employer administrative guide
TRANSCRIPT

EMPLOYERADMINISTRATIVE GUIDE

www.calchoice.comwww.calchoice.com
What’s Inside:Contact Information ........................................................................................................................................2
Member Privacy Statement ....................................................................................................................................3-4
Top Coverage Issues ........................................................................................................................................6
Coverage Eligibility Requirements ........................................................................................................................................7
Administration Basics NewHireEnrollment..................................................................................................8 LateEnrollee................................................................................................................9 Rehires..........................................................................................................................9 MilitaryLeave...............................................................................................................9 Voluntary/InvoluntaryTermination—Employees................................................ 10 UnderstandingYourBenefitChoices................................................................... 11
Family Coverage DependentEligibility................................................................................................ 12 DomesticPartnerEligibility................................................................................... 13 ChildrenOfDomesticPartnerEligibility.............................................................. 13 TerminatingDependents........................................................................................ 14 TerminatingOver-AgeDependents...................................................................... 14 SpecialEnrollmentPeriods.................................................................................... 15
Change in Family Status NewDependent(s)Enrollment.............................................................................. 16
Change in Group Policy GroupChangeGuidelines................................................................................17-18
About COBRA and Cal-COBRA EmployersSubjectToCOBRA(Federal)............................................................. 19 DomesticPartnerEligibilityUnderCOBRA......................................................... 20 EmployerResponsibilitiesForCOBRA................................................................. 20 EmployersSubjectToCal-COBRA(State)......................................................... 21 DomesticPartnerEligibilityUnderCal-COBRA................................................. 21 Employee/DependentResponsibilities................................................................ 22 EmployerResponsibilitiesForCal-COBRA......................................................... 22 LengthOfEligibilityContinuationOfCoverage.................................................. 23 HIPAA......................................................................................................................... 23
Billing YourPremiumStatement...................................................................................... 24 TheBillingCycle...................................................................................................... 25 RateSchedule.......................................................................................................... 25 Credits/Fees............................................................................................................. 25 GroupCancellations................................................................................................ 25
Annual Renewal Timeline ..................................................................................................................................... 26
Ancillary and Voluntary Benefits Dentegra®SmileClub............................................................................................ 27 VoluntaryDentalProgram...................................................................................... 28 VoluntaryVisionProgram...................................................................................... 28 EyeMedVisionDiscountProgram........................................................................ 28Ancillary Benefits ChiropracticAndAcupuncturePrograms........................................................... 29 Section125PremiumOnlyPlan(POP)............................................................. 29 EmployeeLifeInsurance........................................................................................ 30 ClaimFilingProcedures(LossofLife)................................................................ 30 AncillaryDental..................................................................................................31-33
Frequently Asked Questions GeneralInformation................................................................................................. 34 HMO............................................................................................................................ 35 PPO............................................................................................................................. 36 DentegraSmileClub............................................................................................... 36 MetLifeDHMOMET100&MET185,SmileSaverDHMO1000&3000...... 37 AmeritasPPO3000,3500,4000,&5000....................................................... 37
Supply Request Form ..................................................................................................................................... 38

1www.calchoice.com
We’reproudtobeapartofyourhealthprogram!
During the coming coverage year, it’s inevitable that you’ll be presented with
a question or situation that needs clarification. This Employer Administrative
Handbook is intended to guide you through different administrative procedures,
as well as answer general questions about the CaliforniaChoice program. Please
feel free to call our Customer Service Center at (800) 558-8003 if you need
furtherassistance.
Although your application for coverage and monthly billing are processed
by CaliforniaChoice, the Group Service Agreement (contract) for your health
coverage is with each of the applicable Health Plans in the CaliforniaChoice
program. Group Service Agreements from each participating Health Plan are
available on www.calchoice.com. Some of the Agreements may require your
signature. TheAgreements shouldbe retainedwith thisEmployerAdministrative
Handbookforfuturereference.
Keep In A Safe Place
Welcome To CaliforniaChoice®
www.calchoice.com

2
HMO
AnthemBlueCross................................................................................................. (855)383-7248 English/Español,Mon-Fri8:30a.m.-7:00p.m.
HealthNet................................................................................................................. (800)361-3366 English/Español,Mon-Fri8:30a.m.-5:00p.m.
KaiserPermanente................................. English(800)464-4000-Español(800)788-0616 7daysaweek7:00a.m.-7:00p.m.
SharpHealthPlan................................................................................................... (800)359-2002 English/Español,Mon-Fri8:00a.m.-5:00p.m.
SutterHealthPlus................................................................................................... (855)315-5800 English/Español,Mon-Fri8:00a.m.-7:00p.m.
UnitedHealthcare..................................................................................................... (800)624-8822 English/Español,Mon-Fri8:00a.m.-9:00p.m.
WesternHealthAdvantage.................................................................................... (888)563-2250 English/Español,Mon-Fri8:00a.m.-5:00p.m.EPO
AnthemBlueCross................................................................................................. (855)383-7248 English/Español,Mon-Fri8:30a.m.-7:00p.m.
Cigna+Oscar......................................................................................................... (855)672-2789 English,Mon-Fri8:00a.m.-8:00p.m.;Sat.-Sun9:00a.m.-5:00p.m.
Oscar.......................................................................................................................... (855)672-2755 English,Mon-Fri8:00a.m.-8:00p.m.;Sat.-Sun9:00a.m.-5:00p.m.PPO
AnthemBlueCross................................................................................................. (855)383-7248 English/Español,Mon-Fri8:30a.m.-7:00p.m.Dental
Ameritas.................................................................................................................... (877)203-0036 English/Español,Mon-Thurs5:00a.m.-10:00p.m.;Fri.5:00a.m.-4:30p.m.
Dentegra®SmileClub............................................................................................. (877)280-4204English/Español,Mon-Fri4:15a.m.-5:00p.m.
MetLife&SmileSaverSM.......................................................................................... (800)880-1800English/Español,Mon-Fri8:00a.m.-5:00p.m.
Vision
EyeMedVoluntaryVision...................................................................................... (866)299-1358 English/Español,Mon-Fri8:00a.m.-6:00p.m.
EyeMedVisionDiscountProgram...................................................................... (866)723-0391 English/Español,Mon-Fri8:00a.m.-6:00p.m
VSPVoluntaryVision.............................................................................................. (800)877-7195 English/Español,Mon-Fri5:00a.m.-7:00p.m.;Sat.6:00a.m.-2:30p.m.
Chiropractic/Acupuncture
LandmarkHealthplan.............................................................................................. (800)298-4975 English/Español,Mon-Fri5:00a.m.-5:30p.m.
Contact InformationEmployers:Administrativeandbillingquestions?(800)558-8003
Employees:
www.calchoice.com

3www.calchoice.com
Member Privacy StatementCaliforniaChoice® is proud to provide quality employee benefit products andservices to our customers. Keeping your personal information secure andprotecting your privacy rights are important to you, and it is one of our toppriorities. This statement tells you about the information we request from ourcustomers. It also tells you how we safeguard the personal information andprotecttheprivacyrightsofourcurrentandformercustomers.
Our Privacy Commitment to YouCaliforniaChoice will safeguard your personal information and protect theprivacy rights of our customers in accordance with state and federal laws.Wewillaccomplishthisinwaysthatarereasonableandconsistentwithsoundbusinesspractices.
Protecting Your Health InformationWe do not share your personal health information (such as medicalquestionnaires)exceptwhennecessary toconductunderwriting reviewsat thetime of your Employer’s initial enrollment through CaliforniaChoice or upon anEmployer requested underwriting review at a subsequent renewal. In certaincircumstances,wemay share your personal health information if permitted orrequiredbylaw.
CaliforniaChoiceiscommittedtoprotectingtheconfidentialityandsecurityofyourprivate health information. We maintain physical, electronic, and processsafeguardsthatrestrictunauthorizedaccesstoyourpersonalhealthinformation.Thesesecurityprocedures include lockedfilesand informationsystemsecuritymeasuressuchasuserpasswords,dataencryptionorfirewalltechnology.CaliforniaChoice employees are required to comply with our policies andprocedurestoprotecttheconfidentialityofyourpersonalhealthinformation.Anyemployee who violates our privacy policy is subject to a disciplinary process.
Employeeaccesstoprivateinformationislimitedonabusiness“need-to-know”basis such as: when necessary to conduct underwriting reviews, or foranonymousstatisticalanalysis.
Information About Our CustomersCaliforniaChoice receives information about you in order to provide customerservice, offer new products or services, administer our products, and fulfillotherlegalandregulatoryrequirements.Wewillprovideyouwithaccesstothisinformation and the ability to review, amend, correct or copy this information,ifwearerequiredtodosounderstateandfederallaw.Themethodsweusetoprotect this information are similar to those described above to protect yourhealthinformation.
The information we receive may vary by product; therefore, the examples thatfollow may not apply to all customers but are designed to show the generalcategories of information that may be received and maintainedbyCaliforniaChoice: n Informationprovidedby you on applications, forms, surveys and our
Websites,suchasyourname,address,dateofbirth,SocialSecuritynumber,gender,maritalstatusanddependents.
n Informationprovidedbyyouremployer. n Information about your transactions and experiences with
CaliforniaChoice such as: products or services purchased, accountbalances,paymenthistory,policycoverage,andpremiums.
(CONTINUED)
www.calchoice.com

www.calchoice.com www.calchoice.com4
Information Shared Within the Word & Brown Family of Companies While understanding the importance of protecting your personal information,certaininformationwillneedtobesharedduringthenormalcourseofbusiness.We may disclose to the extent permitted by law the personal informationwe receive about you, as described above, within the Word & Brown familyofcompanies.
Information Shared with OthersWemaydisclosethepersonalinformationwereceive,asdescribedabove,tothefollowingtypesofthirdparties: n Other third parties as permitted or required by law, such as for
compliancewithasubpoena,fraudprevention,orinquiriesfromstateorfederalregulatoryagencies.
n Financialservicecompanieswithwhomwehaveagreements,suchas:insurancecompanies,insurancebrokersoragents,administrators,andserviceproviders.
We maintain written contracts with third parties to help ensure that thepersonal information we share about our customers is used for a legitimatebusinesspurpose.
Access and Amendment of Your RecordsYouhavetherighttoaccessandamendyourrecords.Youmayexercisethisrightbyrequestingtousinwritingtoaccessand/oramendyourrecords.Pleasesendsuchrequeststo:
CaliforniaChoice®
721SouthParker,Suite200Orange,CA92868
Changes to our Notice of Privacy Policy and Insurance Information PracticesWereserve the right tochangeourprivacypoliciesand insurance informationpractices.Ifwemakeanychangestoourpoliciesorpractices,wewillprovideyouwithacopyofarevisednoticeasrequiredbyapplicablelaw.
Our CommitmentCaliforniaChoicevaluesyouasacustomer,andwearecommittedtobringingyou products and services that help you to feel healthier and more secure.Ourgoal is to alwaysuse your information in a responsiblebusinessmanner.If there are state and federal law requirements that prohibit sharing yourinformation without your written permission, CaliforniaChoice will complywiththoserequirements.
We maintain physical, electronic, and process safeguards that restrict unauthorized access to your personal health information.
Member Privacy Statement

