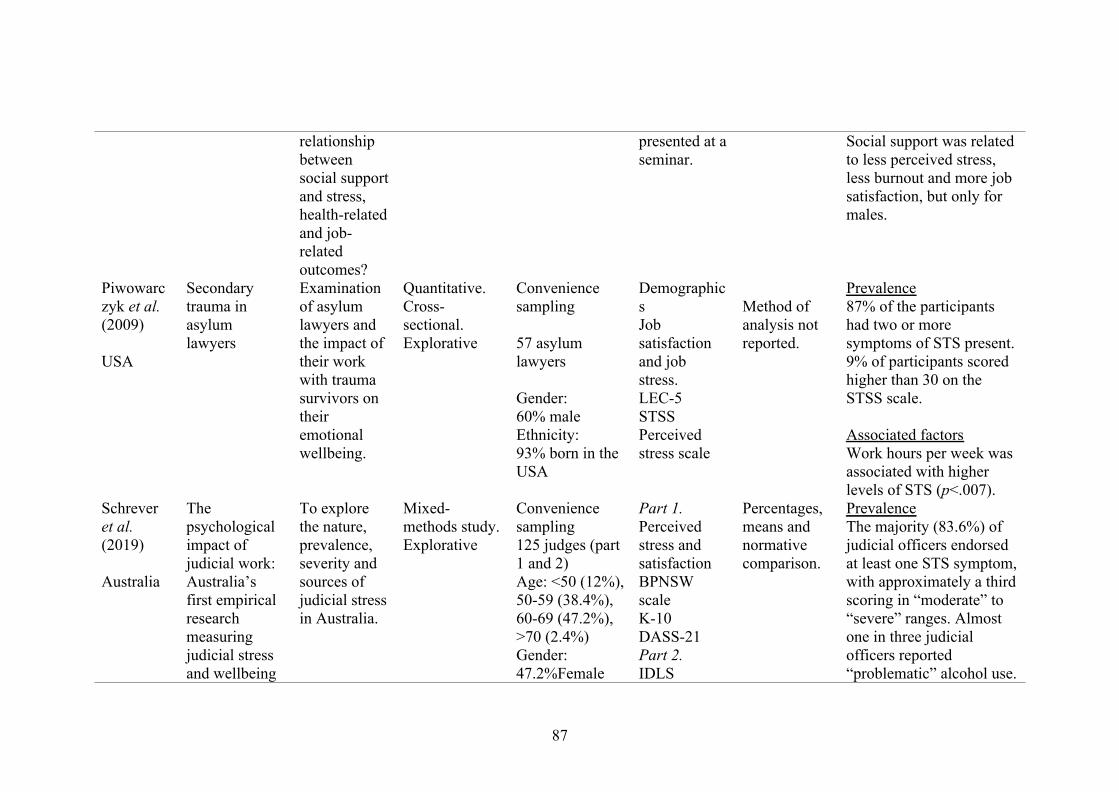
relationshipbetweensocial supportand stress,health-relatedand job-relatedoutcomes?
presented at aseminar.
Social support was relatedto less perceived stress,less burnout and more jobsatisfaction, but only formales.
Piwowarczyk et al.(2009)
USA
Secondarytrauma inasylumlawyers
Examinationof asylumlawyers andthe impact oftheir workwith traumasurvivors ontheiremotionalwellbeing.
Quantitative.Cross-sectional.Explorative
Conveniencesampling
57 asylumlawyers
Gender:60% maleEthnicity:93% born in theUSA
DemographicsJobsatisfactionand jobstress.LEC-5STSSPerceivedstress scale
Method ofanalysis notreported.
Prevalence87% of the participantshad two or moresymptoms of STS present.9% of participants scoredhigher than 30 on theSTSS scale.
Associated factorsWork hours per week wasassociated with higherlevels of STS (p<.007).
Schreveret al.(2019)
Australia
Thepsychologicalimpact ofjudicial work:Australia’sfirst empiricalresearchmeasuringjudicial stressand wellbeing
To explorethe nature,prevalence,severity andsources ofjudicial stressin Australia.
Mixed-methods study.Explorative
Conveniencesampling125 judges (part1 and 2)Age: <50 (12%),50-59 (38.4%),60-69 (47.2%),>70 (2.4%)Gender:47.2%Female
Part 1.Perceivedstress andsatisfactionBPNSWscaleK-10DASS-21Part 2.IDLS
Percentages,means andnormativecomparison.
PrevalenceThe majority (83.6%) ofjudicial officers endorsedat least one STS symptom,with approximately a thirdscoring in “moderate” to“severe” ranges. Almostone in three judicialofficers reported“problematic” alcohol use.