5
Accessforms,directories,Doctor/Rxsearch,andplaninformation24/7.
Completeup-to-dateinformationisjustaclickaway.
Find what you need fast at www.calchoice.com
Pleasebeadvisedthatsomeformsandwrittencommunicationsareavailableonourwebsitein
the following languages: Chinese, Korean, Russian, Spanish, Tagalog, and Vietnamese.
Employees can register their applicable, Plan-specific preferred language by completing the
LanguageAssistancePreferenceFormalsofoundonourwebsitewww.calchoice.com.
www.calchoice.com www.calchoice.com

www.calchoice.com6
Top Coverage IssuesMostserviceproblemsexperiencedbyemployeescanbeeasilyavoidedwitha littlepreventiveattention.Hereare themostcommonlyoverlookeditemsthatcancausedelaysorcoveragelapses:
n UnsignedApplicationsorChangeRequestForms
n Forgettingtoaddnewborns/newspousestocoverage
n Omittinginformationonforms,suchasdateoffull-timeemployment,dateofbirth,etc.
n Notselectingahealthplan/benefitlevel
n NotselectingaPrimaryCarePhysician(PCP)
n Notelectingdependentcoverage
n Notcompletingawaiverfordependents
n Notensuringthatcheckboxesareclearlymarkedonforms
n Notusingtheproperforms

7
Fourconditionsmustbemetforanemployeetogainandkeepcoverage.Everyemployeemust:
1 Meet the employer’s selected waiting period
2 Be permanent and actively working an average of 30+ hours per week over the course of a month, at the small employer’s regular place of business or 20+ hours per normal work week for at least 50% of the weeks in the previous calendar quarter.
3 Be a permanent employee who is not eligible for medical healthcare coverage offered by or through a labor union
4 Be paid on a salary/hourly basis (not 1099, commissioned or substitute)
Coverage Eligibility Requirements
www.calchoice.com

www.calchoice.com www.calchoice.com8
n Theemployercane-mail,faxormailtheoriginaltoCaliforniaChoiceassoonaspossible,butnomorethan90daysprioror30daysaftertheemployee’s effective date of coverage (please retain a copy of thecompletedapplicationforyourrecords).
Fax: (714)558-8000 Mail:CaliforniaChoice 721SouthParker,Suite200 Orange,CA92868 E-mail:[email protected]
n Coverage for new employees and their dependents will be effective on the first day of the month following the completion of thegroup’swaitingperiod,nottoexceed90daysfromthedateofhire.
n New employees will be mailed one or more information packets to their residence which will include ID card(s); a description of their selectedbenefitplans;andinstructionsonhowtousetheplans.
Note: Please contact CaliforniaChoice Customer Service Center within 7 businessdaystoconfirmreceiptofallmaileditems.
New Hire Enrollment Benefit eligibility is based on the completion of the waiting period by newemployees. Employersmay request aNewHire EnrollmentQuoteRequest fornewemployees at any time.Alongwith this handbook, your employer packetincludesNewHireEnrollmentQuoteRequestformsandEnrollmentApplications.
Enrolling a New Hire is Easy:
n CompletetheNew Hire Enrollment Quote Requestformandfaxitto(714)953-4097toobtainacustomizedenrollmentquotefornewemployees. The enrollment quote will be returned to your attentionwithin a few days, along with an Enrollment Guide and EmployeeEnrollmentApplication.
n Foran immediatequote,visitourwebsiteat:www.calchoice.com,login,select“managemyaccount”and“newhirequote.”
n Employees who wish to obtain coverage through CaliforniaChoice®
mustcompletetheEnrollment Application.
n Employersshouldprovidethegroupnumberinthetopsectionofthefrontpageoftheapplication.
Administration Basics
Waiving Coverage: It is extremely important that employees wishing towaive coveragecomplete the CaliforniaChoice Medical / Dental WaiverportionoftheEnrollmentApplicationadvisingthemoftheirlegalrights.Pursuantto the Knox Keene Act, Section 1357(d)(4)(A), employees wishing to waivecoveragemust execute a written waiverandEmployers are required to maintain that waiver on file. Waivers may also be submitted toCaliforniaChoiceviafaxat(714)558-8000forretentioninourfiles.
Shouldtheemployeeseekcoverageaftertheireligibilityperiodandtheemployerfailedtoobtainthewaiver, theEmployer may be held liable for thecostofhealthcareservicestheEmployeelaterincurs.
Life Insurance: When employers offer life insurance, ALL employees considered eligible for medical coverage must enroll in life insurance coverage even if they do not wish to enroll in medical or dental coverage through CaliforniaChoice. Please have each employee completetheEmployeeEnrollmentApplicationforlifeinsurancecoverage.
Important
Example:JanewashiredonMarch 2nd. Thegrouphasa60-daywaitingperiod.JanewillcompletethewaitingperiodonApril30th.Jane’seffectivedatewillbeMay1sttoensurethewaitingperioddoesnotexceed90days.
Example:JanewashiredonMarch 5th. Thegrouphasa60-daywaitingperiod.JanewillcompletethewaitingperiodonMay3rd.Jane’seffectivedatewillbeJune1st.
(CONTINUED)

www.calchoice.com www.calchoice.com 9
Employee/dependents had previously waived enrollment* due to other coverage in force but lost that coverage. Lossofcoveragemustresultfromcircumstancesbeyondtheindividual’scontrol.
Late EnrolleeCaliforniaChoice®willallowaddinganemployeeand/ordependentsotherthanduringRenewalIFthe:
Employees must provide the following documentation and submit eachitem to CaliforniaChoice within 60 days of change in family statusor loss of coverage:
n An Enrollment Application (for employee and dependents) n AChange Request Form(dependentsonly) n Proofoflossofothercoverage(i.e.,HIPAACertificate) n Proofofchangeinfamilystatus(i.e.,marriagecertificate,
DeclarationofDomesticPartnership**,birthcertificate,legaladoptiondocumentation)
Coveragewillbeeffectiveasfollows:Change of Family Status:Marriage/DomesticPartnership/Stepchild—Ifallrequireddocumentationisreceivedbeforethe16thdayofthemonthofmarriage/establishmentofdomesticpartnership,premiumsarechargedforthefullmonthandcoveragebeginsonthedateofmarriage/establishmentofdomesticpartnership.Ifallrequireddocumentationisreceivedonorafterthe16thdayofthemonthofmarriage/establishmentofdomesticpartnership,coveragebeginsonthe1stofthemonthfollowingthedateofreceipt.
Birth, Adoption, Legal Guardianship, Eligible Dependent Child — If birth/date of placementoccurredbeforethe16thofthemonth,coveragebeginson1stdayof themonthof thedateof their birth/placement. If birth/date of placement occurred on the 16th or after, child isautomatically covered at no cost underSubscriber betweendate of birth/placement and the1st of the following month. Coverage for the dependent begins on the 1st of the monthfollowingthebirth/dateofplacement.
** IfdomesticpartnershavefiledaDeclarationofDomesticPartnershipandhavenotyetreceivedacopyfromthestate,asignedAffidavitofDomesticPartnershipwillbeaccepted.DomesticPartnersagreetoprovideacopyoftheDeclarationofDomesticPartnershipwithin60daysofissuance.
NOTE:TherewillbesomebenefitrestrictionsforAmeritasDentalPPO3000,3500,4000and5000.
*Submittedmedical/dentalwaiver
1Employee/dependents declined to enroll previously* due to other coverage in forceandEmployercontributionstowardthatcoveragehavebeenexhaustedordramaticallyreduced.2Employee declined to enroll previously* butthenexperiencedachangeinfamilystatus(i.e.,employeegotmarried,enteredintoadomesticpartnership,gavebirth,adoptedachild,orestablishedaparent-childrelationship).3
How To Obtain Coverage As A Late Enrollee:
Administration BasicsRehiresA former employee who has been rehired may be eligible for re-enrollmentwithoutcompletingthewaitingperiodifheorshemeetsthefollowingcriteria:
• Employeepreviouslycompletedyourcompany’swaitingperiod
• Employeehasbeenrehiredwithinsixmonthsofleavingthecompany
• Rehiredemployeeshavethesameenrollmentoptionsasnewhires
Anenrollmentapplicationmustbereceivedwithin60 daysoftheemployee’sreturntowork,accompaniedbyawrittenrequesttowaivethewaitingperiodandproofoffull-timeemployment.Coveragewillbeeffectivefirstofthemonthfollowingtherehiredate.
PLEASENOTE:Iftheemployeedoesnotmeetthecriteriaindicatedabove,thencoveragewillbecomeeffectivefirstof themonthfollowingcompletionofthecompany’swaitingperiod.
Return from Military Leave or California National GuardAnemployeewhowaspreviouslycoveredundertheplanandhasreturnedfromMilitary Leave or California National Guard will be allowed to re-enroll intocoveragewithoutcompletingthewaitingperiod.Anenrollmentapplicationmustbereceivedwithin60daysoftheemployee’sreturntowork,accompaniedbyawrittenrequesttowaivethewaitingperiodandproofoffull-timeemployment.Coveragewillbeeffectivefirstofthemonthfollowingthedateofreturn.
(CONTINUED)

www.calchoice.com10
Voluntary Termination—EmployeesAn employee may choose to voluntarily withdraw coverage for themselvesand/or their dependents by completing and submitting a Change Request FormtoCaliforniaChoice®.Therequestmustbereceivedwithin30daysfromthe date the Change Request form was signed. The request will become effective the last day of the month following receipt of the form by CaliforniaChoice. This type of request will not be processed retroactively.The employee will be ineligible for re-enrollment until the Renewal period.
Involuntary Termination—EmployeesAll employees who become ineligible for group coverage must be terminatedfrom the group plan. Employers must complete an Employee Termination Notification Form, and submit to CaliforniaChoice within 30 days fromthelastdayemployed.
Cal-COBRA law requires you, as the employer, to notify CaliforniaChoice of all employee terminations within 30 days from their last day employed.
Coverage will cease at the end of the month following the last day employed, for the employee and his/her dependents.
3 Ways to Notify CaliforniaChoice of an Employee Termination:
For your convenience, you may notify CaliforniaChoice of anemployeeterminationbyusingoneofthesemethods:
1. Faxingore-mailingcompletedEmployee Termination Notification Form* totheCaliforniaChoiceMemberProcessingCenter:
Fax:(714)558-8000 E-mail:[email protected]
2. CompletingtheEmployee Termination Notification Form*onthebackofthepremiumstatementofyourinvoiceandreturningwithyourpremiumpayment.(Retainacopyforyourrecords.)
3. Byvisitingourwebsiteat:www.calchoice.com
<P.S.>Pleasereviewtheinvoicereceivedimmediatelyfollowingyourrequesttoterminatean employee to ensure that youareno longer beingbilled for that employee. Ifemployee and premium appear, please contact the CaliforniaChoice CustomerServiceCenterat(800)558-8003forimmediateassistance.
PleaseDONOTsendnotificationofanemployeeterminationuntilafterthelastdayofemployment.Terminationrequestsmadepriortothelastdayemployedcannotbeprocessed.Also,pleaseDONOTself-adjustyourbillingstatement.PAYMENT,asbilled,willneedtobeMADEINFULL.CaliforniaChoicewillcreditpremiumonthebillingstatementthatfollowstheprocessingofthetermination.
Administration Basics
*FormmustbesignedanddatedbyanauthorizedgroupcontactonfilewithinCaliforniaChoiceinorderfortheterminationrequesttobeprocessed.