87
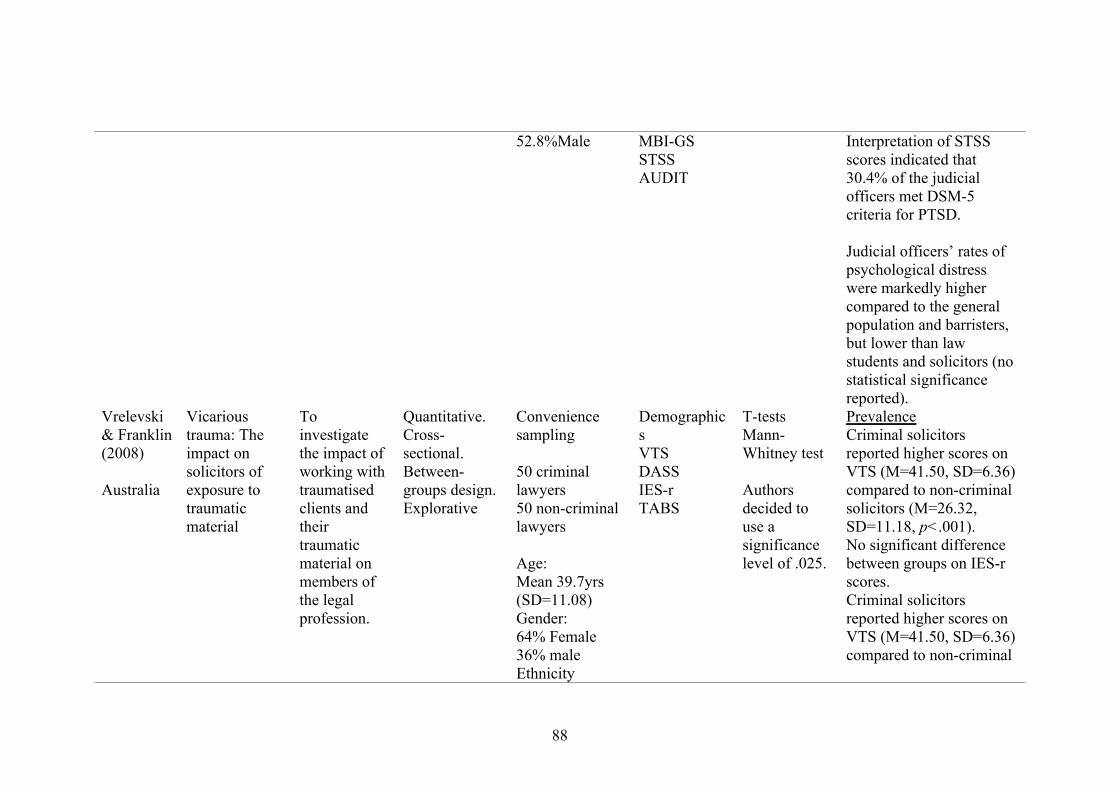
52.8%Male MBI-GSSTSSAUDIT
Interpretation of STSSscores indicated that30.4% of the judicialofficers met DSM-5criteria for PTSD.
Judicial officers’ rates ofpsychological distresswere markedly highercompared to the generalpopulation and barristers,but lower than lawstudents and solicitors (nostatistical significancereported).
Vrelevski& Franklin(2008)
Australia
Vicarioustrauma: Theimpact onsolicitors ofexposure totraumaticmaterial
Toinvestigatethe impact ofworking withtraumatisedclients andtheirtraumaticmaterial onmembers ofthe legalprofession.
Quantitative.Cross-sectional.Between-groups design.Explorative
Conveniencesampling
50 criminallawyers50 non-criminallawyers
Age:Mean 39.7yrs(SD=11.08)Gender:64% Female36% maleEthnicity
DemographicsVTSDASSIES-rTABS
T-testsMann-Whitney test
Authorsdecided touse asignificancelevel of .025.
PrevalenceCriminal solicitorsreported higher scores onVTS (M=41.50, SD=6.36)compared to non-criminalsolicitors (M=26.32,SD=11.18, p<.001).No significant differencebetween groups on IES-rscores.Criminal solicitorsreported higher scores onVTS (M=41.50, SD=6.36)compared to non-criminal
88
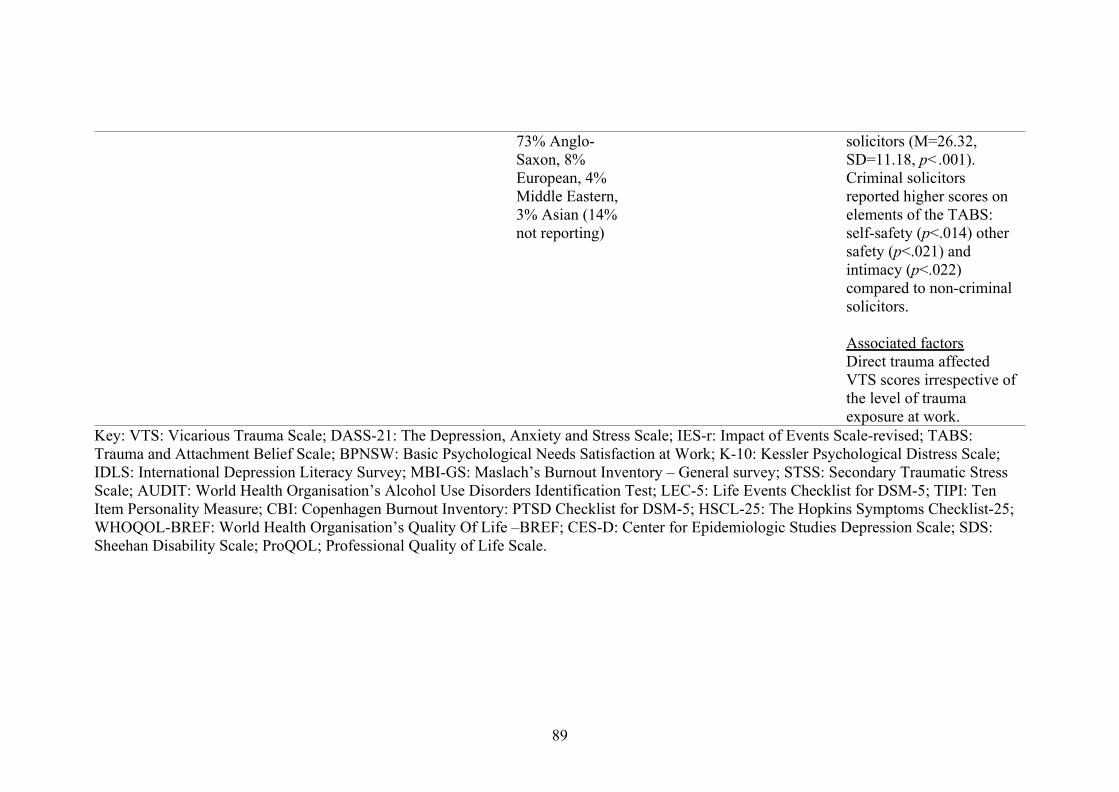
73% Anglo-Saxon, 8%European, 4%Middle Eastern,3% Asian (14%not reporting)
solicitors (M=26.32,SD=11.18, p<.001).Criminal solicitorsreported higher scores onelements of the TABS:self-safety (p<.014) othersafety (p<.021) andintimacy (p<.022)compared to non-criminalsolicitors.
Associated factorsDirect trauma affectedVTS scores irrespective ofthe level of traumaexposure at work.
Key: VTS: Vicarious Trauma Scale; DASS-21: The Depression, Anxiety and Stress Scale; IES-r: Impact of Events Scale-revised; TABS:Trauma and Attachment Belief Scale; BPNSW: Basic Psychological Needs Satisfaction at Work; K-10: Kessler Psychological Distress Scale;IDLS: International Depression Literacy Survey; MBI-GS: Maslach’s Burnout Inventory – General survey; STSS: Secondary Traumatic StressScale; AUDIT: World Health Organisation’s Alcohol Use Disorders Identification Test; LEC-5: Life Events Checklist for DSM-5; TIPI: TenItem Personality Measure; CBI: Copenhagen Burnout Inventory: PTSD Checklist for DSM-5; HSCL-25: The Hopkins Symptoms Checklist-25;WHOQOL-BREF: World Health Organisation’s Quality Of Life –BREF; CES-D: Center for Epidemiologic Studies Depression Scale; SDS:Sheehan Disability Scale; ProQOL; Professional Quality of Life Scale.
89
Appendix F*: Guidelines to authors for journal targeted for research project
Background to the Journal: Since its inception in 2007, the iIIRG’s research outlet
was the Bulletin, however, given its success, it was decided to re-name the Bulletin to
make it more focussed on the group’s main activities (e.g., research and practice). As
such, from April 2012, the Bulletin was renamed to: Investigative Interviewing:
Research and Practice (II-RP), and is the official journal of the iIIRG. From March
2013, II-RP will be included in EBSCOhost™ databases.
Submission Guidelines: Investigative Interviewing: Research and Practice (II-RP) is
the official journal of the iIIRG and is a peer-reviewed, professional outlet for members
and non-members of the iIIRG to publish their articles. Given the multi-disciplinary
nature of the Group, the worldwide circulation of this Journal and strong practitioner
focus, a wide range of articles will be considered for inclusion. These may include
individual research papers or practitioner case studies in relation to the following
specialist areas: investigative interviewing of suspects, witnesses or victims; expert
advice to interviewers; interview training and policy; interview decision-making
processes; false confessions; detecting deception; forensic linguistics. The list of topic
areas is purely indicative and should not be seen as exhaustive.
Submission of Articles: All submissions made to Investigative Interviewing: Research
and Practice (II-RP) should be in English and submitted online via www.iiirg.org.
Authors should prepare and upload one version of their article. The article will be dealt
with by the Editor or the Deputy Editor. Each article will be independently read by at
least two referees (blind review process).
Submission of an article to II-RP will be taken to imply that it represents original work
not previously published and is not being considered elsewhere for publication and, if
accepted for publication, it will not be published elsewhere in the same form, in any
language, without the consent of the II-RP editor. It is a condition of the acceptance by
the editor of an article for publication that the iIIRG acquires the copyright of the article
throughout the world. Prior to publication, the author/s will be required to sign and
return a Copyright Agreement before the article can be published in II-RP. The Editorial
team retains the discretion to accept or decline any submitted article and to make minor
amendments to all work submitted prior to publication. Any major changes will be
made in consultation with the author/s.
90

Format of Articles: Articles can be in these formats: (i) practitioner case studies; (ii)
reviews of previous bodies of literature; (iii) reviews of conference or other specialist
events; (iv) opinion papers; (v) topical commentaries and; (vi) book reviews.
Manuscripts should be typed in double-space with wide margins (3 cm). As a general
guide, articles should not exceed 5,000 words, although the Editor retains discretion to
accept longer articles where it is considered appropriate. Please make sure that all
acronyms are clearly defined in brackets the first time they are used.