11
Understanding Your Benefit Choices
www.calchoice.com
PPOMember
In-NetworkHospitalization
orOut-of-NetworkHospitalization
In-Network Physicians & Specialists
EPOMember
In-NetworkHospitalization
In-Network Physicians & Specialists
EPO Benefit Plan Under an EPO plan, members do not choose a Primary Care Physician (PCP). EPO members can receive their care from any of the in-network doctors and self-refer to in-network specialist.
PPO Benefit Plan
Under a PPO plan, members do not choose a Primary Care Physician (PCP). PPO members may self-refer to specialist. Members can receive care from 2 levels of in-network doctors or go out-of-network for lower benefits.
Out-of-Network Physicians & Specialists
HMOMember
Primary CarePhysician Hospitalization
Specialist
HMO Benefit PlanUnder an HMO plan, all access to specialist and hospitalization must be facilitated through the member’s Primary Care Physician (PCP).
COMPARISON OFHMO, EPO, AND PPO BENEFITS

www.calchoice.com12
New Spouse/ New Stepchild
Family CoverageWho can be covered? Requirements that MUST be met:
(CONTINUED)
Effective dates
n New spouse must be legally married to the employee, copy of marriage certificaterequired
n New stepchild must also meet the dependent children requirements listed in thefollowingsections
Ifallrequireddocumentationisreceivedbeforethe16thdayofthemonthofmarriage,premiumsarechargedforthefullmonthandcoveragebeginsonthedateofmarriage.
Ifallrequireddocumentationisreceivedonorafterthe16thdayofthemonthofmarriage,coveragebeginsonthe1stofthemonthfollowingthedateofreceipt.
Birth/Adoption/Legal Guardianship/
Eligible Dependent Child
Ifbirth/dateofplacementoccurredbeforethe16thofthemonth,coveragebeginson1stdayofthemonthofthedateoftheirbirth/placement.
Ifbirth/dateofplacementoccurredonthe16thorafter,childisautomaticallycoveredatnocostunderSubscriberbetweendateofbirth/placementandthe1stofthefollowingmonth.Coverageforthedependentbeginsonthe1stofthemonthfollowingthebirth/dateofplacement. DisabledDependents:
Dependentswhoareincapableofself-supportbecauseofcontinuousmentalorphysicaldisabilitythatexistedbeforetheagelimitareeligibleforcoverageuntiltheincapacityends.Documentationofdisabilitywillberequested.Oncethechildreachestheagelimitforcoverage,verificationofeligibilitywilloccurannuallyatthechild’sbirthday.
Dependents must meet all requirements listed in order to be eligible for enrollment
MEDICAL,CHIRO,VISIONandMETTLIFE & SMILESAVERDENTALDependenteligibility:n Bornto,astep-childorlegalwardof,adoptedby,orhaveanestablishedparent-child relationshipwiththeeligibleemployee,employeespouseordomesticpartnern Underage26(unlessdisabled,disabilitydiagnosedpriortoage26)AMERITASDENTALDependenteligibility:n Bornto,astep-childorlegalwardof,adoptedby,orhaveanestablishedparent-child
relationshipwiththeeligibleemployee,employeespouseordomesticpartnern FinanciallydependentupontheemployeeperIRSguidelinesn Unmarriedornotinvolvedinadomesticpartnershipn Underage26(unlessdisabled,disabilitydiagnosedpriortoage26)

13
Domestic Partner/ Child of Domestic
Partner
Who can be covered? Requirements that MUST be met:Effective dates
www.calchoice.com
Family Coverage
Dependents must meet all requirements listed in order to be eligible for enrollment
ForaDomesticPartnertoqualify,EmployeeandDomesticPartnermust: n BothhavefiledadulyexecutedDeclarationofDomesticPartnershipwiththeSecretaryof
StateandwillprovidecopiestoCaliforniaChoice®within60daysofitsissue n AgreetonotifyCaliforniaChoiceimmediatelyuponterminationofdomesticpartnership
ChildrenofDomesticPartnermustalsomeetthedependentchildrenrequirementslisted intheprecedingsections.
DuringInitialEnrollmentorGroup’sAnnualRenewal:Coveragebeginsongroup’seffectivedate.
InvoluntaryLossofOtherCoverage:DomesticPartnercanbeaddedoutsideofRenewalonlyifhe/shelosesothercoverageinvoluntarily.Coverageiseffectivethe1stoffollowingmonth.
Mid-YearAddition:Mid-YearAddition:Mid-yearadditionsofadomesticpartnerwillrequireastate-stampedcopyoftheDeclarationofDomesticPartnershipfromtheCaliforniaSecretaryofStatewithin60daysofissuance.IfdomesticpartnershavefiledaDeclarationofDomesticPartnershipandhavenotyetreceivedacopyfromthestate,asignedAffidavitofDomesticPartnershipwillbeaccepted.DomesticPartnersagreetoprovideacopyoftheDeclarationofDomesticPartnershipwithin60daysofissuance.Ifallrequireddocumentationisreceivedbeforethe16thdayofthemonthinwhichthedomesticpartnershipwasestablished,premiumsarechargedforthefullmonthandcoveragebeginsonthedateoftheevent.Ifallrequireddocumentationisreceivedonorafterthe16thdayofthemonthinwhichthedomesticpartnershipwasestablished,coveragebeginsonthe1stofthemonthfollowingthedateofreceipt.
ForCOBRA/Cal-COBRAeligibilityinformationforDomesticPartnersandtheircovereddependents,pleaseseepages20-22

www.calchoice.com14
Terminating DependentsA covered employee’s dependent may lose eligibility for coverage even if theemployee’s coverage continues (i.e., when a dependent child reaches themaximumageforcoverage).Coveragefor thedependent(s)wouldterminateattheendof themonth.ACaliforniaChoice®Change Request Form shouldbesubmittedtoCaliforniaChoiceineachofthefollowingsituations:
n Adivorce,annulment,dissolutionofmarriage,terminationofdomesticpartnershiporlegalseparation†
n Adependentchildceasestoqualifyasadependent
n Deathofemployee
n Medicareentitlementofemployee
Terminationof coveragewill takeplaceat theendof themonth following theevent provided the group notifies CaliforniaChoice of the qualifying/triggeringevent within the timeframe allowed by law (within 60 days from qualifying/triggeringevent).
†If divorce or termination of domestic partnership is not final and
member cancels coverage, dependent cannot be reinstated until
group’s next Renewal.
Terminating Over-age DependentsCoverage for dependent children automatically terminates when they reach aspecifiedage.
A notification letter will be sent to the employee 90 days before theirdependents coverage terminates. The employer is not involved in this processbut should be aware of its occurrence. CaliforniaChoice will advise thedependenttocontacttheGroupPlanAdministratorregardingtheireligibilityforbenefitsunderCOBRAcontinuation.
Your billing statement will be adjusted automatically according to any changeindependentcoveragestatusforeachemployee.
DisabledDependents:Dependents who are incapable of self-support because of a continuous mental or physicaldisability that existed before the age limit are eligible for coverage until the incapacity ends.Documentationofdisabilitywillberequested.Oncethechildreachestheagelimitforcoverage,re-verificationofdisabilitywillberequiredannually.Verificationofeligibilitywilloccurannuallyatthechild’sbirthday.
Family Coverage

15
Belowisalistofthemostcommonlyencounteredqualifying/triggeringevents.TheseeventstriggeraSpecialEnrollmentPeriod,duringwhichanemployeeordependentmaymakeachangetotheirenrollmentduringthecoverageyear.
n Involuntarylossofminimumessentialcoverage(including,butnotlimitedto,thefollowingexamples:lossofotheremployercoverage,lossofCOBRAduetoexhaustion,etc.)
n Marriage/DomesticPartnership
n Birth/Adoption/LegalGuardianship/EligibleDependentChild
n CourtOrder
n Movingoutofcoveragearea
n ReturnfromactivedutyfromMilitaryorCaliforniaNationalGuard
n ReleasefromIncarceration
n EnrollmentorplanchangeonceamonthduetoNativeAmericanstatus
n Otherexceptionalcircumstances(subjecttoCaliforniaChoice®approval)
Qualifying/triggeringeventsthatarenotcoveredunderChangeinFamilyStatus(seenextpage)willbeeffectivefirstofthemonthfollowingreceiptofrequiredformsandnecessarysupportingdocumentationtoCaliforniaChoice.TheemployeemustcompleteandsubmitthenecessaryitemstoCaliforniaChoicewithin60 days of the qualifying/triggering event.
Special Enrollment Periods
www.calchoice.com
www.calchoice.com16
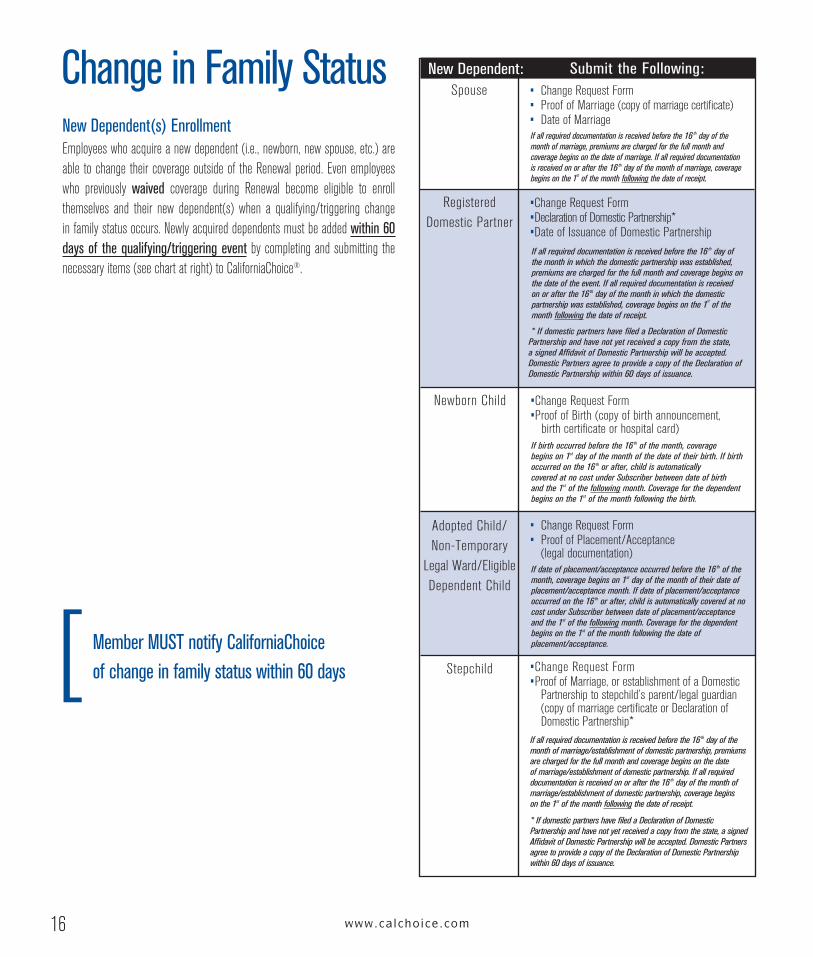
Change in Family StatusNew Dependent(s) EnrollmentEmployeeswhoacquireanewdependent(i.e.,newborn,newspouse,etc.)areable tochange theircoverageoutsideof theRenewalperiod.Evenemployeeswho previously waived coverage during Renewal become eligible to enrollthemselves and their new dependent(s) when a qualifying/triggering changeinfamilystatusoccurs.Newlyacquireddependentsmustbeaddedwithin 60 days of the qualifying/triggering eventbycompletingandsubmitting thenecessaryitems(seechartatright)toCaliforniaChoice®.
Member MUST notify CaliforniaChoice of change in family status within 60 days
Submit the Following:New Dependent:
NewbornChild •ChangeRequestForm •ProofofBirth(copyofbirthannouncement, birthcertificateorhospitalcard)
Spouse • ChangeRequestForm • ProofofMarriage(copyofmarriagecertificate) • DateofMarriage
If birth occurred before the 16 th of the month, coverage begins on 1st day of the month of the date of their birth. If birth occurred on the 16 th or after, child is automatically covered at no cost under Subscriber between date of birth and the 1st of the following month. Coverage for the dependent begins on the 1st of the month following the birth.
RegisteredDomesticPartner
•ChangeRequestForm •DeclarationofDomesticPartnership* •DateofIssuanceofDomesticPartnership
If all required documentation is received before the 16 th day of the month in which the domestic partnership was established, premiums are charged for the full month and coverage begins on the date of the event. If all required documentation is received on or after the 16 th day of the month in which the domestic partnership was established, coverage begins on the 1st of the month following the date of receipt.
AdoptedChild/Non-Temporary
LegalWard/EligibleDependentChild
• ChangeRequestForm • ProofofPlacement/Acceptance (legaldocumentation) If date of placement/acceptance occurred before the 16 th of the
month, coverage begins on 1st day of the month of their date of placement/acceptance month. If date of placement/acceptance occurred on the 16 th or after, child is automatically covered at no cost under Subscriber between date of placement/acceptance and the 1st of the following month. Coverage for the dependent begins on the 1st of the month following the date of placement/acceptance.
* If domestic partners have filed a Declaration of Domestic Partnership and have not yet received a copy from the state, a signed Affidavit of Domestic Partnership will be accepted. Domestic Partners agree to provide a copy of the Declaration of Domestic Partnership within 60 days of issuance.
Stepchild •ChangeRequestForm •ProofofMarriage,orestablishmentofaDomestic Partnershiptostepchild’sparent/legalguardian
(copyofmarriagecertificateorDeclarationofDomesticPartnership*
If all required documentation is received before the 16 th day of the month of marriage/establishment of domestic partnership, premiums are charged for the full month and coverage begins on the date of marriage/establishment of domestic partnership. If all required documentation is received on or after the 16 th day of the month of marriage/establishment of domestic partnership, coverage begins on the 1st of the month following the date of receipt.
* If domestic partners have filed a Declaration of Domestic Partnership and have not yet received a copy from the state, a signed Affidavit of Domestic Partnership will be accepted. Domestic Partners agree to provide a copy of the Declaration of Domestic Partnership within 60 days of issuance.
If all required documentation is received before the 16 th day of the month of marriage, premiums are charged for the full month and coverage begins on the date of marriage. If all required documentation is received on or after the 16 th day of the month of marriage, coverage begins on the 1st of the month following the date of receipt.