Title page: This should contain the title of the paper, the name and full
institutional/organisational postal address of each author and an indication of which
author will be responsible for correspondence and proofs (this should also include e-
mail address). Abbreviations in the title should be avoided.
Abstract: This should not exceed 200 words and should be presented on a separate
page (together with the title of the article) summarising the significant coverage and/or
findings.
Keywords: Abstract should be accompanied by five key words or phrases that between
them characterise the contents of the paper. These will be used for indexing and data
retrieval purposes.
Style guidelines: If you are an academic, it is expected that prior to submission your
article will be formatted to the latest standards of the Publication Manual of the
American Psychological Association (APA). If you are not an academic, there is no
requirement for your work to conform to the format standards of the APA, however,
you must reference your article (where appropriate) and the Editor/s will format it prior
to publication (should it be required). Any consistent spelling style is acceptable. Use
single quotation marks with double within if needed. If you have any questions about
references or formatting your article, please contact the Editor, Kirk Luther,
Figures: All figures should be numbered with consecutive Arabic numerals, have
descriptive captions and be mentioned in the text. Figures should be kept within the
text. It is the author’s responsibility to obtain permission for any reproduction from
other sources.
Preparation: Figures must be of a high enough standard for direct reproduction with all
the lettering and symbols included. Axes of graphs should be properly labelled and
91

appropriate units given. Photographs intended for half-tone reproduction must be high
resolution.
Size: Figures should be planned so that they reproduce to 10.5 cm column width. The
preferred width of submitted drawings is 16 – 21 cm with capital lettering 4 mm high,
for reduction by one-half. Photographs for halftone reproduction should be
approximately twice the desired size.
Tables: Tables should be clearly typed with double spacing and should be kept within
the text. Tables should have consecutive Arabic numerals and give each a clear
descriptive heading. Avoid the use of vertical rules in tables. Table footnotes should be
typed below the table, designated by superior lower-case letters.
Copyright and Author Rights: It is a condition of publication that authors assign
copyright or license the publication rights in their articles, including abstracts, to the
iIIRG BEFORE the article or case study can be published in II-RP. This enables the
iIIRG to ensure full copyright protection and to disseminate the article, and of course
the Journal, to the widest possible readership in electronic format (and occasionally
print) as appropriate. Authors are, themselves, responsible for obtaining permission to
reproduce copyright material from other sources. Download the iIIRG Copyright
Agreement, complete and sign it, then return to the Editor, Kirk Luther, electronically
at [email protected] (please mention the article/case study title in your email so
that it can be easily identified).
Exceptions are made for certain Governments’ employees whose policies require that
copyright cannot be transferred to other parties. We ask that a signed statement to this
effect is submitted when returning proofs for accepted papers.
92

Appendix G*: Ethics letter of approval from UOL, UK
93
94

Appendix H*: Norwegian ethics approval from Regional committee for medical
and health related research ethics (written in Norwegian)
From: [email protected] <[email protected]>
Sent: Thursday, September 12, 2019 2:26 PM
To:
Subject: Svarbrev
Alle skriftlige henvendelser om saken må sendes via REK-portalen
Du finner informasjon om REK på våre hjemmesider rekportalen.no
Region:
REK midt
Saksbehandler: Vår dato:
12.09.2019
Vår referanse:
7168
Deres referanse:
7168 Empati, resiliens og omsorgstrettet hos etterforskere av overgrep mot barn
Forskningsansvarlig: Norges teknisk-naturvitenskapelige universitet
Søker:
Søkers beskrivelse av formål:
Vold og overgrep mot barn er et prioritert område. For å kunne prioritere dette, må
fokuset rettes mot de som jobber med å etterforske disse sakene. Tidligere forskning har
vist at denne type arbeid kan være helseskadelig, også for ansatte i politiet, som anses
som en gruppe som er spesielt motstandsdyktig når det gjelder stress. Det er begrenset
med forskning på hvilke faktorer som er avgjørende for den totale belastningen i slike
yrker, men studier fra USA, samt foreløpige funn fra en kvalitativ studie fra Trøndelag
politidistrikt (STRESOB), indikerer at arbeidets organisering og støtte fra kollega og
leder er avgjørende. I denne studien vil det fokuseres både på personlige og
organisatoriske ressurser, hos etterforskere med og uten spesialisering i tilrettelagte
avhør av barn. Studien vil inkludere ansatte i politiet i Norge og Storbritannia. Funnene
fra dette forskningsprosjektet vil kunne bidra til optimal organisering av arbeidet med å
etterforske vold og overgrep mot barn.
REKs vurdering
95
Vi viser til søknad om forhåndsgodkjenning av ovennevnte forskningsprosjekt.
Søknaden ble behandlet av Regional komité for medisinsk og helsefaglig
forskningsetikk (REK midt) i møtet 21.08.2019. Vurderingen er gjort med hjemmel i
helseforskningsloven § 10.
Forsvarlighet: Vi har vurdert søknad, forskningsprotokoll, målsetting og plan for
gjennomføring. Under forutsetning av at du tar vilkårene nedenfor til følge vurderer vi
at prosjektet er forsvarlig, og at hensynet til deltakernes velferd og integritet er ivaretatt.
Forbedring av informasjonsskriv
- Opplys hvor lang tid det vil ta å besvare spørreskjemaet.
- Opplys om at studien innebærer et samarbeid med Storbritannia.
Prosjektets varighet
Prosjektstart og prosjektslutt er i søknaden registrert med samme dato. Vi ber deg om å
sende oss en prosjektendring der du spesifiserer hva sluttdatoen skal være.
Vilkår for godkjenning
1. Revidert informasjonsskriv skal sendes komiteen til vurdering. Vi vil opprette en
oppgave til deg for dette i portalen. Du vil motta en epost fra oss når oppgaven er
opprettet.
2. Komiteen forutsetter at ingen personidentifiserbare opplysninger kan framkomme
ved publisering eller annen offentliggjøring.
3. Komiteen forutsetter at du og alle prosjektmedarbeiderne følger institusjonens
bestemmelser for å ivareta informasjonssikkerhet og personvern ved innsamling, bruk,
oppbevaring, deling og utlevering av personopplysninger.
4. Av dokumentasjonshensyn må du oppbevare opplysningene i 5 år etter prosjektslutt.
Opplysningene skal oppbevares avidentifisert, dvs. atskilt i en nøkkel- og en datafil.
Opplysningene skal deretter slettes eller anonymiseres.
Vedtak
Godkjent med vilkår
96
Appendix I*: Participant information sheet
97

98

Appendix J*: Online consent form
99

Appendix K*: Complete online questionnaires, with public measures.
100

101

102

103

104
105
106
107
108
109
References
Baron-Cohen, S., & Wheelwright, S. (2004). The empathy quotient: An investigation of
adults with Asperger syndrome or high functioning autism, and normal sex
differences. Journal of Autism and Developmental Disorders, 34(2), 163–175
Eisenberger, R., Huntington, R., Hutchison, S., & Sowa, D. (1986). Perceived
organizational support. Journal of Applied Psychology, 71(3), 500-507.
Eisenberger, R. (2019) Perceived Organizational Support.
http://classweb.uh.edu/eisenberger/perceived-organizational-support/ Retrieved
on 12th February 2019
Stamm, B. H. (2010). The concise ProQOL manual, 2nd ed. Pocatello, ID: ProQOL.org.
Zigmond, A.S. & Snaith, R.P. (1983). The Hospital Anxiety and Depression Scale. Acta
Psychiatrica Scandinavica. 67(6)
110
Appendix L: Exploration of missing dataThe missing gender data was explored using a one-way between subjects ANOVA,
coding data as male, female and missing. The effect of gender was explored to compare
means of CS, STS, burnout, anxiety, depression, empathy and perceived organisational
support. There was no significant effects of gender with an alpha value set at p=.01; CS
(F(2,89)=.094, p=.911), STS (F(2,89)=.012, p=.988), burnout (F(2,89)=2.499, p=.088),
anxiety (F(2,89)=.632, p=.534), depression (F(2,89)=.156, p=.856), empathy
(F(2,89)=.462, p=.632) and perceived organisational support (F(2,89)=.193, p=.825).
These data suggest that the missing gender data did not significantly differ from the data
reported as male or female.
111
Appendix M: Evaluation of assumptions.
After missing data were addressed, data were then explored to determine whether
statistical assumptions for parametric analyses were met. Normality was assessed by
checking histograms, Q-Q plots, box plots, skewness and kurtosis values. No significant
findings were found in skewness, but there were significant findings of negative and
positive values for kurtosis. Several outliers were identified in box plots and histograms.
The Kolmogorov-Smirnov test, which is preferred to Shapiro-Wilk because N exceeded
50 (Clark-Carter, 2010), further indicated non-normality. For t-tests, Levene’s statistics
were also referred to for each of the comparative variables.
Assumptions were explored for bivariate correlations, to examine linearity,
homoscedasticity and type of data scales (interval and ratio). Gender data was included
as nominal data, as the data was coded in two levels. Scatterplots indicated that
homoscedasticity was present. Given violations of normality and linearity, a
Spearman’s rho correlation was chosen.
To undergo linear regressions, assumptions of multivariate normality,
multicollinearity and homoscedasticity were explored. Two outcome variables were
found to be normally distributed. A multiple regression was completed for the CS
model with three predictor variables (anxiety, EQ and SPOS) and a Simple linear
regression for the STS model with one predictor (anxiety). Both models met all
assumptions when examining multicollinearity, P-P plots, scatterplots, std. residuals and
Cooks distance. The outcome variable burnout with two predictor variables (anxiety and
depression), failed the assumption of normality. Other assumptions were met when
examining standard residuals, and ANOVA indicated significant linear relationship.