17
Group Change GuidelinesThe following charts identify various changes you may make to your groupcoveragepolicy(whenpermitted)andthechangerequirements.Visitcalchoice.comtodownloadrequiredforms.
www.calchoice.com
Change in Group Policy
*1stofthemontheffectivedateonly.
Visitwww.calchoice.comtodownloadrequiredforms.
Mailorfaxcompletedformsto: CaliforniaChoice®721SouthParker,Suite200Orange,CA92868Fax:(714)558-8000
Change Type When Allowed* Deadline to Submit Requirements To Process
Address Atanytime None Oneofthefollowing:• Employer’swrittennotificationprovidingnewaddress
andspecifyingbillingand/orstreetaddressandreferencinggroupnumber.StreetaddresscannotbeaP.O.BoxoroutsideofCalifornia
• Onlineatwww.calchoice.com• EmployerChangeRequestForm
Buy-UpDentalMetLifeDHMO
MET100&MET185,SmileSaverDHMO
1000&3000,AmeritasPPO3000,3500,4000&5000
(Seepage31-32foreligibilityrequirements)
AtanytimeonceayearandatRenewal
25thofthemonthpriortorequestedeffectivedate(ifRenewal,within30daysofanniversarydate,butbenefitscannotbeaccesseduntilgroupreceiveswrittenconfirmationofapprovalfromCaliforniaChoice)
• DentalApplication• ReconciledQuarterly/AnnualWageReport
Chiropractic/AcupuncturePlan
(Change)
RenewalOnly Priortorequestedeffectivedate • EmployerChangeRequestForm
Chiropractic/AcupuncturePlan
(Add)
AtanytimeonceayearandatRenewal
Within30daysofrequestedeffectivedate
• EmployerChangeRequestForm
CompanyName Atanytime None • E-mailorletterheadfromauthorizedgroupcontactprovidinggroupnumber,newcompanynameandreferencingoldcompanyname
ContactPerson Atanytime None Oneofthefollowing:• Employer-writtenrequestprovidingcontactname,job
title,phone,faxande-mailandreferencinggroup#• Onlineatwww.calchoice.com• EmployerChangeRequestForm• GroupContactChangeRequest
Contribution RenewalOnly Within30daysofRenewal • EmployerChangeRequestForm• Employercontributionmustbeaminimumof50%of
thelowestcostplanavailabletotheemployeebasedonemployeeZIPCode
(CONTINUED)

FederalTaxIDNumber
LifeInsurance
MetalTier(s)
PayPeriodforEnrollmentQuote
Section125
TerminationofCoverage
VoluntaryDental
VoluntaryVision
WaitingPeriod
Atanytime
AtanytimeonceayearandatRenewal
RenewalOnly*
Atanytime
Atanytime
Atanytimewith30daysnotice
Atanytimeonceayear(butnottoreplacebuy-updental)andatRenewal
Atanytimeonceayear
RenewalOnly*
www.calchoice.com18
• E-mailorletterheadfromauthorizedgroupcontactprovidinggroupnumber,newtaxIDnumberandreferencingoldtaxIDnumber
• EmployerChangeRequestForm • ReconciledQuarterly/AnnualWageReport • EmployeeEnrollmentApplicationsforalleligibleemployees • CompletedStatementofHealthforalleligibleemployees ifrequestingamountaboveguaranteedissue(subjectto medicalunderwriting)
• EmployerChangeRequestForm • EmployeeEnrollmentApplications(fornon-enrolled
employeesonly) And/Or • EmployeeChangeRequestForms
• Employer-writtenrequest
Oneofthefollowing: • EmployerChangeRequestForm •OptionalBenefitsApplication(requestedeffective datemustbeincluded) • Employer-writtenrequesttoincludelastday ofcoverage
•DentalApplication • Mustenrolloneormoreemployees
• VoluntaryVisionApplication
•EmployerChangeRequestForm
*1stofthemontheffectivedateonly.
Requirements To ProcessDeadline to SubmitWhen Allowed*Change Type
Visitwww.calchoice.comtodownloadrequiredforms.
Mailorfaxcompletedformsto: CaliforniaChoice®721SouthParker,Suite200Orange,CA92868Fax:(714)558-8000
Change in Group Policy
None
25thofthemonthpriortorequestedeffectivedate(ifRenewal,within30daysofanniversarydate,butbenefitscannotbeaccesseduntilgroupreceiveswrittenconfirmationofapprovalfromCaliforniaChoice)
Aminimumof5businessdayspriortoRenewalDate
None(changeeffectiveuponentry)
None
30dayspriortorequestedeffectivedate(terminationwillbeeffectivenoearlierthanthelastdayofthemonthfollowingrequest)
25thofthemonthpriortorequestedeffectivedate(ifRenewal,within30daysofanniversarydate,butbenefitscannotbeaccesseduntilgroupreceiveswrittenconfirmationofapprovalfromCaliforniaChoice)
Within30daysofrequestedeffectivedate
Within30daysofRenewal

19
COBRA (Federal) andCal-COBRA (State) lawsallow for continuationof grouphealthbenefitstoindividualswholosecoverageasaresultofcertain“qualifying/triggeringevents”(e.g.terminationofemployment,deathofemployee,reductionof work hours, divorce, legal separation, Medicare entitlement, and loss ofdependentchildstatus).
Thelawdefines“grouphealthbenefits”asmedical,dental,chiropractic,vision,prescription drug programs, and any self-insured arrangements that providesimilar benefit coverage. These individuals are allowed to retain the types ofcoveragetheyhadpriortotheeventtakingplaceandmustbegiventhesamerightsasactiveeligibleemployeeswith respect toRenewalperiods,changingplansorbenefitsandaddingorterminatingdependents.
Employers Subject to COBRA (Federal)Generally,acompanyissubjecttotheprovisionsofFederalCOBRAif itoffersagrouphealthplanandhas20ormoreemployeesonat least50percentofitstypicalbusinessdaysduring the preceding calendar year.
Both full-time and part-time employees are considered as employees forpurposesofthisruleregardlessofwhetherornottheyareeligibleforcoverageunder the employer’s group health plan. However, under the 1999 final IRSregulations,anemployerisonlyrequiredtocountcommon-lawemployeeswhendeterminingwhether theymeet the20-employeerequirement.Self-employed individuals, agents, independent contractors and corporate directors are not treated as employees for COBRA purposes and need not be counted.Employers must aggregate employees from all divisions, subsidiaries and anyother entities that make up a controlled group of corporations. In general, acontrolled group of corporations may consist of a parent-subsidiary controlledgroup,brother-sistercontrolledgroup,oracombinedgroupasdefinedundertheIRSCodeSection414b.
In addition, under the 1999 final IRS rules, a part-time employee may becounted as a fraction of a full-time employee, with the fraction equal to thenumberofhoursanemployeemustwork inorder tobeconsidereda full-timeemployee, not to exceed 40 hours per week. Under these same rules,employers are also permitted to use daily or pay periodmethods of counting.
It isthesoleresponsibilityoftheemployertonotify itsemployeesormembersof the availability, terms, and conditions of COBRA continuation and providethem with the necessary information/forms for COBRA election. Suchresponsibilitywill be satisfied if the formermember is notifiedwithin 14daysafterthelastdayofcoverageundertheGroupPlan.
In thecaseof terminatingemployees/dependentsand lossofdependentchildstatus, uponproper notification, a letter fromCaliforniaChoice®will be sent tothe individual informing themtocontact theGroupPlanAdministrator toverifyiftheyareeligibleforCOBRAcontinuation.
COBRA enrollees will only be allowed to continue on their current coverage(Health Care Service Plan/Benefit Plan). Enrollees who expect to move toan area where their current Health Plan is not available should contact theCaliforniaChoiceCustomerServiceCenterat(800)558-8003.
COBRA Basics: n COBRA is designed to extend health benefits to people
who lose their coverage due to a COBRA Qualifying/Triggering Event
n Generally, a company is subject to the provisions of Federal COBRA if it offers a group health plan and has 20 or more employees on 50% of its “typical business days” during the preceding calendar year
n It is the sole responsibility of the employer to notify its employees or members of the availability, terms, and conditions of COBRA continuation
(CONTINUED)
About COBRA
www.calchoice.com