112
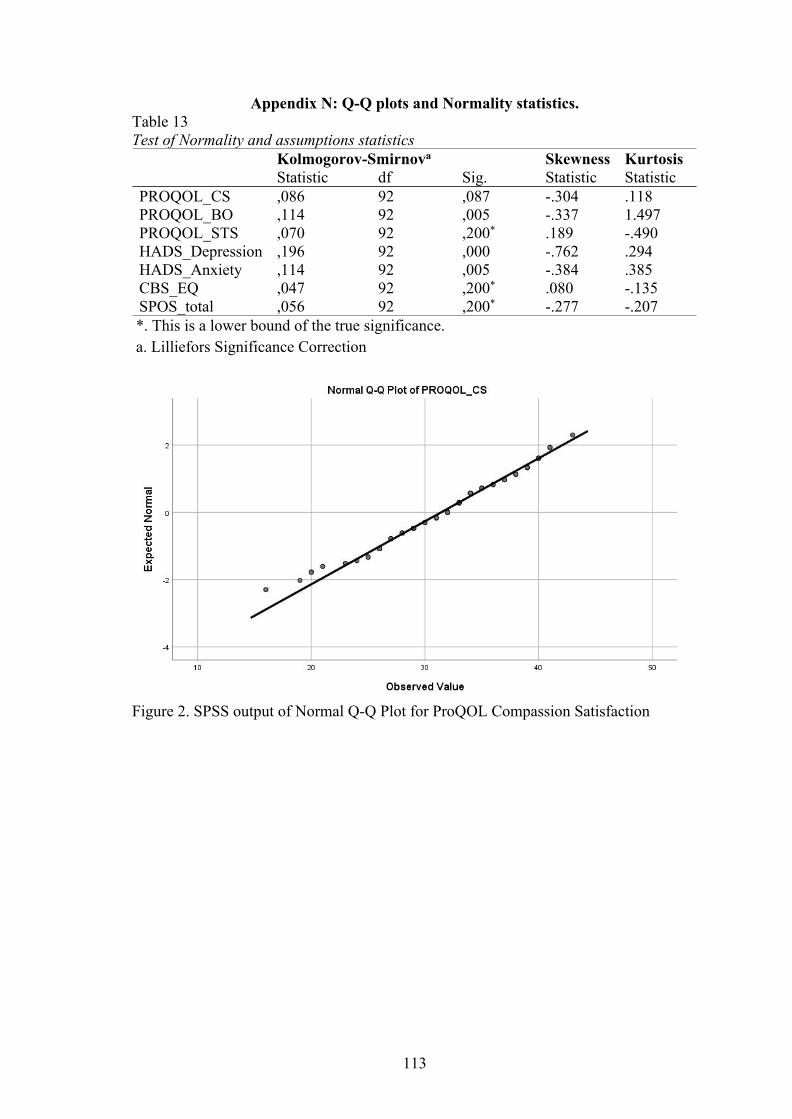
Appendix N: Q-Q plots and Normality statistics.Table 13Test of Normality and assumptions statistics
Kolmogorov-Smirnova Skewness KurtosisStatistic df Sig. Statistic Statistic
PROQOL_CS ,086 92 ,087 -.304 .118PROQOL_BO ,114 92 ,005 -.337 1.497PROQOL_STS ,070 92 ,200* .189 -.490HADS_Depression ,196 92 ,000 -.762 .294HADS_Anxiety ,114 92 ,005 -.384 .385CBS_EQ ,047 92 ,200* .080 -.135SPOS_total ,056 92 ,200* -.277 -.207*. This is a lower bound of the true significance.a. Lilliefors Significance Correction
Figure 2. SPSS output of Normal Q-Q Plot for ProQOL Compassion Satisfaction
113
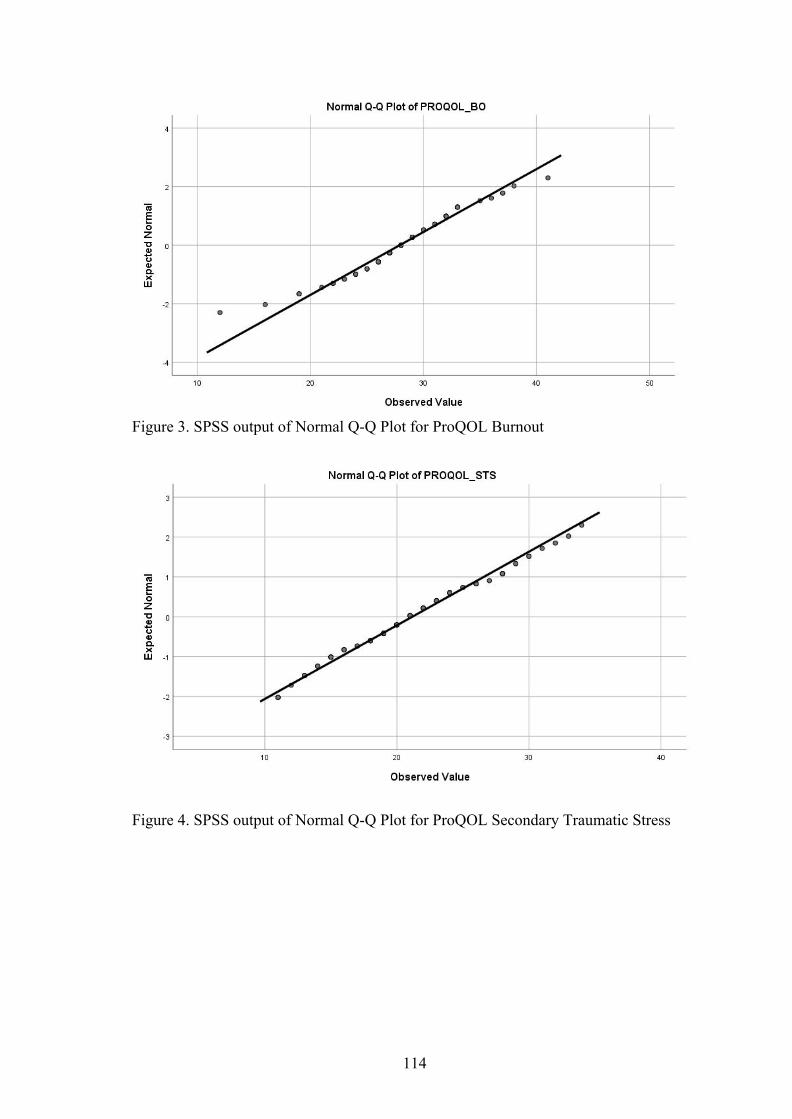
Figure 3. SPSS output of Normal Q-Q Plot for ProQOL Burnout
Figure 4. SPSS output of Normal Q-Q Plot for ProQOL Secondary Traumatic Stress
114
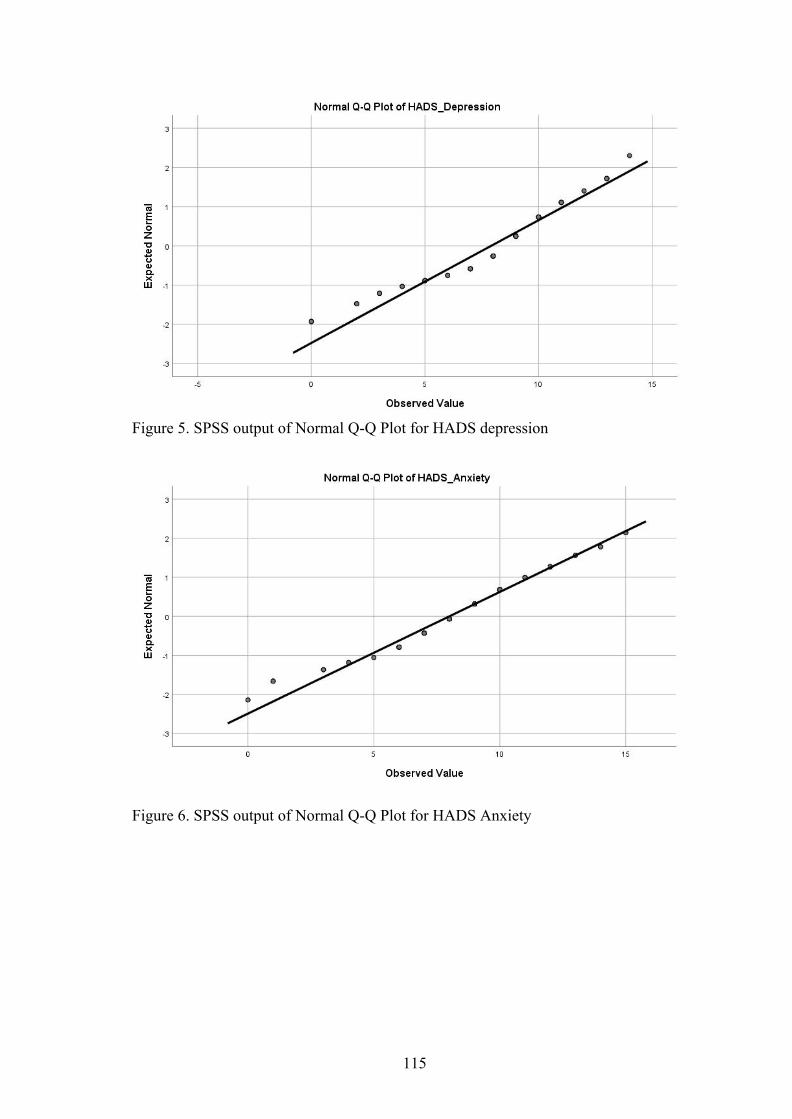
Figure 5. SPSS output of Normal Q-Q Plot for HADS depression
Figure 6. SPSS output of Normal Q-Q Plot for HADS Anxiety
115
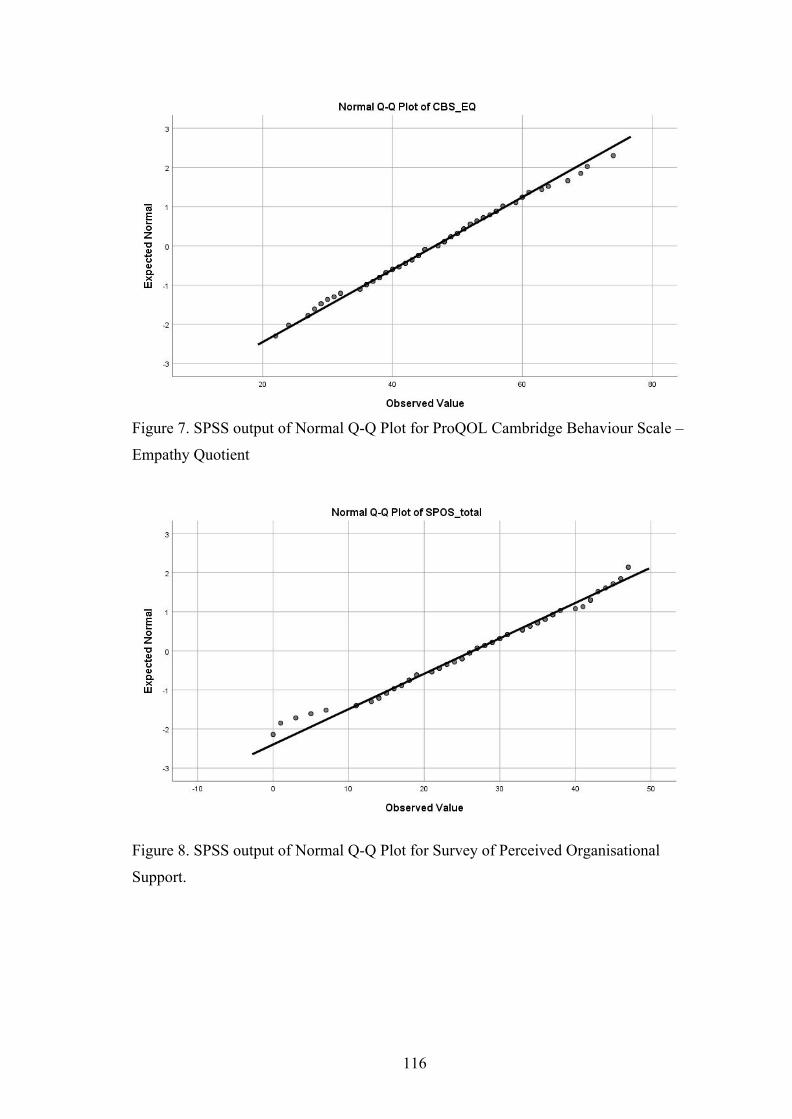
Figure 7. SPSS output of Normal Q-Q Plot for ProQOL Cambridge Behaviour Scale –
Empathy Quotient
Figure 8. SPSS output of Normal Q-Q Plot for Survey of Perceived Organisational
Support.
116

Appendix O*: Checklist assuring confidentiality and anonymity of participants.
Checked in
Executive
Summary/
Abstract/ Overview
(If included in
assignment)
Checked
in main
text
Checked in
appendices
Pseudonym or false initials used
N/A N/A N/A
Reference to pseudonym/false
initials as a footnote N/A N/A N/A
Removed any reference to names of
Trusts/ hospitals/ clinics/ services
(including letterhead if including
letters in appendices)
Removed any reference to names/
specific dates of birth/ specific date
of clinical appointments/
addresses/location of client(s),
participant(s), relatives, caregivers,
and supervisor(s). For research thesis
– supervisors can be named in the
research thesis “acknowledgements”
section.
Removed/altered references to
client(s) jobs/professions /nationality
where this may potentially identify
them. [For research thesis – removed
potential for an individual research
participant to be identifiable (e.g., by
a colleague of the participant who
might read the thesis on the internet
and be able to identify a participant
117
using a combination of the
participants specific job title, role,
age, and gender)]
Removed any information that may
identify the trainee (consult with
course staff if this will detract from
the points the trainee is making)
N/A N/A N/A
No Tippex or other method has been
used to obliterate the original text –
unless the paper is subsequently
photocopied and the trainee has
ensured that the obliterated text
cannot be read
The "find and replace" function in
word processing has been used to
check the assignment for use of
client(s) names/other confidential
information
118

Appendix P*: Chronology of research process
Dates Research activity
January 2018 Research proposal form submitted to University.
Research supervisor allocated.
May 2018 Initial research proposal submitted.
June 2018 Panel review meeting of initial research proposal.
July –
November 2018
Development of research proposal
December 2018 University peer review process completed.
February 2019 Service user review completed
May 2019 Ethical approval and sponsorship from University of Leicester for
English data.
October 2019 –
March 2020
Recruitment for empirical study.
September 2019 Ethical approval from REK in Norway.
October 2019 1st draft of systematic literature review.
February 2020 Final draft of systematic literature review