www.calchoice.com20
ThefollowingisabriefsummaryoftheCOBRAadministrationservicesofferedbyCONEXIS,adivisionofWageWorks,Inc.forCaliforniaChoicegroups:
1) Once CaliforniaChoice receives a COBRA Enrollment Application,CONEXIS (a company contracted by CaliforniaChoice) will senda confirmation of COBRA election letter and courtesy invoice toCOBRA enrollees. COBRA enrollees will be charged the currentpremiumineffectfortheemployer,butwithanadditional2%chargeforadministration.
2) For thedurationof thecontinuationcoverage,CONEXISwillsendacourtesy invoice to the COBRA participant for continuationcoveragepremiums.
3) COBRA participant payments collected by CONEXIS are forwardedtoCaliforniaChoice.
4) BecauseCOBRAEnrolleesmustbetreatedthesameasyouractiveeligible employees, COBRA enrollees will be allowed to amendcoverage for themselves and/or their dependents or add anyadditionalapplicablebenefitsofferedby the formeremployer. (Lifeinsurancenotincluded.)
5) CONEXIS will notify each COBRA participant of their possibleconversion and extension rights near the end of their COBRAcontinuationcoverageperiod.
6) CONEXIS will track each participant and notify them andCaliforniaChoiceofterminationoftheirCOBRAcoverage.
NOTE: The services listed above do not alleviate a group’sresponsibilities under COBRA law. These services only apply tonon-directbillgroups.
DirectBillGroups:GroupswhohaveelectedtobebilledfortheirCOBRAparticipants. For additional informationonDirectBill, pleasecontact ourCustomerServiceCenterat(800)558-8003.
COBRA Compliance Made Simple
Domestic Partner Eligibility under COBRADomestic Partners do not meet the definition of a Qualified Beneficiaryas defined under COBRA law. Therefore, Domestic Partners are not eligibleforthesameCOBRArightsasaQualifiedBeneficiary.
TheDomesticPartner is only eligible for COBRA Continuation of Coverage if he or she remains a dependent under the employee’s election.HeorshedoesnothaveaseparateelectionrightunderCOBRAlawbecauseheorsheisnotaQualified Beneficiary. If an employee experiences a COBRA qualifying/triggeringevent, theDomesticPartner isonlyeligible tocontinuehisorherhealth insurancebenefitsiftheemployeealsocontinueshisorherbenefitsunderCOBRA.Heorshecannot make an election separate from the employee. In addition, dependentqualifying/triggeringeventsdo not applytoDomesticPartners.
Employer Responsibilities for COBRA
n The employer must continue to comply with all COBRA requirements (including proper notification of all active planparticipants, notification of all qualified beneficiaries followingqualifying/triggeringevent,etc.)
n The employer must send a completed COBRA Enrollment Application to CaliforniaChoice® for all qualified beneficiaries who elect COBRA continuation coverage.(ThecompletedCOBRAenrollment application must be returned to the employer to forward
toCaliforniaChoicewithintheregulatedtimeframes.)
About COBRA

21www.calchoice.com
Employers Subject to Cal-COBRA (State)Generally, a company is subject to the provisions of Cal-COBRA if it offersa group health plan and only has 1 to 19 eligible employees on at least50percentofitstypicalbusinessdaysduring the preceding calendar year.All full-time employees, part-time employees and self-employed persons(e.g.partnersinalawfirm)areconsideredemployeesforthepurposesofthisrule regardless of whether or not they are eligible for coverage under theemployer’s group health plan. Leased employees also count as employees.However, all agents or independent contractors (and their employees, agentsand independent contractors), as well as corporate directors, are treated asemployeesonlyiftheyareeligibleforcoverageunderthegrouphealthplan.
Employersmust aggregateemployees fromall divisions, subsidiaries andanyother entities that make up a controlled group of corporations. In general, acontrolledgroupofcorporationsmayconsistofaparent-subsidiarycontrolledgroup, brother-sister controlled group, or a combined group as defined byIRSCodeSection414b.
UnlikeCOBRA,itistheresponsibilityoftheHealthPlanstosendoutnotificationsto former employees/dependents of their rights to continue coverage underCal-COBRA.TheHealthPlansintheCaliforniaChoice®programhavecontractedwith CONEXIS to provide those services. (See next page for information onCal-COBRAservicesofferedbyCONEXIS.)
Uponnotificationofaqualifying/triggeringevent,CONEXISwillautomaticallynotifythosemembersof theirCal-COBRA rightsbysendinganelectionnotice to thequalifiedbeneficiaries’lastknownaddressviafirstclassmailandgivethemtheopportunitytoelecttocontinuetheircoveragethroughCal-COBRA.
Domestic Partner Eligibility under Cal-COBRAUnderanewlawentitledtheInsuranceEqualityAct,effectiveJanuary1,2005,anycoverageofferedtothespouseofanemployeemustalsobeofferedtoaregistereddomesticpartner.
TheDomesticPartneriseligibleforCal-COBRAContinuationofCoverageandhasthesameelectionrightsasaspouse.
n Generally, a company is subject to the provisions of Cal-COBRA if it offers a group health plan and only has 1 to 19 eligible employees on at least 50% of its typical
business days during the preceding calendar year
n All full-time, part-time and self-employed persons (e.g. partners in a law firm) are considered employees
n Unlike COBRA, it is the responsibility of the Health Plans to send out notifications to former members of their rights to continue coverage under Cal-COBRA
Cal-COBRA Basics:
(CONTINUED)
About Cal-COBRA

www.calchoice.com22
About Cal-COBRAEmployee/Dependent ResponsibilitiesIfacovereddependentloseshisorhereligibilityduetodivorce,legalseparation,death of employee or loss of dependent child eligibility, the employee ordependent must notify CaliforniaChoice® of the event (within 60 days). Fordivorce, legal separation, or loss of dependent eligibility the employee mustsubmitaChange Request Form.Coveragewillbeterminatedattheendofthemonthfollowingthequalifying/triggeringeventdate.ThedependentmustsubmitaCOBRAEnrollmentApplicationtoelectCOBRA.
Employer Responsibilities for Cal-COBRA
n The Employer must notify CaliforniaChoice of employee address changeswithin30daysof theemployeeprovidingsuch information totheEmployer
n TheEmployermustnotifyCaliforniaChoiceofemployeeterminations,employee deaths, and reductions in hours that cause a loss ofcoveragewithin30daysof theevent takingplacebysubmittinganEmployeeTerminationNotificationForm.
The following is a brief summary of the Cal-COBRA administration servicesofferedbyCONEXIS,adivisionofWageWorks,Inc.forCaliforniaChoicegroups:
1) Following notification of termination of employment, employeedeath, or a reduction in hours, CONEXIS will send information
to the member including their Cal-COBRA rights and a Cal-COBRA electionform.
2) At this point CONEXIS will make arrangements for the Cal-COBRAenrolleestomaketheirpaymentsdirectlytoCONEXIS.
3) Cal-COBRA enrollees will be charged the current premium in effect with the employer, but with an additional 10% charge foradministration.
4) CONEXIS will notify Cal-COBRA enrollees of their options during theannualRenewalperiod.
BecauseCal-COBRAenrolleesmustbetreatedthesameasyouractiveeligible employees, Cal-COBRA enrollees will be allowed
to add any additional applicable benefits offered by the formeremployer as well as any eligible dependents not previously covered
underCal-COBRA(exceptlifeinsurancecoverage).
5) CONEXIS will notify each Cal-COBRA participant of their possibleconversionneartheendoftheirCal-COBRAcontinuationperiod.
6) CONEXIS will track each Cal-COBRA participant and notify them and CaliforniaChoice- of termination of their Cal-COBRA coverage.
Cal-COBRA Compliance Made Simple

23
Length of Eligibility for Continuation of CoverageIn September 2002, California passed a state law extending the maximumamountoftimeforcontinuationcoverageunderCal-COBRAregulations.
Under Cal-COBRA regulations, anyone with a Qualifying/Triggering EventresultingintheircontinuationcoverageperiodbeginningonJanuary1,2003or thereafter will be eligible for 36 months of coverage. COBRA coveragebeginningpriortothisdateisnoteligibleforthisextension.
If thegroup’scoveragethroughCaliforniaChoice®isterminated,allmembers,includingthosewhohaveelectedCOBRA/Cal-COBRAcontinuationcoveragewillbe terminated.Theemployer’sobligation to theCOBRA/Cal-COBRAqualifiedbeneficiariesistoprovidethemwiththesamecoveragecurrentlyprovidedtoactiveemployees.
A company’s obligation to comply with COBRA is the same regardless of the number of employees it has during the current year.
Health Insurance Portability and Accountability Act of 1996 (HIPAA)InOctober of1996, theHealth InsurancePortability andAccountabilityAct of1996 (HIPAA)wassigned into law. InApril of1997,Federal regulationswerepublishedtoassistPlanholders(Employers)tocomplywiththislaw.
Themajorcomponentsofthelawapplytomedicallyinsuredmembersandareasfollows:
n ACertificateofCoveragemustbeprovided toall insuredemployeesandtheirdependentswhentheircoverageends.CaliforniaChoicewillautomatically send this certificate upon termination and additionalcopiesuponrequest.
Employersare responsible fornotifyingCaliforniaChoiceofanemployee’snewaddress informationwithin 30 days of an address change. Because of theobligations imposed by Federal and State laws, CaliforniaChoice cannotbe responsible for misdirected HIPAA/COBRA/Cal-COBRA information as aresult of the failure to provide correct residence address information for allinsuredemployees.
NOTE: Life Insurance coverage may allow for disability extensions and policyconversion based on policy guidelines. The Employer is responsible for initialnotificationoftheserights.Formoreinformation,pleaseseeacopyofthemasterpolicyatwww.calchoice.comunder“DownloadForms,BrochuresandGuides”orcontactourCustomerServiceCenterat(800)558-8003.
Related COBRA Laws
Anyone with a Qualifying/Triggering Event resulting in their continuation coverage period beginning on January 1, 2003 may qualify for up to 36 months of coverage
www.calchoice.com

www.calchoice.com24
Your Premium StatementEach month you will receive a Premium Statement including your policyinformation and total balance due, Invoice Pages breaking down employeecoverage information and, if applicable, Invoice Adjustment Pages reflectinganychanges,creditsoradjustmentsmadetoyouraccount.
n POLICY INFORMATION reflects your current optional benefits,COBRA status,waitingperiod, renewal date andminimumhours foreligibility.The informationprovidedreflectsyouraccount informationasitexistsonrecordasofthestatementdate.
n The TOTAL OF CONTRACT BALANCE(S) DUE is always theoutstandingbalanceasofthestatementdate.Paymentsoradjustmentsmade after that date will be reflected on your next statement.
n YourINVOICE PAGESwilllistallemployeescurrentlyenrolledintheplan,includingtheiragesandZIPCodes,theircoverage,abreakdownoftheirpremiumsandemployercontributions.
n TheADJUSTMENT PAGEwillreflectemployeeplanchangesmadesincethelaststatement.Pleasepayspecialattentiontothisareatoverifyadjustments.
Youshouldalwaysreturntheremittanceportionofthepremiumstatementwithyour payment and indicate the group number on your check. Please do notstaple/tapeyourchecktotheremittanceportion.
Do not self-adjust or submit changes on your statement. Changes can onlybe processed using the correct forms. Please use the forms provided inyour administrative kit or log on to our website at calchoice.com. Forms canbedownloadedorprinted from thesiteandmaybeemailed, faxedormailedtoCaliforniaChoice®.
<P.S.>
What the Employee ChangeCodes Mean on Your StatementListedbelowaretheemployeechangecodesthatmayappearonyourstatements:
Billing
A AdditionAC AddCOBRAC ChangePlanCA ChangeAgeCE ChangeEnrollDateCI ChangeInformationCO CorrectionDA DependentAddDT DependentTerminationER EmployeeReinstatementGR GroupReinstatementIN InvoluntaryTerminationNT NewTerminationPP PartialPaymentTerminationRA RetroactiveAddRC RetroactiveChangePlanRDA RetroactiveDependentAdditionRDT RetroactiveDependentTerminationRE ResignationRT RetroactiveTerminationVC LifeVolumeChange
(CONTINUED)

25
The Billing CycleYour premium statements are produced by CaliforniaChoice® the1st of each month for the following month’s coverage. These statements aremailedand/ore-mailedtotheGroupContact.Hereisanexample:
n Premiumpaymentsneedtobereceivedbytheduedateindicatedoneachstatementandshouldbepaidasbilled.Adjustmentsprocessedafterthestatementdatewillreflectonyournextstatement.
n Allpaymentsareappliedtoyouroldestopenbalancefirst,with anyremainingportionbeingappliedtosubsequentbalances. n PaymentOptionsincludecheckbymailandon-linepayments(onetime
andrecurring). n Cutofftimeforpaymentsmadeon-lineis3:00pm(PST).Note:Premiumsarealwaysduepriortothemonthofcoverage.Medical Rate ScheduleThe groups medical rate schedule is guaranteed for the group’s plan year.Employee/dependentratesaresubjecttochangebasedonemployeequalifying/triggeringeventslistedonpage16.Life Rate SchedulesIndividual employee rates are subject to change based on employee age andlifeamount.
Credits/FeesIf there isacreditonyouraccountduetoanoverpaymentoradjustment, thecreditwillreflectontheinvoicefollowingthedateofthecredit.Theamountduefortheinvoicefollowingthecreditwillbereducedbythecreditamount.
TheadministrativefeeisbasedonthetotalnumberofemployeesenrolledinanycoveragethroughCaliforniaChoiceatthetimeofinvoicingandis,therefore,subjecttochangeonamonthlybasis.Administrativefeesareasfollows:
1-8 employees $30 9-50 employees $40 51+ employees $50
(In addition to the monthly administrative fee, CaliforniaChoice is remuneratedfromthesubscriberpaymentcollected)
Returned checks must be replaced immediately with a cashier’s checkor money order - company checks will not be accepted. There isa $25 fee for all returned checks. If there are 3 or more returned checkswithin a 12-month period, payment with certified funds will be requiredforoneyear.
Group CancellationsShouldpremiumpayment(s)notbereceivedinfullbytheduedate,a“NoticeofStartofGracePeriod”shallbesenttothegroupprovidinga30-daygraceperiodthat begins theday the “NoticeofStart ofGrace” isdatedand lasts at least30days.Ifpremiumpayment(s)arenotreceivedinfullbytheendofthegraceperiod,orapartialpaymentisreceived,yourcoverage(s)willbecancelledperthehierarchyincludedintheCaliforniaChoiceSupplementtotheGroupServiceAgreement(GSA).Cancellationofcoverage(s)willbeeffectivethedayafterthelastdayofthegraceperiod*,12:00midnight(PacificTime).Insuchacase,a“NoticeofEndofCoverage”willbemailed.Yourcoverage(s)willcontinueduringthegraceperiod;however,youarestill responsibletopayunpaidpremium(s)and any copayments, coinsurances, or deductible amounts as required underyourplancontract(s)throughthelastdayofcoverage..
*SincethemonthofFebruaryconsistsofonly28/29days,groupsthatdonotpayFebruary’spremiumby theendof the30-daygraceperiodwill terminateonthelastdayofMarch.
LIFE TABLE
0-1920-2425-2930-3435-3940-4445-4950-5455-5960-6465-6970-7475-7980-8485-8990-9495-99100+
www.calchoice.com
Billing
MEDICAL TABLE
0-1415-1516-1617-1718-1819-1920-2021-2122-2223-2324-2425-25
26-2627-2728-2829-2930-3031-3132-3233-3334-3435-3536-3637-37
38-3839-3940-4041-4142-4243-4344-4445-4546-4647-4748-4849-49
50-5051-5152-5253-5354-5455-5556-5657-5758-5859-5960-6061-61
62-6263-6364+

www.calchoice.com26
n Approximately60daysprior to thegroupanniversarydate,CaliforniaChoice®will send the renewalpremiumsbasedonyouremployees’currentHealthPlan/Benefitselections.Forexample:
DuringRenewal,youremployeeswillhavetheopportunitytochangetheircurrentHealthPlan/Benefitselectionsandaddeligibledependentsnotpreviouslycoveredontheprogram.Employeeswhopreviouslywaivedareeligibletoenrollatthistime.Coveragewillbemadeeffectivethefirstoftherenewalmonth.
YoumaycontactyourRenewalSpecialistforassistancewithyourgroup’srenewal.
Annual Renewal Timeline
JULY 1Company Anniversary Date
Requested Changesgo into effect
JUNE 1Renewal Ends
All Enrollment Applications or Change Request Forms need to
be received by this date
MAY 1Renewal Begins
Employer will receive renewal package by
this date

27
Dentegra® Smile ClubThisdentaldiscountprogramisavalue-added,start-upfeatureavailabletoEmployerswhodonotcurrentlyofferdentalcoveragetotheirEmployees.DentegraSmileClubmaybeincludedinyourbenefitspackageatnocosttotheemployeroremployees.ItisnotmeanttotaketheplaceofthemorecomprehensivedentalprogramsofferedbyCaliforniaChoice®orotherdentalproviders.
How It Works:
n NewemployeescanenrollinDentegraSmileClubbyfirstenrollinginCaliforniaChoicemedicalcoverage.Theycanthenvisitwww.calchoice.com,loginandclick“MemberValueSuite”.Thenregister*byclicking“JointheClub”andgetaDentegraSmileClubgroupIDnumbertoqualifyfordiscounts..
n Whenmedicalcoverageterminatesforanemployeeand/ordependents,coverageinDentegraSmileClubwillautomaticallyterminate.
*Ifyouhaveanyissueswithregistering,pleasecontactDentegraCustomerServiceat(877)280-4204.
Dentegra Smile Club Participation Requirements
Employer: MustcurrentlyoffermedicalcoveragethroughCaliforniaChoicetoalleligibleemployees
Nocurrentdentalplanbeingofferedtoanyemployees(byeitheranotherdentalcarrierorCaliforniaChoice)
Employee: Contingentuponemployereligibility,and:
EmployeemustbeenrolledintheCaliforniaChoicemedicalprogramandresideinCalifornia
Dependent: Contingentuponemployeeeligibility,and:
DependentmustbeenrolledintheCaliforniaChoicemedicalprogram
AllchangerequestssubmittedtotheCaliforniaChoiceProcessingCenterrelatedto medical coverage will automatically be reflected in Dentegra Smile Clubmembership.
<P.S.>
Ancillary and Voluntary Benefits
www.calchoice.com
(CONTINUED)

www.calchoice.com28
Our innovative mix of Optional and Voluntary benefits helps employers offer more coverage while limiting healthcare costs.
Voluntary Dental ProgramCaliforniaChoice®memberscanenroll inoneof the voluntarydentalplansbyAmeritas,MetLife andSmileSaverSM,with nominimumemployeeparticipation.Ameritas PPO benefits offer low deductible that allow members to visit anydentalprovidertheyprefer,in-orout-of-network.MetLifeandSmileSaverDHMObenefitsareavailable fora lowmonthlypremium(paidby theemployee)andofferfreeofficevisits,oralexams,X-raysandtwocleaningsperyear.
How It Works:
n New employee enrollment in EyeMed is automatic upon enrollment forCaliforniaChoicemedicaland/ordentalcoveragewithnomonthlypremium.
Voluntary Vision ProgramCaliforniaChoice members can enroll in one of the voluntary vision plansby EyeMed and VSP, both are provided by Ameritas in addition to theautomatic EyeMed Vision Discount Program. For a low monthlypremium (paid by the employee), the Voluntary Vision plans allow themto save additional costs related to exams, frames, lenses and more.
How Voluntary Plans Work:
n Theemployermustoffertheplan. n Theemployeemustpayforpremiums.
EyeMed Vision Discount Program (provided by Ameritas)All CaliforniaChoice medical and/or dental enrollees are automatically eligiblefor discounts on eye exams, lenses, frames, contacts and LASIK proceduresthroughtheEyeMedVisionDiscountProgram.Thesediscountsarehonoredatover2500locationsnationwide.Fordetails,gotowww.calchoice.com,select“Benefits”and“Vision.”
Ancillary and Voluntary Benefits