May 2020 Received data from Norway
June 2020 Thesis submitted to University of Leicester (04.06.2020)
July 2020 Research viva
July –
September 2020
Preparation and submission of work for publication
119

Appendix Q*: Statement of epistemological position taken
The researcher adopted a positivist epistemological position for both the literature
review and the research report. Positivism considers research as an objective empirical
truth that can be scientifically verified, preferably by making use of logical and
mathematical proof (Cohen et al., 2013). Variables are considered as objective
constructs, which are measured using validated measurable methods. The proposed
research questions and chosen methodological measures and procedure considered
quantifiable data, where statistical analyses were used to inform interpretation and
drawing conclusions.
Prior to carrying out this project, the researcher had limited knowledge and
experience in the field of occupational distress and secondary trauma, both regarding
the legal professions and law enforcement. As such, the researcher was perceived to
have an objective viewpoint to the research findings and holding limited prior
conceptions. In addition, the research was kept independent from any data-collection or
possible participants who completed self-reporting questionnaires via an online survey.
Although a positivistic stance can be helpful to identify and quantify reported or
observable trends in a population, some limitations of the model are still acknowledged.
The empirical nature of the positivistic model can limit potential understanding of
personal experience and meaning-making which is not specifically captured by the
measures.
Cohen, L., Manion, L., & Morrison, K. (2013). Research methods in education. New
York: Routledge.
120