29
Chiropractic and Acupuncture ProgramsCaliforniaChoice®offerseachemployergroupachoiceoftwoChiropracticplans.One of those plans also includes Acupuncture services. These services areprovided through Landmark Healthcare. Please see our Optional Benefitsbrochure for plan details. You may contact our Customer Service Center at(800)558-8003orgoonlineatwww.calchoice.comforadditionalinformation.
How It works:
n Employerpays100%ofalowmonthlypremium.
n Once offered, employee/dependent enrollment is automatic uponenrollmentforCaliforniaChoicemedicalcoverage.
n When medical coverage terminates for an employee and/ordependents,thiscoveragewillautomaticallyterminate.
Ancillary BenefitsSection 125 Premium Only Plan (POP)*Electing this optional benefit allows the Employer to take salary deductionsforcertainhealthandinsuranceprogramsonapre-taxbasis.TheEmployee’sinsurance premium deduction (the amount the Employee pays towardmedical/dental insurance for himself and/or dependents) is taken out ofgrosswages.Byreducingthegrosswageamount,thisinturnreducespayrolltaxesforboththeEmployerandtheEmployees.
AtthetimeyourcompanycompleteditsinitialenrollmentintoCaliforniaChoice,youweregiventheopportunitytoelecttheSection125program.Ifyoudidnottakeadvantageof thisbenefitat that time,youmaystilladdtheSection125program.PleasecallourCustomerServiceCenteroryourinsurancebrokerforenrollmentinformation.
*Initialset-upfeeiscoveredatnocost.
Ifyourcompanydoesnotcurrentlyofferthesebenefitsandyouwouldlikemoreinformation,pleasecontactyourbroker.
<P.S.>Chiropractic and Acupuncture Participation Requirements
Employer: MustcurrentlyoffermedicalcoveragethroughCaliforniaChoice
Mustpay100%ofChiropracticplanpremium
Employee: MustbeenrolledintheCaliforniaChoicemedicalprogramandresideinCalifornia
Dependent: MustbeenrolledintheCaliforniaChoicemedicalprogramandresideinCalifornia
www.calchoice.com
(CONTINUED)
Claim Filing Procedures (Loss of Life)ClaimFilingRequirementsforEmployers:
1) ContactourCustomerServiceCenterat(800)558-8003
2) CompletetheLife,AD&DandWaiverofPremiumClaimInformationform#01-878-01114
3) CompletetheEmployeeTerminationNotificationForm
4) Oncetheaboverequirementsareallcompletedinfull,allitemsshouldbefaxedormailedtoCaliforniaChoiceattheaddresslistedbelow:
Attn:LifeClaims CaliforniaChoice 721SouthParker,Suite200 Orange,CA92868 Fax:(714)558-8000
www.calchoice.com30
Employee Life InsuranceAt the time your company completed initial enrollment into theCaliforniaChoice®program,youweregiventheopportunitytoprovideemployeelifeinsurancecoverage.
Ifyoudeclinedthiscoverageinitially,youareallowedtoaddemployeelifeinsurance at anytime throughout the year. Please contact your insurancebrokerforenrollmentrequirements.
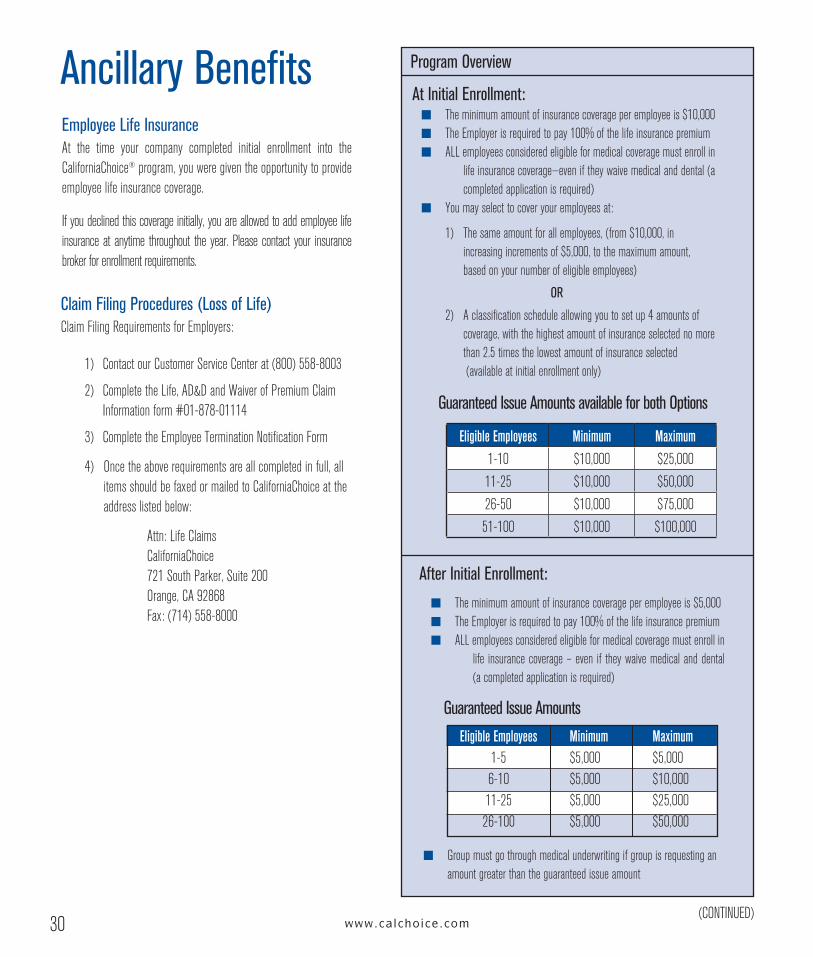
Ancillary Benefits Program Overview
At Initial Enrollment:
After Initial Enrollment:
Guaranteed Issue Amounts available for both Options
n Theminimumamountofinsurancecoverageperemployeeis$10,000n TheEmployerisrequiredtopay100%ofthelifeinsurancepremiumn ALLemployeesconsideredeligibleformedicalcoveragemustenrollin
lifeinsurancecoverage—eveniftheywaivemedicalanddental(acompletedapplicationisrequired)
n Youmayselecttocoveryouremployeesat:
1) Thesameamountforallemployees,(from$10,000,inincreasingincrementsof$5,000,tothemaximumamount,basedonyournumberofeligibleemployees)
OR
2) Aclassificationscheduleallowingyoutosetup4amountsofcoverage,withthehighestamountofinsuranceselectednomorethan2.5timesthelowestamountofinsuranceselected(availableatinitialenrollmentonly)
n Groupmustgothroughmedicalunderwritingifgroupisrequestingan amountgreaterthantheguaranteedissueamount
Guaranteed Issue Amounts
n Theminimumamountofinsurancecoverageperemployeeis$5,000n TheEmployerisrequiredtopay100%ofthelifeinsurancepremiumn ALLemployeesconsideredeligibleformedicalcoveragemustenrollin
life insurancecoverage–even if theywaivemedicalanddental(acompletedapplicationisrequired)
Eligible Employees Minimum Maximum
1-10 $10,000 $25,000
11-25 $10,000 $50,000
26-50 $10,000 $75,000
51-100 $10,000 $100,000
(CONTINUED)
Eligible Employees 1-5 6-10 11-25 26-100
Minimum $5,000 $5,000 $5,000 $5,000
Maximum$5,000$10,000$25,000$50,000

Employee Dental InsuranceAtthetimeyourcompanycompletedinitialenrollmentintotheCaliforniaChoice®program,youweregiventheopportunitytoprovideemployeedentalcoverage.Ifyoudeclinedthiscoverageinitially,youareallowedtoaddemployeedentalinsuranceatanytimethroughouttheyear,subjecttounderwriting.Pleasecontactyourinsurancebrokerforenrollmentrequirements.
31
Ancillary Dental
www.calchoice.com
(CONTINUED)
MetLife DHMO MET100 & MET185, SmileSaver DHMO 1000 & 3000, Ameritas PPO 3000, 3500†, 4000†, & 5000†
†Onlygroupswith5ormoreeligibleemployeesqualifyforOrthodontiabenefits
Participation Requirements
Employer
Employee EligibilityiscontingentuponEmployereligibilityANDthefollowing: n Expectedtomeettheestablishedwaitingperiod n Permanentandactivelyworkinganaverageof30+hoursperweekoverthecourseofamonth,atthesmallemployer’s
regularplaceofbusinessor20+hourspernormalworkweekforatleast50%oftheweeksinthepreviouscalendarquarter n Paidonasalary/hourlybasis(not1099,commissioned,orsubstitute) n Employeeshiredafterplaninstallmentaresubjecttothewaitingperiod
Dependent Spouse EligibilityiscontingentuponEmployereligibilityANDthefollowing: n LegallymarriedtotheEmployee
n CurrentlyofferingmedicalcoveragethroughCaliforniaChoicetoalleligibleemployees n Nocurrentdentalplanbeingofferedtoanyemployees(byanotherdentalcarrier) n 1-2Employees:100%ofallemployees.Allgroupsmustincludeatleastonedentalenrolledemployeewhoisnotabusinessowneror
spouseofbusinessowner 3-100Employees:70%ofeligibleemployeesenrollinginCaliforniaChoice n Employeeswithothergroupcoveragearenotcountedtowardsparticipationunlessemployercontributionis100% n TheEmployermustcontributeaminimumof50%oftheEmployeepremiumofthelowestcostdentalplanavailabletoemployees n EmployeesselectingDental3000,3500,4000or5000aresubjecttoa12-monthwaitingperiodformajorservices;12 monthsforOrthodontia.Takeovercreditisavailabletogroupsconsistingof10+eligibleemployeeswithcomparableprior groupdentalplanandnolapseincoverage n EmployermustsubmitthefollowingtoreceivetakeovercredittowardswaitingperiodformajorservicesandOrthodontia: •Priordentalbillingstatement(nolapseincoverageallowed) •Priordentalbillingstatementfrom12monthspriororfirststatementifcoveragehasbeeninforcelessthan12months •Priordentalbillingstatementfrom12monthspriorfororthodonticoption.Statementmustshowbenefitsforothrodontia n Deductibletakeoverisnotavailable

www.calchoice.com32
Ancillary DentalMetLife DHMO MET100 & MET185, SmileSaver DHMO 1000 & 3000, Ameritas PPO 3000, 3500†, 4000†, & 5000†
†Onlygroupsof5ormoreeligibleemployeesqualifyforOrthodontiaBenefits
Domestic Partner EmployeeandDomesticPartnermustfallintoallofthefollowingcategories:
n BothhavefiledadulyexecutedDeclarationofDomesticPartnershipwiththeSecretaryofStateandwillprovidecopiestoCaliforniaChoice®within60daysofitsissue
n AgreetonotifyCaliforniaChoiceimmediatelyuponterminationofdomesticpartnershipForCOBRA/Cal-COBRAeligibilityinformationforDomesticPartnersandtheircovereddependents,pleaseseepages20-22
Dependent Children
DisabledDependents:
Dependentswhoareincapableofself-supportbecauseofcontinuousmentalorphysicaldisabilitythatexistedbeforetheagelimitareeligibleforcoverageuntiltheincapacityends.Documentationofdisabilitywillberequested.Oncethechildreachestheagelimitforcoverage,verificationofeligibilitywilloccurannuallyatthechild’sbirthday.
Dependents must meet all requirements listed in order to be eligible for enrollment
METLIFE and SMILESAVERDENTALDependenteligibility:n Born to,astep-childor legalwardof,adoptedby,onoriginal request,orhaveanestablishedparent-child
relationshipwiththeeligibleemployee,employeespouseordomesticpartnern Underage26(unlessdisabled,disabilitydiagnosedpriortoage26)
AMERITASDENTALDependenteligibility:n Born to, a step-childor legalwardof, adoptedby, onoriginal request orhaveanestablishedparent-child
relationshipwiththeeligibleemployee,employeespouseordomesticpartnern FinanciallydependentupontheemployeeperIRSguidelinesn Unmarriedornotinvolvedinadomesticpartnershipn Underage26(unlessdisabled,disabilitydiagnosedpriortoage26)
(CONTINUED)

33
How to Contact the Customer Service Center for Ancillary (Buy-Up) Dental Plans
EmployersshouldcalltheCaliforniaChoice®CustomerServiceCenterat(800)558-8003iftheyhavequestionsrelatedtoadministrativeprocedures.
MetLife DHMO MET100, MET185 and SmileSaver DHMO 1000, 3000
Issue:
MetLife and SmileSaverSM, Customer Service:(800) 880-1800
n HavenotreceivedtheirpermanentIDcard(s)within3-4weeksafterreceiving theirconfirmationofacceptanceletter
n NeedtoreplacealostIDcard(s)
n Havequestionsabouthowtousetheplan
n Havequestionsaboutbenefits
n Haveaproblemorcomplaintrelatedtoservice
n ReceiveabillfromtheirDentalOfficeoranyotherdentalfacilityforservices approvedbytheirDentalOffice
n NeedtofileaclaimforEmergencydentalservices
Employeeshouldcontact:
Ameritas PPO 3000, 3500, 4000, & 5000
CaliforniaChoice Customer Service Center:(800) 558-8003
n Needclaimforms
Ameritas(877) 203-0036
n Haveaquestionaboutbenefits
n Wanttoinquireaboutasubmittedclaim
Issue: Employeeshouldcontact:
www.calchoice.com
Ancillary Dental

www.calchoice.com34
Frequently Asked Questions General Information
Who is CaliforniaChoice®?CaliforniaChoiceistheTPA(ThirdPartyAdministrator)thathasbroughtseveralinsurance companies together to allow you and your employees the ability toselectdifferentplansofhealthcoverage.
Who is the Group Plan Administrator?TheGroupPlanAdministrator istheemployeeselectedbyyourcompanytobethemaincontacttoCaliforniaChoice.
Who is my Health Plan?Your Health Plan is the participating insurance company you selected underthe CaliforniaChoice program to provide your health care. Each one ofyour employees made his or her selection during initial enrollment(i.e., Anthem Blue Cross, Cigna + Oscar, Health Net, Kaiser Permanente, Oscar,SharpHealthPlan,SutterHealthPlus,UnitedHealthcare,WesternHealthAdvantage).
Can a member change their health plan or benefit plan?Yes, during the annual renewal period or when the employee moves to anareawhere therearenomedicalprovidersunder thecurrenthealthplan. (It isimportanttonotifyCaliforniaChoiceofanaddresschangeimmediately.)
Iftheemployeeexperiencedaqualifying/triggeringevent(seepage15foralistofqualifying/triggeringevents),CaliforniaChoicewillallowtheemployeetochangehisorherhealthplan/benefitplanoutsideoftheirrenewalperiod.Seepage16forfurtherdetails.
Can each family member select a different health plan?No,allfamilymembersmustselectthesamehealthplan,howevereachmembermaychooseadifferentPrimaryCarePhysician(PCP).
What is my benefit plan?Thelevelofcoverage/benefitsisonyourenrollmentapplication(i.e.,HMO,EPO,andPPOplans).
Can each family member select a different benefit plan?No,allfamilymembersmustselectthesamebenefitplan.
When can dependents obtain coverage?Eligible dependents may be added at the employee’s initial enrollment, whenacquired (newborn/adoption/marriage/domestic partnership), or during the annualrenewalperiod.Otherthanduringtheannualrenewalperiod,*dependentsmayonlybeaddedwhenfirsteligible(i.e.,newbornsandnewlyacquireddependentsmaybeenrolledwithin60daysofthequalifying/triggeringevent:dateofbirth,adoption,marriage,domesticpartnership).Pleasereferto“NewDependent(s)Enrollment”onpage16forinstructions.
What is an Orientation Period?EmployersofferinggroupcoveragemaychoosetoimposeanOrientationPeriodthatisnotlongerthan“onemonth”asdefinedin45 CFR 147.UseofOrientationPeriodsareateachemployer’sdiscretion;however,theyshouldnotbeexecutedinanattempttodelayhealthenrollment.EmployersshouldbeabletosupportthattheirOrientationPeriodsareforlegitimatebusinesspurposessuchasorientationcertificationortraining.
Does the Orientation Period Count Against the Waiting Period?No,theWaitingPeriodstartsthedayaftertheOrientationPeriodends.
When is my company’s annual renewal?Your company’s annual renewal period is usually two months prior to theanniversarydate(yourcompany’sinitialeffectivedate).Allchangesmadeduringtheannualrenewalareeffectiveonthecompany’sanniversarydate.CheckwiththeGroupPlanAdministratorfortheexactdate.
What payment options do I have?Youcanmailinacheckorlogintoyouraccountatwww.calchoice.comtomakeaone-timeonlinepaymentorset-uprecurringpayments.
*See“LateEnrollee”onpage9forfurtherinformation.
(CONTINUED)
35
HMO
What is a copayment?The amount the member must pay for medical services (doctor visits, drugprescriptions,hospitalizations,etc.).
Who/What is my Primary Care Physician?APrimaryCarePhysiciancanbeafamilypractitioner,internist,orpediatrician.Atthetimeofenrollment,youmayhaveselected(orbeenassigned)aPrimaryCare Physician for yourself and each dependent. The Primary Care Physiciancoordinatesallhealthcareandmedicalneeds includingbasiccare,preventiveservices,referralstospecialists,andhospitalizationarrangements.
Can each family member select a different Primary Care Physician?Yes,eachfamilymembermaychooseadifferentPrimaryCarePhysicianwhoisbestsuitedtohisorherneeds(i.e.,theemployeeandspousemaywanttoselectageneralpractitioner,whileselectingapediatricianfortheirdependentchildren).
Can I change my Primary Care Physician?Yes; contact your Health Plan’s Member Services Department using thephonenumber on yourmedical ID card.Plansmay allow you to change yourPCPthroughtheirwebsite(somerestrictionsmayapply).
What if I need to see a specialist?Under the HMO plans, your Primary Care Physician, in consultation with acontractedMedicalGrouporIPA,willdeterminethepropertreatmentandmakereferrals to specialistswhennecessary.Achange inPrimaryCarePhysicianorHealthPlancouldcauseaproblemifyouareinthemiddleofspecialisttreatment.
What if medical services are needed before medical ID cards are received?Themembershouldpresenthisorherwelcomeletter,whichhighlightsbenefitcoverage; to thePrimaryCarePhysician selected for services. Thephysician’sofficemaythencontactCaliforniaChoicetoassistwithverifyingcoverage.
What if a prescription is needed before medical ID cards are received?ThemembershouldmakesurethepharmacyheorshewishtouseworkswiththeirHealthPlan.Thememberwillneedtopaythefullamountoftheprescriptionup-front, but may request reimbursement by retaining the paid receipt andcontactingtheHealthPlan’sMemberServicesDepartment.
What if I have an emergency situation?In the event of any emergency, contact your Primary Care Physician first.Dependingonthenatureoftheemergency,yourphysicianwilleither:helpoverthephone;makeanappointmentforyoutocomeinassoonaspossible;ormakeareferraltoanemergencyroomorurgentcarefacility.
Iftheemergencyislifethreatening,suchasaheartattack,oriscriticallyserious,suchasabroken leg,godirectly to thenearestmedical facility.However, you(orafamilymember)mustcontactyourPrimaryCarePhysicianwithin24hours.IfyouareunabletogetintouchwithyourPrimaryCarePhysician,contacttheHealthPlan’sMemberServicesDepartmentonyourIDcard.
If hospitalization is necessary, which hospital will I use?PrimaryCarePhysiciansworkwith specifichospitals; checkyour IDcard, theproviderdirectory,oraskyourPrimaryCarePhysician.Inanemergencysituation,alwaysgotothenearestavailablehospital.
What if I need to see a doctor while away from home?IfyouareawayfromhomeandcannotseeyourPrimaryCarePhysician,youwillonly be covered for emergency treatment that ismedically necessary. ContactyourPrimaryCarePhysicianfirsttoobtainauthorization.Ifyouareunabletogetin touch with your Primary Care Physician, contact the Health Plan’s MemberServicesDepartmentonyourIDcard.
What if I receive a bill?Althoughyoushouldnotreceivebills formedicalcareprovidedorapprovedbyyourPrimaryCarePhysician,youmayreceiveabillinerror.Inthatevent,contactyourHealthPlan’sMemberServicesDepartmentforassistance.
(CONTINUED)
www.calchoice.com
Frequently Asked Questions

PPO Plans
What if a prescription is needed before medical ID cards are received?The member should make sure the pharmacy he or she wish to use iscontractedwiththeselectedhealthplan.Someplansrequireadeductiblebemetpriortoprescriptioncopays.Thememberwillneedtopaythefullamountof theprescriptionup-front,butmayrequestreimbursementbyretainingthepaidreceiptandcallingtheHealthPlan’sMemberServicesDepartmentafteramedicalIDcardhasbeenreceived.
If hospitalization is necessary, what hospital will I use?The accredited hospital you choose to use is up to you, but remember thatmedical services will be covered at a greater percentage at those hospitalslistedinyourprovidernetwork.CheckwithyourHealthPlan’sMemberServicesDepartmentifyouareunsureifthehospitalyouareconsideringisaproviderinthenetworkforyourHealthPlan.Inanemergencysituation,alwaysgotothenearestavailablehospital.
Dentegra® Smile Club
What is Dentegra Smile Club?Dentegra Smile Club is not insurance; it is a no-cost membership wellnessprogram that allows members to receive negotiated discounted rates fromDentegra network dentists. Because it is not a dental insurance product,membersareresponsibleforallpaymentstoprovidersforanyservicesrendered.MembershipisavailableonlyinCaliforniaandTexas.
I’m not enrolled in the medical program. Can I (or my dependents) join Dentegra Smile Club? No, only those persons who are enrolled in the medical program qualify forDentegraSmileClubmembership
Can each family member go to a different dental office? Yes. Familymembersmay visit thedental officeof their choice, however, thefacilityanddentistmustbeaDentegraSmileClubprovider.
Who should I call with questions about coverage?Members can call Dentegra customer service at (877) 280-4204 or visitwww.dentegrasmileclub.comifthey:
n NeedtoreplacealostIDcard(s) n Havequestionsabouthowtousetheplan n Needtoobtainalistofdentalofficesintheirarea.
www.calchoice.com36
Frequently Asked Questions

37www.calchoice.com
Frequently Asked Questions MetLife DHMO MET100, MET185 or SmileSaver DHMO 1000, 3000
What is my dental plan design?MetLifeDHMOMET100orMET185orSmileSaverDHMO1000or3000.
May I or my dependents obtain MetLife or SmileSaver DHMO coverage, but not be enrolled in the medical program?Yes.
Can each family member go to a different dental office?Yes, each family member can go to a different dental office/dentist. If youand/or your dependents would like to switch dental offices/dentists, contactCustomerServiceDepartmentat(800)880-1800.
What if I receive a bill?Although you should not receive bills for dental care provided or approved byyour dental office, you may receive a bill in error. Contact the Customer ServiceDepartmentat(800)880-1800forassistance.
Ameritas PPO 3000, 3500, 4000, & 5000
May I or my dependents obtain Ameritas PPO coverage but not be enrolled in the medical program?Yes.
Can each family member go to a different dental office?Yes,eachfamilymembercangotoadifferentdentaloffice/dentist.
What if I need to see a dentist while away from home?Youarenot restricted toseeanyspecificdentist. However, thebenefitswillbecoveredataloweramountformajorservicesprovidedbyanon-contractingdentist.
What if I receive a bill?Ifyoutakeyourclaimformwithyoutoyourdentalvisit,thedentistwillgenerallycompleteallofthepaperworkandsendyouabillonlyfortheamountyouareresponsibletopay.

38
MailSuppliesTo:
Attn: _____________________________________________________
CompanyName:_______________________________________________
Address:___________________________________________________
Phone#:___________________________________________________
Group#:____________
This Form May Be Photocopied and Used As Necessary
Formscanalsobedownloadedatwww.calchoice.comafteryouremployerlogin.
Date:____________
MailorFaxSupplyRequestFormTo:
CaliforniaChoiceSupplyRequest721SouthParker,Suite200,Orange,California92868FAX(714)953-4097
QuantityQuantity
www.calchoice.com
Pleasebeadvised that some formsandwrittencommunicationsareavailable onourwebsite
in the following languages: Chinese, Korean, Russian, Spanish, Tagalog, and Vietnamese.
Employees can register their applicable, Plan-specific preferred language by completing the
LanguageAssistancePreferenceFormalsofoundonourwebsite(www.calchoice.com).
_____ ChangeRequestForm
_____ DeathClaimPacket
_____ Misc.
_____ EmployerChangeRequestForm
_____ EmployeeEnrollmentPacket
_____ NewHireEnrollmentQuoteRequestForm
_____ COBRA/Cal-COBRAEnrollmentForm
_____ AffidavitofDomesticPartnership
Supplies Requested:
CaliforniaChoiceSupply Request Form

39

A CALIFORNIA
DIFFERENT WAY To Do Health Care
800.558.8003www.calchoice .comCC.0230_7.21_Eff.7.1.21 License # 0B42994 – CaliforniaChoice Benefit Administrators, Inc.